Back to Journals » Patient Preference and Adherence » Volume 16
Perceptions of Participants on Trial Participation and Adherence to Tai Chi: A Qualitative Study
Authors Yang G ![]() , Li X, Peel N, Klupp N
, Li X, Peel N, Klupp N ![]() , Liu JP
, Liu JP ![]() , Bensoussan A, Kiat H, Chang D
, Bensoussan A, Kiat H, Chang D
Received 15 July 2022
Accepted for publication 2 September 2022
Published 28 September 2022 Volume 2022:16 Pages 2695—2707
DOI https://doi.org/10.2147/PPA.S380780
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Guoyan Yang,1 Xun Li,2 Nicole Peel,3 Nerida Klupp,1,3 Jian-Ping Liu,2 Alan Bensoussan,1 Hosen Kiat,1,4– 6 Dennis Chang1
1NICM Health Research Institute, Western Sydney University, Penrith, NSW, 2751, Australia; 2Center for Evidence-Based Chinese Medicine, Beijing University of Chinese Medicine, Beijing, 100029, People’s Republic of China; 3School of Health and Sciences, Western Sydney University, Penrith, NSW, 2751, Australia; 4Faculty of Medicine, Human and Health Sciences, Macquarie University, Macquarie, NSW, 2109, Australia; 5ANU College of Health and Medicine, Australian National University, Canberra, ACT, 2600, Australia; 6Cardiac Health Institute, Sydney, NSW, 2122, Australia
Correspondence: Dennis Chang; Guoyan Yang, NICM Health Research Institute, Western Sydney University, Locked Bag, 1797, Penrith, NSW, 2751, Australia, Tel +61 2 9685 4725, Fax +61 2 9685 4760, Email [email protected]; [email protected]
Purpose: Trial participation and adherence to interventions can directly influence the evaluation of outcomes in clinical trials for real world applications. The factors that influence trial participation and adherence to Tai Chi interventions in people with cardiovascular diseases remains unknown. This study aimed to explore participants’ perceptions of influential factors on their trial participation and adherence to a Tai Chi intervention within a trial setting.
Patients and Methods: Participants had coronary heart disease and/or hypertension in a randomized controlled trial comparing Tai Chi with a waitlist control. Data were collected via face-to-face, semi-structured interviews and analyzed using thematic analysis.
Results: Thirty-four participants from the Tai Chi group who completed the randomized trial were interviewed. Six dominating themes and four sub-themes are discussed under the facilitators of internal and external motivation, positive feelings, benefits of Tai Chi and future practice with an overall internal motivation to improve health. Positive feelings had three sub-themes: positive feelings toward Tai Chi, the project, and the learning experience. The Tai Chi instructor(s) was found to be a crucial element in motivating participants’ adherence to Tai Chi.
Conclusion: From the perception of participants, the facilitators to their trial participation and adherence to a Tai Chi intervention included internal and external motivation, positive feelings towards Tai Chi, the project and the learning experience, and perceived benefits of Tai Chi. Perceived barriers included concerns about the safety and complexity of Tai Chi practice, lack of group atmosphere outside of class, and scheduling conflicts. Future researchers can address these factors to improve trial recruitment and implementation of Tai Chi and other mind-body interventions in research and for real world applications.
Keywords: Tai Chi, trial participation, adherence, cardiovascular disease, interview
Introduction
Tai Chi is a traditional mind-body exercise originated in China. The main components of Tai Chi include movement, meditation and visualization, and abdominal breathing.1 In the past decade, the health benefits of Tai Chi have been widely documented in clinical studies on a variety of diseases and conditions, particularly cardiovascular diseases (CVDs) or associated risk factors.2 Considerable literature exists documenting therapeutic benefits of Tai Chi in controlling hypertension3,4 and blood lipid profile,4,5 reducing anxiety and depression,6 and improving functional capacity7,8 and quality of life.6,9 Nevertheless, more high-quality research is warranted in this field to inform evidence-based practice.6
Successful trial recruitment of participants and adherence to intervention is critical to the validity of findings of clinical trials and to practice an effective intervention among the target population in real world applications. Accessibility, alternative learning modalities, quality of teaching, perceived health benefits and community and social support are reported to be critical to participation and satisfaction with Tai Chi interventions in diverse population groups.10−14 However, less is known about the facilitators and barriers to trial participation and adherence to Tai Chi intervention in people with CVD or cardiovascular risk factors. Understanding these factors can inform future clinical trial design, recruitment, implementation, and real-world applications in this population.
This study therefore aimed to explore the perceptions of participants with CVD or cardiovascular risk factors about their trial participation and adherence to the Tai Chi intervention.
Materials and Methods
This study was conducted as a qualitative sub-study embedded in a prospective, multi-center, randomized controlled trial (RCT). It aimed to evaluate the effects of Tai Chi on stress and cardiovascular functions compared with waitlist control. This trial has been registered in Australian New Zealand Clinical Trials Registry (Registration ID: ACTRN12616001204437) and the findings will be published separately. A total of 120 participants with coronary heart diseases (CHD) and/or hypertension recruited from Beijing and Sydney recruitment centers were randomly allocated into a Tai Chi group (N=60) or waitlist group (N=60). Of them, 102 (85.0%) completed the trial, with 53 (52.0%) in the Tai Chi group. The class attendance rate of participants in the Tai Chi group was similar in Beijing (83.5%) and Sydney (80.2%) in recruitment centers, while median frequency of practice at home was 5 days per week for both sites. Missed sessions were typically attributable to scheduling conflict, such as doctor’s visit and family responsibility, based on the records of class attendance and patient diaries.
