Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 15
Performance of Multidimensional Severity Scoring Systems in Patients with Post‐Tuberculosis Bronchiectasis
Authors AL-Harbi A ![]() , AL-Ghamdi M
, AL-Ghamdi M ![]() , Khan M, AL-Rajhi S
, Khan M, AL-Rajhi S ![]() , AL-Jahdali H
, AL-Jahdali H
Received 12 May 2020
Accepted for publication 28 August 2020
Published 14 September 2020 Volume 2020:15 Pages 2157—2165
DOI https://doi.org/10.2147/COPD.S261797
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Abdullah AL-Harbi,1– 3 Majed AL-Ghamdi,1– 3 Mohammad Khan,1– 3 Sulaiman AL-Rajhi,1,3,4 Hamdan AL-Jahdali1– 3
1College of Medicine, King Saud University for Health Sciences, Riyadh, Saudi Arabia; 2Department of Medicine, Pulmonary Division, Ministry of National Guard-Health Affairs, Riyadh, Saudi Arabia; 3King Abdullah International Medical Research Center, Riyadh, Saudi Arabia; 4Department of Medical Imaging, Ministry of National Guard-Health Affairs, Riyadh, Saudi Arabia
Correspondence: Abdullah AL-Harbi
Department of Medicine, Pulmonary Division, Ministry of National Guard-Health Affairs, King Abdulaziz Medical City, PO Box 22490, MC 1443, Riyadh 11426, Saudi Arabia
Email [email protected]
Objective: The aim of this study was to assess the clinical characteristics and outcomes of patients with post‐tuberculosis (post-TB) bronchiectasis. We also evaluated the performance of various multidimensional severity score systems to predict mortality, future exacerbation, and hospitalization.
Methods: We conducted a prospective observational cohort study to evaluate the etiology of bronchiectasis in 301 patients. Patients fell into three groups: post-TB (129 [43%]), idiopathic (76 [25%]), and other (96 [32%]) etiologies of bronchiectasis. Four multidimensional grading scales, including the Bronchiectasis Severity Index (BSI), the FACED score, and two derivative versions of the FACED score, Exacerbation (Exa-FACED and E-FACED), were calculated and compared for each patient.
Results: Patients with post-TB bronchiectasis were predominantly female (61%) with a mean age of 68± 11 years. Moreover, 26% of post-TB bronchiectasis patients were colonized with Pseudomonas aeruginosa. At baseline, patients with post-TB bronchiectasis were older, had higher severity scores, and were more likely to have experienced severe exacerbations that required hospitalization compared to patients with idiopathic bronchiectasis or bronchiectasis arising from other causes. During follow-up, 52% of patients required hospitalization, 58% had frequent (≥ 2 per year) acute exacerbations, and the overall 5-year mortality rate was 30%. Five-year survival was efficiently predicted by each of the grading scales. Although the modified variations of the FACED outperformed the original FACED scale in predicting forthcoming frequent acute exacerbations and hospitalization, the BSI outperformed all three systems in this regard.
Conclusion: Patients with post-TB bronchiectasis had higher severity scores than patients with idiopathic bronchiectasis or bronchiectasis arising from other causes. In addition, all scoring systems performed adequately in 5-year mortality projections. BSI and the modified versions of the FACED outperformed the FACED in predicting forthcoming exacerbations and hospitalizations.
Keywords: bronchiectasis, post-TB bronchiectasis, Bronchiectasis Severity Index, BSI, FACED score, acute exacerbation, hospitalization, Exacerbation-FACED score, Exa-FACED score, E-FACED score
Introduction
In 2018, the World Health Organization (WHO) estimated that approximately 10 million people were affected by tuberculosis (TB), and 1.2 million people had died from the disease.1 Saudi Arabia is a moderate TB incidence country with an incidence rate of 10 cases per 100,000 population.1 The incidence rate has been decreasing over the past 50 years. Moreover, a recent meta-analysis demonstrated that patients who survived and completed TB treatment were three times more likely to die compared to the general population or to matched controls.2 The increased risk of mortality in post-TB patients has been attributed to permanent lung damage acquired during the disease duration or treatment but is not fully understood. Pulmonary sequel involvement occurs in more than half of TB patients and ranges from a simple radiological finding to severe pleuro-parenchymal destruction with severe physiological impairment, which can lead to respiratory failure and death.2–8 Bronchiectasis is another common complication of TB, and the prevalence of post-TB bronchiectasis has been found to range from 35% to 86% based on radiological findings.8 A recent prospective study of 405 TB patients in Malawi found that 44% of patients demonstrated bronchiectasis at the completion of pulmonary TB treatment.7 Moreover, TB is one of the most common causes of bronchiectasis in developing countries.9,10 As post-TB patients are at increased risk of mortality, it is important to understand the resulting pulmonary complications to improve patient care efforts for this high-risk patient group.
