Back to Journals » Research and Reports in Urology » Volume 14
Penile Vibratory Stimulation for Semen Retrieval in Men with Spinal Cord Injury: Patient Perspectives
Authors Ibrahim E ![]() , Brackett NL, Lynne CM
, Brackett NL, Lynne CM
Received 9 March 2022
Accepted for publication 12 April 2022
Published 21 April 2022 Volume 2022:14 Pages 149—157
DOI https://doi.org/10.2147/RRU.S278797
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Panagiotis J Vlachostergios
Emad Ibrahim,1,2 Nancy L Brackett,1,2 Charles M Lynne1,2
1The Desai Sethi Urology Institute, University of Miami Miller School of Medicine, Miami, FL, USA; 2The Miami Project to Cure Paralysis, University of Miami Miller School of Medicine, Miami, FL, USA
Correspondence: Emad Ibrahim, The Desai Sethi Urology Institute/The Miami Project to Cure Paralysis, University of Miami Miller School of Medicine, 1611 NW 12th Ave, 2nd floor, Rm 2.147, Miami, FL 33136, USA, Tel +1 305 243 9083, Fax +1 305 243 3913, Email [email protected]
Abstract: Spinal cord injury (SCI) is a catastrophic event with sequelae that are not often apparent. For the spinal cord injured man, the inability to become a biologic father because of reproductive dysfunction becomes a major negative factor in his self-esteem and a hindrance to his social rehabilitation. Approximately, 90% of men with SCI develop ejaculatory dysfunction and only 10% can ejaculate by masturbation or during sexual activity. It is only over the last 40 years that it has been possible to properly study and understand the various factors contributing to the problem. Advances have been made in governmental and societal attitudes that have led to improvements in the treatment and rehabilitation of persons with SCI and other disabilities. It is now possible to retrieve sperm reliably and safely from men with SCI. Although their semen quality is often impaired, there is a very reasonable chance for achieving biologic fatherhood using assisted reproductive techniques. Penile vibratory stimulation (PVS) is a safe, reliable, efficient, and cost-effective, method of sperm retrieval that will produce an ejaculate in up to 86% of the patients with a level of injury T10 or rostral, which accounts for approximately 80% of the SCI population. Some motile sperm will be present in 90% of these ejaculates. In approximately 75% of the ejaculates, there will be greater than 5 million motile sperm, allowing a couple to explore all the options available to a couple seeking help in conceiving a child. The Male Fertility Program of the Miami Project to Cure Paralysis is at the leading edge of basic and clinical research contributing to the management of infertility in men with SCI. This review will outline “how we got there” enabling us to recommend PVS as the first choice in assisting men with SCI to become biologic parents.
Keywords: anejaculation, fertility, sperm, conception, reproduction, child
Introduction
Much of the research presented in this review was possible because of the commitment of the Miami Project to Cure Paralysis (Miami Project), an organization dedicated to improving the quality of life and, ultimately, finding a cure for paralysis. The organization rapidly evolved into an internationally recognized center for basic, clinical, and translational research and education in the field of spinal cord injury (SCI). In 1991, the Male Fertility Program of the Miami Project was established. This paper is primarily based on the experience of this program over 30 years of research in the management of infertility in men with SCI. In addition, this review describes how concomitant advances two fields – assisted reproductive technology, and infertility in men with SCI – led, synergistically, to optimal outcomes for men with SCI who desire biologic fatherhood.
