Back to Journals » Clinical Interventions in Aging » Volume 21
Perioperative Anemia and Transfusion Management in Older Adults with Osteoporotic Hip Fractures: A Narrative Review of Current Evidence and Emerging Strategies
Authors Xu X, Wang Z, Zhao C, Fan H, Guo J
Received 27 April 2026
Accepted for publication 25 June 2026
Published 9 July 2026 Volume 2026:21 620352
DOI https://doi.org/10.2147/CIA.S620352
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Xin Xu,1– 3,* Zheng Wang,1,* Chengcheng Zhao,1,2 Hua Fan,1 Junfei Guo1,2
1Department of Joint Surgery, Honghui Hospital, Xi’an Jiaotong University, Xi’an, Shaanxi, People’s Republic of China; 2Key Laboratory of Pathogenesis and Precision Treatment of Arthritis, Xi’an, Shaanxi, People’s Republic of China; 3Translational Medicine Centre, Honghui Hospital, Xi’an Jiaotong University, Xi’an, Shaanxi, People’s Republic of China
*Xin Xu and Zheng Wang contributed equally to this work
Correspondence: Junfei Guo, Department of Joint Surgery, Honghui Hospital, Xi’an Jiaotong University, Xi’an, Shaanxi, People’s Republic of China, Email [email protected] Hua Fan, Department of Joint Surgery, Honghui Hospital, Xi’an Jiaotong University, Xi’an, Shaanxi, People’s Republic of China, Email [email protected]
Abstract: Osteoporotic hip fractures represent a major and escalating public health burden in aging populations, carrying substantial morbidity, mortality, and healthcare costs. Perioperative anemia is exceedingly common in this frail cohort, with reported preoperative prevalence ranging from 40% to over 50%, and is an established independent predictor of adverse short- and long-term outcomes including mortality, impaired functional recovery, postoperative delirium, and prolonged hospitalization. The management of anemia and the judicious use of allogeneic blood transfusion are central to the multidisciplinary care of these patients. This narrative review provides a comprehensive and critical appraisal of the contemporary evidence governing perioperative anemia management in elderly osteoporotic hip fracture patients, drawing on randomized controlled trials, meta-analyses, and large observational studies identified through searches of major bibliographic databases. We critically examine the epidemiology and multifactorial etiology of perioperative anemia; the evolution of transfusion-risk prediction from traditional clinical indices to machine learning; pharmacological blood conservation, with robust evidence for tranexamic acid and intravenous iron; the debate between restrictive and liberal transfusion thresholds and the need for individualized, physiologically guided decision-making; the perioperative management of patients on antithrombotic therapy; and the influence of surgical technique, fracture type, and nutritional and frailty status. Several practical messages emerge: a restrictive transfusion strategy (hemoglobin 7– 8 g/dL) is appropriate for most patients but should be individualized, favoring a more liberal approach in frail, cardiovascularly vulnerable, or delirium-prone patients and nursing-home residents; early and intraoperative tranexamic acid and intravenous iron meaningfully reduce transfusion requirements; surgery should generally not be delayed solely because of antithrombotic medication; and care is best delivered through a multimodal, stepwise Patient Blood Management approach embedded within integrated orthogeriatric care pathways. Priorities for future research include the prospective validation of individualized, physiologically guided transfusion algorithms, the adoption of patient-centered outcome measures, and the rigorous evaluation of emerging technologies.
Keywords: hip fracture, osteoporotic, perioperative anemia, allogeneic blood transfusion, transfusion threshold, patient blood management
Introduction
Osteoporotic hip fractures (OHFs) represent a major public health challenge, particularly in aging populations, and are associated with substantial morbidity, mortality, and healthcare costs.1 As reported, the annual incidence in adults aged 45 years and older is approximately 148.7 per 100,000, with a female-to-male ratio approaching 3:1.2 The perioperative period for these frail patients is fraught with physiological disturbances, with anemia standing out as a pervasive and consequential complication. The management of perioperative anemia and the judicious use of blood transfusions are central to the multidisciplinary care of patients with OHFs, directly impacting clinical outcomes and resource utilization.3
Anemia is exceedingly common in elderly patients presenting with OHFs. Multiple studies confirm that preoperative anemia is present in approximately 40–60% of patients,4–7 with moderate-to-severe anemia accounting for over 20% of cases.8,9 This high prevalence is inextricably linked to the chronic disease burden, nutritional deficiency, and age-related decline in hematopoietic reserve characteristic of this population.10 Nationwide study reports transfusion rates during admission ranging from approximately 17% to 37%, underscoring the clinical frequency of this issue.11 Postoperatively, the prevalence escalates further due to fracture- and surgery-related blood loss.12,13 The burden of anemia extends far beyond laboratory values, as it is intricately linked to a spectrum of adverse short- and long-term outcomes.14–16 Yombi et al confirmed that low Hb at admission was significantly associated with mortality at 90, 180 days, and one year after surgery.17 Furthermore, allogeneic red blood cell transfusion (ARBCT) itself has also been identified as an independent risk factor for short-term mortality in recent studies.18,19 Beyond mortality, preoperative anemia has also been independently associated with an increased risk of in-hospital postoperative complications in large OHFs cohorts.20
Besides mortality, the detrimental effects of anemia permeate functional recovery and quality of life. Patients with severe preoperative anemia exhibit poorer physical function, lower Harris Hip Scores, and reduced health-related quality of life (SF-36) at six months post-surgery compared to those with higher Hb levels.21 The severity of anemia appears to exhibit a dose-response relationship with adverse outcomes that Hb below 10 g/dL or even below 7.1 g/dL, is associated with a further escalation in the risk of complications.9,22 In addition, the cumulative time spent with low perioperative Hb levels has also been linked to adverse outcomes including delirium and a trend towards higher mortality.23 Consistently, a recent observational cohort study (n = 322) demonstrated that anemia at admission was positively associated with delirium, postoperative complications, length of hospital stay and all-cause mortality in hip fracture patients.24 From a healthcare resource perspective, anemia is also a significant risk factor of increased length of hospital stay (LOS). A nonlinear relationship exists, where for Hb levels below 10 g/dL, each 1 g/dL increase is associated with a reduction in LOS of approximately 0.735 days, highlighting a critical threshold for intervention. Above this level, the association is no longer statistically significant, suggesting a floor effect of particular clinical relevance.25 Similarly, anemia also contributes to higher rates of hospital readmission and greater consumption of resources, including intensive care.26,27
The etiology of perioperative anemia in OHF patients is multifactorial, involving patient-related, fracture-related, and management-related factors. Advanced age, female sex, lower body mass index (BMI), and a higher burden of comorbidities are independent patient-related risk factors for requiring postoperative blood transfusion.11,19,27,28 Comorbidities such as Parkinson’s disease, type 2 diabetes with high HbA1c variability, and cognitive impairment further compound fracture risk and may independently worsen perioperative anemia.29,30 Nutritional status, reflected by indices like the Prognostic Nutritional Index (PNI) or Geriatric Nutritional Risk Index (GNRI) is also associated with lower perioperative Hb, higher transfusion rates, and increased mortality.31,32 Furthermore, the type and location of the fracture significantly influence blood loss and transfusion requirements. Previous studies reported that intertrochanteric and subtrochanteric fractures are associated with markedly greater preoperative Hb decline and higher risk-adjusted incidence of postoperative transfusion compared to femoral neck fractures.11,33–35 Accordingly, the choice of surgical implant also plays a role that intramedullary nailing for pertrochanteric fractures correlating with higher transfusion rates compared to other fixation methods.36
In summary, perioperative anemia imposes a heavy burden on patients with OHF, exacerbating mortality risk, impairing functional recovery, increasing complication rates, and straining healthcare systems. Its high prevalence and profound impact necessitate a standardized, evidence-based approach to its detection, evaluation, and management throughout the perioperative period. This article is a narrative review intended to provide an expert, integrative synthesis of current concepts, controversies, and emerging strategies in perioperative blood management for older adults with osteoporotic hip fractures, rather than a systematic review. We searched PubMed/MEDLINE, Embase, the Cochrane Library, and Web of Science for English-language articles published up to January 2026, using combinations of terms including “hip fracture”, “osteoporotic”, “perioperative an(a)emia”, “blood transfusion”, “transfusion threshold”, “tranexamic acid”, “iron”, “anticoagulant”, and “patient blood management”. We prioritized randomized controlled trials, systematic reviews and meta-analyses, and large observational and cohort studies, and screened the reference lists of key articles to identify additional relevant publications. Given the breadth of the topic and the marked heterogeneity of the available evidence, a narrative approach was deliberately adopted in order to integrate clinical, pharmacological, and organizational perspectives into a coherent, practice-oriented synthesis; accordingly, no formal quantitative pooling or risk-of-bias assessment was undertaken, and the cited literature was selected to be representative rather than exhaustive. Throughout, we frame perioperative blood management around the three complementary pillars of Patient Blood Management—optimizing erythropoiesis, minimizing blood loss, and enhancing tolerance of anemia, which together provide the conceptual structure for the strategies discussed in the sections that follow.
Preoperative Assessment and Optimization of Anemia
Given the significant burden of perioperative anemia, its systematic assessment and proactive management from the moment of hospital admission become important. While OHF surgery is often an emergency procedure, a strategic window exists for preoperative evaluation and targeted intervention to mitigate risks and improve outcomes. A comprehensive preoperative assessment aims not only to diagnose anemia but also to understand its etiology, identify patients at high risk for requiring ARBCT, and initiate corrective measures within the constraints of an expedited surgical timeline.
Initial Recognition and Etiological Understand
The initial step involves prompt recognition and quantification of anemia. A substantial proportion of elderly OHF patients present with anemia upon admission,6,7 which is a powerful independent predictor of both short- and long-term mortality, even after adjusting for comorbidities and age.14–17,37 The assessment begins with a complete blood count to determine the Hb concentration and red cell indices. The World Health Organization (WHO) definition of anemia provides a standard threshold, but clinical significance is graded, with severe anemia being particularly detrimental and linked to worse functional outcomes and increased LOS.21,25
Beyond the simple Hb value, a thorough preoperative evaluation seeks to identify contributing factors and associated risks. The etiology of anemia in this population is complex, encompassing anemia of chronic disease, nutritional deficiency (iron, vitamin B12, folate), and acute hemorrhage from the fracture.10,38 Key laboratory parameters include serum ferritin and transferrin saturation to assess iron stores, creatinine to evaluate renal function, and albumin as a marker of nutritional status.39,40 Comorbidities, quantified by tools such as the Charlson Comorbidity Index (CCI) and modified Elixhauser’s Comorbidity Measure (mECM), are linked with both the presence of anemia and the need for perioperative transfusion.14,41–43 Other modifiable factors, such as hypocalcemia (corrected calcium <2.11 mmol/L), have also been identified as independent associates of increased perioperative blood loss and transfusion risk.44 Furthermore, endocrine responses to trauma, such as Euthyroid Sick Syndrome, may also exacerbate anemia risk.45
Risk Stratification: From Traditional Models to Machine Learning
