Back to Journals » Psychology Research and Behavior Management » Volume 13
Perceptions of Caring Behavior Among Undergraduate Nursing Students: A Three-Cohort Observational Study
Authors Ferri P ![]() , Stifani S, Morotti E, Nuvoletta M, Bonetti L
, Stifani S, Morotti E, Nuvoletta M, Bonetti L ![]() , Rovesti S
, Rovesti S ![]() , Cutino A, Di Lorenzo R
, Cutino A, Di Lorenzo R ![]()
Received 27 August 2020
Accepted for publication 11 November 2020
Published 24 December 2020 Volume 2020:13 Pages 1311—1322
DOI https://doi.org/10.2147/PRBM.S279063
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Igor Elman
Paola Ferri,1 Serena Stifani,2 Elena Morotti,2 Maria Nuvoletta,3 Loris Bonetti,4 Sergio Rovesti,1 Anna Cutino,5 Rosaria Di Lorenzo6
1Department of Biomedical, Metabolic and Neural Sciences, University of Modena and Reggio Emilia, Modena 41125, Italy; 2School of Nursing, University of Modena and Reggio Emilia, Modena 41124, Italy; 3Occupational Medicine, Maserati SPA, Modena 41121, Italy; 4Nursing Research and Development Unit, Oncology Institute of Southern Switzerland, Bellinzona 6500, Switzerland; 5Psychiatry, University of Modena and Reggio Emilia, Modena 41124, Italy; 6Psychiatric Intensive Treatment Facility, Mental Health and Drug Abuse Department of AUSL-Modena, Modena 41122, Italy
Correspondence: Paola Ferri
Department of Biomedical, Metabolic and Neural Sciences, University of Modena and Reggio Emilia, via Campi, 287, Modena 41125, Italy
Email [email protected]
Introduction: Increase in the knowledge of “caring science” among nurses plays a key role in ensuring a correct caring behavior towards patients. Caring training for students is a priority in nursing education, but unfortunately there are limited and conflicting studies which explore this outcome. The purpose of this observational study was to explore the perceptions of caring behaviors by nursing students during their clinical practice training in order to highlight if the level of caring behaviors changes as the nursing course progresses.
Materials and Methods: The Caring Behaviors Inventory-24 (CBI-24) was administered to 331 students, enrolled in the three years of an Italian Nursing Course, who accepted to participate in the study (89.2% response rate). The data were analyzed using SPSS software version 26.0 (SPSS Inc., Chicago, IL).
Results: The total mean score of CBI-24 was 4.82 in the first, 5.12 in the second and 5.26 in the third-year students. The CBI-24 dimensions “Responding to individual needs” and “Being with” obtained the highest scores among the students of the first year. At the end of the first year, our students were already able to perform expressive caring, whereas instrumental caring developed at a high level in the second and third years. We did not highlight any statistically significant difference between the two gender CBI-24 item scores.
Conclusion: In light of our results, we put in evidence that Nursing Degree Programme favours the development in students of both relational and technical components of caring behaviors. We hope that in future students’ self-assessment of caring behaviors could be considered an educational outcome for Nursing Programme.
Keywords: Caring Behaviors Inventory, caring, expressive caring, instrumental caring, nursing education, nursing students
Introduction
Caring is considered the foundation of nursing, as suggested by nursing practice and theories as well as the nurse–patient relationship.1–3 It represents a very complex concept not exhaustively explained by a single definition.4 In the past, authors attributed the term “caring” to the restrictive meaning of a guide to nursing care. In recent definitions proposed by most authors, the meaning of “caring” is based on a less rigid and more detailed analysis of nursing practice.5 There are many caring theories but that proposed by Jean Watson is one of the most important. In fact, it influenced the development of nursing care as a discipline and in particular as “caring science”,6 defined by Watson and Smith as the evolution of nursing in a model that includes science and humanism by incorporating caring and individual perspectives.7 It is currently affirmed as the most advanced paradigm for nursing care, since it allows us the integration of both philosophical and ethical points of view in accordance with the awareness of humanistic and ethical evolution.8 According to many nursing theorists, the patient assumes a central role in caring, based not only on personal but also scientific knowledge, relating to the state of health and the treatment plan of the patient.4 Nurse-patient caring takes place in daily practice and cannot be restricted to the dialogue or relationship between patients and nurses. The caring meeting is in fact based on the reciprocity of the relationship between two subjects, differently from the caring relationship in which the patient can be psychologically dependent on nurses.9 A caring meeting is influenced by the expectations of both patients and nurses. It is considered positive for the patient when the nurse is competent, compassionate, able to care for patients, inspiring trust.10 Nurses’ expressions of care perceived by patients are related to patient well-being and satisfaction as well as quality of care.11–14 The increase in knowledge of “caring science” among professional nurses15 and nursing students plays a key role in ensuring a correct caring behavior towards patients.15–19 Therefore, the study of nursing theories,6 the learning of ethics and caring,12 as well as the students’ self-assessments on caring behavior give value and usefulness to the university curriculum.20 In university education, learning and teaching caring require considerable efforts; therefore, the nursing study program must be flexible and dynamic and, in accordance with guidelines,21 applying various strategies of learning and assessment of educational processes.22 The student capacity for learning caring is also conditioned by the quality of the learning environment12,23 and by the training in clinical practice which increases a humanistic vision of caring from both theoretical and practical knowledge.24 Even if students recognize caring as one of the most important professional values,25,26 their perception can be changed over the years of Nursing since it is sensitive to curricular training.12,27–30
