Back to Journals » Clinical Ophthalmology » Volume 20
Perfluorodecalin and Viscoelastic-Assisted Internal Limiting Membrane Flap Technique for High Myopia Macular Hole Retinal Detachment
Received 29 December 2025
Accepted for publication 26 March 2026
Published 2 April 2026 Volume 2026:20 592451
DOI https://doi.org/10.2147/OPTH.S592451
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yousef Fouad
Junwen He,1 Li Yan,1 Shan Wang2
1Department of Retinal & Vitreous Diseases, Aier Eye Hospital of Wuhan University, Wuhan, People’s Republic of China; 2Department of Ophthalmic Imaging, Aier Eye Hospital of Wuhan University, Wuhan, People’s Republic of China
Correspondence: Shan Wang, Department of Ophthalmic Imaging, Aier Eye Hospital of Wuhan University, Wuhan, People’s Republic of China, Email [email protected] Li Yan, Department of Retinal & Vitreous Diseases, Aier Eye Hospital of Wuhan University, Wuhan, People’s Republic of China, Email [email protected]
Purpose: To evaluate the feasibility and outcomes of a novel surgical technique using a sub-perfluorodecalin (PFD, RT DECALIN) injection of ophthalmic viscosurgical device (OVD) to stabilize inverted internal limiting membrane (ILM) flaps for the treatment of macular hole retinal detachment (MHRD) in highly myopic eyes. This technique addresses the challenges of ILM flap displacement and stability.
Patients and Methods: This retrospective, interventional case series included seven eyes of seven patients with MHRD who underwent surgery using sub-PFD injection of OVD to stabilize inverted ILM flaps. Pre- and postoperative best-corrected visual acuity (BCVA) was compared using the Wilcoxon signed-rank test. Ethical approval was obtained, and all patients provided informed consent. Fundus color photography and optical coherence tomography (OCT) were used to assess anatomical outcomes.
Results: The study included seven eyes of seven patients (mean age: 61.86± 4.30 years; follow-up: 6 months). All eyes achieved successful macular hole closure, with near-normal foveal contour observed in five (71.43%) eyes at the final follow-up. BCVA improved significantly from 2.03± 0.38 logMAR to 1.20± 0.54 logMAR (P = 0.0024). No intraoperative or postoperative complications were observed.
Conclusion: Sub-PFD injection of OVD for stabilization of the inverted ILM flap was feasible and was associated with favorable short-term anatomical outcomes in highly myopic eyes with MHRD. Improvement in BCVA was also observed during follow-up. This innovative approach offers a promising solution to the challenges associated with MHRD in highly myopic eyes.
Keywords: MHRD, optical coherence tomography, anatomical closure, pathologic myopia
Introduction
Macular hole retinal detachment (MHRD) is a vision-threatening condition predominantly affecting patients with high myopia (HM), characterized by a full-thickness macular defect with associated retinal detachment.1 This disease is characterized by a full-thickness retinal defect at the macular center accompanied by retinal detachment, representing a typical manifestation of pathological changes in HM.2 In HM, the marked elongation of the axial length leads to anatomical and functional alterations, including progressive retinal thinning, reduced choroidal blood circulation, vitreous degeneration, and the development of posterior staphyloma.3 These pathological factors render the macular region in HM more susceptible to hole formation, which can progress to retinal detachment under vitreous traction or other mechanical forces. Without timely intervention, MHRD often results in irreversible vision loss and even blindness, severely impacting the patient’s quality of life. Therefore, effective treatment of MHRD and the improvement of postoperative visual outcomes are critical issues in both clinical and research domains.
Optical coherence tomography (OCT), one of the most widely used non-invasive ophthalmic imaging modalities in clinical practice,4 provides high-resolution tomographic images that clearly delineate structural abnormalities in the macular region. It is also instrumental in postoperative follow-up for dynamically assessing macular holes (MH) closure and retinal recovery.5 Concurrently, fundus photography serves as a fundamental imaging technique, documenting overall morphological changes in the fundus, such as MH, retinal detachment, and retinal pigment epithelium alterations.6 Best-corrected visual acuity (BCVA) is the most commonly used measure of visual function and is typically expressed as the logarithm of the minimum angle of resolution (logMAR), with lower logMAR values indicating better visual acuity.7
Pars plana vitrectomy (PPV) has become the standard surgical approach for treating MHRD. The primary objective of PPV is to promote retinal reattachment by removing the vitreous and relieving tractional forces. Additionally, fluid-air exchange (FAE) is often employed to replace intraocular fluid with air or other gases, facilitating retinal reattachment and creating a stable environment for subsequent retinal laser photocoagulation and tamponade with silicone oil or long-acting gases.2,8 However, the fragile nature of the retina in HM and the limited regenerative capacity of tissues around the hole often result in suboptimal closure rates and functional recovery with traditional methods. To address these limitations, the introduction of internal limiting membrane (ILM) manipulation techniques has significantly advanced the management of MHRD.9
The ILM, the innermost layer of the retina, plays a pivotal role in MHRD surgery. Its peeling or inversion effectively alleviates mechanical traction in the macular region, creating a more favorable environment for hole closure and tissue repair.10 Studies have shown that ILM inversion stabilizes the local microenvironment, reducing fluid accumulation around the hole and accelerating its healing.9 However, in HM patients, the elongated axial length and increased retinal curvature complicate vitreous traction dynamics, leading to a higher risk of postoperative ILM flap displacement and subsequent treatment failure.11 To enhance surgical precision, indocyanine green (ICG) is commonly used as an auxiliary dye in MHRD surgeries to facilitate the visualization and peeling of the ILM.12 Although ICG has potential retinal toxicity, its use in low concentrations and with rapid rinsing minimizes associated risks, making it a standard choice for ILM staining.13