Risk stratification is a cornerstone of effective preoperative planning (Table 1). Several studies have developed and validated predictive models to identify patients at high risk for requiring perioperative ARBCT. Traditional models consistently highlight a core set of independent risk factors including lower preoperative Hb level, advanced age, the presence of specific fracture types, and poorer overall health status.11,33,46–48
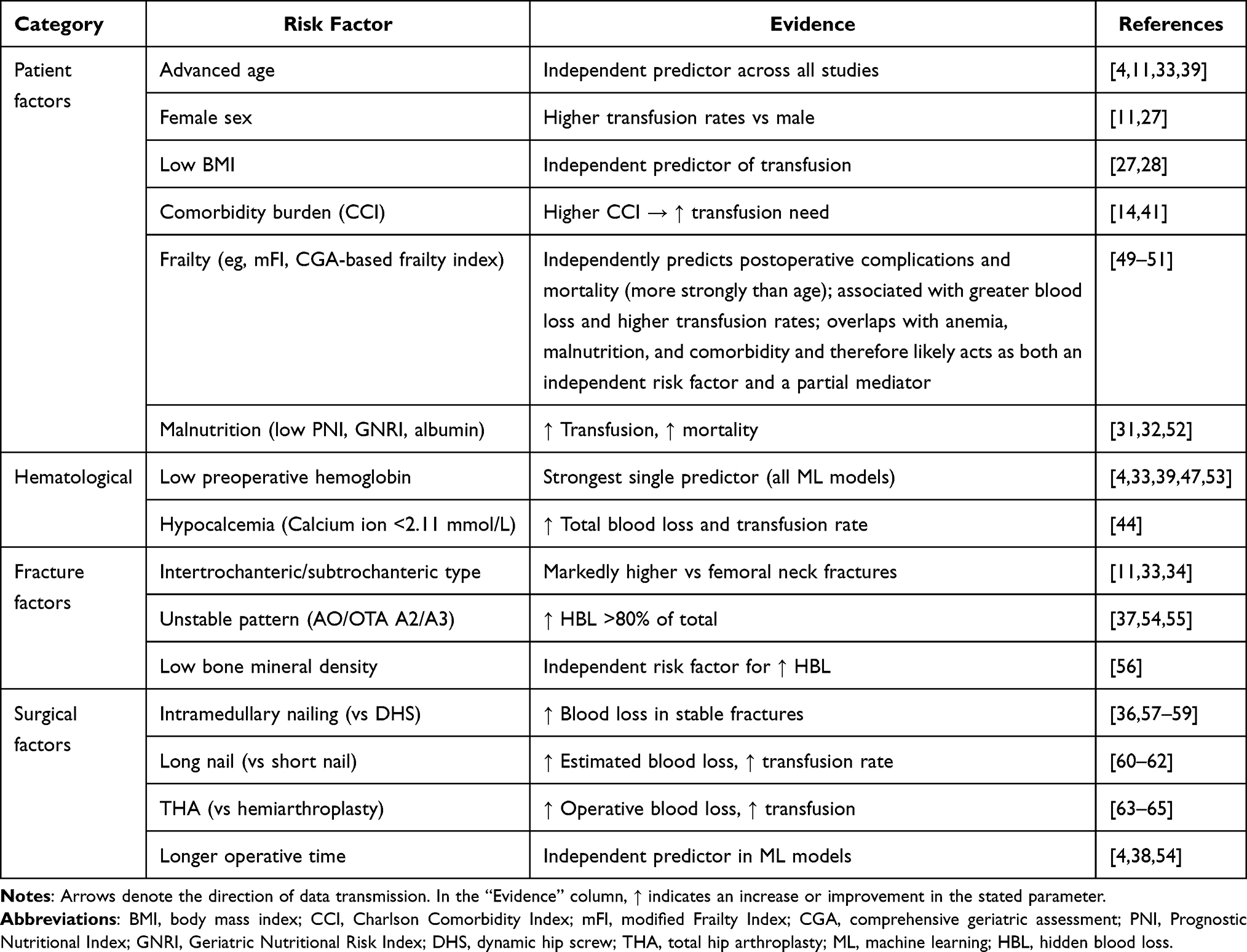 |
Table 1 Risk Factors for Perioperative Blood Transfusion in Elderly Patients with Osteoporotic Hip Fractures |
In recent years, machine learning (ML) algorithms have demonstrated a marked superiority over traditional statistical methods in predicting perioperative transfusion risk, capable of capturing complex, non-linear relationships and interaction effects that conventional models may miss. Zhou et al developed a random forest (RF) model that achieved an area under the receiver operating characteristic curve (AUC) of 0.887 in internal validation and 0.834 in external validation, identifying estimated surgical duration, preoperative anemia, advanced age, hypoalbuminemia, and internal fixation as the top five predictive variables.4 Guo et al compared eight ML algorithms and found that the XGBoost model performed optimally, with Matthews Correlation Coefficients of 0.828 and 0.939 in training and validation sets, respectively, selecting eight key features including age, fracture timing, fracture type, Hb, albumin, creatinine, ionized calcium, and activated partial thromboplastin time.39 Chen et al developed five ML models with a mean AUC of 0.912 ± 0.021, and SHAP (SHapley Additive exPlanations) analysis confirmed Hb as the most influential predictor.53 Wei et al further developed a novel predictive nomogram specifically for proximal femoral anti-rotation nailing (PFNA), incorporating variables such as albumin and creatinine with high discriminatory power.40 Importantly, ML approaches have revealed interaction effects not captured by traditional models, which further improved model performance.53
Despite these advances, the widespread clinical deployment of ML-based prediction models faces considerable challenges. Most published models have been derived from single-center, retrospective datasets and report discriminative performance (AUC) with limited assessment of calibration; relatively few have undergone rigorous external validation, and fewer still have been validated prospectively or across temporally and geographically distinct cohorts, raising concerns regarding overfitting, optimism, and dataset shift. Additional barriers include limited model interpretability, demanding data-quality and missing-data requirements, and uncertain generalizability across diverse healthcare settings. Critically, no model has yet demonstrated improved patient-centered outcomes or clinical utility in a prospective impact study. Future research should therefore prioritize external and prospective validation, transparent calibration reporting, and the development of interpretable, user-friendly clinical decision-support systems integrated into electronic health records before such tools can be recommended for routine practice.39,40
Preoperative Optimization Strategies
Preoperative optimization, though time-limited, encompasses several evidence-based strategies. The most immediate decision often revolves around preoperative ARBCT. A restrictive transfusion strategy, typically triggered at an Hb threshold of 8 g/dL or for symptomatic anemia, is now widely recommended and has been shown to be safe without increasing mortality or major complications compared to a liberal strategy.66 Meta-analysis indicate that preoperative intravenous (IV) iron can enhance Hb recovery, reduce postoperative transfusion rates, and is associated with lower short-term mortality.67 In addition, the combination of IV iron and erythropoietin (EPO) appears effective in stimulating erythropoiesis and reducing ARBCT when administered preoperatively.68 While a large randomized trial did not show a reduction in transfusion rates with ferric carboxymaltose with or without EPO, it confirmed improved Hb recovery.69 Correction of other deficiencies, such as vitamin D and vitamin K, may also form part of a comprehensive nutritional support strategy, though direct evidence for impacting transfusion needs is less robust.12,70
The timing of surgery itself is a critical variable in the perioperative anemia equation. While expedited surgery is a key standard of care to reduce morbidity and mortality, its relationship with transfusion requirements is nuanced. Recently, several studies suggest that surgery within the first 48 hours may be associated with a higher transfusion rate.33,43 However, Kim et al found that delaying surgery primarily increases preoperative transfusion needs without necessarily altering the total perioperative transfusion volume.71 Therefore, the decision must balance the general benefits of early surgery against the opportunity for targeted anemia management in selected high-risk patients.
Frailty, Anemia, and Comprehensive Geriatric Assessment
Anemia and frailty are closely and bidirectionally linked in older adults with OHFs, and their co-occurrence has important physiological implications for perioperative blood management. Frailty denotes a state of diminished physiological reserve and reduced capacity to withstand stressors, and anemia is both a recognized contributor to, and a clinical marker of, this state. Several overlapping mechanisms underlie this relationship. The chronic low-grade inflammation characteristic of aging (“inflammaging”), with elevated interleukin-6 and other pro-inflammatory cytokines, upregulates hepcidin, thereby restricting intestinal iron absorption and sequestering iron within the reticuloendothelial system to produce a functional iron deficiency and anemia of inflammation that is relatively refractory to oral iron. Aging is further associated with a blunted erythropoietin response, reduced hematopoietic reserve, a higher prevalence of nutritional deficiencies (iron, vitamin B12, folate), and impaired renal function, all of which limit the erythropoietic response to the acute blood loss of fracture and surgery. Critically, the reduced cardiovascular and physiological reserve of frail patients lowers their capacity to compensate for a given degree of anemia, narrowing the margin of safety and rendering them more vulnerable to the consequences of both anemia and its treatments. These considerations help explain why a single hemoglobin threshold is inadequate in this population and why frailty status should be formally integrated into perioperative decision-making. Comprehensive geriatric assessment as a multidimensional evaluation of medical, functional, cognitive, nutritional, and social domains, delivered within orthogeriatric co-management models provides a structured means of identifying frailty, anticipating transfusion requirements, and individualizing optimization, and has been associated with improved outcomes after hip fracture.72–75
The relationship between frailty and perioperative transfusion warrants specific comment. Frailty appears to act both as an independent risk factor and as a marker of shared underlying vulnerability. On the one hand, validated frailty measures independently predict adverse perioperative outcomes after hip fracture surgery: a preoperative modified Frailty Index (mFI) is independently associated with a higher severity of postoperative complications,49 and frailty predicts postoperative mortality more strongly than chronological age.50 Because frailer patients tend to sustain greater perioperative blood loss and are transfused more frequently, frailty is also closely associated with increased transfusion requirements. On the other hand, frailty overlaps mechanistically with anemia, malnutrition, and comorbidity, such that part of its association with transfusion is likely mediated through these shared pathways; consistent with this, the propensity to be transfused in older surgical patients has been linked more closely to comorbidity burden than to age per se.51 Frailty should therefore be regarded as both a genuine independent predictor and, in part, a downstream marker of cumulative physiological deficit—an interpretation that reinforces the rationale for formal frailty assessment rather than reliance on any single parameter. More broadly, frailty seldom occurs in isolation but frequently coexists with other geriatric syndromes including sarcopenia, malnutrition, cognitive impairment, and polypharmacy that further erode physiological reserve and recovery capacity; sarcopenia in particular overlaps with both anemia and frailty and is associated with poorer functional recovery and worse outcomes after hip fracture. These considerations reinforce the value of incorporating formal frailty, nutritional, and sarcopenia assessment within comprehensive geriatric evaluation when planning perioperative blood management.
Pharmacological Interventions and Blood Conservation Strategies
Building upon a multidisciplinary preoperative assessment, targeted pharmacological and procedural interventions during the intraoperative and immediate postoperative phases are crucial components of a comprehensive Patient Blood Management (PBM) protocol for OHFs. The goal is to minimize iatrogenic blood loss, optimize hemostasis, and support erythropoiesis, thereby reducing the reliance on ARBCT and its associated risks.
Tranexamic Acid
The most extensively studied and supported pharmacological agent is tranexamic acid (TXA), an antifibrinolytic that inhibits the breakdown of blood clots by blocking the lysine-binding sites on plasminogen. A Cochrane overview of systematic reviews, encompassing data from 21 RCTs and 2148 participants, concluded that TXA probably reduces the need for ARBCT in adults undergoing OHF surgery, with a risk ratio of 0.56, translating to approximately 194 fewer people per 1000 requiring a transfusion.38 This efficacy is consistently demonstrated across various meta-analyses, regardless of fracture type or surgical procedure including in hip hemiarthroplasty,76 intertrochanteric fracture surgery,77 and femoral neck fractures treated with arthroplasty.78 Moreover, the reduction in transfusion requirements is paralleled by a significant decrease in calculated total blood loss, often by over 200 mL,79,80 and an attenuated postoperative decline in Hb levels.81,82
Importantly, the safety of TXA in this vulnerable population appears favorable. Multiple high-level syntheses have found no statistically significant increase in the risk of thromboembolic events, including deep vein thrombosis (DVT) and pulmonary embolism (PE), myocardial infarction, cerebrovascular accidents, or mortality when compared to placebo or control.38,79–81,83 In a meta-analysis encompassing over 54,000 patients, Augustinus et al reported that 30-day mortality was lower in the TXA group.76 One large observational study found a higher incidence of diagnosed PE with TXA use but without an associated increase in 30-day mortality.84 Nonetheless, these reassuring data derive largely from randomized trials and meta-analyses that may be underpowered to detect rare thromboembolic events and that frequently excluded patients at the highest thrombotic risk, such as those with recent venous thromboembolism, active arterial or venous thrombosis, or severe renal impairment. The favorable safety profile of TXA should therefore not be over-generalized to these subgroups, in whom dedicated evidence remains sparse and individualized caution is warranted. The interaction between TXA and preoperative chemoprophylaxis for DVT does not appear to alter its effect on transfusion rates, suggesting they can be used concurrently.85
Regarding administration, evidence supports both IV and topical routes with similar efficacy and safety.78,86 Oral TXA (2 g, 2 hours preoperatively) has been shown to be non-inferior to IV TXA (1 g, 15 minutes preoperatively) in terms of total blood loss and transfusion rates, with significantly lower cost, offering a more economical alternative.86 The combination of IV and topical administration may provide synergistic hemostatic benefit for intertrochanteric fracture fixation compared to either route alone. While single and multiple dosing regimens show comparable reductions in blood loss,79 a single preoperative IV dose of 1 g or 15 mg/kg is widely used and effective.87,88 Evidence suggests that very early, pre-emptive administration (within 72 hours of injury, especially within 24 hours) may be particularly effective in reducing hidden blood loss (HBL) that occurs prior to surgery.89 However, delayed administration beyond 72 hours may not confer the same benefit.90 An emerging and clinically important consideration is the influence of nutritional status on TXA efficacy. Xie et al demonstrated that patients with adequate nutritional status, as defined by the GNRI, exhibited significant reductions in transfusion rates and Hb decline with TXA, whereas the effect was markedly attenuated in malnourished patients.52 This finding suggests that nutritional status may be a key modulator of TXA responsiveness and warrants consideration when evaluating the expected benefit of antifibrinolytic therapy (Table 2).
