Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 11
Perioperative Administration of Emend® (Aprepitant) at a Tertiary Care Children’s Hospital: A 12-Month Survey
Authors Kanaparthi A, Kukura S, Slenkovich N, AlGhamdi F, Shafy SZ, Hakim M ![]() , Tobias JD
, Tobias JD ![]()
Received 3 July 2019
Accepted for publication 18 November 2019
Published 27 November 2019 Volume 2019:11 Pages 155—160
DOI https://doi.org/10.2147/CPAA.S221736
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Arthur E. Frankel
Anuradha Kanaparthi,1 Sarah Kukura,2 Natalie Slenkovich,2 Faris AlGhamdi,2 Shabana Z Shafy,2 Mohammed Hakim,2 Joseph D Tobias2,3
1College of Medicine, Northeast Ohio Medical University (NEOMED), Rootstown, Ohio, USA; 2Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, Columbus, Ohio, USA; 3Department of Anesthesiology & Pain Medicine, The Ohio State University College of Medicine, Columbus, Ohio, USA
Correspondence: Anuradha Kanaparthi
Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, 700 Children’s Drive, Columbus, Ohio 43205 Tel +1614 722-4200
Fax +1614 722-4203
Email [email protected]
Introduction: Aprepitant (Emend®) is a novel antiemetic agent that works through antagonism of neurokinin-1 (NK-1) receptors. To date, there are limited data regarding its use to prevent postoperative nausea and vomiting (PONV) in children. We retrospectively reviewed our initial 12-months experience with aprepitant after it was made available for perioperative use.
Methods: The anesthetic records of patients who received aprepitant were retrospectively reviewed and demographic, surgical, and medication data retrieved.
Results: The study cohort included 31 patients (15 male and 16 female) ranging in age from 4 to 27 years (15.7 ± 7.4 years) and in weight from 14.4 to 175.7 kilograms (59.3 ± 30.2 kgs). Most of the patients (30 of 31) received the capsule form and 1 received the liquid. The average dose of aprepitant administered was 0.9 ± 0.6 mg/kg; however, only one patient received dosing expressed as mg/kg, and the majority received a 40 mg capsule. All of the patients in the cohort had either a previous history of PONV or risk factors for PONV. PONV occurred in the PACU in 1 patient and during the first 24 postoperative hours in 3 additional patients. No adverse effects related to aprepitant use were noted.
Conclusion: Aprepitant was easily added to the preoperative regimen for pediatric patients who may require it. Our approach limited overuse and subsequent cost concerns. Future studies with a comparator group and a greater sample size are needed to demonstrate its efficacy, especially in comparison to time-honored agents such as ondansetron. No adverse effects were noted in our limited study cohort.
Keywords: aprepitant, postoperative nausea and vomiting, pediatric
Introduction
The incidence of postoperative nausea and vomiting (PONV) in children has been estimated at 30% without the administration of prophylactic medications and up to 80% in high-risk patients, such as those with a previous history of PONV or other risk factors, including female gender, non-smoker status, surgical procedure, and anesthetic regimen.1,2 In addition to patient distress and discomfort, PONV may result in slower recovery, prolonged postoperative stays, postponed hospital discharges, and hospital readmissions.3,4
Perioperative management strategies include either prophylactic treatment or rescue therapy once PONV has occurred. Prophylactic treatment commonly used includes a two-medication regimen consisting of the corticosteroid, dexamethasone, and a 5-hydroxytryptamine-3 (5HT3) receptor antagonist, such as ondansetron.1–4 Despite the general efficacy of this combination, specific clinical scenarios may contraindicate the use of these agents. A recent study advises providers to use clinical judgment before using corticosteroids in patients with diabetes mellitus and while dexamethasone administration has anecdotally been associated with acute adrenal insufficiency.5,6 Ondansetron and other 5-HT3 antagonists may prolong QT intervals, especially in certain at-risk populations.7,8
Given the potential for failure with other agents, adverse effect profiles of commonly used agents, and potential contraindications, there remains a place for novel agents in the treatment and prevention of PONV. We describe our initial experience with the prophylactic use of aprepitant, a novel antiemetic agent that works through antagonism of neurokinin-1 (NK-1) receptors.9
Methods
This study was approved by the Institutional Review Board of Nationwide Children’s Hospital. As a retrospective chart review, the need for informed consent was waived. All data collected during this study were stored in a secure location, and only the collaborators directly involved with this research project had access to this information. All electronic files were stored on a secure, password-protected network. Nationwide Children’s Hospital is a 500-bed tertiary care children’s hospital that provides anesthetic care for more than 38,000 patients per year. Aprepitant was made available in the preoperative area of the main operating room starting February 2018. Aprepitant was stocked in the Pyxis machine in our preoperative area, and an order set was added to the electronic medical record.