Bronchiectasis is currently evaluated by several multidimensional scoring systems, including the Bronchiectasis Severity Index (BSI), the FACED score, and two derivative versions of the FACED score: Exacerbation (Exa-FACED and E-FACED). These multidimensional scoring systems were designed to assess mortality and to predict the risk of future acute exacerbations and hospitalizations of bronchiectasis patients.11–14 The performance of these multidimensional scoring systems among patients with post-TB bronchiectasis is unknown. One previously published study compared the performance of the BSI and the FACED scoring system among patients with post-TB bronchiectasis and found that both scores accurately predicted mortality at 48 months. However, neither scoring system had adequate accuracy or power to predict readmission or exacerbation.15
The aim of this study was to assess the clinical characteristics and outcomes of patients with post‐TB bronchiectasis in comparison to patients with idiopathic bronchiectasis or bronchiectasis arising from other causes. Idiopathic bronchiectasis was chosen for comparisons based on its abundant prevalence and the perception that idiopathic bronchiectasis has a better prognosis.16,17 In addition, we assessed the performance of multidimensional severity scoring systems, including the BSI, the FACED, and the two derivative versions of the FACED, to predict mortality, future exacerbation, and hospitalization among patients with post-TB bronchiectasis.
Patients and Methods
Patient Cohort
The study cohort included patients enrolled in the King Abdulaziz Medical City-Riyadh bronchiectasis research database between January 2010 and December 2018. The aim of the research database is to assess the prevalence, characteristics, and long-term prognosis of patients with bronchiectasis. Adult patients were included if they had a primary diagnosis of bronchiectasis and were able to perform pulmonary function tests (PFTs). Patients were excluded if they had a primary diagnosis of cystic fibrosis, interstitial lung disease, obstructive airway diseases (COPD, asthma, or bronchiolitis obliterans), active mycobacterial infections, or active malignancy. Patients with multiple co-morbidities or expected survival of less than one year were also excluded from the study. Patients were evaluated and managed according to published guidelines.10,16,18 The study was approved by the institutional review board of King Abdullah International Medical Research Center (KAIMRC) in Riyadh, Saudi Arabia.
Bronchiectasis Diagnosis
The primary diagnosis of bronchiectasis was based on High resolution computed tomography (HRCT) chest findings and physician diagnosis. The etiology of bronchiectasis was assigned to each patient according to published guidelines.10,16 Post-TB bronchiectasis was assigned when history or clinical evidence of TB was evident and radiological findings of bronchiectasis in the same lung zone previously affected by TB. In the absence of TB history, the diagnosis was based on the clinical judgment of the physician and compatible HRCT findings that were suggestive of TB, such as pleuro-parenchymal scarring of the upper lobes, granuloma, and cavitation. Chronic respiratory colonization with bacteria was defined as “the isolation of potentially pathogenic bacteria in sputum culture on two or more occasions, at least 3 months apart in a 1-year period”.11,19 When a patient was unable to provide sputum samples, the patient was assumed to have no colonization. Exacerbation of bronchiectasis was defined as worsening of respiratory symptoms that required the patient to be treated with antibiotics at the exclusion of other potential causes of deterioration.10,16
Multidimensional Severity Scoring of Bronchiectasis
Four baseline risk prediction models were used, including the BSI, the FACED score, and the two derivative versions of the FACED score: Exacerbation-FACED (Exa-FACED) and E-FACED.11–14 BSI is calculated based on age, body mass index (BMI), predicted forced expiratory volume in one second (FEV1)%, history of respiratory hospitalization in the preceding 2 years, number of exacerbations in the previous year, Medical Research Council (MRC) Breathlessness Score, Pseudomonas colonization, colonization with other organisms, and radiological extension of the disease based on HRCT findings.11 The FACED score is calculated based on age, predicted FEV1%, MRC Breathlessness Score, Pseudomonas colonization, and radiological extension of the disease based on HRCT findings.12 The two modified versions of the FACED (Exa-FACED and E-FACED) expanded the original FACED score to include the number of exacerbations and/or hospitalizations in the previous year in the Exa-FACED and the number of hospitalizations in the previous year in the E-FACED.13,14 All variables in the risk prediction models were collected prospectively after the original publication of the BSI and FACED scores in January 201411,12 and retrospectively for the Exa-FACED and E-FACED scoring systems.13,14 Patients were classified as mild, moderate, and severe as defined in previous publications.11–14 All-cause mortality was evaluated up to 5 years after the severity score calculation. Additionally, severe acute exacerbations that required hospitalization were recorded up to one year after the severity score calculation.
Statistical Analyses
Statistical analyses were performed using standard software (SPSS v22 [IBM, Armonk, NY, USA] and MedCalc v18.11 [MedCalc Software, Ostend, Belgium]). We used descriptive statistics to summarize the data. Student’s t-test, Mann–Whitney U-test, Kruskal–Wallis test, chi-square test, and Fisher’s exact test were used to compare groups, as appropriate. Survival analyses were performed using the Kaplan-Meier and Cox proportional hazards regression methods. Hazard ratios (HRs) and their 95% confidence intervals (CIs) were determined. Multivariate logistic regression analyses were adjusted for different severity scores to compare groups for future acute exacerbations and hospitalization. The performance of the severity scores was evaluated by receiver operating characteristic (ROC) curves to identify the cut-off points of the BSI, FACED, Exa-FACED, and E-FACED scales in predicting mortality, future exacerbations, and hospitalizations. To compare dependent ROC curves, we utilized Delong’s method.20 Statistical significance was defined as a two-sided P-value <0.05.
