Back to Journals » OncoTargets and Therapy » Volume 8
Perineural invasion correlates with postoperative distant metastasis and poor overall survival in patients with PT1–3N0M0 esophageal squamous cell carcinoma
Received 22 June 2015
Accepted for publication 11 September 2015
Published 27 October 2015 Volume 2015:8 Pages 3153—3157
DOI https://doi.org/10.2147/OTT.S90909
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Daniele Santini
Liming Sheng, Yongling Ji, Xianghui Du
Department of Radiotherapy, Zhejiang Cancer Hospital and Key Laboratory Diagnosis and Treatment Technology on Thoracic Oncology, Hangzhou, Zhejiang, People’s Republic of China
Abstract: The aim of this study was to determine the prognostic value of perineural invasion (PNI) in patients with PT1–3N0M0 esophageal squamous cell carcinoma (ESCC) who underwent curative resection. A total of 148 patients with PT1–3N0M0 ESCC, who underwent surgery in Zhejiang Cancer Hospital (Hangzhou, People’s Republic of China), between 2006 and 2009, were evaluated in this retrospective study. The effects of PNI on distant metastasis-free survival (DMFS) and overall survival (OS) were assessed using Kaplan–Meier analysis. Independent prognostic factors were identified by multivariate Cox analysis. Positive PNI was identified in 25.0% of all the cases. The depth of invasion (PT stage) was closely associated with the PNI positivity (P<0.001). The 5-year DMFS rate and OS rate of the PNI-positive patients were significantly worse than those of the PNI-negative patients (DMFS: 37.2% vs 62.3%, P=0.009; OS: 31.3% vs 74.3%, P<0.001). Multivariate analysis indicated that the positivity of PNI was an independent prognostic factor for both DMFS (hazard ratio [HR] =2.35, P=0.039) and OS (HR =3.56, P=0.002). Our results suggest that PNI was a predictor of distant metastasis and independently associated with prognosis of patients with PT1–3N0M0 ESCC.
Keywords: esophageal squamous cell carcinoma, perineural invasion, metastasis, prognosis
Introduction
Esophageal cancer is one of the most common malignancies worldwide. It is the leading cancer-related cause of deaths in the People’s Republic of China. Esophageal squamous cell carcinoma (ESCC) accounts for 80% of all esophageal cancer in eastern Asia. The incidence of esophageal cancer continued to rise in past decades, likely as a result of increased public awareness and implementation of screening programs. Early-stage (PT1–3N0M0) ESCC forms a subset of relatively favorable prognosis, with a low incidence of distant organ metastasis, local recurrence, and death.1 Adjuvant chemoradiotherapy is not routinely recommended in this population. The mainstay of treatment of PT1–3N0M0 ESCC is curative resection. However, only approximately 50%–60% of these tumors can be cured by surgery alone.2 Recently, the role of adjuvant chemoradiotherapy for PT1–3N0M0 ESCC has been justified in some high-risk patients, with decisions directed by the presence of adverse or clinicopathological features, such as close or involved surgical margin, tumor length, lymphovascular involvement, and extracapsular spread.3–5 Besides the economic constraints that health-care systems are increasingly facing, oncologists also need to carefully weigh the benefits and risks of future treatment. Adjuvant chemoradiotherapy is associated with significant side effects and morbidity.6 In view of this, the risk of recurrence and the potential benefit of adjuvant chemoradiotherapy have to be evaluated to select the proper patients with PT1–3N0M0 ESCC.