Sampling Strategy
A purposive sampling was applied to maximize the depth and richness of the data. Participants from the RCT who were assigned to the Tai Chi group and completed the 24-week Tai Chi intervention in Beijing, China and Sydney, Australia recruitment centers were all invited to participate in the face-to-face interviews within two weeks after the completion of the trial (N=53). Participation was voluntary and no financial incentives were offered for participants.
Ethical Consideration
This study was conducted in accordance with the seventh revision of the Declaration of Helsinki.15,16 Ethical approval for this qualitative sub-study was covered in the approval for the RCT (Ethics approval number: H11189; 2015BZHYLL0233). Written informed consent was obtained from each interviewee before the interview, including the publication of anonymized responses. In addition, verbal confirmation to record the interview was obtained at the beginning of each session.
Data Collection
Face-to-face, one-to-one, semi-structured interviews were used to allow more in-depth understanding from participants.17 Each interview lasted for approximately 30 minutes. The interviews took place in the same location where the participants undertook Tai Chi classes to ensure a sense of familiarity and security. The principal investigator (GYY) facilitated all the interviews in English or Chinese (Mandarin). Interviewees were familiar with the interviewer, in her role as the researcher of the study and one of the Tai Chi instructors. The established relationship and the familiar environment enhanced rapport and trust, creating a relaxed, comfortable atmosphere during interviews. Interviews were guided by ten open-ended questions (Table 1).
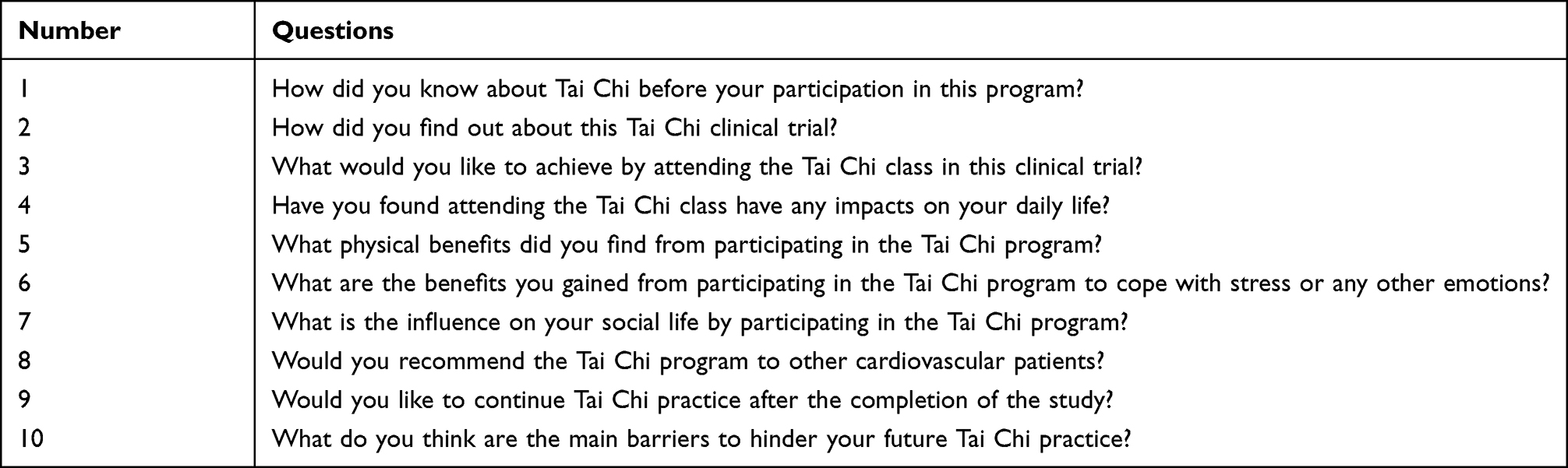 |
Table 1 Core Questions Used for the Semi-Structured Exit Interview |
Data Processing
The interviews were audio-recorded, transcribed verbatim and imported into the NVivo (Version 11, QSR International Pty Ltd.) software. NVivo is a popular computer-assisted qualitative data analysis software program.18
Data Analysis
Thematic analysis was chosen for analyzing the interviews as it provides a standard procedure to gain a deeper understanding of what participants are thinking and ensures clarity and rigor.19 Thematic analysis consisted of six steps, including familiarizing with the data, generating initial codes, searching for themes, reviewing potential themes, defining and naming themes, and producing the report.20
Verbatim transcripts of the interviews were generated in English or Chinese depending on the language spoken by the participants. Two bilingual researchers (GYY and XL), both fluent in Chinese and English, independently read each transcript carefully several times, and took notes on initial ideas on the text.
This initial coding process involved reading the transcripts and allocating codes to segments of the data that conveyed what was happening in concise terms. The two researchers independently coded four transcripts manually as a pilot and generated a codebook. Constant comparing and contrasting techniques were facilitated across codes by recording memos and queries to establish category boundaries, systematically assigning data segments to categories, and summarizing the content of each category.21 Caution was taken by the two researchers to ensure the categories reflected the data instead of forcing the data to fit within the categories.
When the codebook was refined and finalized, all transcripts were then entered into NVivo software. The Appendix demonstrates examples of the coding process. The codes were then sorted into potential themes using NVivo software and focused on the broader level of themes. After continuous revision and clarification to ensure the essence and meaning of each theme, sub-themes were then identified where appropriate meaning was seen. The final step involved interrelated themes being integrated into domains.
