Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 17
Perceptions, Challenges and Barriers to HIV Care in Mbujimayi in the East Kasai Province, DR Congo: A Qualitative Study
Authors Baloji D ![]() , Ntambwe G, Ntambua AK, Kidinda W, Kazadi MB, Mpanya A, Mukuna B, Ngongo L, Mjumbe CK
, Ntambwe G, Ntambua AK, Kidinda W, Kazadi MB, Mpanya A, Mukuna B, Ngongo L, Mjumbe CK ![]() , Mutombo K A, Lutumba P
, Mutombo K A, Lutumba P ![]()
Received 19 May 2025
Accepted for publication 5 September 2025
Published 12 September 2025 Volume 2025:17 Pages 297—311
DOI https://doi.org/10.2147/HIV.S541334
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Olubunmi Akindele Ogunrin
Désiré Baloji,1 Georges Ntambwe,1 Alix Kamina Ntambua,1 William Kidinda,1 Marie Benoit Kazadi,1 Alain Mpanya,2 Bertin Mukuna,3 Laetitia Ngongo,4 Criss Koba Mjumbe,4 André Mutombo K,5 Pascal Lutumba6
1Faculty of Public Health, Mbujimayi Official University, Mbujimayi, Democratic Republic of the Congo; 2Community Health Section, Higher Institute of Medical Techniques of Lubumbashi, Lubumbashi, Democratic Republic of the Congo; 3Department of Nursing Sciences, Faculty of Health Sciences, National Pedagogical University, Kinshasa, Democratic Republic of the Congo; 4Department of Public Health, Faculty of Medicine, University of Lubumbashi, Lubumbashi, Democratic Republic of the Congo; 5Department of Pediatrics, Faculty of Medicine, Mbujimayi Official University, Mbujimayi, Democratic Republic of the Congo; 6Department of Tropical Medicine and Infectious Diseases, Faculty of Medicine, University of Kinshasa, Kinshasa, Democratic Republic of the Congo
Correspondence: Criss Koba Mjumbe, Email [email protected]
Background: This study was carried out in East Kasai Province, DR Congo, to explore the perceptions, challenges, and barriers associated with HIV/AIDS care. The aim was to understand perceptions of HIV/AIDS, identify barriers, and analyze the factors influencing the effectiveness of care.
Methodology: This study involved semi-structured interviews with healthcare professionals and focus group discussions with PLWHA.
Results: Several contrasting perceptions of HIV/AIDS were revealed, ranging from disease stigma to some acceptance of antiretroviral treatments, although hesitation remains among the population due to cultural beliefs and misinformation. The main challenges identified include dietary problems, side effects, drop-outs, failure to keep appointments, superstition and uninformed travel of patients. Patients often have difficulty gaining access to healthcare facilities because of distance, transport costs, and a lack of financial means. In addition, drug shortages in health facilities exacerbate the situation. Sociocultural barriers also play a major role. Stigma and discrimination against PLWHA are still visible, and these negative attitudes can dissuade individuals from being tested, adhering or adhering to treatment. In addition, superstitions and myths about treatment fuel mistrust and hesitation toward treatment. Healthcare providers face difficulties in managing patients due to limited resources and a lack of ongoing training on new therapeutic approaches.
Conclusion: This study highlights the many challenges that need to be overcome to improve HIV/AIDS care, particularly in terms of accessing care and combating stigma. To improve the effectiveness of health programs, an integrated multisectoral approach involving communities, health authorities and international partners is crucial. This will help overcome existing barriers and ensure equitable access to care while reducing the impact of HIV/AIDS.
Keywords: perceptions, challenges, barriers, care, HIV
Introduction
Acquired immunodeficiency syndrome (AIDS) is a global public health problem and one of the leading causes of death worldwide. The management of HIV/AIDS remains a major public health challenge, despite significant advances in recent decades. The perceptions, challenges, and barriers associated with managing the disease vary considerably according to cultural, economic, and geographical context, which has a direct influence on the effectiveness of interventions.1,2
According to UNAIDS, in many regions, HIV/AIDS is still associated with considerable stigma. This stigma is at the root of people’s discouragement from being tested, disclosing their status, or seeking care for fear of judgment or discrimination.3,4 Misconceptions about HIV transmission and the effects of treatment are also common, reinforcing the need for education and awareness programs to change mentalities.3,5–7
Managing HIV/AIDS involves many complex challenges, among which adherence to antiretroviral therapy (ART) is one of the most critical. To maintain an undetectable viral load, patients must adhere scrupulously to their treatment regimen, which can be difficult because of side effects, economic difficulties, and a lack of social support.8 In addition, healthcare systems in many developing countries often lack adequate resources, limiting access to medicines, screening tests, and quality healthcare.1,9 It is also clear that there are numerous and often interconnected barriers to the effective management of HIV/AIDS. Economic barriers include the cost of drugs, consultations, and travel to health centers. Sociocultural barriers, such as stigma and gender norms, can also deter individuals from seeking care.8,10,11 Finally, structural barriers, such as ineffective health policies and inadequate infrastructure, further complicate access to prevention and treatment services.12
The aim of this study was to explore perceptions, identify barriers and analyze challenges related to access to HIV/AIDS care in Mbujimayi to better understand the sociocultural, economic and structural factors influencing the care of PLWHA.
Materials and Methods
Study Framework
Located in the center of the Democratic Republic of Congo, Mbujimayi is the capital of East Kasai Province, one of the provincial entities enshrined in the Republic’s 2006 Constitution. It is located 930 km from Kinshasa, the capital of the Democratic Republic of Congo. As the provincial capital, Mbujimayi is the seat of East Kasai’s provincial institutions.
Type of Study
We conducted a qualitative study to document the factors that may influence appropriate ART adherence among PLWHA.
Study Population
In the semi-structured interviews, we interviewed healthcare providers, and in the focus group discussions, we interviewed PLWHA on ART, with respect to their age and gender.
Study Eligibility Criteria
The inclusion criteria for study participants were individuals to meet the following conditions: all HIV patients on ART who provided informed consent to participate in the focused discussion and who were not ashamed to disclose their serostatus, as well as healthcare providers trained and involved in HIV/AIDS management.
Sampling
PLWHA on ART were subjected to focus group discussions (FGDs). These FGDs were carried out until saturation was reached, with 4 FGDs. Healthcare providers were subjected to semi-structured interviews.
Techniques and Instruments
The qualitative approach combined individual interviews with healthcare providers and focus group discussions with PLWHA to understand the reasons for good or poor treatment adherence and to document perceptions of antiretroviral treatment.
Semi-Structured Interviews
We conducted individual interviews with the most senior healthcare providers working in antiretroviral treatment facilities, as well as with peer educators. The interviews were conducted in the language of the interviewee’s choice and according to their availability at the location of their choice. An interview guide was used as a support with the following themes: duration in the care of PLWHA, training and retraining on HIV/AIDS, practice of the care protocol, obstacles and challenges. These FGDs were carried out until saturation was reached, and we reached saturation with 4 FGDs in care, viral load and providers’ expectations for treatment. The interviews were recorded on digital media.
