Back to Journals » Clinical Optometry » Volume 18
Patterns and Predictors of Upper Limb and Neck Work-Related Musculoskeletal Disorders Among Practicing Optometrists in Jordan: A Cross-Sectional Survey
Authors Haddad MF, Almhdawi K, Zraigat LA
Received 3 January 2026
Accepted for publication 2 April 2026
Published 21 April 2026 Volume 2026:18 593432
DOI https://doi.org/10.2147/OPTO.S593432
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Chris Lievens
Mera F Haddad,1 Khader Almhdawi,2,3 Lama A Zraigat2
1Department of Allied Medical Sciences, Jordan University of Science and Technology, Irbid, Jordan; 2Department of Rehabilitation Sciences, Jordan University of Science and Technology, Irbid, Jordan; 3Occupational Therapy Department, Faculty of Allied Health Sciences, Kuwait University, Kuwait City, Kuwait
Correspondence: Mera F Haddad, Department of Allied Medical Sciences Jordan University of science and technology, POBox 3030, Irbid, 22110, Jordan, Tel +00962 (2)7201000, Email [email protected]
Purpose: To investigate the prevalence and predictors of upper quadrant work-related musculoskeletal disorders (WMSDs) among practicing optometrists in Jordan and to highlight potential occupational health implications.
Patients and Methods: A cross-sectional survey was distributed to registered optometrists working in public and private health sectors in Jordan. A total of 138 optometrists (n=138) participated in the study. Standardized instruments were used, including the Nordic Musculoskeletal Questionnaire (NMQ), the Depression Anxiety Stress Scale (DASS), the Pittsburgh Sleep Quality Index (PSQI), and the International Physical Activity Questionnaire (IPAQ). Sociodemographic characteristics, work practices, and ergonomic factors were also collected. Descriptive statistics were used to determine the prevalence of musculoskeletal complaints, while logistic regression analysis identified predictors of WMSDs across upper quadrant body regions.
Results: The 12-month prevalence of musculoskeletal pain was highest in the shoulders (73.9%), neck (70.3%), and upper back (62.3%), followed by wrists and hands (24.6%), while elbows had the lowest prevalence (15.2%). Several factors were significantly associated with increased WMSDs (p < 0.05). Notably, marital status showed a strong association with neck pain (OR ≈ 7.1), while other predictors included writing and typing during work, poor ergonomics during vision testing, cigarette smoking, poor sleep quality, and psychological stress.
Conclusion: Upper quadrant WMSDs are highly prevalent among practicing optometrists in Jordan and may negatively affect occupational well-being and work performance. These findings highlight the need for targeted ergonomic interventions, improved clinical workstation design, and occupational health programs to reduce musculoskeletal strain and support healthier workplace practices among eye care professionals.
Keywords: work-related musculoskeletal disorders, optometrists, ergonomics, occupational health, Jordan
Introduction
Work-related musculoskeletal disorders (WMSDs) are common and might impact a large number of people around the world.1 WMSDs are among the most common occupational health problems worldwide and represent a major cause of disability, reduced productivity, and decreased quality of life among healthcare professionals.2
The term WMSDs has gained increasing attention in recent decades due to their significant impact on both individuals and society. These disorders can lead to physical and functional limitations as well as adverse psychosocial and economic consequences.3 In some occupations, persistent pain and neck injuries may even force individuals to stop working prematurely, leading to early retirement.4 Moreover, WMSDs can negatively affect professional performance by reducing productivity, increasing absenteeism, and potentially compromising the quality of patient care, as ongoing musculoskeletal pain may impair concentration and clinical efficiency.5
Healthcare professionals are considered among those at highest risk of developing WMSDs.6,7 Hanson et al8 noted that healthcare workers, particularly those with direct patient contact, face an elevated risk, likely due to high job demands and sustained awkward postures throughout their workdays. Similarly, Anderson and Oakman9 reported that allied health professionals are exposed to considerable physical and psychosocial stressors that contribute to this increased risk.