The hospital pharmacy database was queried, and patients who received aprepitant for the initial 12 months after its introduction for perioperative use were identified. The anesthetic records of patients who received aprepitant were retrospectively reviewed, and the perioperative administration of the medication was confirmed. The following demographic and surgical data were retrieved: age, weight, gender, and history of PONV with previous anesthetic, associated conditions known to increase the risk of PONV, contraindications to the use of routine agents (dexamethasone or ondansetron), type of surgery, planned inpatient or outpatient procedure, and length of stay. The formulation of aprepitant (capsule or liquid) was noted. If the capsule was used, it was determined whether the capsule was opened and administered as a liquid. Intraoperative data included the use of other antiemetic agents, such as ondansetron or dexamethasone, as well as the type of anesthesia used (volatile-based or propofol-based) and any adverse events. The postoperative records were reviewed to determine if PONV or abdominal pain occurred or if other anti-emetic agents were administered during the postoperative period.
Results
The demographics of the study cohort of 31 pediatric patients are listed in Table 1. The types of surgical case are listed in Table 2. In all cases, aprepitant was administered preoperatively 46–60 mins prior to the induction of anesthesia and the start of the surgical procedure. The medication was administered orally to all patients. The majority of patients (30 of 31) received the capsule form of aprepitant while 1 of 31 received the liquid form. When the capsule was used, in all except one case, it was opened, and its contents were placed in a small volume of liquid to ease preoperative administration. The average dose of aprepitant was 0.9 ± 0.6 mg/kg; however, only one patient received dosing expressed as mg/kg. This patient received 1 mg/kg while all others received a specific-sized capsule. Twenty-eight patients received 40 mg, one received 80 mg, and one received 125 mg.
 |
Table 1 Demographics of the Study Cohort |
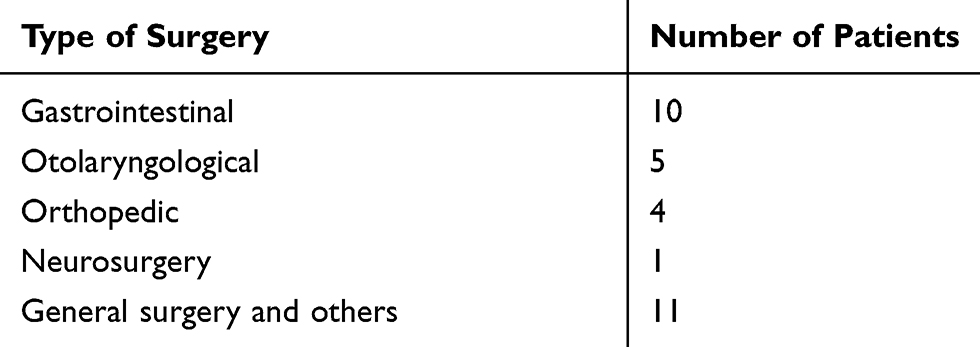 |
Table 2 Type of Surgical Procedure |
All of the patients in the cohort had either a previous history of PONV (13 patients) or other risk factors for PONV (18 patients). Other risk factors identified included the type of surgery, a strong family history of PONV, female gender, or a history of motion sickness. All of the patients had a volatile-based anesthetic after either intravenous induction with propofol or inhalation induction with sevoflurane. Nitrous oxide was not used for maintenance anesthesia in any of the cases. Intraoperative opioids were administered to 25 of 31 patients, and intraoperative dexmedetomidine was administered to 18 patients. Intraoperatively, 21 patients received both ondansetron and dexamethasone, 6 received only ondansetron, and 4 received only dexamethasone. PONV occurred in the post-anesthesia care unit (PACU) in 1 patient and during the first 24 postoperative hours in 3 additional patients for an incidence of 12.9%. There were no unplanned admissions related to PONV. There were no adverse effects related to aprepitant use.