Perineural invasion (PNI) is a pathological process characterized by cancer cells surrounding nerve fibers and entering the perineurium or neural fascicles. It is an underrecognized route of metastatic spread, which can occur in the absence of lymphatic or vascular involvement. Metastasis, the ability of cancer cells to spread from a primary site to form a new tumor at distant sites, is the main reason for death caused by cancer. Therefore, it is reported that PNI was a rucial route for the local spread and distant metastasis of cancer, associated with poor prognosis, especially in prostate cancer7,8 and pancreatic carcinoma.9,10
Methods
Patients
A total of 148 consecutive patients who underwent curative surgery for PT1–3N0M0 ESCC were diagnosed and treated in Zhejiang Cancer Hospital, Hangzhou, People’s Republic of China, between October 2006 and December 2009. The selective criteria included the following: newly confirmed to have ESCC and had not received treatment previously; a negative incised margin; no distant metastasis; postoperative survival expectancy was longer than 3 months. Clinicopathological information such as age, sex, resection type, tumor location, histopathology, tumor stage, tumor length, lymphatic vessel invasion, resection margins, recurrence, and survival was obtained from patient charts.
Pathological evaluation
A thorough histopathological examination of the surgical excision specimen stained with hematoxylin and eosin (H&E) was performed to document all foci of PNI on each 5 μm thick slide if present. PNI was defined as cancer cells surrounding at least one-third of the nerve without invading through the nerve sheath, as well as tumor cells within any of the three layers of the nerve sheath. Histopathological slides were independently reviewed by two pathologists who were blinded to other information of the patients.
Follow-up
All patients received standardized follow-up at 3-month intervals for the first 2 years after operation, at 6-month intervals in the third year, and yearly thereafter. Evaluation comprised a physical examination, upper gastrointestinal endoscopy, complete blood count, chest and abdomen computed tomography. Distant metastasis-free survival (DMFS) covering the date of definitive surgery to the date of distant metastasis was diagnosed. Overall survival (OS) was calculated as the time from the date of surgery to death or censoring.
Statistical analysis
All statistical calculations were performed using SPSS 13.0 for Windows (SPSS Inc., Chicago, IL, USA). The relationship between PNI positivity and the other clinicopathological factors was analyzed by the chi-square test. DMFS and OS were analyzed by Kaplan–Meier analysis with log-rank test. Multivariate Cox proportional hazards regression model with forward stepwise approach was constructed to identify independent prognostic factors. A 95% confidence interval (95% CI) was used to quantify the relationship between survival time and each independent factor. All P-values were two-sided in the tests. The values of P<0.05 were considered statistically significant.
Results
A total of 148 patients who had undergone curative resection for PT1–3N0 ESCC were retrospectively analyzed; eleven patients were women and 137 were men. The baseline characteristics of these ESCC patients are summarized in Table 1. The median age was 58 years, (range: 38–75 years). In terms of the new American Joint Committee on Cancer tumor node metastasis staging system, there were 35 (23.6%) T1, 36 (24.3%) T2, and 77 (52.1%) T3. PNI was detected as positive in 37 of the 148 patients (25.0%). The relationship between PNI and clinicopathological factors is shown in Table 1. There was no significant association between the presence of PNI and patients’ sex, age, smoking status, alcohol status, tumor cell differentiation, and tumor length (P>0.05). The depth of invasion (PT stage) was closely associated with the PNI positivity (P<0.001).