Several studies identified both physical and psychosocial risk factors for WMSDs among the medical population. Physical factors included strenuous work conditions such as lifting or carrying heavy loads, maintaining tiring or awkward postures, and performing repetitive movements.10 Psychosocial factors included time pressure, low job control, limited social or supervisory support, effort–reward imbalance, and work–life conflict.11 In addition, studies stated that mental health and vitality can predict back pain in healthcare workers. Those reporting low to moderate mental health and vitality were experiencing greater spinal pain intensity than those with better mental health and higher vitality.12
The term WMSDs has recently been raised among ophthalmologists and optometrists. Optometrists may be particularly vulnerable to WMSDs due to the nature of their clinical work. Routine procedures such as refraction, retinoscopy, slit-lamp examination, and prolonged computer-based documentation often require sustained static postures, repetitive upper limb movements, and prolonged near visual tasks. These occupational demands frequently involve forward head posture, neck flexion, and awkward shoulder positioning, which may increase mechanical strain on the cervical spine and upper extremities. Over time, these biomechanical stresses can contribute to the development of musculoskeletal pain and discomfort among practicing optometrists13,14 and thus, significant financial and personal costs. Long et al15 reported that some optometrists either reduced their working hours or left the profession due to work related physical discomfort.
Common symptoms of WMSDs have been identified among eye care practitioners worldwide. These included Low back pain, followed by upper extremity symptoms and neck pain.16 Kitzmann et al14 found that eye care physicians (optometrists and ophthalmologists) had significantly higher prevalence of neck, hand/wrist, and lower back pain compared with family medicine physicians. The authors also reported that repetitive tasks, prolonged or awkward/cramped positions, and bending/twisting were the most contributory factors associated with participants’ WMSDs symptoms. Similarly, Long et al15 reported that female and younger optometrists, as well as those performing a high number of daily consultations, were at greater risk of physical discomfort. Continuing to work while injured and performing repetitive tasks further increased the severity of discomfort.
Previous international studies have reported a high prevalence of musculoskeletal symptoms among optometrists and other eye-care professionals, particularly affecting the neck, shoulders, and upper back, largely attributed to prolonged near work and non-neutral working postures.5,14,16 In Saudi Arabia neck and back pain were reported by 70% of eye care professionals and the pain was believed to be work related in 50% of the cases.17 Venkatesh et al18 reported similar findings among ophthalmologists in India where back pain was linked with awkward posture and prolonged working hours. Comparable high WMSDs prevalence was also reported among ophthalmologists in Germany and the United Kingdom.19,20
Jordanian optometrists are no different than optometrists worldwide. According to the national professional records reported by the Jordanian syndicate of optometrists, licensed optometrists currently practice in Jordan play a vital role in providing primary eye care services. These optometrists work in diverse setting such as hospitals, clinics and retail optical shops, where clinical and administrative tasks often involve prolonged periods of visually demanding work and repetitive procedures. Despite these occupational demands associated with optometric practice, there is a lack of evidence regarding ergonomics awareness or occupational health policies targeting musculoskeletal risk among optometrists in Jordan. This lack of preventive guidelines may contribute to occupational problems among practitioners.
Given the limited regional evidence, this study aimed to investigate the prevalence of WMSDs of upper quadrant (Neck, shoulders, upper limbs and upper back) and their associated factors among practicing optometrists in Jordan across different practice settings. Findings from this research may contribute to raising awareness, guiding ergonomic interventions, and supporting workplace health policies within the optometric profession in Jordan.
Materials and Methods
Study Design and Sample
A cross-sectional survey was utilized in this work. The study sample included qualified practicing optometrists registered with the Jordanian optometric association and the Jordanian Association of Optics. Optometrists in the north, middle and south of Jordan were enrolled in the study. The sample size was determined based on previously reported prevalence rates of WMSDs among healthcare professionals, along with feasibility considerations related to participant accessibility. Sample size determination was conducted utilizing G-power calculations (assuming 15 predictors and effect size of 0.15), a minimum sample of 123 participants were needed to guarantee a statistical power of 80%.21 Accounting for drop outs, a total of 160 optometrists were invited to participate based on accessibility and professional networks, of whom 138 completed the survey (response rate: 86.3%). Participants were recruited using a convenience sampling approach from optometrists working in public and private sectors across Jordan.