Results
The findings are presented with selected illustrative quotations from participant interviews. Illustrative quotations were selected and discussed for their appropriateness by two researchers. At this stage, all Chinese quotations were translated into English by one researcher and verified by a second researcher.
Participant Characteristics
Thirty-four out of the 53 (64.2%) participants in the Tai Chi group completed the interviews. The face-to-face interviews were conducted in March and April 2016 in Beijing, and April and May 2017 in Sydney. Of the 34 participants in the study, 19 (55.9%) were Chinese from the Beijing recruitment center and 15 (44.9%) were Chinese Australians from the Sydney recruitment center. The mean age of participants was 66.35±4.87 years, and 55.9% were women. In total, 31 (91.2%) had hypertension, 8 (23.5%) had CHD, and 5 (14.7%) had both hypertension and CHD. Participant characteristics of the qualitative sub-study are presented in Table 2 below.
 |
Table 2 Characteristics of the Participants |
Synthesis and Interpretation
The analysis resulted in two major domains with six dominating themes containing 31 codes as overviews in Table 3.
 |
Table 3 Sub-Themes, Themes and Domains Identified in the Qualitative Study |
Facilitators to Participation and Adherence
Theme 1: Internal/External Motivation
Improving health was a major motivator to participate in the project and to adhere to the Tai Chi intervention. Some participants reported that although they would like to improve their health through exercise in the past, they felt they had limited choices because of their age and health conditions. Some participants expressed that they were interested in any activity that was good for their health, and they realized that Tai Chi was a good choice for them.
Only in recent years I feel my body, physical movement does not coordinate with my mind, I start to explore some means…It stays in my mind to learn Tai Chi, to improve my physical health, to coordinate my mind and my arms and legs, to prevent falling, when I was invited to this class. (Male, 66 years, Sydney)
Learning Tai Chi was a long-cherished wish of some participants. They had heard of Tai Chi and its potential benefits for health or had observed Tai Chi practice but had never had chance to learn previously.
I watched Tai Chi practice years ago, Yang style, so I always want to learn Tai Chi. However, not until this time, the opportunity never comes. (Female, 63 years, Beijing)
Cherishing the learning opportunity offered in this project, participants had a good participation and adherence to the Tai Chi program. Some participants were curious about Tai Chi and its potential benefits for health; for them, one motivation to participate was to see what would happen in relation to their health.
Try and see. I never learned Tai Chi before. I had no idea of Tai Chi in the past. Because I have hypertension, I think Tai Chi might be helpful…So I participated to try and see what would happen to me. (Male, 71 years, Sydney)
Curiosity motivated participants to engage in the Tai Chi program. Moreover, their curiosity about the potential impacts on their health during the learning process enhanced their adherence to Tai Chi both during and after the completion of the study. Emotional or practical family support was also a facilitator for some participants to participate in the Tai Chi trial, particularly for those who were usually committed with family and domestic responsibilities.
My husband helped with housework or other matters, as a support. He supports me to learn Tai Chi, so I am very happy. (Female, 64 years, Beijing)
Theme 2: Positive Feeling
Feelings toward Tai Chi. It was frequently mentioned that their perception of Tai Chi had changed over the duration of the 24-week program. Prior to participation, most had only a little understanding of Tai Chi. Participants in Sydney with Chinese heritage mentioned their passion for Chinese culture. They regarded Tai Chi as “an essential treasure of Chinese culture” with a long history; this was a big motivator for them to participate in the trial.
Before I leant Tai Chi, I had already known that Tai Chi is a treasure of our Chinese culture, with a long history. Without this belief I don’t think I would join the class. (Male, 64, Sydney)
During and after their participation, participants established new views on Tai Chi. The terms “profound” “unlimited” and “regularly” were frequently used to describe the Tai Chi intervention by some participants.
After I learnt Tai Chi, I started to realize that Tai Chi is so profound, not just movements. I only know a little about it, so I am keen to know more, all of them. This is just a beginning. (Female, 67 years, Beijing)
In addition, the Tai Chi program used in the trial was easy to learn and convenient to practice due to no requirements for the location or equipment. Specifically, the participants felt that the Tai Chi protocol used in the trial was well suited to their health condition and exercise capacity.
Tai Chi is particularly suitable for the elderly to practice. No very vigorous movement such as kicking legs. I dare not to bend my knees too much, because I heard it will do harm to the knees. There is no such problem in our 13-form Tai Chi program. (Male, 67 years, Sydney)
Feelings toward the project. The target disease/condition of the Tai Chi randomized trial matched participants’ health status. Some participants expressed positively towards the program, as it was facilitated by health researchers from a known university and doctors from local hospitals. One participant believed that the project was led by a qualified Tai Chi instructor, which motivated her to participate in the trial.
I thought this was such a good opportunity, because the teacher was from Western Sydney University, a PhD candidate, and had a background of Chinese medicine. I thought the teacher should be very qualified. Where can you find such a good teacher? (Female, 63 years, Sydney)
Feelings about the learning experience. All participants we interviewed reported high satisfaction with their learning experience with most identifying the characteristics of the Tai Chi instructors and the quality of teaching as the major factors in motivating them to complete the 24-week clinical trial. Participants frequently used the terms “earnest” “responsible” “patient” “selfless” “knowledgeable” “nice” and “dedicated” to describing the characteristics of the Tai Chi instructors. Participants expressed that their Tai Chi instructor gave them “clear” “precise” “detailed” instructions and demonstrations, which were essential in developing and maintaining their learning interest and adherence to the Tai Chi program.