Results
The study population included 345 patients with bronchiectasis who were enrolled in the King Abdulaziz Medical City-Riyadh prospective bronchiectasis research database. In total, 44 patients were excluded from analysis due to lack of PFT data (n=31), lost follow-up data (n=9), or refusal to participate in the study (n=4). The final study population included 129 (43%) patients with post-TB bronchiectasis, 76 (25%) patients with idiopathic bronchiectasis, and 96 patients (32%) with bronchiectasis arising from other causes.
The demographic and clinical characteristics of the patient cohort as well as comparisons between these characteristics in post-TB bronchiectasis patients and patients with idiopathic bronchiectasis or bronchiectasis arising from other causes are detailed in Table 1. The post-TB bronchiectasis group was predominantly female (61%) with a mean age of 68±11 years. Additionally, 26% of post-TB bronchiectasis patients were colonized with Pseudomonas aeruginosa, and cystic disease was noted by HRCT in 74% of these patients. The mean frequency of acute exacerbations in the previous year was 2.8%, and 52% of post-TB bronchiectasis patients had a severe acute exacerbation that required hospitalization. Overall, patients with post-TB bronchiectasis were older, had higher severity scores, were more likely to have experienced severe exacerbations that required hospitalization, were less likely to be colonized with Pseudomonas, and had a lower extent of lobes involvement compared to patients with idiopathic bronchiectasis (P<0.05 for all comparisons). Compared to patients with bronchiectasis that arose from other causes, post-TB bronchiectasis patients were older, had higher severity scores, had lower predicted FEV1%, experienced more acute exacerbations, required a greater number of hospitalizations, had a higher extent of lobes involvement, and were more likely to have cystic disease (P<0.05 for all comparisons) (Table 1).
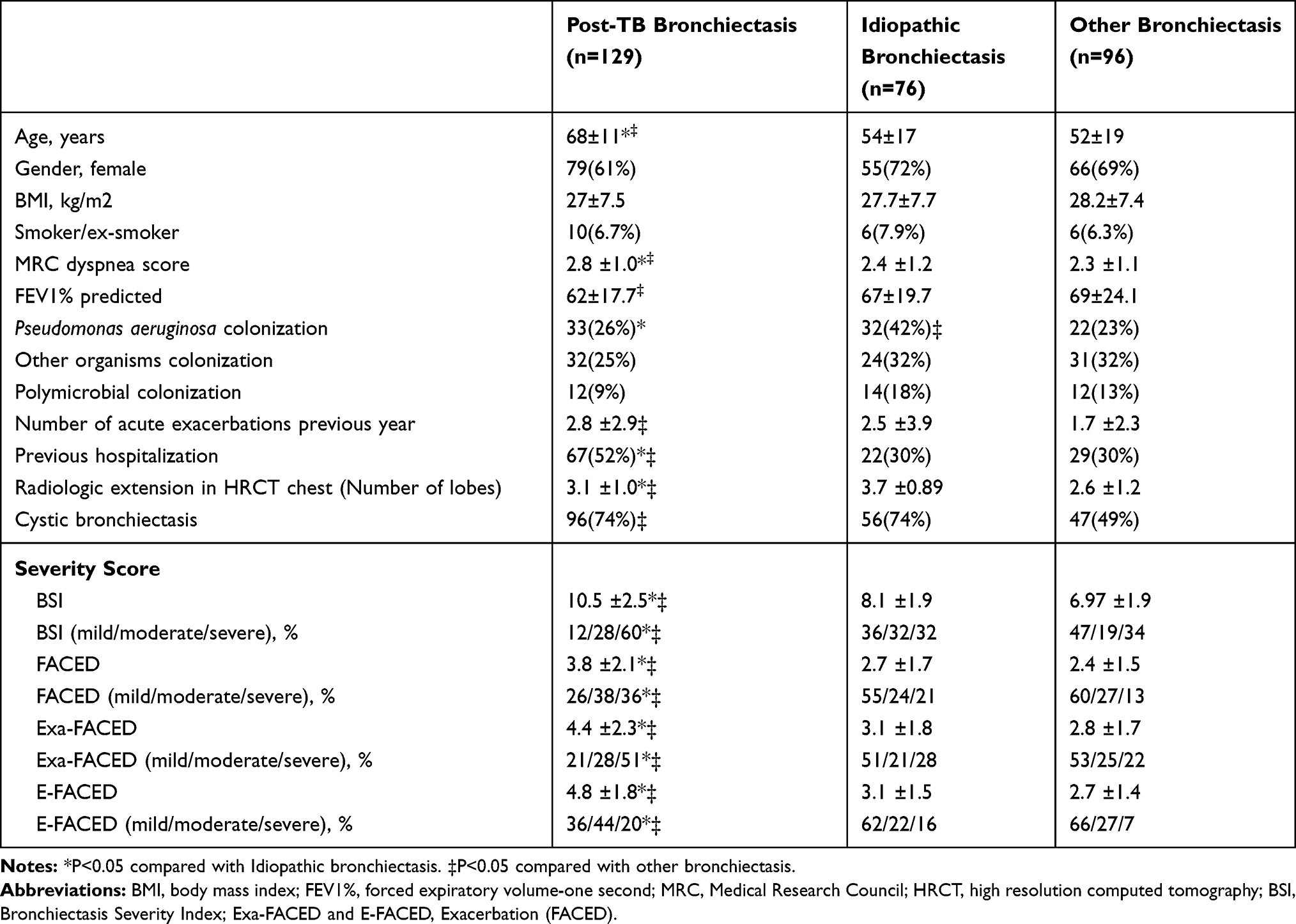 |
Table 1 Demographic and Clinical Characteristics of the Study Population |
Next, we compared the severity scores of the BSI, FACED, Exa-FACED, and E-FACED multidimensional scoring systems in post-TB bronchiectasis patients. The BSI score classified 16 (12%) post-TB bronchiectasis patients as mild, 36 (28%) as moderate, and 77 (60%) as severe. In contrast, the FACED score classified 33 (26%) post-TB bronchiectasis patients as mild, 49 (38%) as moderate, and 47 (36%) as severe (Table 2). There was fair agreement between the BSI and FACED scores (κ=0.28 [95% CI, 0.20 to 0.37], P<0.001). The Exa-FACED score reclassified 27 (21%) patients as mild, 36 (28%) as moderate, and 66 (51%) as severe, which demonstrated moderate agreement with the BSI score (κ=0.50 [95% CI, 0.38 to 0.63], P<0.001). Finally, the E-FACED score reclassified 47 (36%) patients as mild, 57 (44%) as moderate, and 25 (20%) as severe, which showed fair agreement with the BSI score (κ=0.14 [95% CI, 0.05 to 0.24], P<0.001) (Table 2).
