Back to Journals » International Medical Case Reports Journal » Volume 16
Perioperative Anesthesia Management for Pregnant Mother with Multivalvular Heart Disease and Moderate Pulmonary Hypertension Who Underwent Caesarean Section, in Resource Limiting Area 2022: A Case Report
Authors Adare OE, Seife MA, Abate LG ![]()
Received 26 January 2023
Accepted for publication 18 May 2023
Published 22 May 2023 Volume 2023:16 Pages 311—317
DOI https://doi.org/10.2147/IMCRJ.S405699
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Professor Ronald Prineas
Video abstract presented by Minda Abebe Seife.
Views: 175
Oliyad Eshetu Adare,1 Minda Abebe Seife,1 Lamesgen Geta Abate2
1Department of Anesthesia, College of Medicine and Health Sciences, Hawassa University, Hawassa, Ethiopia; 2Department of Anesthesia, College of Medicine and Health Sciences, Debre Markos University, Debre Markos, Ethiopia
Correspondence: Minda Abebe Seife, Email [email protected]
Introduction: As measured by a right heart catheterization, pulmonary hypertension is an increase in mean pulmonary arterial pressure of more than 25 mmHg at rest or more than 30 mmHg during exercise. Some of the cardiac heart conditions that may develop during pregnancy include severe mitral regurgitation and mild tricuspid regurgitation. Prior to delivery, pregnant patients with pulmonary hypertension and significant multivalvular heart disease need to undergo careful preoperative, multidisciplinary assessment, and anaesthetic planning to maximize cardiac function during the peripartum period and make informed decisions about the delivery mood and anaesthetic technique.
Case Presentation: A 30-year-old Para two Gravid three pregnant mother presented with chronic rheumatic heart disease, severe mitral regurgitation, moderate pulmonary hypertension, severe left atrial dilatation, mild aortic regurgitation, and mild tricuspid regurgitation scheduled for elective cesarean section. She had one previous cesarean section four years ago with an indication of fetal macrosomia. Her cardiac condition, however, was moderate mitral regurgitation, mild left atrial dilatation, mild pulmonary hypertension, and no tricuspid or aortic regurgitation. She had continuous follow-ups after diagnosis until now but has not taken any medication.
Conclusion: Anaesthesia management in a patient with severe mitral regurgitation, moderate pulmonary hypertension, severe left atrial dilatation, mild aortic regurgitation, and mild tricuspid regurgitation was challenging in resource limited area. Even if spontaneous delivery is recommended for the patients with cardiac findings, a cesarean delivery will need in the area where limited access to support it. Goal-directed perioperative management with multidisciplinary involvement helps the patient to have a good outcome.
Keywords: pulmonary hypertension, multivalvular heart disease, low dose bupivacaine, transabdominal nerve block, anesthesia management, case report
Introduction
Pulmonary hypertension is defined as an increase in mean pulmonary arterial pressure of more than 25 mmHg at rest1 or more than 30 mmHg with exercise, as measured by echocardiography or right heart catheterization.2,3 It is associated with pulmonary vascular vessel conversion, narrowing of blood vessels, and thrombosis. The etiological agent can be idiopathic, such as in collagen vascular disease, congenital systemic (such as pulmonary shunts), human immunodeficiency virus (HIV) infection, or medication.2 Pulmonary hypertension is a sporadic illness that occurs during pregnancy and might cause high maternal morbidity and mortality.4,5 Our case report is in line with SCARE Guidelines.6
Analgesics with pulmonary vasoconstriction, such as nitrous oxide, should be avoided while treating spontaneous labour in pregnant women with pulmonary hypertension. Due to anesthesia-induced vasodilation, which lowers RV preload, lowers coronary artery perfusion pressure, and worsens leftward septal shifting, general or regional anaesthesia during a caesarean section can impact either the right or left ventricle’s ability to pump blood.7,8