Perfluorodecalin (PFD), a high-density liquid, assists in the removal of subretinal fluid (SRF) and reduces tension around the hole.14 Despite its advantages, PFD has limitations in complex cases, where ILM flaps may displace under external forces postoperatively, compromising MH closure. To address this, PFD is often combined with adhesives like silicone oil to mitigate symptoms such as retinal detachment.15 However, previously described adjunctive approaches in MH-related surgery have also included viscoelastic materials, autologous blood, and heavy liquids. In the present approach, PFD was primarily used to provide a stable intraoperative environment for ILM flap manipulation and to facilitate controlled SRF displacement, whereas ophthalmic viscosurgical device (OVD) was applied to enhance local adhesion and maintain flap apposition over the MH. Thus, the combination of PFD and OVD was intended to integrate the mechanical stabilizing effect of PFD with the adhesive property of OVD, rather than relying on either adjunct alone. Previous reports have described adjunctive strategies to improve ILM flap stabilization or macular hole coverage in complex macular hole surgery, including sub-perfluorocarbon viscoelastic-assisted flap manipulation, viscoelastic-supported ILM flap techniques, and autologous blood-assisted flap coverage. These approaches suggest that biomaterial or heavy-liquid adjuncts may help maintain flap position in technically challenging cases, although the specific sequence and intraoperative application of such maneuvers vary across studies. In this context, the present study evaluated a combined PFD- and OVD-assisted inverted ILM flap approach for MHRD in highly myopic eyes.16–18
This study aims to assess the feasibility and short-term outcomes of a modified ILM inversion technique combining PFD and OVD in MHRD surgery, focusing on its impact on MH closure rates and retinal reattachment. In addition, we explored the relationship between selected patient characteristics and postoperative outcomes.
Materials and Methods
This retrospective study included 7 eyes from 7 patients with HM who underwent MHRD surgery between May 2022 and March 2024 and met the study inclusion criteria, with a follow-up period of 6 months. All eyes underwent 23-gauge PPV, during which PFD was used to assist in creating inverted ILM flaps, stabilized with an injection of OVD under PFD. The study adhered to the Declaration of Helsinki and was approved by the Ethics Committee of Wuhan Aier Eye Hospital (Approval No.: 2021IRBLW01). Written informed consent was obtained from all participants.
Inclusion criteria included patients with high myopia (axial length ≥28 mm) diagnosed with MHRD involving the macular area. Exclusion criteria were prior retinal surgeries, significant ocular comorbidities, or systemic conditions potentially affecting the retina. Comprehensive ophthalmological examinations were performed preoperatively and postoperatively, including BCVA measured in logMAR units, color fundus photography, and OCT imaging. MHRD was classified based on the extent of retinal detachment. BCVA outcomes before and after surgery were compared using the Wilcoxon signed-rank test as a nonparametric paired analysis. Given the small sample size, the statistical results were interpreted descriptively and with caution. Statistical analyses were conducted using SPSS software (version 21.0; IBM, NY, USA).
Surgical Technique
This study employed 23-gauge pars plana vitrectomy, combined with ICG-assisted ILM staining, PFD tamponade, and inverted ILM flap techniques, to treat MHRD. During surgery, 1 mg/mL ICG (Daiichi, Tokyo, Japan), dissolved in 50% glucose solution, was injected into the macular area to stain the ILM (Figure 1A). Excess dye was aspirated, and most SRF was simultaneously removed (Figure 1B). PFD was then injected to cover the MH, ensuring the bubble edge extended slightly beyond the vascular arcades (Figure 1C). Under PFD tamponade, the ILM was peeled with microforceps and inverted to cover the MH (Figure 1D). Subsequently, 1 mL of OVD (17 mg/mL; Bausch & Lomb, NY, USA) was slowly injected using a sterile single-use 5 mL syringe fitted with a sterile single-use flat-tip irrigating needle (0.5 mm) to cover the surface of the inverted ILM flap (Figure 1E). The OVD was gradually injected under PFD to stabilize the ILM flap. In this procedure, the specific purpose of sub-PFD OVD injection was to maintain flap apposition over the MH during subsequent SRF drainage and FAE. After PFD placement and OVD injection, the SRF was gently displaced toward the peripheral margin of the detached retina, and posterior drainage retinotomy was performed in the peripheral retinal detachment area when needed (Figure 1F). In eyes in which the neurosensory retinal detachment was confined to the area near the vascular arcades, no additional drainage retinotomy was created; instead, the SRF was drained through the pre-existing MH using a soft-tip cannula before PFD and OVD injection. To further evacuate the SRF, FAE was performed in the retinal detachment area at the edge of the PFD bubble, and the remaining SRF was drained while the PFD was gradually removed (Figure 1G). The size and configuration of the ILM flap were determined intraoperatively according to the size and configuration of the MH, with the aim of achieving complete hole coverage and stable flap apposition. During FAE, residual SRF was aspirated through the retinotomy, and the PFD was completely removed (Figure 1H). The duration of intraoperative PFD exposure was not preset, but depended on the progress of each procedure and the time required to complete ILM flap manipulation, OVD stabilization, SRF displacement, and FAE. Care was taken to avoid visible retention of PFD at the end of the fluid-air exchange step. Because the ICG-stained ILM flap could be visually distinguished from the surrounding neurosensory retina devoid of ILM, its position could be monitored throughout FAE. Owing to the strong adhesiveness of the OVD and its immiscibility with PFD, the OVD remained concentrated over the surface of the inverted ILM flap rather than being washed away during FAE. During low-vacuum aspiration of PFD, the stained ILM flap remained stably apposed over the MH surface. In eyes with posterior staphyloma, before complete removal of PFD, the patient’s head position was slightly adjusted, without compromising the surgical view, to direct the residual PFD away from the ILM flap and OVD, thereby reducing the risk of flap displacement caused by the aspiration cannula. With these maneuvers, no obvious flap displacement was observed after FAE. At the conclusion of surgery, the inverted ILM flap was observed to be stably attached over the MH. Laser photocoagulation was applied around the retinotomy site, and silicone oil was used to tamponade the vitreous cavity (Figure 1I). Postoperatively, patients were instructed to maintain a prone position for 2 weeks and underwent silicone oil removal 3 months after surgery.