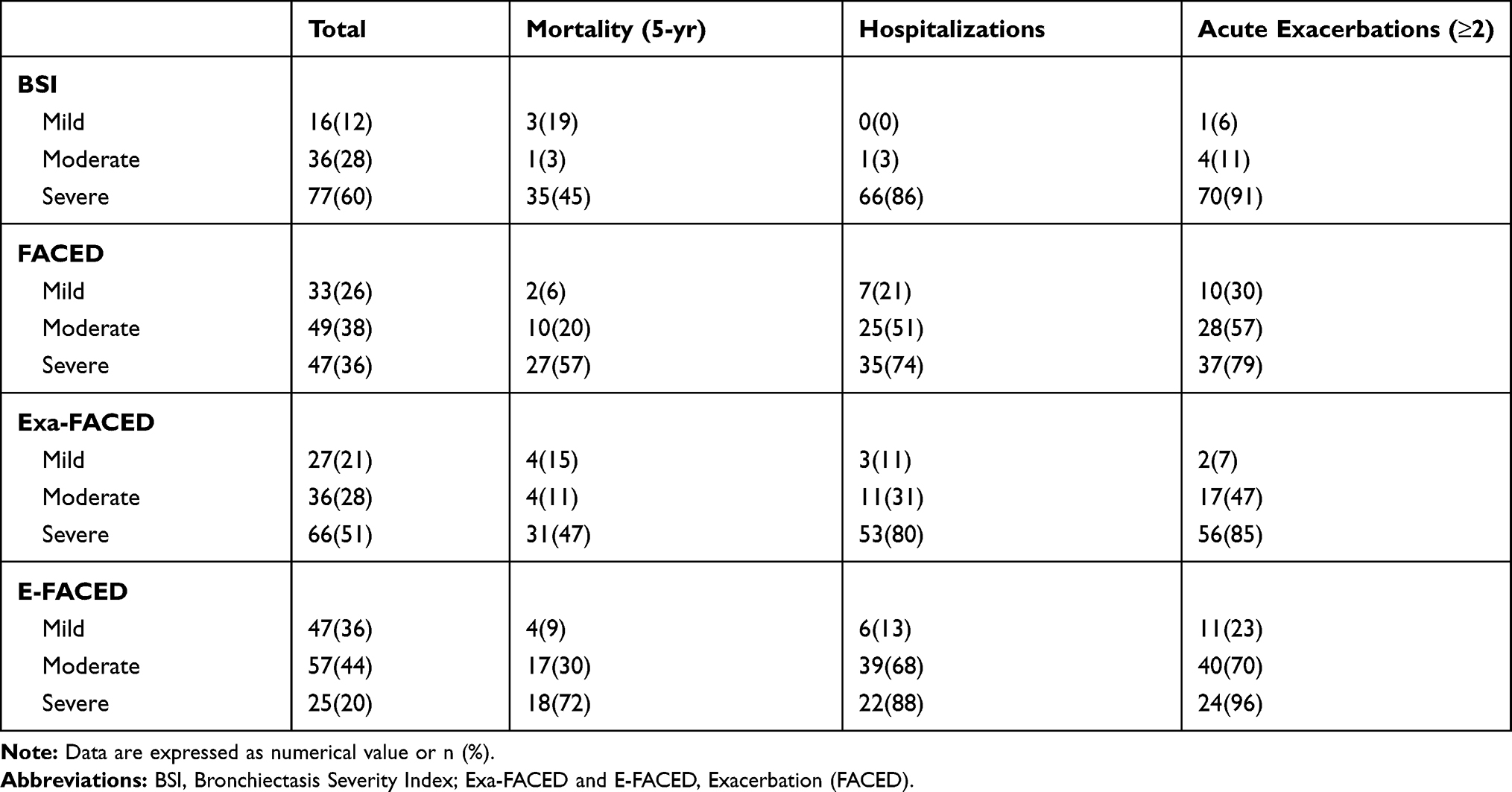 |
Table 2 Clinical Outcomes of Patients with Post-TB Bronchiectasis by Severity Scale (n=129) |
To evaluate the efficacy of the multidimensional severity scoring systems, we then compared the calculated severity scores with the patient outcomes observed during follow-up. There were 63 (21%) total deaths during the study period, and the overall 5-year mortality rate was 30% in patients with post-TB bronchiectasis, 18% in patients with idiopathic bronchiectasis, and 10% patients with bronchiectasis that arose from other causes. The mortality rate of patients with post-TB bronchiectasis differed across the severity scores. According to each of the scoring systems, low mortality was observed in mild cases (6–19%), and high mortality was observed in severe cases (45–57%) (Table 2). Each score demonstrated the ability to predict 5-year survival. The area under the curve (AUC) for the BSI score was 0.77 (95% CI, 0.69 to 0.84), which was not statistically different from that of the FACED (0.73 [95% CI, 0.64 to 0.80]), Exa-FACED (0.75 [95% CI, 0.66 to 0.82]), or E-FACED (0.77 [95% CI, 0.69 to 0.84]) scores (Figure 1). Kaplan-Meier survival curves are shown in Figure 2. The overall survival of patients with post-TB bronchiectasis was similar to that of patients with idiopathic bronchiectasis (log-rank, P=0.053) and was significantly lower than that of patients with bronchiectasis arising from other causes (log-rank, P<0.001). In contrast, multivariate Cox regression analyses (including etiology, all of the variables included in the calculation of the BSI score, and the BSI score) showed no differences in mortality rates between the three different etiologies of bronchiectasis. Compared to the post-TB bronchiectasis group, the hazard ratio for mortality was 1.27 (95% CI, 0.59 to 2.75, P=0.54) in the idiopathic bronchiectasis group and was 0.58 (95% CI, 0.27 to 1.27, P=0.17) in the other causes of bronchiectasis group. Similar results were observed when analyses were corrected for each severity score separately (all P-values P>0.05).
