Back to Journals » Clinical Ophthalmology » Volume 19
Perforating Scleral Vessels and Their Influence on Myopic Macular Neovascularization
Authors Coelho-Costa I ![]() , Gama-Castro A, Ferreira AM
, Gama-Castro A, Ferreira AM ![]() , Teixeira-Martins R
, Teixeira-Martins R ![]() , Marques-Couto P
, Marques-Couto P ![]() , Rodrigues R, Pedrosa AC, Laiginhas R, Rocha-Sousa A
, Rodrigues R, Pedrosa AC, Laiginhas R, Rocha-Sousa A ![]() , Falcão M, Carneiro Â
, Falcão M, Carneiro Â
Received 7 July 2025
Accepted for publication 5 September 2025
Published 25 October 2025 Volume 2025:19 Pages 3941—3947
DOI https://doi.org/10.2147/OPTH.S552038
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Inês Coelho-Costa,1 Ana Gama-Castro,1 Ana Margarida Ferreira,1 Rita Teixeira-Martins,1 Pedro Marques-Couto,1 Rita Rodrigues,1 Ana Catarina Pedrosa,1,2 Rita Laiginhas,1,2 Amândio Rocha-Sousa,1,2 Manuel Falcão,1,2 Ângela Carneiro1,2
1Ophthalmology Department, Unidade Local de Saúde São João, Porto, Portugal; 2RISE-Health, Surgery and Physiology Department, Faculty of Medicine, University of Porto, Porto, 4200-450, Portugal
Correspondence: Inês Coelho-Costa, Ophthalmology Department, Unidade Local de Saúde São João, Alameda Prof. Hernâni Monteiro, Porto, 4200-319, Portugal, Tel +351 918 590 111, Email [email protected]
Purpose: To evaluate the relationship between the presence and spatial relationship of perforating scleral vessels (PSVs) to the neovascular membrane, as seen on spectral-domain optical coherence tomography (SD-OCT), in eyes with myopic macular neovascularization (mMNV), and their association with clinical, anatomical, and treatment-related features.
Methods: This retrospective case series included patients from the Portuguese Retina Study Group registry (Retina.com.pt) with a diagnosis of mMNV and active follow-up at ULS-SJ. Clinical data were collected and SD-OCT macular scans reviewed to determine PSV presence and spatial relation to the neovascular membrane.
Results: We analyzed 100 eyes from 83 patients. PSVs were identified in 69 eyes (69%), and in 47 of these (68%), they were in direct contact with the neovascular membrane. PSV presence was significantly associated with older age (p = 0.019, Cohen’s d = – 0.57), thinner choroid (p < 0.001, r = – 0.34), and greater macular thickness at diagnosis (p = 0.009, Cohen’s d = – 0.58). It was also associated with a higher likelihood of anti-VEGF treatment switch (OR = 7.44, p = 0.022), but not with recurrence (OR = 1.30, p = 0.806), injection frequency (p = 0.258), or change in visual acuity (p = 0.093, r = 0.17). PSV-lesion contact was associated with older age (mean: 60.9 vs 49.8 years, p < 0.001, Cohen’s d = 0.83) and thinner choroid (mean rank: 39.98 vs 56.02, p = 0.005, r = 0.29).
Conclusion: PSVs were frequently observed in eyes with mMNV and were associated with older age, thinner choroid, and greater macular thickness at baseline, as well as a higher likelihood of requiring treatment switch. However, neither their presence nor lesion contact independently predicted a worse disease course or functional outcome.