The current health context is complex, with a high technological orientation that can influence relationships with patients.31 Moreover, the shortage in nurses, work overload and work pressure could force nurses to give priority to implementing technological tasks and instrumental procedures, leaving aside the patient’s psychosocial and emotional needs.32 Furthermore, nursing practice based on task-oriented care, where tasks are considered isolated duties, risks providing fragmented and non-person-centred care, fostering the depersonalization of caring.33
The characteristics of the clinical learning environment could negatively influence students’ learning in clinical setting. Nurse educators should encourage the creation of a positive learning environment that models and promotes caring through positive faculty and role modelling, since, as Labrague et al12 suggested, instructors who teach caring positively influence nursing students’ caring behavior.34 Students’ reflection on caring is recommended as a key strategy in the process of teaching and learning nursing discipline.24 Students’ periodic self-assessments of their caring behaviors help them reflect on themselves in order to better understand the importance of building caring relationships with the patient during clinical practice.35
Developing caring competences is considered to be one of the most important aims of undergraduate nursing education;12 individuals who enter nursing must possess caring behavior and continue to allow growth as they progress through the various educational levels. But, unfortunately, the few studies which explore this outcome report conflicting results.
The longitudinal study of Watson et al highlighted positive changes between junior and senior nursing students, since, after two years of training, students were influenced by technical and professional skills as far as their perceptions of caring.36 Nevertheless, these results are in contrast with the findings of another study, implemented in one of Singapore’s largest nursing schools, which indicated a statistically significant reduction in the overall level of caring behavior in first to final year students, measured with CBI.16 Other studies did not highlight significant changes among the student cohorts of different years of Nursing Course.27,37 A recent international cross-cultural study, which investigated the changes of caring perception between first- and third-year nursing students of different countries (Slovene, Croatian, Chinese and Russian Federation), found statistically significant differences only among Slovene students.38
Many authors highlight that caring is composed of two principal components: instrumental and expressive behaviors, which are differently emphasized by studies.38
In general, nursing students perceive that instrumental behavior is more prevalent than expressive in caring.18,20,27,36,37 Nevertheless, as suggested by a recent study, more emphasis on expressive behaviors is needed during nursing education, in order to complete learning and training on caring.38
Regarding student gender and caring behavior, research is limited and with inconsistent results.18
Students’ reflections on caring are recommended as a key strategy in the process of teaching and learning nursing discipline.24 Students’ periodic self-assessments of their caring behaviors help them reflect on themselves in order to better understand the importance of building caring relationships with the patient during clinical practice.35
Research Questions
- What are the levels of caring behaviors manifested by nursing students?
- Are there differences in the perceptions of caring behaviors between first-, second, and third-year students?
- Are there differences in the perceptions of caring behaviors between the two genders in nursing students?
The purpose of this study was to explore the perceptions of caring behaviors by nursing students during their clinical practice experience and to reveal whether the levels of caring behaviors change according to demographic characteristics and the year of the course attended.
Materials and Methods
Study Design
This three-cohort observational study was implemented in the Nursing Programme of the University of Modena and Reggio Emilia, Italy, in order to evaluate the quality of education concerning the caring behaviors among the nursing students from all 3 course years.
Sample and Setting
The sample consisted of all the students enrolled in the A.Y. 2018/2019, in the first, second and third years (n=415) of Nursing Degree Programme of Modena, at the University of Modena and Reggio Emilia. In Italy, standard nursing education programmes last 3 years (180 ECTS) and the curricula is composed of theoretical teaching and practical training. In our Nursing Degree Programme, a specific caring module “Principles and techniques of the care relationship” has been implemented with the aim of enhancing caring behaviors and, in order to develop students’ empathic abilities, a training session with a patient expert in the role of trainer is implemented during the first semester of each year.39
All students who had attended the clinical practice for about a month were considered eligible, whereas the students who had attended the internship for less than one month and those who were involved in Erasmus courses were excluded.
Sample size was calculated using the population size, the confidence level (95%) and margin of error (5%).40 The approximate required sample size was n=200.
