Back to Journals » Psychology Research and Behavior Management » Volume 12
Peer victimization, depressive symptoms and non-suicidal self-injury behavior in Chinese migrant children: the roles of gender and stressful life events
Received 10 May 2019
Accepted for publication 23 July 2019
Published 13 August 2019 Volume 2019:12 Pages 661—673
DOI https://doi.org/10.2147/PRBM.S215246
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Quanquan Wang, Xia Liu
Institute of Developmental Psychology, Faculty of Psychology, Beijing Normal University, Beijing, People’s Republic of China
Background: Non-suicidal self-injury (NSSI) has become a worldwide health concern, especially for the disadvantaged group such as Chinese rural-to-urban migrant children. Peer victimization is a risk factor for NSSI and is quite common among Chinese migrant children. However, few studies that focused on this group have paid attention to the relationship between peer victimization and NSSI. The current study addressed this gap in the literature by examining the mediating role of depressive symptoms and the moderating role of stressful life events in the relationship between peer victimization and NSSI in male and female migrant children.
Methods: A total of 650 migrant children completed self-report surveys that addressed peer victimization, NSSI, depressive symptoms, and stressful life events.
Results: Results showed that peer victimization was significantly related to NSSI for both migrant girls and boys. Depressive symptoms mediated the relationship between peer victimization and NSSI among girls, but not among boys. Additionally, stressful life events significantly moderated the relationships between depressive symptoms and NSSI and between peer victimization and NSSI among girls; higher levels of depressive symptoms or peer victimization coupled with more stressful life events related to a higher probability of NSSI. For boys, stressful life events moderated the relationship between peer victimization and NSSI; higher levels of peer victimization combined with increased NSSI behaviors among the boys who reported more stressful life events.
Conclusions: These findings contribute to the understanding of the mechanisms that inform the relationship between peer victimization and NSSI. Moreover, they indicate that future interventions can be enhanced by targeting depressive symptoms among girls and stressful life events among both girls and boys.
Keywords: peer victimization, non-suicidal self-injury, depressive symptoms, stressful life events, gender, Chinese migrant children
Introduction
Non-suicidal self-injury (NSSI) is defined as the deliberate and direct mutilation of one’s own body tissue without suicidal intent;1 it may include hitting, burning, cutting, scratching, and banging.2 NSSI usually peaks in adolescence and has been shown to be associated with many mental health issues such as depression, substance use, eating disorders, borderline personality disorder, and even suicidal behavior.2,3 Given its high prevalence and serious consequences for adolescents, NSSI has become a prominent worldwide health concern. In China, the incidence rate has ranged from 17.0% to 29.2% in different non-clinical samples.4,5
Adolescents who experience adversity tend to engage in NSSI.2 Chinese rural-to-urban migrant children are such a disadvantaged group due to parental migration. An unprecedented rural-to-urban migration has accompanied the rapid industrialization that began in China during the early 1980s. Hundreds of millions of rural farmers flooded the big cities in search of a better life. In contrast to past migration patterns, many parents now migrate with their children.6 By the end of 2015, the number of migrant children had reached 14 million, representing an increase of 10.14% since 2010.6 However, due to China’s household registration system, migrants—especially children—endure marginalization.7 The Chinese household registration system creates a dual system of citizenship and represents a formidable institutional barrier for migrant children to the rights granted their local peers.8 According to this policy, resource allocation is based upon a household’s registration in their place of origin. People from rural areas are unable to obtain this registration, even when they have settled in a place for years. Therefore, migrant children are often treated quite differently from the locals in many aspects, including restricted access to local schools, health care, and social services.9 Given this negative developmental environment, it is urgent to pay special attention to migrant children’s mental health. Previous studies have shown that migrant children are more vulnerable to various psychological problems than their local counterparts.10 However, little is known about the prevalence of the serious behavioral problem of NSSI and associated mechanisms among this group.
Peer victimization is a risk factor for NSSI.2 Peer victimization is “the experience among children of being a target of the aggressive behavior of other children.”11 It is one of the biggest challenges that migrant children have faced due to their designation as “outsiders” or “newcomers”.12,13 Related studies have shown that approximately 21.8% of migrant children had been bullied14 and over 70% had experienced peer victimization,15 a number much greater than the average rate of 19% in other samples.16 These negative peer relationships could result in serious consequences for mental health.11 The relationship between peer victimization and NSSI also has been proven in both cross-sectional and longitudinal studies using ordinary samples.17 However for Chinese migrant children, despite the high prevalence of peer victimization, little is known about its relationship with NSSI behavior. Therefore, the first aim of the present study was to examine the relationship between peer victimization and NSSI among Chinese rural-to-urban migrant children.
The fact that not all migrant children who have experienced peer victimization would engage in NSSI implied that there might be other factors which influence the connection between the two. Based on previous findings, the present study aimed to examine depressive symptoms as the mediator, as well as stressful life events as the moderator in this process. We identified depressive symptoms as the mediator for two reasons. First, many empirical studies evidenced peer victimization to be a predictor of depression among adolescents.11,18 Stress theory19 explains the connection by suggesting that the stress resulting from peer victimization could impair individuals’ psychosocial functioning and cause distress emotions such as depression.18 Second, the link between depressive symptoms and NSSI has been documented, and this can be interpreted as depression impacts the affect-regulation function that contributes to self-injury behavior.20,21 Moreover, general strain theory22 provided a theoretical foundation for the mediating role of depressive symptoms. According to this theory, peer victimization is a good example of the type of relationship that could cause high levels of strain or stress. Consequently, the strain could arouse negative emotions such as depression that, could cause individuals to engage in problem behaviors such as NSSI. Some scholars have used this theory to explore the relationship among peer victimization, depression, and NSSI to identify a partially mediating role of depression.23,24
However, previous evidence of the mediating role of depressive symptoms in the association between peer victimization and NSSI was limited and sometimes equivocal,25 indicating that this mediation link might be influenced by other factors. We proposed that gender differences could impact the role that depression potentially plays in the relationship between peer victimization and NSSI. For example, there are gender differences relating to NSSI. First, prior research has shown that gender is an important predictor of NSSI, with greater prevalence among females than males.26,27 Second, other studies implied that there were gender differences regarding the NSSI characteristics or developmental patterns,28,29 indicating that there could be different mechanisms in males and females. In addition to NSSI, gender differences also existed in depressive symptoms.30 Related empirical studies have shown that adolescent girls are more likely to experience higher levels of depression than boys.31 Taken together, these gender differences relating to NSSI and depressive symptoms could, therefore, shape the role that depressive symptoms might play in the relationship between peer victimization and NSSI.