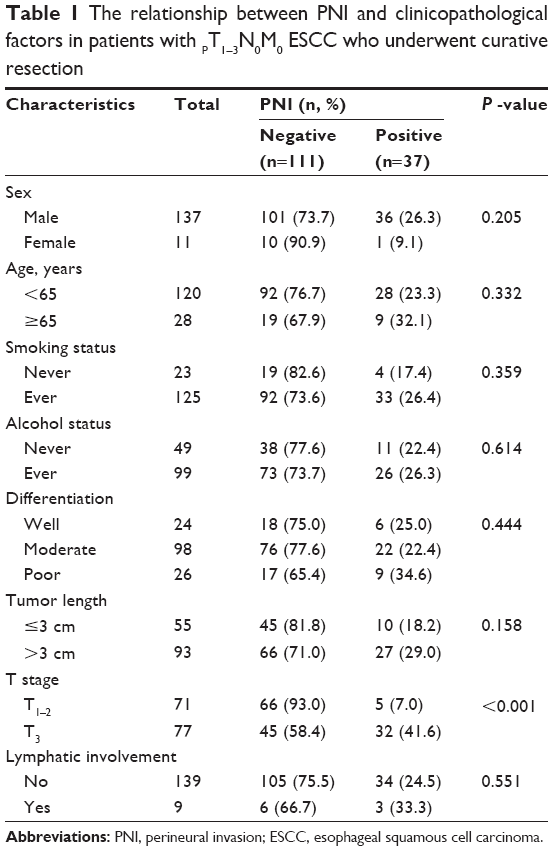 | Table 1 The relationship between PNI and clinicopathological factors in patients with PT1–3N0M0 ESCC who underwent curative resection |
At the median follow-up of 30 months (range: 4–96 months), the 5-year DMFS rate and OS rate were 56.8% and 66.4%, respectively. For patients who had PNI negativity, the 5-year DMFS rate and OS rate were 62.3% and 74.3%, respectively. For the PNI-positive patients, the 5-year DMFS rate and OS rate were 37.2% and 31.3%, respectively. Then, the prognostic significance of PNI and other clinicopathological variables was examined using univariate regression models (shown in Table 2). The presence of PNI was significantly associated with DMFS in the univariate analysis (P=0.009, Figure 1). The likelihood of developing distant metastasis was 2.34-fold greater in patients with PNI-positive tumors than in those with PNI-negative tumors. Similar results were also observed for the 5-year OS (81.2% vs 52.5%, P<0.001, Figure 2). Furthermore, we performed multivariate analysis with Cox regression method in order to evaluate the prognostic significance of PNI and the other clinicopathological factors. Table 3 shows the results of multivariate analysis in all patients. Multivariate analysis indicated that the positivity of PNI was an independent prognostic factor. Patients with PNI had an elevated risk of distant metastasis and death compared to those without PNI. The hazard ratio was 2.35 (95% CI: 1.04–5.29) for metastasis and 3.56 (95% CI: 1.62–7.84) for death. These analyses were adjusted for patients’ age, sex, smoking status, and PT stage.