The cardiac valve heart disorders that might develop during pregnancy include severe mitral regurgitation and moderate tricuspid regurgitation. The goals of anaesthesia management for pregnant patients with severe mitral regurgitation include preventing an increased SVR, maintaining a normal to slightly elevated heart rate, sinus rhythm, treating acute atrial fibrillation, avoiding aortocaval compression, maintaining venous return, avoiding myocardial depression during general anaesthesia, and avoiding an increased PVR. Mothers with mitral regurgitation benefit from reflex tachycardia brought on by spinal anaesthesia because it causes arteriolar dilatation, which lowers SVR.4,9
Prior to delivery, pregnant patients with pulmonary hypertension and significant multivalvular heart disease need to undergo careful preoperative, multidisciplinary assessment, and anaesthetic planning to maximize cardiac function during the peripartum period and make informed decisions about the delivery mood and anaesthetic technique.4 In patients with severe mitral regurgitation, labour and delivery should be performed under carefully titrated regional anaesthesia and invasive hemodynamic monitoring.10
This case report aims to describe perioperative anesthesia management of patients with rheumatic heart disease, moderate pulmonary hypertension, severe mitral regurgitation, moderate tricuspid regurgitation, mild aortic regurgitation and left atrium dilatation requiring emergency cesarean section in resources limited area.
Case Report
Thirty years-old Para two Gravida three gestational ages of 39 weeks and 4-day pregnant mother currently presents with chronic rheumatic heart disease, severe mitral regurgitation, moderate pulmonary hypertension, severe left atrial dilatation, mild aortic regurgitation, and mild tricuspid regurgitation scheduled for elective caesarean section. She had one previous caesarean section four years ago with an indication of fetal macrosomia. Her cardiac condition, however, was moderate mitral regurgitation, mild left atrial dilatation, mild pulmonary hypertension, and no tricuspid or aortic regurgitation. The patient had continuous follow-up after diagnosis until now but has not taken any medication since 8 years ago.
On the preoperative assessment, the mothers had shortness of breath during exercise, exercise intolerance after 1 year, an intermittent productive cough, and a history of anaesthesia. Otherwise, she had no history of hypertension, diabetes mellitus, asthma, or a central nervous system disorder. Her vital signs were 110/70 mmHg non-invasive blood pressure, 90 beats per minute heart rate, 20 breaths per minute respiratory rate, and 36.7 °C temperature. On her entire preoperative follow-up, her blood pressure was in the lower border and maximum of 110/70 and the remaining blood pressure was less than this value. She appeared healthy, with adequate mouth opening and Mallampati class 1. Her atlantoccipital and temporomandibular joints were functional, had no tenderness, could move freely in all directions, and could bite her upper lip without difficulty. The spine examination was normal. Graham Steele heard a murmur in the left upper lobe during chest auscultation, and the third heart sound (a holosystolic (pansystolic) murmur) was heard at the apex via the diaphragm of the stethoscope in the left lateral decubitus position.
The patient’s CBC was 12.8 g/dl, Hct was 38%, and Plt was 176 x 103/l, according to the laboratory results. WBC was 6.3 x 103/l, RBC was 4.36 x 106/l, BG-O +ve organ function test Cr 0.4 mg/dl, SGPT 13.6 u/l, SGOT 20.5 u/l, and electrolytes were normal. ECG results showed a left atrial abnormality. Echocardiography presented chronic rheumatic heart disease: severe left atrial dilatation (68 mm), severe mitral regurgitation, mild aortic regurgitation, mild tricuspid regurgitation, moderate pulmonary hypertension, and an ejection fraction of 65% as shown in (Table 1).
