Back to Journals » Journal of Blood Medicine » Volume 13
Patterns of Bone Marrow Confirmed Malignant and Non-Malignant Hematological Disorders in Patients with Abnormal Hematological Parameters in Northeast Ethiopia
Authors Ebrahim H ![]() , Fisha T
, Fisha T ![]() , Debash H, Bisetegn H
, Debash H, Bisetegn H ![]()
Received 25 October 2021
Accepted for publication 24 January 2022
Published 15 February 2022 Volume 2022:13 Pages 51—60
DOI https://doi.org/10.2147/JBM.S346091
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Hussen Ebrahim, Temesgen Fisha, Habtu Debash, Habtye Bisetegn
Department of Medical Laboratory Sciences, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia
Correspondence: Hussen Ebrahim, Department of Medical Laboratory Sciences, College of Medicine and Health Sciences, Wollo University, Dessie, 1145, Ethiopia, Tel +251 921332772, Email [email protected]
Background: Hematological disorders are heterogeneous conditions ranging from malignant to non-malignant disorders. Hematological malignancies comprise a collection of heterogeneous conditions originating from cells of the bone marrow and the lymphatic system. Therefore, this study aimed to determine the pattern of bone marrow confirmed malignant and non-malignant hematological disorders in patients with abnormal hematological parameters.
Methods: Institutional-based cross-sectional study was conducted in Dessie town from April 2020 to June 2021. A total of 228 study participants who had abnormal hematological parameters and referred for bone marrow examination were included consecutively. About 1.5 mL of bone marrow sample and 3 mL of venous blood sample were collected for bone marrow examination, complete blood count analysis and peripheral blood morphology examination. Wright stain, Sudan black B, and Prussian blue stains were used for staining the bone marrow and peripheral blood smears. The result was expressed in mean and standard deviation and presented in texts and tables. Ratio, frequency, and percentage were used to express the magnitude of malignant and non-malignant hematological disorders.
Results: The overall prevalence of hematological malignancies among the study participants was 11.4% with 8.8% in male patients. The prevalence of hematological malignancies were 3.5% CML, 2.6% AML, 1.8% CLL and MM, 0.9% ALL and undifferentiated acute leukemia. On the other hand, 57.0% of the study participants had non-malignant hematological disorders. Regarding non-malignant hematological cases, 24.6% were erythroid hyperplasia, 10.5% aplastic anemia, 8.8% concomitant IDA and MBA, 7.0% MBA, 3.5% leukemoid reaction, 1.8% IDA, and 0.9% visceral leishmaniasis. In patients with HM, 66.7% of AML, 100% of CML and CLL, and 75% of MM patients had increased total WBC count, whereas 66.7% of AML, 62.5% of CML, 75% of CLL, and 50% of MM patients had decreased hemoglobin level. On the other hand, 66.7% of AML, and 50% of CML, ALL, and CLL patients had decreased platelet count.
Conclusion: In this study, 11.4% of the patients had hematological malignant cases, whereas 57% of the patients had non-malignant hematological cases. Therefore, in patients with hematological abnormalities and where conclusive diagnosis could not be made through clinical and other laboratory investigations, bone marrow examination should be done for definitive diagnosis, management and prognosis.
Keywords: hematological malignancies, non-malignant hematological disorders, leukemia, anemia, Ethiopia
Background
Hematological disorders are heterogeneous conditions ranging from malignant to non-malignant disorders.1,2 Hematological malignancies comprises a collection of heterogeneous conditions originating from cells of the bone marrow and the lymphatic system.3 The World Health Organization (WHO) classified hematologic malignancies into myeloid neoplasms, lymphoid neoplasms, mast cell disorders, and histiocytic neoplasms primarily based on cell line involvement in neoplastic transformation.4,5 Distinct neoplasms are defined and characterized according to a combination of morphology, immunophenotype, genetic, and clinical features of the patients.6 Bone marrow examination (BME) is required as complementary with complete blood count analysis and peripheral blood morphology examination to confirm the diagnosis of hematological disorders.1,7
Hematologcial malignancies can be classified into different groups that include leukemia, lymphoma, multiple myeloma (MM), myelodysplastic syndrome (MDS), polycytemia vera (PV), myeloproliferative neoplasms (MPNs) and primary myelofibrosis.8,9 Based on hematopoietic stem cell involvement and progression of the diseases, leukemia can be grouped into four main groups that include acute myeloid leukemia (AML), acute lymphoblastic leukemia (ALL), chronic myeloid leukemia (CML), chronic lymphocytic leukemia (CLL) whereas lymphoma can be grouped into non-Hodgkin lymphoma (NHL) and Hodgkin lymphoma (HL).10,11
Acute leukemia is a proliferation and invasion of immature hematopoietic cells (blasts) in the bone marrow as well as invasion of peripheral blood circulation, solid organs, and lymphatic system. French American British (FAB) has been traditionally set as a minimum of 30% blast cells to diagnose acute leukemia.12 However, WHO revised the criteria and set as the minimum of 20% of blast cells to diagnose acute leukemia.4,5 Acute myelogenous leukemia is the proliferation of leukemic blasts including myeloblasts, monoblasts, megakaryoblasts, erythroblasts, and their precursors in undifferentiated, minimally, or moderately differentiated stages in the bone marrow.13 Acute lymphoblastic leukemia is a malignant transformation and proliferation of lymphoid progenitor cells characterized by uncontrolled proliferation of abnormal, immature lymphocytes and their progenitors of B and T-lymphocytes. Moreover, ALL is predominant leukemia that affects children. However, around 75% of adult ALL cases affect the B-cell phenotype, whereas the remaining 25% cases affect the T-cell phenotype.14
Chronic leukemia is characterized by uncontrolled proliferation and expansion of mature, differentiated cells of the hematopoietic system in the bone marrow as well as in peripheral circulation.8 Chronic myeloid leukemia is a group of heterogeneous related conditions that affects the myeloid hematopoietic cell lines including the granulocyte, monocyte, erythrocyte, and megakaryocyte cells.15 Chronic lymphocytic leukemia relatively affects mature lymphoid cells of the B and T-cell phenotypes.16 According to the global cancer statistics report by 2018, there was an estimate of a total of 437 thousand new cases and 309 thousand cancer-related deaths from leukemia worldwide. It is the eleventh leading cause of cancer-related mortality.17 Leukemia accounted for approximately 3.4% of all new cancer cases and 3.8% of all cancer-related deaths worldwide in 2020.18 Hematological malignancies can affect all age groups but children and older adult individuals are the most affected populations. The incidence rates of all types of leukemia are slightly higher in males as compared to females and it might be affected by geographical and ethnic variations.19 The causes for HM are not precisely known. Epidemiological studies have been suggested that several risk factors might be associated with the development and the increased risk for HM such as prolonged exposure to ionizing radiation, exposure to benzene, formaldehyde, organic solvents, agricultural pesticides, and herbicides, cigarette smoking, previous cancer treatment with both chemotherapy and radiation therapy, immunological, genetic disorders, and infection with oncogenic retroviruses.3,19