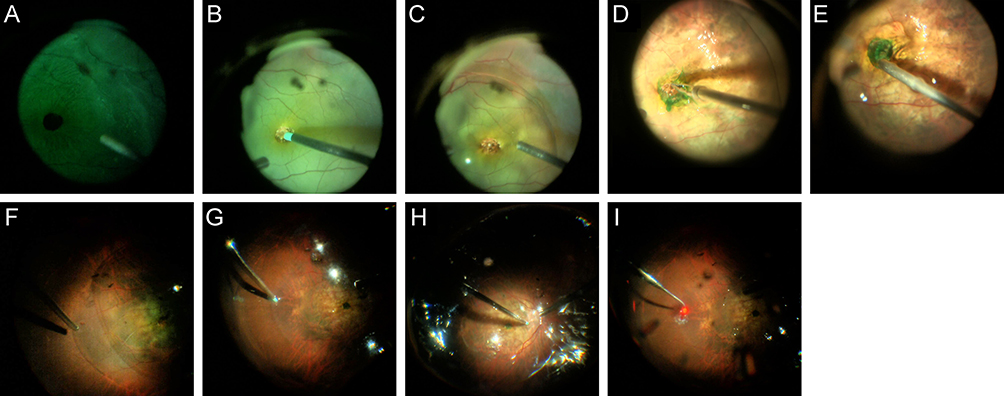 |
Figure 1 Surgical steps of treating MHRD using ICG, PFD, and OVD under FAE. (A) ICG dye was injected into the macular area to stain the ILM. (B) Excess ICG dye was aspirated along with most of the SRF to prepare the surgical field. (C) PFD was injected as a single bubble covering the macular hole, with its edges extending slightly beyond the vascular arcades. (D) The ILM was peeled circumferentially, approximately 4-disc diameters in size, using forceps under PFD tamponade. The peeled ILM layers were then inverted to cover the macular hole. (E) A small amount of OVD was injected under the PFD bubble to cover the inverted ILM flap. (F) The needle was carefully inserted under the PFD bubble, suspended above the ILM flap, and OVD was slowly injected to stabilize the flap over the macular hole. (G) Peripheral retinal detachment was addressed by performing small retinal incisions (approximately half-disc diameter) at the edge of the PFD bubble to drain any remaining SRF. (H) During FAE, the residual SRF was aspirated through the retinal incision site, and the PFD bubble was completely removed. (I) Laser photocoagulation was applied around the retinotomy site, and silicone oil was used to tamponade the vitreous cavity. |
Results
Baseline Clinical Characteristics of Patients
This study included 7 eyes from 7 patients with HM and MHRD, comprising 3 female patients (42.9%) and 4 male patients (57.1%). The age of female patients ranged from 56 to 65 years, with a mean age of 61.33 ± 4.73 years, while male patients ranged from 56 to 67 years, with a mean age of 62.25 ± 4.65 years. The overall mean age of all patients was 61.86 ± 4.30 years, with no significant difference between genders (P > 0.05). The axial lengths of the patients ranged from 28.48 mm to 32.11 mm, with a mean of 30.06 ± 1.31 mm. The mean axial length was 30.52 ± 1.55 mm in female patients and 29.71 ± 1.21 mm in male patients, with no significant difference between genders (P > 0.05). The baseline clinical characteristics of the patients are shown in Table 1.
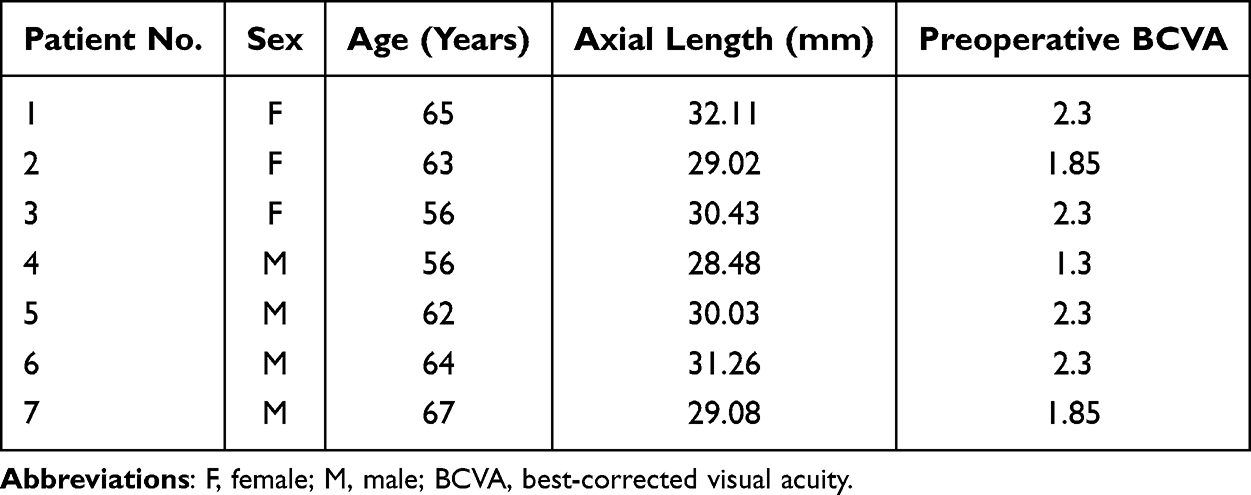 |
Table 1 Preoperative Clinical Characteristics of the Seven Eyes Included in This Study |
Preoperative Fundus Photography Findings
Preoperative fundus photography (Figure 2A–G) revealed round or oval-shaped MH in the central macula of MHRD eyes, with edges that were either smooth or slightly irregular. The macular holes were accompanied by a loss of macular reflex, and retinal detachment below the holes presented as localized retinal elevation or SRF accumulation, forming darkened areas. Retinal pigment epithelium in the macular hole region exhibited pigment loss or irregular proliferation. Additionally, as all patients had HM, fundus photography showed features such as lacquer cracks, choroidal atrophy, and posterior staphyloma. In some cases, cystoid edema presented as circular reflective regions, or retinal folds were observed due to posterior vitreous detachment. The presence of epiretinal membranes or peripheral retinal breaks was noted around the macular hole in some cases.