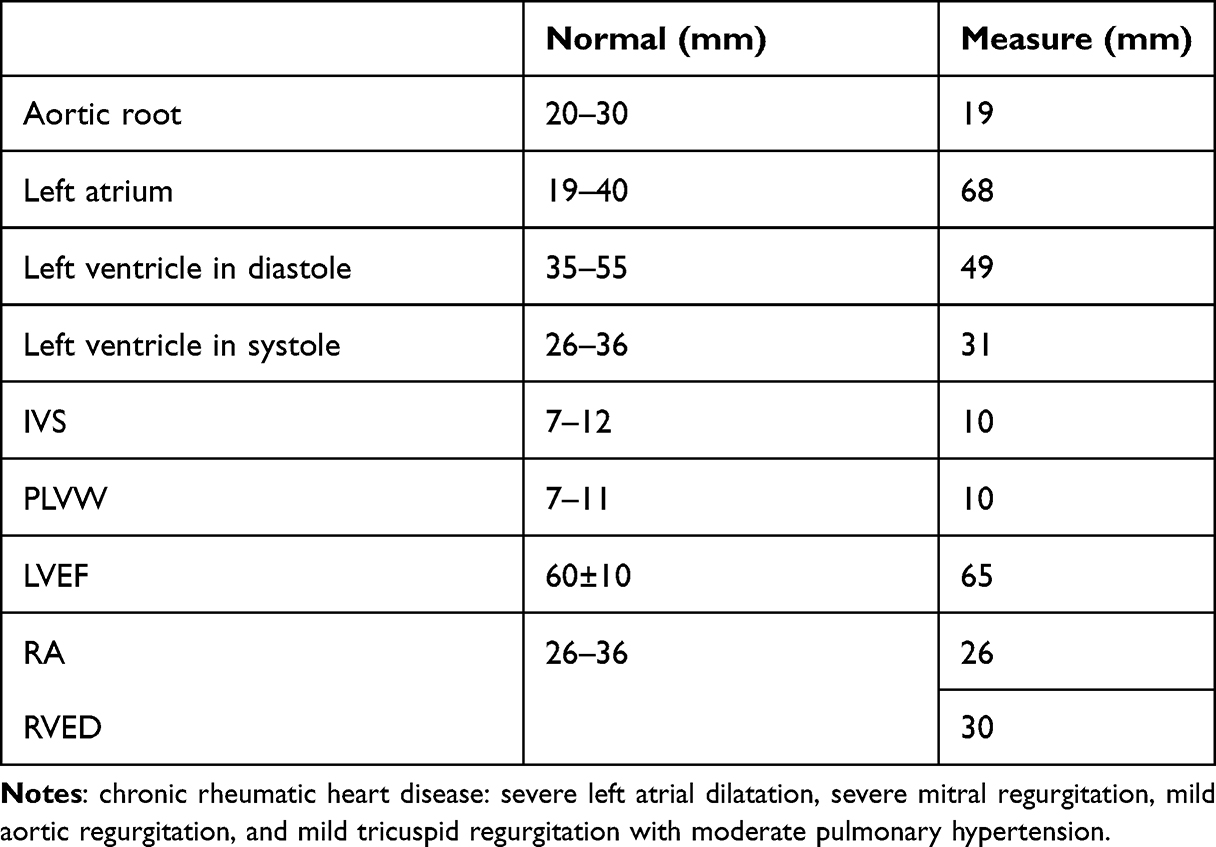 |
Table 1 30 Years Old with Chronic Rheumatic Heart Disease and Moderate Pulmonary Hypertension Pregnant Mother’s ECHO Finding Details |
When the patient had been fully informed of the advantages and disadvantages of anaesthesia and surgery, she accepted her ASA Class III status before having her formal informed consent obtained. She transferred to the operating room after obtaining bilateral large-bore IV access. Apart for capnography, the patient was being monitored per usual procedure.
The patient’s vital signs at baseline were 102/61 mmHg BP, 90 bpm HR, 36.5 oC Toc from axilla, and 97% oxygen saturation. We intend to administer lower-dose local anaesthesia with opioid spinal anaesthesia along with trans-abdominal (TAP) block because we are a developing nation and do not currently have an epidural anaesthesia kit or an IV anaesthesia agent on hand to maintain the anaesthesia goal for mitral regurgitation and moderate pulmonary hypertension.