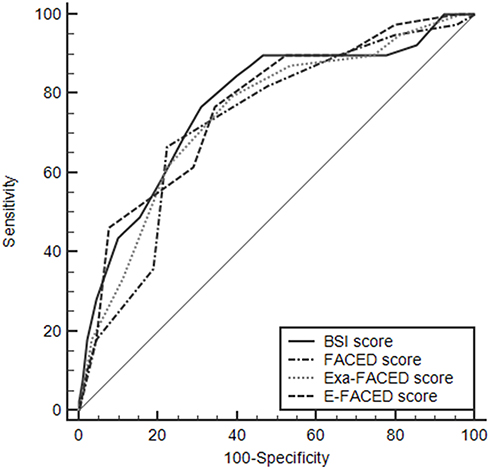 |
Figure 1 Receiver operating characteristic curves for bronchiectasis severity scales in predicting 5-year mortality. |
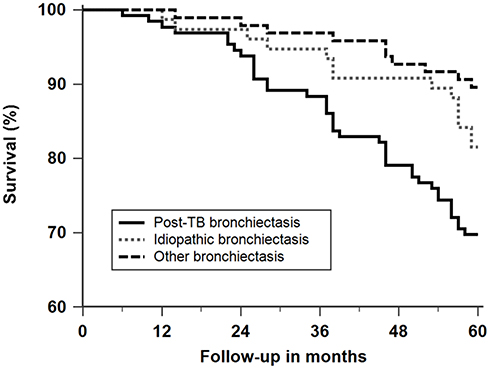 |
Figure 2 Kaplan–Meier curves comparing the survival rates of patients with post-TB, idiopathic, and other bronchiectasis. |
Beyond patient mortality, we were interested in the occurrence of disease complications and hospitalizations, as the risk of these events in post-TB bronchiectasis patients is currently unknown. Sixty-seven (52%) post-TB bronchiectasis patients, 22 (29%) idiopathic bronchiectasis patients, and 29 (30%) patients with bronchiectasis arising from other causes required hospitalization during the study period. After adjusting for BSI score, multivariate logistic regression analysis demonstrated no difference in the rate of hospitalization among the three etiologies of bronchiectasis. Compared to the post-TB bronchiectasis group, the idiopathic group had an odds ratio of 0.92 ([95% CI, 0.21 to 4.07]; P=0.91) and the other cause bronchiectasis group had an odds ratio of 2.28 ([95% CI, 0.68 to 7.60]; P=0.18). Similar results were observed when analyses were adjusted for each severity score separately (all P-values P>0.05).
We then assessed the ability of the multidimensional severity scoring systems to predict hospitalizations. The BSI score outperformed the other three scores in predicting the patients that required hospitalization for severe acute exacerbation. More specifically, of the patients with mild to moderate BSI scores, few patients (0–3%) required hospitalization. In contrast, hospitalization was required for the majority of patients with severe BSI scores (86%) (Table 2). The AUC for the BSI score was 0.98 (95% CI, 0.93 to 0.99), which was statistically different from the AUC of the FACED score (0.74 [95% CI, 0.65 to 0.81]), the Exa-FACED score (0.81 [95% CI, 0.74 to 0.88]), and the E-FACED score (0.83 [95% CI, 0.75 to 0.89]) (all P-values P<0.0001) (Figure 3A).