Discussion
Oral aprepitant (Emend®) and the intravenous, water-soluble prodrug, fosaprepitant, are novel antiemetic agents that antagonize the NK-1 G-protein coupled receptor, thereby alleviating vomiting in both adults and children. After binding its ligand, substance P, the NK-1 receptor signals the vomiting center, comprised of sensory and motor vagal nuclei, and the area postrema located in the medulla oblongata.10 By antagonizing NK-1 receptor and its effects mediated by the vagus nerve, aprepitant effectively prevents substance P binding and subsequent NK-1 and peripheral pain pathway signal transductions.
The primary intent of the current study was to investigate the general use and dosing practices following the introduction of aprepitant to the perioperative setting at a tertiary care children’s hospital. We specifically wanted to ensure, due to cost constraints, that we were not overusing this novel medication. Prior to its addition to our PONV armamentarium, we provided educational background to anesthesia providers (pediatric anesthesiology attendings, CRNAs, and pediatric anesthesiology fellows) for this initiative via e-mail and at our monthly departmental outcomes conferences. Potential indications for aprepitant were discussed, dosing reviewed, and cost information provided (Table 3).
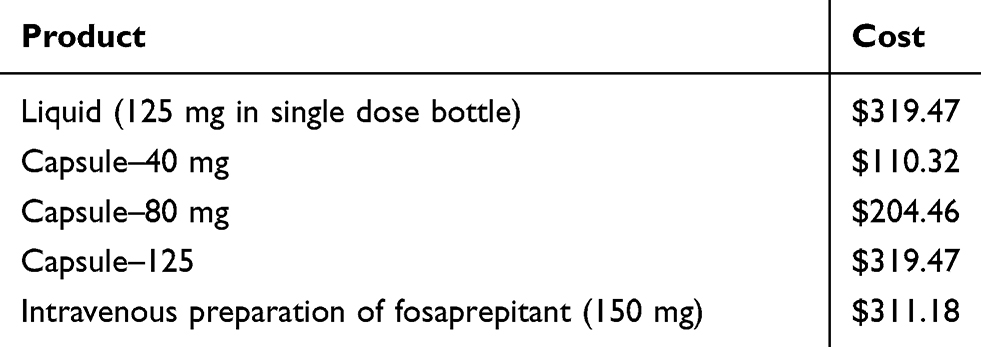 |
Table 3 Cost Information for Aprepitant |
In this initial 12-month period, during which there were more than 14,000 surgical cases in the main operating room of our hospital, aprepitant was administered to only 31 patients. Practitioners who used aprepitant preoperatively also administered other antiemetic agents intraoperatively, with the entire cohort receiving at least one other agent and 21 of 31 patients receiving both ondansetron and dexamethasone. The patients who received aprepitant were generally older than our general surgical population with an average age of 15.7 years. All of the patients had a history of PONV or other identified risk factors for PONV. Given that the study cohort was close to adult weight parameters, dosing was not generally based on an mg/kg parameter. Although the dose was approximately 1 mg/kg when considering the entire cohort, 28 of the 31 patients received the 40 mg capsule. To limit costs, in 30 of the 31 patients, the capsule was opened and administered in a small volume of water. In the routine practice of pediatric anesthesiology, premedication (oral midazolam) or other medications (anticonvulsants) may be preoperatively administered. This practice is in accordance with nil per os guidelines for the operating room. No concerns over the administration of an oral medication prior to surgical procedure were expressed by the anesthesia providers.