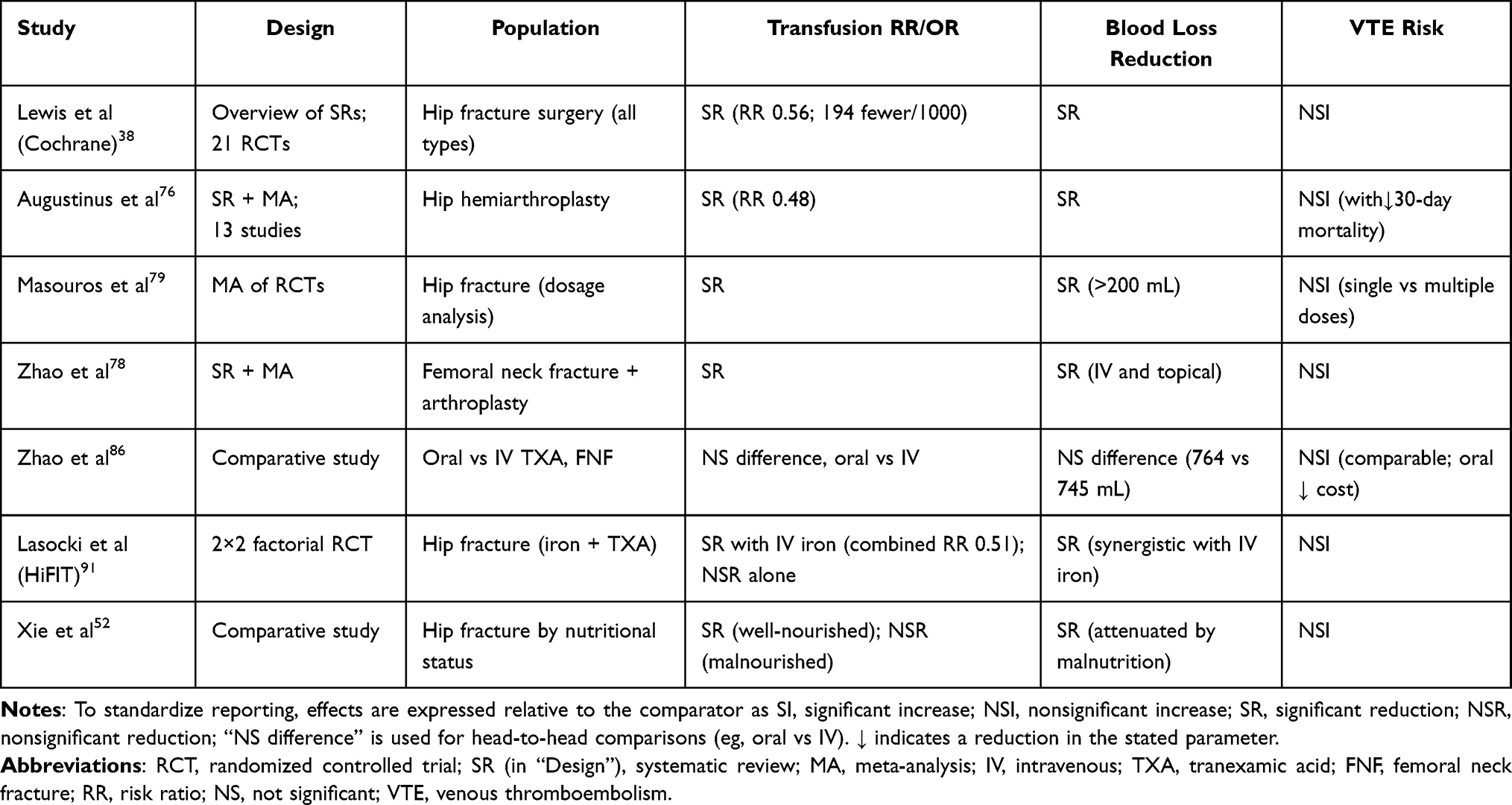 |
Table 2 Summary of Key Evidence for Tranexamic Acid (TXA) in Hip Fracture Surgery |
Intravenous Iron Supplementation
In contrast to the strong evidence for TXA, the role of IV iron supplementation in the acute perioperative setting is less definitive. The aforementioned Cochrane overview found only low-certainty evidence from a few small studies suggesting there may be little or no difference in transfusion requirements, infection rates, or mortality with IV iron administration.38 A meta-analysis including six RCTs found that perioperative IV iron had no significant impact on transfusion rates.92 The IRON NOF trial similarly found no reduction in the overall proportion of patients transfused, though a possible benefit for younger patients was noted.93 Chen et al94 reported that iron supplementation was not associated with a reduced transfusion rate in the overall analysis but did note a significant reduction in transfusion volume and LOS, and a potential reduction in infection risk. Subgroup analyses suggest that preoperative IV iron, particularly at doses of 200–300 mg, may be the most beneficial regimen. Another meta-analysis focusing on acute surgery found that IV iron therapy was associated with a lower 30-day mortality and a reduction in postoperative infections and ARBCT, though these findings were largely driven by observational studies.67
The combination of IV iron with EPO has been investigated, with one RCT finding that while it improved Hb recovery at 60 days post-discharge, it did not reduce the immediate need for perioperative ARBCT compared to placebo.69 A particularly informative contribution is the HiFIT trial, a multicenter, 2×2 factorial, double-blind RCT, which evaluated ferric derisomaltose (20 mg/kg) and TXA, alone or combined, for reducing ARBCT in OHF patients. Interestingly, neither iron nor TXA alone significantly reduced transfusion rates in this trial, but their combination produced a significant reduction, suggesting a potential synergistic mechanism whereby TXA reduces acute loss while iron supports erythropoietic recovery, which is a key finding that may reshape future multimodal PBM protocols.91 Therefore, while IV iron appears safe and may aid in longer-term Hb recovery and potentially reduce LOS, its ability to independently and reliably avert perioperative transfusions in OHF requires confirmation from larger, high-quality RCTs. Its greatest value may lie as a component of multimodal PBM, particularly when combined with TXA.
Surgical Technique and Implant Choice
Beyond specific hemostatic drugs, the choice of surgical implant and technique constitutes a critical non-pharmacological blood conservation strategy. For intertrochanteric fractures, the debate between extramedullary (eg, dynamic hip screw, DHS) and intramedullary (eg, cephalomedullary nail, CMN) fixation has implications for blood loss. While previous meta-analyses found no significant difference in transfusion rates between the two,95,96 more recent and specific analyses suggest nuances based on fracture stability. For stable (AO/OTA 31-A1) intertrochanteric fractures, several studies indicate that DHS fixation is associated with less intraoperative blood loss and lower postoperative transfusion rates compared to CMN.57 Cai et al conducted a prospective RCT and confirmed that intramedullary fixation was associated with significantly greater total blood loss and HBL.58 For unstable (AO/OTA 31-A2/A3) patterns, the evidence is mixed, with some studies favoring CMN36,59 and others suggesting DHS with a trochanteric stabilization plate may be a valid alternative.97 In addition, when an intramedullary nail is chosen for an intertrochanteric fracture, the use of a short nail is associated with less estimated blood loss, shorter operative time, and a lower transfusion rate compared to a long nail, without compromising healing.60–62 In regards of femoral neck fractures requiring arthroplasty, hemiarthroplasty (HA) is consistently associated with less operative blood loss and lower transfusion rates than total hip arthroplasty (THA).63–65
Besides, minimally invasive surgical techniques also contribute to blood conservation. A randomized trial comparing a minimally invasive side plate system to a conventional implant for trochanteric fractures found a significant reduction in perioperative bleeding with the minimally invasive approach.98 Furthermore, external fixation, as a minimally invasive alternative for high-risk patients, has been shown to drastically reduce transfusion needs and LOS compared to DHS.99
Hidden Blood Loss and Other Perioperative Considerations
A significant and often underappreciated component of perioperative blood loss is HBL, which comprises extravasation into tissues and hemolysis, not captured in surgical suction or drains. In elderly patients with intertrochanteric fractures undergoing intramedullary nailing, HBL can account for over 80% of total perioperative blood loss.37,54 Factors independently associated with increased perioperative HBL include unstable fracture patterns (AO/OTA 31-A2.2 to A3.3), male sex, hypertension, low bone density, longer operative time (≥60 min), time from injury to operation (<2 days), blood transfusion, and without anticoagulation.37,55,56,100 Cooperated with early administration of TXA, meticulous surgical technique to minimize soft tissue dissection and operative time, alongside the use of minimally invasive approaches where appropriate, are practical measures to reduce both visible and hidden losses.
Other perioperative strategies hold physiological rationale. Intraoperative hypothermia is a modifiable risk factor for coagulopathy and increased bleeding, maintaining normothermia is therefore a simple yet important component of blood conservation.101 Intraoperative cell salvage is being actively investigated through RCTs like the WHITE 9 study, which aims to determine its clinical and cost-effectiveness in OHF surgery.102 Local hemostatic agents such as fibrin sealants, have also demonstrated reductions in transfusion rates compared to standard drainage in HA for femoral neck fractures.103
Transfusion Strategies: Thresholds, Outcomes, and the Case for Individualization
Despite comprehensive blood conservation strategies, ARBCT remains a common intervention in OHF perioperative care, with reported rates varying widely from 12.1% to over 40% across different settings.11,104 This variation underscores the absence of a universal consensus on the optimal transfusion trigger, making the development of evidence-based strategies for when to transfuse a critical component of perioperative management.
The Risk-Benefit Analysis of Allogeneic Transfusion
The decision to administer blood is complex, balancing the potential benefits of correcting anemia to improve oxygen delivery against the well-documented risks associated with transfusion, including immunomodulation, transfusion-related acute lung injury (TRALI), acute kidney injury (AKI), transfusion-associated circulatory overload (TACO), and infection.105–109 Regarding OHF, where patients are typically elderly with multiple comorbidities, this risk-benefit analysis is particularly nuanced. Observational data consistently link perioperative blood transfusion with adverse outcomes such as increased mortality, LOS, and higher readmission rates.18,19,27 A nationwide study in Scotland found transfusion was independently associated with higher 30- and 60-day mortality, delayed mobilization, and longer LOS. The authors concluded this was most likely a marker of perioperative anemia and patient vulnerability rather than a direct causal effect of transfusion.11 This is supported by analyses using propensity scoring to adjust for the likelihood of receiving a transfusion, which often negate the independent association between transfusion and mortality.110 Furthermore, the characteristics of the blood product itself, such as the storage duration, have not been conclusively shown to affect mortality or morbidity in OHF patients.111 Therefore, the focus should shift from viewing transfusion as a primary risk factor to recognizing it as a signal of a high-risk patient recognition, where the underlying anemia and its causes are the primary therapeutic targets.
The Restrictive versus Liberal Threshold Debate
Regarding the debate between restrictive and liberal transfusion thresholds, a restrictive strategy typically involves transfusing only when Hb falls below a specific trigger (eg, 7.0–8.0 g/dL) in asymptomatic, hemodynamically stable patients, while a liberal strategy uses a higher trigger (eg, 9.0–10.0 g/dL). A landmark Cochrane meta-analysis of 61 RCTs demonstrated that a restrictive threshold reduces transfusion rates by 42% without increasing 30-day mortality.112 A Cochrane review specific to OHF surgery and including six trials, found low-quality evidence of no significant difference in 30- or 60-day mortality, functional recovery, or most postoperative morbidities between liberal (Hb ~10 g/dL) and restrictive (Hb ~8 g/dL) thresholds. Notably, this review suggested a possible increased risk of myocardial infarction with a restrictive strategy.105 The FOCUS trial, as the largest RCT in this field, demonstrated no significant difference in three-year mortality or cause of death between a liberal strategy (maintaining Hb ≥10 g/dL) and a restrictive strategy (transfusion for symptoms or Hb <8 g/dL), supporting the safety of restrictive transfusion in the majority of elderly OHF patients.113 Another study implementing a protocol with an even more restrictive threshold of <7 g/dL for stable patients demonstrated a significant reduction in blood utilization (transfusion rate from 51% to 33%) and inpatient cardiac morbidity, with no increase in mortality, readmissions, or LOS.114
However, the application of a single Hb threshold for all frail, elderly OHF patients is challenged by evidence suggesting that certain vulnerable subgroups may benefit from a more liberal strategy. The TRIFE RCT in frail anemic patients from nursing homes or sheltered housing found no overall benefit of a liberal strategy (Hb target 11.3 g/dL) over a restrictive one (9.7 g/dL) for physical recovery or mortality at 30 days. However, a per-protocol analysis revealed a higher 30-day mortality with the restrictive strategy, and a prespecified subgroup analysis demonstrated a statistically significant lower 90-day mortality with the liberal strategy among nursing home residents (20% vs. 36%).115 A post-hoc analysis of this trial further demonstrated that a liberal transfusion strategy was associated with a significantly lower risk of postoperative delirium on day 10 compared to a restrictive strategy.116 This is a critical finding given that postoperative delirium is itself a strong independent predictor of increased 90-day mortality. Another RCT in cognitively intact patients found that while a liberal threshold (10.0 g/dL) did not improve ambulation scores compared to a restrictive one (8.0 g/dL), it was associated with fewer cardiovascular complications (2% vs. 10%) and lower in-hospital mortality (0% vs. 8%).117 In a meta-analysis, Gu et al specifically examining orthopedic patients revealed that restrictive strategies increased the risk of cardiovascular events, with the effect being particularly pronounced in OHF surgery.118 These studies collectively highlight that the factors beyond a simple Hb number such as baseline frailty, cognitive status, cardiovascular comorbidity, and the presence of symptoms like delirium or hemodynamic instability, must be integrated into the transfusion decision (Table 3).