Keywords: retinal neovascularization, optical coherence tomography, choroidal neovascularization, myopia, degenerative
Introduction
Myopia stands as the most prevalent refractive error globally and remains a primary contributor to visual impairment.1 Notably, the prevalence of myopia continues to escalate, and it is anticipated that by 2050, the global population with myopia will soar to 4,758 million, with 938 million individuals affected by high myopia.2
High myopia (defined as a spherical equivalent refractive error of ≤ −6.00 diopters (D) when ocular accommodation is relaxed)3 places patients at an increased risk of developing pathologic myopia (PM). PM is characterized by a progressive axial elongation of the eyeball with various characteristic changes in the macula, peripheral retina, and optic nerve that may lead to irreversible blindness.4,5 Among the macular changes (termed myopic macular degeneration or myopic maculopathy) observed in PM, myopic macular neovascularization (mMNV) denotes a major complication often causing sudden, progressive, and potentially irreversible, loss of central vision when not promptly treated.6,7 It is estimated that up to 11% of individuals with PM will develop mMNV,8 and, notably, 35% of these will develop bilateral disease within eight years.9 While the term “myopic choroidal neovascularization” (mCNV) remains widely used in the literature, we adopt the term “myopic macular neovascularization” throughout this study to reflect the uncertain vascular origin of these lesions, particularly in eyes with extreme choroidal thinning or atrophy. Although no formal nomenclature revision currently exists for myopia-associated neovascularization, this terminology is conceptually aligned with recent updates in neovascular AMD classification, which similarly abandoned the term “choroidal” in favor of anatomically neutral descriptors.10
Numerous factors have been found to be more common in PM eyes that develop mMNV. These include the presence of lacquer cracks, chorioretinal atrophy, a greater posterior staphyloma height, a thinner choroid, and a higher aqueous humor level of vascular endothelial growth factor (VEGF) and interleukin-8 (IL-8)9,11. Nonetheless, the exact pathophysiology of mMNV remains uncertain, but the origin of these neovascular vessels has long been believed to be from the choroidal vasculature, even though the choroid is extremely thin in these eyes.12,13
High myopes have inherently thin posterior pole structures, which allow for deeper penetration of optical coherence tomography (OCT) signal and improved visualization of posterior structures like the choroid, sclera, and deep scleral vessels.13 Perforating scleral vessels (PSVs) are an OCT imaging finding most commonly observed in eyes with pathologic myopia. They appear as vertically oriented, hyporeflective linear structures that traverse the sclera and extend toward the choroid. They are mainly see in areas of advanced choroidal and RPE thinning, where these deeper structures become more readily visible.14–16 Although their precise anatomical identity remains uncertain, PSVs have been hypothesized to correspond to short posterior ciliary arteries (SPCAs) or their branches with an altered distribution at the edge of the posterior staphyloma, and made visible by scleral thinning and axial elongation in myopic eyes.12,14–16 However, other authors have proposed that these vessels may represent intrascleral vascular remnants or non-SPCA channels exposed by advanced choroidal atrophy and scleral remodeling, particularly in highly myopic eyes.16
Several publications have reported on the presence of PSVs in proximity to neovascular membranes in highly myopic patients, suggesting the possibility that mMNVs can be related to these vessels given the almost “absent” choroid in many cases.12,17–20 It has been proposed that PSVs in proximity to neovascular lesions may exacerbate the microenvironment conducive to neovascularization and influence the activity of these abnormal blood vessels and their response to treatment, although results have been inconsistent.12,17,18,20,21 The anatomical and clinical relevance of PSVs in the context of mMNV remains poorly defined, and it is still unclear whether their presence or lesion contact influences disease activity or treatment response. In particular, the need for anti-VEGF treatment switching often prompted by suboptimal therapeutic response, may represent a clinically meaningful indicator of lesion behavior, yet its potential association with PSV characteristics has not been thoroughly investigated.
The aim of this study was to characterize the relationship between the presence of PSVs on spectral domain OCT (SD-OCT) in a population of patients with mMNV, namely, their spatial relation to the lesion, their influence on disease course, response to treatment with anti-VEGF intravitreal injections (IVIs) and their impact on visual acuity.
Methods
This retrospective observational study was conducted at Unidade Local de Saúde de São João (ULS-SJ), Porto, Portugal. Inclusion criteria comprised all patients registered in the Portuguese National Retina Study Group registry, retina.pt (https://retina.com.pt), with a diagnosis of mMNV (defined as macular neovascularization in eyes with pathologic myopia) in at least one eye and with active follow-up at the time of data collection. The retina.pt dataset began collecting data at ULS-SJ in 2017 and includes both newly diagnosed patients and historical cases who initiated follow-up at our institution prior to 2017 but remain under active surveillance. All patients included in the retina.pt registry provided written informed consent at the time of enrollment. The study adhered to the tenets of the Declaration of Helsinki. All data was anonymized and handled in accordance with data protection regulations to ensure patient confidentiality.
Patients’ electronic hospital records were reviewed to collect data on age, sex, refractive error, best corrected visual acuity (BCVA) measured with the Early Treatment of Diabetic Retinopathy Study (ETDRS) scale at diagnosis and at the time of the final available follow-up visit, number of follow-up months, number of appointments, and whether disease reactivation occurred. Reactivation was defined as the need to restart anti-VEGF treatment following a period of suspension due to disease inactivation of at least 6 months. Data regarding the total number of intravitreal injections and the anti-VEGF agents administered were also extracted.