There have been a variety of institutional and environmental challenges that migrant children have faced, such as discrimination, strict access to schools, and cultural adaption.10 These stressful life events that have permeated many aspects of migrant children’s lives should be of great concern because they have been proven to be prominent risk factors for NSSI.32 The current study included a close examination of the moderating effect of stressful life events. The diathesis-stress model provides a theoretical foundation for an exploration of the interaction between stress and depression.33 The model suggests that adolescents with certain diatheses, such as risk-related cognitive types, “vulnerability” or “provoking” factors, and genetic inheritance, are at high risk for severe mental problems when exposed to stressful life events.33 Empirical studies on suicidal behavior and NSSI have provided evidence for this model that accounts for the moderating effect of stressful life events.27,34 In the current study, migrant children who have experienced depressive symptoms may be regarded as vulnerable and more likely to face the stress that could cause NSSI. Thus, we hypothesized that stressful life events would moderate the relationship between depression and NSSI.
Moreover, we anticipated that stressful events would also interact with peer victimization in the association with depressive symptoms and NSSI. Although there has been no direct evidence about the interaction between stressful life events and peer victimization yet, related studies found that recent stressful events or perceived stress could create risk for the poor quality of peer relationship,35,36 which has been proven to be associated with depressive symptoms and NSSI.37,38 Meanwhile, as a negative peer relationship, peer victimization can be regarded as specific interpersonal stress,39 whereas stressful life events include the general stress result from daily life events involves many domains, such as failing an exam, being criticized by teacher, having a quarrel with a good friend. Previous studies have shown that the combination of certain specific stress and chronic daily stressful events have an accumulative negative effect that could impact an individual’s mental health.40 Furthermore, the increase of stressful life events might impair the positive effect of certain protective factors, and in turn enhance the likelihood of mental health problems. For example, it has been found that in the context of extreme adversity, resilience would lose its power in countering the negative outcomes.41
In summary, the current study aimed to address the gap in the literature regarding the relationship between peer victimization and NSSI through an examination of the mediating role of depressive symptoms and the moderating effect of stressful life events among Chinese migrant boys and girls. Several hypotheses guided the research: 1) The relationship between peer victimization and NSSI would be significant among both girls and boys; 2) depressive symptoms would mediate the relationship between peer victimization and NSSI, the mediating effect would be moderated by gender, with stronger mediating effect among migrant girls than boys; 3) The moderating effect of stressful life events on the relationship between peer victimization and NSSI via depressive symptoms would be significant among both boys and girls, including all three stages of the mediated model through depressive symptoms. The hypothesized model appears in Figure 1.
 |
Figure 1 Hypothesized model of the relationship among peer victimization, non-suicidal self-injury, depressive symptoms and stressful life events for both girls and boys. |
Methods
Participants
To select the target subjects, we first contacted the principal of local educational center (Urumqi city, China) to launch an announcement about the survey and recruit eligible adolescents. A total of 701 migrant children were recruited and fully completed the survey. 51 subjects were excluded for the following reasons: from non-intact family due to parental divorce, from non-intact family due to parental loss, mistakes in the answers. The final sample consisted of 650 students; 332 boys and 318 girls. The average age was 13.37 years (SD=1.48, range=10–15). All participants migrated with their parents from rural areas to local cities. The average length of residence in the local city was 5.86 years (SD=1.88). All participants belonged to the Han ethnic group, which is the predominant ethnic group in China. The education level of their parents ranged from primary school or below to college degree or above, with an average education between junior high school and high school.
The study was approved by the Research Ethics Committee of Beijing Normal University and complied with the Declaration of Helsinki involving human subjects. Prior to the study, consent letters including the introduction of the survey were sent to participants and their parents. They were also informed that the participation was completely voluntary. Written informed consent was obtained from all participants and their parents. The questionnaires were completed during school hours, lasted approximately 40 mins. During the session, two of the researchers and at least one teacher from the school were present. All participants were encouraged to provide honest answers. After the survey, each participant received a prize through pens and notebooks.
Measures
Peer victimization
Peer victimization was measured with an adapted version of the Multidimensional Peer-Victimization Scale.42 The adapted version consists of 21 items, covering four types of peer victimization including physical victimization (item such as “during the semester, other classmates have pushed or kicked me”), verbal victimization (“during the semester, other classmates have scolded me”), relational victimization (“during the semester, other classmates have ignored me on purpose”), and property victimization (“during the semester, other classmates have stolen from me”). Participants rated all items on a 4-point Likert scale with “0=never” to “3=always.” Mean scores of all items were used; higher scores indicated a greater number of peer victimization incidents. The scale has been successfully used in Chinese children and exhibited good validity.43 The Cronbach’s alpha was 0.94.
NSSI
We used a modified version of the Deliberate Self-Harm Inventory (DSHI) to measure migrant children’s NSSI. The original scale was constructed and validated by Gratz,44 then adapted by Lundh, Karim, and Quilisch45 for adolescents, with good validity. Participants rated each item (“I pierce my skin with sharp objects”) on a 5-point scale from “1=never” to “5=always” according to their experiences during the past six months. Mean scores were used, and higher scores indicated a greater frequency of NSSI. The Cronbach’s alpha coefficient was 0.90.
Depression
The Center for Epidemiologic Studies Depression Scale for children (CES-DC)46 was used for screening depressive symptoms in migrant children during the past semester in school.47 The CES-DC exhibited good validity in previous studies with Chinese adolescents.48 Participants responded to 20 items (such as “I don’t think I can concentrate on my work”) on a 4-point Likert scale ranging from 1 (never) to 4 (always). Mean scores were used for analysis. Higher scores indicated a greater risk for depression. The Cronbach’s alpha coefficient was 0.98.
Stressful life events
Stressful life events were measured with the Stressful Life Events Scale for Chinese migrant children and adolescents.49 The Scale consisted of twelve items involve many domains, such as “I failed the exam,” “I was criticized or punished by the teacher,” and “I had a quarrel with my good friend.” Each event was weighted indifferently. Participants responded to each item on a 3-point scale ranging from 1 (never) to 3 (always) according to their experiences during the past 12 months. Higher scores indicated that the participants had experienced more stressful life events than those with lower scores. This scale has been successfully used in previous research with Chinese migrant children.50 The Cronbach’ alpha was 0.76.