Non-malignant hematological disorders are agroup of diverse conditions ranging from inherited conditions like hemophilia and sickle cell disease to common non-hereditary conditions such as venous thromboembolism and different types of anemia.20 Anemia is the condition associated with reduced numbers of red blood cells (RBC) or decreased hemoglobin level (Hgb) and it can be grouped into different categories based on the cause such as nutritional, hemolytic, and aplastic anemia.21,22 Nutritional anemia is mainly associated with the deficiency of iron, vitamin B12, folic acid, hormones, other vitamins, and minerals, whereas hemolytic anemia occurs due to premature RBCdestruction and aplastic anemia is due to bone marrow failure.20,23
Bone marrow examination has wide application in clinical medicine for the diagnosis and monitoring of the therapy of malignant, non-malignant hematological disorders, and various systemic diseases of unknown origin.24,25 There have been few studies conducted to investigate the magnitude of malignant and non-malignant hematological disorders using bone marrow examinations in poor resource setting countries including Ethiopia. Even, there was no similar study conducted in the study area to assess the magnitude of malignant and non-malignant hematological disorders which are difficult to make conclusive differential diagnosis through clinical and other laboratory investigations. Therefore, the main aim of this study is to determine the magnitude of malignant and non-malignant hematological disorders among patients with abnormal hematological parameters.
Methods and Materials
Study Design, Period, and Area
A prospective institutional-based cross-sectional study was conducted in Dessie town diagnostic medical laboratory pathology department, Northeast Ethiopia from April 2020 to June 2021. The diagnostic laboratory is found in Dessie town about 401 Km far from the North of Addis Ababa, the capital of Ethiopia. The diagnostic laboratory gives both routine and advanced medical laboratory services for patients who came from private and governmental health institutions. It serves as a bone marrow examination and diagnostic center for hematological malignancies referred from both private and government health institutions in the town as well as from the surrounding area.
Study Population, Participants, and Sampling Techniques
The study population comprises all patients who had abnormal hematological parameters and referred to underwent bone marrow examination by their physicians. Thus, a total of 228 study participants who visited the diagnostic laboratory with a request form for bone marrow examination were included in the study consecutively during the study period.
Data Collection and Laboratory Analysis
Socio-demographic characteristics information of study participants were collected using a structured questionnaire. About 1.5 mL of bone marrow sample was collected aseptically by an experienced and licensed internist from the iliac bone after giving local anesthesia of 2% lidocaine hydrochloride and direct bone marrow smears were prepared for examinations. About 3 mL of venous blood sample was collected for complete blood count (CBC) analysis as well as peripheral blood smear preparations. Furthermore, wright stain, Sudan black B, and Prussian blue stains were used for staining the smears and then the preparations were examined by experienced and licensed pathologist.
Data Quality Management
Bone marrow and blood samples were collected and processed according to the standard operating procedures (SOPs). Then, blood samples were properly mixed and homogenized by inverting 8–10 times following strict specimen safety and handling procedures. Bone marrow and peripheral blood smears preparation and examinations were conducted strictly according to SOPs. The performance of the automated hematology analyzer was maintained through the daily running of three-level controls (low level, medium level, and high level) quality control materials. Furthermore, daily background checking was carried out routinely. Automated analyzers and other equipment were cleaned daily before leaving the laboratory as routine day-to-day activities.
Data Management, Statistical Analysis, and Interpretation
Data were coded, entered, and cleaned using Epi Data 3.1 version and then exported to statistical package for social sciences (SPSS) version 23.0 (IBM Corporation, Armonk, NY, USA). The result was expressed in mean and standard deviation and presented in texts and tables. Ratio, frequency, and percentage were used to express the magnitude of malignant and non-malignant hematological disorders.
Results
Magnitude of Hematological Malignancies Among Study Participants
In this study, a total of 228 study participants who had abnormal hematological parameters and were referred for bone marrow examination were included. The mean ± SD age of the study participants was 35.51 (±14.02) with the minimum and maximum age of the study participants included in the study between 15 and 75 years. Out of 228 study participants, 130 (57%) were males. Furthermore, the majority of the study participants, 128 (56.1%) were grouped within the age between 15 and 35 years. Moreover, the overall prevalence of HM was 11.4% (26/228) with a higher prevalence was among male patients with a prevalence of 8.8% (20/228). The prevalence of HM diagnosed was; 3.5% of CML, 2.6% of AML, 1.8% of CLL, and MM, 0.9% of ALL, and undifferentiated acute leukemia. Besides, 76.9% of hematological malignant cases were dominant among male patients as compared to females (3.3:1 ratio). In addition, 38.5% of HM cases were acute leukemia (AL) and 46.2% cases were chronic leukemia (CL). In this study, 30.8% of cases of AL were found within the younger age range between 15 and 35 years, whereas 38.5% of cases of CL were found within the adult age range between 36 and 55 years. However, 7.7% of cases MM were found within the younger age range and the remaining 7.7% cases of MM were found within the adult age range (Table 1).