Data were collected using both paper-based and electronic questionnaires, depending on participant preference, with a trained research assistant who was ready to answer or clarify any information needed by the participants. No formal assessment of mode effects was conducted. Data were collected between January and August, 2025. Eligible participants were required to be licensed optometrists with at least one year of work experience. Optometrists who were on long-term analgesic medication, had psychiatric or congenital disorders, a history of spine surgery, or major chronic illnesses associated with musculoskeletal pain were excluded. Due to the cross-sectional design of the study, causal or temporal relationships between identified risk factors and WMSDs cannot be established.
Outcome Measures
Qualified optometrists were asked to complete a three-section questionnaire. The sociodemographic section required data about age, gender, marital status, province, health self-evaluation, diet self-evaluation, smoking, weight, height, work experience, working hours, place of work. The second section collected data on work ergonomics including body postures and discomfort while performing vision examination eg. visual acuity, retinoscopy and subjective tests. The third section included the following standardized outcome measures:
Nordic Musculoskeletal Questionnaire (NMQ)
This is a standardized questionnaire developed in the late 1980s and has been used extensively in clinical studies since then. This instrument evaluates the prevalence of musculoskeletal pain over the past 12 months and the previous 7 days, in addition to the functional limitations associated with these complaints. An example item from the NMQ is: “Have you at any time during the last 12 months had trouble (ache, pain, discomfort) in.?” The NMQ has been demonstrated to be a valid and reliable measure for assessing work-related musculoskeletal disorders (WMSDs) in the upper quadrant.22
Depression Anxiety Stress Scale (DASS21)
This is a well-established questionnaire used to assess core symptoms of depression, anxiety and stress. The scoring of the questionnaire is a four-point likert scale ranging from “0” did not apply to me at all to “4” applied to me very much or most of the time. The higher the DASS score, the more severe the symptoms of stress and depression.23
Pittsburgh Sleep Quality Index (PSQI)
This questionnaire was used to measure general sleep quality. The PSQI is a 19-item self-reported questionnaire used for assessing sleep quality over the previous month. The global score of PSQI ranges from 0 to 21 with a higher score indicating worse sleep quality.24
International Physical Activity Questionnaire–Short Form (IPAQ-SF)
This is the most widely used physical activity questionnaire with its two versions: long form (IPAQ-LF 31 items and the short form (IPAQ-SF) of 9 outcome measures. The IPAQ-SF was used in this study to reflect the physical activity levels of the participant.25
Work-related musculoskeletal disorders were assessed using the Standardized Nordic Musculoskeletal Questionnaire (NMQ), which evaluates the presence of musculoskeletal symptoms in specific body regions over the past 12 months to reflect recent but not longitudinal trends. Predictor variables included sociodemographic characteristics, work-related factors (eg., working hours, type of tasks, ergonomic practices), and psychosocial and lifestyle measures assessed using validated instruments including the DASS, PSQI, and IPAQ. Standardized validated instruments (NMQ, DASS, PSQI, IPAQ) were used in their original formats to ensure reliability and comparability with previous studies.
Statistical Analysis
Data were analyzed using SPSS (IBM SPSS version 27). Descriptive statistics were used to summarize participant characteristics and prevalence of WMSDs. Logistic regression analyses were performed to identify predictors of WMSDs. Variables with p < 0.05 in univariate analysis were included in multivariate models to control for potential confounders. For body regions with low prevalence, caution was taken in interpreting regression results due to potential limitations in the number of events per variable.
Ethics Approval
The ethics approval for conducting this work was granted by the Institutional Review Board (IRB) committee at Jordan University of Science and Technology (approval number 24/155/2023). An informed consent was obtained from all participants prior to their participation, and the study protocol complied with the guidelines of the Declaration of Helsinki. Data were collected anonymously, and confidentiality was strictly maintained.
Results
Participants’ Sociodemographic, Health, and Lifestyle Characteristics
The survey was successfully completed by 138 optometrists, resulting in a response rate of 86.3%. The mean age of participants was 31.59 (±8.254) years with female participants representing approximately 63% and the majority (73.9%) held a bachelor’s degrees. Table 1 shows participants sociodemographic, health and lifestyle characteristics, in addition to physical and mental status.