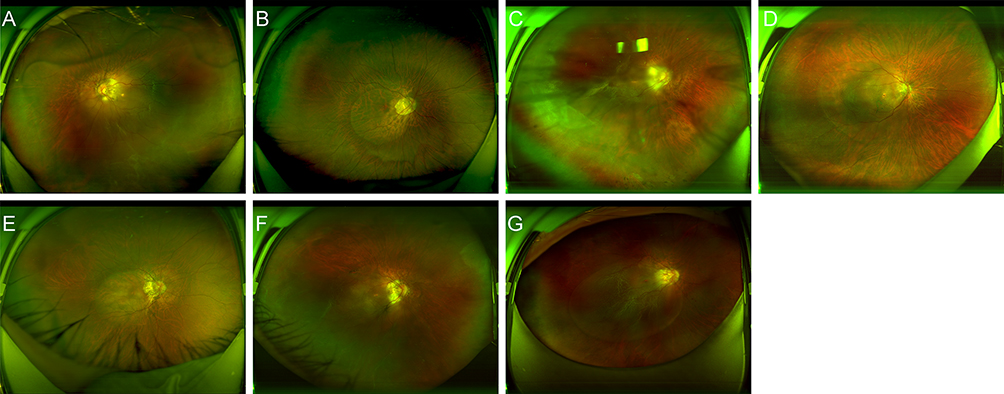 |
Figure 2 Preoperative fundus photographs of the seven eyes from the seven patients included in this study. (A–G) Correspond to Patients 1–7, respectively. |
Preoperative OCT Imaging Characteristics
Preoperative OCT images (Figure 3A–G) of MHRD eyes demonstrated full-thickness retinal defects in the central macula, with upturned or torn retinal edges. Some patients showed SRF accumulation at the base of the macular holes, appearing as dark, band-like low-reflective signals. The retinal layers surrounding the macular holes displayed cystic degeneration, characterized by hyper-reflective cystic cavities indicative of intraretinal fluid accumulation. The retinal neuroepithelium was significantly thinned in the macular hole region, with thickened retinal layers around the hole edges. In some cases, RPE deformation due to structural compression was observed in the hole region. These HM patients also exhibited arcuate changes due to posterior staphyloma, with retinal layer curvature and abnormal extension. Signs of vitreoretinal traction were observed in some cases, with high-reflective connections between the vitreous and retina, indicating the mechanical effect of the vitreous as a potential cause of hole formation and retinal detachment.
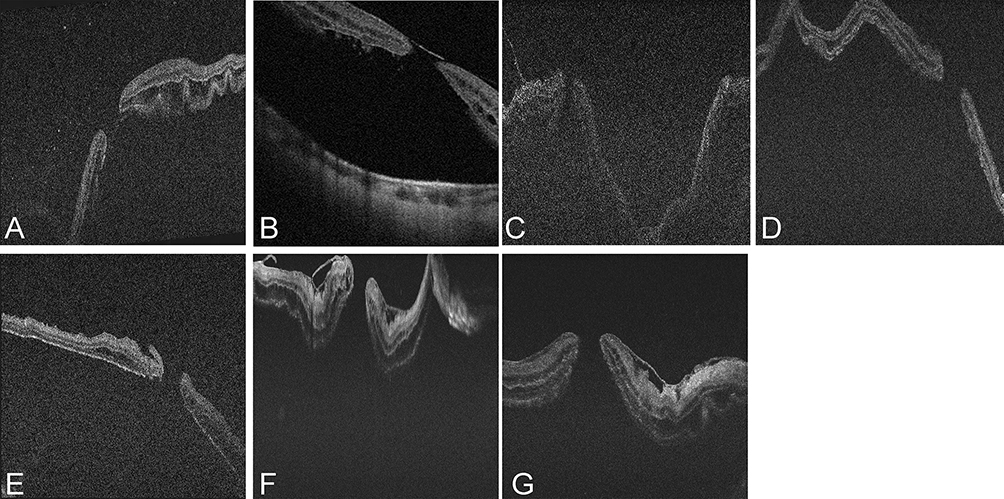 |
Figure 3 Preoperative OCT examinations of the seven eyes from the seven patients included in this study. (A–G) Correspond to Patients 1–7, respectively. |
Postoperative Anatomical and Functional Outcomes
Postoperatively, macular hole closure and complete retinal reattachment were achieved in all 7 eyes (100%) (Figure 4A–Figure 4G and Figure 5A–Figure 5G). No complications such as PFD entrapment within OVD or subretinal migration of PFD were observed during the injection of OVD under PFD. There were no cases of postoperative intraocular pressure abnormalities. OCT imaging demonstrated that 5 eyes (71.43%) achieved near-normal foveal contours at the final follow-up (Figure 5A, B, E–G). Meanwhile, one eye (14.29%) exhibited macular hole closure with a steep foveal contour (Figure 5C), and another eye (14.29%) showed an irregular foveal contour (Figure 5D). No cases showed ILM flaps sunken into the macular hole. Among the 5 eyes with near-normal foveal contours, one eye displayed a marginally displaced ILM flap (Figure 5G). All 7 eyes (100%) experienced an improvement in BCVA.