Focus Group Discussion (FGD)
We organized FGDs with PLWHA. The FGDs were held in a quiet room, either at the hospital or wherever the PLWHA wished, and were conducted in the local language, Tshiluba, and digital media was recorded. These FGDs were carried out up to the saturation point, and we reached saturation with 4 FGDs. The men were separated from the women. For this purpose, we used a focused discussion guide that addressed the following themes: knowledge of the disease and means of prevention (condoms), therapeutic adherence, condom use, degree of satisfaction, and the concept of viral load.
Techniques for Processing and Analyzing Data
The data were recorded on a recording device, transcribed using Microsoft Word 2019 and then transformed into plain text format. These textual data were analyzed using Atlas.ti® Qualitative Data Analysis software version 6.1.1 (Scientific Software Development GmbH Berlin, Germany). Translation and transcription of FGD audio and semi-structured interviews in the Tshiluba language into French were carried out, and all the transcripts were edited for translation clarifications. Codes were developed on the basis of themes from the individual and group interview guide. Additional codes were added during the coding process as needed.
Conceptual Models
Health Belief Model
The Health Belief Model (HBM) was developed to explain acceptance or non-acceptance of screening for asymptomatic diseases, behaviors associated with disease prevention, medical treatment adherence and health behaviors such as lifestyle habits. Referring to the Health Belief Model, an individual is likely to accept correct adherence to antiretroviral treatment if he or she possesses minimal health knowledge and considers his or her health to be an important component of his or her life. The determinants that drive them to act are: the perception of a threat to their health, combining vulnerability to HIV and the perception of the seriousness or consequence of HIV. Many people do not feel at risk despite the high prevalence of HIV due to a lack of information or cultural believes (perceived susceptibility), and HIV may be perceived as a shameful or incurable disease, leading to denial or avoidance of screening. Conversely, some believe that treatment is sufficient, reducing the urgency of prevention (perceived seriousness); social stigmatization, discrimination and lack of knowledge and traditional or religious believes hinder understanding of HIV and treatment (perceived barriers).13–15
We will use this conceptual model in the discussion section of our work to better understand why the at-risk population does or does not accept HIV testing and treatment (See Figure 1).
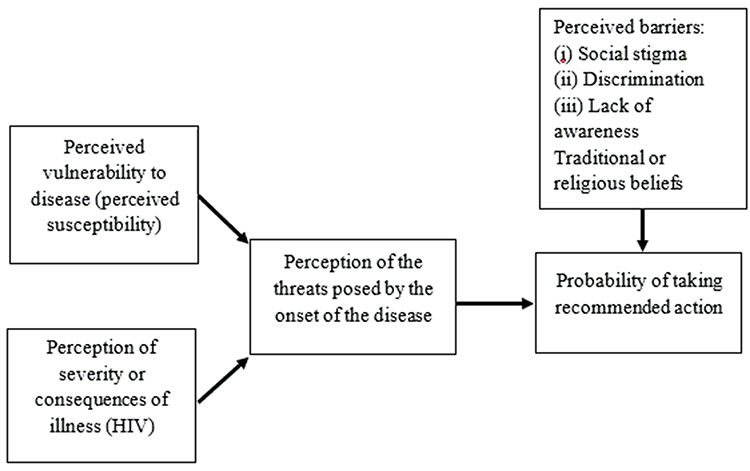 |
Figure 1 Adapted BECKER’s health belief model (1974). |
Precede-Proceed Model
The Precede-Proceed Model (PPM) is one of the intervention planning and evaluation models used in health promotion to improve the quality of life in communities. PPM is an ecological approach to health promotion. We will use the PPM as an organizing framework to translate our findings into an HIV-related health promotion approach to help reduce HIV-related mortality and morbidity in communities. This nine-step model is subdivided into two main parts: planning and evaluation (See Figure 2):
- Planning (steps 1 to 5): this part begins with the social diagnosis of the quality of life in the community which consists of identifying the major concerns of local communities: HIV stigmatization, poverty, post-conflict instability, limited access to care (step 1); epidemiological diagnosis (step 2), which defines key indicators; environmental and behavioral diagnosis (step 3), which defines intervention objectives and identifies risk behaviors (non-use of condoms, low level of voluntary testing, viral load testing) and environmental factors such as the lack of specialized laboratories at provincial level, and lack of ongoing training; the educational and ecological diagnosis (step 4), which includes predisposing factors (lack of information, cultural believes and superstition), factors to be reinforced and factors favoring health promotion; and the administrative, political and organizational diagnosis (step 5), which defines local policies, available resources and institutional capacities for health promotion.15,16
- Evaluation (steps 6 to 9): step 6 is the implementation of health promotion activities (awareness-raising, condom distribution, capacity-building) and steps 7, 8 and 9 evaluate the process, impact and results of health promotion.15,16
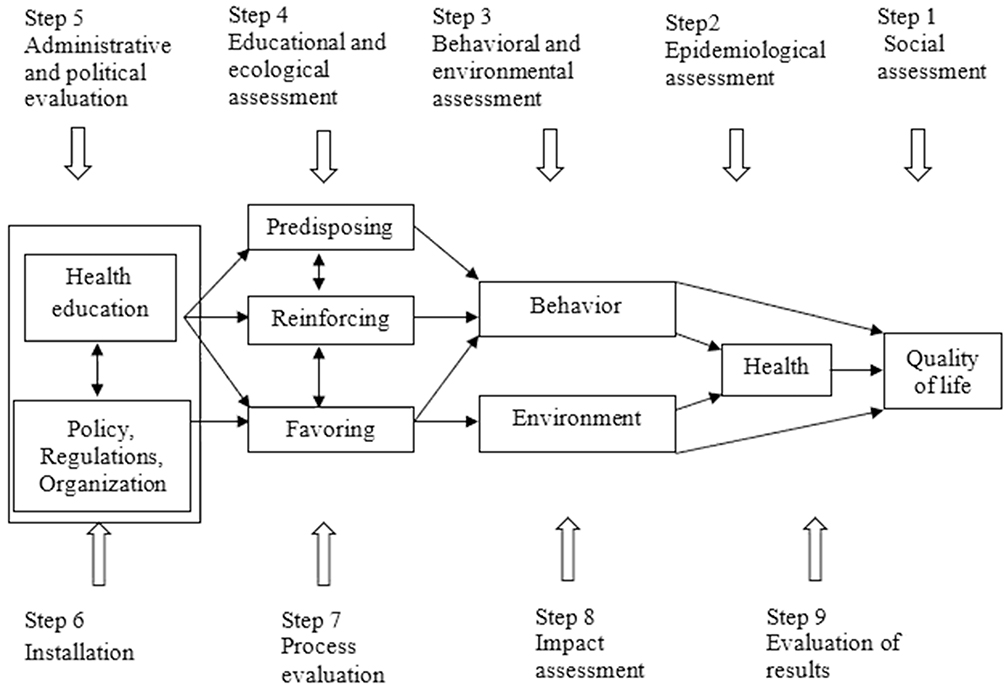 |
Figure 2 Visual representation of the Precede-Proceed planning model. Source Green and Kreuter,1999. |
In this study, we focused specifically on step 3, addressing behavioral aspects, and step 5, concerning local policies. We believe that the components provided a solid foundation for the discussion of our finding. The remaining steps of the model may be explored in future research.