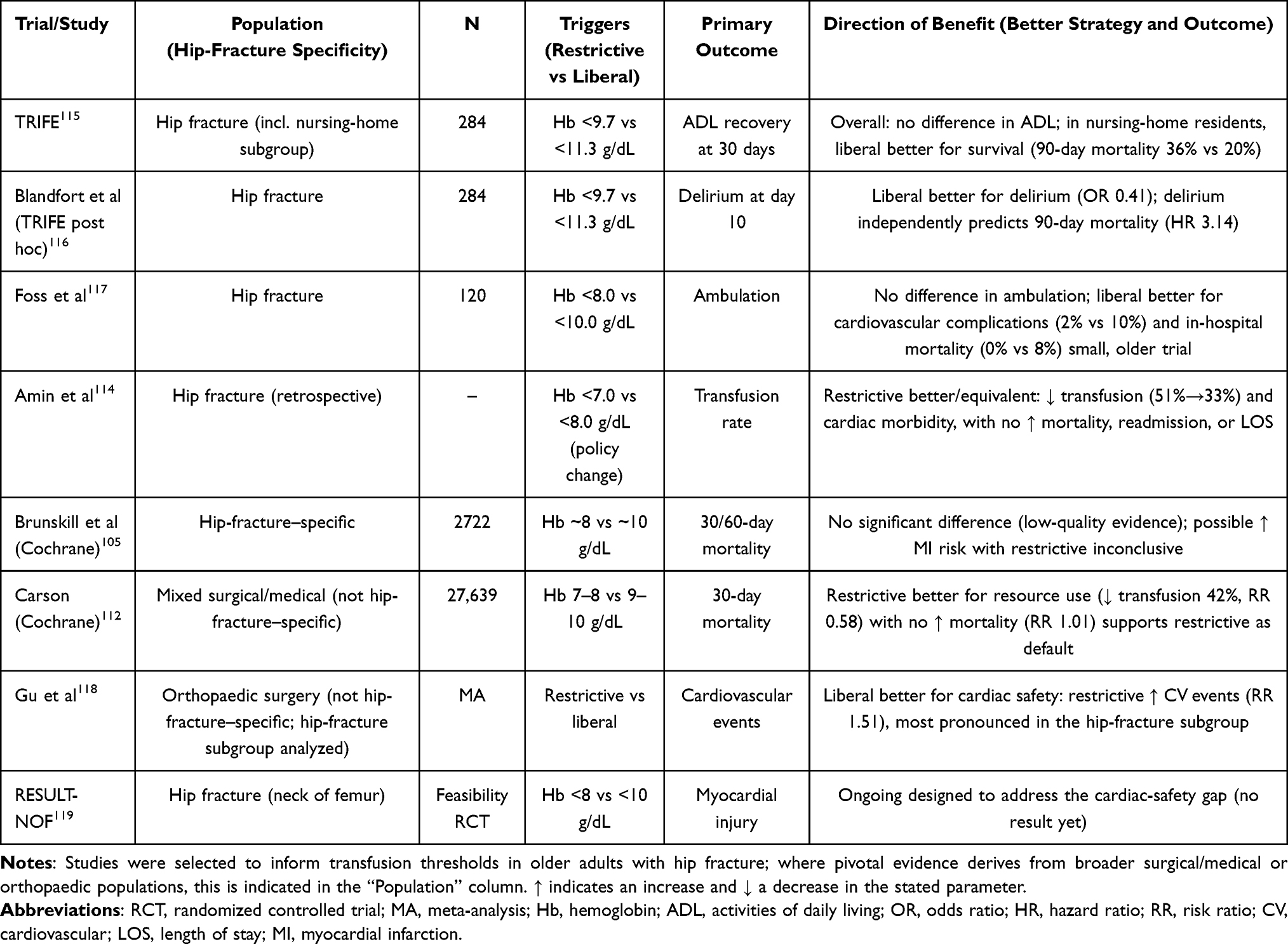 |
Table 3 Comparison of Restrictive versus Liberal Transfusion Strategies: Key Clinical Trials and Meta-Analyses in Hip Fracture Patients |
Individualized, Physiologically Guided Transfusion
The evidence above underscores the need for a more individualized, physiologically guided approach. The concept of “symptomatic anemia” is often cited in restrictive protocols but remains poorly defined. Emerging research points to dynamic physiological parameters that could refine decision-making. A multicenter cohort study in acute surgical patients including those with OHF, found that the combination of low Hb (<9.7 g/dL) and a low peripheral perfusion index (PPI<1.5) was strongly associated with increased 90-day mortality and severe complications. Notably, patients with low Hb but high PPI had a significantly better outcome, suggesting that PPI may help stratify risk among anemic patients and identify those who might benefit from earlier transfusion irrespective of the absolute Hb level.120 Furthermore, the duration and burden of anemia may be as important as its nadir. A prospective observational study using continuous non-invasive Hb monitoring revealed a significant delay in detecting anemia via intermittent blood sampling and found that the total accumulated time spent with low perioperative Hb (<10 g/dL) was associated with a higher incidence of postoperative delirium, suggesting that minimizing both the depth and duration of anemia, rather than just reacting to a single low value, could be a relevant therapeutic goal.23 The concept of the oxygen extraction ratio (P(v-a)CO2/C(a-v)O2), which reflects the balance between oxygen delivery and consumption, has been proposed as a physiologically rational transfusion trigger in sepsis and may have potential applicability in the perioperative OHF setting.121 However, it must be critically noted that these physiological parameters and continuous monitoring modalities remain largely exploratory in the orthogeriatric population; their diagnostic accuracy, cost-effectiveness, and definitive impact on clinical hard outcomes require validation in large-scale randomized trials before they can complement or replace standard hemoglobin triggers.
In clinical practice, the transfusion decision should therefore not be reduced to a single Hb threshold. A personalized approach should integrate the absolute Hb level with the patient’s symptom profile including cognitive and cardiovascular status, hemodynamic stability, anticipated further blood loss, trajectory of Hb change, and comorbid disease burden.114,117,119 The RESULT-NOF feasibility trial, which compared a restrictive (Hb <8 g/dL) and a liberal (Hb <10 g/dL) strategy specifically to prevent myocardial injury, represents ongoing efforts to define optimal thresholds for high-risk subgroups.119
Patient Blood Management Programs
The success of a restrictive transfusion policy is heavily dependent on parallel efforts to reduce bleeding and stimulate erythropoiesis within a formalized PBM approach. The implementation of a formal, multimodal PBM program has been shown to improve outcomes. A study evaluating a revised PBM protocol demonstrated a significant increase in the appropriateness of ARBCT transfusions (from 54% to 95%) alongside a decrease in transfusion rates, LOS, and 30-day readmissions.122 Observational data specifically associated IV iron administration on the third postoperative day with a lower 30-day mortality risk compared to no treatment in anemic OHF patients, highlighting that structured, protocol-driven care focusing on the entire patient management can optimize blood use and improve quality of care beyond merely adjusting a transfusion trigger.123 Comprehensive multimodal PBM incorporating perioperative IV iron (with or without rHuEPO) has been associated with reduced ARBCT rates, lower postoperative infection rates, and decreased 30-day mortality in pooled analyses.124 The widespread implementation of PBM remains variable across institutions, and harmonizing practice through standardized protocols is a key priority.125 An integrated, stage-based PBM pathway summarizing these recommendations is presented in Figure 1.
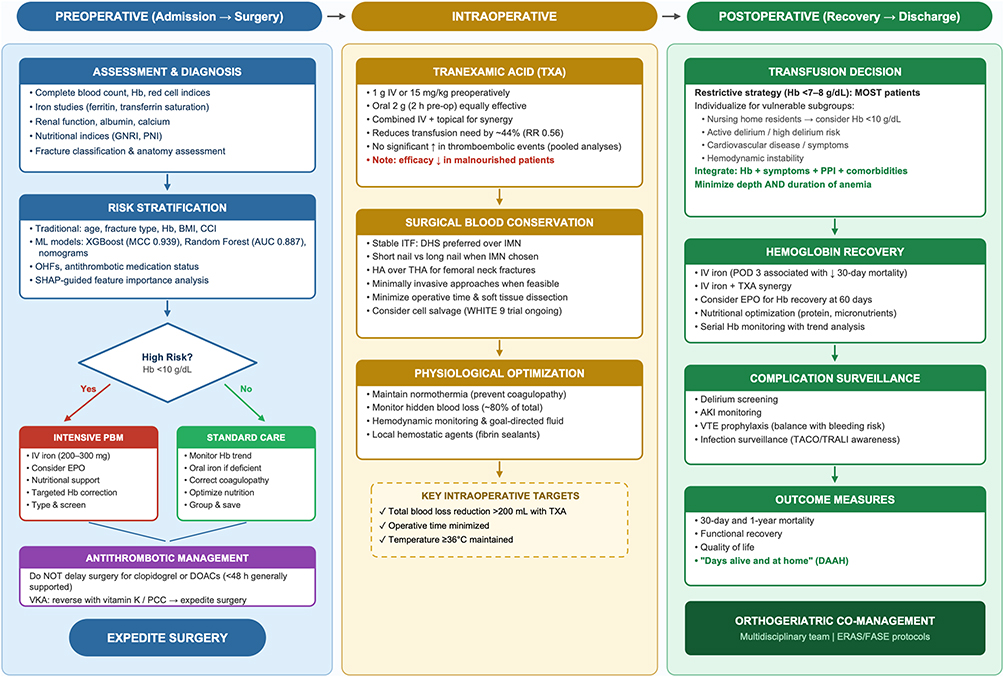 |
Figure 1 Multimodal Patient Blood Management (PBM) pathway for older adults with osteoporotic Hip fracture. Abbreviations: Hb, hemoglobin; GNRI, Geriatric Nutritional Risk Index; PNI, Prognostic Nutritional Index; CCI, Charlson Comorbidity Index; BMI, body mass index; ML, machine learning; MCC, Matthews Correlation Coefficient; AUC, area under the receiver operating characteristic curve; OHFs, osteoporotic hip fractures; SHAP, SHapley Additive exPlanations; IV, intravenous; EPO, erythropoietin; PBM, Patient Blood Management; DOACs, direct oral anticoagulants; TXA, tranexamic acid; ITF, intertrochanteric fractures; IMN, intramedullary nail; HA, hemiarthroplasty; THA, total hip arthroplasty; PPI, peripheral perfusion index; TACO, transfusion-associated circulatory; TRALI, transfusion-related acute lung injury; DAAH, days alive and at home. Notes: Arrows indicate the sequential progression of steps and the decision-making flow within the algorithm. ↑ indicates an increase or improvement, and ↓ indicates a reduction or decrease in the respective metric. |
Perioperative Management of Patients on Antithrombotic Therapy
A quintessential example of the high-risk patient cohort requiring individualized perioperative blood management is the growing cohort of elderly OHF patients receiving antithrombotic therapy. The management of antiplatelet agents (eg, clopidogrel, aspirin) and oral anticoagulants (vitamin K antagonists, direct oral anticoagulants) presents a significant clinical dilemma: balancing the imperatives of early surgical fixation against the perceived risks of increased perioperative bleeding. This conflict frequently results in surgical delays, which themselves are independently associated with poorer outcomes.126,127 Contemporary evidence, however, increasingly challenges the necessity of such delays, advocating for a more nuanced, patient-centered approach (Table 4).
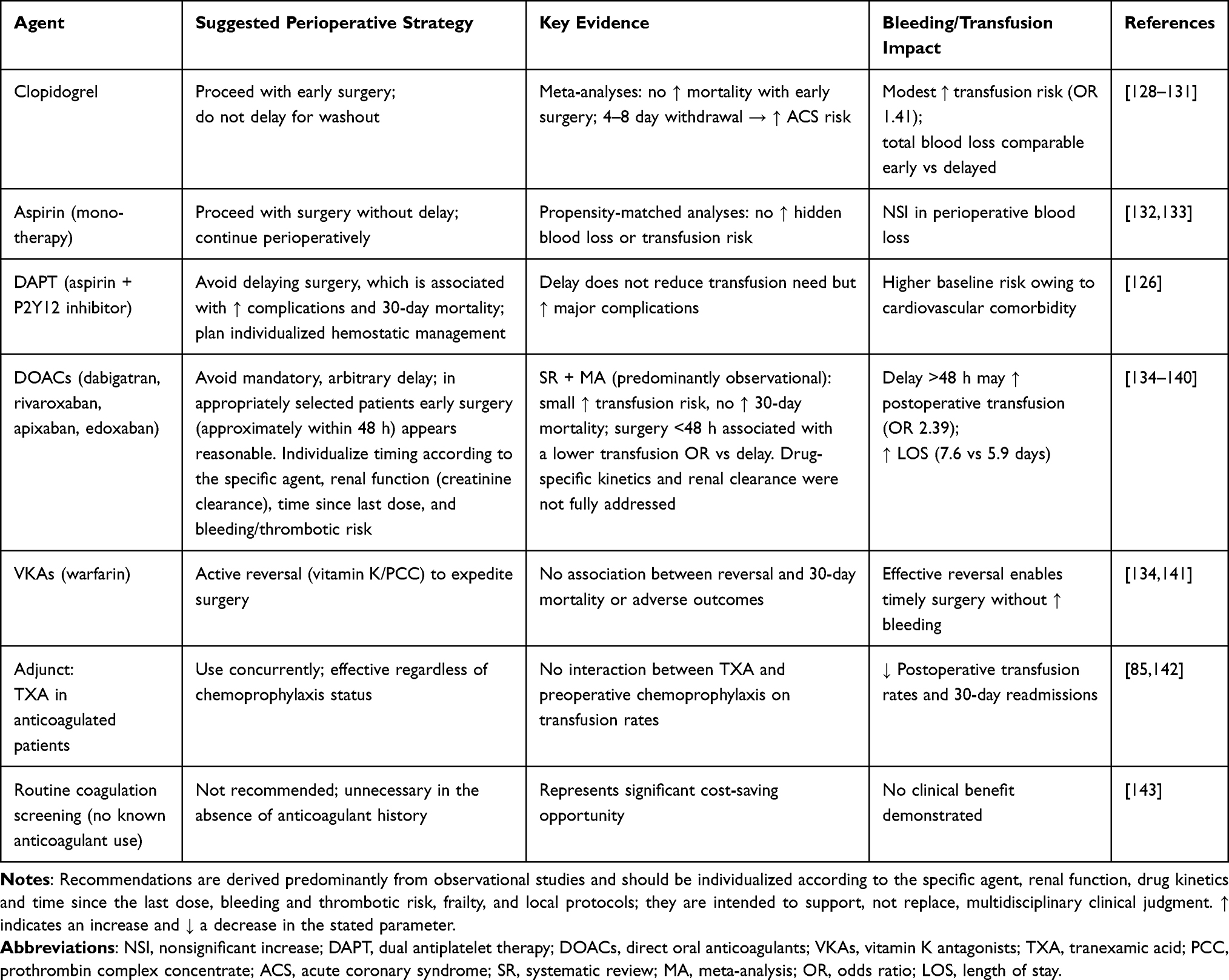 |
Table 4 Perioperative Management of Antithrombotic Therapy in Elderly Hip Fracture Patients: Evidence-Based Recommendations |
Patients on Clopidogrel and Antiplatelet Agents
For patients on clopidogrel, systematic reviews and meta-analyses have provided substantial evidence supporting the safety of early surgery. A meta-analysis found that early surgery in patients on clopidogrel was not associated with increased overall or 30-day mortality, while providing a significantly reduced LOS, despite a modest increase in transfusion risk.128 Soo et al concluded that early surgery was safe without a statistically significant increase in transfusion odds, recommending against withholding clopidogrel perioperatively due to the elevated risk of cardiovascular events associated with its discontinuation.129 Indeed, withdrawal of clopidogrel, particularly for 4 to 8 days, is associated with a significantly increased incidence of in-hospital acute coronary syndrome.130 Research indicates that while the timing of bleeding may differ with early surgery leading to more intraoperative loss and delayed surgery to more preoperative loss, the total blood loss and transfusion requirements are often comparable.131 Furthermore, delaying surgery in patients on dual antiplatelet therapy does not reduce transfusion need but is associated with increased probabilities of major complications and higher 30-day mortality.126 For patients on aspirin alone, propensity-matched analyses suggest it does not significantly increase perioperative HBL or transfusion risk, supporting immediate surgery.132,133
Patients on Direct Oral Anticoagulants
The management of patients on direct oral anticoagulants (DOACs) has also been studied. A systematic review concluded that performing surgery within 48 hours for DOAC-treated patients appears safe, with only a small associated increase in blood transfusion risk and no increase in 30-day mortality, although the underlying evidence is predominantly observational.134 Numerous cohort studies are consistent with this finding, reporting that expedited surgery is not associated with increased perioperative blood loss, transfusion rates, or major bleeding complications compared with delayed surgery.135–139 These studies are, however, susceptible to confounding by indication, as the decision to operate early may itself reflect a lower perceived bleeding risk. Brameier et al found that surgery within 48 hours of the last DOAC dose was associated with lower transfusion requirements (OR 2.39 for delayed surgery), shorter hospital stays (5.9 vs. 7.6 days), and no difference in complication rates.138 Kolodychuk et al similarly confirmed that early surgery for DOAC patients did not increase transfusion risk or mortality.140 While DOAC use is generally associated with a longer time to surgery compared to non-anticoagulated patients,127,142,144–146 protocols that do not mandate arbitrary delays can achieve comparable timelines.147
Patients on Vitamin K Antagonists and Perioperative Optimization
For patients on vitamin K antagonists, the implementation of reversal protocols using vitamin K or prothrombin complex concentrate has proven effective in reducing time to surgery without increasing bleeding risk.134,141 Yoo et al found no significant association between preoperative anticoagulation reversal and 30-day mortality or other outcomes.141 In addition, Salar et al demonstrated routine preoperative coagulation screening in the absence of known anticoagulant use appears unnecessary and represents a cost-saving opportunity.143
Several perioperative management strategies can further optimize outcomes in anticoagulated patients. The concomitant use of TXA is a key blood conservation strategy. Evidence from acetabular fracture surgery suggests that holding preoperative chemoprophylaxis does not alter TXA’s effect on transfusion rates, indicating TXA can be used effectively even in anticoagulated patients.85 In OHF, intravenous TXA has been associated with reduced postoperative transfusion rates and 30-day readmissions.142 Regional techniques like the lateral femoral cutaneous and over the hip block have been shown to be safe in anticoagulated patients, allowing for shorter time to surgery.148
It is crucial to contextualize the bleeding risk within the broader profile of these patients. Those on antithrombotic agents invariably have significant cardiovascular comorbidities, which explain their higher baseline risk. A Danish nationwide study found that preoperative antiplatelet use was associated with increased risks of transfusion and 30-day mortality, whereas DOACs were linked only to a slightly increased transfusion risk.149 The HASTE study reported that anticoagulated patients had a longer time to surgery and a higher 30-day mortality rate, but no difference in transfusion rates, suggesting that the delay itself may contribute to the mortality difference.127 Therefore, the increased mortality observed in several studies of anticoagulated patients is likely a marker of their greater burden of illness and frailty, rather than a direct consequence of the anticoagulant or its perioperative management, which is analogous to the interpretation of transfusion as a risk marker discussed previously.
