Back to Journals » Clinical Ophthalmology » Volume 20
Perceived Trust in Artificial Intelligence in Eye Care: Demographic Determinants and Variations in Attitudes Among Ophthalmologists and Residents
Authors Radeva MN ![]() , Hristova EG, Georgiev RT, Boyadzhiev DH, Zlatarova ZI
, Hristova EG, Georgiev RT, Boyadzhiev DH, Zlatarova ZI
Received 6 August 2025
Accepted for publication 7 February 2026
Published 17 February 2026 Volume 2026:20 557302
DOI https://doi.org/10.2147/OPTH.S557302
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Mladena N Radeva,1 Elitsa G Hristova,2 Rosen Tsv Georgiev,1 Dobrin Hr Boyadzhiev,1 Zornitsa I Zlatarova1
1Department of Ophthalmology and Visual Science, Medical University - Varna, Varna, Bulgaria; 2Department of Optometry and Occupational Diseases, Medical University - Varna, Varna, Bulgaria
Correspondence: Mladena N Radeva, Department of Ophthalmology and Visual Science, Medical University – Varna, Marin Drinov Str 55, Varna, 9000, Bulgaria, Email [email protected]
Purpose: To investigate demographic and professional determinants of perceived trust and attitudes toward artificial intelligence (AI) in ophthalmology among ophthalmologists and residents, addressing gaps in understanding factors influencing AI adoption in eye care.
Patients and Methods: This cross-sectional study surveyed 156 participants (73.1% female; median age 35 years) from Bulgaria, including specialists (two-thirds) and residents (one-third). A structured questionnaire assessed awareness, trust in AI for diagnostics and therapeutics, expectations, and concerns. Ethical approval was obtained, and informed consent secured. Data were analyzed using chi-square tests for gender differences, Spearman correlations for age, Kruskal–Wallis tests for experience, and thematic analysis for qualitative responses.
Results: Significant gender differences included higher self-perceived AI knowledge among males (χ2 = 35.2, p < 0.001) but lower diagnostic trust (χ2 = 11.6, p =0.009), with females unanimously rejecting AI as a physician replacement (χ2 = 54.4, p < 0.001). Older participants perceived greater AI utility in glaucoma care (ρ =0.268, p < 0.001) and anticipated delayed integration (ρ =0.163, p =0.042), while younger ones believed in potential replacement (ρ = – 0.217, p =0.007). Less experienced participants (< 5 years) reported higher awareness (χ2 = 17.89, p < 0.001) and faster expected integration (χ2 = 11.29, p =0.010). Residents showed greater awareness and readiness to follow AI recommendations than specialists (p < 0.05). Overall, 64.6% were informed about AI, but trust was low (7.5% for diagnostics); qualitative themes highlighted benefits like diagnostic precision and challenges like regulation gaps.
Conclusion: Demographic and professional factors significantly influence AI attitudes in ophthalmology, with limited trust despite optimism. Targeted education and regulatory frameworks are essential to enhance adoption and address variations.