The majority of men with an SCI are in an age group in which achieving biologic fatherhood and establishing a family are of great importance. Greater than 90% of these men are anejaculatory (unable to ejaculate via sexual activity) and will need some type of assisted reproduction to achieve biologic fatherhood. In its simplest form, assisted reproduction is a means of getting sperm in contact with the female reproductive tract so that fertilization of an egg can occur when this cannot be accomplished through sexual intercourse. John Hunter in London is credited with first description of human intravaginal placement of sperm.1 In 1784, artificial insemination of a dog was reported by an Italian scientist. The late 1800s into the first half of the 20th century saw much activity in the field of animal intravaginal insemination.2
In more modern times, prior to the 1980s, little organized research had been published about fertility in men with SCI even though as early as 1948 Horne published a brief paper in which he described a crude transrectal electrostimulation technique followed by massage of the prostate and seminal vesicles which was very successful in obtaining sperm from a small group of SCI patients at a VA hospital.3 The reasons for this apparent lack of interest were numerous and varied. Vibrators had a low success rate, and surgical methods of sperm retrieval, although known, were not widely used because organized medicine had seen very little success with assisted reproduction using the low numbers of sperm typically obtained by surgical methods. The use of intracytoplasmic sperm injection (ICSI) to address this problem, was still experimental.
In the societal/governmental milieu, there had been only slow movement toward integration of persons with SCI, despite passage of The Rehabilitation Act of 1973 (and its amendments) which stated that
no otherwise qualified individual with a disability in the United States shall solely by reason of her or his disability be excluded from participation in, be denied benefits of, or be subjected to discrimination under any program or activity receiving financial assistance.
Patients were often told that they would never walk again. Male patients were told that they would never father children.
Events in both medicine and society helped to change this bleak outlook. (1) The birth of Louise Brown on July 25,1978 in a hospital just outside of Manchester, England, let the world know that biologic parenting could be a reality for those couples who had only a small number of their sperm available. (2) In the mid-1980s Stephen Seager, DVM, developed a device for semen retrieval in men who were anejaculatory. This device, adapted from veterinary medicine, delivered electrical stimulation via a rectal probe to obtain semen for animal breeding. This method, called electroejaculation (EEJ), became a safe, reliable and reproducible tool for obtaining sperm from men with SCI, most of whom are anejaculatory.4 (3) In 1994, Jens Sonksen, MD, PhD, showed that a device vibrating at 2.5 mm amplitude when placed on the glans penis, was optimal in obtaining an ejaculatory response in men with SCI.5 He then developed the Ferticare vibrator, based on that principle. The method, called penile vibratory stimulation (PVS) was safe and reliable for obtaining an ejaculate from men with SCI. Compared to EEJ, PVS was preferred more by patients because it was less invasive and easier to administer. (4) The Americans with Disabilities Act was passed in 1990. Title 1 prohibited discrimination in employment specifically addressing the inaccessibility of systems or services required to obtain and maintain employment. Title 2 addressed communications with persons with disabilities saying they must be as effective as communications with others in public entities. Title 3 dealt with nondiscrimination toward people with disabilities in places of public accommodation.
The majority of men who sustain a SCI, with resultant paraplegia or tetraplegia, are of an age at which developing and raising a family is of great importance, whether or not they have a female partner at the time of the injury. Ninety percent of these men will be unable to father children without medical assistance because they are anejaculatory. Even though normal numbers of sperm can be obtained by PVS or EEJ, the percentage of motile sperm is well below normal.
The most common assisted reproductive technologies in use today are intrauterine insemination (IUI); and the two in vitro techniques, “classical” in vitro insemination (IVF), and intracytoplasmic sperm injection (ICSI). If there are no female factors, the choice of IUI versus IVF/ICSI in any given cycle is, for the most part, determined by the available number of motile sperm. For a reasonable chance of success with IUI, 5 million total motile sperm (TMS) are recommended. For IVF, a few hundred thousand TMS are necessary, and for ICSI, theoretically, only a single motile sperm is necessary.