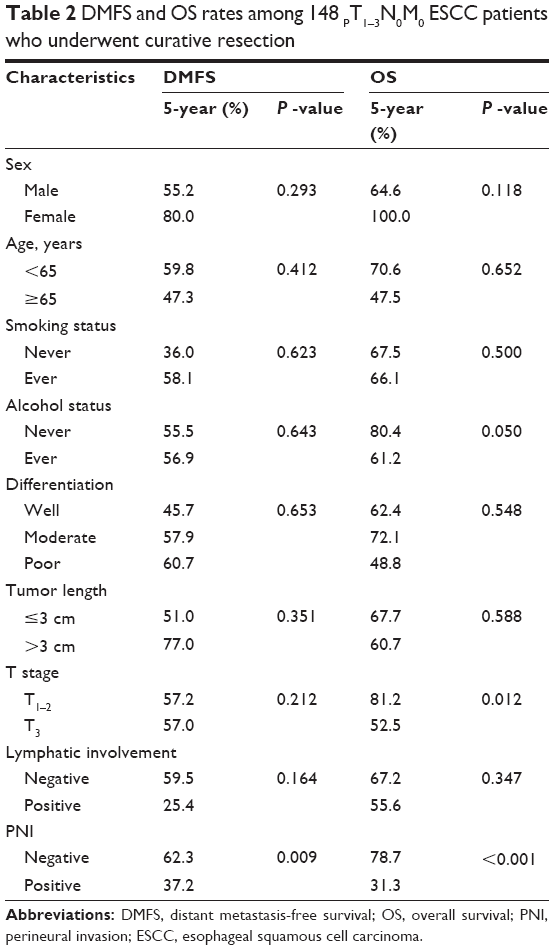 | Table 2 DMFS and OS rates among 148 PT1–3N0M0 ESCC patients who underwent curative resection |
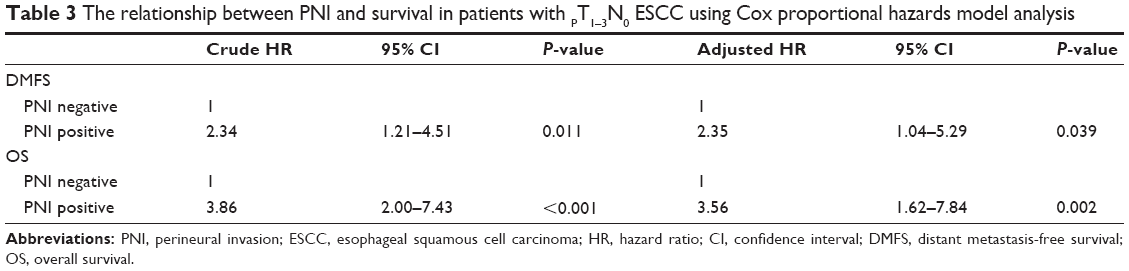 | Table 3 The relationship between PNI and survival in patients with PT1–3N0 ESCC using Cox proportional hazards model analysis |
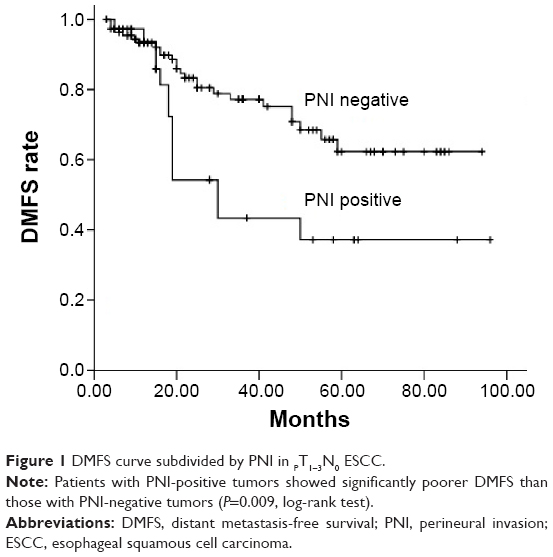 | Figure 1 DMFS curve subdivided by PNI in PT1–3N0 ESCC. |
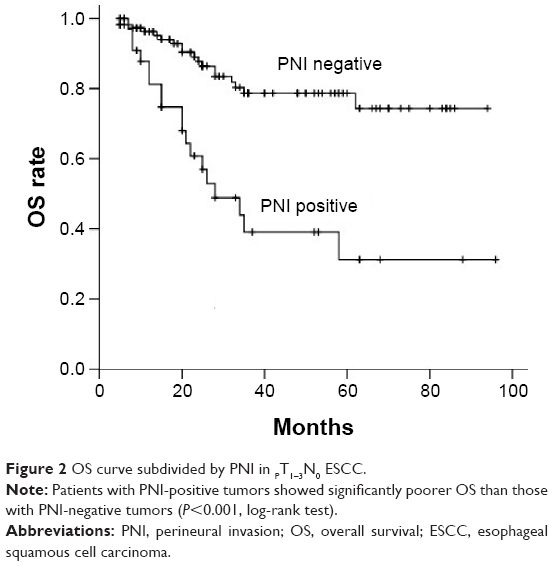 | Figure 2 OS curve subdivided by PNI in PT1–3N0 ESCC. |
Discussion
In this study, surgical specimens were stained with H&E to determine the positivity of PNI and analyze treatment decisions in relation to PNI status in PT1–3N0M0 ESCC. Despite the progression of adjuvant treatment, PT1–3N0M0 ESCC is always excluded from the recommendation for adjuvant chemoradiotherapy in the People’s Republic of China. However, our study clearly identified a worse prognostic subgroup in PT1–3N0M0 ESCC. According to the multivariate analysis, PNI was the only one independent prognostic factor. PT1–3N0M0 ESCC with positive PNI exhibited a markedly poorer prognosis and a higher rate of distant metastasis, suggesting an indication for additional adjuvant chemotherapy.