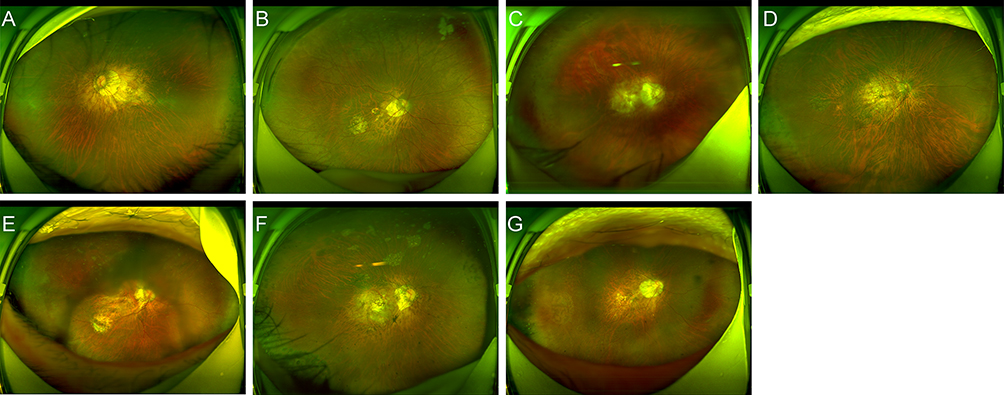 |
Figure 4 Postoperative fundus photographs of the seven eyes from the seven patients included in this study. (A–G) Correspond to Patients 1–7, respectively. |
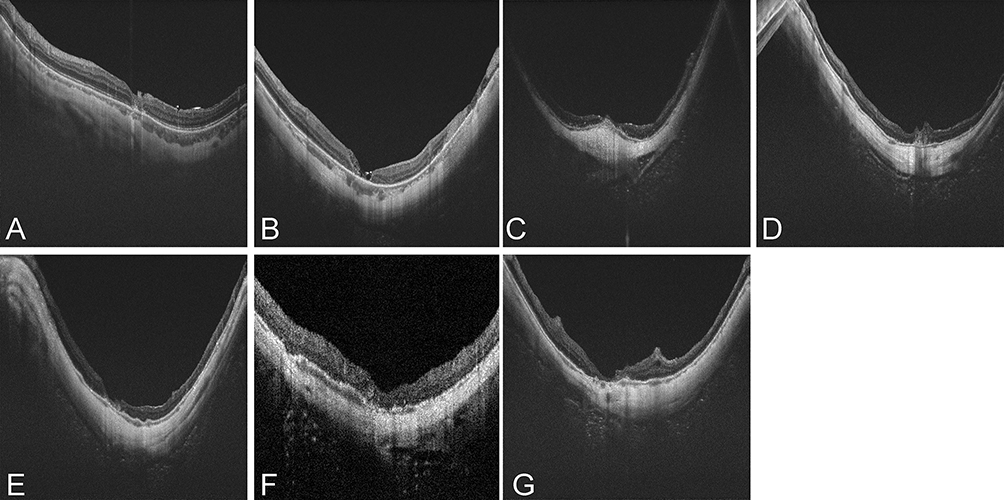 |
Figure 5 Postoperative OCT examinations of the seven eyes from the seven patients included in this study. (A–G) correspond to Patients 1–7, respectively. |
Postoperative Clinical Characteristics and Visual Recovery
Postoperative clinical characteristics are summarized in Table 2. In patients with longer axial lengths, such as Patient 1 (female), axial elongation was commonly associated with HM, while shorter axial lengths, such as in Patient 4 (male), were linked to better postoperative visual recovery potential. Preoperative BCVA ranged from 1.3 to 2.3 logMAR, significantly improving to 0.4 to 1.85 logMAR postoperatively, indicating a substantial impact of surgery on visual recovery (P = 0.0024). The mean preoperative BCVA in female patients was 2.15 ± 0.26 logMAR, improving to 1.28 ± 0.58 logMAR postoperatively. In male patients, mean BCVA improved from 1.94 ± 0.48 logMAR preoperatively to 1.14 ± 0.59 logMAR postoperatively. Despite poorer baseline visual acuity, female patients demonstrated greater postoperative improvement. For example, Patient 3 (female, aged 56 years, axial length 30.43 mm) improved significantly from a preoperative BCVA of 2.3 logMAR to 0.7 logMAR postoperatively, suggesting that patients with moderate axial length and less severe macular damage achieved better functional recovery. Conversely, Patient 1 (female, aged 65 years, axial length 32.11 mm) showed limited improvement from 2.3 logMAR to 1.85 logMAR, potentially due to irreversible retinal damage caused by excessive axial elongation. In contrast, Patient 4 (male, aged 56 years, axial length 28.48 mm) achieved a BCVA improvement to 0.4 logMAR, representing one of the best outcomes, further supporting the potential advantage of shorter axial lengths in postoperative recovery. Regarding lens status, 3 patients were pseudophakic, and 4 had cataracts. Pseudophakic patients exhibited relatively smaller postoperative visual improvements compared to cataract patients. The mean preoperative BCVA did not differ significantly between the two groups (2.15 ± 0.26 vs 1.94 ± 0.48 logMAR; P > 0.05). However, postoperative BCVA improvement was significantly less in pseudophakic patients compared to cataract patients (1.67 ± 0.32 vs 0.85 ± 0.37 logMAR; P = 0.0282). Overall, all patients achieved macular hole closure (100%) and complete retinal reattachment, with a high surgical success rate.