Mention should be made of the method of intravaginal insemination of unprocessed semen. This method can be done anytime an antegrade ejaculate is obtained and found to have a reasonable number of TMS and timed to the partner’s ovulatory cycle. It can be performed as an office procedure and can also be performed by a couple at home. It is recommended that the couple first be instructed on the safe administration of PVS, which includes management of autonomic dysreflexia, an uninhibited sympathetic discharge triggered by the noxious stimulus below the level of injury. Pregnancy rates using at home intravaginal insemination range from 25% to 70% per couple.6 Sperm retrieval methods that have the potential for yielding the largest number of TMS give the couple the most options and choices for achieving pregnancy. When used in IUI or IVF/ICSI, ejaculated sperm from men with SCI result in similar pregnancy rates as sperm from other etiologies of male factor infertility.7
Materials and Methods
Methods of Sperm Retrieval for Men with SCI
There are basically four methods available for sperm retrieval for men with SCI. Penile vibratory stimulation (PVS) is performed by placing a vibrating device against the glans penis and delivering mechanical stimulation to induce ejaculation. PVS is safe, efficient, easy to learn, and requires a relatively low investment of time and money. The success rate is highest in patients with a level of injury T10 or rostral (86%) versus a 17% success rate in patients with a level of injury below T10. Compared to other methods of sperm retrieval in men with SCI, PVS results in the highest yield of TMS, most of which is antegrade versus retrograde. PVS can be performed at home for intravaginal insemination. As with other methods of semen retrieval, PVS can elicit autonomic dysreflexia.
Electroejaculation (EEJ) is performed by placing a probe into the rectum and delivering electric current to induce ejaculation. EEJ is safe, and nearly 100% successful at all levels of injury. There are several drawbacks to this method. For example, the start-up equipment cost is relatively high, and the method must be administered by a specially trained physician. In addition, retrograde ejaculation is typical, requiring bladder preparation prior to EEJ, and retrieval of sperm from the bladder following EEJ. Compared to PVS, EEJ results in a lower percent of motile sperm in the antegrade fraction.8,9 As with other methods, EEJ can stimulate autonomic dysreflexia.
Prostatic massage is performed by a physician inserting a finger into the patient’s rectum and pressing on the prostate and seminal vesicles to push out semen through the urethra. This method is fast, easy, inexpensive, and requires no specialized equipment. The downside to prostatic massage is that the results are inconsistent, and the yield of sperm is typically low. Autonomic dysreflexia is also possible.
Surgical sperm retrieval (SSR) is performed by surgically removing sperm from reproductive tissues such as the testicle or epididymis. SSR may lessen the risk of autonomic dysreflexia in some instances. There is a high chance of obtaining some healthy sperm in patients with little or no sperm in their ejaculates. The downside to SSR is that the method is invasive and expensive. The yield of motile sperm is very low which limits options for the couple. For these reasons, SSR should be the choice of last resort.
Neurologic Considerations
The neurologic control of ejaculation, as in most other systems or end organs, depends upon intact spinal cord reflexes which, in a non-SCI situation, receive positive and/or negative inputs from the supra-spinal portions of the nervous system, ie, the brain. For normal ejaculation, spinal cord segments T10 to L2 must be intact for emission of semen to occur, and spinal cord segments S2 to S4 must be intact for expulsion of semen to occur. According to data from the annual report of the National Spinal Cord Injury Center, approximately 80% of spinal cord injuries occur at the level of T10 or rostral,10 suggesting that the majority of men seeking assistance for sperm retrieval will be candidates for a technique that utilizes an intact ejaculatory reflex.
It is important to note that level of injury is generally assigned by sensory testing which starts at the head and neck and continues down the body. The point at which normal sensation ends becomes the assigned level of injury. This testing method is useful in most cases but does not provide information regarding a secondary area of damage below that level. The ability to elicit a bulbocavernosus reflex (BCR) and hip flexor reflex (HFR) can help confirm the integrity of the spinal cord segments required for ejaculation.11 PVS depends upon the recruitment of an intact ejaculatory reflex arc by providing a high level of input via the dorsal nerve of the penis, which innervates of the glans.12
In 2001, the Male Fertility Program research team published their observations in all SCI patients undergoing PVS trials between 1995 and 1998. Only patients who suffered traumatic spinal cord injury at least 2 years prior were included (n = 123). Patients were stratified into three groups by level of injury: cervical, T1-T6, and T7-T12. All patients were examined for the presence or absence of the BCR and HFR reflexes to determine if these reflexes could be indicators of an ejaculatory response to PVS. The results of the study showed the following. (1) For patients with a level of injury in the cervical segments, the presence or absence of the BCR and/or HFR were no more predictive of an ejaculatory response than level of injury alone. (2) For patients with a level of injury between T1 and T6, the presence of at least one of the reflexes was a good predictor of ejaculation, whereas absence of both reflexes predicted no response. (3) For patients with a level of injury between T7 and T12, the absence of the BCR reflex indicated no response.11 In addition to the BCR and HFR, specific somatic reflexes occurred more often in PVS trials in which ejaculation occurred (ejaculation (+) trials) versus PVS trials in which ejaculation did not occur (ejaculation(–) trials, see Table 1).