Keywords: artificial intelligence, ophthalmology, trust, demographics, artificial intelligence adoption, machine learning in medicine
Introduction
Artificial intelligence (AI) is poised to revolutionize ophthalmology by enhancing diagnostic accuracy, optimizing treatment planning, and improving patient outcomes.1 AI is highly applicable in diagnosing eye diseases, thanks to its ability to process vast amounts of high-resolution medical images from devices like retinal fundus cameras, optical coherence tomography (OCT) scanners, and perimetry tools. It can identify subtle patterns and anomalies with speed and accuracy that often surpass human capabilities in tasks such as detecting diabetic retinopathy or glaucoma.2
As of 2025, AI is extensively applied in ophthalmology for diagnostic screening, disease monitoring, surgical assistance, and public health initiatives, leveraging deep learning and machine learning on imaging data to address conditions like diabetic retinopathy (DR), glaucoma, age-related macular degeneration (AMD), and cataracts. In public health, AI enhances ophthalmic data management through computer vision for image enhancement, segmentation, and registration, while natural language processing analyzes electronic medical records to enable efficient disease screening via convolutional neural networks on fundus photos and OCT scans, as exemplified by Google’s DeepMind system achieving high accuracy for multiple eye diseases. For specific subspecialties, AI automates DR screening with sensitivities up to 97.5% using retinal fundus photographs, predicts glaucoma progression with Area Under the Curve (AUCs) of 0.98 on OCT, detects AMD with AUC 0.93, aids in uveitis quantification, supports ocular oncology differentiation with AUC 0.88 for choroidal lesions, enables keratoconus detection with 96–99% accuracy, and facilitates retinopathy of prematurity staging. Additionally, AI supports telemedicine and resource allocation with robot-assisted surgeries, provides personalized patient education via apps, and addresses ethical considerations like privacy and bias mitigation in diagnostic algorithms to ensure fairness and build long-term trust.3–5
There are significant challenges to the large-scale clinical adoption of AI in ophthalmology, including the availability of validated AI solutions, heterogeneous patient populations, varying acquisition standards and image quality, discrepancies in threshold levels and values for intervention, and the need to establish trust in AI systems for critical decision-making.6,7 Another key challenge is building trust and acceptance among healthcare professionals, which can be influenced by demographic and professional factors. Understanding these influences is essential for developing strategies to facilitate AI adoption in eye care. While previous multinational and regional surveys have assessed general attitudes toward AI among ophthalmologists (eg, younger clinicians tend to be more receptive, particularly those with greater digital interest and experience), few studies have systematically examined the differential impacts of demographic and professional variables—such as gender, age, experience, and training status—on nuanced aspects like trust, awareness, and expectations. This is especially true when distinguishing residents from established practitioners. This study aims to address this gap by investigating how these factors shape ophthalmologists’ and residents’ attitudes toward AI in ophthalmic practice, providing novel insights to inform tailored educational and implementation frameworks for enhanced adoption.8,9
Patients and Methods
Study Design and Participants
This cross-sectional study involved 156 participants (ophthalmologists and residents). The cohort and sample size were determined by the number of participants who completed the survey, as the study relied on voluntary participation in an online or distributed questionnaire among ophthalmologists and residents.
Ethical approval was obtained from the Committee of Medical University of Varna, with number 81/28.02.2020. Informed consent was secured from all participants, in compliance with the Declaration of Helsinki. The majority were female (73.1%), with a median age of 35 years. Approximately one-third had less than 5 years of experience. Specialists comprised nearly two-thirds, residents the remaining third.
Data Collection
Data were collected using a structured questionnaire (Supplementary Material 1), comprising both closed-ended (Q8, Q12–Q18) and open-ended questions (Q23–Q25). Data were collected using a structured questionnaire with closed-ended (Q8, Q12–Q18) and open-ended questions (Q23–Q25). Closed-ended questions assessed awareness (Q12), trust in AI’s diagnostic (Q13) and therapeutic capabilities (Q15, Q16), expectations for AI’s impact (Q17), and concerns about professional replacement (Q18). Open-ended questions explored perceived benefits, challenges, and integration requirements.
It is important to note that the questionnaire did not include specific questions regarding respondents’ personal or institutional use of AI technologies in eye care. The primary aim was to assess general attitudes, expectations, and perceived barriers, irrespective of direct user experience.
Statistical Analysis
Normality tests (Shapiro–Wilk) indicated non-normal distribution for all key variables (p <0.001), necessitating non-parametric tests. Chi-square tests evaluated associations between gender and AI-related attitudes. Spearman correlation analysis assessed relationships between age and scaled responses. The Kruskal–Wallis test examined the influence of professional experience. Qualitative responses were analyzed using thematic content analysis.
Results
Demographic and Professional Influences
Differences by Gender
Chi-square tests revealed significant gender-based differences in attitudes toward artificial intelligence in ophthalmology. Males reported higher self-perceived knowledge of AI compared to females (Q12; χ2 = 35.2, df = 4, p <0.001). Gender was also found to significantly influence respondents’ trust in AI’s diagnostic role (Q13; χ2 = 11.6, df = 3, p =0.009). As illustrated in Figure 1, male respondents more frequently reported moderate or complete distrust toward AI, while female respondents tended to express greater openness to AI-generated diagnostic suggestions. Additionally, a larger proportion of female participants indicated uncertainty regarding AI’s reliability due to insufficient personal experience with such systems.