Limitations
Several limitations of the current evidence base, and of this review, warrant acknowledgment. First, as a narrative review, this synthesis did not employ a formal systematic search or quantitative pooling, and the selection of studies, although intended to be representative, may be subject to selection bias. Second, much of the available evidence particularly regarding transfusion thresholds in specific subgroups, the perioperative management of anticoagulated patients, and the comparative effects of surgical techniques derives from retrospective and observational studies, which are inherently susceptible to confounding by indication and selection bias; the consistent associations between transfusion or anticoagulant use and adverse outcomes most likely reflect the greater frailty and comorbidity burden of the patients receiving these interventions rather than direct causal effects, an interpretation we have emphasized throughout. Third, prospective randomized validation remains limited for several of the strategies discussed, including individualized, physiologically guided transfusion triggers, the optimal management of antithrombotic therapy, and multimodal PBM bundles, so that a number of recommendations are necessarily provisional. Fourth, considerable clinical and methodological heterogeneity exists across studies with respect to patient populations, definitions of anemia and frailty, hemoglobin thresholds, outcome measures, and follow-up duration, limiting direct comparison and the generalizability of pooled estimates. Fifth, the evidence is least certain precisely in the most vulnerable groups of frail patients, nursing-home residents, and those with significant cardiovascular disease, in whom the balance between the risks of anemia and the risks of transfusion or surgical delay may differ from that in the broader population, yet who remain underrepresented in randomized trials. Finally, machine learning–based transfusion prediction models, although promising, currently share important limitations, most notably a predominance of single-center retrospective derivation, limited external and prospective validation, and an absence of demonstrated improvement in patient-centered outcomes. These limitations should be borne in mind when translating the evidence summarized here into individual clinical decisions.
Clinical Implications, Knowledge Gaps, and Conclusion
The perioperative management of anemia and the judicious use of blood transfusions in older adults with OHFs represent a cornerstone of high-quality, patient-centered care. This population, characterized by frailty, multimorbidity, and a high prevalence of preoperative anemia, is uniquely vulnerable to the detrimental effects of both anemia and its treatments. The accumulated evidence underscores that anemia is not merely a laboratory finding to be corrected, but a critical modifiable risk factor embedded within a complex clinical environment. Therefore, effective management transcends a simple Hb-centric transfusion trigger, demanding an individualized and proactive approach encompassing the entire perioperative management period from admission to recovery.
Core Evidence-Based Recommendations
Current evidence strongly supports the integration of several key principles into structured care pathways. First, systematic preoperative assessment and risk stratification increasingly augmented by ML-based predictive models, enable early identification of high-risk patients and targeted intervention. Second, TXA is an effective blood conservation agent with a favorable safety profile in most patients and is endorsed by major guidelines as a core component of PBM; caution nonetheless remains warranted in individuals at high thromboembolic risk, for whom dedicated evidence is limited. Emerging data further suggest that its combination with IV iron may yield synergistic benefits. Third, a restrictive transfusion strategy (Hb trigger of 7–8 g/dL) is safe for the majority of patients, but an individualized approach incorporating physiological parameters, symptom burden, and frailty status is essential for the most vulnerable subgroups, particularly nursing home residents and those at high risk for delirium or cardiovascular events. Fourth, current evidence, although predominantly observational and therefore susceptible to confounding, suggests that surgery generally need not be delayed solely on the basis of antithrombotic medication status, as the risks of delay appear to outweigh the modest incremental bleeding risk in most patients. This approach should nonetheless be individualized according to each patient’s bleeding and thrombotic risk, the specific agent involved, and local protocols, particularly in the absence of large randomized trials. The establishment of Fast Access to Surgery in Emergency (FASE) strategies and Enhanced Recovery After Surgery (ERAS) protocols demonstrates tangible benefits in streamlining care, reducing time-to-surgery, and potentially minimizing perioperative blood loss. The evolution of orthogeriatric co-management models, now extending into elective orthopedic settings, provides a robust organizational template for integrated, multidisciplinary care.
Unresolved Controversies and Evidence Gaps
Technological innovations continue to refine perioperative blood conservation, including the ongoing evaluation of intraoperative cell salvage in the WHITE 9 trial,102 and the advent of robot-assisted techniques for fracture fixation showing promise in reducing intraoperative blood loss.150 The application of ML to develop increasingly accurate and interpretable predictive models for transfusion risk represents a significant advancement towards truly personalized care. Future efforts should prioritize the development of user-friendly clinical decision support systems that can be integrated into electronic health records for real-time risk assessment. The validation of emerging physiological biomarkers such as the PPI and continuous non-invasive Hb monitoring, as dynamic transfusion triggers, also warrants prospective investigation. In addition, a critical future direction is the adoption of more patient-centered outcome measures. Traditional endpoints like mortality and LOS, while important, may not fully capture the functional recovery and quality of life that matter most to older patients. For instance, the metric “days alive and at home” has been validated as a meaningful composite outcome that reflects a patient’s ability to return to their pre-fracture environment and independence.151 Its use in clinical trials and quality audits can shift the focus towards outcomes that align with patient priorities.
Future Perspectives and Methodological Horizons
In conclusion, the management of perioperative anemia in OHF care is a dynamic field at the intersection of geriatrics, hematology, anesthesiology, and surgery. The path forward is characterized by a shift from reactive transfusion to proactive, multimodal PBM embedded within integrated care pathways. Success depends on the seamless collaboration of a multidisciplinary team, the implementation of evidence-based protocols, the strategic adoption of supportive technologies, and a steadfast commitment to measuring what truly matters to patients. As demographic pressures mount, refining and disseminating these comprehensive management strategies will be paramount to improving survival, function, and quality of life for these growing number of older adults suffering from devastating injuries.
Furthermore, a critical paradigm shift must occur in clinical trial methodology: future research should transition from traditional, short-term endpoints (such as in-hospital length of stay or 30-day mortality) toward broader, patient-centered composite metrics. The validation and adoption of metrics like “Days Alive and At Home” (DAAH) will ensure that future blood management strategies align directly with the recovery of independence, functional mobility, and quality of life that matter most to our aging patient population. Notably, functional outcome assessments should move beyond generic mobility scores to encompass culturally specific activities of daily living. As highlighted by recent initiatives,152 recognizing and measuring distinct activities such as specific prayer movements, is essential for a more granular, inclusive, and culturally competent evaluation of post-fracture recovery.
Abbreviations
OHFs, Osteoporotic hip fractures; ARBCT, allogeneic red blood cell transfusion; LOS, length of hospital stay; BMI, body mass index; PNI, Prognostic Nutritional Index; GNRI, Geriatric Nutritional Risk Index; CCI, Charlson Comorbidity Index; mFI, modified Frailty Index; mECM, modified Elixhauser’s Comorbidity Measure; ML, machine learning; RF, random forest; AUC, area under the receiver operating characteristic curve; SHAP, SHapley Additive exPlanations; PFNA, proximal femoral anti-rotation nailing; IV, intravenous; EPO, erythropoietin; PBM, Patient Blood Management; TXA, tranexamic acid; DVT, deep vein thrombosis; PE, pulmonary embolism; HBL, hidden blood loss; DHS, dynamic hip screw; CMN, cephalomedullary nail; HA, hemiarthroplasty; THA, total hip arthroplasty; TRALI, transfusion-related acute lung injury; AKI, acute kidney injury; TACO, transfusion-associated circulatory overload; PPI, peripheral perfusion index; DOACs, direct oral anticoagulants; FASE, Fast Access to Surgery in Emergency; ERAS, Enhanced Recovery After Surgery; DAAH, Days Alive and At Home.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Natural Science Foundation of China (No.82502974), Natural Science Basic Research Program of Shaanxi Province (No. 2025JC-YBQN-1113 and 2025JC-YBQN-1181), Youth Top-Notch Talent Support Program of Honghui Hospital, Xi’an Jiaotong University (ynrc2024044), the Seed Funding Program of the Honghui Hospital, Xi’an Jiaotong University (No. 2025zz-qn03), and the Fundamental Research Fund of Xi’an Jiaotong University (No. xzy012026149 and xzy012026153). The funding source had no influence on the study design, data collection, analysis, or interpretation of the findings.
Disclosure
The authors declare that they have no conflict of interest to disclose.
References
1. Chen M, Zhang Y, Du Y, et al. Epidemiological and clinical study of hip fracture in hospitalized elderly patients in Shanghai, China. Arch Osteoporos. 2019;14(1):37. doi:10.1007/s11657-019-0580-7
2. Quevedo I, Ormeño JC, Weissglas B, Opazo C. Epidemiology and direct medical cost of osteoporotic hip fracture in Chile. J Osteoporos. 2020;2020:5360467. doi:10.1155/2020/5360467
3. Griffiths R, Babu S, Dixon P, et al. Guideline for the management of hip fractures 2020: guideline by the association of anaesthetists. Anaesthesia. 2021;76(2):225–21. doi:10.1111/anae.15291
4. Zhou Y, Wang S, Wu Z, et al. An explainable and supervised machine learning model for prediction of red blood cell transfusion in patients during Hip fracture surgery. BMC Anesthesiol. 2024;24(1):467. doi:10.1186/s12871-024-02832-y
5. Šarić Jadrijev A, Bego A, Lojpur B, et al. Admission hemoglobin associated with increased mortality in hip fracture surgical patients: an observational study. Biomedicines. 2024;12(9):2041. doi:10.3390/biomedicines12092041
6. Puckeridge G, Terblanche M, Wallis M, Fung YL. Blood management in hip fractures; are we leaving it too late? A retrospective observational study. BMC Geriatr. 2019;19(1):79. doi:10.1186/s12877-019-1099-x
7. Potter LJ, Doleman B, Moppett IK. A systematic review of pre-operative anaemia and blood transfusion in patients with fractured hips. Anaesthesia. 2015;70(4):483–500. doi:10.1111/anae.12978
8. Min L, Linyi Y, Chen L, Jiang S, Chen C. Preoperative moderate to severe anemia is associated with increased postoperative major adverse cardiac and cerebral events and pulmonary complications: a propensity score-matched analysis in Hip fracture surgery patients over 80 years old. Perioper Med. 2023;12(1):56. doi:10.1186/s13741-023-00349-5
9. Li M, Chen C, Shen J, Yang L. Preoperative hemoglobin <10 g/DL predicts an increase in major adverse cardiac events in patients with hip fracture over 80 years: a retrospective cohort study. Geriatr Orthop Surg Rehabil. 2023;14:21514593231183611. doi:10.1177/21514593231183611
10. Smith A, Moon T, Pak T, Park B, Urman RD. Preoperative anemia treatment with intravenous iron in patients undergoing major orthopedic surgery: a systematic review. Geriatr Orthop Surg Rehabil. 2020;11:2151459320935094. doi:10.1177/2151459320935094
11. Farrow L, Brasnic L, Martin C, et al. A nationwide study of blood transfusion in hip fracture patients: linked analysis from the Scottish Hip Fracture Audit and the Scottish National Blood Transfusion Service. Bone Joint J. 2022;104-B(11):1266–1272. doi:10.1302/0301-620X.104B11.BJJ-2022-0450.R1
12. Khan I, Jawaid A, Ahmad K, Noordin S. Hip fragility fractures: anaemia, calcium and vitamin D supplementation. J Pak Med Assoc. 2015;65(11 Suppl 3):S55–8.