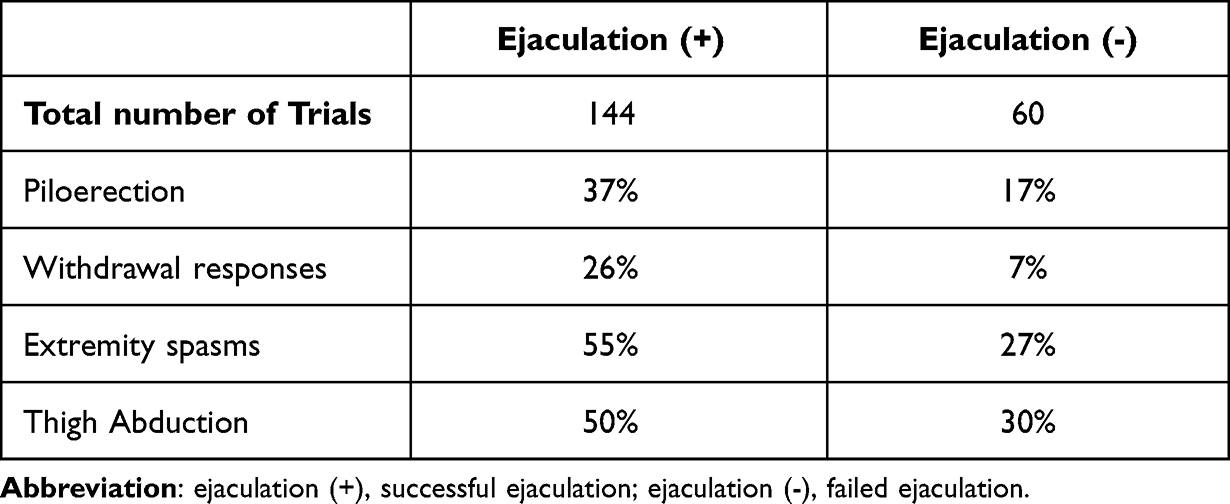 |
Table 1 Occurrence of Somatic Responses in Ejaculation (+) vs Ejaculation (-) Trials |
These findings have been shown to be useful tools in patient selection for PVS, particularly in cases in which the first attempt fails. Presence of one or more predictors may help inform the decision to perform a second trial of PVS or go on to a more aggressive method of sperm retrieval, such as EEJ.
Autonomic Dysreflexia
When there is no peripheral nerve damage to the patient with SCI, input from the periphery can and will continue, and may result in untoward or dangerous reflex activity in the segments below the level of injury which cannot receive mitigating or controlling activity from supra-spinal centers. In patients who have spinal cord lesions at or rostral to T6, autonomic dysreflexia may occur. Autonomic dysreflexia is an uninhibited sympathetic discharge triggered by the noxious stimulus below the level of injury. The symptoms include elevated blood pressure (sometimes to dangerous levels), headache, sweating, nasal congestion, flushing, and in classic cases, bradycardia, although sometimes tachycardia is seen. Our recommendation has been to pretreat, with an appropriate blood pressure medication, all patients at risk for autonomic dysreflexia, regardless of previous history of autonomic dysreflexia. Our preferred pre-treatment regimen is 20 mg of nifedipine, sublingually, 15 minutes prior to stimulation onset. Other medications are also effective for this purpose.13–17
Why PVS?