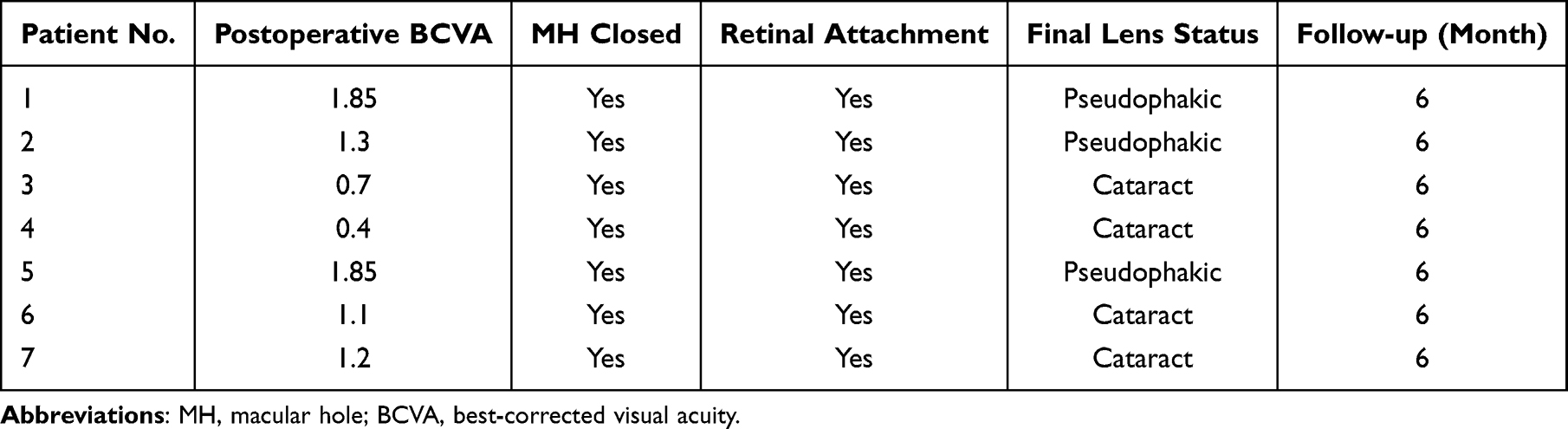 |
Table 2 Postoperative Outcomes of the Seven Eyes Included in This Study |
Discussion
The ILM flap technique has been widely applied in the treatment of MH and associated MHRD. However, in HM patients, the challenges of excessive axial length leading to abnormal retinal curvature, increased tissue fragility, and complex vitreoretinal traction often limit the surgical efficacy and postoperative outcomes of traditional ILM flap techniques.19 This study evaluated a modified surgical approach combining PFD and OVD for MHRD in highly myopic eyes. In this small retrospective series, favorable short-term anatomical outcomes and postoperative visual improvement were observed.
In this study, all eyes achieved MH closure and retinal reattachment at the final follow-up. These findings suggest that the combined PFD and OVD-assisted procedure was feasible in the included cases; however, in the absence of a comparator group, no conclusion can be drawn regarding superiority over conventional techniques. In traditional ILM flap techniques, flap displacement often occurs intraoperatively or postoperatively, especially in HM patients, due to the unique challenges of retinal curvature and fragile tissue characteristics.20 The high density and interfacial tension of PFD provide mechanical support during surgery, reducing retinal trauma and improving flap flipping and fixation. OVD’s high viscoelasticity forms a protective barrier postoperatively, preventing flap displacement and significantly increasing closure rates. Postoperative OCT imaging revealed that 71.43% of patients achieved near-normal foveal contours, highlighting the effectiveness of this technique in restoring macular anatomical structures.
Since SRF may cause displacement of the ILM flap fixed with viscoelastic agents, this study leverages the physical properties of PFD to stabilize the SRF during its management, while injecting OVD to seal the MH. This strategy prevents complications associated with SRF drainage and utilizes SRF as a buffer to minimize direct mechanical damage to the retina by surgical instruments. To prevent the displacement of the internal limiting membrane flap and the ophthalmic viscosurgical device caused by the egress of subretinal fluid through the macular hole during fluid-air exchange, we performed a limited retinotomy in the peripheral retina to drain the residual subretinal fluid, thereby enhancing the stability of the ILM flap and the overlying OVD. These procedural adjustments were intended to improve intraoperative stability and reduce the risk of flap displacement during surgery. However, because this study did not include a comparator group, the relative safety or stability of this approach compared with conventional techniques cannot be determined.18 In the present series, no intraoperative observations or postoperative OCT/fundus findings suggested clinically significant retained subfoveal OVD or residual PFD, and no related complications were identified during follow-up. Nevertheless, given the small sample size and limited follow-up duration, subtle or delayed effects related to retained materials cannot be completely excluded and warrant further evaluation in larger studies. Similar adjunctive strategies have been reported in MH-related surgery, including the use of viscoelastic-assisted flap positioning, autologous blood-assisted coverage, and perfluorocarbon-assisted ILM flap techniques to improve flap support or macular hole coverage.21–23 Therefore, the present technique should be interpreted as a procedural modification within an evolving surgical framework rather than as a wholly independent concept. In this context, the potential value of our approach lies in combining the intraoperative stabilizing effect of PFD with the adhesive property of OVD during flap manipulation in highly myopic eyes with MHRD, although further comparative studies are still required to determine whether this combination offers advantages over other published modifications.