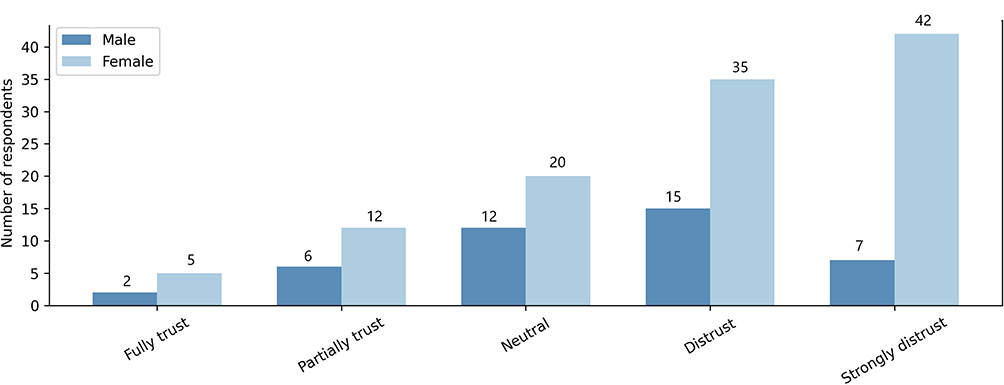 |
Figure 1 Awareness of AI in ophthalmic diagnostics, by gender. Proportion of respondents who reported being “informed” or “partially informed” about the role of AI in ophthalmology, stratified by gender. Females reported significantly higher awareness than males (χ2 = 6.21, p = 0.013). Counts (n) and percentages are shown within the bars. |
Gender-based divergence was likewise observed regarding the expected timeframe for AI implementation in clinical practice (Q17; χ2 = 24.1, df = 5, p <0.001). As shown in Figure 2, female participants most frequently selected a 1–5 year integration horizon, whereas male responses were more varied and included both shorter and longer timelines.
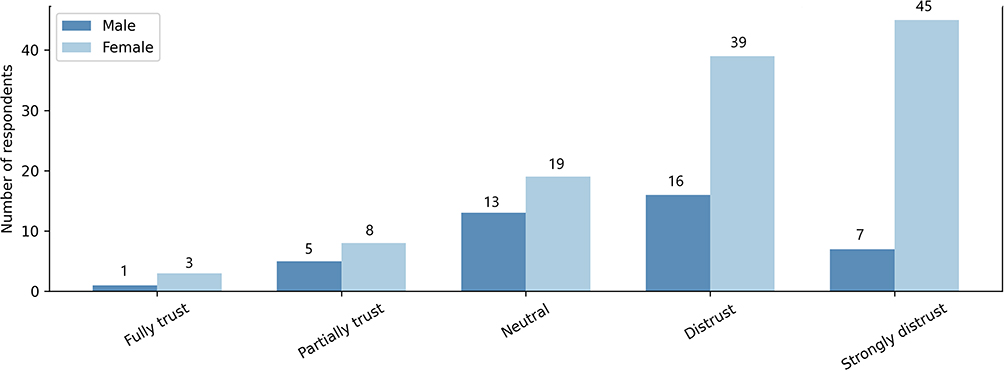 |
Figure 2 Trust in AI-supported diagnostics, by practice setting. Levels of trust in AI-generated diagnostic suggestions across different clinical settings (public, private, or both). Bars represent absolute counts and corresponding proportions. |
A particularly pronounced gender-based contrast emerged in relation to the perception of AI as a threat to the medical profession. Female respondents unanimously disagreed that AI could replace physicians (Q18; χ2 = 54.4, df = 3, p <0.001), highlighting a more firmly grounded stance on the irreplaceability of the clinician’s role. Demographic and professional characteristics of the study participants (Table 1).