Spectralis SD-OCT (Heidelberg Engineering, Heidelberg, Germany) macular scans were reviewed at the time of diagnosis to assess the presence or absence of perforating scleral vessels (PSV) and their location relative to the neovascular membrane (NM). Neovascular membranes were identified on diagnostic scans as hyperreflective material in the subretinal space or in the outer nuclear layer, typically located above the retinal pigment epithelium band.21 PSVs were defined as hyporeflective linear structures extending through the sclera to the choroid14 (Figure 1). The relative position of the PSV and the neovascular membrane was also recorded. PSVs were considered in contact with the neovascular membrane if they terminated directly beneath the hyperreflective material on OCT. Two of the authors (I.C.-C. and A. G.-C.) independently evaluated the presence of PSV in the macular region and its association with mMNV. In cases of uncertainty, assessments were discussed with a senior reviewer (A.C) to reach consensus. Central macular retinal and choroidal thickness were measured in the same OCT scans at diagnosis and the last follow-up.
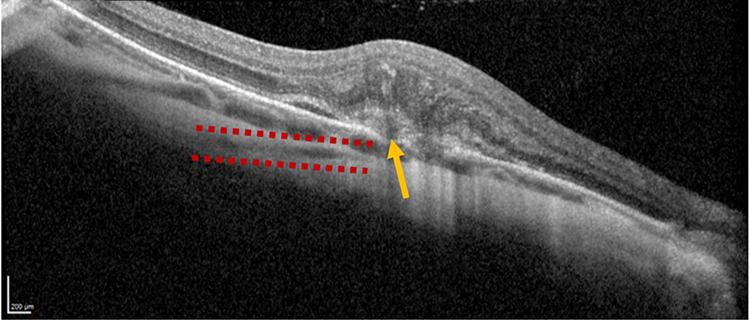 |
Figure 1 A macular SD-OCT scan of one of the patients included in the study with a PSV in contact with the neovascular membrane. The red dotted line delimitates the PSV that traverses the sclera and ends at the level of the choroid, just below the neovascular membrane (yellow arrow). |
All statistical analyses were conducted using IBM SPSS Statistics, version 29.0 (IBM Corp., Armonk, NY, USA). A two-tailed p-value < 0.05 was considered statistically significant. Normality of continuous variables was assessed using the Kolmogorov–Smirnov test along with visual inspection of histograms and Q-Q plots. Descriptive statistics were reported as mean ± standard deviation (SD) for normally distributed variables, and as median and interquartile range (IQR) otherwise. Categorical variables were presented as frequencies and percentages. Group comparisons were performed using the Mann–Whitney U-test or Kruskal–Wallis test for continuous variables and the chi-square test for categorical variables. Associations between PSV presence or location and treatment outcomes were further assessed using ordinal logistic regression, adjusting for follow-up duration. Model fit and assumptions (eg, proportional odds) were verified using appropriate diagnostics. Effect sizes (Cohen’s d for normally distributed continuous variables, r for non-parametric comparisons, and odds ratios [OR] for logistic regression) were reported to convey the magnitude of associations. There were no missing data for the variables included in the analyses.
Results
Sample Characteristics
Our study included 100 eyes from 83 patients diagnosed with mMNV, with bilateral involvement in 17% of cases. Most patients were female (n = 73, 88%). We detected perforating scleral vessels in 69 eyes (69%); in 68% of these (n = 47), the vessel was directly beneath the neovascular lesion.
Patients attended a median of 9 hospital appointments (IQR: 5–24) over a follow-up period of 54.2 months (IQR: 17.8–101.9). Patients received a median of 8 anti-VEGF injections (IQR: 4–17) over the course of follow-up, corresponding to a median of 2.93 IVIs per year (IQR: 1.03–6.42). Bevacizumab (Avastin®) was the most frequently administered agent, used in 93% of eyes, followed by aflibercept (Eylea®) in 17% and ranibizumab (Lucentis®) in 10%. This distribution reflects the treatment protocol in place at ULS-SJ, where bevacizumab is used as the first-line agent for most cases. Most eyes (77%) were treated with a single anti-VEGF agent, while 17% received two agents and 3% received all three. Disease recurrence occurred in 26% of eyes during follow-up and is further explored in relation to anatomical and treatment variables in the subsequent section. Visual acuity improved over the course of follow-up, with a median BCVA gain of +5 ETDRS letters (IQR: –3.5 to +19.8). Additional baseline anatomical and functional characteristics are summarized in Table 1.
