Back to Journals » Medical Devices: Evidence and Research » Volume 15
Performance of Centargo: A Novel Piston-Based Injection System for High Throughput in CE CT
Authors Kemper CA ![]() , Mihl C, Martens B
, Mihl C, Martens B ![]() , McDermott MC, Hendriks BMF
, McDermott MC, Hendriks BMF ![]()
Received 9 December 2021
Accepted for publication 23 March 2022
Published 5 April 2022 Volume 2022:15 Pages 79—87
DOI https://doi.org/10.2147/MDER.S353221
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Corey A Kemper,1 Casper Mihl,2,3 Bibi Martens,2,3 Michael C McDermott,2,4 Babs MF Hendriks2,3
1Bayer U.S. LLC, Bayer Pharmaceuticals, Radiology R&D, Indianola, PA, USA; 2Department of Radiology & Nuclear Medicine, Maastricht University Medical Center, Maastricht, the Netherlands; 3Cardiovascular Research Institute Maastricht (CARIM), Maastricht University, Maastricht, the Netherlands; 4Bayer AG, Radiology R&D, Berlin, Germany
Correspondence: Corey A Kemper, Bayer U.S. LLC, Bayer Pharmaceuticals, Radiology R&D, 1 Bayer Dr, Indianola, PA, USA, Tel +1 412 225 3907, Email [email protected]
Purpose: To compare an investigational device (MEDRAD® Centargo CT Injection System, “Centargo”) to the currently available MEDRAD® Stellant CT Injection System (“Stellant”), in terms of efficiency, injector performance, and user satisfaction.
Patients and Methods: A total of 425 patients at two sites were enrolled; 198 patients in phase one, a randomized study (98 Stellant and 100 Centargo). The second observational phase included 227 patients who were injected with Centargo. Phase one recorded times for setup, disassembly, and patient changeovers. Demographic data, subjective image quality, and injection parameters were collected. Phase two assessed usability via a questionnaire provided to all end-users of both systems (radiographers).
Results: Patient changeover times were statistically significantly faster with Centargo (15.4s ± 8.7s vs 53.7s ± 19.6s, p < 0.001). Centargo day-setup times were similar to Stellant (138.1s ± 92s vs 151.8s ± 30.6s, p = 0.33) and end-of-day-disassembly times were significantly slower (60.6s ± 27s vs 17.1s ± 12.9s, p < 0.001). Based on four different scenarios modelling patient throughput, the projected time savings with Centargo over Stellant was 40– 63%, with the highest efficiency improvements for higher throughputs and the use of larger contrast medium bottles. Both Centargo and Stellant usability averaged between “Very Easy” and “Easy” in all responses to the questionnaire. There were no instances of interrupted injections due to communication loss or detected air and no insufficient images due to injector performance. No safety issues were identified.
Conclusion: Centargo was able to demonstrate improved efficiency as compared to Stellant while maintaining injector performance and high usability scores.