13. Rocos B, Whitehouse MR, Kelly MB. Resuscitation in Hip fractures: a systematic review. BMJ Open. 2017;7(4):e015906. doi:10.1136/bmjopen-2017-015906
14. Espinosa KA, Gélvez AG, Torres LP, García MF, Peña OR. Pre-operative factors associated with increased mortality in elderly patients with a Hip fracture: a cohort study in a developing country. Injury. 2018;49(6):1162–1168. doi:10.1016/j.injury.2018.04.007
15. Ryan G, Nowak L, Melo L, et al. Anemia at presentation predicts acute mortality and need for readmission following geriatric hip fracture. JB JS Open Access. 2020;5(3). doi:10.2106/JBJS.OA.20.00048.
16. Zhang L, Yin P, Lv H, et al. Anemia on admission is an independent predictor of long-term mortality in hip fracture population: a prospective study with 2-year follow-up. Medicine. 2016;95(5):e2469. doi:10.1097/MD.0000000000002469
17. Yombi JC, Putineanu DC, Cornu O, Lavand’homme P, Cornette P, Castanares-Zapatero D. Low haemoglobin at admission is associated with mortality after Hip fractures in elderly patients. Bone Joint J. 2019;101-B(9):1122–1128. doi:10.1302/0301-620X.101B9.BJJ-2019-0526.R1
18. Shin HJ, Kim JH, Han SB, Park JH, Jang WY. Allogeneic red blood cell transfusion is an independent risk factor for 1-year mortality in elderly patients undergoing femoral neck fracture surgery: retrospective study. Medicine. 2020;99(35):e21897. doi:10.1097/MD.0000000000021897
19. Guo J, Geng Q, Xu K, et al. Development and validation of models for predicting mortality in intertrochanteric fracture surgery patients with perioperative blood transfusion: a prospective multicenter cohort study. Int J Surg. 2024;110(8):4754–4766. doi:10.1097/JS9.0000000000001472
20. Jiang Y, Lin X, Wang Y, et al. Preoperative anemia and risk of in-hospital postoperative complications in patients with hip fracture. Clin Interv Aging. 2023;18:639–653. doi:10.2147/CIA.S404211
21. Sim YE, Sim SD, Seng C, Howe TS, Koh SB, Abdullah HR. Preoperative anemia, functional outcomes, and quality of life after hip fracture surgery. J Am Geriatr Soc. 2018;66(8):1524–1531. doi:10.1111/jgs.15428
22. Bruce K, Mangram A, Sucher JF, et al. Consequences of anemia in geriatric hip fractures: how low is too low? Trauma Surg Acute Care Open. 2024;9(1):e001175. doi:10.1136/tsaco-2023-001175
23. Clemmesen CG, Palm H, Foss NB. Delay in detection and treatment of perioperative anemia in hip fracture surgery and its impact on postoperative outcomes. Injury. 2019;50(11):2034–2039. doi:10.1016/j.injury.2019.09.001
24. Syamala S, Tarazona-Santabalbina FJ, Passarelli JL, Nadukkandiyil N, Saleh H, Alhamad H. Preoperative hemoglobin level and its relationship with mortality and adverse outcomes in older hip fracture patients from Qatar. BMC Geriatr. 2025;25(1):959. doi:10.1186/s12877-025-06653-7
25. Zhang N, Zhang D, Ren S, Gao Y, Sun W, Yang S. Relationship between preoperative hemoglobin levels and length of stay in elderly patients with hip fractures: a retrospective cohort study. Medicine. 2024;103(25):e38518. doi:10.1097/MD.0000000000038518
26. Guo Z, Zhao F, Wang Y, Wang X. Intensive care unit resource utilization after hip fracture surgery in elderly patients: risk factor identification and risk stratification. Orthopedics. 2020;43(3):e159–e165. doi:10.3928/01477447-20200129-02
27. Arshi A, Lai WC, Iglesias BC, et al. Blood transfusion rates and predictors following geriatric Hip fracture surgery. Hip Int. 2021;31(2):272–279. doi:10.1177/1120700019897878
28. Mori Y, Tarasawa K, Tanaka H, et al. Low BMI and postoperative outcomes in elderly Hip fracture patients: a Japanese nationwide database study. J Bone Miner Metab. 2026;44(1):97–105. doi:10.1007/s00774-025-01660-5
29. Lui DTW, Lee CH, Chan YH, et al. HbA1c variability, in addition to mean HbA1c, predicts incident hip fractures in Chinese people with type 2 diabetes. Osteoporos Int. 2020;31(10):1955–1964. doi:10.1007/s00198-020-05395-z
30. Scott D, Seibel MJ, Cumming R, et al. Comparison of clinical risk factors for incident fracture in obese and non-obese community-dwelling older men. Bone. 2020;137:115433. doi:10.1016/j.bone.2020.115433
31. Tunçez M, Bulut T, Süner U, Önder Y, Kazımoğlu C. Prognostic nutritional index (PNI) is an independent risk factor for the postoperative mortality in geriatric patients undergoing Hip arthroplasty for femoral neck fracture? A prospective controlled study. Arch Orthop Trauma Surg. 2024;144(3):1289–1295. doi:10.1007/s00402-024-05201-z
32. Yokoyama K, Ukai T, Watanabe M. Effect of nutritional status before femoral neck fracture surgery on postoperative outcomes: a retrospective study. BMC Musculoskelet Disord. 2021;22(1):1027. doi:10.1186/s12891-021-04913-2
33. Segura-Nuez JC, Herranz-Andrés P, Infantes-Morales M, Segura-Nuez J, Martín-Hernández C, Roche-Albero A. Blood transfusion risk factors in patients with osteoporotic hip fracture. Arch Orthop Trauma Surg. 2025;145(1):314. doi:10.1007/s00402-025-05930-9
34. Harper KD, Navo P, Ramsey F, Jallow S, Rehman S. “Hidden” preoperative blood loss with extracapsular versus intracapsular hip fractures: what is the difference? Geriatr Orthop Surg Rehabil. 2017;8(4):202–207. doi:10.1177/2151458517729615
35. Hourston GJM, Chan JJ, Cooper H, Quinn KR, Parker M. The impact of Hip fracture anatomy on admission haemoglobin levels and perioperative transfusion requirements: a 32-year experience. Eur J Orthop Surg Traumatol. 2025;35(1):399. doi:10.1007/s00590-025-04521-z
36. Müller F, Doblinger M, Kottmann T, Füchtmeier B. PFNA and DHS for AO/OTA 31-A2 fractures: radiographic measurements, morbidity and mortality. Eur J Trauma Emerg Surg. 2020;46(5):947–953. doi:10.1007/s00068-019-01251-w
37. Guo J, Zhang Y, Hou Z. Intramedullary fixation does not cause a large amount of hidden blood loss in elderly patients with intertrochanteric fractures. Clin Interv Aging. 2021;16:475–486. doi:10.2147/CIA.S301737
38. Lewis SR, Pritchard MW, Estcourt LJ, Stanworth SJ, Griffin XL. Interventions for reducing red blood cell transfusion in adults undergoing Hip fracture surgery: an overview of systematic reviews. Cochrane Database Syst Rev. 2023;6(6):Cd013737. doi:10.1002/14651858.CD013737.pub2
39. Guo J, He Q, Li Y. Development and validation of machine learning models to predict perioperative transfusion risk for hip fractures in the elderly. Ann Med. 2024;56(1):2357225. doi:10.1080/07853890.2024.2357225
40. Wei D, Jiang Y, Long X, et al. Predicting the perioperative transfusion risk of proximal femoral antirotation nailing (PFNA) for elderly patients with intertrochanteric fractures: a new predictive nomogram. Biomed Eng Online. 2025;24(1):80. doi:10.1186/s12938-025-01419-z
41. Wei J, Zeng L, Li S, Luo F, Xiang Z, Ding Q. Relationship between comorbidities and treatment decision-making in elderly hip fracture patients. Aging Clin Exp Res. 2019;31(12):1735–1741. doi:10.1007/s40520-019-01134-5
42. Guo J, Di J, Gao X, et al. Discriminative ability for adverse outcomes after hip fracture surgery: a comparison of three commonly used comorbidity-based indices. Gerontology. 2022;68(1):62–74. doi:10.1159/000515526
43. Guo J, Zhang B, Yu H, et al. Propensity score matching analysis of early vs. delayed surgery for intertrochanteric fracture in older patients: a retrospective multicenter cohort study of 7414 patients with a mean 4-year follow up. BMC Geriatr. 2024;24(1):821. doi:10.1186/s12877-024-05415-1
44. Zhang Y, Lu K, Liu Q, Liu C, Su S, Yang C. Hypocalcemia was associated with increased perioperative blood loss and blood transfusion in elderly patients with Hip fracture: a retrospective study. BMC Surg. 2025;25(1):134. doi:10.1186/s12893-025-02872-2
45. C M, V R, P C, et al. Euthyroid sick syndrome in Hip fractures: evaluation of postoperative anemia. Injury. 2020;51 Suppl 3:S9–s12. doi:10.1016/j.injury.2020.07.006
46. Bian FC, Cheng XK, An YS. Preoperative risk factors for postoperative blood transfusion after hip fracture surgery: establishment of a nomogram. J Orthop Surg Res. 2021;16(1):406. doi:10.1186/s13018-021-02557-5
47. Amin RM, Puvanesarajah V, Chaudhry YP, et al. Reducing unnecessary crossmatching for hip fracture patients by accounting for preoperative hemoglobin concentration. World J Orthop. 2021;12(5):292–300. doi:10.5312/wjo.v12.i5.292
48. Sun L, Liu Z, Wu H, Liu B, Zhao B. Validation of the nottingham hip fracture score in predicting postoperative outcomes following hip fracture surgery. Orthop Surg. 2023;15(4):1096–1103. doi:10.1111/os.13624
49. Shen Y, Hao Q, Wang Y, et al. The association between preoperative modified frailty index and postoperative complications in Chinese elderly patients with Hip fractures. BMC Geriatr. 2021;21(1):370. doi:10.1186/s12877-021-02330-7
50. Sagona A, Ortega CA, Wang L, et al. Frailty is more predictive of mortality than age in patients with hip fractures. J Orthop Trauma. 2024;38(8):e278–e287. doi:10.1097/BOT.0000000000002844
51. Cozza M, Boccardi V, Duka R, Vashist Y, Marano L. Blood transfusion in older surgical patients: the only option or is there a better approach? Aging Clin Exp Res. 2025;37(1):135. doi:10.1007/s40520-025-03033-4
52. Xie J, Himeno S. Tranexamic acid efficacy in geriatric hip fractures: impact of nutritional status on blood loss, transfusion rates, and safety. BMC Musculoskelet Disord. 2024;25(1):553. doi:10.1186/s12891-024-07665-x
53. Chen X, Pan J, Li Y, Tang R. Application of machine learning model in predicting the likelihood of blood transfusion after hip fracture surgery. Aging Clin Exp Res. 2023;35(11):2643–2656. doi:10.1007/s40520-023-02550-4
54. Luo X, He S, Li Z, Li Q. Quantification and influencing factors of perioperative hidden blood loss during intramedullary fixation for intertrochanteric fractures in the elderly. Arch Orthop Trauma Surg. 2020;140(10):1339–1348. doi:10.1007/s00402-019-03311-7
55. Lin PH, Chien JT, Hung JP, Hong CK, Tsai TY, Yang CC. Unstable intertrochanteric fractures are associated with a greater hemoglobin drop during the perioperative period: a retrospective case control study. BMC Musculoskelet Disord. 2020;21(1):244. doi:10.1186/s12891-020-03208-2
56. Cui H, Chen K, Lv S, Yuan C, Wang Y. An analysis of perioperative hidden blood loss in femoral intertrochanteric fractures: bone density is an important influencing factor. BMC Musculoskelet Disord. 2021;22(1):6. doi:10.1186/s12891-020-03922-x
57. Alessio-Mazzola M, Traverso G, Coccarello F, Sanguineti F, Formica M. Dynamic Hip screw versus intramedullary nailing for the treatment of A1 intertrochanteric fractures: a retrospective, comparative study and cost analysis. Jt Dis Relat Surg. 2022;33(2):314–322. doi:10.52312/jdrs.2022.646
58. Cai L, Wang T, Di L, Hu W, Wang J. Comparison of intramedullary and extramedullary fixation of stable intertrochanteric fractures in the elderly: a prospective randomised controlled trial exploring hidden perioperative blood loss. BMC Musculoskelet Disord. 2016;17(1):475. doi:10.1186/s12891-016-1333-z
59. Ronga M, Bonzini D, Valoroso M, et al. Blood loss in trochanteric fractures: multivariate analysis comparing dynamic hip screw and Gamma nail. Injury. 2017;48 Suppl 3:S44–S47. doi:10.1016/S0020-1383(17)30657-5
60. Cinque ME, Goodnough LH, BJS M, et al. Short versus long cephalomedullary nailing of intertrochanteric fractures: a meta-analysis of 3208 patients. Arch Orthop Trauma Surg. 2022;142(7):1367–1374. doi:10.1007/s00402-021-03752-z
61. Zhang Y, Zhang S, Wang S, et al. Long and short intramedullary nails for fixation of intertrochanteric femur fractures (OTA 31-A1, A2 and A3): a systematic review and meta-analysis. Orthop Traumatol Surg Res. 2017;103(5):685–690. doi:10.1016/j.otsr.2017.04.003
62. Konda SR, Merrell LA, Esper GW, et al. No difference in clinical and hospital quality outcomes in treatment of reverse obliquity intertrochanteric hip fractures (AO/OTA 31.A3) based on Cephalomedullary nail length. Injury. 2024;55(4):111463. doi:10.1016/j.injury.2024.111463
63. Yin Z, Zhu Z, Wang C, Jia X, Zou X. Comparison of the surgical efficacy of total Hip replacement versus hemiarthroplasty in the treatment of femoral neck fractures in elderly patients with sarcopenia. PLoS One. 2025;20(4):e0321070. doi:10.1371/journal.pone.0321070
64. Haynes MS, Ondeck NT, Ottesen TD, Malpani R, Rubin LE, Grauer JN. Perioperative outcomes of hemiarthroplasty versus total hip arthroplasty for geriatric hip fracture: the importance of studying matched populations. J Arthroplasty. 2020;35(11):3188–3194. doi:10.1016/j.arth.2020.06.015
65. Lu X, Gou W, Wu S, Wang Y, Wang Z, Xiong Y. Complication rates and survival of nonagenarians after hip hemiarthroplasty versus proximal femoral nail antirotation for intertrochanteric fractures: a 15-year retrospective cohort study of 113 cases. Orthop Surg. 2023;15(12):3231–3242. doi:10.1111/os.13913
66. Yoon BH, Lee BS, Won H, Kim HK, Lee YK, Koo KH. Preoperative iron supplementation and restrictive transfusion strategy in hip fracture surgery. Clin Orthopedic Surg. 2019;11(3):265–269. doi:10.4055/cios.2019.11.3.265
67. Schack A, Berkfors AA, Ekeloef S, Gögenur I, Burcharth J. The effect of perioperative iron therapy in acute major non-cardiac surgery on allogenic blood transfusion and postoperative haemoglobin levels: a systematic review and meta-analysis. World J Surg. 2019;43(7):1677–1691. doi:10.1007/s00268-019-04971-7
68. García-Erce JA, Cuenca J, Haman-Alcober S, Martínez AA, Herrera A, Muñoz M. Efficacy of preoperative recombinant human erythropoietin administration for reducing transfusion requirements in patients undergoing surgery for hip fracture repair. An observational cohort study. Vox Sang. 2009;97(3):260–267.