Data analysis
Three analyses were conducted. First, a preliminary analysis was conducted to compute the correlations among the main variables, including peer victimization, depressive symptoms, NSSI, and stressful life events. Second, we examined the mediated model of peer victimization- depressive symptoms -NSSI for girls and boys. The third analysis tested the moderating effect of stressful life events for girls and boys. Besides, previous research has found that some sociodemographic variables including migrant children’ age and length of residence in the host cities would account for the individual differences relating to peer victimization, stress, and depressive symptoms.10 Thus, age and length of residence were controlled for in all of the following analyses.
We used IBM SPSS version 20 to perform the correlation analysis. For the mediation model analyses, we used PROCESS51,52 to perform bias-corrected bootstrapping mediation analyses with 5000 samples. The mediating effect of depressive symptoms between peer victimization and NSSI was tested by using Model 4. If the mediating model was significant, we continued with the PROCESS to conduct the moderating analyses with Model 59. Consistent with our hypothesis, Model 59 could examine the moderating role of stressful life events in all three stages of the mediation link, including peer victimization and depressive symptoms, depressive symptoms and NSSI, peer victimization and NSSI. However, if the mediating effect was not significant, a hierarchical regression analysis approach was used to test the moderating effect of stressful life events. Slope tests were conducted afterward if any interaction proved significant.
In addition, less than 5% of the data were missing and the chi-square test for Little’s MCAR was non-significant, χ2(38) = 44.39, p = 0.22, indicating that data is missing completely at random. Thus, the listwise deletion was used to deal with the missing data.
Results
Preliminary analyses
A total of 18.9% participants reported having engaged in one or more types of NSSI behavior at least once in the past six months, with no significant difference between boys and girls, χ2 (1, N=650) =0.23, p>0.1. A significant gender difference was found for peer victimization; boys reported having been victimized more than girls (p<0.05). There were no gender differences for the other variables. The means and standard deviations of correlations among the variables of the whole sample were presented in Table 1.
 |
Table 1 Correlations, means, and standard deviations among the study variables (N=650) |
The correlations, means, and standard deviations among the main variables for girls and boys appear in Table 2. As shown, peer victimization was positively correlated with depressive symptoms, NSSI, and stressful life events for both girls and boys. Stressful life events were positively correlated with both depressive symptoms and NSSI among girls and boys. Because age and length of time of residence in host cities were not of primary concern, they were treated as covariates in the subsequent analysis.
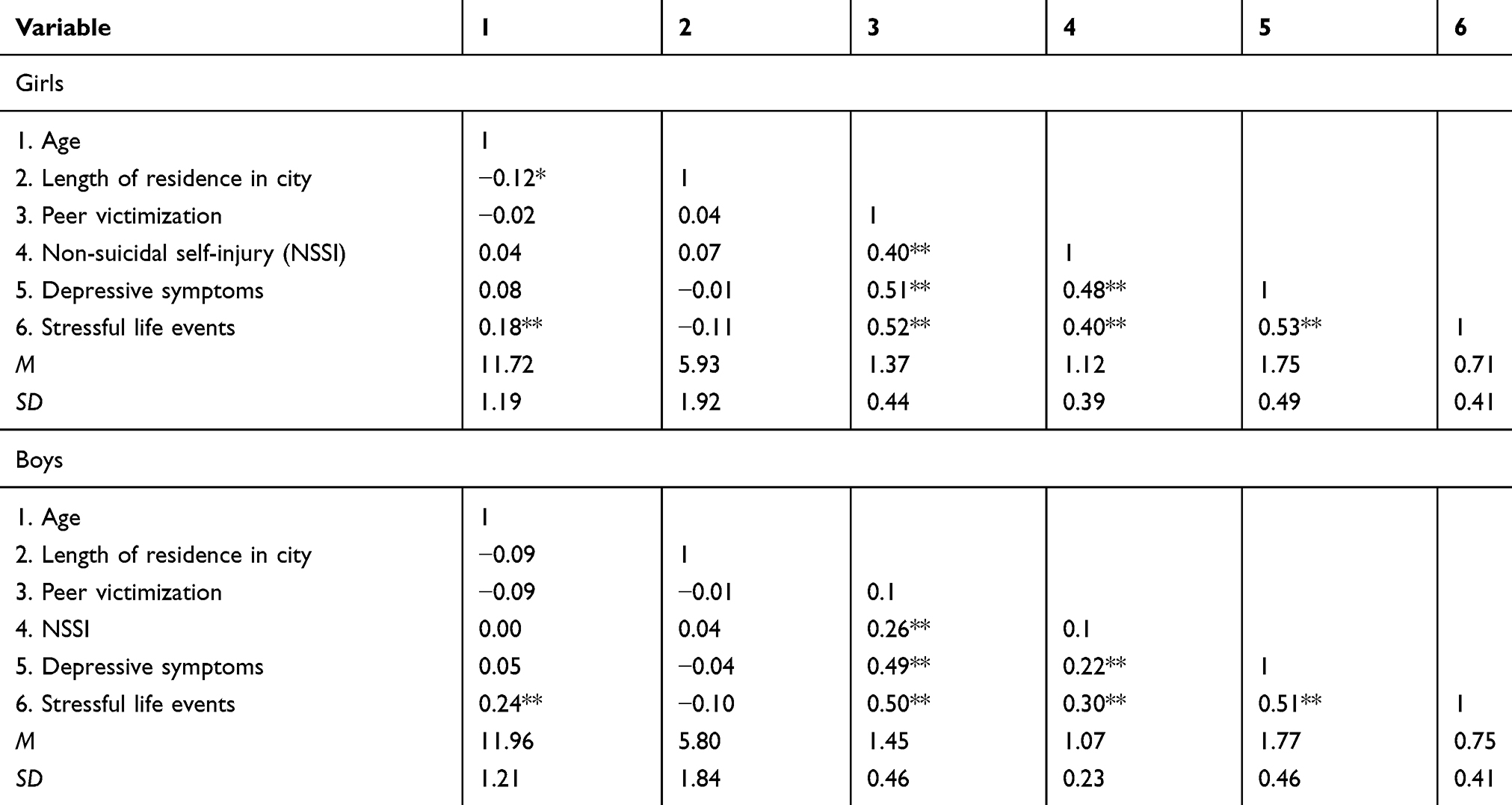 |
Table 2 Correlations, means, and standard deviations among the study variables by gender (N=650) |
Peer victimization, depressive symptoms, stressful life events, and NSSI among girls
Figure 2 illustrates that the link between peer victimization and NSSI via depressive symptoms was significant for the girls in the study, with the indirect effect of depressive symptoms was 0.15, SE=0.06, 95%CI [0.05, 0.29]. In addition, before adding depressive symptoms as a mediator, the regression coefficient for the direct link between peer victimization and NSSI was significant, B=0.35, 95%CI [0.26, 0.44]. With the addition of depressive symptoms to the analysis, the association between peer victimization and NSSI was still significant (B=0.21, SE=0.05, 95%CI [0.10, 0.31], indicating that depressive symptoms played a partial mediating role in the relationship between peer victimization and NSSI. Depressive symptoms accounted for 42.4% of the variance in the total effect of peer victimization on NSSI.