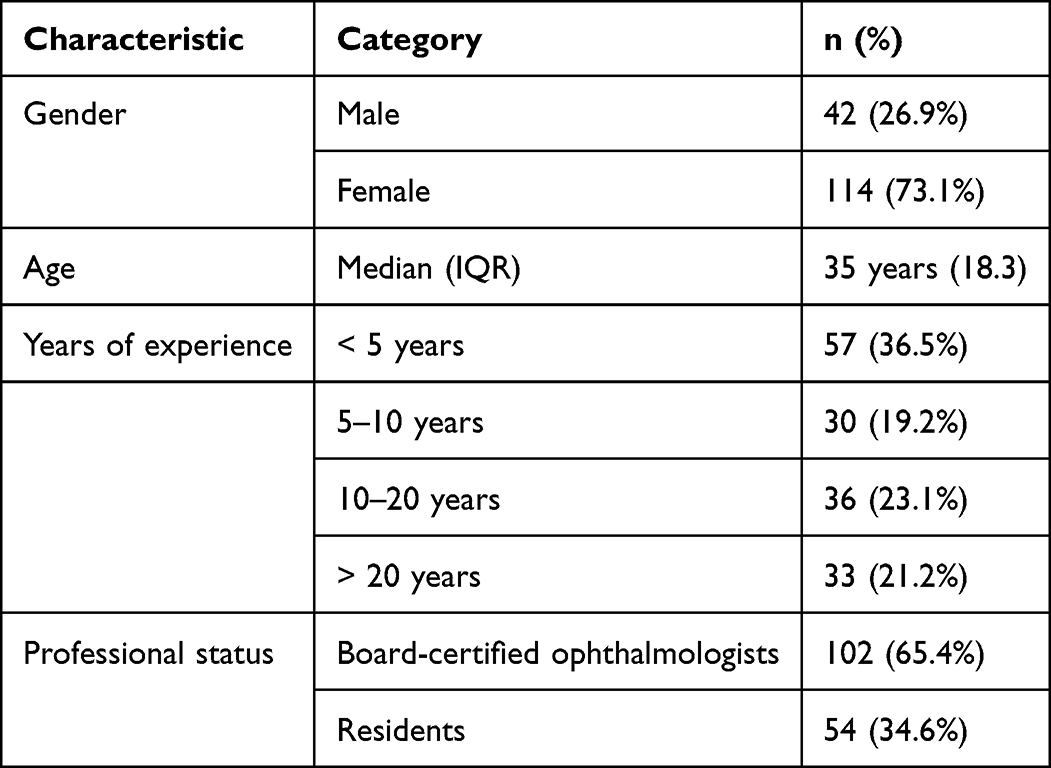 |
Table 1 Demographic and Professional Characteristics of the Study Participants |
Age
To explore the relationships between age and participants’ attitudes toward AI, a series of Spearman correlation analyses was performed and visualized in Figure 3a–c. Older participants were more likely to perceive AI as beneficial in the context of glaucoma care (Figure 3a; ρ =0.268, p <0.001) and anticipated a longer timeframe for its clinical integration (Figure 3b; ρ =0.163, p =0.042). Conversely, younger participants more frequently believed that AI could eventually replace physicians (Figure 3c; ρ = –0.217, p =0.007).
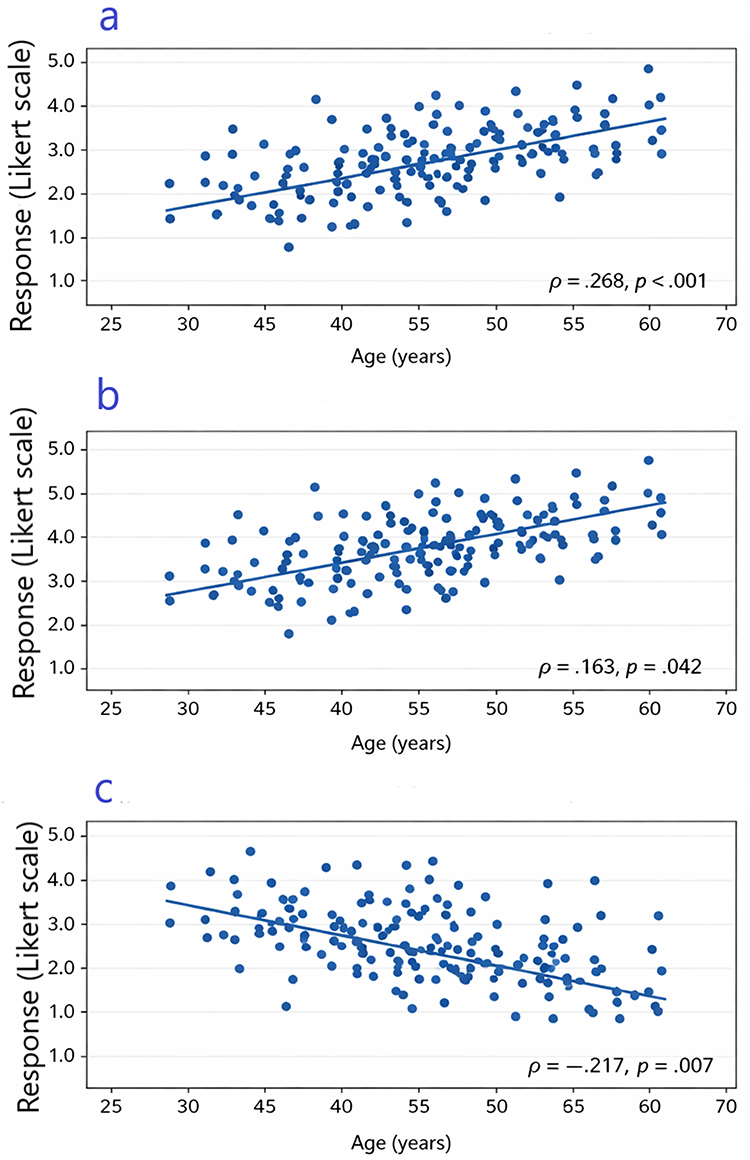 |
Figure 3 Age-related variations in attitudes toward AI in ophthalmology. Associations between age and three key attitude variables are shown: (a) Trust in AI for glaucoma treatment (ρ =0.268, p <0.001); (b) Expected timeframe for AI integration into clinical care (ρ =0.163, p =0.042); (c) Belief that AI may eventually replace physicians (ρ = –0.217, p =0.007). Spearman correlation coefficients (ρ) and exact p-values are displayed within each panel. |
These associations are depicted in the individual scatter plots, where linear regression lines illustrate the direction of correlation, and asterisks indicate statistical significance (p <0.05*<0.01**<0.001***). The questions assessed perceived utility of AI for glaucoma care, expectations for implementation timelines, and beliefs regarding potential replacement of physicians (Table 1).
Professional Experience