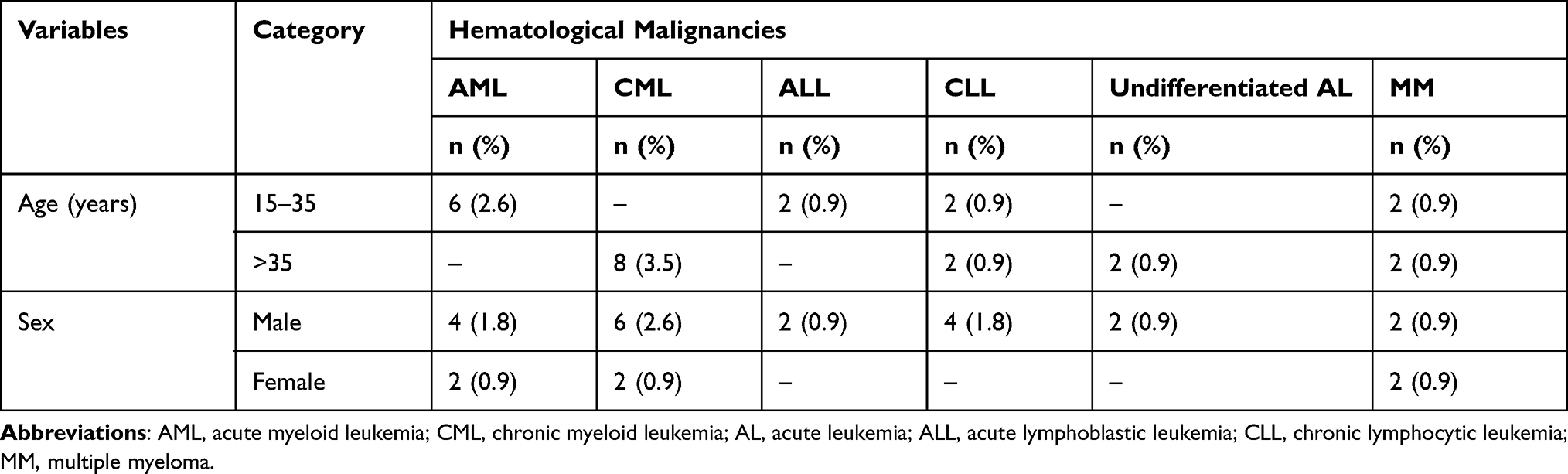 |
Table 1 Magnitude of Hematological Malignancies Among Study Participants in Northeast Ethiopia from April 2020 to August 2021 (n = 228) |
Magnitude of Non-Malignant Hematological Disorders Among Study Participants
In this study, 57% (130/228%) of the patients had non-malignant hematological disorders. Out of this, 74 (32.5%) cases of non-malignant hematological disorders belonged to female patients. Non-malignant hematological disorders diagnosed in the patients were 56 (24.6%) cases of erythroid hyperplasia, 24 (10.5%) cases of aplastic anemia, 20 (8.8%) cases of concomitant IDA and MBA, 16 (7.0%) cases of MBA, 8 (3.5%) cases of leukemoid reaction, 4 (1.8%) cases of IDA, and 2 (0.9%) cases of visceral leishmaniasis. In this study, 30 (13.2%) cases of erythroid hyperplasia followed by 18 (7.9%) cases of concomitant IDA and MBA were found between the age of 15 and 35 years. On the other hand, 20 (8.8%) cases of erythroid hyperplasia followed by 10 (4.4%) cases of aplastic anemia were found between the age of 36 and 55 years. The dominant cases diagnosed in male patients were erythroid hyperplasia accounted for 32 (14%) followed by aplastic anemia accounted for 12 (5.3%) cases, whereas concomitant IDA and MBA which accounted for 20 (8.8%) of cases followed by MBA accounted for 12 (5.3%) cases were dominant in female patients (Table 2).
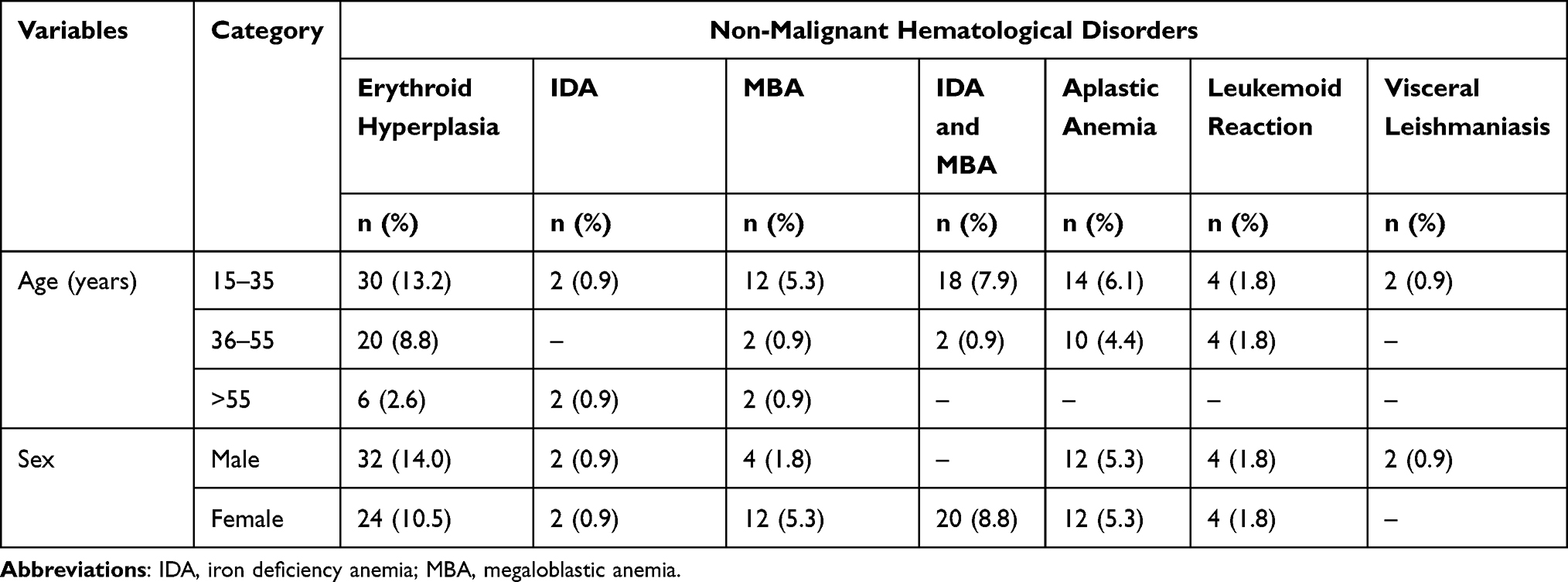 |
Table 2 Magnitude of Non-Malignant Hematological Disorders Among Study Participants in Northeast Ethiopia from April 2020 to August 2021 (n = 228) |
Patterns of Hematological Parameters Among Patients with Hematological Malignancies
In this study, hematological parameters in confirmed patients with HM were assessed. The finding showed that leucocytosis, anemia, and thrombocytopenia were common among patients. Among patients with HM, 66.7% of AML, 100 of % CML and CLL, and 75% of MM patients had increased total WBC count (leucocytosis), whereas 66.7% of AML, 62.5% of CML, 75% of CLL, and 50% of MM patients had decreased hemoglobin levels (anemia). On the other hand, 66.7% of AML, and 50% of CML, ALL, and CLL patients had decreased platelet count (thrombocytopenia) (Table 3).