I was completely a layman, ho ho. I know nothing about Tai Chi. Two main reasons can explain why I can complete the half-year program. Two factors, I think, are very important. Firstly, I met a very good teacher. She gave us Tai Chi instruction very patiently and earnestly…so that I gradually become interested in Tai Chi and had a deeper understanding of it. (Male, 64 years, Sydney)
The teaching was very precise and very earnest. I find I can understand [the instruction]. In addition, what’s the purpose of the movements and how to experience the peace and stillness, [the instructors] gave very detailed explanation… To my surprise, really, I could meet such terrific teachers, so qualified and so excellent. (Female, 67 years, Beijing)
The learning environment of the Tai Chi class was another important facilitator. The venue of the Tai Chi class was described by some participants as “good” “quiet” and “clean”, which all contributed as facilitators for participants to attend the class. Moreover, participants reported that they benefited from the group-learning “atmosphere” in the Tai Chi program. The use of a social media among the participants further facilitated adherence to the Tai Chi program indirectly. In the RCT, the Tai Chi group joined a WeChat group22 that was set up to ensure timely feedback from Tai Chi instructors to support their self-practice at home. Participants found it was “encouraging” when classmates around were learning and practicing earnestly, and they could learn from each other. Timely responses from the instructors through face-to-face or online communications were also important.
I feel it’s different from practicing at home. There is an atmosphere when we practice together, and we can help each other. More importantly, the face-to-face instruction. I am interested in the timely correction and instruction…We have a WeChat group, it’s good that the Tai Chi instructor shares some knowledge there. We can ask questions, share our experience, and have discussions. (Male, 71 years, Sydney)
Theme 3: Benefits of Tai Chi
Participants reported the benefits they gained from attending the Tai Chi program, including psychological well-being, physical health and quality of life.
I was very emotional and easy to be anxious in the past. Now, I cannot say nope. There are always some different things in life and work stress. But, I feel better…Tai Chi broadens my mind. Human should be harmonious with the environment… I would not take things too hard. (Female, 63 years, Sydney)
I find I’m more alert, mentally. May be because of the music and the slow movement, I found I had calm effects. Particularly, strange, I found my short memory is not quite good because when doing Tai Chi, I can’t remember the sequences. And since then, I found there is improvement. It improves my short-term memory. (Male, 75 years, Sydney)
In addition, social supports in the Tai Chi program were also praised. Participants enjoyed the social interaction in the face-to-face Tai Chi group class, during their group practice outside of class, and through WeChat.
We get together to practice Tai Chi on Monday, Wednesday, and Friday in the playground. After practice, we often have a discussion on how to improve. We also share our own experience and always feel very happy…We miss each other if two days no see, so we contact online through WeChat. (Female, 67 years, Beijing)
Furthermore, they identified their participation in the Tai Chi program had positive impacts on their activities of daily living and quality of life because they felt happier and more energetic after Tai Chi practice.
After practice, I am often in very good mood. I feel it’s easier to do some housework. (Female, 67 years, Beijing)
Theme 4: Future Practice
Participants expressed a desire to continue the Tai Chi practice beyond the trial program.
I will continue to practice Tai Chi. For me, Tai Chi and the 13-form Thumping Techniques, I would practice them for the rest of my life. I would say, they will be a part for the rest of my life, an important part. Particularly, for the elderly, it’s much necessary for us to learn Tai Chi and the 13-form Thumping Techniques, so that we can be peace and calm. (Male, 64 years, Sydney)
Participants reported that they were extremely satisfied with their participation in the Tai Chi program and would recommend the program to others if there were more classes available in the future.
I am sure I would like to recommend the Tai Chi class to others, no matter they have cardiovascular diseases or not. For example, I would suggest my wife to come. (Male, 67 years, Sydney)
Barriers to Participation and Adherence
Theme 5: Concerns About Tai Chi
Subjective concerns included possible adverse effects, difficulty of learning the Tai Chi sequence due to the perceived complexity and maintaining self-discipline for home practice.
Participants thought the Tai Chi practice may harm their knees because they heard this from news on the television, so they preferred not to start learning until they found a good teacher.
I heard from television news several times that some people visited doctors because their knees were painful. Why? They all practiced Tai Chi. These people didn’t know how to practice appropriately, and they didn’t master the right postures and skills. So, I dare not to start learning it. (Male, 66 years, Beijing)
Some participants thought Tai Chi was a complex exercise and would be too difficult for them to learn in the beginning. However, their worries were alleviated by learning that this intervention was a specially designed Tai Chi program with only 13 movements.
Tai Chi is too difficult to learn. In the past, I tried three times to learn Tai Chi in my community, but finally I gave up. I thought, alas, why was it so hard to learn? I learned the movements in class, but I forgot all of them when I went home. So, I gave up three times. (Female, 66 years, Beijing)
The participants who often practiced outdoors with group members were keen to continue practicing Tai Chi. However, when probed about the different parts of the Tai Chi program (ie, 13-form Tai Chi, walking, meditation, standing posture and the 13-form Thumping Techniques), some participants explained it was very challenging for them to practice meditation and the 13-form Thumping Techniques by themselves at home, due to their lack of motivation without the group atmosphere.