Ethical Consideration
Ethical clearance was sought from the ethics committee of the Official University of Mbujimayi. Free and informed consent was used in both French and Tshiluba (the local national language) and was given/read to participants before the questionnaire was administered. For participants aged between 15 and 17 years, a parental authorization form was drawn up and made available to parents to give them access to the study, and at the same time, the assent form was also drawn up and made available to them before the questionnaire was administered. This consent form must respect the principles of all medical research, ie, the protection of human life, health, dignity, integrity, the right to self-determination and the confidentiality of the information of the persons involved in the research. The ethical regulations outlined in the Declaration of Helsinki were followed throughout the study. Data collection began only after the ethics committee had given its approval. Face‒to-face interviews involved only the interviewer and the respondent for confidentiality reasons. Verbal informed consent with details about the publication of anonymized responses/direct quotes was obtained from the study participants and this process was acceptable and approved by the ethics committee. The data were stored on a password-protected laptop in a locked cabinet, and only the principal investigator and study supervisor had access to the data.
Results
To document perceptions of HIV/AIDS care, we conducted 4 FGDs with PLWHA and 16 individual interviews with healthcare providers.
Several themes emerged from these individual and group interviews, which we present in 7 headings: (1) knowledge of the disease, (2) perceptions (3) degree of adherence, (4) condom use, (5) barriers (to adherence and viral load testing), (6) factors influencing the availability of services, and (7) perceived factors for improving care.
Characteristics of Participants in Individual and Group Interviews
This table shows the sociodemographic characteristics of the participants in the FGDs and semi-structured interviews. The average age of the participants was 39.5 years (34–44.5) for female participants and 48.5 years (35.5–61.5) for male participants. The median age of healthcare providers was 49.5 years (47–53) for female providers, with a median age of 9.5 years (7–16) of experience in care, and 48.5 years (43–57) for male providers, with 6.5 years (5–10) of experience (Table 1).
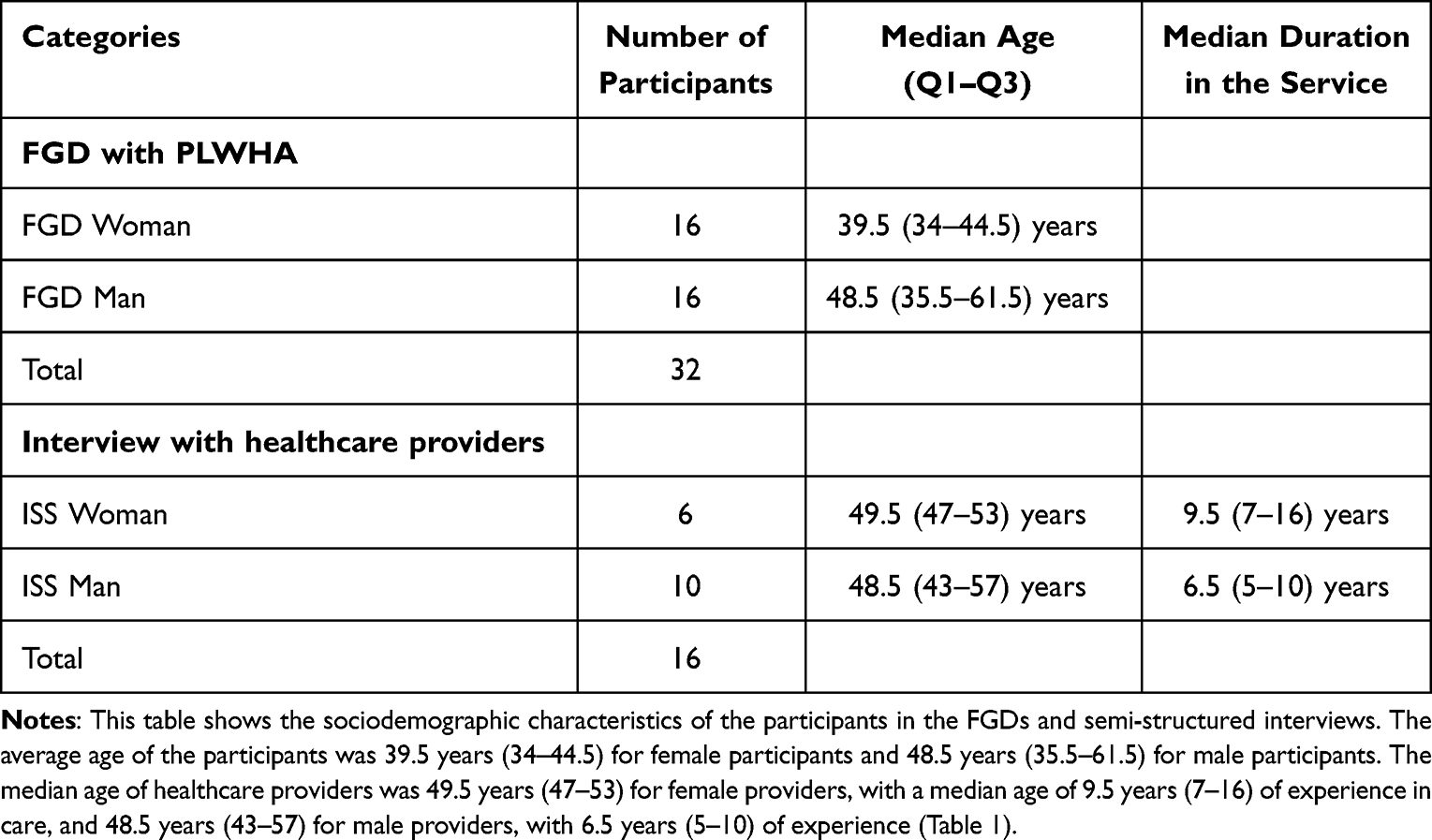 |
Table 1 Sociodemographic Characteristics of Participants in the FGDs and Individual Interviews |
Knowledge About HIV/AIDS
Knowledge of the Disease
In general, PLWHA know much about HIV/AIDS. They define the disease as an acquired immunodeficiency syndrome. The most frequently cited symptoms are weight loss, diarrhea, prolonged fever, and decreased immunity, leading to the onset of other illnesses. The patients also described the disease in Tshiluba, the local language spoken in Mbujimayi, as follows: “Disama dia budi buend’ebu” and/or “Disama dia maleta anayi”, which means the disease of the century or the present and/or the disease of four letters (AIDS). They also explained the various means of transmission, which are sexual, sharp-edged pricks and the horizontal route from the infected mother to the child.
HIV/AIDS is an acquired immunodeficiency syndrome caused by HIV that can be transmitted sexual contact, injections with infected objects, and through transmission from an infected mother to her child during childbirth. (FGD, Woman 10)
Some of them mention other means of transmission, such as sweating or breast milk, which they believe occur when there is a high level of viremia.