Postoperative functional recovery was influenced by factors such as axial length, gender differences, and preoperative retinal conditions. Shorter axial lengths were associated with greater visual improvement, supporting the importance of retinal integrity for functional recovery. Patients with longer axial lengths often exhibited irreversible degenerative changes in the retina and choroid, limiting their potential for postoperative improvement. Moreover, female patients showed more significant postoperative improvements despite poorer baseline visual acuity (2.15 ± 0.26 logMAR). This may be attributed to a higher proportion of moderate axial lengths among female patients and their increased responsiveness to macular structural restoration. For instance, Patient 3 (female, axial length 30.43 mm) demonstrated remarkable visual improvement to 0.7 logMAR postoperatively, whereas Patient 1 (female, axial length 32.11 mm) showed limited improvement (1.85 logMAR) due to severe retinal damage associated with excessive axial elongation. These findings further emphasize the critical role of retinal integrity and axial length in postoperative recovery.
Further analysis indicated that the restoration of postoperative foveal contour was closely related to the optimization of surgical techniques.24 OCT imaging showed that 71.43% of patients achieved near-normal foveal contours postoperatively, while 28.57% (2 cases) displayed abnormalities such as steep or irregular contours. These outcomes may be associated with the number, shape, and tension distribution of the flipped ILM flaps during surgery. While multilayer ILM flaps provide structural scaffolding for the macular hole, facilitating photoreceptor alignment and tissue regeneration, excessive layers may induce gliosis, hindering functional recovery. Therefore, future surgical protocols should aim to optimize ILM flap strategies, balancing MH closure stability with reduced risk of adverse effects on macular restoration.
Another procedural consideration in this study was the use of low-concentration ICG staining under PFD. This approach was intended to facilitate ILM visualization while potentially reducing dye migration into the subretinal space. However, this should be interpreted as a practical intraoperative precaution rather than a novel finding, and its specific contribution cannot be determined in the present non-comparative series. While ICG staining enhances retinal visualization during ILM flap procedures, its potential toxicity poses a significant risk for postoperative outcomes.25 This study employed low-concentration ICG staining combined with PFD injection to prevent dye migration into the subretinal space, thereby reducing toxicity risks. The interfacial tension of PFD effectively blocked ICG leakage and provided a clearer surgical field. This strategy is particularly critical for HM patients, whose reduced macular pigmentation and contrast make surgical manipulation more challenging.26
Despite these promising findings, this study has certain limitations. First, the small sample size (7 patients) restricts the statistical power and generalizability of the results. Second, the absence of a control group precludes direct comparisons between the PFD and OVD combined technique and traditional methods. Third, because the cases were retrospectively selected and were not consecutively enrolled, potential selection bias cannot be excluded. In addition, because silicone oil tamponade and postoperative prone positioning were routinely applied as part of the overall surgical protocol, the observed outcomes cannot be attributed solely to the PFD-OVD-assisted ILM flap step. Therefore, the validity and generalizability of the present conclusions should be interpreted with caution. Future research should validate these findings through multicenter randomized controlled trials and larger patient cohorts. Additionally, the increased complexity and potential cost of this technique warrant further evaluation to ensure its feasibility in diverse healthcare settings.
Conclusion
In conclusion, the combined PFD and OVD technique offers an innovative solution for treating HM-associated MHRD. By optimizing ILM flap stability and reducing postoperative complications, this approach significantly improves MH closure rates and retinal reattachment success while enhancing postoperative visual function. Future studies should further investigate the applicability of this technique across diverse patient populations, extend follow-up periods to evaluate long-term outcomes, and refine procedural workflows to enhance its clinical translatability. The successful application of this technique provides new insights into MHRD management and lays the foundation for developing advanced treatment strategies for more complex cases.
Data Sharing Statement
The de-identified data used to support the findings of this study are available from the corresponding author (Dr. Shan Wang, email: [email protected]) on reasonable request.
Ethics
The Wuhan Aier Eye Hospital approved this retrospective study (approval no. 2021IRBLW01). The study adhered to the tenets of the Declaration of Helsinki. All participants gave written informed consent before any study procedures were performed. Patients were informed that their data (age, sex, axial length, and imaging outcomes) would contribute to advancing medical knowledge.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that they have no financial ties to declare. No funding or sponsors were undertaken in the preparation of the manuscript.