After assessing the location of the needle insertion and performing local infiltration with 2% plain lidocaine while seated, spinal anaesthesia was administered using a rigorously aseptic procedure. After a free flow of CSF and negative blood aspiration, 7.5 mg of heavy bupivacaine + 0.1 mg of morphine were administered via a 24G spinal needle as spinal anaesthesia between the L4 and L5 interspaces. The patient was placed in the supine position, and before making the skin incision, a TAP block with a 0.125% solution (40 mL of bupivacaine) was administered bilaterally. The level of T6 was reached with the spinal blockade. 2 L/min of supplemental oxygen was given through a nasal catheter immediately after spinal anesthesia and supine position (Figure 1)
 |
Figure 1 Summary of intraoperative supplemental oxygen given to 30 years old with chronic rheumatic heart disease and moderate pulmonary hypertension pregnant mother. |
Surgery started after 15 minutes of spinal anesthesia. Following the delivery of the baby, 10 IU of oxytocin IM were administered as uterogenic drugs. The uterus was remained relaxed after 10 IU of oxytocin, therefore the gynaecologist requested more oxytocin, but the patient’s blood pressure was borderline low. Misoprostol 600 mg sublingually was used to prevent hypotension brought on by oxytocin and to promote uterine contraction. Furosemide was given intraoperatively to prevent further exacerbation of pulmonary hypertension.11 In the first five minutes of delivery, the neonatal Apgar score was 9–10/10. It took 45 minutes to complete the procedure.
Total amounts of fluid, blood loss, and urine output were 1500 mL, 400 mL, and 300 mL, respectively. Throughout, we have not encountered any complications associated with spinal anaesthesia. The intraoperative time was mostly uneventful with the exception of a slight tachycardia relative to her baseline heart rate for the first 4 minute (Table 2).
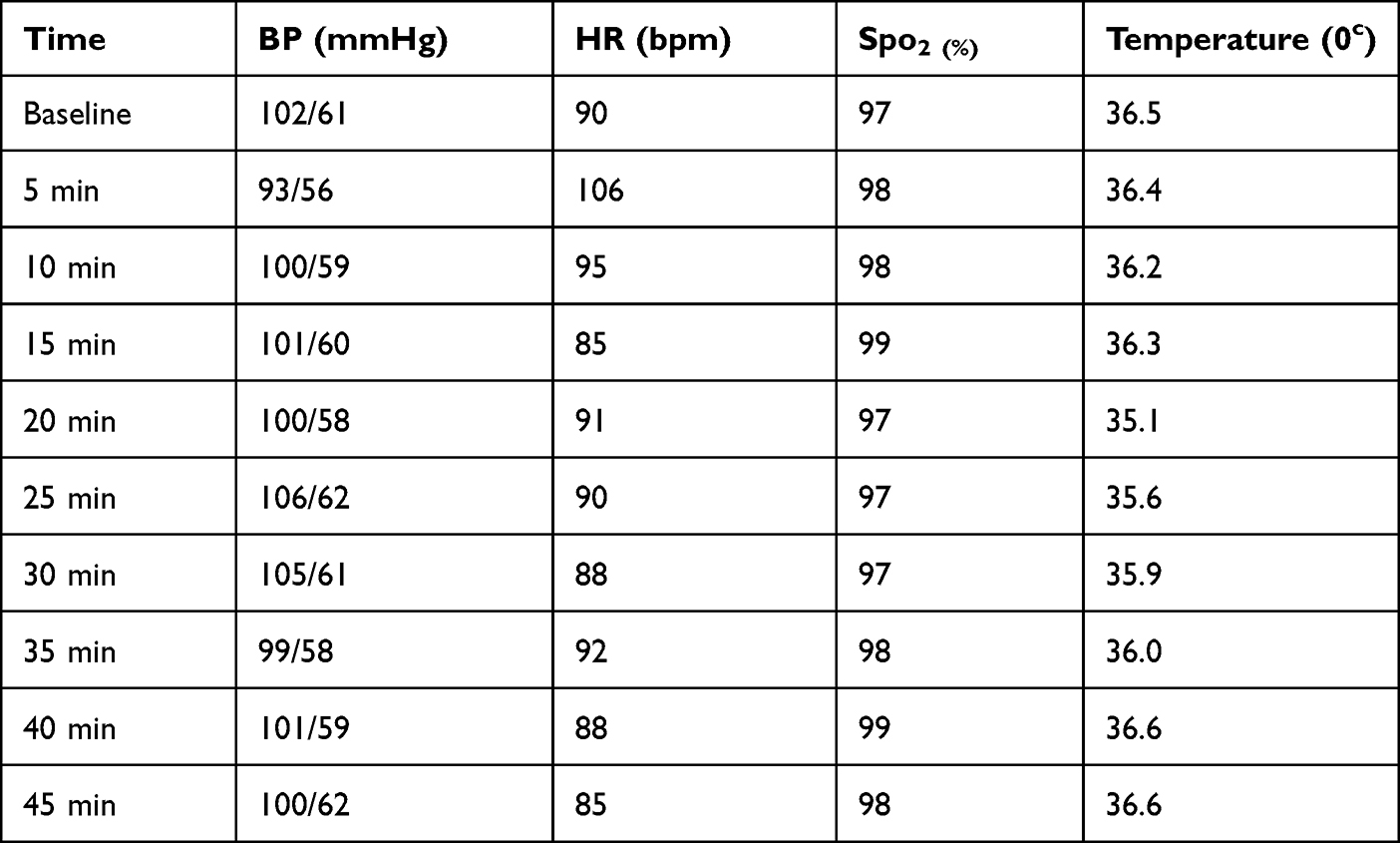 |
Table 2 30 Years Old with Chronic Rheumatic Heart Disease and Moderate Pulmonary Hypertension Pregnant Mother’s Intraoperative Vital Sign Records |