The 13-form Thumping Techniques, for me, it’s hard to do the whole set of it. I have plenty of time, but I think I lack willpower. It’s hard to practice at home. For example, when I just sit there for meditation, my minds were wandering, such as boiling a kettle of water. So, I stand up to boil the water and then do other housework. (Male, 62 years, Beijing)
Theme 6: Barriers for Participants
Barriers which were expressed as potentially inhibiting Tai Chi practice including concerns about the poor quality of the outdoor environment due to high levels of fine particulate matter in the air (PM2.5) (Beijing participant), being sick or occupied by work or other activities, family responsibilities (such as looking after their grandchildren).
I have a grandson to look after. If he is sick, I would be worried about him and not go out. (Female, 60 years, Beijing)
Other barriers to participating and recommending Tai Chi to others included the travel distance and time conflicts.
Discussion
Summary of Main Findings
This study has discussed six dominating themes that influenced the trial participation and adherence to the Tai Chi intervention for participants with CVDs. Facilitators included internal/external motivation, positive feelings, benefits of Tai Chi, and future practices. Barriers were participants’ concerns about Tai Chi execution, environmental factors, travel distances and time conflicts. A clear understanding of these influential factors and a review of Tai Chi program can inform the development of robust strategies to promote recruitment, retention and adherence for other Tai Chi interventions and similar mind-body therapies, to support robust evaluation of any outcomes.
Facilitators to Trial Participation and Adherence
The themes emerged under the domain of facilitators for trial participation and adherence in our study support the factors found in previous qualitative studies and provide additional insight into the beneficial factors that influence the trial participation and adherence of participants.
Internal/External Motivation
Improving health was the major motivator for participants with CHD and/or hypertension to participate in the RCT and complete the Tai Chi program. Health improvement was also identified as a significant facilitator in a community-based Tai Chi program provided to older adults from lower socioeconomic backgrounds in Canada.10
In contrast, the accessibility and convenience (such as community-based classes) were the primary motivators for participation and adherence to a Tai Chi program for women with osteopenia,14 while our participants with CHD or hypertension who attended Tai Chi classes in the trial held at a fixed location and time, did not name accessibility and convenience as their priority. This may be as most participants in our study came from nearby communities and classes were held in facilities close to their homes, so the accessibility and convenience was less of an issue. In our CVD cohort, although accessibility and convenience may have been a concern, the desire to participate in a health promoting activity was a powerful driving force sustaining their trial participation and adherence. Describing scientific evidence of the health benefits of the intervention should be considered as a key factor in the success of future clinical trials and enrolment in Tai Chi program.
Positive Feelings
Our participants expressed that their perception of Tai Chi had changed gradually over the study period. Most participants had minimal knowledge of Tai Chi before participating in the trial, although most had perceived Tai Chi as “good for health.” When they deepened their knowledge and developed more skills of Tai Chi through the learning and practice, they came to regard Tai Chi as “profound” and “unlimited” mind-body exercise. Learning as a motivator can be seen as two-fold. Initially, the interest of learning is a motivator, and secondly, the actual learning experience during the intervention can be seen to sustain engagement in the Tai Chi program over the longer term.
Several participants mentioned Chinese culture, regarding Tai Chi as “an essential treasure of Chinese culture.” Tai Chi, with its long history, has multiple attractive components, integrating the essence of Chinese culture including Chinese folk and military martial arts, breathing and meditative techniques, philosophy of yin and yang, and theory of traditional Chinese medicine.1 For some, Tai Chi may be seen as a way in which to open a door of learning, to understand and experience Chinese culture.
The 13-movement Tai Chi program was designed to be easy to learn, convenient to practice at flexible time and locations, with no specific requirements of equipment for home practice. The design itself enhanced the confidence of participants to practice, particularly for older adults with limited physical capacity. Other advantages of Tai Chi, such as low-to-moderate intensity, should be articulated to potential participants during the recruitment period. Designing or selecting a Tai Chi program suitable for the target population, according to their health, mental and cognitive conditions, and exercise capacity can potentially improve the engagement and compliance. A mixed-methods systematic review also identified the program design as an important facilitator of adherence to community-based group exercise interventions for older people.23
We found Tai Chi instructors were crucial in motivating participants’ adherence to the Tai Chi intervention; this finding is consistent with that of previous literature. Characteristics of Tai Chi instructors, such as their expertise, knowledge and authenticity, patience and providing support, inspired the attendance and performance of participants with osteopenia.14 Similarly, the positive energy and supportive comments from the Tai Chi instructor contributed to ongoing participation and adherence to the Tai Chi program in veterans with post-traumatic stress symptoms.12 Individual attention and modification of movements based on individual needs from Tai Chi instructors are important in sustaining engagement.
Our findings support previous literature that has reported the importance of a helpful learning environment. Community and social support from the Tai Chi instructors, teaching assistants and peers was an incentive for class attendance and regular practice.14 It is reported that social support in the group classes, including motivation from others, shared understandings and difficulty contributed to self-efficacy and empowerment with additional gains being internal focus of control, self-awareness and stress management for participants with heart failure.24 Social support from coaches, other participants and family members was also shown to facilitate long-term exercise adherence in patients with heart failure.25 Community, practical and emotional supports may partially explain why Tai Chi is beneficial for heart health and wellbeing in participants with CVD.