Keywords: power injection, efficiency, time savings, usability, Centargo
Introduction
The number of contrast-enhanced computed tomography (CT) examinations is increasing all over the world each year. Due to the development of the scanner technology and the availability of Multidetector CT (MDCT), the time to conduct the scan itself has become shorter.1
Intravenous injection of iodinated contrast media (CM) can aid in visualizing the vasculature, organs, and pathologies.2 Power injection systems are commonly used for contrast-enhanced CT (CE CT) to achieve consistent flow rates and to allow for control of the injection remotely, outside the scan room. Most common are syringe-based systems, where one or two empty, disposable syringes are filled from CM bottles and saline bags.3 The injection system mechanically drives a piston forward through each syringe, generating sufficient pressure to administer the programmed injection protocol, which is determined based on a variety of patient and procedure specific factors.4 While performance of such devices is well-accepted, there are limitations from a workflow efficiency perspective. The time to prepare the CM injection often takes longer than the image acquisition itself. There are “syringeless” systems that instead utilize peristaltic pumps to deliver the fluid, which have been shown to shorten setup and changeover time,5,5,6,6,7 but the performance is not in all aspects comparable to a piston-based system. Maximum pressures can be lower, leading to lower achievable iodine delivery rates,8 and the pulsatility of the flow is higher.9 Both of these factors can lead to inferior CM enhancement, which in turn can produce CT images with a reduced diagnostic quality.4,10,11
A novel CT injection system has been designed to maintain the fluid delivery advantages of a piston-based system (such as the Stellant CT injection system) but with the highest possible time efficiency, allowing the radiographer to spend less time handling the injector and disposables and more time focusing on the patient. While the technical fluid delivery performance is very similar between this novel injection system and the current piston-based system,8 the main differences are in the workflow features. These include an addition of a third syringe for CM, a simplified snap-in patient line designed for changing disposables between procedures, and automated features such as automatic priming and automatic refilling to reduce manual preparation time. The aim of this study is to compare the investigational injection system (Centargo) to the currently available Stellant CT injection system, in terms of efficiency, performance, and user satisfaction.
Materials and Methods
Study Design
This was a randomized multi-center, multi-country prospective clinical study, approved by BellBerry Human Research Ethics Committee (Australia) and the medical ethics research committee METC aZM/UM (the Netherlands). The study-outline was posted on ClinicalTrials.gov with the identifier NCT03875469. The study was performed in accordance with the ICH Good Clinical Practice guidelines. The patient population consisted of adults (≥ 18 years) already referred for a CE CT. All patients provided informed consent. The injection protocols and scanner settings followed the site’s typical practice, which was based on the indication for imaging and any patient-specific needs. No additional injections or scans beyond usual clinical practice were performed. Two centers were participating. First was Medscan Merrylands, an imaging center in Sydney (Australia), focused primarily on cardiac imaging. Their standard CM was iohexol 350 mgI/mL (GE Healthcare) in 200mL bottles. Second was Maastricht University Medical Center, an academic tertiary referral hospital located in Maastricht (the Netherlands). Their standard CM was iopromide 300 mgI/mL (Bayer AG) in 500 mL bottles.
The study was designed with two phases, shown in Figure 1. The first phase was a randomized trial to test Centargo’s time efficiency compared to Stellant, when Stellant is used with a multi-patient (MP) disposable set. Setup time for the MP set, bottle/bag changeover time, patient changeover time, and disassembly time for the MP set were collected. Figure 2 provides an example of the physical interaction steps that were measured using a stopwatch.
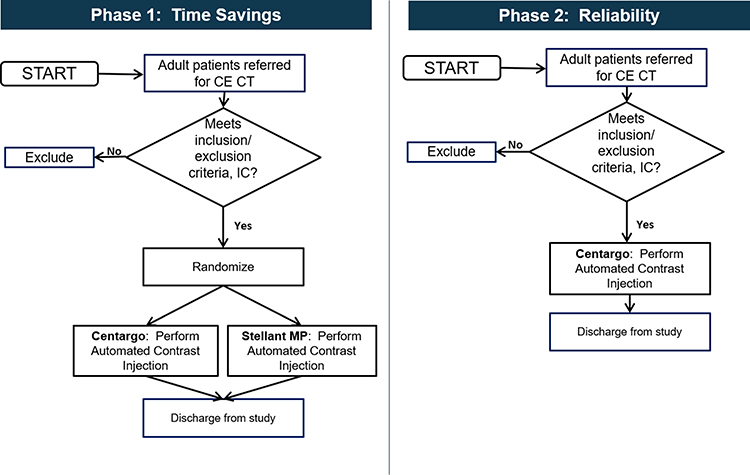 |
Figure 1 Study flowchart for phase 1 and phase 2 of the PerCenT study. |
 |
Figure 2 Overview of the timing process for phase 1 data collection of the study. Light blue dots represent new bottles, and dark blue dots represent new patients. Abbreviations: BC, bottle change; Pt, patient. |
The minimum sample size for phase one of the study was based on the primary endpoint, which was the time efficiency difference between the two injection systems. Based on a preliminary pilot study conducted in a simulated environment, a time savings of approximately 50% was anticipated, assuming a minimum of ten subjects per day, which is a conservative estimate at high throughput sites. Using the standard deviation (SD) from the Stellant dataset of the bench study, for 90% power, group sample sizes of 98 and 98 would be required. To balance enrolment across sites, group sample sizes of 100 and 100 for this phase were required (50 subjects per group per planned site).