Post operatively; SpO2, NIBP, and ECG monitoring were used in the post-anesthesia care unit (PACU), along with oxygen supplementation delivered through a nasal catheter. She remained stable throughout the entire postoperative period. After spending an hour in the PACU, she was moved to the gynecology/obstetrics ward. Her initial analgesic need was not met until 18 hours later, when she received 50 mg of pethidine IV. She had a smooth hospital stay and was released after four days.
Discussion
0.9% to 3.7% of pregnant women have cardiovascular disease. Rheumatic heart disease (RHD) continues to be widespread in developing countries like India, where it accounts for 40–50% of all cardiac conditions during pregnancy. The most prevalent lesion among RHD patients who are pregnant is valvular heart disease.12,13 Postoperative maternal morbidity and death are significantly influenced by heart disease during pregnancy.13 Prior to delivery, pregnant patients with pulmonary hypertension and significant multivalvular heart disease need to undergo careful preoperative, multidisciplinary assessment, and anaesthetic planning to maximize cardiac function during the peripartum period and make informed decisions about the delivery mood and anaesthetic technique.4
Pulmonary hypertension is classified into different categories based on different causes and factors at different times. The classification was based primarily on the presence or absence of identifiable causes or risk factors, clinical features, genetically (familial) therapeutic options, pulmonary veno-occlusive disease (PVOD), and pulmonary capillary hemangiomatosis. A left-side valvular disease or chamber defect may produce pulmonary hypertension as a result of an increase in left atrial pressure, which results in backward transfer of the pressure and a passive rise in pulmonary pressures. Nonetheless, the patient could have a normal or almost normal PVR and left-side cardiac malfunction with a preserved ejection fraction.1,7 In our case report, it serves as the best illustration of how pulmonary hypertension can develop as a result of a left side heart condition. She had significant mitral regurgitation and severe left atrial dilatation, and her pulmonary hypertension was a result of left-side valvular and atrial illness.