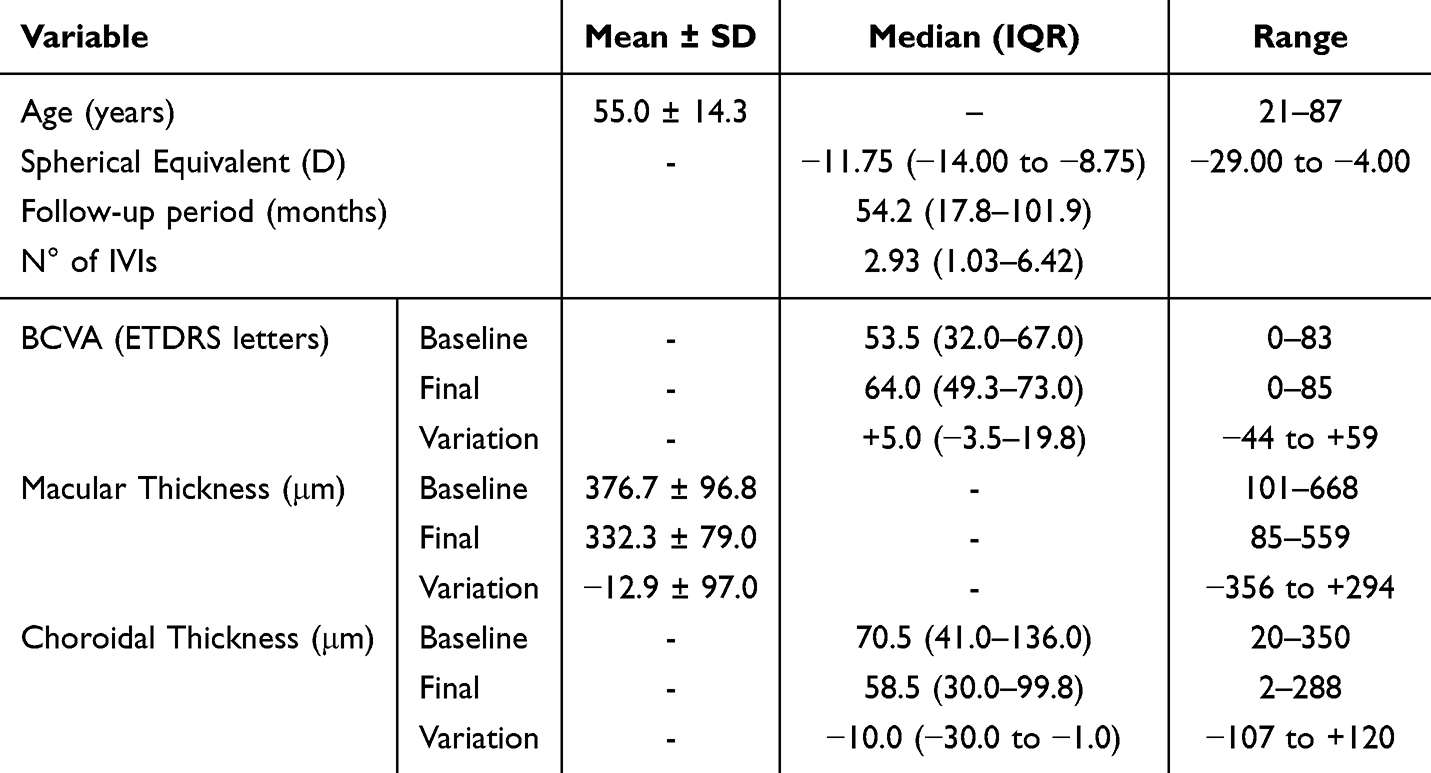 |
Table 1 Descriptive Characteristics of the Study Sample. Values are Reported as Mean ± SD or Median (IQR), as Appropriate. Ranges Indicate Minimum and Maximum Values |
Associations Between Anatomical Features and Disease Activity
Patients with PSVs were significantly older than those without (p = 0.019, Cohen’s d = –0.57), and this association was even stronger when the PSV was in direct contact with the neovascular lesion (p < 0.001, Cohen’s d = 0.83). Eyes with PSVs had significantly greater baseline macular thickness (p = 0.009, Cohen’s d = –0.58) and thinner baseline choroidal thickness (p < 0.001, r = –0.34) compared to those without. Similarly, when the PSV was in direct contact with the neovascular membrane, baseline choroidal thickness was also significantly reduced (p = 0.005, r = 0.34). No significant differences were observed in the variation of macular or choroidal thickness during follow-up.