The second phase was a prospective observational study of Centargo only, in order to test the overall reliability of the system and create additional time for the radiographers (end-users) to use the injector prior to providing feedback. Across both study phases, adverse events and device deficiencies were collected. Additionally, for each patient, demographic data (height, weight, age, and gender), procedure data (indication, CM type and concentration used, catheter type, and injection site) and timing data were recorded in an electronic case report form. Automatic data collection from the injector logged programmed protocols, pressures, flow rates, and any alerts/errors. Finally, in order to compare the qualitative usability of Stellant and Centargo, radiographers were surveyed on their satisfaction with the two systems after study enrolment completed, based on a pre-defined questionnaire. Each question (listed in Table 1) was scored on a scale of 1 (Very Easy) to 5 (Very Hard).
 |
Table 1 User Questionnaire Results per Injection System. Radiographers Scored the Ease of Certain Tasks in Patient Preparation on a 1–5 Scale, Where 1 is “Very Easy” and 5 is “Very Hard” |
Statistical Analysis
Descriptive statistics are provided as mean ± SD for continuous variables and absolute and relative frequencies for categorical variables. Comparisons between the groups with the endpoints specified above were performed by using the χ2 test for categorical variables and t-test or Mann–Whitney-U-test for continuous variables as appropriate. Primary endpoint was the total day-time needed for setup (once a day), per patient change time and teardown time. Study design and sample size calculations were done with PASS15 (PASS 15 Power Analysis and Sample Size Software (2017). NCSS, LLC. Kaysville, Utah, USA, ncss.com/software/pass). P-values are all 2-sided and considered significant when below 0.05. Microsoft Excel for Microsoft 365 MSO (Microsoft Corporation. Redmond, WA, USA) was used in the final analysis.
Results
Enrolment and Patient Demographics
Demographics were similar between the two groups, as shown in Table 2. Site profiles drove differences in indications, procedure types, and CM used. Medscan completed their phase one enrolment at 100 patients total (50 Centargo, 50 Stellant), and then moved onto phase two, where they enrolled an additional 227 patients. Maastricht enrolled 98 patients in phase one (50 Centargo, 48 Stellant) prior to ending the study early due to the COVID-19 situation in March 2020.
 |
Table 2 Patient Baseline Characteristics per Injection System for the Two Study Phases |
Time Comparison
The primary endpoint of the study was measuring workflow efficiency and usability of Centargo vs Stellant. Descriptive statistics for each timing measurement are shown in Table 3, with corresponding box plots in Figure 3. Patient changeover times were statistically significantly faster with Centargo (15.4s ± 8.7s vs 53.7s ± 19.6s, p < 0.001). Centargo day-setup times were similar to Stellant (138.1s ± 92s vs 151.8s ± 30.6s, p = 0.33) and end-of-day-disassembly times were significantly slower (60.6s ± 27s vs 17.1s ± 12.9s, p < 0.001).