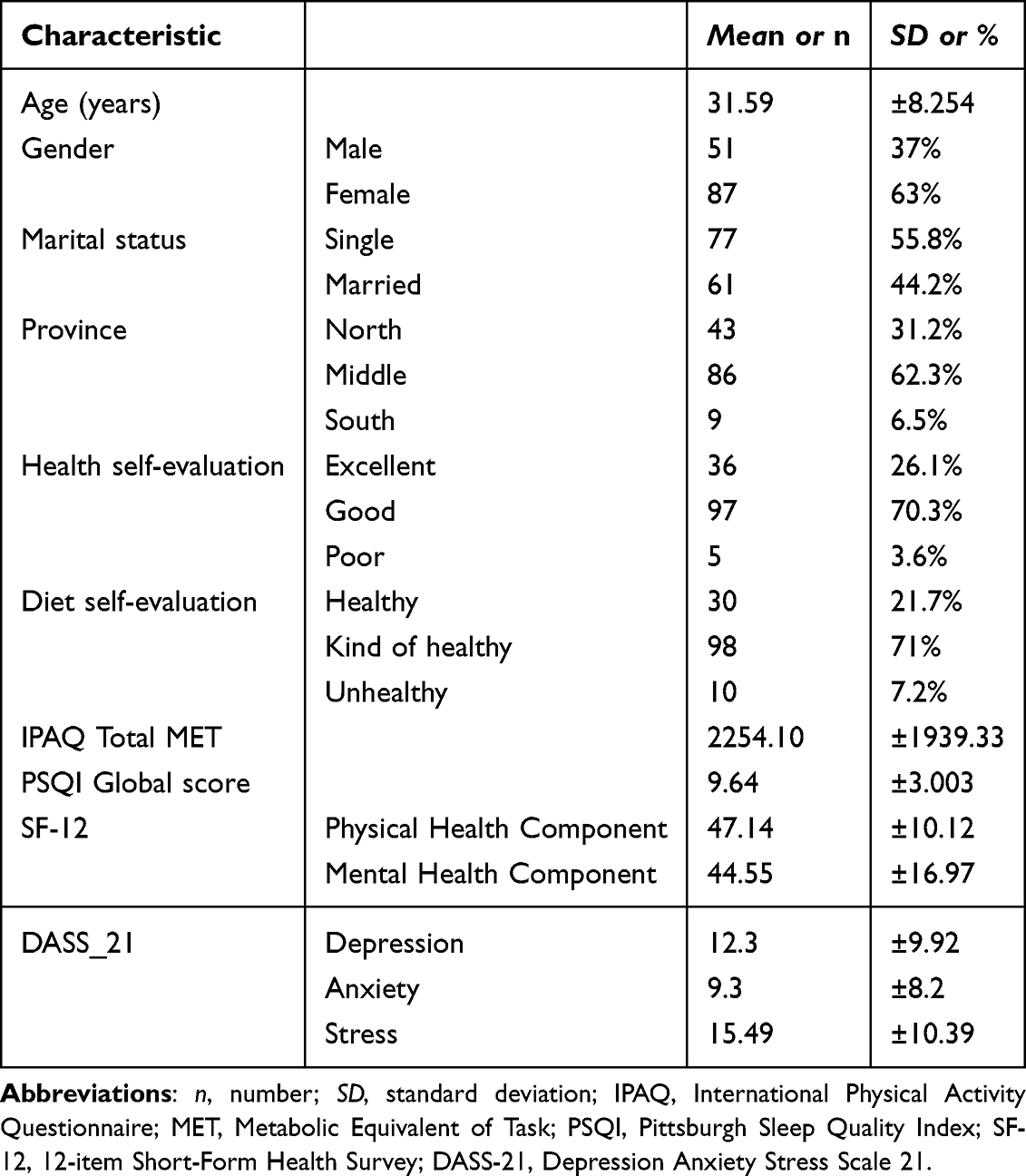 |
Table 1 Participants’ Socioeconomic and Health Characteristics |
Work-Related and Ergonomic Factors
Regarding work-related variables, the mean work experience reported by the participants was 8.86 (±7.64) years, with an average working hours of 44.07 (±16.078) per week. The majority of optometrists were working in the private sector followed by the Royal Medical Services and the public sector (the ministry of health). In term of work-related musculoskeletal injuries, 66 (47.8%) of optometrists reported having musculoskeletal pain in the past 12 months, with an average pain in the last week of 4.7 (±2.56), and 36 (26.1%) took sick leave due to musculoskeletal pain at least once. Tables 2 shows key information about work-related and ergonomic factors related to work injuries.