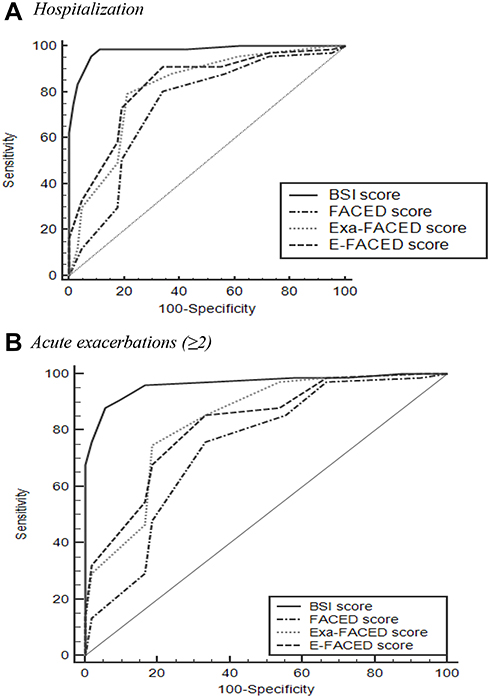 |
Figure 3 Receiver operating characteristics curves for bronchiectasis severity scales in predicting (A) hospitalization and (B) acute exacerbations (≥2). |
Frequent (≥2 per year) acute exacerbations were 75 (58%) among post-TB bronchiectasis, 32 (42%) among idiopathic bronchiectasis, and 35 (36%) among other causes of bronchiectasis. After adjusting for BSI score, multivariate logistic regression analysis demonstrated no difference in the rate of frequent exacerbations between the three etiologies of bronchiectasis. Compared to the other causes of bronchiectasis group, the post-TB bronchiectasis group had an odds ratio of 0.60 ([95% CI, 0.24 to 1.55]; P=0.29) and the idiopathic bronchiectasis group had an odds ratio of 1.27 ([95% CI, 0.45 to 3.55]; P=0.65). Similar results were observed when the analysis was adjusted for each severity score separately (all P-values P>0.05).
Finally, we assessed the ability of the multidimensional severity scoring systems to predict frequent (≥2 per year) acute exacerbations. Again, we found that the BSI score outperformed the other three scores in its ability to predict frequent acute exacerbations. Few patients with mild to moderate BSI scores (6–11%) had frequent acute exacerbations compared to the majority of patients with severe BSI scores (91%) who experienced frequent acute exacerbations (Table 2). The AUC for the BSI score was 0.97 (95% CI, 0.92 to 0.99), which was statistically different from the FACED score (0.74 [95% CI, 0.66 to 0.81]), the Exa-FACED score (0.84 [95% CI, 0.76–0.89]), and the E-FACED score (0.82 [95% CI, 0.75 to 0.88]) (all P-values P<0.0001) (Figure 3B).
Discussion
In this study, we describe the characteristics and outcomes of patients with post-TB bronchiectasis compared to patients with idiopathic bronchiectasis or bronchiectasis arising from other etiologies. At baseline, post-TB bronchiectasis patients were older, had higher severity scores, and were more likely to have experienced severe exacerbations that required hospitalization compared to patients with idiopathic bronchiectasis or other etiologies of bronchiectasis. The higher severity scores were primarily driven by elevated incidences of previous hospitalizations in post-TB bronchiectasis patients. At follow-up, patients with post-TB bronchiectasis had higher rates of mortality, frequent (≥2 per year) acute exacerbations, and severe exacerbations that required hospitalization. Importantly, these outcomes were insignificant when adjusted for the severity of bronchiectasis. In addition, we validated four multidimensional severity scoring systems, namely the BSI, the FACED, and the two derivative versions of the FACED (Exa-FACED and E-FACED), in post-TB bronchiectasis patients. Although each of the scoring systems demonstrated robust prediction of mortality, the BSI exhibited several advantages over the FACED in the prediction of future frequent (≥2 per year) acute exacerbations and hospitalizations. The modified versions of the FACED (Exa-FACED and E-FACED) showed improved performance over the original FACED for ability to predict future frequent acute exacerbations and hospitalizations.