The Kruskal–Wallis test identified significant associations between experience and AI attitudes. Less experienced participants (<5 years) reported higher awareness of AI applications (Q14; χ2 = 17.89, p <0.001) and anticipated faster AI integration (Q17; χ2 = 11.29, p =0.010). Participants with 5–20 years of experience showed greater belief in AI’s potential (Q15; χ2 = 12.54, p =0.006). A marginally significant association suggested that less experienced clinicians perceived AI as a potential threat (Q18; χ2 = 7.95, p =0.047) (Table 1).
Specialists vs Residents
Residents demonstrated higher awareness (Q12) and readiness to follow AI recommendations (Q16) compared to specialists (p <0.05), indicating generational differences.
Quantitative and Qualitative Findings
Of the respondents, 64.6% reported being “informed” or “partially informed” about AI (Q12), but only 7.5% fully trusted AI for diagnostics (Q13) and 5.7% for therapeutic recommendations (Q15). Despite this, 58% expected AI to positively impact ophthalmology (Q17). Thematic analysis identified key benefits, including processing speed, objectivity, mass screening potential, and diagnostic precision. Challenges included lack of regulation, insufficient training, interpretive difficulties, and ethical concerns. Respondents emphasized the need for protocols, specialized training, and clear regulatory frameworks.
Discussion
This study provides valuable insights into how demographic and professional factors influence attitudes toward artificial intelligence (AI) in ophthalmology. By examining the relationships between gender, age, professional experience, and training status with trust, awareness, and expectations regarding AI, we contribute to the growing body of research on technology adoption in healthcare. The findings reveal complex patterns of perception that both align with and extend existing literature, while also highlighting areas for further investigation.