 |
Figure 2 The mediating model of depressive symptoms in the relationship between peer victimization and non-suicidal self-injury among girls. ***p<0.001. |
Also for migrant girls, after adding stressful life events as a moderator, the moderated mediation model was significant (R2=0.39, p<0.001). The interaction between depressive symptoms and stressful life events for NSSI was significant (B=0.62, p<0.001; 95% CI=[0.42, 0.83]), as was the interaction between peer victimization and stressful life events for NSSI (B=−0.45, p<0.001; 95% CI=[−0.69, −0.20]) (see Figure 3). Slopes tests were conducted subsequently. As shown in Figure 4, depressive symptoms was significantly positively associated with NSSI with high (+1 standard deviation) levels of stressful life events (B=0.41, t=6.44, p<0.001), but not with low (−1 standard deviation) levels of stressful life events (B=−0.09, t=−1.21, p>0.05). As displayed by Figure 5, the association between peer victimization and NSSI was significant with high levels of stressful life events (B=0.58, t=5.90, p<0.001), but not with low levels of stressful life events (B=0.08, t=0.98, p>0.05).
 |
Figure 3 Peer victimization, depressive symptoms, stressful life events and non-suicidal self-injury among girls. **p<0.01, ***p<0.001. |
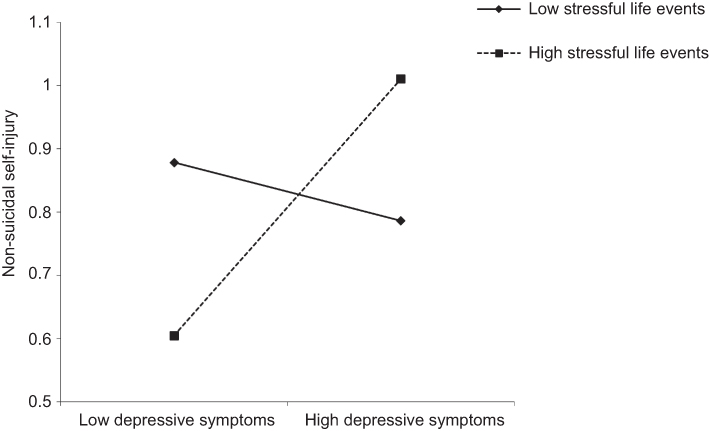 |
Figure 4 Stressful life events as a moderator of the relationship between depressive symptoms and non-suicidal self-injury among girls. |
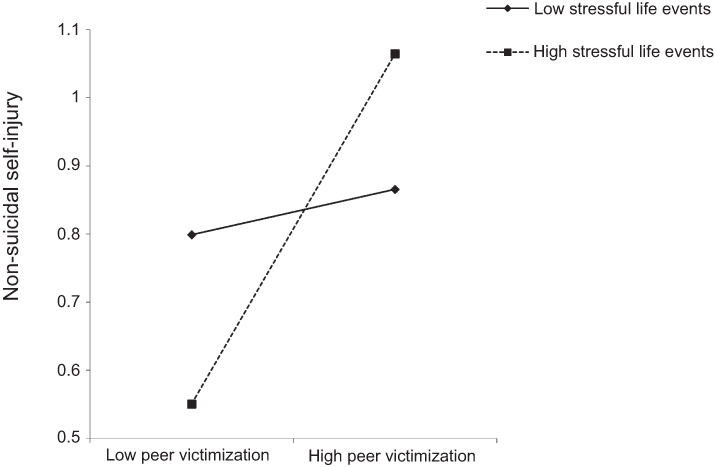 |
Figure 5 Stressful life events as a moderator of the relationship between peer victimization and non-suicidal self-injury among girls. |
Correspondingly, the conditional indirect effect of peer victimization on NSSI through depressive symptoms was significant with high levels of stressful life events, with the indirect effect was 0.17, SE=0.06, 95%CI [0.05, 0.31], but not with the low levels of stressful life events, with the indirect effect was −0.03, SE=0.04, 95%CI [−0.14, 0.02]. The interaction between peer victimization and stressful life events was not significant with regard to depressive symptoms.
Peer victimization, depressive symptoms, stressful life events, and NSSI among boys
The mediating effect of depressive symptoms was not significant among the boys (the indirect effect was=0.03, SE=0.02, 95%CI [−0.02, 0.08]). A hierarchical regression analysis was used to examine the moderating effect of stressful life events on the relationship between peer victimization and NSSI. As shown in Table 3, peer victimization and stressful life events were both positively and significantly related to NSSI. The interaction term (peer victimization × stressful life events) was significant. Thus, stressful life events moderated the relationship between peer victimization and NSSI. As illustrated in Figure 6, a simple slope analysis showed that the association between peer victimization and NSSI was significant with high levels of stressful life events (B=0.12, t=2.79, p<0.01), but not with low levels of stressful life events (B=−0.06, t=−1.02, p>0.05); increased peer victimization, coupled with high levels of stressful events, were more likely to engage in NSSI behaviors.