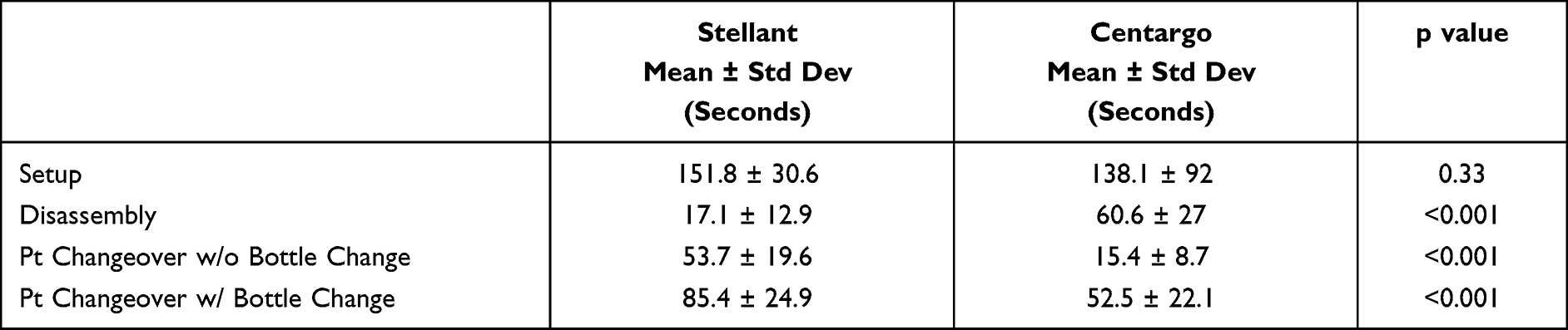 |
Table 3 Mean Handling Times Recorded for Setup, Disassembly, and Patient Changeover, with (w/) and without (w/o) Bottle Changes |
 |
Figure 3 Handling time results for each device at each site: (A) setup times from start of the day. (B) Disassembly times from end of the day. (C) Patient changeover times when a bottle change is required to refill the system. (D) Patient changeover times when only a change of the patient line is required. |
Injection System Performance
Injector performance was analyzed on the basis of phase one data, as this allows for balance between the two sites (50 Centargo patients at each site), instead of the data being dominated by Medscan’s phase two enrolment (an additional 227 Centargo patients). Both injectors were used across a broad range of injection sites, procedure types, and flow rates, with two different CM types and commonly used catheters. All injections were completed successfully. Relative distributions of injection sites and catheter types are shown in Figure 4. As shown in Figure 5, peak pressure increased with increasing flow rate and CM viscosity (iohexol 350 is higher viscosity than iopromide 300).
 |
Figure 4 Intravenous (IV) access information, including IV sites (A) and catheter types (B). Abbreviation: ACF, antecubital fossa. |
 |
Figure 5 Peak pressures generated depending on CM concentration and catheter type. |
User Satisfaction
In order to compare the qualitative usability of Stellant and Centargo, radiographers were surveyed on their satisfaction with the two systems (Table 1). Each question was scored on a scale of 1 (Very Easy) to 5 (Very Hard). Only two questions showed statistically significant differences. Satisfaction with Centargo is higher for connecting a patient line (p < 0.05). This is also consistent with the measured time savings for patient changeovers. Satisfaction with Centargo is lower for opening the Day Set package (p < 0.05).
Reliability
In addition, in terms of overall performance of the investigational system and clinical reliability, there were no injections disarmed by communication loss, nor any recorded electrical or mechanical system faults. Additionally, there were no instances of air being detected from either of the two main air detection mechanisms. No procedures were interrupted or had to be repeated due to the new air detector features. There were also no reports of air injection, cross-contamination, or insufficient images due to injector performance. There was, however, one instance of pressure limiting (reduction of flow rate due to high pressure) at Maastricht.
Minor device deficiencies occurred at both sites, with the majority occurring at the beginning of the day as the injector was powered on and when the Day Set was installed and prior to patient connection. For the device deficiency when the control room display was unresponsive, the scan room display was able to be used successfully with no impact to that patient’s exam. In one other instance, communication loss occurred between the scan room unit and the control room display after the injection started, but the injector is able to complete the injection normally, even if it loses communication with the control room display.