Data Collection and Questionnaire
The data were collected using a questionnaire structured in two parts: (a) demographic information and (b) the Caring Behaviors Inventory (CBI), validated in Italian.41 Students completed a demographic questionnaire with the following information: age, sex and year of the Nursing Programme. The second part of the questionnaire provided for the compilation of the CBI in order to examine the students’ perception of their caring behaviors during the clinical practice. The CBI was originally developed by Wolf42 to analyze patients’ perceptions of nurses’ caring behaviors through the analysis of 75 items, subsequently reduced to 43 items, which investigate 5 dimensions; it was also validated in a group of nurses.42–44 This scale was designed on the basis of “Transpersonal theory” and on the “10 carative factors” highlighted by Jean Watson.1 The CBI items were further reduced to 24 in order to make participation easier and to reduce research costs. In factorial analysis, the following dimensions were identified: “Assurance” (D1) with 8 items; “Knowledge and Skill” (D2) with 5 items; “Respectful” (D3) with 6 items; “Connectedness” (D4) with 5 items. The CBI-24 demonstrated validity and reliability in the evaluation of caring behaviors for both patients and nurses: the overall index of CBI-24 reached high internal consistency (α = 0.96), as did the four subscales, α values ranged from 0.82 to 0.92.45 Tomietto et al41 validated the Italian version of the CBI-24, analyzing two samples, one of patients and one of nurses. This Italian version, called the Italian CBI, was psychometrically analyzed by Fenizia et al35 to validate its use in undergraduate nursing students. The results of the validation among students kept unchanged both the number of items (n = 24) and dimensions (n = 4) but suggested a different distribution of items in the factors and their denomination: “Being with” (D1) with 10 items, “Doing with competence” (D2) with 5 items, “Responding to individual needs” (D3) with 6 items and “Providing effective care” (D4) with 3 items.35 The different item distribution in the dimensions of the CBI-24 according to the authors Wu et al45 and Fenizia et al35 is presented in Table 1.
 |
Table 1 Item Distribution in the Caring Behaviors Inventory Dimensions, in Accordance with Wu et al45 and Fenizia et al35 |
The CBI items report the frequency of caring behaviors in their daily clinical practice subjectively experienced by each student. The frequency of execution of each caring behavior was described by the students on a 6-point Likert scale (1 = “never”, 2 = “almost never”, 3 = “sometimes”, 4 = “usually”, 5 = “often”, 6 = “always”). High item score indicates that caring behavior is present at high level in the student–patient relationship.
Prior to data collection, permission to use the CBI-24 was acquired from the developers of the questionnaire.
In the present study, the Cronbach coefficient α was 0.91.
Operative Procedures
Before the start of the study, at the end of theoretical lessons and before clinical practice training, students from all 3 years received information from a researcher on the study purpose and on methods of collecting data through the Caring Behaviors Inventory scale (CBI), validated in Italian,41 in order to obtain students’ voluntary participation.
The study was conducted in the second half of each year nursing course, at the end of the theoretical lessons and during clinical practice training performed in the following healthcare settings: hospitals, elderly care homes, nursing homes and in other local accredited structures and services dedicated to nursing assistance. In each clinical practicum placement, a briefing was performed by a student tutor not involved in the study and, successively, the questionnaires were distributed to students who met the inclusion criteria. Each student had a 15-day period for completing the CBI. The data collection period was from 8 to 31 July 2019. The method of questionnaire delivery guaranteed respect for the student’s privacy and anonymity. During the study period, the nursing study program was not changed in comparison with previous academic programs and no conferences, student training activities or other extraordinary training events on caring were implemented.
The STROBE checklist for observational studies was followed to enhance methodological rigour.46 In particular, we described all efforts to address potential sources of bias: we collected a representative sample of our population of nursing students enrolled in the 3years of Nursing Degree Programme; we provided complete and homogenous information to all participants, without any form of coercion; we administered validated questionnaires during clinical practice training in order to avoid recall bias.
Statistical Analysis
Descriptive and inferential statistical methods have been used. More specifically, the distribution frequency of the variables was estimated, as well as mean and standard deviation of the quantitative variables. Analysis of variance (ANOVA) has been used to assess the statistically significant differences between the variables. Statistical significance was set for p<0.05. The data were analyzed using SPSS software version 26.0 (SPSS Inc., Chicago, IL).
Ethical Considerations
The present project was conducted in accordance with the principles of the Helsinki Declaration.47 In compliance with the local Ethical Committee guidelines,48 where quality improvement projects do not require any authorization given that they involve voluntary participants who have given their consent and no changes in the practices are introduced, the project was submitted for University authorization. Permission to conduct the project was provided by the Dean of the Nursing Course, University of Modena and Reggio Emilia (28/04/2019 number 4/2019). All participants were informed of the possibility of withdrawing at any study stage without any repercussions on their future study program. Moreover, during the information session provided, they were assured that the participation was voluntary and free from any form of benefits or coercion. Furthermore, eligible participants were informed that the completion of the questionnaire was considered consent to participate in the study. In line with ethical principles, confidentiality was ensured by attributing an identification code to each questionnaire. The data were stored in a secure database that only the research team had access to. In addition, students were left free from any influence by appointing to the team researchers not involved in student evaluation/teaching at the time of the data collection.