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Wang X, Zhu Y, Xu H. Inverted multi-layer internal limiting membrane flap for macular hole retinal detachment in high myopia. Sci Rep. 2022;12:10593. doi:10.1038/s41598-022-14716-7
2. Gao Y, Ruan T, Chen N, et al. A comparison of face-down positioning and adjustable positioning after pars plana vitrectomy for macular hole retinal detachment in high myopia. Front Med. 2022;9:780475. doi:10.3389/fmed.2022.780475
3. Jonas JB, Spaide RF, Ostrin LA, et al. IMI-nonpathological human ocular tissue changes with axial myopia. Invest Ophthalmol Vis Sci. 2023;64:5. doi:10.1167/iovs.64.6.5
4. Tsui MC, Hsieh YT, Lai TT, et al. Full-thickness macular hole formation in proliferative diabetic retinopathy. Sci Rep. 2021;11:23839. doi:10.1038/s41598-021-03239-2
5. Sakaguchi H, Kabata D, Sakimoto S, et al. Relationship between full-thickness macular hole onset and posterior vitreous detachment: a temporal onset theory. Ophthalmol Sci. 2023;3:100339. doi:10.1016/j.xops.2023.100339
6. Li B, Chen H, Zhang B, et al. Development and evaluation of a deep learning model for the detection of multiple fundus diseases based on colour fundus photography. Br J Ophthalmol. 2022;106:1079–11. doi:10.1136/bjophthalmol-2020-316290
7. Li L, Yu Y, Lin S, et al. Changes in best-corrected visual acuity in patients with dry age-related macular degeneration after stem cell transplantation: systematic review and meta-analysis. Stem Cell Res Ther. 2022;13:237. doi:10.1186/s13287-022-02931-y
8. Gayer S, Palte HD, Albini TA, et al. In vivo porcine model of venous air embolism during pars plana vitrectomy. Am J Ophthalmol. 2016;171:139–144. doi:10.1016/j.ajo.2016.06.027
9. Chatziralli I, Machairoudia G, Kazantzis D, et al. Inverted internal limiting membrane flap technique for myopic macular hole: a meta-analysis. Surv Ophthalmol. 2021;66:771–780. doi:10.1016/j.survophthal.2021.02.010
10. Ghoraba H, Rittiphairoj T, Akhavanrezayat A, et al. Pars plana vitrectomy with internal limiting membrane flap versus pars plana vitrectomy with conventional internal limiting membrane peeling for large macular hole. Cochrane Database Syst Rev. 2023;8:CD015031. doi:10.1002/14651858.CD015031.pub2
11. Zhang K, Yang X, Qi B, et al. Internal limiting membrane peeling or inverted flap technique combined with air tamponade in the treatment of macular holes in high myopia. Ophthalmic Res. 2023;66:569–578. doi:10.1159/000529387
12. Zhang XT, Wang JX, Chen S. Clinical observation of vitrectomy combined with endolaser photocoagulation at the edge of posterior scleral staphyloma for macular hole retinal detachment in high myopia. Int J Ophthalmol. 2022;15:1650–1656. doi:10.18240/ijo.2022.10.13
13. Jun SY, Kong M. Microperimetric analysis of eyes after macular hole surgery with indocyanine green staining: a retrospective study. BMC Ophthalmol. 2023;23:430. doi:10.1186/s12886-023-03161-3
14. Tobalem SJ, Weinberger A, Kropp M, et al. Chorioretinal toxicity of perfluorooctane (Ala Octa): results from 48 surgical procedures in Geneva. Am J Ophthalmol. 2020;218:28–39. doi:10.1016/j.ajo.2020.05.014
15. Zanzottera EC, Marchese A, Bandello F, et al. Intraocular perfluorodecalin and silicone oil tamponade (double filling) in the management of complicated retinal detachment: functional and anatomical outcomes using small-gauge surgery. Graefes Arch Clin Exp Ophthalmol. 2022;260:1105–1112. doi:10.1007/s00417-021-05395-7
16. Berco E, Arnon R, Kozlov Y, et al. Internal limiting membrane flap with viscoelastic device for lamellar hole surgery with no postoperative positioning. Graefes Arch Clin Exp Ophthalmol. 2023;261:3395–3401. doi:10.1007/s00417-023-06196-w
17. Chou HD, Chong YJ, Teh WM, et al. Nasal or temporal internal limiting membrane flap assisted by sub-perfluorocarbon viscoelastic injection for macular hole repair. Am J Ophthalmol. 2021;223:296–305. doi:10.1016/j.ajo.2020.09.023
18. Tao J, Zhao S, She X, et al. Inverted internal limiting membrane flap coverage with autologous blood technique after air-fluid exchange and silicone oil tamponade for extensive macular hole retinal detachment in highly myopic eyes. Retina. 2024;44:1268–1273. doi:10.1097/IAE.0000000000004068
19. Yuan J, Zhang LL, Lu YJ, et al. Vitrectomy with internal limiting membrane peeling versus inverted internal limiting membrane flap technique for macular hole-induced retinal detachment: a systematic review of literature and meta-analysis. BMC Ophthalmol. 2017;17:219. doi:10.1186/s12886-017-0619-8
20. Xu C, Feng C, Han M, et al. Inverted internal limiting membrane flap technique for retinal detachment due to macular holes in high myopia with axial length >/= 30 mm. Sci Rep. 2022;12:4258. doi:10.1038/s41598-022-08277-y
21. Cheng AMS, Gupta SK, Abdelfattah NS, et al. Macular hole repair using a refined viscoelastic assisted membrane positioning technique markedly improves surgical success rates. Int Ophthalmol. 2025;45:101. doi:10.1007/s10792-025-03466-w
22. Wang LP, Dang WJ, Yan H, et al. Perfluorocarbon liquid-assisted inverted multilayer internal limiting membrane flaps covering for macular hole retinal detachment in high myopia with axial length >/=30 mm. Int J Ophthalmol. 2025;18:2288–2295. doi:10.18240/ijo.2025.12.09
23. Yao X, Chen D, Lin P, et al. Combined retinal massage and autologous blood covering for persistent macular holes after vitrectomy in high myopia. Indian J Ophthalmol. 2024;72:S758–S762. doi:10.4103/IJO.IJO_68_24
24. Frisina R, Gius I, Palmieri M, et al. Myopic traction maculopathy: diagnostic and management strategies. Clin Ophthalmol. 2020;14:3699–3708. doi:10.2147/OPTH.S237483
25. Tabandeh H, Morozov A, Rezaei KA, et al. Superior wide-base internal limiting membrane flap transposition for macular holes: flap status and outcomes. Ophthalmol Retina. 2021;5:317–323. doi:10.1016/j.oret.2020.12.003
26. Ni Y, Xing S, Chen B, et al. Yin-Yang staining technique to create a nonstained internal limiting membrane flap to cover large idiopathic macular holes. J Vitreoretin Dis. 2024:24741264241308486.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.