In this study, we found that 25.0% of the cases were PNI-positive, an intermediate percentage between the values reported in the literature, which range from 5% to 47.7%.11–13 The staining methods, measurement techniques, differences in histological types, and PNI definition may contribute to this discrepancy, which leads to difficult comparison across different studies. Actually, it also limits the clinical application of PNI. In the study, we used the broader definition as some other investigator described:13,14 cancer cells surrounding at least one-third of the nerve without invading through the nerve sheath, as well as tumor cells within any of the three layers of the nerve sheath. A study of ESCC patients undergoing radical esophagectomy found PNI to be associated with markers of aggressive and advanced disease.15 Chen et al13 found that PNI in ESCC was significantly correlated with tumor differentiation, infiltration depth, PN classification, and stage (P<0.05). Several other authors published similar results.11,16 In our study, PNI was not associated with other markers of cancer stage or aggressiveness except PT stage (P<0.001). Thus, PNI seems to be unrelated to other prognostic factors, such as tumor cell differentiation and tumor length. Furthermore, the 5-year DMFS rate was 37.2% in PT1–3N0M0 ESCC patients with PNI, which was significantly lower than the rate (62.3%) in the patients without PNI. Therefore, we speculated that PNI represents a distinct metastatic process, not simply tumor cell migration. This provides strong evidence for performing adjuvant chemotherapy at the presence of PNI in PT1–3N0M0 ESCC.
According to the National Comprehensive Cancer Network Guidelines®, PNI is considered to be one of the high-risk features in esophagus carcinoma, and chemoradiation therapy was recommended for patients with high-risk features. Recently, Ning et al17 retrospectively reviewed 243 locally advanced ESCC patients who underwent curative resection. PNI was identified in 22.2% (54/243) patients. In PNI-positive ESCC patients, the median disease-free survival time and OS time were longer in patients with postoperative radiotherapy than patients without postoperative radiotherapy. However, there were no statistical differences. In our study, only six patients with PNI received adjuvant chemotherapy, and four patients received adjuvant chemoradiotherapy. Until now, these patients survived without distant metastasis. It seems that adjuvant chemoradiotherapy can prolong disease-free survival and OS time in PNI-positive ESCC patients. Future prospective study is needed to confirm the function of additional adjuvant chemoradiotherapy in PNI ESCC patients.
Limitations
The major limitations of this study are small sample size and relatively short follow-up time. The small number of patients in the subgroup with PNI-positive tumors also limits the subgroup analysis. In addition, the retrospective nature of our study could be considered another significant limitation, which may have influenced this result. However, although our results should be confirmed by prospective studies, we believe that our results contribute to the literature because of the inclusion of only patients with early-stage ESCC. Finally, how PNI influences distant metastasis also remains unclear. The mechanism of nerve–tumor interaction in the perineural microenvironment needs to be understood to help develop novel treatment strategies in the PNI-related metastasis pathway to decrease recurrence.
Conclusion
In summary, this study confirmed the intermediate incidence of PNI in PT1–3N0M0 ESCC. PNI is related to T stage and distant metastasis, postoperatively. Furthermore, PNI contributes important additional information as an independent prognostic indicator for DMFS and OS. Large-scale and well-designed prospective cohort studies will be needed to elucidate how a quantification of PNI status may be used to determine the need for postoperative adjuvant chemoradiotherapy.
Acknowledgments
The authors are grateful to the patients who were included in this study. This study was supported by grants from the Nature Science Foundation of Zhejiang Province (no LY14H160012).
Disclosure
The authors report no conflicts of interests in this work.