Results
The final sample was represented by 371 eligible students divided as follows over the 3 course years: 133 in the first, 118 in the second and 120 in the third year. A total of 331 students took part in the study (response rate 89.2%): 121 in the first year of the course, 106 in the second and 104 in the third. 82.2% were women and 17.8% were men; their ages ranged from 19 to 55 years (M 22.0, SD 3.7). The first-year students included 121 respondents 20 males and 101 females, with mean age of 21.2 years (SD 4.5); second year 106 participants, 22 males and 84 females, with mean age of 22.2 years (SD 3.4); third year 104, 17 males and 87 females, with mean age of 22.7 years (SD 2.5).
As shown in Table 2, all students of the three-year Nursing Programme reported scores higher than 4, according to the Likert scale, in 23 CBI items.
 |
Table 2 CBI Item Scores in the Three Cohorts |
In item number 12, “Knowing how to give shots, IVs, etc.”, the first-year students reported the lowest frequency of caring behavior, with the mean score 2.83 ± 1.8 SD (Figure 1).
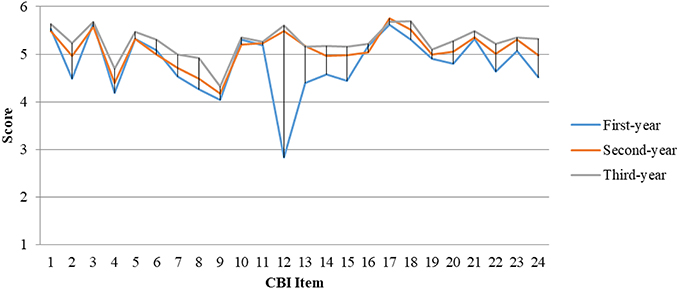 |
Figure 1 CBI item scores in the three cohorts. |
The students enrolled in the first year of Nursing Programme reported a frequency scored just above the value 4 on the Likert scale, including the following: “Returning to the patient voluntarily”, “Spending time with the patient” and “Including the patient in planning his or her care”.
The following caring behaviors presented a high frequency from the first year of the course up to the third, without any statistically significant difference among the three years: “Treating the patient as an individual”, “Treating patient information confidentially”, “Attentively listening to the patient”, “Supporting the patient”, “Showing concern for the patient” and “Talking with the patient”.
The students of the second year reported a significant increase in the frequency of the caring behaviors expressed by the items “Knowing how to give shots, IVs, etc.” (M 5.49 ± 0.8 SD) and “Being confident with the patient” (M 5.17 ± 0.7 SD), which remained steadily high in the item scores reported by the students of the third year.
The following caring behaviors were reported with gradual increased frequency which statistically significantly differed among the three cohorts of students: “Encouraging patient to call if there are problems”, “Giving the patient’s treatments and medications on time”, “Relieving the patient’s symptoms”, “Responding quickly to the patient’s call”, “Giving instructions or teaching the patient”, “Helping to reduce the patient’s pain”, “Demonstrating professional knowledge and skill”, “Managing equipment skillfully”, “Helping the patient grow”. The “Returning to the patient voluntarily” item maintained similar values among the three cohorts of the sample.
The global mean score of CBI, reported by the three cohorts of students, increased in each year of their nursing course, with a statistically significant difference (F = 20.33; p <0.001), as shown in Table 2. Similarly, three dimensions of the scale showed a significant increase in the frequency among the students of the first year compared to the cohort of third year: “Being with” F = 6.85, p = 0.001; “Doing with competence” F = 75.42, p < 0.001 and “Providing effective care” (F = 13.75, p < 0.001) (Table 2).
We did not highlight any statistically significant difference between the two gender CBI item scores, as shown in Table 3.
 |
Table 3 CBI Dimension Scores in Our Sample Divided by Gender |
Discussion
The purpose of this study was to explore the perception of caring behavior by nursing students during their clinical practice training in order to highlight if the level of caring behavior changes as the nursing course progresses.
The high response rate (89.2%) represents a satisfactory participation, showing students’ high interest in this topic. The distribution of gender and age in our sample is similar to other studies that investigated nursing students’ perceptions of caring behaviors.16,38,49
The total mean score of CBI-24 was 4.82 in the first year, 5.12 in the second and 5.26 in the third year cohort of students. These data indicate that students already perceived caring at high level at the end of the first year and, successively, over the three years of the course, they perceived an increase of caring level, in a statistically significant way.