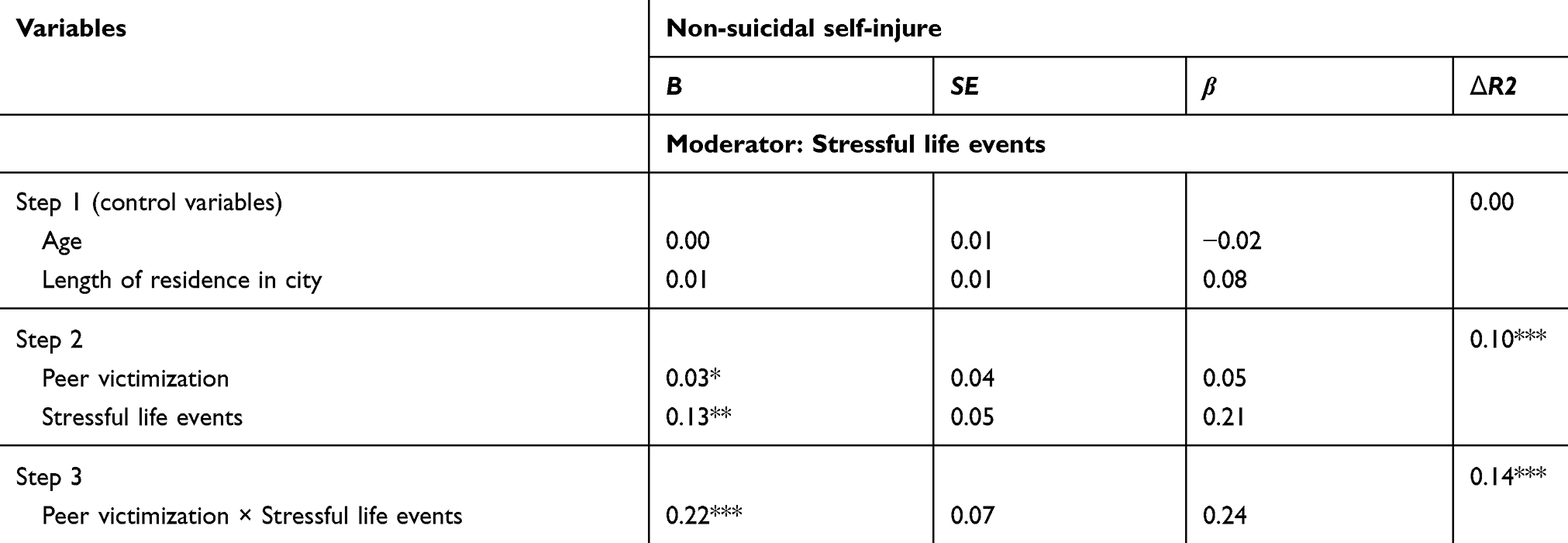 |
Table 3 Hierarchical multiple regression analyses to test the moderating effects of stressful life events on the relationship between peer victimization and non-suicidal self-injury (NSSI) among boys |
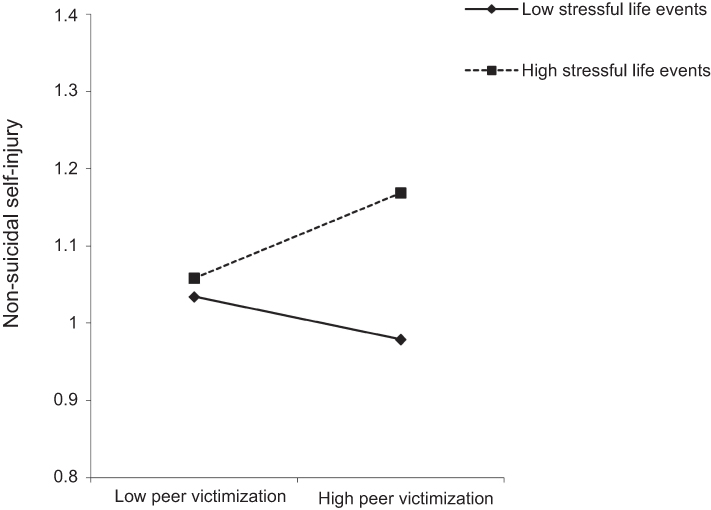 |
Figure 6 Moderating effect of stressful life events on the relationship between peer victimization and non-suicidal self-injury among boys. |
Discussion
Three main conclusions may be derived from this study. First, peer victimization evidenced a significant positive association with NSSI. Second, depressive symptoms mediated the relationship between peer victimization and NSSI among girls, but not among boys. Third, the moderating effect of stressful life events proved significant for both girls and boys. For girls, both the relationships between depressive symptoms and NSSI and between peer victimization and NSSI were moderated. Boys with high levels of stressful life events who experienced peer victimization were more likely to engage in NSSI.
Overall, more than 18.9% of the participants had engaged in at least one form of NSSI during the past six months; there were no significant differences between girls and boys. This rate of NSSI was similar to ones reported in previous studies.4,5 88.0% of the participants reported having experienced peer victimization; a rate much higher than those found in previous studies with non-migrant adolescents.16 Consistent with our hypothesis and also in line with previous findings,17 peer victimization was significantly related to NSSI among migrant children. It is of note that the correlations seem low between peer victimization, depressive symptoms, NSSI, and stressful life events. This might because some protective factors (such as social support) might play a positive effect,10 which was not the primary concern for the current study. More importantly, the low correlations between the main variables echoed the current findings that multiple stressors (such as the interaction of peer victimization and stressful life events) would do greater harm to individuals’ mental health than just one specific source of stress (such as peer victimization only), which we would explain more below.
The second aim of our study was to examine the mediating role of depressive symptoms. Consistent with our hypothesis, the results revealed a gender difference in the link between peer victimization and NSSI via depressive symptoms. Specifically, the girls’ depressive symptoms partially mediated the relationship between peer victimization and NSSI. This result reaffirmed findings from previous studies23,24 and evidenced the general strain theory.22 However, there was no significant mediating effect of depressive symptoms for boys; peer victimization directly related to NSSI behavior. There might be two possible explanations for this deviation. First, the direct link between peer victimization and NSSI without depressive symptoms among boys could be related to norms of male socialization that encourage boys to endure negative events such as peer victimization without expressing their emotions.53 Therefore, it could be that the boys would perceive NSSI as a more appropriate outlet for their feelings. Previous studies have found that a highly developed socialization of masculinity was associated with low levels of depression.54 In addition, the different mediating effects of depressive symptoms could also be due to the different understandings that boys and girls had of peer victimization. Negative relationships with peers often cause girls to experience feelings of “isolation” or “loss” that could elicit negative emotional responses, such as depression.55 For boys, however, peer victimization creates a power imbalance.56 Boys could use self-injury as a means to show strength or seek status among their peers.53
For girls, consistent with our hypothesis and previous studies,32 stressful life events were significantly related to NSSI. The moderating effect of stressful life events in the girls’ mediated model also proved significant. The results showed that both the relationships between depressive symptoms and NSSI and between peer victimization and NSSI were moderated. For the former, the fact that depressive symptoms were significantly associated with higher levels of NSSI among adolescent girls who reported more stressful life events and not among the girls who reported less stressful life events, reaffirmed the diathesis-stress model mentioned above.33 According to this model, high levels of stressful life events placed adolescent girls who already had experienced depression at an increased risk for engaging in NSSI. Another possible explanation focuses on the influence of stressful life events on individuals’ coping strategies. Previous studies have shown that a higher level of stress was associated with increased rumination.57 Rumination has proven to be significantly related to adolescent girls’ depression58 and could account for the occurrence of NSSI.