Although several prediction models have been validated for non-cystic fibrosis bronchiectasis, none have been sufficiently evaluated in patients with post-TB bronchiectasis.11–14 One previous study compared the performance of the BSI and the FACED scoring systems in assessing clinically relevant disease outcomes in 101 patients with post-TB bronchiectasis.15 They found that both methods were capable of predicting mortality at 48 months (FACED, AUC=0.81; BSI, AUC=0.70); however, neither method had adequate accuracy or power to predict hospital readmission (FACED and BSI = 0.56) or exacerbation (FACED and BSI = 0.52).15 Here, we demonstrated that all four severity score models adequately predicted 5-year mortality (AUC: BSI=0.77, FACED=0.73, Exa-FACED=0.75, and E-FACED=0.77). The BSI was developed and validated by Chalmers et al, and the original AUC value of the BSI score for predicting mortality was 0.80 in the in derived cohort and ranged from 0.81 to 0.84 in external validation studies.11 The FACED score was developed and validated by Martinez-Garcia et al, and the original AUC values of the FACED score for predicting 5-year mortality were 0.87 in the construction group and 0.83 in the validation group.12 The two modified versions of the FACED (Exa-FACED and E-FACED) were developed to improve the ability of the FACED to predict the rate of frequent acute exacerbations and hospitalizations by Rosales-Mayor et al and Martinez-Garcia et al, respectively.13,14 Martinez-Garcia et al reported that the predictive ability of the E-FACED for all-cause and respiratory mortality were 0.87 and 0.86, respectively. Both AUCs were similar to those of the FACED.14 Due to the short follow-up period (1 year) of the original study, the Exa-FACED score was not evaluated for its ability to predict mortality.13 Several subsequent studies have confirmed that both the BSI and FACED scoring systems provide good predictive value with respect to mortality.21–24
In the present study, the BSI performed better than the FACED and its two modified versions in predicting future frequent acute exacerbations and hospitalizations. In addition, using the modified FACED scores improved the performance of the original FACED score to predict future frequent acute exacerbations and hospitalizations. The AUCs for hospitalization were 0.98, 0.74, 0.81, and 0.83, and the AUCs for frequent acute exacerbations were 0.97, 0.74, 0.84, and 0.82, for BSI, FACED, Exa-FACED, and E-FACED, respectively. The present study differs from the study by Wang et al, which did not find the BSI and FACED scores to have predictive capacity for hospital readmission or exacerbation in post-TB bronchiectasis patients.15 In previous studies of patients with non-cystic fibrosis bronchiectasis, the BSI was superior to the FACED in predicting frequent (≥2 per year) acute exacerbations and severe acute exacerbations that required hospitalization. Additionally, in a study by McDonnell et al, BSI was superior to FACED in predicting hospital admissions, and the AUCs for hospitalization were 0.82 for BSI and 0.65 for FACED in the pooled cohort.21 BSI was also a better predictor of exacerbations or hospitalization than FACED in a study reported by Rosales-Mayor et al In that study, the AUCs for hospitalization were 0.89 for BSI and 0.81 for FACED, and the AUCs for acute exacerbations were 0.81 for BSI and 0.73 for FACED. Importantly, both of the modified versions of the FACED improved on key aspects of the predictive value of the original FACED. The Exa-FACED improved the prediction for exacerbations (AUC=0.76) and hospitalizations (AUC=0.82).13 Moreover, the E-FACED improved the capacity to predict future frequent acute exacerbations (AUC=0.82) and hospitalizations (AUC=0.87) compared to that of the FACED (AUC: 0.72 and 0.78, respectively).14
There are several limitations to our study that should be acknowledged. First, the patients included in the study were recruited from a subspecialty clinic in a tertiary center with small number of post-TB bronchiectasis patients. The small sample size and the method of sampling may introduce referral and selection bias, which limits the generalization of our findings to other populations and settings. Second, although we collected the clinical data for Exa-FACED and E-FACED scores prospectively, we calculated the scores retrospectively, as recently published.13,14 Therefore, the revised FACED scores may need to be validated in a prospective study to be considered fully validated. Nevertheless, the only differences we observed between the FACED score and its modified versions were the number of exacerbations and hospitalizations in the previous year, which were readily available in our database, because they are also used to calculate the BSI. This suggests that although we calculated the modified FACED scores retrospectively, the validity of our findings was not impacted. Third, patients with multiple major co-morbidities were excluded from the study, which is similar to previous validation studies in bronchiectasis. As a result, our study included selected patients and was not representative of the whole bronchiectasis patient population. Patients with bronchiectasis frequently have co-morbidities, such as COPD, pulmonary hypertension, cardiovascular disease, and cancers, which may impact patient morbidity and mortality.
In conclusion, post-TB bronchiectasis patients were older and had higher severity scores compared to idiopathic bronchiectasis patients and patients with bronchiectasis arising from other causes. We found no difference in mortality, frequent acute exacerbations, or hospitalizations between the etiological groups of bronchiectasis patients after adjusting for bronchiectasis severity. Our study also provides external validation of the four multidimensional severity scoring systems (BSI, FACED, Exa-FACED, and E-FACED) in patients with post-TB bronchiectasis. Although each of the scoring systems adequately predicted 5-year mortality, the BSI and the two modified versions of the FACED performed better in terms of predicting future frequent acute exacerbations and hospitalizations compared with the FACED. Future prospective research in larger cohorts from diverse geographical areas is necessary to confirm these findings.
Abbreviations
Post-TB, post‐tuberculosis; BSI, Bronchiectasis Severity Index; Exa-FACED, Exacerbation-FACED; E-FACED, Exacerbation-FACED; WHO, World Health Organization; TB, tuberculosis; KAIMRC, King Abdullah International Medical Research Center; HRCT, high resolution computed tomography; FEV1, forced expiratory volume in one second; MRC, Medical Research Council; HR, hazard ratio; CI, confidence interval; ROC, receiver operating characteristics; AUC, the area under the curve.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics and Consent Statement
The study was approved by the institutional review board of King Abdullah International Medical Research Center (KAIMRC) in Riyadh, Saudi Arabia. Written informed consent was obtained from individual participants and from the parents for patients who are less than 16 years old.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. WHO. Global Tuberculosis Report 2019. Geneva: World Health Organization; 2020. Available from: https://apps.who.int/iris/bitstream/handle/10665/329368/9789241565714-eng.pdf?ua=1.