In addition, the use of the smartphone social media tool (WeChat)22 in our trial to support home practice, helped to actively engage participants and improve compliance. The WeChat group was a platform where participants could gain additional social support and timely feedback for home practice. Similarly, a Cochrane review found that mobile phone text messaging improves medication adherence in secondary prevention of CVD.26
Benefits of Tai Chi
Self-reported benefits of Tai Chi cover psychosocial well-being, physical health, and quality of life. Participants described that their perceived health benefits motivate toward completion of the Tai Chi program. Previous studies also demonstrated that perceived health benefits were an important facilitator of exercise adherence among people with heart failure and adherence to community-based group exercise among older adults.23,25
In addition, these perceived benefits of Tai Chi may lead to the conceptualization of future research projects, such as exploring the benefits of Tai Chi on sleep, memory, loneliness, or social isolation for people at risk of CHD. Physical activity plays a vital role in the prevention and control of CVD and in addressing overweight and obesity.27,28 However, the increasingly busy environment is reducing opportunities for physical activity, particularly in urban settings.28 Our findings indicate that Tai Chi practice is one enjoyable option for people to improve their regular physical activity, and ultimately improve their cardiovascular and general health.
Future Practice
Our participants expressed to continue with their Tai Chi practice after the 24-week trial. One underlying reason for this may be because we continually stressed the importance of the long-term learning and regular practice of Tai Chi throughout the intervention. Most importantly, in comparison with other physical activities, Tai Chi has a special advantage in that it is a life-long enjoyable learning process with multiple levels to achieve rather than the simple repetition of movements. Furthermore, it is easy to tailor the intensity and structure of a Tai Chi program to the health conditions and requirements of participants. Enhancing appreciations and understandings of the necessity and feasibility of maintaining a Tai Chi program may therefore improve long-term adherence after study completion.
Barriers to Trial Participation and Adherence
Our findings suggested the barriers to trial participation and adherence from the perspective of participants, including concerns related to the Tai Chi intervention, personal reasons, environmental factors, travel distance and time conflicts. Fischer et al (2014) identified travel considerations and time-related factors (time required for Tai Chi practice and the 9-month duration of the trial) as barriers to participation and adherence in participants.14
In our study, a concern about the potential harm of inappropriate Tai Chi practice was raised by some participants. A systematic review evaluating the safety of Tai Chi found that although unlikely to cause serious adverse events, Tai Chi practice may be associated with minor musculoskeletal aches and pains.29 Hence, future clinical trial researchers should ensure appropriate evidence-based communication and discussion on the potential risks and benefits of Tai Chi interventions with potential participants. Researchers should also consider an initiative-taking approach to develop strategies to manage potential risks. One of the strategies could be involving an experienced Tai Chi instructor when develop the Tai Chi intervention for the target population.
Furthermore, the negative experiences of Tai Chi practice and perceptions about the complexity of Tai Chi can influence the participation and adherence to Tai Chi clinical trials. Previous studies have shown that existential thoughts about exercise, namely fear of exercise, had a negative impact on the participants’ attendance of exercise-based cardiac rehabilitation and outcomes.30,31 Therefore, it is crucial to involve an experienced Tai Chi instructor to design a tailored intervention for the target population and build trust in the interaction with participants. Importantly, clinical trial researchers should clarify the requirement of physical capacity for their Tai Chi interventions in the participant recruitment stage.
Other barriers, such as lack of motivation or group atmosphere in home practice, could be addressed through remote reminder or other support approaches to facilitate home practice. For concerns about outdoor Tai Chi practice due to outdoor air pollution, if outdoor practice is not a requirement of the study design, researchers should inform participants that Tai Chi can be practiced both indoor and outdoor, with no requirements of time, location, and equipment.
Limitations
The interviewer was one of the Tai Chi instructors in the program. As a result, a reporting bias from participants may exist as the participants may report what they thought the interviewer and instructor was expecting to hear. Therefore, the positive health benefits generated from this qualitative study should be interpreted with caution. To reduce reporting bias, all interviews were conducted at the end of the trial when all participants in the Tai Chi group had completed their program. In addition, the responses were consistent with those self-reported in the weekly patient diaries.
Participants who choose not to participate in this trial or withdraw from the trial could potentially provide insight to improve trial recruitment. However, this was not the focus of the study, and we were not able to interview those people because the exit interviews occurred when the trial was completed. Moreover, our findings were derived from the perspectives of a small group of Chinese and Chinese-Australian participants with CVD or cardiovascular risk factors in a clinical trial, the generalizability of the results may be limited and may not be applicable to people from other diverse cultural and linguistic backgrounds. However, this in-depth qualitative study helped uncover the potential complex reasons that cause participants to participate in a clinical trial and adhere to the intervention, readers may interpret the findings in relation to their existing professional and experiential knowledge.
Influences on Cultural Context
Although from different geographic locations, namely Beijing and Sydney, our participants are all Chinese or Chinese-Australian. They shared similarities in perception of participation and adherence to Tai Chi. The major differences were due to the influences on cultural context among our participants presented as follows:
- Only Beijing participants mentioned their motivations including family support or their concerns of time conflict because of “looking after the grandchildren.” The underlying reason might because it is a tradition in China that the grandparents are expected to help look after their grandchildren and there is a high expectation of their family responsibilities.
- Only Sydney participants reported their belief that Tai Chi is “an essential treasure of Chinese culture.” For some Chinese participants in Australia, Tai Chi is regarded as a way of learning, understanding, and experiencing Chinese culture.
- Only Beijing participants expressed one of their facilitators of adherence is “group atmosphere” and one barrier for home practice and future practice is “lack of group atmosphere” outside of class or after the study. The underlying reason is that the population in Beijing is much larger and denser than that of Sydney. It is easier for participants in Beijing to form a group to practice together after class during the study compared to those in Sydney. They were accustomed to practice in a group, and it would be a challenge for them to continue the practice by themselves at home.