Also among girls, for the interaction between stressful life events and peer victimization regarding NSSI, results showed that the increase of peer victimization among participants who had experienced higher levels of stressful life events resulted in a greater likelihood of engaging in NSSI than their peers who had experienced lower levels of stress. This finding is consistent with previous studies that suggested the role played by stressful life events in the accumulative effect of multilevel stressors.40 This finding has important implications for migrant children as a group that has faced various stressors in their daily lives other than peer victimization.10 Daily stresses increased individuals’ arousal and make them more sensitive to negative events59 that, in turn, add to the effect of peer victimization on NSSI. Contrary to our hypothesis, the indirect path from peer victimization to depressive symptoms was not moderated by stressful life events. This could be related to the unique link between peer victimization and depression. Previous studies have shown that different types of stressors would lead to different psychological problems.60 It could be that stressful life events might be more weakly linked to depressive symptoms than peer victimization for these migrant girls.
The entire model of moderating and mediating factors for migrant girls proved dependent on the level of stressful life events. The mediating effect through depressive symptoms is only significant when accompanied by high levels of stressful life events. It could be that with a decrease in stressful life events, the combination of stressors with peer victimization also decreased; protective factors functioned. As mentioned above, previous research has shown that certain protective factors, such as resilience, could prove ineffective at countering the negative outcomes in the context of extreme adversity.41 Therefore, in this study, a decrease in overall stress could provide an opportunity for possible protective factors related to NSSI to function, such as resilience.
For migrant boys, depressive symptoms did not mediate the relationship between peer victimization and NSSI. However, similar with girls, stressful life events moderated the association between peer victimization and NSSI; higher levels of victimization related to higher levels of NSSI for the boys who reported high levels of stressful life events. These findings again highlight the effect of multiple stressors. This would suggest that a decrease in stressful life events could reduce the association between peer victimization and NSSI.
Several limitations merit attention. First, regarding peer victimization, we evaluated the general peer victimization instead of distinguishing the different subtypes, such as physical victimization, verbal victimization, relational victimization, and property victimization. It could be that different types of victimization related to NSSI represent different mechanisms.60 Future research could attend to the types of peer victimization relating to NSSI. In addition, we used the CES-DC to assess depressive symptoms in the current study, rather than DSM depression symptoms or depression diagnoses, future research should adopt more diverse tools (such as the DSM or depression diagnoses) to obtain a broader picture of this issue. The same goes for NSSI that only the NSSI frequency was considered in the current study, but not severity and types. Future research should address this issue. Second, the results could have proven more compelling, if methods in addition to self-reporting had been used to assess the key variables. Future studies can use reports from parents, teachers, and peers to cross-validate the self-reported data. Third, the current study used a cross-sectional design which might have limited our ability to explore the precise temporal sequence of the data. The assumption of the mediation link of peer victimization - depressive symptoms - NSSI in the current study is based on a solid theoretical and empirical foundation. We have also run the test to further check the alternative model of depressive symptoms-peer victimization–NSSI. The result showed that the association between depression and NSSI via peer victimization was not significant (the indirect effect was 0.09, p>0.05), indicating that the mediating model of peer victimization-depressive symptoms-NSSI was more effective. Yet, a longitudinal study in the future is recommended to get a deeper understanding of the relationships among peer victimization, depression, stressful life events, and NSSI. Fourth, a control group of non-migrant children has not included in the current study. Future research may sample local adolescents who are non-migrants as well to gain greater insight into the relationships among peer victimization, NSSI, depressive symptoms, and stressful life events. Moreover, given the disadvantaged environment for migrant children, a critical next step in this important and novel line of work will be to explore the perceived reasons for victimization.
Despite these limitations, there are several important contributions to this study. For the first time, gender differences were examined in the mediating model of peer victimization and NSSI via depressive symptoms. This finding suggests that intervention strategies would need to be designed in such a way that attends to these gender differences. For example, the mediating effect of depressive symptoms among girls suggests that mental health interventions could be included when there have been incidents of peer victimization.61 Schools could provide psychological counseling on a regular basis to assure that emotional problems are identified in a timely fashion. Thus, we can break the link between peer victimization and NSSI by avoiding depressive symptoms among migrant girls. For migrant boys, since the link between peer victimization and NSSI was direct, and independent of depressive symptoms, parents and teachers should give more attention to reduce their experiences of peer victimization. For example, the anti-bullying programs62 may aid in decreasing the prevalence of peer victimization for migrant boys.
The finding that depression or peer victimization was associated with NSSI with high levels of stressful life events but not with low levels of stressful life events, indicated that there is a need for greater attention to the stress that migrant children endure. The accumulation of stressors, including peer victimization and stressful life events, were critical to the development of NSSI among both girls and boys. This finding contributes to the literature on NSSI in general as they suggest that the impact of peer victimization should be examined in relation to general stress rather than as independent risk factor. Future interventions designed to prevent migrant children who experience peer victimization from engaging in NSSI behavior should focus on minimizing the general stressful events that could affect them, because peer victimization proved more strongly associated with NSSI when other stressors were present. Given their important role in migrant children’s lives, schools could prove quite valuable as sites for interventions. Previous studies have shown that some social activities initiated by school teachers or social workers provided migrant children opportunities to adapt to the school environment, as well as to enjoy respect and care from their teachers and peers.63 Besides, although this study did not examine the effect of protective factors directly, the results implied that these factors would be effective in the context of low levels of stressful life events. Consequently, schools and families could cultivate positive environmental and individual’ factors, such as high-quality parent-child relationships64 and appropriate coping strategies57 that would help to manage stress.
Acknowledgments
We would like to acknowledge all participating schools, the participants, and our cooperators for assistance in data collection. This work was supported by National Social Science Fund of China (14BSH078).
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th Edition, American Psychiatric Publishing, Arlington, 2013.
2. Nock MK. Self-injury. Annu Rev Clin Psychol. 2010;6:339–363. doi:10.1146/annurev.clinpsy.121208.131258
3. Hamza CA, Stewart SL, Willoughby T. Examining the link between non-suicidal self-injury and suicidal behavior: a review of the literature and an integrated model. Clin Psychol Rev. 2012;32:482–495. doi:10.1016/j.cpr.2012.05.003
4. Tang J, Li J, Chen B, et al. Prevalence of and risk factors for non-suicidal self-injury in rural China: results from a nationwide survey in China. J Affect Disord. 2018;226(15):188–195. doi:10.1016/j.jad.2017.09.051
5. Wan YH, Xu SJ, Chen J, Hu CL, Tao FB. Longitudinal effects of psychological symptoms on non-suicidal self-injury: a difference between adolescents and young adults in China. Soc Psychiatry Psychiatr Epidemiol. 2015;50(2):237–247. doi:10.1007/s00127-014-0917-x
6. Yang DP, Wei JY, Qin DP. Annual Report on Education for China’s Migrant Children (2016). Beijing: Social Sciences Academic Press; 2017.