69. Bernabeu-Wittel M, Romero M, Ollero-Baturone M, et al. Ferric carboxymaltose with or without erythropoietin in anemic patients with Hip fracture: a randomized clinical trial. Transfusion. 2016;56(9):2199–2211. doi:10.1111/trf.13624
70. Bultynck C, Munim N, Harrington DJ, et al. Prevalence of vitamin K deficiency in older people with Hip fracture. Acta Clin Belg. 2020;75(2):136–140. doi:10.1080/17843286.2018.1564174
71. Kim KH, Kim NY. Can early surgery reduce the need to packed red blood cell transfusion in elderly patients with intertrochanteric femur fractures? Injury. 2021;52(10):3047–3050. doi:10.1016/j.injury.2021.01.036
72. Kappenschneider T, Maderbacher G, Weber M, et al. Special orthopaedic geriatrics (SOG) - a new multiprofessional care model for elderly patients in elective orthopaedic surgery: a study protocol for a prospective randomized controlled trial of a multimodal intervention in frail patients with Hip and knee replacement. BMC Musculoskelet Disord. 2022;23(1):1079. doi:10.1186/s12891-022-05955-w
73. Hili S, Dawe EJ, Lindisfarne EA, Stott PM. Perioperative management of elderly patients suffering a Hip fracture. Br J Hosp Med. 2014;75(2):78–82. doi:10.12968/hmed.2014.75.2.78
74. Fu M, Guo J, Zhang Y, et al. Effect of integrated management bundle on 1-year overall survival outcomes and perioperative outcomes in super elderly patients aged 90 and over with Hip fracture: non-concurrent cohort study. BMC Musculoskelet Disord. 2022;23(1):778. doi:10.1186/s12891-022-05720-z
75. Fu M, Zhang Y, Guo J, et al. Application of integrated management bundle incorporating with multidisciplinary measures improved in-hospital outcomes and early survival in geriatric Hip fracture patients with perioperative heart failure: a retrospective cohort study. Aging Clin Exp Res. 2022;34(5):1149–1158. doi:10.1007/s40520-021-02038-z
76. Augustinus S, Mulders MAM, Gardenbroek TJ, Goslings JC. Tranexamic acid in Hip hemiarthroplasty surgery: a systematic review and meta-analysis. Eur J Trauma Emerg Surg. 2023;49(3):1247–1258. doi:10.1007/s00068-022-02180-x
77. Jiang W, Shang L. Tranexamic acid can reduce blood loss in patients undergoing intertrochanteric fracture surgery: a meta-analysis. Medicine. 2019;98(11):e14564. doi:10.1097/MD.0000000000014564
78. Zhao YK, Zhang C, Zhang YW, et al. Efficacy and safety of tranexamic acid in elderly patients with femoral neck fracture treated with Hip arthroplasty: a systematic review and meta-analysis. J Orthopaed Sci. 2024;29(2):542–551. doi:10.1016/j.jos.2023.01.010
79. Masouros P, Antoniou G, Nikolaou VS. Efficacy and safety of tranexamic acid in Hip fracture surgery. How does dosage affect outcomes: a meta-analysis of randomized controlled trials. Injury. 2022;53(2):294–300. doi:10.1016/j.injury.2021.09.063
80. Baskaran D, Rahman S, Salmasi Y, Froghi S, Berber O, George M. Effect of tranexamic acid use on blood loss and thromboembolic risk in Hip fracture surgery: systematic review and meta-analysis. Hip Int. 2018;28(1):3–10. doi:10.5301/hipint.5000556
81. Leverett GD, Marriott A. Intravenous tranexamic acid and thromboembolic events in Hip fracture surgery: a systematic review and meta-analysis. Orthop Traumatol Surg Res. 2023;109(2):103337. doi:10.1016/j.otsr.2022.103337
82. Graif N, Warschawski Y, Amzallag N, et al. Effect of intraoperative tranexamic acid on blood loss and outcomes in intertrochanteric fractures: a retrospective study of 1728 patients. Eur J Orthop Surg Traumatol. 2025;35(1):380. doi:10.1007/s00590-025-04504-0
83. Haj-Younes B, Sivakumar BS, Wang M, An VV, Lorentzos P, Adie S. Tranexamic acid in Hip fracture surgery: a systematic review and meta-analysis. J Orthopaed Surg. 2020;28(1):2309499019887995. doi:10.1177/2309499019887995
84. van Rijckevorsel V, Roukema GR, Kuijper TM, de Jong L. Clinical outcomes of tranexamic acid in acute Hip hemiarthroplasties in frail geriatric patients. Orthop Traumatol Surg Res. 2022;108(5):103219. doi:10.1016/j.otsr.2022.103219
85. Wadhwa H, Rohde M, Oquendo Y, et al. Interaction of preoperative chemoprophylaxis and tranexamic acid use does not affect transfusion in acetabular fracture surgery. Eur J Orthop Surg Traumatol. 2024;34(2):1025–1029. doi:10.1007/s00590-023-03763-z
86. Zhao YK, Zhang C, Zhang YW, et al. Efficacy and safety of orally and intravenously administration of tranexamic acid in patients with elderly femoral neck fracture. Orthop Surg. 2024;16(7):1581–1591. doi:10.1111/os.14089
87. Berg AJ, Naylor T, Johnson DS. PATHS Study Collaborators. Perioperative administration of tranexamic acid in Hip fracture surgery (The PATHS study): national audit of current practice. Ann R Coll Surg Engl. 2023;105(2):142–149. doi:10.1308/rcsann.2021.0273
88. Miralles-Muñoz FA, Martin-Grandes R, Pineda-Salazar M, Bello-Tejeda LL, Pinta-Zazo DELA, Farrer-Muñoz C. Preoperative dose of intravenous tranexamic acid safely reduces blood loss and transfusion in patients undergoing Hip hemiarthroplasty for femoral neck fracture. A randomized controlled trial. Acta Orthop Belg. 2024;90(3):403–408. doi:10.52628/90.3.11635
89. Luo G, Liu J, Ni W, Huang W. The role of post-traumatic antifibrinolysis in the perioperative blood management of elderly patients with intertrochanteric fractures treated with PFNA: a randomised controlled trial. Injury. 2024;55(12):111877. doi:10.1016/j.injury.2024.111877
90. Liu J, Lei Y, Liao J, Liang X, Hu N, Huang W. Pre-emptive antifibrinolysis: its role and efficacy in hip fracture patients undergoing total hip arthroplasty. J Arthroplasty. 2022;37(4):755–762. doi:10.1016/j.arth.2021.12.034
91. Lasocki S, Capdevila X, Vielle B, et al; HiFIT Investigators; SFAR research network. Ferric derisomaltose and tranexamic acid, combined or alone, for reducing blood transfusion in patients with hip fracture (the HiFIT trial): a multicentre,2 × 2 factorial, randomised, double-blind, controlled trial. Lancet Haematol. 2023;10(9):e747–e755. doi:10.1016/S2352-3026(23)00163-1
92. Low WX, Friend H, Dulleston J, Heppenstall S, Spacey K, Liew I. Outcomes of perioperative intravenous iron infusion in femoral fracture surgery: a systematic review and meta-analysis of randomised controlled trials. Surgeon. 2024;22(5):e171–e180. doi:10.1016/j.surge.2024.07.005
93. O’Loughlin E, Chih H, Sivalingam P, et al. IRON NOF trial: IV iron for anaemic patients with femoral fracture. BJA Open. 2023;7:100222. doi:10.1016/j.bjao.2023.100222
94. Chen R, Li L, Xiang Z, Li H, Hou XL. Association of iron supplementation with risk of transfusion, hospital length of stay, and mortality in geriatric patients undergoing Hip fracture surgeries: a meta-analysis. Eur Geriatr Med. 2021;12(1):5–15. doi:10.1007/s41999-020-00366-3
95. Li AB, Zhang WJ, Wang J, Guo WJ, Wang XH, Zhao YM. Intramedullary and extramedullary fixations for the treatment of unstable femoral intertrochanteric fractures: a meta-analysis of prospective randomized controlled trials. Int Orthop. 2017;41(2):403–413. doi:10.1007/s00264-016-3308-y
96. Huang X, Leung F, Xiang Z, et al. Proximal femoral nail versus dynamic Hip screw fixation for trochanteric fractures: a meta-analysis of randomized controlled trials. ScientificWorldJournal. 2013;2013:805805. doi:10.1155/2013/805805
97. Geetala R, Wakefield E, Bradshaw F, Zhang J, Krkovic M. Comparison of intra-operative outcomes following internal fixation with trochanteric stabilisation plate or intramedullary nail in intertrochanteric fractures. Eur J Orthop Surg Traumatol. 2024;34(2):1193–1199. doi:10.1007/s00590-023-03779-5
98. Besnard M, Léger J, Babusiaux D, et al. Comparison of bleeding during trochanteric fracture fixation with mini-invasive or conventional side plate fixation: a randomized controlled trial. Orthop Traumatol Surg Res. 2023;109(7):103661. doi:10.1016/j.otsr.2023.103661
99. Kazemian GH, Manafi AR, Najafi F, Najafi MA. Treatment of intertrochanteric fractures in elderly highrisk patients: dynamic Hip screw vs. external fixation. Injury. 2014;45(3):568–572. doi:10.1016/j.injury.2013.11.020
100. Wang T, Guo J, Hou Z. Risk factors for perioperative hidden blood loss after intertrochanteric fracture surgery in Chinese patients: a meta-analysis. Geriatr Orthop Surg Rehabil. 2022;13:21514593221083816. doi:10.1177/21514593221083816
101. Goel R, Boissonneault A, Grissom H, et al. Impact of intraoperative hypothermia on transfusion requirements in patients with pelvic and acetabular trauma. J Orthop Trauma. 2021;35(12):632–636. doi:10.1097/BOT.0000000000002136
102. Dickenson E, Griffin XL, Achten J, et al. Randomised controlled trial comparing intraoperative cell salvage and autotransfusion with standard care in the treatment of Hip fractures: a protocol for the WHITE 9 study. BMJ Open. 2022;12(6):e062338. doi:10.1136/bmjopen-2022-062338
103. Ziranu A, Meschini C, De Marco D, et al. Prevention of postoperative anemia in Hip hemiarthroplasty for femoral neck fractures: comparison between local haemostatic agents. Orthop Rev. 2022;14(6):38574. doi:10.52965/001c.38574
104. Dawod MS, Alswerki MN, Ar Altamimi A, et al. Comparative analysis of geriatric hip fracture management outcomes in teaching and nonteaching hospitals in Jordan. Sci Rep. 2024;14(1):16053. doi:10.1038/s41598-024-66016-x
105. Brunskill SJ, Millette SL, Shokoohi A, et al. Red blood cell transfusion for people undergoing hip fracture surgery. Cochrane Database Syst Rev. 2015;2015(4):CD009699. doi:10.1002/14651858.CD009699.pub2
106. Nishida T, Kinoshita T, Yamakawa K. Tranexamic acid and trauma-induced coagulopathy. J Intensive Care. 2017;5:5. doi:10.1186/s40560-016-0201-0
107. He YK, Li HZ, Lu HD. Is blood transfusion associated with an increased risk of infection among spine surgery patients?: a meta-analysis. Medicine. 2019;98(28):e16287. doi:10.1097/MD.0000000000016287
108. Braüner Christensen J, Aasbrenn M, Sandoval Castillo L, et al. Predictors of acute kidney injury after hip fracture in older adults. Geriatr Orthop Surg Rehabil. 2020;11:2151459320920088. doi:10.1177/2151459320920088
109. Callum JL, Cohen R, Cressman AM, et al. Cardiac stress biomarkers after red blood cell transfusion in patients at risk for transfusion-associated circulatory overload: a prospective observational study. Transfusion. 2018;58(9):2139–2148. doi:10.1111/trf.14820
110. Smeets SJM, Verbruggen JPAM, Poeze M. Effect of blood transfusion on survival after hip fracture surgery. Eur J Orthop Surg Traumatol. 2018;28(7):1297–1303. doi:10.1007/s00590-018-2205-z