HIV can also be transmitted through sweat and breast milk when the viruses are so high and numerous in the body. (FGD, Woman 6)
Healthcare providers have practical knowledge of counseling, postexposure prophylaxis for children of HIV-positive mothers, the attitude to adopt in the case of discordant couples where counseling is performed as a couple, and the sharing of results, which is always done separately while respecting confidentiality. Providers tell us that they always ask the couple to share information with each other. Counseling is often performed in two ways, ie, pretest counseling and post-test counseling, precisely when the provider already has results. They also say that during these counseling sessions, the explanations given to the couple are part of the preparations for accepting the results in the event of a positive test.
The healthcare providers gave us the various steps involved in confirming positive results. A battery of tests is performed to ensure that the person is infected. The different tests were performed in the following order: (1) Determine HIV, (2) HIV ½ Stat Pak, and (3) Uni Gold HIV.
Screening begins with the patient’s free and informed consent, followed by the test’s performance (Determine HIV, HIV½ Stat Pak, Uni Gold HIV, etc.). If the result is positive, the provider announces the result and shows the importance of ART, and if the agrees to take the treatment, he will be referred to the person in charge. (INT, Provider 1)
They say that counseling of the pregnant Woman is done only at the prenatal consultation and that all the counseling steps are also respected. Explanations on the test pathway, on the type of result expected, are also given to the person as well as the importance of preventing mother-to-child transmission if the result is positive. In pregnant women, the tests used are as follows: (1) Duo-test and/or Determine HIV, (2) HIV ½ Stat Pak, and (3) Uni Gold HIV.
With the new test (Duo test), especially in pregnant women, we do counseling by advising the Woman to show her the effects on prevention for the child. (INT, Provider 16)
All healthcare providers also provided procedures for postexposure prophylaxis in newborns of infected mothers. The procedure reported by the providers is as follows: (1) For a child under 18 months of age, we perform the test, and if it is positive, we also consider the viral load. Prophylactic treatment, which involves nevirapine, will be given to the child, and some providers add that we can give isoniazid to this child. (2) For a child over 18 months of age, we will perform the test, and if it is negative, we will conclude that it is just maternal antibodies and that we will stop the treatment; if it is positive, we will continue with the treatment.
Concerning the discordant couple, all the providers gave us a pathway in such a situation where one of the partners is positive. They told us that this is a situation they encounter a lot in their services. In such a situation, we do the counseling, the results are given separately to the couple, and we always ask the couple to share the information with each other to avoid problems within the couple.
First, we have to do the test separately for each couple, and the result will be given individually and we’ll ask the partner if they could share the result between them, but there’s the couple who agrees to share and there’s another couple who doesn’t agree to share, but we always ask them to share the information. (INT, Provider 10)
Perceptions
Perceptions of Care
In general, providers stated that each time the management protocol is renewed, they are informed through participation in training, briefing sessions or circular notes. Some providers mentioned that they self-train by using the focal point for the retrieval of renewed management protocols to deepen their knowledge.
Every time there’s a new protocol, I’m called in for training (INT, Provider 1) … We’re brought up to speed by the central office through briefings to inform us about the renewal of the management protocol. (INT, Provider 4)
All providers affirm that they follow the management protocol correctly, applying all the algorithms for confirming results and therapeutic regimens. On the other hand, some providers say that they are still encountering difficulties in their management. They claim to be making efforts to improve their services by referring to experienced providers.
We follow the protocol, but small mistakes are bound to happen, and in this respect, we always make an effort to improve. (INT, Provider 15)
In general, we found that all PLWHA know about antiretroviral treatment and its importance for their health. They affirm that treatment is free and must be taken regularly every day for life. They also say that this treatment helps us to recover our health.
HIV/AIDS treatment is essential for our well-being and helps us to regain our health (FGD, Woman 2) … First, the drug is free and was given it in sufficient quantity to improve our health and control our viral load. Second, the treatment must be taken regularly and for life. (FGD, Man, 11)
Perceptions of Therapeutic Adherence
Overall, all the participants said that adherence to treatment is useful and helps reduce the viral load. They also reported that adherence helps avoid resistance to antiretrovirals. They also affirmed that patients must adhere to treatment properly for good progress.
Care providers affirmed that adherence to treatment is the key to viral load suppression and/or undetectability. As long as patients adhere correctly to treatment, there will be no resistance to antiretrovirals, the patient will be able to live as if disease-free, and his or her lifespan will also increase. They will no longer contract opportunistic diseases, as their immunity is strengthened by good compliance with treatment, and transmission of the virus will be virtually nonexistent.
Patients must adhere correctly to treatment to avoid the onset of resistance and to reduce the viral load. (INT, Provider 10)
The focus group discussions with PLWHA show that they are concerned about the fact that they have to take antiretrovirals every day to feel well. They are aware that they have to take their treatment correctly to suppress their viral load and avoid transmitting the disease.
We are obliged to always take the products daily and correctly, because it is for our own good and we can avoid transmitting the disease. (FGD, Woman 1)
In general, all PLWHA say that if treatment is not followed correctly, several consequences will occur. There are several consequences, the most cited being (1) failure to suppress the viral load, (2) worsening of the disease and (3) death. All these consequences have been grouped into three categories (personal, family and community) as follows:
- Personal: reduced immunity, weight loss, worsening of the disease and death;
- At the family level, the person will be a burden on other family members; in the long run, the family will tire him/her and reject him/her. If the person is the head of the household, his or her illness will prevent him or her from providing for the family;
- At the community level, if a person does not receive treatment properly, the viral load will always remain high, and the person could be a source of contamination for other members of the community.
At the individual level, the person will not be in good health, he will lose a lot of weight, and he may return to his pretreatment state and even die [.]; at the family level, the person will be a burden for others and abandoned by his family, and if it is a person who provides all for the family, there will not be good survival of the family because he will not know how to properly take care of his family. (FGD, Woman 8)
With respect to patients who fail to comply with treatment, all the providers said that they continue to advise and raise awareness among patients of the need for compliance. They also affirm that the moment a patient abandons correct medication, there will be a rebound in viral load, leading to a resurgence of opportunistic infections.
We make patients aware of the consequences of noncompliance. (INT, Provider 6)
Perception of Viral Load Achievement
All providers claim to know something about the viral load. They state that the viral load is an indicator of patient follow-up, a necessary means of evaluating their services. They also say that this test is carried out on patients who have been on ART for 6 months; the period during which it is carried out ranges from 3‒12 months, depending on the case.
Viral load helps us assess our performance in terms of patient management if the viral load has been suppressed or is in the process of being suppressed. (INT, Provider 16)
According to PLWHA, the viral load is a useful test for determining the level or number of viruses in the body. They also say that this test is necessary to ascertain whether the disease is progressing well or not. They say the test is performed within 6‒12 months.
The viral load helps to determine whether the viremia has increased or decreased and whether patients are taking their medication correctly or not (FGD, Woman 2) … The viral load is carried out when you are already on treatment and within 6‒12 months. (FGD, Man 9)
One provider stated that he did not know exactly when the viral load would be carried out. The reasons given are (1) the fact that they have not been made aware of the algorithm for performing the viral load, due to nonparticipation in training and/or briefings on the different themes of HIV/AIDS management, and (2) the fact that they are underinformed.
For the viral load, we have only recently been informed about the viral load test, and I would not know how to give an answer for a topic that has not yet been tested. (INT, Provider 2)
Degree of Therapeutic Compliance
In general, providers say that the degree of compliance is obtained by subtracting the quantity of product remaining from the quantity received. This calculation is performed by the provider during the patient’s visit. After calculation, if the rate was 90%, the patient missed 3 days of treatment.