Early investigations of the male fertility program established that the percent of motile sperm, and the percent of sperm with rapid linear motility, was higher in ejaculates obtained by PVS versus EEJ, even within a group of the same subjects.8 A PVS trial has remained the first procedure performed on every new patient seen in the program, keeping our data collection method consistent even to this date. In 2010, we reviewed our experience of 3152 semen retrieval procedures in 500 men with SCI, spanning an 18-year period.18 A management algorithm was developed, incorporating the neurophysiology of the ejaculatory process, the relationship of level of injury to response with PVS, and other relevant clinical observations (Figure 1). The algorithm minimizes morbidity and maximizes cost-effectiveness in obtaining the highest number of TMS possible. In combination with the information gained from the patient’s history and physical, this algorithm will provide useful guidance in the management of the sperm retrieval efforts in a man with SCI.19
 |
Figure 1 A step by step algorithm for semen and/or sperm retrieval in men with spinal cord injury. Adapted from Brackett NL, Ibrahim E, Iremashvili V, Aballa TC, Lynne CM. Treatment for ejaculatory dysfunction in men with spinal cord injury: an 18-year single center experience. J Urol. 183(6):2304-2308. Available from: https://www.auajournals.org/doi/10.1016/j.juro.2010.02.018. © 2010 by American Urological Association Education and Research, Inc.18 Abbreviations: PVS, penile vibratory stimulation; EEJ, electroejaculation; SSR, surgical sperm retrieval; BCR, bulbocavernosus reflex; HFR, hip flexor reflex. |
With PVS, the ejaculation success rate was 54% when including all patients at all levels of injury. The success rate increased to 86% in when including patients whose level of injury was at or rostral to T10 (60% if the initial trial was performed with one vibrator, with an additional 26% salvage of failures if two vibrators were applied to the penis). The ejaculation success rate with PVS dropped to 21% in the group of patients whose level of injury was T11 or caudal.
The Algorithm
This algorithm (Figure 1) excludes the approximately 10% of men with SCI who can ejaculate by masturbation. If a patient is unable to ejaculate by masturbation, the first trial should be PVS, regardless of level of injury. This trial should be administered with one vibrator. If that trial fails, the choice should be made about a second trial with one vibrator, and/or a trial with two vibrators, considering the patient’s level of injury and the presence or absence of the BCR and/or HFR reflexes. If the patient fails to ejaculate by this point, he is referred for EEJ. In Brackett et al,18 sperm were found in over 90% of the patients completing the treatment algorithm.
Sperm Motility
In Brackett et al,18 some motile sperm were found in approximately 90% of the antegrade ejaculates obtained by PVS. In approximately 70% of the ejaculates obtained by PVS, ≥5million TMS were found. Table 2 shows the advantage of PVS versus EEJ in obtaining an ejaculate with the highest percent of motile sperm possible.20
 |
Table 2 Sperm Motility in Antegrade Ejaculates by Method of Ejaculation |
The Patient Encounter
On the patient’s first visit, a standard history and physical should be performed. Additionally, presence or absence of the BCR and HFR reflexes should be assessed. The patient’s level of injury should be verified according to the International Standards for Neurological Classification of Spinal Cord Injury (ISNCSCI).21 The patient should be counseled about options for assisted reproductive technologies, including the relevance of TMS to the success of each method. The initial counseling should outline the steps that will be followed in an effort to obtain the highest possible number of TMS, and how the methods for sperm retrieval will be tailored, as much as possible, to the individual’s neurological status. If applicable, discuss the management of autonomic dysreflexia, and the possible need for a bladder lavage, if little or no antegrade ejaculate is obtained.