111. Kadar A, Chechik O, Katz E, et al. The effects of ‘old’ red blood cell transfusion on mortality and morbidity in elderly patients with hip fractures--a retrospective study. Injury. 2013;44(6):747–750. doi:10.1016/j.injury.2013.02.011
112. Carson JL, Stanworth SJ, Dennis JA, et al. Transfusion thresholds and other strategies for guiding red blood cell transfusion. Cochrane Database Syst Rev. 2025;10(10):CD002042. doi:10.1002/14651858.CD002042.pub6
113. Carson JL, Sieber F, Cook DR, et al. Liberal versus restrictive blood transfusion strategy: 3-year survival and cause of death results from the FOCUS randomised controlled trial. Lancet. 2015;385(9974):1183–1189. doi:10.1016/S0140-6736(14)62286-8
114. Amin RM, DeMario VM, Best MJ, et al. A restrictive hemoglobin transfusion threshold of less than 7 g/dl decreases blood utilization without compromising outcomes in patients with hip fractures. J Am Acad Orthop Surg. 2019;27(23):887–894. doi:10.5435/JAAOS-D-18-00374
115. Gregersen M, Borris LC, Damsgaard EM. Postoperative blood transfusion strategy in frail, anemic elderly patients with Hip fracture: the TRIFE randomized controlled trial. Acta Orthop. 2015;86(3):363–372. doi:10.3109/17453674.2015.1006980
116. Blandfort S, Gregersen M, Borris LC, Damsgaard EM. Blood transfusion strategy and risk of postoperative delirium in nursing homes residents with Hip fracture. A post hoc analysis based on the TRIFE randomized controlled trial. Aging Clin Exp Res. 2017;29(3):459–466. doi:10.1007/s40520-016-0587-5
117. Foss NB, Kristensen MT, Jensen PS, Palm H, Krasheninnikoff M, Kehlet H. The effects of liberal versus restrictive transfusion thresholds on ambulation after Hip fracture surgery. Transfusion. 2009;49(2):227–234. doi:10.1111/j.1537-2995.2008.01967.x
118. Gu WJ, Gu XP, Wu XD, et al. Restrictive versus liberal strategy for red blood-cell transfusion: a systematic review and meta-analysis in orthopaedic patients. J Bone Joint Surg Am. 2018;100(8):686–695. doi:10.2106/JBJS.17.00375
119. Gillies MA, Ghaffar S, Moppett IK, et al. A restrictive versus liberal transfusion strategy to prevent myocardial injury in patients undergoing surgery for fractured neck of femur: a feasibility randomised trial (RESULT-NOF). Br J Anaesth. 2021;126(1):77–86. doi:10.1016/j.bja.2020.06.048
120. Lau FF, Agerskov M, Thusholdt ANW, et al. Peripheral perfusion index stratifies risk in patients with intraoperative anemia: a multicentre cohort study. J Clin Anesth. 2024;95:111472. doi:10.1016/j.jclinane.2024.111472
121. Gu WJ, Kong YJ, Li YJ, Wang CM. P(v-a)CO2/C(a-v)O2 as a red blood cell transfusion trigger and prognostic indicator for sepsis-related anaemia: protocol for a prospective cohort study. BMJ Open. 2022;12(10):e059454. doi:10.1136/bmjopen-2021-059454
122. Kim JH, Shin HJ, You HS, et al; Korea University Bloodless Medicine Center Scientific Committee. Effect of a patient blood management program on the appropriateness of red blood cell transfusion and clinical outcomes in elderly patients undergoing hip fracture surgery. J Korean Med Sci. 2023;38(8):e64. doi:10.3346/jkms.2023.38.e64
123. Clemmensen SZ, Kragholm KH, Melgaard D, et al. Association between intravenous iron therapy and short-term mortality risk in older patients undergoing Hip fracture surgery: an observational study. J Orthop Surg Res. 2021;16(1):320. doi:10.1186/s13018-021-02462-x
124. Muñoz M, Gómez-Ramírez S, Cuenca J, et al. Very-short-term perioperative intravenous iron administration and postoperative outcome in major orthopedic surgery: a pooled analysis of observational data from 2547 patients. Transfusion. 2014;54(2):289–299. doi:10.1111/trf.12195
125. Van der Linden P, Hardy JF. Implementation of patient blood management remains extremely variable in Europe and Canada: the NATA benchmark project: an observational study. Eur J Anaesthesiol. 2016;33(12):913–921. doi:10.1097/EJA.0000000000000519
126. Tarrant SM, Kim RG, McGregor KL, Palazzi K, Attia J, Balogh ZJ. Dual antiplatelet therapy and surgical timing in geriatric hip fracture. J Orthop Trauma. 2020;34(10):559–565. doi:10.1097/BOT.0000000000001779
127. Farhan-Alanie MM, Chinweze R, Walker R, Eardley WGP, collaborators HASTE. The impact of anticoagulant medications on fragility femur fracture care: the hip and femoral fracture anticoagulation surgical timing evaluation (HASTE) study. Injury. 2024;55(6):111451. doi:10.1016/j.injury.2024.111451
128. Doleman B, Moppett IK. Is early hip fracture surgery safe for patients on clopidogrel? Systematic review, meta-analysis and meta-regression. Injury. 2015;46(6):954–962. doi:10.1016/j.injury.2015.03.024
129. Soo CG, Della Torre PK, Yolland TJ, Shatwell MA. Clopidogrel and Hip fractures, is it safe? A systematic review and meta-analysis. BMC Musculoskelet Disord. 2016;17:136. doi:10.1186/s12891-016-0988-9
130. Collyer TC, Reynolds HC, Truyens E, Kilshaw L, Corcoran T. Perioperative management of clopidogrel therapy: the effects on in-hospital cardiac morbidity in older patients with Hip fractures. Br J Anaesth. 2011;107(6):911–915. doi:10.1093/bja/aer288
131. Pailleret C, Ait Hamou Z, Rosencher N, et al. A retrospective comparison between delayed and early Hip fracture surgery in patients taking clopidogrel: same total bleeding but different timing of blood transfusion. Int Orthop. 2017;41(9):1839–1844. doi:10.1007/s00264-017-3571-6
132. Kim CH, Chang JS, Lim Y, Lim D, Kim JW. Safety of urgent surgery for the patients with proximal femur fracture treated with platelet aggregation inhibitors: a propensity-score matching analysis. Eur J Trauma Emerg Surg. 2024;50(2):347–358. doi:10.1007/s00068-023-02368-9
133. Ohmori T, Toda K, Kanazawa T, Tada K, Yagata Y, Ito Y. Retrospective high volume comparative study suggests that patients on aspirin could have immediate surgery for Hip fractures without significant blood loss. Int Orthop. 2021;45(3):543–549. doi:10.1007/s00264-021-04941-6
134. You D, Xu Y, Krzyzaniak H, Korley R, Carrier M, Schneider P. Safety of expedited-surgery protocols in anticoagulant-treated patients with Hip fracture: a systematic review and meta-analysis. Can J Surg. 2023;66(2):E170–E180. doi:10.1503/cjs.010021
135. Wang J, Giammanco PA, Nilssen P, et al. Expedited hip fracture surgery in patients on direct oral anticoagulants does not increase perioperative blood loss. J Orthop Trauma. 2025;39(6):314–319. doi:10.1097/BOT.0000000000002974
136. Schermann H, Gurel R, Gold A, et al. Safety of urgent Hip fracture surgery protocol under influence of direct oral anticoagulation medications. Injury. 2019;50(2):398–402. doi:10.1016/j.injury.2018.10.033
137. Levack AE, Moore HG, Stephan S, et al. Delayed surgery does not reduce transfusion rates in low-energy hip fractures on direct oral anticoagulants. J Orthop Trauma. 2022;36(4):172–178. doi:10.1097/BOT.0000000000002251
138. Brameier DT, Tischler EH, Ottesen TD, et al. Use of direct oral anticoagulants among patients with hip fracture is not an indication to delay surgical intervention. J Orthop Trauma. 2024;38(3):148–154. doi:10.1097/BOT.0000000000002753
139. Weihs V, Humenberger M, Sturz G, et al. Early surgical fixation of proximal femur fractures under active direct oral anticoagulation (DOAC) therapy does not increase the postoperative blood loss. Results from a prospective cohort study with a matched-pair analysis. Arch Orthop Trauma Surg. 2025;145(1):243. doi:10.1007/s00402-025-05870-4
140. Kolodychuk NL, Godshaw B, Nammour M, Starring H, Mautner J. Early Hip fracture surgery is safe for patients on direct oral anticoagulants. OTA Int. 2023;6(2):e252. doi:10.1097/OI9.0000000000000252
141. Yoo MS, Zhu S, Jiang SF, et al. Association of reversal of anticoagulation preoperatively on 30-day mortality and outcomes for hip fracture surgery. Am J Med. 2020;133(8):969–975.e2. doi:10.1016/j.amjmed.2020.01.002
142. Baldino JB, Bellas NJ, Solomito MJ, Kumar M, Davis SL. Direct oral anticoagulants (DOACs) increase time to operating room without increasing postoperative hematologic complications in patients with fragility fractures of the proximal femur. Injury. 2025;56(3):112217. doi:10.1016/j.injury.2025.112217
143. Salar O, Holley J, Baker B, Ollivere BJ, Moran CG. Omitting pre-operative coagulation screening tests in Hip fracture patients: stopping the financial cascade? Injury. 2014;45(12):1938–1941. doi:10.1016/j.injury.2014.08.032
144. Rostagno C, Cartei A, Polidori G, et al. Management of ongoing direct anticoagulant treatment in patients with Hip fracture. Sci Rep. 2021;11(1):9467. doi:10.1038/s41598-021-89077-8
145. Creeper K, Stafford A, Reynolds S, et al. Outcomes and anticoagulation use for elderly patients that present with an acute Hip fracture: multi-centre, retrospective analysis. Intern Med J. 2022;52(3):418–425. doi:10.1111/imj.15007
146. Leer-Salvesen S, Dybvik E, Ranhoff AH, et al. Do direct oral anticoagulants (DOACs) cause delayed surgery, longer length of hospital stay, and poorer outcome for Hip fracture patients? Eur Geriatr Med. 2020;11(4):563–569. doi:10.1007/s41999-020-00319-w
147. Bernate JD, López AM, Rojas Liévano J, et al. Preoperative anticoagulation and its impact on surgical timing and postoperative outcomes in Hip fracture surgery: a retrospective study at an Orthogeriatrics Clinical Care Center in Colombia. Eur J Orthop Surg Traumatol. 2025;35(1):170. doi:10.1007/s00590-025-04286-5
148. Herbosa C, Petit C, Konda S, et al. Is regional only anesthesia a safe choice in anticoagulated Hip fracture patients? Eur J Orthop Surg Traumatol. 2025;35(1):435. doi:10.1007/s00590-025-04519-7
149. Daugaard C, Pedersen AB, Kristensen NR, Johnsen SP. Preoperative antithrombotic therapy and risk of blood transfusion and mortality following Hip fracture surgery: a Danish nationwide cohort study. Osteoporos Int. 2019;30(3):583–591. doi:10.1007/s00198-018-4786-0
150. Lu C, Wei X, Li L, et al. Robot-assisted PFNA surgery improves clinical outcomes in the treatment of unstable femoral intertrochanteric fractures in elderly patients compared with traditional PFNA surgery. Sci Rep. 2025;15(1):3836. doi:10.1038/s41598-025-88229-4
151. Wu A, Fahey MT, Cui D, El-Behesy B, Story DA. An evaluation of the outcome metric ‘days alive and at home’ in older patients after Hip fracture surgery. Anaesthesia. 2022;77(8):901–909. doi:10.1111/anae.15742
152. Mihcin S, Sahin AM, Yilmaz M, et al. Database covering the prayer movements which were not available previously. Sci Data. 2023;10(1):276. doi:10.1038/s41597-023-02196-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.