With regard to missing a day’s medication, some providers claim that there is good adherence and/or compliance. In this case, they say it is important to look for the various causes behind the forgetfulness.
We remind patients to always take the medication, and we ask them not to take 2 tablets to make up for the delay either. (INT, Provider 11)
Other providers believe that missing a day’s treatment makes patients noncompliant. They also say that patients do not take their medication on purpose. They also say that they look for the cause of noncompliance.
In my opinion, the person is in the wrong category because he is deliberately not taking the product, so it is poor compliance. (INT, Provider 15)
Using Condoms
We found that some focus group participants said they had accepted the use of condoms after receiving repeated advice from providers to avoid coinfection, superinfection and unwanted pregnancies. One participant said that, at first, he was unaware of her husband’s illness and refused to have sex when she needed it, whereas her husband, already aware of his serostatus, had hidden it and avoided contaminating his partner. When she learned of the disease, she decided to use a condom because she had also become ill.
At first, I did not know my husband had the disease, and he did not want us to have sex regularly, but once I knew he had the disease, we only started using condoms. (FGD, Woman 5)
It does not bring sexual pleasure, but we only try to use it. (FGD, Man 5)
Some PLWHA said that they did not accept condoms, citing a lack of satisfaction during intercourse as the reason. Some participants mentioned the idea that those who do not want to accept and/or use condoms should abstain to avoid all the consequences of not accepting and using condoms.
For himself, he must avoid sexual intercourse if he is single; for the community, he must abstain. (FGD, Man 14)
With respect to the degree of satisfaction with condom use, the participants said that condoms do not increase satisfaction during sexual intercourse as they do during unprotected intercourse, but they use them just for protection.
The only drawback we find is the lack of pleasure; it does not give me the same satisfaction when we do not use it, that is why my husband does not like to use it yet. (FGD, Woman 3)
In general, all PLWHA claim to prefer male condoms to female condoms. They say that the male condom is easier to use than the female condom.
The male condom is easy to use. It needs just to remove the wrapping. The man have to put it on his penis without difficulty. The penis must be erect. (FGD, Woman 9)
Barriers
Barriers to Therapeutic Adherence
In general, all PLWHA affirmed that there are factors that prevent them from complying with their treatment regimens. These factors cited by patients are (1) insufficient food, (2) forgetting to take medication, and (3) untimely drug shortages in health care facilities.
If we do not eat enough, we will not take the products, and sometimes we forget to take the medicine, and if there are no medicines in the hospital. (FGD, Woman 3)
Providers also assert the existence of factors that prevent patients from complying with treatment. These factors are (1) the occurrence of adverse effects, (2) ignorance, (3) poor preparation before starting treatment, (4) the duration of treatment, (5) religious (superstition) and/or cultural beliefs, (6) stigma, (7) shame or not coming out of hiding, (8) providers not respecting confidentiality, (9) poverty, (9) a long distance to travel, (10) allergy to product components, (11) cost of care and (12) complexity of dosage.
Religious belief, stigma, shame and ignorance, poor preparation (counseling) before starting treatment” (INT, Provider 5).” Ignorance, occurrence of adverse effects, cost of care, long distance to travel, complexity of dosage, duration of treatment, evolution of symptoms, belief, poverty and stigma. (INT, Provider 16)
Barriers to Viral Load Testing
In general, PLWHA say that providers expect providers to determine the viral load rate. They also say that providers prefer the following: (1) for those with a falling viral load, they encourage them to continue treatment as usual without giving the rate; (2) for those with a high rate, or who initially had a fall but have risen again, providers call them in for an awareness session and advise them to resume treatment correctly. With this approach, patients say that they are discouraged from taking blood samples for this test.
We’re only told that it is fine and to continue taking the product as usual, without being told whether the load is suppressed or undetectable, and this sometimes discourages us. (FGD, Woman 3)
Another participant stated that he had taken part in an education session on adherence to treatment and followed a testimony from one of them who had not complied with the treatment, and the provider had not given him the result but had just given him advice on good adherence to treatment with the aim of suppressing the viral load.
Once we called another person to tell him that he was not taking his treatment properly because his load was high, and he came to our meetings to tell us that I was not taking the medicine normally yet because I did not have any food, and we advised him again to always take his treatment regularly. (FGD, Woman 7)
Factors Influencing Service Availability
Challenges to Care
All the providers affirmed that there are certain challenges to be met to provide good care. These challenges include (1) the problem of insufficient food, (2) the problem of side effects, (3) the lack of inputs and cartridges at the provincial laboratory for viral load testing, (4) staff training or retraining in new approaches to HIV/AIDS, (5) sensitization and availability of inputs and medicines, (6) dropouts and people lost to follow-up, (7) precariousness of patients, (8) failure to keep appointments, (9) disorientation of patients owing to superstition on the part of pastors and fetishists, and (10) uninformed displacement of patients.
We have to ask certain pastors and fetishists to allow patients to become disoriented and not take their medication, on the pretext that the illness is not real. (INT, Provider 9)
Obstacles to Care
In general, providers say that there are certain factors or obstacles that prevent patients from being properly cared for. The most frequently cited were (1) the unavailability of inputs (DBS) and GeneXpert cartridges, (2) the unavailability of results for samples sent to Kinshasa or Lubumbashi for analysis, (3) side effects, (4) the problem of moving patients, (5) recurrent shortages of ARVs, (6) nonadherence to ART, (7) the high level of precariousness, (8) refusal to take medication correctly because of superstition, (9) forgetting to take medication because of negligence, and (10) refusal to share results with one’s spouse.
We see many obstacles, such as treatment abandonment, lack of confidence, frequent breakages, forgetfulness, precariousness, sending samples to Kinshasa for analysis and unavailability of results. (INT, Provider 4)
All providers cited the lack of availability of results as the most important element missing from patient follow-up. This unavailability occurred because all the samples were sent to Kinshasa or Lubumbashi for analysis. They also say that fewer results are made available, making it impossible to see how each patient is progressing.
Regarding viral load testing, it’s truly difficult to do; we can take the samples and send them to Kinshasa, but the results do not reach us. (INT, Provider 3)
Despite the unavailability of viral load results, providers reveal that if a patient adheres correctly to his treatment, we are certain that his viral load will be suppressed or undetectable
There are patients who suppress their viral load and others who do not. We have observed that most patients who have not suppressed do not adhere to treatment, or there are patients who have gone on to take other strains. (INT, Provider 7)
Some providers reveal that there is already discouragement and dissatisfaction among patients who have not received their previous test results. They also say that these patients are sometimes beginning to object to further sampling for the purpose of another viral load analysis. Some providers deplore the fact that their facilities are not authorized to take viral load samples and are obliged to send patients to authorized facilities, resulting in a lack of trust.
It is an examination that has already discouraged us, because we take samples but we never get the results, and every time we encounter a delicate problem because we have patients who ask to have the viral load done, but the difficulty we encounter is sending patients to hospital for sampling, which the patients do not want. (INT, Provider 10)
For reaching the 95-95-95 targets, all the providers say that, for the moment, it is difficult to achieve these objectives because the only problem lies in following up with patients because of the unavailability of viral load tests.