Regarding the impact of PSV presence on clinical outcomes, PSVs were significantly associated with the need for treatment switch due to suboptimal response (p = 0.022; OR = 7.44, 95% CI: 1.33–41.5), independent of follow-up duration. This association was confirmed by ordinal logistic regression, which demonstrated satisfactory model fit (p = 0.008). Longer follow-up time was also significantly associated with higher recurrence rates (p < 0.001), whereas PSV presence (p = 0.289) and PSV-lesion contact (p = 0.150) were not. Visual acuity variation during follow-up did not differ significantly based on PSV presence (p = 0.093, r = 0.17) or lesion contact (p = 0.201, r = –0.13). Similarly, no significant differences were found in the number of intravitreal injections per year between eyes with or without PSVs (p = 0.873, r = –0.06) or based on PSV-lesion contact (p = 0.550, r = –0.06).
Additional comparisons between anatomical or demographic variables and PSV presence or location are summarized in Table 2.
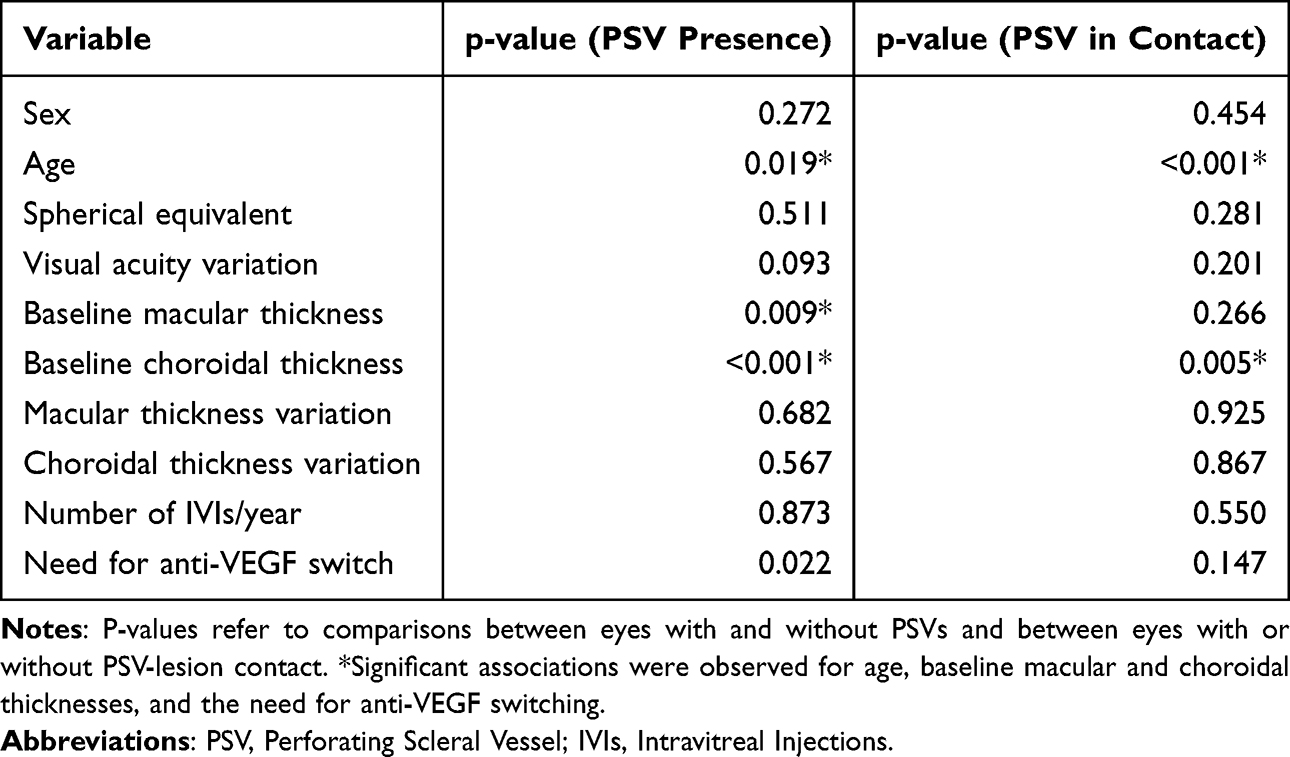 |
Table 2 Associations Between the Presence of PSVs and PSVs in Contact with the Neovascular Membrane on OCT and Clinical or Anatomical Variables |
Discussion
This retrospective study, including 100 eyes from 83 patients, demonstrated that the presence of PSVs in eyes with mMNV was significantly associated with older age, distinct baseline choroidal and macular anatomical features, and a higher likelihood of anti-VEGF treatment switch, but not with disease reactivation, visual acuity outcomes, or injection frequency during follow-up.