2. Romanowski K, Baumann B, Basham CA, Ahmad Khan F, Fox GJ, Johnston JC. Long-term all-cause mortality in people treated for tuberculosis: a systematic review and meta-analysis. Lancet Infect Dis. 2019. doi:10.1016/S1473-3099(19)30309-3
3. Ravimohan S, Kornfeld H, Weissman D, Bisson GP. Tuberculosis and lung damage: from epidemiology to pathophysiology. Eur Respir Rev. 2018. doi:10.1183/16000617.0077-2017
4. Pasipanodya JG, Miller TL, Vecino M, et al. Pulmonary impairment after tuberculosis. Chest. 2007. doi:10.1378/chest.06-2949
5. Ralph AP, Kenangalem E, Waramori G, et al. High morbidity during treatment and residual pulmonary disability in pulmonary tuberculosis: under-recognised phenomena. PLoS One. 2013. doi:10.1371/journal.pone.0080302
6. Maguire GP, Anstey NM, Ardian M, et al. Pulmonary tuberculosis, impaired lung function, disability and quality of life in a high-burden setting. Int J Tuberc Lung Dis. 2009;13:1500–1506.
7. Meghji J, Lesosky M, Joekes E, et al. Patient outcomes associated with post-tuberculosis lung damage in Malawi: a prospective cohort study. Thorax. 2020. doi:10.1136/thoraxjnl-2019-213808
8. Meghji J, Simpson H, Squire SB, Mortimer K. A systematic review of the prevalence and pattern of imaging defined post-TB lung disease. PLoS One. 2016. doi:10.1371/journal.pone.0161176
9. Hua GY, Jie GW, Xia LS, et al. Aetiology of bronchiectasis in adults: a systematic literature review. Respirology. 2016. doi:10.1111/resp.12832
10. Al-Jahdali H, Alshimemeri A, Mobeireek A, et al. The Saudi Thoracic Society guidelines for diagnosis and management of noncystic fibrosis bronchiectasis. Ann Thorac Med. 2017;12(3):135. doi:10.4103/atm.ATM_171_17
11. Chalmers JD, Goeminne P, Aliberti S, et al. The Bronchiectasis Severity Index. An international derivation and validation study. Am J Respir Crit Care Med. 2014;189(5):576–585. doi:10.1164/rccm.201309-1575OC
12. Martínez-García MA, De Gracia J, Relat MV, et al. Multidimensional approach to non-cystic fibrosis bronchiectasis: the FACED score. Eur Respir J. 2014;43(5):1357–1367. doi:10.1183/09031936.00026313
13. Rosales-Mayor E, Polverino E, Raguer L, et al. Comparison of two prognostic scores (BSI and FACED) in a Spanish cohort of adult patients with bronchiectasis and improvement of the FACED predictive capacity for exacerbations. PLoS One. 2017;12(4):e0175171. doi:10.1371/journal.pone.0175171
14. Martinez-Garcia MA, Athanazio RA, Girón R, et al. Predicting high risk of exacerbations in bronchiectasis: the E-FACED score. Int J COPD. 2017;12:275–284. doi:10.2147/COPD.S121943
15. Wang H, Bin JX, Li CW, et al. Clinical characteristics and validation of bronchiectasis severity score systems for post-tuberculosis bronchiectasis. Clin Respir J. 2018. doi:10.1111/crj.12911
16. Pasteur MC, Bilton D, Hill AT. British thoracic society guideline for non-CF bronchiectasis. Thorax. 2010. doi:10.1136/thx.2010.142778
17. De Soyza A, McDonnell MJ, Goeminne PC, et al. Bronchiectasis rheumatoid overlap syndrome is an independent risk factor for mortality in patients with bronchiectasis: a multicenter cohort study. Chest. 2017. doi:10.1016/j.chest.2016.12.024
18. Polverino E, Goeminne PC, McDonnell MJ, et al. European Respiratory Society guidelines for the management of adult bronchiectasis. Eur Respir J. 2017. doi:10.1183/13993003.00629-2017
19. Pasteur MC, Helliwell SM, Houghton SJ, et al. An investigation into causative factors in patients with bronchiectasis. Am J Respir Crit Care Med. 2000. doi:10.1164/ajrccm.162.4.9906120
20. DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988. doi:10.2307/2531595
21. McDonnell MJ, Aliberti S, Goeminne PC, et al. Multidimensional severity assessment in bronchiectasis: an analysis of seven European cohorts. Thorax. 2016. doi:10.1136/thoraxjnl-2016-208481
22. Ellis HC, Cowman S, Fernandes M, Wilson R, Loebinger MR. Predicting mortality in bronchiectasis using bronchiectasis severity index and FACED scores: a 19-year cohort study. Eur Respir J. 2016. doi:10.1183/13993003.01312-2015
23. Athanazio R, Pereira MC, Gramblicka G, et al. Latin America validation of FACED score in patients with bronchiectasis: an analysis of six cohorts. BMC Pulm Med. 2017. doi:10.1186/s12890-017-0417-3
24. Menéndez R, Méndez R, Polverino E, et al. Factors associated with hospitalization in bronchiectasis exacerbations: A one-year follow-up study. Respir Res. 2017. doi:10.1186/s12931-017-0659-x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.