The problem will only remain that of monitoring patient via the viral load. How can we assess patient progress without this very important and indispensable test?. (INT, Provider 14)
Perceived Factors for Improving HIV/AIDS Care
In general, the participants (providers and PLWHA) listed several factors that they perceived as effective ways of improving HIV/AIDS care in Mbujimayi. They believe that if these factors are considered, there will certainly be an improvement in HIV care.
The most frequently cited factors are as follows:
- Make the provincial laboratory operational by making sufficient inputs (cartridges, sampling materials) available for any onsite viral load analyses;
- Make inputs available (tests, condoms, and drugs, especially pediatric drugs) to prevent shortages;
- Increase refresher training for providers on new approaches to HIV/AIDS care and train other providers in facilities lacking qualified personnel;
- Organize and perpetuate therapeutic compliance education sessions;
- The organization of good counseling by providers to facilitate treatment adherence;
- Make drugs available for opportunistic infections;
- Availability of protective inputs such as gloves and masks;
- Provide incentives in terms of remuneration for service providers;
- Provide patients with financial support, as the majority of patients are unable to create income-generating activities;
- Make short-term treatment available, as in the case of tuberculosis, or provide patients with treatment to be taken at least once a month or once a year to avoid treatment dropouts and those lost to follow-up;
- Providing nutritional care for PLWHA to ensure good treatment adherence;
- Make viral load results available and communicate them to those concerned (PLWHA);
- Continuously test for viral load levels.
We need to provide our laboratory with a GeneXpert machine and cartridges for our machine to ensure proper patient follow-up; we also need to make sufficient inputs and tests available. (INT, Provider 8)
We need the test to continue, but we’re told that there are no DBSs for sampling, and we want them to start giving us flour and oil, that the World Food Program (WFP) used to give us. (FGD, Man 2)
Discussion
This study highlights the following points: the perceptions and barriers to HIV care that influence the availability of services, as well as the perceived factors for improvement, were also listed by the participants, notably, the problems of moving patients, recurrent shortages of ART, nonadherence to ART, sigma, a high level of precariousness, refusal to take medication correctly because of superstition and forgetting to take medication because of negligence.
With respect to perceptions of treatment adherence, we found in our series that participants stated that they were aware of the benefits and advantages of treatment adherence. They noted that it is useful for reducing the viral load and preventing resistance to antiretrovirals.
In our series, we found that nonadherence led to no suppression and/or increased viral load, worsening of the disease and possibly death. At the same time, we affirmed that they had been made aware of and advised on therapeutic adherence.
In some African studies, the authors claimed that social support outside the healthcare setting was effective for ART initiation.10,11,17 Other studies confirmed that social support related to ART initiation, adherence, and retention associated with the disclosure of men’s HIV status to their partners was important and facilitated a range of partner support.17,18 In a study conducted in Iraq, the main reasons cited for noncompliance were forgetting to take the medication at the scheduled time, traveling, probably due to distractions and stress related to being away from home, running out of medication while traveling, the unavailability of HIV medications in Iraqi hospitals, family emergencies also playing a crucial role in missed doses, side effects, and difficulties in renewing prescriptions.19 On the other hand, some factors motivating treatment adherence that were mentioned included the desire to live a healthy life, fear of premature death, positive and promising laboratory results, and family factors such as social support, the intention to have children, and the desire to protect one’s relationship.19
Regarding the perception of the viral load, in our study, we found that participants affirmed that their knowledge of the viral load was a key indicator for patient follow-up. This test can be carried out between 3 and 12 months depending on the case.
Perceived success in viral load suppression was almost universal among those who reported knowing their viral load.20 Some authors did not assess participants’ experience with viral load testing accurately because of their limited knowledge.17,20–23 Some authors have shown that a suppressed viral load was seen by participants as a predictor of good health and adherence. Despite this perception, some patients are confused and upset when faced with viral load failure, and viral load results are often poorly understood, particularly when failure is detected despite good adherence, a situation that has challenged the patient–provider relationship.21,24 Pita et al reported that most PLWHA had some understanding of the viral load, but they often confused CD4 counts with the viral load, as well as the meaning of a positive result. This confusion among PLWHA was clarified by nurses.25
In our work, we found that all participants affirmed the existence of barriers that would be at the root of nonadherence. The most frequently cited are adverse effects, lack of food, forgetfulness, drug shortages at facilities, ignorance, length of treatment, religious and/or cultural beliefs, stigma, shame or not coming out of hiding, providers not respecting confidentiality, poverty, and a long travel distance. Our results corroborate the observations of some authors that barriers and challenges to improving adherence among patients.8,19,23,25 Other authors have reported that the inclusion of personal religious beliefs in the provision of healthcare to PLWHA has led to a conflict between personal religious values and professional expectations.8,26 Patient mobility and emigration have also been shown by providers to undermine targeted adherence efforts.20
In our study, all the participants listed various barriers to performing viral load tests. The most frequently cited limitations were the lack of inputs for sample collection, the lack of cartridges for the provincial laboratory, and the delay in obtaining results. Despite the unavailability of viral load results, providers revealed that if compliance is correctly observed, they expect that the viral load is suppressed and/or undetectable When viral load results are not available, providers advise patients to continue therapeutic adherence, which ensures that the viral load is suppressed.
Some studies have claimed that providers view viral load education as a tool to increase engagement in care. Viral load monitoring and counseling have been reported to increase patient and provider knowledge about viral load.20–22 They also reported that rapid results enabled early intervention with patients facing treatment failure or poor ART adherence.22 The unavailability of viral load inputs in the laboratory hinders the proper follow-up of patients. This same finding was reported in studies carried out in Mozambique and Kenya, where the authors reported shortcomings in the test reagent supply chain.21,22 Given that the provincial laboratory has a GeneXpert® device and the lack of cartridges for viral load analysis, it is imperative that the cartridge be made available for the proper monitoring of patients in a context with limited resources such as ours.
In our study, the providers mentioned the various challenges they had to provide care. The most frequently cited problems were insufficient food, side effects, lack of inputs and cartridges at the provincial laboratory for viral load testing, staff training or retraining on new approaches to HIV/AIDS, awareness-raising and availability of inputs, patients abandoned and lost to follow-up, patients’ precariousness, failure to keep appointments, disorientation of patients due to superstitions on the part of pastors and fetishists, and uninformed displacement of patients.
Some studies have reported that providers and patients expressed the same challenges related to care. Repeated HIV testing, stigma, nondisclosure of HIV status, misconceptions about ART, and population mobility were also cited.1,4,8,20,24,27–32 Drug stock-outs present challenges for longer refills and interfere with drug refills.19,20 Some studies have concluded that patients prioritize their basic needs, such as finding ways to survive, over keeping appointments with providers and their medications.1,20 Certain challenges, such as the aging of people living with HIV as a factor increasing ART-related fatigue, polypharmacy in people with multiple chronic diseases, and the overall long duration of ART, are raised by nurses and policy/implementation actors.25
Fear of HIV-related stigma has been well documented in the literature presented in this study as a barrier to engagement in HIV care.