- Only Beijing participants expressed a concern about the risk of harming knees in Tai Chi practice as indicated by media coverage. It is common in China to see people practice Tai Chi, but not all of them can practice it properly and learned Tai Chi from a qualified instructor who can address safety skills such as how to protect the knees during practice. Therefore, the improper practice did harm to some people’s knees and these cases caught media’s attention.
Implications for Future Research
Recruitment is a key challenge in all clinical trials. To improve recruitment of clinical trials on Tai Chi, effective strategies should address the potential concerns of participants, such as safety concerns of Tai Chi. Therefore, in recruitment, future researchers are suggested to effectively communicate with potential participants on the possible risks of participation and strategies to ensure the safety of participants during the practice, such as skills to protect knees. In addition, developing a Tai Chi protocol that is suitable for their physical capacity of the target population is important to relieve their concerns that to learn and practice Tai Chi is too challenging for them.
Our findings suggested some strategies of promoting adherence in clinical trials of Tai Chi or similar exercises, including addressing motivations of participants, and improving the learning experience. A strong internal motivation of our participants was to improve their health. The characteristics of the Tai Chi instructors and the quality of teaching were also important facilitators to high adherence and retention. It is strongly suggested that an experienced Tai Chi instructor should be involved in the protocol development and intervention instructions in a clinical trial. In addition, using smartphone social media (such as WeChat)22 is a good way to enhance the participant’s engagement, social support, and support for community- or home-based practice, particularly when face-to-face group exercise is not feasible such as during COVID-19 pandemic.
Tai Chi practice seems enjoyable and well accepted by people with CVD and/or cardiovascular risk factors. Our participants in this study reported that they enjoyed the learning experience and would like to continue with Tai Chi after the completion of the 24-week trial. The adoption of Tai Chi may be helpful to address the long-term prevention and management of CVD and other non-communicable chronic diseases.
Conclusion
Participants identified the influential factors that may have facilitated their participation and completion of a clinical trial and hindered their adherence to a Tai Chi intervention. Improving health is a major motivator. Other facilitators that were perceived to contribute to participants’ trial participation and adherence included positive feelings toward Tai Chi, the project and learning experience, characteristics, and teaching quality of Tai Chi instructors. Notably, participants’ concerns about the safety and complexity of Tai Chi practice might be mitigated by communicating evidence-based information. Understanding of these factors will likely assist in future research design, recruitment, and implementation of clinical trial on Tai Chi and other mind-body or exercise interventions in people with CVD or other chronic diseases and facilitate real world applications of Tai-Chi based preventative and treatment interventions.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article and its Appendix.
Ethics Approval and Consent to Participate
This qualitative study is a sub-study of an international, randomized, controlled trial, which was approved by the local human research ethics committees from both the Western Sydney University (Ethics approval number: H11189) and Beijing University of Chinese Medicine (Ethics approval number: 2015BZHYLL0233) before the commencement of the study.
Consent for Publication
Written consent for publication was obtained from all participants.
Acknowledgments
We would like to thank all the participants who were enrolled in the interviews of this study to share their experiences and insights.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. However, the first author (GYY) was supported by the Research Training Scheme from Western Sydney University, International Postgraduate Research Scholarship (IPRS) and Australian Postgraduate Award (International) from Western Sydney University. As a medical research institute, NICM Health Research Institute, Western Sydney University receives research grants and donations from foundations, universities, government agencies, individuals, and industry. Sponsors and donors also provide untied funding for work to advance the vision and mission of the Institute.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Tang H, Gu L. The history and development of Tai Chi. In: Study on Tai Chi. Beijing: People’s Sport Publishing House of China; 2012.
2. Yang GY, Sabag A, Hao WL, et al. Tai Chi for health and well-being: a bibliometric analysis of published clinical studies between 2010 and 2020. Complement Ther Med. 2021;60:102748. doi:10.1016/j.ctim.2021.102748
3. Zhong D, Li J, Yang H, et al. Tai Chi for essential hypertension: a systematic review of randomized controlled trials. Curr Hypertens Rep. 2020;22(3):25. doi:10.1007/s11906-020-1031-y
4. Tam HL, Leung LYL, Chan ASW. Effectiveness of Tai Chi in patients with hypertension: an overview of meta-analyses. J Cardiovasc Nurs. 2022. doi:10.1097/JCN.0000000000000921