Our study was neither powered nor designed to determine efficacy or compare aprepitant to other agents. PONV was noted in only 4 patients during the first 24 postoperative hours (one in the PACU and three after PACU discharge). The lack of a comparator group and limited sample size did not allow for rigorous analysis, determination of variables associated with PONV, or establishment of efficacy. However, given that aprepitant was administered only to high risk patients, we would postulate that the incidence of PONV would be high in this cohort, perhaps up to 50–80%, without the administration of anti-emetic agents. No discernable associations were noted between the demographic and clinical characteristics of the four patients who experienced PONV either in-PACU or post-PACU. Although there were no unplanned admissions, the incidence of this is generally low.
To date, the majority of clinical experience with aprepitant in both children and adults is in the prevention of chemotherapy-induced nausea and vomiting (CINV), generally when added to the standard anti-emetic regimen.11–14 Felix-Ukwu et al reported a significant reduction in both methotrexate-induced nausea and vomiting and as-needed antiemetic usage in children and adolescents with acute lymphoblastic leukemia when an aprepitant infusion was added to the standard antiemetic regimen of 5-HT3-antagonist and dexamethasone.14 Kang et al reported that oral aprepitant administered with ondansetron resulted in a higher reduction of CINV when compared to placebo and ondansetron in pediatric patients.12 Fifty-one percent of the patients treated with aprepitant and ondansetron did not experience vomiting or retching and did not require rescue medications compared to only 26% in the control group. Aprepitant has also been shown to decrease the incidence of PONV in adults, with an efficacy equal to or greater than commonly used agents such as ondansetron.15–18
Outside of the prevention of CINV, there are limited data regarding the use of aprepitant in the pediatric population. Salman et al evaluated the pharmacokinetics, pharmacodynamics, safety, and tolerability of aprepitant in pediatric patients up to 17 years of age during the perioperative period.19 The study included a control group who received intravenous ondansetron and three study groups who received a single oral dose of aprepitant adjusted to be equivalent to adult doses of 10, 40, or 125 mg. The complete response and no vomiting rates were high (>80%) across treatment groups and similar to patients receiving intravenous ondansetron. Additional experience with aprepitant in children was presented by Cristofori et al who retrospectively reported the potential efficacy of aprepitant in a cohort of 41 children with cyclic vomiting syndrome.20
To date, the adverse effect profile of aprepitant has been limited. Aprepitant and fosaprepitant as moderate and weak inhibitors of CYP3A4, respectively, may demonstrate a clinically significant interaction with some medications that are CYP3A4 or CYP2C9 substrates.21 The other issue regarding aprepitant is its potential to decrease the efficacy of oral contraceptive agents.22,23 Patients should use a non‐hormonal form of birth control during treatment with aprepitant and for 28 days after the last dose. To ensure that appropriate patient information and education is provided, our electronic medical record provides a prompt so that an information sheet is given to every patient who received aprepitant (Figure 1).