7. Wong DFK, Chang YL, He XS. Rural migrant workers in urban China: living a marginalized life. Int J Soc Welf. 2007;16(1):32–40. doi:10.1111/j.1468-2397.2007.00475.x
8. Fan X. Educational Innovation. Changsha: Hunan People’s Publishing House; 2001.
9. Wang JL, Hsieh HF, Assari S, Gaskin J, Rost DH. The protective effects of social support and engagement coping strategy on the relationship between perceived discrimination and psychological distress among Chinese migrant children. Youth Soc. 2018;50(5):593–614. doi:10.1177/0044118X15619804
10. Shen JL. The Psychological Development and Education of Disadvantaged Children. Beijing: Economic Science Press; 2009.
11. Hawker DS, Boulton MJ. Twenty years’ research on peer victimization and psychosocial maladjustment: a meta-analytic review of cross-sectional studies. J Child Psychol Psychiatry. 2000;41:441–455. doi:10.1111/1469-7610.00629
12. Fan Y. Research on the integration of migration children and local students. Contemp Youth Stud. 2008;6:23–28.
13. Ye Z, Chen LH, Harrison SE, Guo HY, Li XM, Lin DH. Peer victimization and depressive symptoms among rural-to-Urban migrant children in China: the protective role of resilience. Front Psychol. 2016;7. doi:10.3389/fpsyg.2016.01542
14. Tan Q. School bullying and school adjustment among urban migrant children in China. Theory Pract Contemp Edu. 2010;2:94–96.
15. Guo HY, Chen LH, YE Z, Pan J, Lin DH. Characteristics of peer victimization and the bidirectional relationship between peer victimization and internalizing problems among rural-to-urban migrant children in China: a longitudinal study. Acta Psychologica Sinica. 2017;49(3):336–348. doi:10.3724/SP.J.1041.2017.00336
16. Zhang W. Prevalence and major characteristics of bullying/victimization among primary and junior middle school children. J Chin Psychol Acta Psychologica Sinica. 2002;34(4):387–394.
17. Van Geel M, Goemans A, Vedder P. A meta-analysis on the relation between peer victimization and adolescent non-suicidal self-injury. Psychiatry Res. 2015;230:364–368. doi:10.1016/j.psychres.2015.08.029
18. Pouwelse M, Bolman C, Lodewijkx H, Spaa M. Gender differences and social support: mediators or moderators between peer victimization and depressive feelings? Psychol Sch. 2011;48(8):800–814. doi:10.1002/pits.v48.8
19. Zautra AJ. Emotions, Stress and Health. New York: University Press; 2003.
20. Klonsky ED. The functions of deliberate self-injury: a review of the evidence. Clin Psychol Rev. 2007;27:226–239. doi:10.1016/j.cpr.2006.08.002
21. Wang Q, Wei M, Liu X. The psychological mechanism and influential factors of adolescent NSSI: an emotion regulation perspective. Psychol Dev Educ. 2017;33(6):759–768.
22. Agnew R, Brezina T, Wright JP, Cullen FT. Strain, personality traits, and delinquency: extending general strain theory. Criminology. 2002;40:43–72. doi:10.1111/crim.2002.40.issue-1
23. Claes L, Luyckx K, Baetens I, Van de Ven M, Witteman C. Bullying and victimization, depressive mood, and non-suicidal self-injury in adolescents: the moderating role of parental support. J Child Fam Stud. 2015;24(11):3363–3371. doi:10.1007/s10826-015-0138-2
24. Hay C, Meldrum R. Bullying victimization and adolescent self-harm: testing hypotheses from general strain theory. J Youth Adolesc. 2010;39:446–459. doi:10.1007/s10964-009-9502-0
25. Karanikola MNK, Lyberg A, Holm A, Severinsson E. The association between deliberate self-harm and school bullying victimization and the mediating effect of depressive symptoms and self-stigma: a systematic review. Biomed Res Int. 2018;2018. doi:10.1155/2018/4745791
26. Bresin K, Schoenleber M. Gender differences in the prevalence of non-suicidal self-injury: a meta-analysis. Clin Psychol Rev. 2015;38:55–64. doi:10.1016/j.cpr.2015.02.009
27. Guerry JD, Prinstein MJ. Longitudinal prediction of adolescent non-suicidal self-injury: examination of a cognitive vulnerability-stress model. J Clin Child Adolesc Psychol. 2010;39:77–89. doi:10.1080/15374410903401195
28. Margaret SA, Jennifer MP, Brandon EG, Carolyn MP. An examination of non-suicidal self-injury in men: do men differ from women in basic NSSI characteristics? Arch Suicide Res. 2010;14:79–88. doi:10.1080/13811110903479086
29. Yang XY, Xin MY. “Boy crisis” or “girl risk”? The gender difference in nonsuicidal self-injurious behavior among middle-school students in China and its relationship to gender role conflict and violent experiences. Am J Men’s Health. 2018;12(5):1275–1285. doi:10.1177/1557988318763522
30. Nolen-Hoeksema S. Gender differences in depression. Curr Dir Psychol Sci. 2001;10(5):173–176. doi:10.1111/1467-8721.00142
31. Salk RH, Hyde JS, Abramson LY. Gender differences in depression in representative national samples: meta-analyses of diagnoses and symptoms. Psychol Bull. 2017;143(8):783–822. doi:10.1037/bul0000102
32. Tang J, Yang W, Ahmed NI, et al. Stressful life events as a predictor for non-suicidal self-injury in southern Chinese adolescence: a cross-sectional study. Medicine. 2016;95(9). doi:10.1097/MD.0000000000002637
33. Scott BP. Major depression epidemiology from a diathesis-stress conceptualization. Patten BMC Psychiatry. 2013; 13. doi:10.1186/1471-244X-13-19
34. Wang YQ, Sareen J, Afifi TO, Bolton SL, Johnson EA, Bolton JM. A population-based longitudinal study of recent stressful life events as risk factors for suicidal behavior in major depressive disorder. Arch Suicide Res. 2015;19(2):202–217. doi:10.1080/13811118.2014.957448
35. Bonn M. Associations between peer relations in childhood and adversity. Early Child Dev Care. 1995;105:77–91. doi:10.1080/0300443951050109
36. Herd T, Li MJ, Maciejewski D, et al. Inhibitory control mediates the association between perceived stress and secure relationship quality. Front Psychol. 2018;9. doi:10.3389/fpsyg.2018.00217
37. Smith M, Calam R, Bolton C. Psychological factors linked to self-reported depression symptoms in late adolescence. Behav Cogn Psychother. 2009;37:73–85. doi:10.1017/S1352465808004724
38. Yurkowski K, Martin J, Levesque C, Bureau JF, Lafontaine MF, Cloutier P. Emotion dysregulation mediates the influence of relationship difficulties on non-suicidal self-injury behavior in young adults. Psychiatry Res. 2015;228(3):871–878. doi:10.1016/j.psychres.2015.05.006
39. Swearer SM, Hymel S. Understanding the psychology of bullying moving toward a social-ecological diathesis-stress model. Am Psychol. 2015;70(4):344–353. doi:10.1037/a0038929
40. March-LlanesLaia J, Marqués-Feixa L, Mezquita L, Fañanás L, Moya-Higueras J. Stressful life events during adolescence and risk for externalizing and internalizing psychopathology: a meta-analysis. Eur Child Adolesc Psychiatry. 2017;26(12):1409–1422. doi:10.1007/s00787-017-0996-9
41. Vanderbilt-Adriance E, Shaw DS. Conceptualizing and re-evaluating resilience across levels of risk, time, and domains of competence. Clinical child and family. Psychol Rev. 2008;11:30–58.