One of the main causes of postoperative morbidity and mortality for patients undergoing cardiac and non-cardiac surgery is pulmonary hypertension. This is due to the fact that surgical stress, discomfort, ventilation, medicine, and inflammation connected to the surgery all contribute to pressure elevation, PVR, and right-sided heart failure.14
For patients with pulmonary hypertension, perioperative anaesthesia care focuses on avoiding any conditions that raise pulmonary vascular resistance and pressure, including as discomfort, acidosis, hypoxia, hypovolemia, alkalosis, and fluid overload. General anaesthesia is not as effective as regional anaesthesia procedures. This is because regional anaesthesia avoids raising pulmonary pressure, which is brought on by mechanical ventilation, and does not interfere with spontaneous breathing. It also offers sufficient postoperative analgesia. But in order to prevent a large reduction in systemic vascular resistance, a reduction in coronary perfusion, and right-heart failure, the commencement of epidural analgesia, administration, and dosing of local anaesthetics should be carried out cautiously and fractionated.14,15
In our instance of a resource-constrained environment, we attempt to reduce the hemodynamic consequences of spinal anaesthesia by lowering the dose of local anaesthesia and incorporating morphine to maintain hemodynamic status and extend the analgesic impact of bupivacaine. To prevent somatic pain, which exacerbates pulmonary hypertension, we were also given a trans abdominal pain block.
In a situation with limited resources, this case report covers a wide variety of significant issues relating to the anaesthetic care of expectant mothers with multivalvular heart disease and pulmonary hypertension. Like, it remark on what pre-question should be evaluated in patients with pulmonary hypertension and multivalvular heart disease, how anaesthesia management is carried out to achieve the target anaesthesia goal in a resource-limited area, and the question of the impact on the anaesthesia provider as well as other healthcare professionals.
In this instance, the mothers had pulmonary hypertension and persistent rheumatic heart disease for 8 years. Her cardiac condition has now deteriorated to a dangerous state (mild to severe). To prevent further worsening of elevated pulmonary pressure and cardiac events, all anaesthetic assessments must be precise. A decrease in SVR, maintenance of sinus rhythm, maintenance of a normal to slightly elevated heart rate, treatment of acute atrial fibrillation, avoidance of aortocaval compression, maintenance of venous return, and avoidance of factors that increased PVR were the main goals of anaesthesia in pregnancy during caesarean sections.4,9
Following sympathetic blockade, neuraxial blockades can cause substantial cardiovascular alterations, including a drop in cardiac output due to a reduction in preload. SVR will be reduced by arteriolar dilation, which may result in a stroke. In both the mitral and aortic valves, reflex tachycardia is poorly tolerated, as are aortic stenosis and coronary artery disease. Low SVR can cause catastrophic reductions in pulmonary blood flow by reversing the pressure gradient across a left-to-right intracardiac shunt. These modifications are significant. With a single spinal anaesthetic, the pain is frequently more acute compared to continuous blockage of the centroneuraxis.4,9 Nonetheless, neuraxial blockade has benefited from significant technical and pharmacological advancements in recent years, allowing it to be adjusted to the patient’s demands as well as the obstetric course. Most parturient with symptomatic cardiac disease benefit from carefully administered neuraxial procedures for labor analgesia, vaginal delivery, and Caesarean section.16 Even though general anesthesia is safe for oxygenation and uncomplicated airway management,15 maintenance of spontaneous breathing is one benefit of regional anaesthetic, preventing the increase in pulmonary pressures brought on by mechanical ventilation.14,16,17