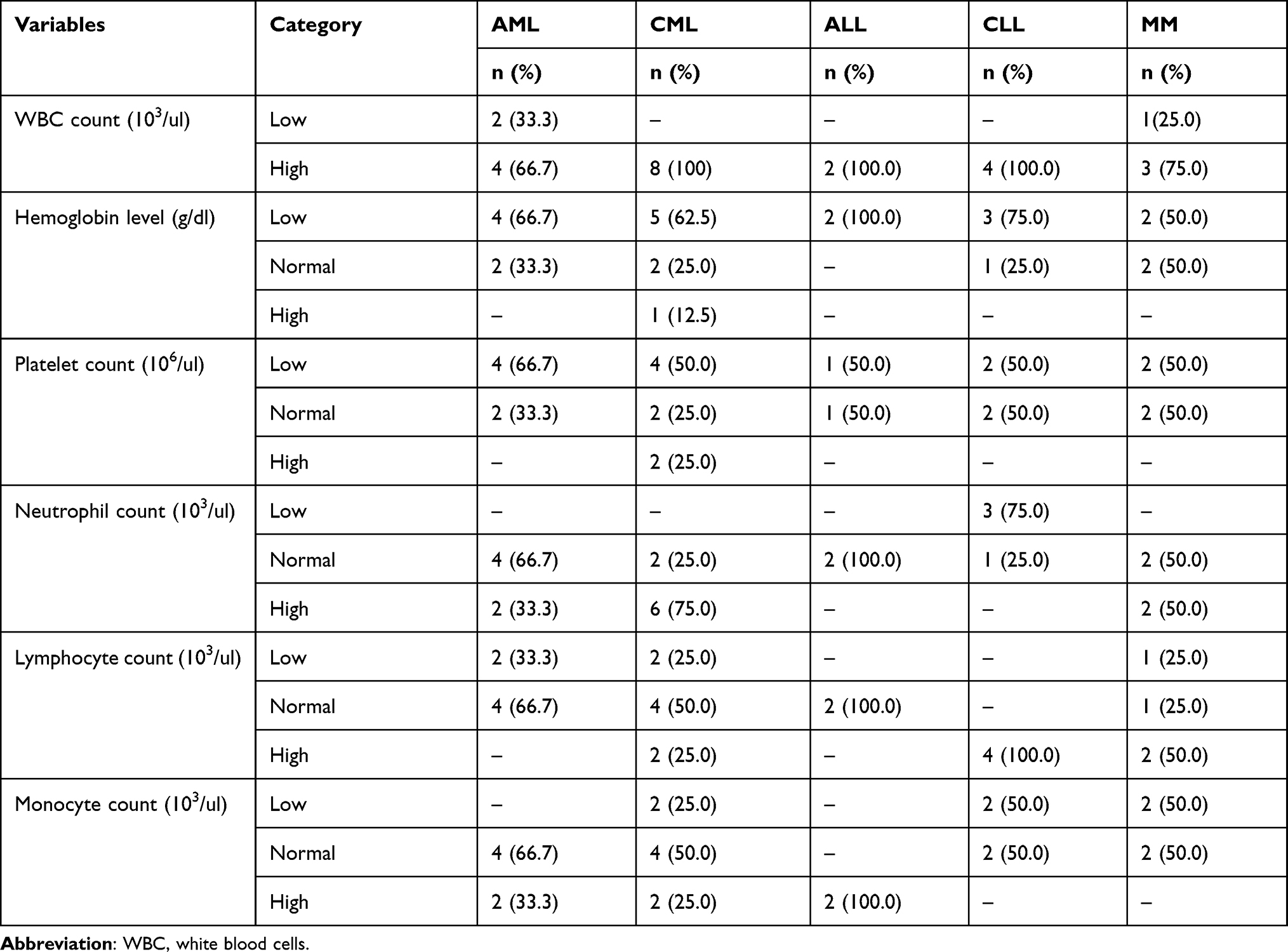 |
Table 3 Patterns of Hematological Parameters in Patients with Hematological Malignancies in Northeast Ethiopia from April 2020 to August 2021 (n = 26) |
Discussion
Hematological malignancies are a group of neoplastic disorders that arise from a malignant transformation of cells of the bone marrow or the lymphatic systems.8 A multi-diagnostic approach should be used for the correct diagnosis of hematological malignancies.26,27 In this study, the overall prevalence of HM was 11.4% (26/228) in which CML was the dominant case accounted for 3.5% followed by AML (2.6%) then, CLL and MM (1.8%), and ALL and undifferentiated acute leukemia (0.9%). This result was similar to the findings reported in Morocco (10.9%), and Ethiopia (9.3%).26,28 The current prevalence was low compared to the result reported in Eritrea (25.1%), in India (58%), and Togo (31%).29–31 The possible reasons for this variation might be the variations in sample size, study population, geographical location, and socio-demographic pattern.