The demographic and clinical characteristics of our sample are in line with those reported in previous studies of mMNV. The mean age was 55 years, comparable to that described in other cohorts,8,12,17,18,20–22 and there was a predominance of female patients (88%). Female predominance in patients with mMNV has been consistently reported17, believed to be influenced by hormonal factors, including estrogen receptor expression within neovascular tissue.19 Bilateral disease was found in 17% of our sample, slightly lower than reported in other series with mMNV patients.9,22,23
PSVs were identified in 69% of eyes in our cohort, consistent with previously reported rates ranging from 69% to 94%.12,17,18,20,21 In our analysis, PSV presence was found to have a statistically significant association with older age, a finding that contrasts with previous reports by Giuffrè et al20 and Ruiz-Medrano et al,24 who observed no such correlation.
Eyes with PSVs demonstrated significantly greater baseline macular thickness and thinner choroidal thickness. Ruiz-Medrano et al24 and, more recently, She et al,22 also reported significantly thinner choroids in eyes with PSVs compared to those without. Although the observed difference may partly be explained by improved OCT signal penetration in eyes with thinner choroids, making scleral vessels easier to visualize, it has been proposed that choroidal thinning reflects an advanced stage of high myopia characterized by biomechanical fragility and altered perfusion, which may facilitate the protrusion of PSVs through Bruch’s membrane and contribute to neovascular membrane formation. In this series, eyes where PSVs were located in direct contact with the neovascular lesion also exhibited significantly thinner choroid, although no additional differences were found in macular thickness.
Baseline macular thickness was measured at the time of mMNV diagnosis, which likely accounts for the increased thickness due to the presence of the neovascular membrane and, in some cases, associated exudation. The observed association between PSVs and greater baseline macular thickness has not been previously reported and may suggest that these vessels are more frequently visualized in eyes with more prominent or active lesions at presentation.
In our cohort, the presence of PSVs was also significantly associated with a higher likelihood of anti-VEGF treatment drug switch. This association has not been widely explored in previous studies, although Yao et al16 reported that eyes with PSVs adjacent to mMNV tended to show less reduction in central macular thickness during follow-up. While their findings did not reach statistical significance, the authors interpreted this trend as indicative of a suboptimal anatomical response. In our study, the lack of association between PSVs and either injection frequency or disease recurrence suggests that treatment switches may have been prompted by limited early anatomical improvement rather than by increased lesion activity. Notably, the routine use of bevacizumab as a first-line agent at our center may have contributed to the initial suboptimal response observed in some cases, given its potentially lower efficacy in certain neovascular profiles. These observations raise the possibility that the presence of PSVs may be a marker of a neovascular phenotype with altered response to first-line anti-VEGF therapy, potentially prompting earlier treatment modification. The lack of increased recurrence or injection burden reinforces this interpretation, supporting the idea that switching may have reflected early structural non-response rather than heightened lesion aggressiveness.
The presence of PSVs was not associated with better or worse visual acuity outcomes during follow-up. This contrasts with the findings of Giuffrè et al20 and She et al,22 who reported significantly worse final BCVA in eyes with PSVs, suggesting a possible link between these vessels and poorer functional prognosis. However, other studies, like in our case, including Ruiz-Medrano et al23 and Yao et al,16 did not observe a statistically significant difference in visual outcomes based on PSV presence. The absence of an association in our cohort may reflect effective control of lesion activity with anti-VEGF therapy across groups or differences in follow-up duration, baseline lesion characteristics, or visual acuity measurement timepoints. These findings highlight the inconsistency in the current literature regarding the functional relevance of PSVs.
PSV-lesion contact was only significantly associated with thinner choroid and older age, similarly to PSV presence regardless of contact. Beyond this, lesion contact was not linked to differences in recurrence, visual acuity, or treatment intensity (Table 2), suggesting that contact alone may not indicate a more aggressive lesion profile. Similarly, Ruiz-Medrano et al24 and She et al22 also reported that PSV-lesion contact did not influence recurrence rates, treatment burden, or visual outcomes, supporting the idea that contact alone may not signal a more aggressive lesion.