This finding is in agreement with the study of Watson et al,36 but is in contrast with the results of other studies which highlighted a reduction or no difference in caring level during the Nursing Degree Programme in nursing students.16,27,37,38
In our sample, the CBI-24 dimensions “Responding to individual needs” and “Being with”, obtained the highest scores (M = 5.20 and M = 4.85) among the students of first year, indicating good perception of expressing caring. At the end of third year, 3 of the 4 CBI-24 dimensions, statistically significant increased: “Being with” (F = 6.85, p = 0.001); “Doing with competence” (F = 75.42, p < 0.001) and “Providing effective care” (F = 13.75, p < 0.001), suggesting that both components of caring, expressive and instrumental, were perceived by students as prominent in the relationship with patients. The two CBI-24 dimensions, “Doing with competence” (D2) and “Providing effective care” (D4), presented the greatest increase during nursing training. These two dimensions concern the instrumental domains of caring, which normally increase as the nursing course progresses probably because students frequently attend simulations in nursing skill labs and are more trained in the use of technical instruments. Two Iranian studies found that nursing students perceived practical (to give patient’s treatments and medications on time) and cognitive caring behavior (monitors and follows through, explains and facilitates) as the most important and emotional ones (trusting relationship, comforts) as the least important behaviors.27,37 In a longitudinal survey conducted in a sample of Scottish nursing students, caring was largely perceived as a technical dimension.36 Similar results were found by a multicultural study conducted across Nigeria, India, Greece, and The Philippines.20
Regarding D2, the only behavior that is frequently adopted by students from the beginning without any change is “Being patient or tireless with the patient”. This finding is in line with that of the study of Schofield et al,50 which highlighted that nursing students defined caring precisely as “Just being available for them, being patient with them”.50
The CBI-24 dimension “Being with” (D1) presented higher scores than the previous two dimensions, showing a significant increase over the three-year training period. However, each item individually analyzed showed difference. In fact, only the items which describe behavior closely related to the expressive domain of caring obtained high scores by the end of first year and remained constantly high to the end of Nursing Programme: “Attentively listening to the patient”, “Treating the patient as an individual”, “Supporting the patient”, “Being empathetic”. By contrast, 4 items of D1 showed gradual increase from the first to the third year: “Giving instructions or teaching the patient”, “Spending time with the patient”, “Helping the patient grow” and “Including the patient in planning his or her care”. This result indicates that, with the advancement of training, the student more often performs an approach based on scientific knowledge and technical instruments, while maintaining an empathic approach aimed at respecting patient dignity. The increase in skills over the years of study leads students to give importance to “Include the patient in the planning of his care”. The learning of new theoretical skills in the Nursing Course allows the student to “Give instructions or teach the patient” with greater independence and in an ever more detailed/in-depth manner within the therapeutic relationship with the patient. Moreover, students’ awareness of their level of education increases this caring behavior in the academic years, increasing the “Being empathetic or identifying with the patient”, “Returning to the patient voluntarily”, “Talking with the patient”.
In D1, the item “Attentively listening to the patient” describes a behavior considered a priority in the caring process by students of all three cohorts. The importance of active patient listening emerged as relevant data in the narratives of nursing students on the experiences of caring relationships during clinical practice.51
The study by Macaden et al,52 highlighted that nursing students consider the following behaviors fundamental for the respect of patient dignity: listening to patients, involving them in decision-making and maintaining their privacy.52 Similar results were highlighted in a study that investigated respect for dignity from the patient’s point of view.53 Respect for the person, identified in the item “Treating the patient as an individual”, is the behavior most frequently performed by all participants, considered fundamental in the caring relationship between nurse and patient as well as being the basis of ethical principles, in line with another study.54
Our students believe that nurse-patient communication is necessary in order to understand the patient’s physical and psychological needs, with the relevant objective, for our sample, of “Supporting the patient” during caring, as observed by another study.55 Communication with the patient is considered a basic element of the caring process.51,54 In fact, in the interaction with the patient, even the choice of appropriate tone of voice and words is considered an essential element.50 The results observed in our study are in line with the literature: all our students gave high and constant importance to the behavior “Talking with the patient” during the course of studies. Moreover, “Being empathetic or identifying with the patient” was perceived by students as a high value caring behavior.
These results suggest a good ability of our sample in establishing a trusting and emphatic relationship with patients, a prerequisite for any caring behavior.49 In this regard, maintaining ethical principles of behavior contributes to developing the ability to manage emotions, thoughts and decisions in caring practices.56
The “Responding to individual needs” dimension reported the highest values in all three cohorts of students, with a minimal incremental change from the first to the third year. In this dimension, 4 items reported high values already at the beginning without any statistically significant change during the course: “Allowing the patient to express feelings about his or her disease and treatment”, “Treating patient information confidentially”, “Meeting the patient’s stated and unstated needs”, “Showing concern for the patient”. This result does not overlap another longitudinal study, which highlighted that patient intimacy and support became evident as students progressed through the Nursing Programme.36 The D4, like D1, is mainly characterized by behavior related to the psychosocial or expressive domain of caring: unconditional acceptance, empathy, genuineness, respect, and treating others as family members.27 The “Responding to individual needs” dimension, which indicates that clinical assistance has to be tailored to the needs of the individual patient, was perceived as very important by our students. This result, which suggests that our students were highly sensitive to both real and potential patient needs and expectations, is in line with the literature. In another study, nursing students described caring as knowing the individual as a person with human adversities.50 Another author pointed out that nursing students believe that the purpose of the professional relationship with the patient is to help him/her in satisfying his basic needs.54 In this dimension, the behavior described by the two items, “Encouraging patient to call if there are problems” and “Responding quickly to the patient’s call”, became more frequent among students in the last year of the course, probably because they were particularly trained in handling patients’ problems and had developed clinical reasoning skills in addition to relational abilities, as students typically do by the end of the Nursing Programme.