In this study, the finding showed that 38.5% of HM cases were AL out of confirmed cases. This was consistent with the findings reported in India, Saudi Arabia, and Bangladesh.32–34 Acute leukemia is a malignant clonal disorder of blood-forming organs involving one or more cell lines in the hematopoietic system characterized by diffuse replacement of bone marrow with abnormal immature and undifferentiated hematopoietic cells (blasts).35–37 In the current study, the result showed that 46.2% of HM was chronic leukemia. This result was in line with the findings reported in India (49.5%) and in Togo (46.7%)31,32 while low findings were reported in India (28.5%) and Bangladesh (18.2%) compared to the present finding.9,30 Chronic leukemia is a broad spectrum of diseases characterized by uncontrolled proliferation and expansion of mature, differentiated cells of the hematopoietic system.15,38,39 Furthermore, multiple myeloma (MM) was the lowest case accounted 15.4% out of confirmed HM cases. This result was consistent with the finding in Morocco (12.4%)26 whereas the present result was higher in comparison with other findings done in Bangladesh (10.5%) and Pakistan (9.7%).9,40 Multiple myeloma (MM) is a clonal plasma cell neoplastic disorder characterized by proliferation of neoplastic monoclonal plasma cells in the bone marrow that impede hematopoiesis, causes the activation of osteoclasts, suppression of osteoblasts, resulting in bone loss, and triggers production and release of monoclonal antibodies in serum and/or urine of the patient.10,41,42
In this study, the finding showed that 30.8% of cases of acute leukemia (AL) were found within the younger age range between 15 and 35 years, whereas 38.5% cases of chronic leukemia (CL) were found within the adult age range between 36 and 55 years. However, 7.7% of cases of multiple myeloma (MM) were found within the younger age range whereas 7.7% cases of MM were found within the adult age range. This result was in line with the findings reported in Eritrea and Morocco where the higher cases of AL were found in younger age, CL cases in the middle adult age and MM cases in the adult and older age group, in Bangladesh in which AML (28.3%) was dominant within a median age of 35 years and CML (18.2%) was found within the median age of 40 years.9,26,29
In this study, 76.9% of hematological malignant cases were found in male patients as compared to females (3.3:1 ratio). This was in concurrent findings reported in Bangladesh in which HM was dominant in male patients with a male to female ratio of 2.2:1, and leukemia was more prevalent in male patients and male to female ratio was 1.8:1, in India male preponderance with a male to female ratio of 2.3:1, in Pakistan HM is more common in male with the ratio of 2.5:1.9,30,40,43 The possible justification might be that male individuals are comparatively more exposed to the occupational and environmental carcinogenic agents which are at higher risk to the incidence of all kinds of leukemia.44
In the current study, the myeloid type of HM was dominant and accounted for 53.8% of cases and CML accounted for 30.8% of the cases whereas AML accounted for 23% out of the confirmed cases. This was in line with the findings done in Togo and Bangladesh.9,31 Interestingly, AML is fast-growing leukemia characterized by clonal expansion of immature blast cells in the peripheral blood and bone marrow resulting in ineffective erythropoiesis and bone marrow failure. Furthermore, CML is a slow-growing clonal myeloproliferative disorder characterized by the presence of all stages of myeloid development in the peripheral blood believed to be driven by the aberrant protein tyrosine kinase.45–47
Moreover, the lymphoid type of HM was accounted for 38.5% of cases in which CLL accounted for 15.4% followed by MM (15.4%), and ALL accounted for 7.7% out of the confirmed cases. This was in line with the findings done in Bangladesh and Nigeria.9,48 Moreover, ALL is a malignant transformation and proliferation of lymphoid progenitor cells characterized by uncontrolled proliferation of abnormal, immature lymphocytes and their progenitors of B and T-lymphocytes. Besides, CLL is an indolent lymphoproliferative disorder manifested by the progressive accumulation of mainly B-lymphocyte in the blood, bone marrow, and lymphatic tissues.38,49,50
In this study, 57.0% study participants had non-malignant hematological disorders. Regarding non-malignant hematological disorders, 56 (24.6%) cases were erythroid hyperplasia, 24 (10.5%) cases aplastic anemia, 20 (8.8%) cases concomitant IDA and MBA, 16 (7.0%) cases MBA, 8 (3.5%) cases leukemoid reaction, 4 (1.8%) cases IDA, and 2 (0.9%) cases visceral leishmaniasis. Concomitant IDA and MBA were dominant and accounted for 8.8% of cases, whereas MBA was dominant and accounted for 5.3% of cases in female patients. The study conducted in Bangladesh showed that 40.8% cases were non-malignant conditions and the common non-malignant hematological conditions diagnosed in the area were aplastic anemia (15.1%).24