References
Ariga H, Nemoto K, Miyazaki S, et al. Prospective comparison of surgery alone and chemoradiotherapy with selective surgery in resectable squamous cell carcinoma of the esophagus. Int J Radiat Oncol Biol Phys. 2009;75:348–356. | ||
Lin Y, Su X, Su H, et al. Prediagnostic smoking and postoperative survival in lymph node-negative esophagus squamous cell carcinoma patients. Cancer Sci. 2012;103:1985–1988. | ||
Song Z, Wang J, Lin B, Zhang Y. Analysis of the tumor length and other prognosis factors in pt1-2 node-negative esophageal squamous cell carcinoma in a Chinese population. World J Surg Oncol. 2012;10:273. | ||
Ando N, Kato H, Igaki H, et al. A randomized trial comparing postoperative adjuvant chemotherapy with cisplatin and 5-fluorouracil versus preoperative chemotherapy for localized advanced squamous cell carcinoma of the thoracic esophagus (jcog9907). Ann Surg Oncol. 2012;19:68–74. | ||
Zafirellis K, Dolan K, Fountoulakis A, Dexter SP, Martin IG, Sue-Ling HM. Multivariate analysis of clinical, operative and pathologic features of esophageal cancer: who needs adjuvant therapy? Dis Esophagus. 2002;15:155–159. | ||
Yoon DH, Jang G, Kim JH, et al. Randomized phase 2 trial of s1 and oxaliplatin-based chemoradiotherapy with or without induction chemotherapy for esophageal cancer. Int J Radiat Oncol Biol Phys. 2015;91:489–496. | ||
Cohn JA, Dangle PP, Wang CE, et al. The prognostic significance of perineural invasion and race in men considering active surveillance. BJU Int. 2014;114:75–80. | ||
Beard CJ, Chen MH, Cote K, et al. Perineural invasion is associated with increased relapse after external beam radiotherapy for men with low-risk prostate cancer and may be a marker for occult, high-grade cancer. Int J Radiat Oncol Biol Phys. 2004;58:19–24. | ||
Song J, Liu H, Li Z, Yang C, Sun Y, Wang C. Long-term prognosis of surgical treatment for early ampullary cancers and implications for local ampullectomy. BMC Surg. 2015;15:32. | ||
Zeng L, Guo Y, Liang J, et al. Perineural invasion and tams in pancreatic ductal adenocarcinomas: review of the original pathology reports using immunohistochemical enhancement and relationships with clinicopathological features. J Cancer. 2014;5:754–760. | ||
Takubo K, Takai A, Yamashita K, et al. Light and electron microscopic studies of perineural invasion by esophageal carcinoma. J Nat Cancer Inst. 1985;74:987–993. | ||
Khan OA, Alexiou C, Soomro I, Duffy JP, Morgan WE, Beggs FD. Pathological determinants of survival in node-negative oesophageal cancer. Br J Surg. 2004;91:1586–1591. | ||
Chen JW, Xie JD, Ling YH, et al. The prognostic effect of perineural invasion in esophageal squamous cell carcinoma. BMC Cancer. 2014;14:313. | ||
Liebig C, Ayala G, Wilks J, et al. Perineural invasion is an independent predictor of outcome in colorectal cancer. J Clin Oncol. 2009;27:5131–5137. | ||
Torres CM, Wang HH, Turner JR, et al. Pathologic prognostic factors in esophageal squamous cell carcinoma: a follow-up study of 74 patients with or without preoperative chemoradiation therapy. Modern Pathol. 1999;12:961–968. | ||
Ochiai M, Arai K, Funabiki T, et al. Local spread of carcinoma of the esophagus by perineural invasion. Nihon Geka Gakkai Zasshi. 1995;96:137–144. | ||
Ning ZH, Zhao W, Li XD, et al. The status of perineural invasion predicts the outcomes of postoperative radiotherapy in locally advanced esophageal squamous cell carcinoma. Int J Clin Exp Pathol. 2015;8:6881–6890. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.