Discussion
The results of this study demonstrate an excellent time efficiency for patient changeovers of a new piston-based CM injector, compared to its technical predecessor. Centargo shows time efficiency benefits that previously have only been demonstrated for peristaltic-pump based systems, whilst also providing superior fluid delivery performances in terms of flow rate consistency and maximum achievable iodine delivery rates.8 These results are attributed to the snap-in connection, automatic re-filling, and automatic priming. This is the first study that also included workflow differences across two very different clinical sites, one imaging center and one academic research center, with different CM bottle sizes (200 mL bottles vs 500 mL bottles) available. Finally, it establishes that even for a new, unfamiliar device, staff members were able to quickly learn how to set up the disposables and run the user interface. Compared to a device that both sites had been using for over a decade, user satisfaction scores and timing measurements were comparable.
Because study enrolment could not reflect actual patient throughput due to patient eligibility, staffing constraints and the need for informed consent, any calculations regarding total daily interaction time with the injector therefore would be skewed. They would include fewer patient changeovers than would occur in a normal setting and would be dominated by setup and disassembly, which are required each day. However, the individual timings for each interaction type (setup, patient changeover, disassembly) are still representative of what one expects to see clinically. For that reason, to estimate what projected time savings would be in normal clinical use where all injections would be performed with a single injector, four different scenarios were modelled (Table 4). There are three main aspects to consider: number of hours the department must be available, the patient throughput, and the CM bottle sizes available. For each of the scenarios, the number of setups, disassemblies, bottle changes, and patient changeovers are shown graphically in the Figure 6. It is important to note that because the MP kit for Stellant has a maximum 12 hour in-use time, and the Day Set for Centargo has a maximum 24 hour in-use time, two Stellant MP kits are required for departments that are open for more than 12 hours. There are a variety of other combinations that could be considered, such as sites that use more than one CM concentration, which would require changing of the Stellant MP kit but could be supported with only one Centargo Day Set due to having an additional reservoir. Patient throughput is also not limited to 20 per day; there are many sites that are more demanding and may run more than twice that number. Modelling of these scenarios is intended only to provide a reasonable representation of example sites.
 |
Table 4 Hypothetical Clinical Workflow Scenarios Used to Project Differences in Average Touch Time |
 |
Figure 6 Schematics of each hypothetical clinical workflow (A–D) used for timing projections. Light blue dots represent new bottles, and dark blue dots represent new patients. |
Using the median timing values measured in the study in order to avoid the effect on outliers on the average values, the equation below was used to calculate the average injector touch times per patient in each of the four scenarios.

Results are shown in Figure 7. The projected per-patient injector touch time savings ranged from 40–63%, depending on operating hours, patient throughput, and the size of the CM bottles available at each center. As the number of CE CT exams per day increases, the amount of time saved would be expected to increase as well. Further work would need to be done after the injector is no longer an investigational device to study the potential implications of these time savings in terms of staffing and resources needs, length of appointment timeslots and number of patients who can be scanned per day on a given scanner. Because the preparation of the injector for each patient is only a subset of the overall time required for the exam, it would not be anticipated that the total exam time per-patient would be reduced by this same factor. However, eliminating manual tasks and minimizing touch time would be expected to lead to a more streamlined workflow.
 |
Figure 7 Projected time savings depending on patient throughput, operating hours, and bottle size availability. |
Limitations
Limitations of the clinical investigation were tied to two main aspects. First, because of the nature of a clinical study, informed consent was required, and patients were randomized between the control group and the investigational device group. This meant that, at most, Centargo was used on fewer than 50% of the patients assigned to a particular scanner, which is not a realistic use of the injector, where it would normally be used for all contrast enhanced scans. Therefore, features such as the second CM loading location, were not used as part of the study. Due to the unpredictability in enrolment, it was not possible for sites to plan for how many patients would receive injections each day. This limited any optimization for bottle change-overs and waste reduction. The statistical test for the primary endpoint is regarded inferential, all other statistical tests are regarded descriptive and hypothesis-generating only.