Gender Differences in AI Perceptions
Significant gender-based differences emerged in this study, offering a nuanced view of AI acceptance. Males reported higher self-perceived knowledge of AI (Q12; χ2 = 35.2, df = 4, p <0.001) but lower trust in its diagnostic accuracy (Q13; χ2 = 11.6, df = 3, p =0.009), despite greater trust in its therapeutic recommendations (Q16; χ2 = 9.07, df = 2, p =0.011). This paradox suggests that knowledge does not inherently foster trust, resonating with the Technology Acceptance Model (TAM), which emphasizes perceived usefulness and ease of use as key drivers of adoption.10 Males’ skepticism toward diagnostic accuracy might reflect a critical awareness of AI’s current limitations, possibly informed by their higher knowledge or concerns about professional autonomy. Blease et al (2020) similarly found that male clinicians exhibit greater technological confidence but remain wary of AI reliability in clinical settings.11
In contrast, females unanimously disagreed that AI could replace physicians (Q18; χ2 = 54.4, df = 3, p <0.001), potentially reflecting a stronger valuation of human judgment, empathy, and patient interaction in medical practice. This aligns with Fan et al (2021), who noted that women in healthcare often prioritize relational aspects, viewing AI as a supportive rather than substitutive tool.12 Gender roles and societal norms may further shape these perceptions, as women, historically underrepresented in technology fields, might approach AI with caution.13 These findings suggest that gender-specific educational strategies—enhancing knowledge for females and addressing trust barriers for males—could optimize AI integration in ophthalmology.
Age-Related Variations in AI Attitudes
Age significantly influenced perceptions of AI’s utility and potential impact. Older participants viewed AI as more useful for glaucoma care (Q15; ρ =0.268, p <0.001) but anticipated a delayed clinical impact (Q17; ρ =0.163, p =0.042), while younger participants were more likely to believe AI could replace physicians (Q18; ρ = –0.217, p =0.007). These trends corroborate Oh et al (2019), who found younger clinicians more optimistic about AI due to greater familiarity with technology.14 Liu et al (2022) also noted that younger ophthalmologists adopt AI-driven tools more readily, likely due to exposure in modern training.14 Conversely, older clinicians’ tempered expectations may stem from practical experience with the slow pace of healthcare innovation, including validation and regulatory hurdles.
The optimism among younger participants raises concerns about overreliance on AI, potentially at the expense of clinical judgment development. Topol (2019) warns of this risk, advocating for a balanced approach to technology adoption among early-career professionals.15 Bridging this generational gap through mentorship—pairing younger enthusiasm with older caution—could foster a more measured integration of AI into ophthalmic practice.
Influence of Professional Experience
Professional experience shaped distinct attitudes toward AI. Participants with less than 5 years of experience reported higher awareness of AI applications (Q14; χ2 = 17.89, p <0.001) and anticipated faster integration (Q17; χ2 = 11.29, p =0.010), likely due to recent education incorporating AI concepts.10 Mid-career clinicians (5–20 years) showed greater belief in AI’s diagnostic and therapeutic potential (Q15; χ2 = 12.54, p =0.006), reflecting a balanced perspective honed by practice. Abdullahi et al (2023) observed similar openness among mid-career clinicians, attributing it to experience with both traditional limitations and technological promise.16
Less experienced clinicians’ marginal concern about AI replacing physicians (Q18; χ2 = 7.95, p =0.047) echoes Davenport and Kalakota (2019), who suggest early-career professionals may perceive AI as a job security threat.17 Targeted training emphasizing AI’s collaborative role could alleviate such fears, enhancing readiness across experience levels.
Specialists vs Residents: Training and Exposure
Residents exhibited higher awareness (Q12) and readiness to follow AI recommendations (Q16) compared to specialists (p <0.05), highlighting a training-related divide. This aligns with Oh et al (2019), who noted residents’ early adoption due to contemporary curricula.5 Specialists’ more reserved stance may reflect practical concerns—cost, compatibility, or safety—tempered by years of practice. Residency programs thus offer a critical opportunity to build AI literacy, provided they balance enthusiasm with critical evaluation.
Qualitative Insights: Opportunities and Barriers
Qualitative findings underscored AI’s perceived benefits—diagnostic precision, mass screening, and workload reduction—consistent with Campbell et al (2022), who highlighted AI’s efficacy in resource-limited settings.18 However, challenges such as lack of regulation, inadequate training, and ethical concerns mirror broader literature. He et al (2021) stress the need for protocols to address bias and consent,19 while Reddy et al (2020) identify privacy and clinician resistance as persistent barriers.20 The consensus on AI’s supportive role aligns with the “augmented intelligence” paradigm, emphasizing enhancement over replacement.21 Overcoming these hurdles requires comprehensive training, transparent AI development, and regulatory collaboration.