The most frequently cited barriers to treatment in our study are the unavailability of inputs and cartridges, the unavailability of results, side effects, the problem of patient travel, recurrent drug shortages, the unacceptability of ART, the high level of poverty, the refusal to take medicines correctly, forgetting to take medicines and the refusal of spouses to share results.
Some authors have pointed to barriers linked to access problems and limitations to social security and low socioeconomic status, lack of trust in providers and information about medicines, and difficulty in tracking mobile or migrant patients.1,20 Some authors have reported that delays in communicating viral load test results to patients are among the factors that have hampered patient flow and the effectiveness of care. They also reported that a one-month breakdown of the central laboratory’s machines led to delays in testing and required the rescheduling of many patient follow-up visits.33 This is also observed in our setting, where tests are performed centrally and take time due to the nonfunctioning of the provincial laboratory. Unfortunately, in the absence of an established notification system, patients continue to visit the clinic despite the unavailability of results. The authors suggested that providers use SMS to facilitate faster communication of results.33 Some authors have suggested that reducing obstacles and/or barriers to care is a goal that often includes community-based HIV testing, rapid ART initiation, cell phone assistance, and viral load-sensitive care.34–36 These findings highlight the importance of retaining other elements, including training to improve patient‒clinician relationships, providing care for other non-HIV conditions and improving patient and clinician knowledge about HIV.11,20
To improve HIV/AIDS care, our study identified several factors, including the operationalization of the provincial laboratory, the availability of medicines and supplies, the retraining of healthcare providers, awareness-raising, the availability of motivated healthcare providers, nutritional care, and the availability of viral load results. Some authors have made several recommendations to improve care for HIV patients, including the creation of a dental clinic within the HIV center, strengthening confidentiality for people with AIDS, the need for a continuous supply of medication, the introduction of a special identity card to facilitate access to care for AIDS patients, and access to a psychiatrist for their support.19
Conclusion
This study on perceptions, challenges and barriers to HIV/AIDS care in Eastern Kasai province highlights the complex and multidimensional obstacles faced by people living with HIV in the province. Despite progress in treatment with ART, access to care remains limited. In addition, stigma, misinformation surrounding HIV and deeply rooted cultural beliefs further complicate prevention efforts and lead to resistance for HIV testing, treatment initiation and better treatment adherence. Perceptions of HIV/AIDS which is influenced by cultural beliefs and myths, contribute to people’s reluctance to be tested or to take ART. The lack of ongoing training for health workers, shortages of supplies and drug shortages also complicate effective management. Considering these findings, it becomes evident that policy responses must evolve beyond technical solutions to embrace community-based perceptions and needs, culturally grounded interventions. Improving care access requires sustained investment in supply chain systems and the reinforcement of local health infrastructure. Equally important is the implementation of targeted awareness campaigns that address stigma and misconceptions through dialog and local ownership.
However, despite these advances, many challenges remain. Factors such as treatment adherence, drug side effects, socioeconomic barriers, and stigma continue to influence the efficacy of viral suppression. The data collected also revealed that some populations, particularly those living in rural or marginalized areas, face additional difficulties in accessing treatment and receiving adequate medical follow-up. To improve HIV/AIDS care, it is essential to adopt an integrated approach that considers perceptions, challenges, and barriers to each context. This involves strengthening awareness-raising efforts, providing adequate economic and social support, and implementing structural reforms to improve access to healthcare. By combining these efforts, we can hopefully reduce the impact of HIV/AIDS and improve the quality of life of PLWHA.
The results of this study offer concrete avenues for public health decision-makers: they shed light on the blind spots in current policies and call for a reconfiguration of interventions based on stories from the field and real-life experiences. By building on existing structures, this work contributes to a better contextualization of HIV/AIDS policies, with a view to equity, sustainability, and social transformation.
Study Limitations
Our study population included PLWHA, a category of patients who are still subject to discrimination and stigmatization. We encountered difficulties in collecting data because of the confidential and stigmatizing nature of the survey. Some patients refused to take part in the survey and/or in the focus group discussions, fearing that their status could be revealed and/or hiding themselves. This led us to turn to care providers to gain the trust of respondents to fill in the missing information. The providers were extremely helpful in our acceptance of the study population.
Abbreviations
AIDS, Acquired immunodeficiency syndrome; ART, Antiretroviral therapy; FGD, Focus group discussions; HBM, Health Belief Model; HIV, Human immunodeficiency virus; INT, Semi-structured interviews; PLWHA, People living with HIV/AIDS, PPM, Precede Proceed Model.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Arnold EA, Weeks J, Benjamin M, et al. Identifying social and economic barriers to regular care and treatment for Black men who have sex with men and women (BMSMW) and who are living with HIV: a qualitative study from the Bruthas cohort. BMC Health Serv Res. 2017;17(1):90. doi:10.1186/s12913-017-2011-z
2. Gwadz M, Serrano S, Linnemayr S, et al. Behavioral intervention grounded in motivational interviewing and behavioral economics shows promise with Black and English-speaking Latino persons living with HIV with unsuppressed HIV viral load in New York City: a mixed methods pilot study. Front Public Health. 2022;10:916224. doi:10.3389/fpubh.2022.916224
3. Kabunga A, Nabasirye CK, Kigingo E, et al. HIV-related stigma among pregnant adolescents: a qualitative study of patient perspectives in Southwestern Uganda. HIV AIDS. 2024;16:217–227. doi:10.2147/hiv.S463506
4. Nakasujja N, Nakigudde J, Lwanga IB, Sezibera V. “I haven’t told other people. I want to keep my dignity”: HIV related stigma among the elderly in Uganda. HIV AIDS. 2024;16:477–484. doi:10.2147/hiv.S480355
5. UNAIDS. Global AIDS Update 2021; 2021.
6. Hlophe LD, Tamuzi JL, Shumba C, Nyasulu PS. Barriers to anti-retroviral therapy adherence among adolescents aged 10 to 19 years living with HIV in sub-Saharan Africa: a mixed-methods systematic review protocol. PLoS One. 2022;17(9):e0273435. doi:10.1371/journal.pone.0273435
7. Nakigozi G, Atuyambe L, Kamya M, et al. A qualitative study of barriers to enrollment into free HIV care: perspectives of never-in-care HIV-positive patients and providers in Rakai, Uganda. Biomed Res Int. 2013;2013:470245. doi:10.1155/2013/470245
8. Fauk NK, Ward PR, Hawke K, Mwanri L. HIV stigma and discrimination: perspectives and personal experiences of healthcare providers in Yogyakarta and Belu, Indonesia. Front Med Lausanne. 2021;8:625787. doi:10.3389/fmed.2021.625787
9. WHO. Global Health Sector Strategy on HIV 2016–2021 Towards Ending AIDS. Vol. 1. World Health Organization; 2016.
10. Camlin CS, Marson K, Ndyabakira A, et al. Understanding the role of incentives for achieving and sustaining viral suppression: a qualitative sub-study of a financial incentives trial in Uganda. PLoS One. 2022;17(6):e0270180. doi:10.1371/journal.pone.0270180
11. Chimoyi L, Chikovore J, Musenge E, et al. Understanding factors influencing utilization of HIV prevention and treatment services among patients and providers in a heterogeneous setting: a qualitative study from South Africa. PLOS Glob Public Health. 2022;2(2):e0000132. doi:10.1371/journal.pgph.0000132