Brief Description of the Procedure
If the patient’s level of injury is T6 or rostral, he should be pretreated appropriately to prevent or mitigate autonomic dysreflexia. Regardless, the blood pressure should be monitored throughout the procedure, preferably at one-minute intervals. Although we have, on occasion, been able to perform PVS with the patient in his wheelchair, it is preferable to transfer the patient to an exam table for ease of specimen collection, as well as safety in the event the patient develops strong spasms which could cause an injury if the patient is seated or restrained in a wheelchair. Be sure to position the blood pressure monitor so that it will be constantly visible to you or your assistant. The vibrator is then applied to the glans penis. Most patients who ejaculate do so within the first two minutes. If more time is needed, stop at the two-minute interval and check the integrity of the glans. Stop every two minutes thereafter to recheck the penile skin. A trial using two vibrators can be attempted on the same day. We recommend that no more than 10 minutes be spent at this attempt. If there is no response, a decision should be made regarding a second PVS attempt on another day using a single vibrator, two vibrators or referral for EEJ, as outlined in the algorithm (Greater detail may be found in the following references).22–24
Bladder Preparation
The bladder is always prepared in the patient’s initial visit due to the possibility of having retrograde ejaculation and in patients likely to ejaculate urine with antegrade semen. The bladder is drained applying the same method the patient uses for his daily clean intermittent catheterization. Twenty to 25 mL of sperm washing buffer is instilled into the bladder immediately prior to PVS to prevent accumulation of urine with time.
If the patient has a suprapubic catheter, the old catheter must be replaced with a new sterile one to prevent leakage due to the possible presence of sediments and bacteria in the old catheter. Bladder lavage is performed using normal saline followed by sperm wash medium to remove all sediments. Finally, 20–25 mL of sperm washing medium is left in the bladder. During the entire PVS procedure, the suprapubic catheter is clamped. Antegrade ejaculate is collected from the penile meatus as the suprapubic catheter does not preclude antegrade ejaculation.
Tips and Pointers
- Make sure the female partner has had at least a basic gynecological evaluation with respect to her fertility status.
- Monitor the blood pressure of all patients undergoing PVS.
- Patients less than one-year post-injury may be inconsistent or non-responders.
- Many patients are anxious and have their own manner in which they like to be transferred or positioned. We have found it helpful, and many of the patients are more comfortable, if their wife is present and assisting in some way. She may be the patient’s primary caregiver. Obviously, all three of you should be comfortable with this arrangement.
- Item 4 above notwithstanding, always have your own medical assistant in the room with you to help with positioning the patient, monitoring blood pressure, collecting the specimen, etc.
- Most patients will respond to PVS within 2 minutes of application of the vibrator.
- Some patients may not ejaculate on their first PVS trial. A decision about what should be the next step can be easily made by following the algorithm provided. In patients brought back for a trial with 2 vibrators, we recommend first trying again with a single vibrator. Often, this is sufficient to induce ejaculation.
- Most patients who respond to PVS, have little or no retrograde ejaculate. If no retrograde ejaculate is present on the first PVS trial, it is rarely present on subsequent PVS trials. Thus, it may not be practical to perform bladder preparation and lavage to examine the retrograde fraction in all patients, particularly if the patient’s injury is at or rostral to T10.
- It is optimal to have a microscope available to examine a drop of semen for the presence or absence of motile sperm. If motile sperm are present, follow-up semen analysis reveals ≥5 million TMS on 70% of trials.6,7,25
- The seminal plasma of men with SCI contains many white blood cells, as well as toxic cytokines. In the laboratory, the sperm motility in semen from men with SCI decreases much more rapidly than semen from non-SCI men. This decrease is exacerbated, if SCI men’s semen is stored in a 37°C incubator versus at room temperature.26 However, once processed for freezing, sperm from men with SCI freeze as reliably as samples from other non-injured men.27
Discussion
For the Practitioner Considering Incorporating PVS into His or Her Practice
You can help a lot of people. In practical terms, it may not be cost effective for many practitioners to invest in the equipment necessary to perform EEJ. Remember that only approximately 20% of the SCI population have lesions below the level of T10. Normally, they would be the population who are primary candidates for EEJ, however note that, in our experience, about 15% of this population will be found to respond to PVS, so if you become adept and comfortable with PVS only, you will have the potential to help 80% or more of the male population of SCI persons. The relatively low expense involved in obtaining one or preferably two optimized vibrators should make it reasonable for any practitioner to offer PVS to all men with SCI, knowing that you will be able to obtain an ejaculate from the overwhelming majority of them while being comfortable referring non-responders to a center where EEJ is practiced. If you are not comfortable dealing with patients with SCI, try to visit a practice or center that deals with them. Plan to have at least one of your personnel who will be helping you accompany you. A Genito-urinary fertility practice that does PVS/EEJ is preferable since you will get tips on management of both PVS and autonomic dysreflexia. The male fertility program at the Miami Project is available for teaching practitioners.