Limitations of the Study
This study has several notable limitations. The reliance on self-reported data may introduce bias, as participants’ perceptions might not accurately reflect their actual knowledge or behavior. The variables’ non-normal distribution also limited statistical power, and while the sample size of 156 is sufficient, it may not fully represent diverse ophthalmic contexts or regions, thereby reducing generalizability. Furthermore, the cross-sectional, single-center design (based at the Medical University of Varna) precludes tracking attitudinal changes over time as AI evolves, and the cultural context may influence AI attitudes, limiting external validity—even though the online survey targeted all ophthalmologists in Bulgaria.
Another limitation involves the response options for trust-related questions, which range from “I don’t trust it at all” to “I cannot estimate” without including positive choices (eg, “I somewhat trust it” or “I fully trust it”), potentially biasing responses toward negativity. The questionnaire also omitted an item assessing whether participants currently use AI technologies in clinical practice, hindering the ability to contextualize attitudes based on actual experience. Future research should explicitly distinguish between AI users and non-users in ophthalmology to capture a more nuanced understanding of perceptions and acceptance.
Theoretical Frameworks
In our study, demographic differences in AI acceptance align partially with the APPRAISE study, where older age (OR 1.03) and male gender (OR 1.40) correlated with higher diagnostic tool acceptance, and ≥20 years of experience boosted assistive tool acceptance (OR 3.70), suggesting our variations may reflect similar age and tenure influences. The APPRAISE study also highlighted regional effects, like elevated organizational willingness in North America (OR 8.54) and reduced in resource-abundant areas (OR 0.39), which could benchmark our findings against geographic or resource-based demographics. Comparatively, the 2025 global survey by Ferro Desideri et al demonstrates these patterns, underlying that ophthalmologists with >20 years of experience were more supportive of AI adoption (OR 1.5), while academic clinicians showed higher familiarity (p=0.0011), potentially explaining our demographic variations through professional setting and seniority. However, Ferro Desideri et al reported lower overall regular AI use (7.2%) despite recognized potential (69.5%), emphasizing barriers like training gaps and ethics that APPRAISE also identified, offering a broader framework via the Technology Acceptance Model to interpret our results without deep theoretical engagement.8,22
Future Research Directions
Future studies could address these gaps through longitudinal designs to monitor evolving perceptions, objective measures (eg, AI competency assessments), and broader, more diverse samples. Investigating specific barriers—cost, infrastructure, regulation—and comparing ophthalmology with other specialties could refine implementation strategies. Including patient perspectives would further enrich understanding of AI’s holistic impact in eye care.
Conclusion
Demographic and professional factors significantly shape attitudes toward AI in ophthalmology. While awareness and optimism are prevalent, trust remains limited, particularly among males and experienced clinicians. Addressing these variations through targeted training, clear protocols, and regulatory frameworks is essential for successful AI integration. Future research should explore longitudinal changes in perceptions as AI technologies evolve.