In studies done in Pakistan (10.9%) and India (30%) of the patients had MBA which was higher than the current finding.2,51 The different blood cells isolated from patients with MBA are large oval erythrocytes, hyper segmented neutrophils, and abnormal giant platelets.52 The causes for MBA might be associated with the deficiencies of vitamin B12, folic acid, nutritional inadequacy, malabsorption, increased demands or utilization of the vitamins, chronic diarrhea, and worm infection.53,54 Furthermore, in the studies done in Pakistan, 5.9% and 9.4% of the patients had erythroid hyperplasia.24,55 The reason for erythroid hyperplasia may be due to a response to peripheral red blood cell loss or destruction and/or ineffective erythropoiesis associated with hemorrhage, hemolytic anemia, anemia of chronic disease, intrinsic bone marrow disease including aplastic anemia and malignant neoplasms.55–57 Moreover, in studies done in Pakistan and India 5.3% and 6.2% of the patients had aplastic anemia, respectively.2,58 In studies done in Pakistan, 3.3% and 5.7% and in India 3.2% of the patients had IDA whereas 2.7% and 7.9% had mixed IDA and MBA.2,55,59
In this study, the finding showed that leucocytosis, anemia, and thrombocytopenia were common in confirmed HM patients. Among patients with HM, 66.7% of AML, 100% of CML and CLL, 75% MM patients had high total WBC count (leucocytosis) whereas 66.7% of AML, 62.5% of CML, 75% of CLL, and 50% of MM patients had low hemoglobin level (anemia). In addition, 66.7% of AML, and 50% of CML, ALL, and CLL patients had low platelet count (thrombocytopenia). This was in line with the findings reported in Kenya in which patients with CML had low platelet count and higher bleeding tendency.60 On the other hand, a study done in Brazil showed that a high proportion of patients with AML had a high total WBC count and low platelet count61 and in Sudan high absolute lymphocyte count and thrombocytopenia (39.1%) were reported in CLL patients.62 Furthermore, in Pakistan, 80.1% and 96.3 % of AML patients had leucocytosis and thrombocytopenia.63 Another study done in Pakistan showed that total WBC count was high in 52%, 66.6%, 87.5%, and 66.6% of ALL, AML, CML, and CLL cases, respectively, and low hemoglobin level was reported in 82%, 97.4%, 87.5%, and 100% of ALL, AML, CML and CLL cases whereas low platelet count was found in 88%, 92.3%, and 58% ALL, AML and CLL cases, respectively.64
Conclusion
The overall prevalence of hematological malignancies in the study was 11.4% and 8.8% of cases were diagnosed in male patients. Generally, the prevalence of hematological malignancies diagnosed were 3.5% of CML, 2.6% of AML, 1.8% of CLL and MM, and 0.9% of ALL and undifferentiated acute leukemia. On the other hand, 57.0% of study participants had non-malignant hematological disorders which includes 56 (24.6%) cases were erythroid hyperplasia, 24 (10.5%) cases aplastic anemia, 20 (8.8%) cases concomitant IDA and MBA, 16 (7.0%) cases MBA, 8 (3.5%) cases leukemoid reaction, 4(1.8%) cases IDA, and 2 (0.9%) cases visceral leishmaniasis. Concomitant IDA and MBA were dominant and accounted for 8.8% of cases followed by MBA accounted for 5.3% of cases in female patients. Therefore, in patients with hematological abnormalities and where conclusive diagnosis could not be made through clinical and other laboratory investigations, bone marrow examination should be done for definitive diagnosis, management and prognosis.
Abbreviations
AL, acute leukemia; ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; BME, bone marrow examination; CBC, complete blood count; CL, chronic leukemia; CLL, chronic lymphocytic leukemia; CML, chronic myeloid leukemia; FAB, French American British; FNAC, fine-needle aspiration cytology; IDA, iron deficiency anemia; HM, hematological malignancies; MBA, megaloblastic anemia; MDS, myelodysplastic syndrome; MM, multiple myeloma; MPN, myeloproliferative neoplasms; PBM, peripheral blood morphology; RBC, red blood cell; SD, standard deviation; SOP, standard operating procedures; WBC, white blood cells; WHO, World Health Organization.
Data Sharing Statement
The authors confirmed that all the data for this manuscript are available; if someone wants to request the data they can contact the corresponding author.
Ethics and Consent Statement
The study was approved by Research and Ethics Review Committee of the College of Medicine and Health Sciences, Wollo University. A support letter was secured from Dessie zonal health office and a permission letter was obtained from the chief executive officer of the diagnostic medical laboratory. Moreover, written informed consent was taken from each study participant before conducting the investigation. This study was conducted in accordance with the declaration of Helsinki.
Acknowledgments
We would like to thank the study participants and data collectors who participated in this study. Furthermore, we would also give our heartfelt thanks to all who support and stood by our side during the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study did not receive any official funding.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Joshi S, Wader J, Kanethkar S. Bone marrow aspiration and bone marrow biopsy in hematological disorders. Biomed Pharmacol J. 2020;13(02):799–804. doi:10.13005/bpj/1944
2. Khan MI, Yasmeen N, Fatima SH. The spectrum of malignant and non-malignant hematological disorders in a tertiary care centre. Int J Res Med Sci. 2018;6(7):2361–2364. doi:10.18203/2320-6012.ijrms20182817
3. Rodriguez-Abreu D, Bordoni A, Zucca E. Epidemiology of hematological malignancies. Ann Oncol. 2007;18(supl1):i3–i8. doi:10.1093/annonc/mdl443
4. Swerdlow SH, Campo E, Pileri SA, et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood. 2016;127(20):2375–2390. doi:10.1182/blood-2016-01-643569
5. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20):2391–2405. doi:10.1182/blood-2016-03-643544
6. Harris NL, Jaffe ES, Diebold J, et al. The World Health Organization classification of hematological malignancies report of the Clinical Advisory Committee Meeting, Airlie House, Virginia, November 1997. Mod Pathol. 2000;13(2):193–207. doi:10.1038/modpathol.3880035