 |
Figure 1 Prompt from the electronic medical record which is provided to the patient as information regarding the potential interaction of aprepitant with hormonal contraceptive agents. |
Certain limitations of the current study must be recognized. First, as noted previously, the study did not intend to and was not powered to prove the efficacy of aprepitant. There was no control or comparator group against which to clearly compare those patients who received aprepitant. Postulated efficacy would have to be based on an estimate of the expected incidence of PONV in high-risk patients. However, we saw limited incidence of PONV (12.9%) in our high-risk patients, even when a volatile-based anesthetic regimen was used. A second limitation was that as a retrospective study, we were not able to clearly define outcomes such as nausea and abdominal pain which may not have been recorded in the EMR. As the study included all patients presenting to our main operating room, as with most pediatric studies, there was a significant variation in the age and weight ranges. Based on our initial literature review and preliminary experience, a dose of 40 mg was used in the majority of patients. Additional clinical work is needed to further define the appropriate dosing regimen as studies on nausea and vomiting in other clinical scenarios have used larger doses. Finally, all of the patients received at least one additional anti-emetic agent intraoperatively while the majority (21 of 31) patients0 received two (ondansetron and dexamethasone) in addition to aprepitant.
In summary, aprepitant can be easily added to the preoperative regimen and perioperative management of patients with a predisposition to PONV. As noted by our study, the preoperative process can be modified to include use of this novel anti-emetic agent. Pediatric dosing regimens have generally been extrapolated from adult regimens for PONV with the administration of 1 mg/kg up to 40 mg. Future studies are needed to more clearly define appropriate dosing regimens to prevent PONV. We found the 40 mg capsule can be easily opened and the contents placed in a small volume of liquid to allow for preoperative oral administration in pediatric patients who may not be able to swallow a capsule. Future studies are needed to demonstrate its efficacy when used alone versus in addition to other commonly used anti-emetic agents.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tateosian VS, Champagne K, Gan TJ. What is new in the battle against postoperative nausea and vomiting? Best Pract Res Clin Anaesthesiol. 2018;32:137–148. doi:10.1016/j.bpa.2018.06.005
2. Cao X, White PF, Ma H. An update on the management of postoperative nausea and vomiting. J Anesth. 2017;31:617–626. doi:10.1007/s00540-017-2363-x
3. Hohne C. Postoperative nausea and vomiting in pediatric anesthesia. Curr Opin Anaesthesiol. 2014;27:303–308. doi:10.1097/ACO.0000000000000073
4. Öbrink E, Jildenstål P, Oddby E, Jakobsson JG. Post-operative nausea and vomiting: update on predicting the probability and ways to minimize its occurrence, with focus on ambulatory surgery. Int J Surg. 2015;15:100–106. doi:10.1016/j.ijsu.2015.01.024
5. Purushothaman AM, Pujari VS, et al. A prospective randomized study on the impact of low-dose dexamethasone on perioperative blood glucose concentrations in diabetics and nondiabetics. Saudi J Anaesth. 2018;12:198–203. doi:10.4103/sja.SJA_409_17
6. Landa AB, Viswanath O, D’Mello J. Acute adrenal insufficiency after an antiemetic dose of dexamethasone: a case report. AA Pract. 2019;12:424–425.