Patients with cardiac illnesses are linked to decreased local anesthetic clearance, which would justify lowering the dose of local anesthetics agents administered for neuraxial blockage. Using local anesthetic agents with additive drugs like opioids would minimize the total quantity of local anesthetic necessary in the early stages, reducing the total amount of local anesthetic required.17–19 According to the Obstetric Anaesthetists Association of the United Kingdom, neuroaxial blockade was used in 73% of cardiac parturient who had vaginal deliveries. A spinal anaesthetic was given to 12% of Caesarean section patients, whereas 40% received either an epidural anaesthetic with low doses of local anaesthetic or a CSE anaesthetic.16
The pregnant patient can tolerate both mitral insufficiency and mitral prolapse because a drop in SVR reduces regurgitated flow. Important concerns include atrial arrhythmias and the risk of embolism from atrial thrombi. SVR will automatically increase in response to pain, and sufficient labor analgesia should reduce peripheral vasoconstriction, avoiding an increase in left ventricular afterload. Systemic vascular resistance is further reduced by additional sympathetic blockage. If preload is raised to maintain left ventricular filling capacity, neuraxial procedures are advised for labor, vaginal delivery, and Caesarean section. Only symptomatic patients require invasive monitoring.9
In our case, we performed a trans abdominals block prior to the procedure caesarean section to alleviate somatic pain, which increased both SVR and PVR as a multimodal analgesic, TAP block provides analgesia for the somatic source of pain for a short period of time with a single shot.20 The practice of TAP blocks increased as therapeutic adjuncts for analgesia following lower abdominal surgeries like caesarean section, hysterectomy, cholecystectomy, colectomy, prostatectomy, and hernia repair.21–23
Conclusion
Anaesthesia management in patient with severe mitral regurgitation, moderate pulmonary hypertension, severe left atrial dilatation, mild aortic regurgitation, and mild tricuspid regurgitation was challenging in our setup. Even if spontaneous delivery is recommended in patient with cardiac finding, caesarean section is needed in area where limited access to support spontaneous delivery. Goal directed perioperative management with multidisciplinary involvement helps the patient to have good outcome.
Spinal anaesthesia with heavy bupivacaine may result decrement in blood pressure in the first few minute. This change is more significant in patient with chronic rheumatic heart disease and moderate pulmonary hypertension pregnant mother’s. Spinal anesthesia with low dose of bupivacaine and 0.1 mg of morphine is tolerable in patients with chronic rheumatic heart disease and pulmonary hypertension. The derangement in blood pressure can managed with head up positioning and fluid. Bilateral Tran’s abdominal plain nerve (TAP) block with the concentration of 0.125% of 40mL bupivacaine helps treat somatic pain. There must be close post-operative monitoring and follow-up in post anaesthesia care unit (PACU) as well as wards for pregnant mothers with chronic rheumatic heart disease and moderate pulmonary hypertension.
Ethics Approval and Consent to Participate
For both procedural and anaesthetic purposes, as well as to take part in this study, we had the required patient and family consent. The patient gave her permission for the clinical information and images to be included in the paper for publication. Throughout along, confidentiality was upheld, and appropriate efforts were made to protect her privacy.
Publication Consent
Written informed consent has been provided by the patient for publication of the case details.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Simonneau G, Montani D, Celermajer DS, et al. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur Respir J. 2019;53(1):1801913. doi:10.1183/13993003.01913-2018
2. Blaise G, Langleben D, Hubert B. Pulmonary arterial hypertension: pathophysiology and anesthetic approach. Anesthesiology. 2003;99(6):1415–1432. doi:10.1097/00000542-200312000-00027