This study has several limitations inherent to its single center retrospective design, including potential selection and documentation bias and the absence of standardized treatment protocols or imaging intervals. Because of the study’s retrospective nature, the identification of PSVs relied exclusively on structural OCT, as additional imaging modalities such as OCT angiography or indocyanine green angiography were not systematically performed and were therefore unavailable for most patients. This limited the ability to perform detailed vascular characterization and flow assessment, which could have enhanced the anatomical interpretation of PSVs. The absence of a control group of highly myopic eyes without neovascularization also limits our ability to determine whether PSVs are specifically associated with the development or risk of mMNV or simply reflect advanced myopic macular degeneration. Additionally, from a methodological perspective, the absence of correction for multiple comparisons may increase the risk of type I error in interpreting some associations. Although this was an exploratory analysis, we acknowledge this limitation and encourage cautious interpretation of p-values. While the sample size and extended follow-up strengthen the clinical relevance of our findings, further prospective studies using high-resolution, multimodal imaging and standardized outcome metrics are needed to validate the role of PSVs as biomarkers in myopic macular neovascularization.
Conclusions
Our findings suggest that while perforating scleral vessels were frequently observed in our study cohort in eyes with mMNV and were associated with distinct anatomical features and a higher likelihood of treatment modification, their presence and proximity to lesions did not independently predict worse visual or anatomical outcomes. These results challenge the assumption that PSVs signal a more aggressive neovascular phenotype, highlighting the complexity of interpreting structural findings in pathologic myopia. Clinically, PSV presence alone should not prompt intensified treatment or follow-up, although it may warrant closer anatomical monitoring in the early treatment phase, particularly when using bevacizumab as first-line therapy. As this was a retrospective, single-center study based on structural OCT alone, further prospective research with standardized treatment protocols and multimodal imaging is warranted to clarify the prognostic and therapeutic relevance of PSVs in mMNV.
Ethics Approval and Informed Consent
The retina.pt registry has received prior approval from national ethics committees and complies with Portuguese data protection regulations. For this retrospective study, additional ethical approval was waived by the Ethics Committee of ULS São João as the study involved fully anonymized data extracted from a pre-approved national registry. No patient-identifiable information was accessed or recorded.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, or publication of this article, and no sponsor was involved in any stage of the study.
Disclosure
The authors declare that they have no financial or non-financial competing interests related to the content of this manuscript.
References
1. Morgan IG, Ohno-Matsui K, Saw SM. Myopia. Lancet. 2012;379(9827):1739–1748. doi:10.1016/S0140-6736(12)60272-4
2. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036–1042. doi:10.1016/j.ophtha.2016.01.006
3. Flitcroft DI, He M, Jonas JB, et al. IMI – defining and classifying myopia: a proposed set of standards for clinical and epidemiologic studies. Invest Ophthalmol Vis Sci. 2019;60(3):M20. doi:10.1167/iovs.18-25957
4. Ohno-Matsui K. What is the fundamental nature of pathologic myopia? Retina. 2017;37(6):1043–1048. doi:10.1097/IAE.0000000000001348
5. Wong YL, Saw SM. Epidemiology of pathologic myopia in Asia and Worldwide. Asia-Pac J Ophthalmol. 2016;5(6):394–402. doi:10.1097/APO.0000000000000234
6. Ruiz-Medrano J, Montero JA, Flores-Moreno I, Arias L, García-Layana A, Ruiz-Moreno JM. Myopic maculopathy: current status and proposal for a new classification and grading system (ATN). Prog Retinal Eye Res. 2019;69:80–115. doi:10.1016/j.preteyeres.2018.10.005