42. Mynard H, Joseph S. Development of the multidimensional peer-victimization scale. Aggress Behav. 2000;26:169–178. doi:10.1002/(ISSN)1098-2337
43. Zhu B, Lei L. The relationship between perceptions of control and victimization of adolescents. Psychol Dev Educ. 2005;21(1):91–95.
44. Gratz KL. Measurement of deliberate self-harm: preliminary data on the deliberate self-harm inventory. J Psychopathol Behav Assess. 2001;23(4):253–263. doi:10.1023/A:1012779403943
45. Lundh LG, Karim J, Quilisch E. Deliberate self-harm in 15-year-old adolescents: a pilot study with a modified version of the deliberate self-harm inventory. Scand J Psychol. 2007;48(1):33–41. doi:10.1111/j.1467-9450.2007.00567.x
46. Fendrich M, Warner V, Weissman MM. Family risk factors, parental depression, and psychopathology in off spring. Dev Psychol. 1990;26:40–50. doi:10.1037/0012-1649.26.1.40
47. Olsson G, von Knorring A-L. Depression among Swedish adolescents measured by the self-rating scale Center for Epidemiology Studies- Depression Child (CES-DC). Eur Child Adolesc Psychiatry. 1997;6:81–87.
48. Yuan XJ, Fang XY, Liu Y, Lin XY. The relationship between stress coping, depression and social anxiety among migrant children: a longitudinal study. Psychol Dev Educ. 2012;28(3):283–291.
49. Wang H, Xiong Y, Liu X. The protective roles of parent-child relationship and friend support on emotional and behavioral adjustment of migrant adolescents. Psychol Dev Educ. 2018;34(5):614–624.
50. Liu JR, Wang Q. Stressful life events and the development of integrity of rural-to-urban migrant children: the moderating role of social support and beliefs about adversity. Dev Educ Psychol. 2018;34(5):548–557.
51. Hayes AF. An Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression- Based Approach. New York, NY: Guilford Press; 2013.
52. Hayes AF. 2016. Process Version 2.16.2. Available from : http://processmacro.org/index.html
53. Jonathan DG, Jaclyn CK, Annie ML, Michael EA, Brian PM. The association between masculinity and non-suicidal self-injury. Am J Men’s Health. 2018;12(1):30–40. doi:10.1177/1557988315624508
54. Wupperman P, Neumann CS. Depressive symptoms as a function of sex-role, rumination, and neuroticism. Pers Individ Dif. 2006;49(2):189–201. doi:10.1016/j.paid.2005.05.017
55. Rose AJ, Rudolph KD. A review of sex differences in peer relationship processes: potential trade-offs for the emotional and behavioral development of girls and boys. Psychol Bull. 2006;132:98–131. doi:10.1037/0033-2909.132.1.98
56. Luukkonen AH, Räsänen P, Hakko H, Riala K. Bullying behavior is related to suicide attempts but not to self-mutilation among psychiatric inpatient adolescents. Psychopathology. 2009;42:131–138. doi:10.1159/000204764
57. Michl LC, McLaughlin KA, Shepherd K, Nolen-Hoeksema S. Rumination as a mechanism linking stressful life events to symptoms of depression and anxiety: longitudinal evidence in early adolescents and adults. J Abnorm Psychol. 2013;122(2):339–352. doi:10.1037/a0031994
58. Jose PE, Brown I. When does the gender difference in rumination begin? Gender and age differences in the use of rumination by adolescents. J Youth Adolesc. 2008;37(2):180–192. doi:10.1007/s10964-006-9166-y
59. Langrock AM, Compas BE, Keller G, Merchant MJ, Copeland ME. Coping with the stress of parental depression: parents’ reports of children’s coping, emotional, and behavioral problems. J Clin Child Adolesc Psychol. 2002;31:312–324. doi:10.1207/S15374424JCCP3103_03
60. Martin PB, Johan O, Frank CV, Albertine JO. Peer stressors and gender differences in adolescents’ mental health: the TRAILS study. J Adolesc Health. 2010;46:444–450. doi:10.1016/j.jadohealth.2009.10.002
61. Meng N. Reflections on the mental health education in schools. Educ Explor. 2006;2:88–89.
62. Ttofi MM, Farrington DP. Effectiveness of school-based programs to reduce bullying: a systematic and meta-analytic review. J Exp Criminol. 2011;7:27–56. doi:10.1007/s11292-010-9109-1
63. Wang L (2015). A Group Social Work Plan: Peer Group Social Support Positively Affects Migrant Children [Doctoral dissertation]. Wuhan, China: Central China Normal University. doi:10.1094/PDIS-09-14-0954-PDN
64. Zhang WX, Fuligni AJ. Authority, autonomy, and family relationships among adolescents in urban and rural China. J Res Adolesc. 2006;12(4):527–537. doi:10.1111/j.1532-7795.2006.00506.x
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.