Funding
This study was funded by Medical University of Varna, Varna, Bulgaria.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhang H, Li Z, Chan HC, Song X, Zhou H, Fan X. Artificial intelligence in thyroid eye disease imaging: a systematic review. Surv Ophthalmol. 2026;71(1):142–9. doi:10.1016/j.survophthal.2025.07.008
2. Rahat Qureshi A, Micieli JA, Wong JCY. Generative artificial intelligence in ophthalmology: a scoping review of current applications, opportunities, and challenges. Eye. 2025;39(16):2860–2871. doi:10.1038/s41433-025-04006-7
3. Chen X, Yang Y, Yun D, et al. Current status and solutions for AI ethics in ophthalmology: a bibliometric analysis. Npj Digit Med. 2025;8(1):594. doi:10.1038/s41746-025-01976-6
4. Khan AYR, Malik MB, Khan AYR, Malik MB. Artificial intelligence in ophthalmology: practical applications, subspecialty evidence and real-world deployment. Cureus. 2025;17(11):e96121. doi:10.7759/cureus.96121
5. Chen S, Bai W. Artificial intelligence technology in ophthalmology public health: current applications and future directions. Front Cell Dev Biol. 2025;13:1576465. doi:10.3389/fcell.2025.1576465
6. Oshika T. Artificial intelligence applications in ophthalmology. JMA J. 2025;8(1):66–75. doi:10.31662/jmaj.2024-0139
7. Suganya Devi K, Vasireddi HK, Reddy GR, Satti SK. Unfolding the diagnostic pipeline of diabetic retinopathy with artificial intelligence: a systematic review. Surv Ophthalmol. 2025;
8. Tappeiner C. Artificial intelligence in ophthalmology: acceptance, clinical integration, and educational needs in Switzerland. J Clin Med. 2025;14(17):6307. doi:10.3390/jcm14176307
9. Gunasekeran DV, Zheng F, Lim GYS, et al. Acceptance and Perception of Artificial Intelligence Usability in Eye Care (APPRAISE) for ophthalmologists: a multinational perspective. Front Med. 2022;9:875242. doi:10.3389/fmed.2022.875242
10. Kazemzadeh K. Artificial intelligence in ophthalmology: opportunities, challenges, and ethical considerations. Med Hypothesis Discov Innov Ophthalmol. 2025;14(1):255–272. doi:10.51329/mehdiophthal1517
11. Cosgriff CV, Stone DJ, Weissman G, Pirracchio R, Celi LA. The clinical artificial intelligence department: a prerequisite for success. BMJ Health Care Inform. 2020;27(1):e100183. doi:10.1136/bmjhci-2020-100183
12. Møgelvang A, Bjelland C, Grassini S, et al. Gender differences in the use of generative artificial intelligence Chatbots in higher education: characteristics and consequences. Educ Sci. 2024;14(12):1363. doi:10.3390/educsci14121363
13. Juravle G, Boudouraki A, Terziyska M, Rezlescu C. Trust in artificial intelligence for medical diagnoses. Prog Brain Res. 2020;253:263–282. doi:10.1016/bs.pbr.2020.06.006
14. Heinrichs H, Kies A, Nagel SK, Kiessling F. Physicians’ attitudes toward artificial intelligence in medicine: mixed methods survey and interview study. J Med Internet Res. 2025;27(1):e74187. doi:10.2196/74187
15. Zhang J, Fenton SH. Preparing healthcare education for an AI-augmented future. Npj Health Syst. 2024;1(1):4. doi:10.1038/s44401-024-00006-z
16. Ayorinde A, Mensah DO, Walsh J, et al. Health Care Professionals’ experience of using AI: systematic review with narrative synthesis. J Med Internet Res. 2024;26:e55766. doi:10.2196/55766
17. Davenport T, Kalakota R. The potential for artificial intelligence in healthcare. Future Healthc J. 2019;6(2):94–98. doi:10.7861/futurehosp.6-2-94
18. Campbell CG, Ting DSW, Keane PA, Foster PJ. The potential application of artificial intelligence for diagnosis and management of glaucoma in adults. Br Med Bull. 2020;134(1):21–33. doi:10.1093/bmb/ldaa012
19. Gerke S, Minssen T, Cohen G. Ethical and legal challenges of artificial intelligence-driven healthcare. Artif Intell Healthc. 2020;295–336. doi:10.1016/B978-0-12-818438-7.00012-5
20. Assadullah MM. Barriers to artificial intelligence adoption in healthcare management: a systematic review. Soc Sci Res Netw. 2019. doi:10.2139/ssrn.3530598
21. Moodley K. Artificial intelligence (AI) or augmented intelligence? How big data and AI are transforming healthcare: challenges and opportunities. S Afr Gen Pract. 2024;5(4):170–175. doi:10.7196/SAMJ.2024.v114i2.1631
22. Ferro Desideri L, Subhi Y, Roth J, et al. Global perspectives of ophthalmologists on artificial intelligence adoption in clinical practice. Int J Retina Vitreous. 2025. doi:10.1186/s40942-025-00764-4
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparing Ophthalmologist and Artificial Intelligence Chatbot Responses to Patient Questions
Bondok M, Selvakumar R, Law C, Ing EB, Bakshi NK, Felfeli T
Clinical Ophthalmology 2025, 19:4293-4300
Published Date: 25 November 2025