7. Davis AS, Viera AJ, Mead MD. Leukemia: an overview for primary care. Am Fam Physician. 2014;89(9):8.
8. Taylor J, Xiao W, Abdel-Wahab O. Diagnosis and classification of hematologic malignancies on the basis of genetics. Blood. 2017;130(4):410–423. doi:10.1182/blood-2017-02-734541
9. Hossain MS, Iqbal MS, Khan MA, et al. Diagnosed hematological malignancies in Bangladesh - a retrospective analysis of over 5000 cases from 10 specialized hospitals. BMC Cancer. 2014;14(1):438. doi:10.1186/1471-2407-14-438
10. Huang S-Y, Yao M, Tang J-L, et al. Epidemiology of multiple myeloma in Taiwan: increasing incidence for the past 25 years and higher prevalence of extramedullary myeloma in patients younger than 55 years. Cancer. 2007;110(4):896–905. doi:10.1002/cncr.22850
11. Bennett JM, Catovsky D, Daniel M-T, et al. Proposals for the classification of the acute leukaemias French-American-British (FAB) co-operative group. Br J Haematol. 1976;33(4):451–458. doi:10.1111/j.1365-2141.1976.tb03563.x
12. Abdul-Hamid G. Classification of Acute Leukemia. Acute Leukemia-The Scientist’s Perspective and Challenge. InTech; 2011; doi:10.5772/19848
13. Segeren C, Vantveer M. The FAB classification for acute myeloid leukaemia? Is it outdated? Neth J Med. 1996;49(3):126–131. doi:10.1016/0300-2977(96)00024-1
14. Onciu M. Acute Lymphoblastic Leukemia. Hematol Oncol Clin North Am. 2009;23(4):655–674. doi:10.1016/j.hoc.2009.04.009
15. Shet A, Jahagirdar B, Verfaillie C. Chronic myelogenous leukemia: mechanisms underlying disease progression. Leukemia. 2002;16(8):1402–1411. doi:10.1038/sj.leu.2402577
16. Oertel J, Kastner M, Bai AR, Kleiner S, Huhn D. Analysis of chronic lymphoid leukaemias according to FAB. Leuk Res. 1992;16(9):919–927. doi:10.1016/0145-2126(92)90037-8
17. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
18. Lin X, Wang J, Huang X, et al. Global, regional, and national burdens of leukemia from 1990 to 2017: a systematic analysis of the global burden of disease 2017 study. Aging. 2021;13(7):10468–10489. doi:10.18632/aging.202809
19. Bochtler T, Haag G-M, Schott S, Kloor M, Krämer A, Müller-Tidow C. Hematological malignancies in adults with a family predisposition. Dtsch Aerzteblatt. 2018;115:848–854. doi:10.3238/arztebl.2018.0848
20. Boström EA, Lira-Junior R. Non-malignant blood disorders and their impact on oral health: an overview. Curr Oral Health Rep. 2019;6(2):161–168. doi:10.1007/s40496-019-0211-9
21. Shallis RM, Ahmad R, Zeidan AM. Aplastic anemia: etiology, molecular pathogenesis, and emerging concepts. Eur J Haematol. 2018;101(6):711–720. doi:10.1111/ejh.13153
22. Rai RK, Fawzi WW, Barik A, Chowdhury A. The burden of iron-deficiency anaemia among women in India: how have iron and folic acid interventions fared? WHO South East Asia J Public Health. 2018;7(1):18–23. doi:10.4103/2224-3151.228423
23. McLean E, Cogswell M, Egli I, Wojdyla D, de Benoist B. Worldwide prevalence of anaemia, WHO vitamin and mineral nutrition information system, 1993–2005. Public Health Nutr. 2009;12(04):444–454. doi:10.1017/S1368980008002401
24. Chowdhury MRK, Rashid MHU, Begum A. Diagnostic role of bone marrow examination in detecting haematological and nonhaematological disorders. Med Today. 2019;31(1):15–18. doi:10.3329/medtoday.v31i1.40315
25. Ozkalemkas F, Ali R, Ozkocaman V, et al. The bone marrow aspirate and biopsy in the diagnosis of unsuspected nonhematologic malignancy: a clinical study of 19 cases. BMC Cancer. 2005;5(1):144. doi:10.1186/1471-2407-5-144
26. Elidrissi Errahhali M, Elidrissi Errahhali M, Boulouiz R, Ouarzane M, Bellaoui M. Distribution and features of hematological malignancies in Eastern Morocco: a retrospective multicenter study over 5 years. BMC Cancer. 2016;16(1):159. doi:10.1186/s12885-016-2205-5
27. Orazi A. Histopathology in the diagnosis and classification of acute myeloid leukemia, myelodysplastic syndromes, and myelodysplastic/myeloproliferative diseases. Pathobiology. 2007;74(2):97–114. doi:10.1159/000101709
28. Kassahun W, Tesfaye G, Bimerew LG, Fufa D, Adissu W, Yemane T. Prevalence of leukemia and associated factors among patients with abnormal hematological parameters in Jimma Medical Center, Southwest Ethiopia: a cross-sectional study. Adv Hematol. 2020;2020:1–7. doi:10.1155/2020/2014152
29. Belai N, Ghebrenegus AS, Alamin AA, Embaye G, Andegiorgish AK. Patterns of bone marrow aspiration confirmed hematological malignancies in Eritrean National Health Laboratory. BMC Hematol. 2019;19(1):8. doi:10.1186/s12878-019-0138-3
30. Kusum A, Negi G, Gaur DS, et al. Hematological malignancies diagnosed by bone marrow examination in a tertiary hospital at Uttarakhand, India. Indian J Hematol Blood Transfus. 2008;24(1):7–11. doi:10.1007/s12288-008-0016-9
31. Messanh Kueviakoe I. Hematological malignancies: analysis of myelogram results over 21 years in lome teaching hospitals. Clin Med Res. 2015;4(4):111–115. doi:10.11648/j.cmr.20150404.14
32. Baviskar JB. Incidence of acute and chronic leukemias in the rural area at a tertiary care teaching hospital: five years of study. Indian J Pathol Oncol. 2016;3(4):710–713. doi:10.5958/2394-6792.2016.00132.0
33. Elasbali AM, Alharbi HH, Onzi ZA, et al. Epidemiology and patterns of leukemia in Northern Saudi Arabia. Int J Med Res Health Sci. 2019;8(1):160–166.