12. Global Health Policy. HIV and AIDS: the path to universal access; 2019.
13. Janz NK, Becker MH. The health belief model: a decade later. Health Educ Q. 1984;11(1):1–47. doi:10.1177/109019818401100101
14. Yarbrough SS, Braden CJ. Utility of health belief model as a guide for explaining or predicting breast cancer screening behaviours. J Adv Nurs Mar. 2001;33(5):677–688. doi:10.1046/j.1365-2648.2001.01699.x
15. Adeyanju OM. A community-based health education analysis of an infectious disease control program in Nigeria. Int Q Commun Health Educ. 1987;8(3):263–279. doi:10.2190/vf7p-xdq1-jn51-ptyl
16. Crosby R, Noar SM. What is a planning model? An introduction to PRECEDE-PROCEED. J Public Health Dent. 2011;71(Suppl 1):S7–15. doi:10.1111/j.1752-7325.2011.00235.x
17. Wiginton JM, Mathur S, Gottert A, Pilgrim N, Pulerwitz J. Hearing from men living with HIV: experiences with HIV testing, treatment, and viral load suppression in four high-prevalence countries in Sub-Saharan Africa. Front Public Health. 2022;10:861431. doi:10.3389/fpubh.2022.861431
18. Mabachi NM, Brown M, Sandbulte M, et al. Using a social support framework to understand how HIV positive Kenyan men engage in PMTCT/EID care: qualitative insights from male partners. AIDS Behav. 2020;24(1):18–28. doi:10.1007/s10461-019-02451-6
19. Talabani SN, Mikhael EM. Exploring adherence, treatment experiences, and quality of healthcare services in HIV management among Iraqi patients: challenges and influential factors. HIV AIDS. 2025;17:227–240. doi:10.2147/HIV.S539087
20. Mwangwa F, Getahun M, Itiakorit H, et al. Provider and patient perspectives of rapid ART initiation and streamlined HIV care: qualitative insights from Eastern African communities. J Int Assoc Provid AIDS Care. 2021;20:23259582211053518. doi:10.1177/23259582211053518
21. Pulido Tarquino IA, Venables E, de Amaral Fidelis JM, Giuliani R, Decroo T. “I take my pills every day, but then it goes up, goes down. I don’t know what’s going on”: perceptions of HIV virological failure in a rural context in Mozambique. A qualitative research study. PLoS One. 2019;14(6):e0218364. doi:10.1371/journal.pone.0218364
22. Qian SRW, Hassan SA, Scallon AJ, et al. “After viral load testing, I get my results so I get to know which path my life is taking me”: qualitative insights on routine centralized and point-of-care viral load testing in western Kenya from the Opt4Kids and Opt4Mamas studies. BMC Health Serv Res. 2022;22(1):1540. doi:10.1186/s12913-022-08593-z
23. Nasuuna E, Kigozi J, Muwanguzi PA, et al. Challenges faced by caregivers of virally non-suppressed children on the intensive adherence counselling program in Uganda: a qualitative study. BMC Health Serv Res. 2019;19(1):150. doi:10.1186/s12913-019-3963-y
24. Kabami J, Akatukwasa C, Kabageni S, et al. “I desire to have an HIV-free baby”: pregnant and breastfeeding mothers’ perceptions of Viral load testing and suppression in HIV care in southwestern Uganda. Discov Soc Sci Health. 2024;4(1):60. doi:10.1007/s44155-024-00120-1
25. Pita TP, Misra S, Madonsela T, et al. “If your CD4 count lowers, that is when you are similar to a person that is non-existent” A qualitative exploration of perceptions around advanced HIV disease in South Africa. BMC Public Health. 2025;25(1):2325. doi:10.1186/s12889-025-23588-1
26. Reyes-Estrada M, Varas-Díaz N, Parker R, Padilla M, Rodríguez-Madera S. Religion and HIV-related stigma among nurses who work with people living with HIV/AIDS in Puerto Rico. J Int Assoc Providers AIDS Care. 2018;17:2325958218773365. doi:10.1177/2325958218773365
27. Nhassengo P, Cataldo F, Magaço A, et al. Barriers and facilitators to the uptake of test and treat in Mozambique: a qualitative study on patient and provider perceptions. PLoS One. 2018;13(12):e0205919. doi:10.1371/journal.pone.0205919
28. Brown LB, Havlir DV, Ayieko J, et al. High levels of retention in care with streamlined care and universal test and treat in East Africa. AIDS. 2016;30(18):2855–2864. doi:10.1097/QAD.0000000000001250
29. Maeri I, El Ayadi A, Getahun M, et al. “How can I tell?” Consequences of HIV status disclosure among couples in Eastern African communities in the context of an ongoing HIV “test-and-treat” trial. AIDS Care. 2016;28(Suppl 3):59–66. doi:10.1080/09540121.2016.1168917
30. Brown LB, Getahun M, Ayieko J, et al. Factors predictive of successful retention in care among HIV-infected men in a universal test-and-treat setting in Uganda and Kenya: a mixed methods analysis. PLoS One. 2019;14(1):e0210126. doi:10.1371/journal.pone.0210126
31. Johnson-Peretz J, Lebu S, Akatukwasa C, et al. “I was still very young”: agency, stigma and HIV care strategies at school, baseline results of a qualitative study among youth in rural Kenya and Uganda. J Int AIDS Soc. 2022;25(Suppl 1):e25919. doi:10.1002/jia2.25919
32. Dirisu O, Eluwa G, Adams E, Torpey K, Shittu O, Adebajo S. “I think this is the only challenge… the stigma” Stakeholder perceptions about barriers to Antenatal care (ANC) and Prevention of mother-to-child transmission (PMTCT) uptake in Kano state, Nigeria. PLoS One. 2020;15(4):e0232028. doi:10.1371/journal.pone.0232028
33. Rutstein SE, Golin CE, Wheeler SB, et al. On the front line of HIV virological monitoring: barriers and facilitators from a provider perspective in resource-limited settings. AIDS Care. 2016;28(1):1–10. doi:10.1080/09540121.2015.1058896
34. Ehrenkranz P, Grimsrud A, Rabkin M. Differentiated service delivery: navigating the path to scale. Curr Opin HIV AIDS. 2019;14(1):60–65. doi:10.1097/coh.0000000000000509
35. Govindasamy D, Meghij J, Kebede Negussi E, Clare Baggaley R, Ford N, Kranzer K. Interventions to improve or facilitate linkage to or retention in pre-ART (HIV) care and initiation of ART in low- and middle-income settings--a systematic review. J Int AIDS Soc. 2014;17(1):19032. doi:10.7448/ias.17.1.19032
36. Chadrack K, Fanny M, Laetitia N, et al. (PDF) Exploration du soutien psychosocial et économique pour les enfants atteints du VIH/SIDA: perspectives des agents de santé et des agents communautaires dans la zone de santé de Katuba, Lubumbashi. Clinicoecon Outcomes Res. 2025;17:
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.