Conclusion
PVS is the first choice as a method of sperm retrieval in men with SCI. It is safe, non-invasive, reliable, and cost effective for both the patient and practitioner. The learning curve is not steep. In many instances, it can be taught to a couple who can then perform PVS at home with intravaginal insemination of the ejaculate timed to the woman’s ovulatory cycle. If the patient has a level of injury which might predispose him to autonomic dysreflexia, certain precautions must be observed as for any procedure on such a patient. PVS is the single most efficacious procedure for sperm retrieval with the potential to offer the most choices in assisted reproduction to the majority of the SCI population.
Acknowledgments
The Miami Project was founded in 1985 by neurosurgeon, Barth Green, MD, in collaboration with the families of three patients suffering from SCI. The author would like to acknowledge Mr. Teodoro C. Aballa for his assistance in collecting data for this review.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wagoner N. John Hunter (1728–1793). Embryo Project Encyclopedia. 2017;2017:38.
2. Ombelet W, Van Robays J. Artificial insemination history: hurdles and milestones. Facts Views Vision ObGyn. 2015;7(2):137–143.
3. Horne HW, Paull DP, Munro D. Fertility studies in the human male with traumatic injuries of the spinal cord and cauda equina. N Engl J Med. 1948;239(25):959–961. doi:10.1056/NEJM194812162392504
4. Halstead LS, VerVoort S, Seager SW. Rectal probe electro stimulation in the treatment of anejaculatory spinal cord injured men. Paraplegia. 1987;25(2):120–129. doi:10.1038/sc.1987.21
5. Sonksen J, Biering-Sorensen F, Kristensen JK. Ejaculation induced by penile vibratory stimulation in men with spinal cord injuries. The importance of the vibratory amplitude. Paraplegia. 1994;32(10):651–660. doi:10.1038/sc.1994.105
6. Kathiresan AS, Ibrahim E, Aballa TC, Attia GR, Lynne CM, Brackett NL. Pregnancy outcomes by intravaginal and intrauterine insemination in 82 couples with male factor infertility due to spinal cord injuries. Fertil Steril. 2011;96(2):328–331.
7. Kathiresan AS, Ibrahim E, Aballa TC, et al. Comparison of in vitro fertilization/intracytoplasmic sperm injection outcomes in male factor infertility patients with and without spinal cord injuries. Fertil Steril. 2011;96(3):562–566. doi:10.1016/j.fertnstert.2011.06.078
8. Brackett NL, Padron OF, Lynne CM. Semen quality of spinal cord injured men is better when obtained by vibratory stimulation versus electroejaculation. J Urol. 1997;157(1):151–157.
9. Ohl DA, Sonksen J, Menge AC, McCabe M, Keller LM. Electroejaculation versus vibratory stimulation in spinal cord injured men: sperm quality and patient preference. J of Urol. 1997;157(6):2147–2149.
10. National SCI Statistical Center. Spinal cord injury facts and figures at a glance. Available from: https://www.nscisc.uab.edu/Public/Facts%20and%20Figures%202020.pdf.
11. Bird VG, Brackett NL, Lynne CM, Aballa TC, Ferrell SM. Reflexes and somatic responses as predictors of ejaculation by penile vibratory stimulation in men with spinal cord injury. Spinal Cord. 2001;39(10):514–519. doi:10.1038/sj.sc.3101200
12. Wieder J, Brackett N, Lynne C, Green J, Aballa T. Anesthetic block of the dorsal penile nerve inhibits vibratory-induced ejaculation in men with spinal cord injuries. Urology. 2000;55(16):915–917. doi:10.1016/S0090-4295(99)00608-1
13. Phillips AA, Elliott SL, Zheng MM, Krassioukov AV. Selective alpha adrenergic antagonist reduces severity of transient hypertension during sexual stimulation after spinal cord injury. J Neurotrauma. 2015;32(6):392–396. doi:10.1089/neu.2014.3590
14. Krassioukov A, Warburton DE, Teasell R, Eng JJ. A systematic review of the management of autonomic dysreflexia after spinal cord injury. Arch Phys Med Rehabil. 2009;90(4):682–695.