5. Pan XH, Mahemuti A, Zhang XH, et al. Effect of Tai Chi exercise on blood lipid profiles: a meta-analysis of randomized controlled trials. J Zhejiang Univ Sci B. 2016;17(8):640–648. doi:10.1631/jzus.B1600052
6. Yang G, Li W, Klupp N, et al. Does tai chi improve psychological well-being and quality of life in patients with cardiovascular disease and/or cardiovascular risk factors? A systematic review. BMC Complement Med Ther. 2022;22(1):3. doi:10.1186/s12906-021-03482-0
7. Gu Q, Wu SJ, Zheng Y, et al. Tai Chi exercise for patients with chronic heart failure: a meta-analysis of randomized controlled trials. Am J Phys Med Rehabil. 2017;96(10):706–716. doi:10.1097/PHM.0000000000000723
8. Wu B, Ding Y, Zhong B, Jin X, Cao Y, Xu D. Intervention treatment for myocardial infarction with Tai Chi: a systematic review and meta-analysis. Arch Phys Med Rehabil. 2020;101(12):2206–2218. doi:10.1016/j.apmr.2020.02.012
9. Taylor-Piliae RE, Finley BA. Tai Chi exercise for psychological well-being among adults with cardiovascular disease: a systematic review and meta-analysis. Eur J Cardiovasc Nurs. 2020;19(7):580–591. doi:10.1177/1474515120926068
10. Manson JD, Tamim H, Baker J. Barriers and promoters for enrollment to a community-based Tai Chi program for older, low-income, and ethnically diverse adults. J Appl Gerontol. 2017;36(5):592–609. doi:10.1177/0733464815597315
11. Saravanakumar P, Higgins IJ, Van Der Riet PJ, Sibbritt D. Tai chi and yoga in residential aged care: perspectives of participants: a qualitative study. Clin Nurs Res. 2018;27(23–24):4390–4399. doi:10.1111/jocn.14590
12. Niles BL, Mori DL, Polizzi CP, Pless Kaiser A, Ledoux AM, Wang C. Feasibility, qualitative findings and satisfaction of a brief Tai Chi mind-body programme for veterans with post-traumatic stress symptoms. BMJ Open. 2016;6(11):e012464. doi:10.1136/bmjopen-2016-012464
13. Siu JY. Coping with future epidemics: tai chi practice as an overcoming strategy used by survivors of severe acute respiratory syndrome (SARS) in post-SARS Hong Kong. Health Expect. 2016;19(3):762–772. doi:10.1111/hex.12270
14. Fischer M, Fugate-Woods N, Wayne PM. Use of pragmatic community-based interventions to enhance recruitment and adherence in a randomized trial of Tai Chi for women with osteopenia: insights from a qualitative substudy. Menopause. 2014;21(11):1181–1189. doi:10.1097/GME.0000000000000257
15. World Medical A. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
16. Krleza-Jeric K, Lemmens T. 7th revision of the Declaration of Helsinki: good news for the transparency of clinical trials. Croat Med J. 2009;50(2):105–110. doi:10.3325/cmj.2009.50.105
17. Mason J. Linking qualitative and quantitative data analysis. In: Bryman A, Burgess B, editors. Analysing Qualitative Data. London: Routledge; 1994:89–110.
18. NVivo. What is NVivo? 2018. Available from: https://www.qsrinternational.com/nvivo/what-is-nvivo.
19. Coffey A, Atkinson P. Making Sense of Qualitative Data: Complementary Research Strategies. Thousand Oaks, CA: Sage Publications; 1996.
20. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
21. Tesch R. Qualitative Research: Analysis Types and Software Tools. London: Falmer; 1990.
22. Chen X, Zhou X, Li H, Li J, Jiang H. The value of WeChat application in chronic diseases management in China. Comput Methods Programs Biomed. 2020;196:105710. doi:10.1016/j.cmpb.2020.105710
23. Farrance C, Tsofliou F, Clark C. Adherence to community based group exercise interventions for older people: a mixed-methods systematic review. Prev Med. 2016;87:155–166. doi:10.1016/j.ypmed.2016.02.037
24. Yeh GY, Chan CW, Wayne PM, Conboy L, Pizzi C. The impact of Tai Chi exercise on self-efficacy, social support, and empowerment in heart failure: insights from a qualitative sub-study from a randomized controlled trial. PLoS One. 2016;11(5):e0154678. doi:10.1371/journal.pone.0154678
25. Warehime S, Dinkel D, Alonso W, Pozehl B. Long-term exercise adherence in patients with heart failure: a qualitative study. Heart Lung. 2020;49(6):696–701. doi:10.1016/j.hrtlng.2020.08.016
26. Adler AJ, Martin N, Mariani J, et al. Mobile phone text messaging to improve medication adherence in secondary prevention of cardiovascular disease. Cochrane Database Syst Rev. 2017;4:CD011851. doi:10.1002/14651858.CD011851.pub2
27. Koolhaas CM, Dhana K, Schoufour JD, Ikram MA, Kavousi M, Franco OH. Impact of physical activity on the association of overweight and obesity with cardiovascular disease: the Rotterdam Study. Eur J Prev Cardiol. 2017;24(9):934–941. doi:10.1177/2047487317693952
28. Myers J, McAuley P, Lavie CJ, Despres JP, Arena R, Kokkinos P. Physical activity and cardiorespiratory fitness as major markers of cardiovascular risk: their independent and interwoven importance to health status. Prog Cardiovasc Dis. 2015;57(4):306–314. doi:10.1016/j.pcad.2014.09.011
29. Wayne PM, Berkowitz DL, Litrownik DE, Buring JE, Yeh GY. What do we really know about the safety of Tai Chi? A systematic review of adverse event reports in randomized trials. Arch Phys Med Rehabil. 2014;95(12):2470–2483. doi:10.1016/j.apmr.2014.05.005
30. Back M, Cider A, Herlitz J, Lundberg M, Jansson B. The impact on kinesiophobia (fear of movement) by clinical variables for patients with coronary artery disease. Int J Cardiol. 2013;167(2):391–397. doi:10.1016/j.ijcard.2011.12.107
31. Back M, Oberg B, Krevers B. Important aspects in relation to patients’ attendance at exercise-based cardiac rehabilitation - facilitators, barriers and physiotherapist’s role: a qualitative study. BMC Cardiovasc Disord. 2017;17(1):77. doi:10.1186/s12872-017-0512-7
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.