34. Kibria S, Islam M, Chowdhury A, et al. Prevalence of hematological disorder: a bone marrow study of 177 cases in a private hospital at Faridpur. Faridpur Med Coll J. 1970;5(1):11–13. doi:10.3329/fmcj.v5i1.6806
35. Silva-Junior AL, Alves FS, Kerr MWA, et al. Acute lymphoid and myeloid leukemia in a Brazilian Amazon population: epidemiology and predictors of comorbidity and deaths. PLoS One. 2019;14(8):e0221518. doi:10.1371/journal.pone.0221518
36. Deschler B, Lübbert M. Acute myeloid leukemia: epidemiology and etiology. Cancer. 2006;107(9):2099–2107. doi:10.1002/cncr.22233
37. Tebbi CK. Etiology of acute leukemia: a review. Cancers. 2021;13(9):2256. doi:10.3390/cancers13092256
38. Delgado J, Nadeu F, Colomer D, Campo E. Chronic lymphocytic leukemia: from molecular pathogenesis to novel therapeutic strategies. Haematologica. 2020;105(9):2205–2217. doi:10.3324/haematol.2019.236000
39. Tejaswi V, Lad DP, Jindal N, et al. Chronic lymphocytic leukemia: real-world data from India. JCO Glob Oncol. 2020;(6):866–872. doi:10.1200/GO.20.00032
40. Khan S, Mir A, Khattak BR, et al. Pattern of adulthood hematological malignancies in Khyber Pakhtunkhwa. J Blood Disord Transfus. 2019;10(2):5. doi:10.4172/2155-9864.1000424
41. Silbermann R, Roodman GD. Myeloma bone disease: pathophysiology and management. J Bone Oncol. 2013;2(2):59–69. doi:10.1016/j.jbo.2013.04.001
42. Terpos E, Ntanasis-Stathopoulos I, Gavriatopoulou M, Dimopoulos MA. Pathogenesis of bone disease in multiple myeloma: from bench to bedside. Blood Cancer J. 2018;8(1):7. doi:10.1038/s41408-017-0037-4
43. Ahmad S, Shah KA, Hussain H, et al. Prevalence of acute and chronic forms of leukemia in various regions of Khyber Pakhtunkhwa, Pakistan: needs much more to be done! Bangla J Med Sci. 2019;18(2):222–227. doi:10.3329/bjms.v18i2.40689
44. Bhutani M, Vora A, Kumar L, Kochupillai V. Lympho-hemopoietic malignancies in India. Med Oncol. 2002;19(3):141–152. doi:10.1385/MO:19:3:141
45. Bennett JM, Catovsky D, Daniel MT, et al. The chronic myeloid leukaemias: guidelines for distinguishing chronic granulocytic, atypical chronic myeloid, and chronic myelomonocytic leukaemia: proposals by the French - American - British Cooperative Leukaemia Group. Br J Haematol. 1994;87(4):746–754. doi:10.1111/j.1365-2141.1994.tb06734.x
46. Deschler B, Lübbert M. Acute myeloid leukemia: epidemiology and etiology. Cancer. 2006;107:1–7. doi:10.1002/cncr.22233
47. Vincelli ID, Cufari P, Toscano C, et al. A patient with chronic lymphocytic leukemia, chronic myeloid leukemia and multiple myeloma. Blood. 2020;136(Supplement 1):37. doi:10.1182/blood-2020-141974
48. Onoja A, Otene S, Onoja A, et al. Prevalence and nature of adult hematological malignancies using bone marrow aspiration cytology in a tertiary health facility: a seven year retrospective review. West J Med Biomed Sci. 2021;2(1):39–45. doi:10.46912/wjmbs.39
49. Terwilliger T, Abdul-Hay M. Acute lymphoblastic leukemia: a comprehensive review and 2017 update. Blood Cancer J. 2017;7(6):e577–e577. doi:10.1038/bcj.2017.53
50. Suttorp M, Millot F, Sembill S, Deutsch H, Metzler M. Definition, epidemiology, pathophysiology, and essential criteria for diagnosis of pediatric chronic myeloid leukemia. Cancers. 2021;13(4):798. doi:10.3390/cancers13040798
51. Suresh T, Anjanappa R, Harendra kumar M, Thiyagarajan P. Bone-marrow spectrum in a tertiary care hospital: clinical indications, peripheral smear correlation and diagnostic value. Med JDY Patil Univ. 2015;8(4):490–494. doi:10.4103/0975-2870.160793
52. Riaz H, Shah MA, Ullah I. Frequency of megaloblastic anemia among patients with various hematological disorders after bone marrow examination in peshawar (a tertiary-care hospital study). KJMS. 2018;11(2):318–321.
53. Aslinia F, Mazza JJ, Yale SH. Megaloblastic anemia and other causes of macrocytosis. Clin Med Res. 2006;4(3):236–241. doi:10.3121/cmr.4.3.236
54. Hariz A, Bhattacharya PT. Megaloblastic anemia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2021.
55. Khan SP, Geelani S, Akhter S, et al. Bone marrow aspiration in haematological disorders: study at a tertiary care centre. Int J Res Med Sci. 2018;6(7):2361–2364.
56. Jha A, Adhikari R, Sarda R. Bone marrow evaluation in patients with fever of unknown origin. J Pathol Nepal. 1970;2(3):231–240. doi:10.3126/jpn.v2i3.6029
57. Orazi A, O’Malley DP, Arber DA. Illustrated pathology of the bone marrow. Cambridge: Cambridge University Press; 2006. Available from: http://ebooks.cambridge.org/ref/id/CBO9780511543531.
58. Gohil M, Rathod K. Bone marrow aspiration cytology study in a Tertiary Care Center, Gujarat, India. Int J Sci Stud. 2018;5(10):11–14.
59. Munir AH, Qayyum S, Gul A, Ashraf Z. Bone marrow aspiration findings in a tertiary care hospital of peshawar. J Postgrad Med Inst. 2015;29(4):297–300.
60. Othieno-Abinya NA, Mwanda WO, Maina MD, Odhiambo AO, Mwanzi SA, Oyiro PO. Haematological parameters in chronic myeloid leukaemia as determinants of clinical manifestations in this disease. J Clin Oncol. 2016;34(15–suppl):e18529–e18529. doi:10.1200/JCO.2016.34.15_suppl.e18529
61. Silva ASJ, Júnior LS, de Oliveira GHM, et al. Evaluation of clinical, hematological and flow cytometry dates in elderly patients with acute myeloid leukemia: impact on clinical outcome. Blood. 2019;134(Supplement–1):5115. doi:10.1182/blood-2019-127319
62. Basabaeen AA, Abdelgader EA, Babekir EA, et al. Clinical presentation and hematological profile among young and old chronic lymphocytic leukemia patients in Sudan. BMC Res Notes. 2019;12(1):202. doi:10.1186/s13104-019-4239-7
63. Chang F, Shamsi TS, Waryah AM. Clinical and hematological profile of acute myeloid leukemia (AML) patients of Sindh. J Hematol Thromboembolic Dis. 2016;04(02). Available from:: http://www.esciencecentral.org/journals/clinical-and-hematological-profile-of-acute-myeloidleukemia-aml-patientsof-sindh-2329-8790-1000239.php?aid=71146.
64. Munir AH, Khan MI. Pattern of basic hematological parameters in acute and chronic leukemias. J Med Sci. 2019;27(2):125–129.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.