3. Warltier DC. Pathophysiology and anesthetic approach. Hypertension. 2003;6:1415–1432.
4. Coskun D, Mahli A, Korkmaz S, et al. Anaesthesia for caesarean section in the presence of multivalvular heart disease and severe pulmonary hypertension: a case report. Cases J. 2009;2(12):1–5. doi:10.1186/1757-1626-2-9383
5. Weiss BM, Hess OM. Pulmonary vascular disease and pregnancy: current controversies, management strategies, and perspectives. Eur Heart J. 2000;21(2):104–115. doi:10.1053/euhj.1999.1701
6. Agha RA, Franchi T, Sohrabi C, et al. The SCARE 2020 guideline: updating consensus surgical case report (SCARE) guidelines. Int J Surg. 2020;84:226–230. doi:10.1016/j.ijsu.2020.10.034
7. Bonnin M, Mercier FJ, Sitbon O, et al. Severe pulmonary hypertension during pregnancy: mode of delivery and anesthetic management of 15 consecutive cases. Anesthesiology. 2005;102(6):1133–1137. doi:10.1097/00000542-200506000-00012
8. Rex S, Devroe S. Anesthesia for pregnant women with pulmonary hypertension. Curr Opin Anaesthesiol. 2016;29(3):273–281. doi:10.1097/ACO.0000000000000310
9. Gomar C, Errando CL. Neuroaxial anaesthesia in obstetrical patients with cardiac disease. Curr Opin Anaesthesiol. 2005;18(5):507–512. doi:10.1097/01.aco.0000183108.27297.3c
10. Tsiaras S, Poppas A. Mitral valve disease in pregnancy: outcomes and management. Obstet Med. 2009;2(1):6–10. doi:10.1258/om.2008.080002
11. Hansen L, Burks M. Volume management in pulmonary arterial hypertension patients. PMC. 2018;4(1):13–27.
12. Tan J, De Swiet M. Prevalence of heart disease diagnosed de novo in pregnancy in a West London population. BJOG an Int J Obstet Gynaecol. 1998;105(11):1185–1188. doi:10.1111/j.1471-0528.1998.tb09972.x
13. Kumari A, Kumar K, Kumar Sinha A. The pattern of valvular heart diseases in India during pregnancy and its outcomes. Cureus. 2021;13(7):e16394.
14. Phulli R, Arora P, Neema PK. Comparison of dexmedetomidine and ketamine versus propofol and ketamine for procedural sedation in children undergoing minor cardiac procedures in cardiac catheterization laboratory. Ann Card Anaesth. 2017;20(1):422–426. doi:10.4103/aca.ACA_16_17
15. Gille J, Seyfarth HJ, Gerlach S, Malcharek M, Czeslick E, Sablotzki A. Perioperative anesthesiological management of patients with pulmonary hypertension. Anesthesiol Res Pract. 2012;2012. doi:10.1155/2012/356982
16. Dob DP, Yentis SM. UK registry of high-risk obstetric anaesthesia: report on cardiorespiratory disease. Int J Obstet Anesth. 2001;10(4):267–272. doi:10.1054/ijoa.2001.0873
17. Rout CC. Anaesthesia and analgesia for the critically ill parturient. Best Pract Res Clin Obstet Gynaecol. 2001;15(4):507–522. doi:10.1053/beog.2001.0197
18. Rosenberg PH, Veering BT, Urmey WF. Maximum recommended doses of local anesthetics: a multifactorial concept. Reg Anesth Pain Med. 2004;29(6):564–575. doi:10.1016/j.rapm.2004.08.003
19. Kuczkowski KM. Labor analgesia for the parturient with cardiac disease: what does an obstetrician need to know? Acta Obstet Gynecol Scand. 2004;83(3):223–233. doi:10.1111/j.0001-6349.2004.0430.x
20. Abdallah FW, Laffey JG, Halpern SH, Brull R. Duration of analgesic effectiveness after the posterior and lateral transversus abdominis plane block techniques for transverse lower abdominal incisions: a meta-analysis. Br J Anaesth. 2013;111(5):721–735. doi:10.1093/bja/aet214
21. Mishriky BM, George RB, Habib AS. Transversus abdominis plane block for analgesia after Cesarean delivery: a systematic review and meta-analysis. Can J Anesth. 2012;59(8):766–778. doi:10.1007/s12630-012-9729-1
22. Gao T, Zhang JJ, Xi FC, et al. Evaluation of Transversus Abdominis Plane (TAP) block in hernia surgery. Clin J Pain. 2017;33(4):369–375. doi:10.1097/AJP.0000000000000412
23. Champaneria R, Shah L, Geoghegan J, Gupta JK, Daniels JP. Analgesic effectiveness of transversus abdominis plane blocks after hysterectomy: a meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2013;166(1):1–9. doi:10.1016/j.ejogrb.2012.09.012
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.