7. Hotchkiss ML, Fine LS. Pathologic myopia and choroidal neovascularization. Am J Ophthalmol. 1981;91(2):177–183. doi:10.1016/0002-9394(81)90170-7
8. Wong TY, Ferreira A, Hughes R, Carter G, Mitchell P. Epidemiology and disease burden of pathologic myopia and myopic choroidal neovascularization: an evidence-based systematic review. Am J Ophthalmol. 2014;157(1):9–25.e12. doi:10.1016/j.ajo.2013.08.010
9. Ohno-Matsui K. Patchy atrophy and lacquer cracks predispose to the development of choroidal neovascularisation in pathological myopia. Br J Ophthalmol. 2003;87(5):570–573. doi:10.1136/bjo.87.5.570
10. Spaide RF, Jaffe GJ, Sarraf D, et al. Consensus nomenclature for reporting neovascular age-related macular degeneration data. Ophthalmology. 2020;127(5):616–636. doi:10.1016/j.ophtha.2019.11.004
11. Zhang XJ, Chen XN, Tang FY, et al. Pathogenesis of myopic choroidal neovascularization: a systematic review and meta-analysis. Surv Ophthalmol. 2023;68(6):1011–1026. doi:10.1016/j.survophthal.2023.07.006
12. Ishida T, Watanabe T, Yokoi T, Shinohara K, Ohno-Matsui K. Possible connection of short posterior ciliary arteries to choroidal neovascularisations in eyes with pathologic myopia. Br J Ophthalmol. 2019;103(4):457–462. doi:10.1136/bjophthalmol-2018-312015
13. Ohno-Matsui K, Akiba M, Modegi T, et al. Association between shape of sclera and myopic retinochoroidal lesions in patients with pathologic myopia. Invest Ophthalmol Vis Sci. 2012;53(10):6046. doi:10.1167/iovs.12-10161
14. Ohno-Matsui K, Akiba M, Ishibashi T, Moriyama M. Observations of vascular structures within and posterior to sclera in eyes with pathologic myopia by swept-source optical coherence tomography. Invest Ophthalmol Vis Sci. 2012;53(11):7290. doi:10.1167/iovs.12-10371
15. Rothenbuehler SP, Maloca P, Scholl HPN, et al. Three-dimensional analysis of submacular perforating scleral vessels by enhanced depth imaging optical coherence tomography. Retina. 2018;38(6):1231–1237. doi:10.1097/IAE.0000000000001686
16. Yao W, Xu J, She X, et al. Perforating scleral vessels adjacent to myopic choroidal neovascularization achieved a poor outcome after intravitreal anti-VEGF therapy. Front Med. 2022;9:1065397. doi:10.3389/fmed.2022.1065397
17. Hayashi K, Ohno-Matsui K, Yoshida T, et al. Characteristics of patients with a favorable natural course of myopic choroidal neovascularization. Graefe’s Arch Clin Exp Ophthalmol. 2005;243(1):13–19. doi:10.1007/s00417-004-0960-5
18. Yoshida T, Ohno-Matsui K, Yasuzumi K, et al. Myopic choroidal neovascularization. Ophthalmology. 2003;110(7):1297–1305. doi:10.1016/s0161-6420(03)00461-5
19. Kobayashi K, Mandai M, Suzuma I, Kobayashi H, Okinami S. Expression of estrogen receptor in the choroidal neovascular membranes in highly myopic eyes. Retina. 2002;22(4):418–422. doi:10.1097/00006982-200208000-00004
20. Giuffrè C, Querques L, Carnevali A, De Vitis LA, Bandello F, Querques G. Choroidal neovascularization and coincident perforating scleral vessels in pathologic myopia. Eur J Ophthalmol. 2017;27(2):e39–e45. doi:10.5301/ejo.5000875
21. Lai TYY, Cheung CMG. Myopic choroidal neovascularization: diagnosis and Treatment. Retina. 2016;36(9):1614–1621. doi:10.1097/IAE.0000000000001227
22. She X, Yao W, Huang G, et al. Myopic choroidal neovascularization with neovascular signal around perforating scleral vessel prone to recur after anti-VEGF therapy. Eye Vis. 2024;11(1):6. doi:10.1186/s40662-024-00374-5
23. Akada M, Miyake M, Hata M, et al. Incidence and clinical practice of myopic macular neovascularization: a nationwide population-based cohort study. Ophthalmol Sci.. 2025;5(6):100834. doi:10.1016/j.xops.2025.100834
24. Ruiz-Medrano J, Almazan-Alonso E, Flores-Moreno I, Puertas M, García-Zamora M, Ruiz-Moreno JM. Relationship between myopic choroidal neovascularization activity and perforating scleral vessels in high myopia. Retina. 2022;42(1):204–209. doi:10.1097/IAE.0000000000003290
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Understanding Posterior Staphyloma in Pathologic Myopia: Current Overview, New Input, and Perspectives
Ehongo A
Clinical Ophthalmology 2023, 17:3825-3853
Published Date: 12 December 2023