Finally, in line with some studies, our findings did not highlight any statistically significant difference between the two gender CBI-24 item scores.30,37 This is in contrast to a previous study where male students had higher mean scores in CBI-24 than female students.18
Limits and Advantages
This study presents a number of limits: our results, limited to a single Nursing Programme, cannot be completely generalized. According to our observational design, we collected data at a single point in time; a longitudinal study could be appropriate to deepen our knowledge of this topic.
Despite these limitations, this research has the advantage of having collected a large sample of three cohorts of students with high response rate, and of having analyzed the development of caring skills, which represent one of the most important aspect of nursing.
Conclusions
The results of the study suggest that students, by the end of the first year, are able to perform expressive caring behavior. This dimension belongs to “Being with” area, which requires students to behave with kindness and empathy, guaranteeing attentive and respectful support to the assisted person in order to ensure tailored and patient-centred care. Instead, behavior of instrumental caring reaches a high level in the second and third years, as reported in literature. This type of caring, belonging in particular to the “Doing with competence” area, responds to patients’ physical health needs through competent and safe technical interventions.
In light of our results, we put in evidence that Nursing Programme favours the development in students of both relational and technical components of caring behaviors. We hope that in future students’ self-assessment of caring behaviors could be considered an educational outcome for Nursing Programme.
Abbreviations
CBI-24, Caring Behaviors Inventory-24; CBI, Caring Behaviors Inventory.
Acknowledgments
The authors would like to thank all students who participated in this study and Orianna Raggioli for her language revision.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no actual or potential conflicts of interest.
References
1. Watson J. Caring as the essence and science of Nursing and health care. Mundo Saúde. 2009;33(2):143–149. doi:10.15343/0104-7809.200933.2.2
2. Cao Q. Humanistic caring: the core of nursing. J Med Coll PLA. 2013;28(2):125–128. doi:10.1016/S1000-1948(13)60026-X
3. Smith MC. Caring and the discipline of nursing. In: Smith MC, Turkel MC, Wolf ZR, editors. Caring in Nursing Classics: An Essential Resource. New York: Springer Publishing Company; 2013:1–8.
4. Cook LB, Peden A. Finding a focus for nursing. The caring concept. Adv Nurs Sci. 2017;40(1):12–23.
5. Sargent A. Reframing caring as discursive practice: a critical review of conceptual analyses of caring in nursing. Nurs Inq. 2012;19(2):134–143. doi:10.1111/j.1440-1800.2011.00559.x
6. Pajnkihar M, McKenna HP, Štiglic G, Vrbnjak D. Fit for practice: analysis and evaluation of Watson’s theory of human caring. Nurs Sci Q. 2017;30(3):243–252. doi:10.1177/0894318417708409
7. Watson J, Smith M. Caring science and the science of unitary human beings: a trans theoretical discourse of nursing knowledge development. J Adv Nurs. 2002;37(5):452–461. doi:10.1046/j.1365-2648.2002.02112.x
8. Turkel MC, Watson J, Giovannoni J. Caring Science or Science of Caring. Nurs Sci Q. 2018;31(1):66–71. doi:10.1177/0894318417741116
9. Holopainen G, Nystrom L, Kasén A. The caring encounter in nursing. Nurs Ethics. 2019;26(1):7–16.
10. Wiechula R, Conroy T, Kitson AL, Marshall RJ, Whitaker N, Rasmussen P. Umbrella review of the evidence: what factors influence the caring relationship between a nurse and patient? J Adv Nurs. 2016;72(4):723–734. doi:10.1111/jan.12862
11. Palese A, Tomietto M, Suhonen R, et al. Surgical patient satisfaction as an outcome of nurses’ caring behaviors: a descriptive and correlational study in six European countries. J Nurs Scholarsh. 2011;43(4):341–350. doi:10.1111/j.1547-5069.2011.01413.x
12. Labrague LJ, McEnroe-Petitte DM, Papathanasiou IV, Edet OB, Arulappan J. Impact of instructors’ caring on students’ perceptions of their own caring behaviors. J Nurs Scholarsh. 2015;47(4):338–346. doi:10.1111/jnu.12139
13. Leyva EWA, Peralta AB, Tejero LMS, Santos MA. Global perspectives of caring: an integrative review. Int J Hum Caring. 2015;19(4):7–29.