7. Charbit B, Albaladejo P, Funck-Brentano C, Legrand M, Samain E, Marty J. Prolongation of QTc interval after postoperative nausea and vomiting treatment by droperidol or ondansetron. Anesthesiology. 2005;102:1094–1100. doi:10.1097/00000542-200506000-00006
8. Freedman SB, Uleryk E, Rumantir M, Finkelstein Y. Ondansetron and the risk of cardiac arrhythmias: a systematic review and postmarketing analysis. Ann Emerg Med. 2014;64:19–25. doi:10.1016/j.annemergmed.2013.10.026
9. Aapro M, Carides A, Rapoport BL, Schmoll H-J, Zhang L, Warr D. Aprepitant and fosaprepitant: a 10-year review of efficacy and safety. Oncologist. 2015;20:450–458. doi:10.1634/theoncologist.2014-0229
10. Okafor D, Kaye AD, Kaye RJ, Urman RD. The role of neurokinin-1 (substance P) antagonists in the prevention of postoperative nausea and vomiting. J Anaesthesiol Clin Pharmacol. 2017;33:441–445. doi:10.4103/0970-9185.222511
11. Abdel-Malek R, Abbas N, Shohdy KS, et al. Addition of 3-day aprepitant to ondansetron and dexamethasone for prophylaxis of chemotherapy-induced nausea and vomiting among patients with diffuse large B cell lymphoma receiving 5-day cisplatin-based chemotherapy. J Egypt Natl Canc Inst. 2017;29:155–158. doi:10.1016/j.jnci.2017.05.001
12. Kang HJ, Loftus S, Taylor A, DiCristina C, Green S, Zwaan CM. Aprepitant for the prevention of chemotherapy-induced nausea and vomiting in children: a randomised, double-blind, phase 3 trial. Lancet Oncol. 2015;16:385–394. doi:10.1016/S1470-2045(15)70061-6
13. Inoue T, Kimura M, Uchida J, et al. Aprepitant for the treatment of breakthrough chemotherapy-induced nausea and vomiting in patients receiving moderately emetogenic chemotherapy. Int J Clin Oncol. 2017;22:600–604. doi:10.1007/s10147-016-1081-y
14. Felix-Ukwu F, Reichert K, Bernhardt MB, Schafer ES, Berger A. Evaluation of aprepitant for acute chemotherapy-induced nausea and vomiting in children and adolescents with acute lymphoblastic leukemia receiving high-dose methotrexate. Pediatr Blood Cancer. 2018;65:e26857. doi:10.1002/pbc.v65.2
15. Singh PM, Borle A, Rewari V, et al. Aprepitant for postoperative nausea and vomiting: a systematic review and meta-analysis. Postgrad Med J. 2016;92:87–98. doi:10.1136/postgradmedj-2015-133515
16. Therneau IW, Martin EE, Sprung J, Kellogg TA, Schroeder DR, Weingarten TN. The role of aprepitant in prevention of postoperative nausea and vomiting after bariatric surgery. Obes Surg. 2018;28:37–43. doi:10.1007/s11695-017-2797-0
17. Moon HY, Baek CW, Choi GJ, et al. Palonosetron and aprepitant for the prevention of postoperative nausea and vomiting in patients indicated for laparoscopic gynaecologic surgery: a double-blind randomised trial. BMC Anesthesiol. 2014;14:68. doi:10.1186/1471-2253-14-68
18. Diemunsch P, Gan TJ, Philip BK, et al. Single-dose aprepitant vs ondansetron for the prevention of postoperative nausea and vomiting: a randomized, double-blind phase III trial in patients undergoing open abdominal surgery. Br J Anaesth. 2007;99:202–211. doi:10.1093/bja/aem133
19. Salman FT, DiCristina C, Chain A, Afzal AS. Pharmacokinetics and pharmacodynamics of aprepitant for the prevention of postoperative nausea and vomiting in pediatric subjects. J Pediatr Surg. 2019;54:1384–1390. doi:10.1016/j.jpedsurg.2018.09.006
20. Cristofori F, Thapar N, Saliakellis E, et al. Efficacy of the neurokinin-1 receptor antagonist aprepitant in children with cyclical vomiting syndrome. Aliment Pharmacol Ther. 2014;40:309–317. doi:10.1111/apt.2014.40.issue-3
21. Patel P, Leeder JS, Piquette-Miller M, Dupuis LL. Aprepitant and fosaprepitant drug interactions: a systematic review. Br J Clin Pharmacol. 2017;83:2148–2162. doi:10.1111/bcp.v83.10
22. Bailard N, Rebello E. Aprepitant and fosaprepitant decrease the effectiveness of hormonal contraceptives. J Clin Pharmacol. 2018;84:602–603. doi:10.1111/bcp.v84.3
23. Aapro MS, Walko CM. Aprepitant: drug‐drug interactions in perspective. Ann Oncol. 2010;21:2316–2323. doi:10.1093/annonc/mdq149
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.