15. Claydon VE, Elliott SL, Sheel AW, Krassioukov A. Cardiovascular responses to vibrostimulation for sperm retrieval in men with spinal cord injury. J Spinal Cord Med. 2006;29(3):207–216. doi:10.1080/10790268.2006.11753876
16. Sheel AW, Krassioukov AV, Inglis JT, Elliott SL. Autonomic dysreflexia during sperm retrieval in spinal cord injury: influence of lesion level and sildenafil citrate. J Appl Physiol. 2005;99(1):53–58.
17. Sinha V, Elliott S, Ibrahim E, Lynne CM, Brackett NL. Reproductive health of men with spinal cord injury. Top Spinal Cord Inj Rehabil. 2017;23(1):31–41. doi:10.1310/sci2301-31
18. Brackett NL, Ibrahim E, Iremashvili V, Aballa TC, Lynne CM. Treatment for ejaculatory dysfunction in men with spinal cord injury: an 18-year single center experience. J Urol. 2010;183(6):2304–2308. doi:10.1016/j.juro.2010.02.018
19. Brackett NL, Lynne CM, Ibrahim E, Ohl DA, Sonksen J. Treatment of infertility in men with spinal cord injury. Nat Rev Urol. 2010;7(3):162–172.
20. Kathiresan AS, Ibrahim E, Modh R, Aballa TC, Lynne CM, Brackett NL. Semen quality in ejaculates produced by masturbation in men with spinal cord injury. Spinal Cord. 2012;50(12):891–894. doi:10.1038/sc.2012.71
21. Betz S, Biering-Sørensen BS. The 2019 revision of the international standards for neurological classification of spinal cord injury (ISNCSCI)-what’s new? Spinal Cord. 2019;57(10):815–817.
22. Ibrahim E, Jensen CFS, Sunara I, et al. Evaluation of a re-engineered device for penile vibratory stimulation in men with spinal cord injury. Spinal Cord. 2021;59(2):151–158. doi:10.1038/s41393-020-0515-6
23. Ibrahim E, Brackett NL, Lynne CM. Advances in the management of infertility in men with spinal cord injury. Asian J Androl. 2016;18(3):382–390. doi:10.4103/1008-682X.178851
24. Brackett NL. Semen retrieval by penile vibratory stimulation in men with spinal cord injury. Hum Reprod Update. 1999;5(3):216–222. doi:10.1093/humupd/5.3.216
25. Kafetsoulis A, Brackett NL, Ibrahim E, Attia GR, Lynne CM. Current trends in the treatment of infertility in men with spinal cord injury. Fertil Steril. 2006;86(4):781–789.
26. Brackett NL, Santa-Cruz C, Lynne CM. Sperm from spinal cord injured men lose motility faster than sperm from normal men: the effect is exacerbated at body compared to room temperature. J Urol. 1997;157(6):2150–2153. doi:10.1016/S0022-5347(01)64699-8
27. Padron OF, Brackett NL, Weizman MS, Lynne CM. Semen of spinal cord injured men freezes reliably. J Androl. 1994;15:266–269.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Antioxidant Nanoparticles Restore Cisplatin-Induced Male Fertility Defects by Promoting MDC1-53bp1-Associated Non-Homologous DNA Repair Mechanism and Sperm Intracellular Calcium Influx
Wei YS, Chen YL, Li WY, Yang YY, Lin SJ, Wu CH, Yang JI, Wang TE, Yu J, Tsai PS
International Journal of Nanomedicine 2023, 18:4313-4327
Published Date: 7 August 2023