Conclusion
In terms of time efficiency gains, the projected per-patient injector touch time savings with Centargo over Stellant was between 40–63%, depending on operating hours, patient throughput, and availability of large CM bottles. This improvement is attributed to the new snap-in patient line, automatic refilling, and automatic priming, which combine to reduce touch time associated with patient changeover by 30–40 seconds. It is also reflected in higher user satisfaction with the ease in patient changeover. Centargo was able to demonstrate improved efficiency as compared to Stellant, while maintaining injector performance and high usability scores.
Data Sharing Statement
Individual deidentified patient data is not available to be shared for legal and ethical reasons.
Acknowledgments
The author team would like to acknowledge the contributions of Carsten Schwenke for the statistical design of the study. In addition, many thanks to the radiographers, technologists, radiologists, and staff at both Medscan Merrylands (Australia) and Maastricht University Medical Center (Netherlands) for their efforts in conducting the study, collecting the data, and providing feedback.
Funding
This clinical study was funded by Bayer.
Disclosure
C.A. Kemper is an employee of Bayer US, LLC, and M.M. McDermott is an employee of Bayer. B.M.F. Hendriks, C. Mihl, and B Martens receive personal fees (speakers bureau) from Bayer. The authors report no other conflicts of interest in this work.
References
1. Lell MM, Wildberger JE, Alkadhi H, Damilakis J, Kachelriess M. Evolution in computed tomography: the battle for speed and dose. Invest Radiol. 2015;50(9):629–644. doi:10.1097/RLI.0000000000000172
2. Rutten A, Prokop M. Contrast agents in X-ray computed tomography and its applications in oncology. Anti-Cancer Agents Med Chem. 2007;7(3):307–316.
3. Indrajit IK, Sivasankar R, D’Souza J, et al. Pressure injectors for radiologists: a review and what is new. Indian J Radiol Imaging. 2015;25(1):2. doi:10.4103/0971-3026.150105
4. Bae KT. Intravenous contrast medium administration and scan timing at CT: considerations and approaches. Radiology. 2010;256(1):32–61. doi:10.1148/radiol.10090908
5. Ma X, Singh A, Fay J, Boland G, Sahani DV. Comparison of dual-syringe and syringeless power injectors in outpatient MDCT practice: impact on the operator’s performance, CT workflow, and operation cost. J Am Coll Radiol. 2012;9(8):578–582. doi:10.1016/j.jacr.2012.04.007
6. Colombo GL, Andreis IA, Di Matteo S, Bruno GM, Mondellini C. Syringeless power injector versus dual-syringe power injector: economic evaluation of user performance, the impact on contrast enhanced computed tomography (CECT) workflow exams, and hospital costs. Med Devices. 2013;6:169.
7. Buerke B, Puesken M, Mellmann A, et al. Automatic MDCT injectors: hygiene and efficiency of disposable, prefilled, and multidosing roller pump systems in clinical routine. Am J Roentgenol. 2011;197(2):W226–32. doi:10.2214/AJR.10.5924
8. McDermott M, Kemper C, Barone W, Jost G, Endrikat J. Impact of CT injector technology and contrast media viscosity on vascular enhancement: evaluation in a circulation phantom. Br J Radiol. 2020;93(1109):20190868. doi:10.1259/bjr.20190868
9. Chaya A, Jost G, Endrikat J. Piston-based vs peristaltic pump-based CT injector systems. Radiol Technol. 2019;90(4):344–352.
10. Hansmann J, Fink C, Jost G, Pietsch H, Meyer M, Nance JJW. Impact of iodine delivery rate with varying flow rates on image quality in dual-energy CT of patients with suspected pulmonary embolism. Acad Radiol. 2013;20(8):962–971. doi:10.1016/j.acra.2013.02.013
11. Chaturvedi A, Oppenheimer D, Rajiah P, Kaproth-Joslin KA, Chaturvedi A. Contrast opacification on thoracic CT angiography: challenges and solutions. Insights Imaging. 2017;8(1):127–140. doi:10.1007/s13244-016-0524-3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.