14. Edvardsson D, Watt E, Pearce F. Patient experiences of caring and person‐centredness are associated with perceived nursing care quality. J Adv Nurs. 2017;73(1):217–227. doi:10.1111/jan.13105
15. Martin MB. Caring in nursing professional development. J Nurses Prof Dev. 2015;31(5):271–277. doi:10.1097/NND.0000000000000172
16. Loke JC, Lee KW, Lee BK, Mohd Noor A. Caring behaviors of student nurses: effects of pre-registration nursing education. Nurse Educ Pract. 2015;15(6):421–429. doi:10.1016/j.nepr.2015.05.005
17. Li YS, Yu WP, Yang BH, Liu CF. A comparison of the caring behaviors of nursing students and registered nurses: implications for nursing education. J Clin Nurs. 2016;25:3317–3325. doi:10.1111/jocn.13397
18. Aupia A, Lee TT, Liu CY, Wu SV, Mills ME. Caring behavior perceived by nurses, patients and nursing students in Indonesia. J Prof Nurs. 2018;34:314–319. doi:10.1016/j.profnurs.2017.11.013
19. Kinchen E. Holistic nursing values in nurse practitioner education. Int J Nurs Educ Scholarsh. 2019;16(1).
20. Labrague LJ, McEnroe-Petitte DM, Papathanasiou IV, Edet OB, Arulappan J, Tsaras K. Nursing students’ perceptions of their own caring behaviors: a multicountry study. Int J Nurs Knowl. 2017;28(4):225–232. doi:10.1111/2047-3095.12108
21. Salehian M, Heydari A, Aghebati N, Karimi Moonaghi H. Faculty-student caring interaction in nursing education: an integrative review. J Caring Sci. 2017;6(3):257–267. doi:10.15171/jcs.2017.025
22. Cook PR, Cullen JA. Caring as an imperative for nursing education. Nurs Educ Perspect. 2003;24(4):192–197.
23. Ma F, Li J, Liang H, Bai Y, Song J. Baccalaureate nursing Students’ perspectives on learning about caring in China: a qualitative descriptive study. BMC Med Educ. 2014;14:42–50. doi:10.1186/1472-6920-14-42
24. Dobrowolska B, Palese A. The caring concept, its behaviors and obstacles: perceptions from a qualitative study of undergraduate nursing students. Nurs Inq. 2016;23:305–314. doi:10.1111/nin.12143
25. Ferri P, Laffi P, Rovesti S, Artioli G, Di Lorenzo R, Magnani D. Motivational factors for choosing the degree course in nursing: a focus group study with nursing students. Acta Bio Medica. 2016;87(Suppl 2):19–27.
26. Poorchangizi B, Borhani F, Abbaszadeh A, Mirzaee M, Farokhzadian J. Professional values of nurses and nursing students: a comparative study. BMC Med Educ. 2019;19:438–445. doi:10.1186/s12909-019-1878-2
27. Zamanzadeh V, Valizadeh L, Azimzadeh R, Aminaie N, Yousefzadeh S. First and fourth-year student’s perceptions about importance of nursing care behaviors: socialization toward caring. J Caring Sci. 2014;3(2):93–101.
28. Phillips J, Cooper K, Rosser E, et al. An exploration of the perceptions of caring held by students entering nursing programmes in the United Kingdom: a longitudinal qualitative study Phase 1. Nurse Educ Pract. 2015;15(6):403–408. doi:10.1016/j.nepr.2015.05.004
29. Rosser EA, Scammell J, Heaslip V, et al. Caring values in undergraduate nurse students: a qualitative longitudinal study. Nurse Educ Today. 2019;77:65–70. doi:10.1016/j.nedt.2019.03.011
30. Trinidad MF, González Pascual JL, García MR. Perception of caring among nursing students: results from a cross-sectional survey. Nurse Educ Today. 2019;83:104196. doi:10.1016/j.nedt.2019.08.014
31. Lapum J, Fredericks S, Beanlands H, McCay E, Schwind J, Romaniuk D. A cyborg ontology in health care: traversing into the liminal space between technology and person‐centred practice. Nurs Philos. 2012;13(4):276–288. doi:10.1111/j.1466-769X.2012.00543.x
32. Papastavrou E, Efstathiou G, Tsangari H, et al. A cross‐cultural study of the concept of caring through behaviors: patients’ and nurses’ perspectives in six different EU countries. J Adv Nurs. 2012;68(5):1026–1037. doi:10.1111/j.1365-2648.2011.05807.x
33. Romero-Martín M, Gómez-Salgado J, Robles-Romero JM, Jiménez-Picón N, Gómez-Urquiza JL, Ponce-Blandón JA. Systematic review of the nature of nursing care described by using the Caring Behaviors Inventory. J Clin Nurs. 2019;28(21–22):3734–3746. doi:10.1111/jocn.15015
34. Eley D, Eley R, Bertello M, Rogers‐Clark C. Why did I become a nurse? Personality traits and reason for entering nursing. J Adv Nurs. 2012;68(7):1546–1555. doi:10.1111/j.1365-2648.2012.05955.x
35. Fenizia E, Marchetti A, Biagioli V, et al. Psychometric testing of the Caring Behaviors Inventory for nursing students. J Clin Nurs. 2019;28(19–20):3567–3574. doi:10.1111/jocn.14950
36. Watson R, Deary IJ, Hoogbruin AL. A 35-item version of the Caring Dimensions Inventory (CDI-35): multivariate analysis and application to a longitudinal study involving student nurses. Int J Nurs Stud. 2001;38(5):511–521. doi:10.1016/S0020-7489(00)00107-3
37. Khademian Z, Vizeshfar F. Nursing students’ perceptions of the importance of caring behaviors. J Adv Nurs. 2008;61(4):456–462. doi:10.1111/j.1365-2648.2007.04509.x
38. Pajnkihar M, Kocbek P, Musović K, et al. An international cross-cultural study of nursing students’ perceptions of caring. Nurse Educ Today. 2020;84:104214. doi:10.1016/j.nedt.2019.104214
39. Ferri P, Rovesti S, Padula MS, D’Amico R, Di Lorenzo R. Effect of expert-patient teaching on empathy in nursing students: a randomized controlled trial. Psychol Res Behav Manag. 2019;12:457–467. doi:10.2147/PRBM.S208427
40. Qualtrics. Sample size calculator. Available from: https://www.qualtrics.com/blog/calculating-sample-size/.
41. Tomietto M, Papastavrou E, Efstathiou G, Palese A. Misurare la percezione di caring in pazienti e infermieri: validazione italiana del Caring Behaviors Inventory (CBIta). [Measuring the perception of caring in patients and in nurses: Italian validation of the Caring Behaviors Inventory (CBIta)]. [Article in Italian]. G Ita Med Lav Ergon. 2014;36(1):38–44.
42. Wolf ZR. The caring concept and nurse identified caring behaviors. Top Clin Nurs. 1986;8(2):84–93.
43. Wolf ZR. The Concept of Caring: Beginning Exploration. Candidacy Paper. Philadelphia: University of Pennsylvania School of Nursing; 1981.
44. Wolf ZR, Giardino ER, Osborne PA, Ambrose MS. Dimensions of nurse caring. Image J Nurs Scholarsh. 1994;26(2):107–111. doi:10.1111/j.1547-5069.1994.tb00927.x
45. Wu Y, Larrabee JH, Putman HP. Caring Behaviors Inventory: a reduction of the 42-item instrument. Nurs Res. 2006;55(1):18–25. doi:10.1097/00006199-200601000-00003
46. Cuschieri S. The STROBE guidelines. Saudi J Anaesth. 2019;13(Suppl 1):S31–S34. doi:10.4103/sja.SJA_543_18
47. World Medical Association. Declaration of Helsinki ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
48. Comitato Etico Area Vasta Emilia Nord. [homepage on the Internet]. Regolamento Costitutivo del Comitato Etico dell’Area Vasta Emilia Nord. [Constitutive Regulation of the Area Vasta Emilia Nord]. Available from: https://www.aou.mo.it/ComitatoEticoAVEN.
49. Konuk TG, Tanyer D. Investigation of nursing students’ perception of caring behaviors. J Caring Sci. 2019;8(4):191–197. doi:10.15171/jcs.2019.027
50. Schofield R, Allan M, Jewiss T, et al. Knowing self and caring through service learning. Int J Nurs Educ Scholarsh. 2013;10(1):267–274. doi:10.1515/ijnes-2013-0009
51. Guarinoni MG, Dignani L, Motta PC. Caring relationship: a qualitative research through the narratives of the students of the Bachelor of Science in Nursing degree. Prof Inferm. 2019;72(2):129–134.
52. Macaden L, Kyle RG, Medford W, Blundell J, Munoz SA, Webster E. Student nurses’ perceptions of dignity in the care of older people. Br J Nurs. 2017;26(5):274. doi:10.12968/bjon.2017.26.5.274
53. Ferri P, Muzzalupo J, Di Lorenzo R. Patients’ perception of dignity in an Italian general hospital: a cross-sectional analysis. BMC Health Serv Res. 2015;15:41. doi:10.1186/s12913-015-0704-8
54. Karaöz S. Turkish nursing students’ perception of caring. Nurse Educ Today. 2005;25(1):31–40. doi:10.1016/j.nedt.2004.09.010
55. Chan ZCY, Lai CKY. The nurse-patient communication: voices from nursing students. Int J Adolesc Med Health. 2016;29(6). doi:10.1515/ijamh-2016-0023
56. Culha Y, Acaroglu R. The relationship amongst student nurses’ values, emotional intelligence and individualised care perceptions. Nurs Ethics. 2019;26(7–8):2373–2383. doi:10.1177/0969733018796682
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.