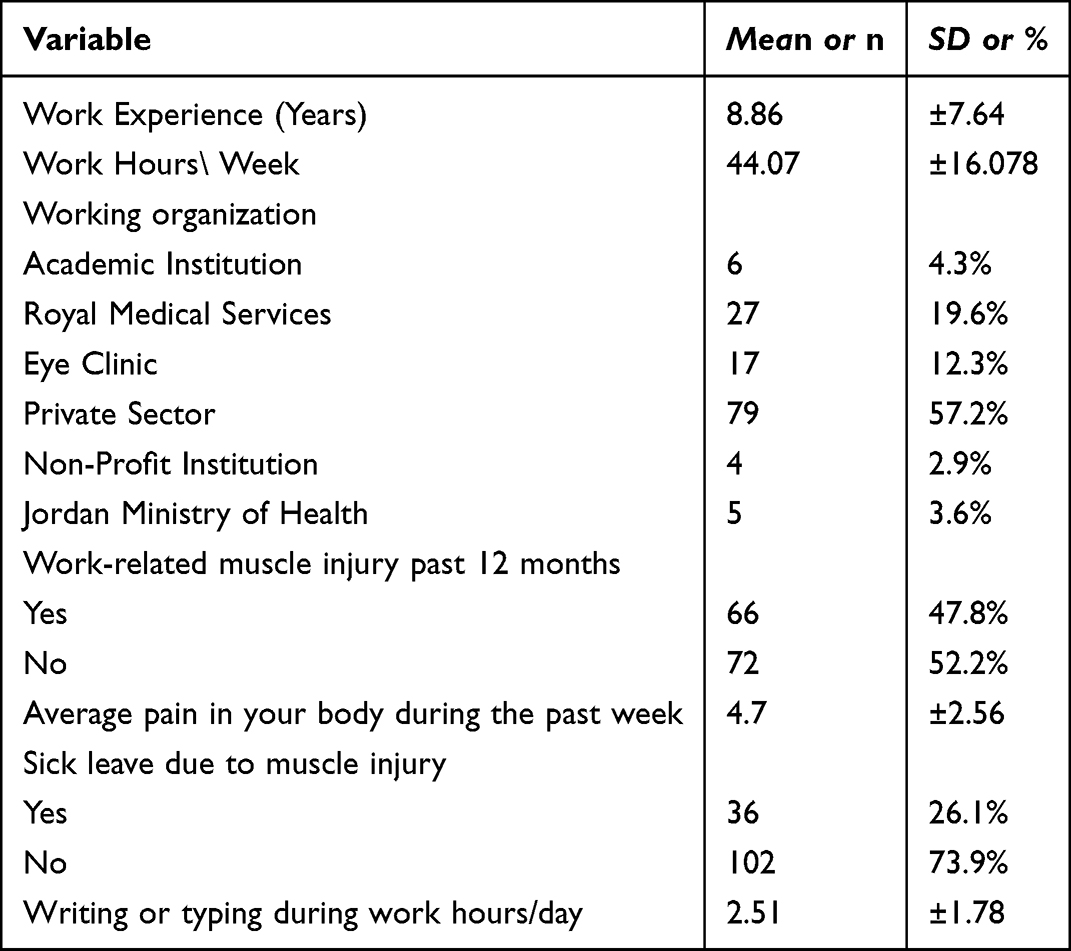 |
Table 2 Work-Related Injuries (N=number, SD=standard Deviation) |
Prevalence of Upper Quadrant 12-month WMSDs
Figure 1 represents the 12-month and 7-day prevalence of WMSDs, as well as the functional limitations associated with these disorders, as measured by NMQ. Results showed that the 12 months prevalence of Musculoskeletal pain in any body site was reported by 131 (94.4%) participants. Twelve-month pain prevalence was the highest for shoulders 102 (73.9%) and lowest for the elbows 21 (15.2%) as shown in Figure 1.
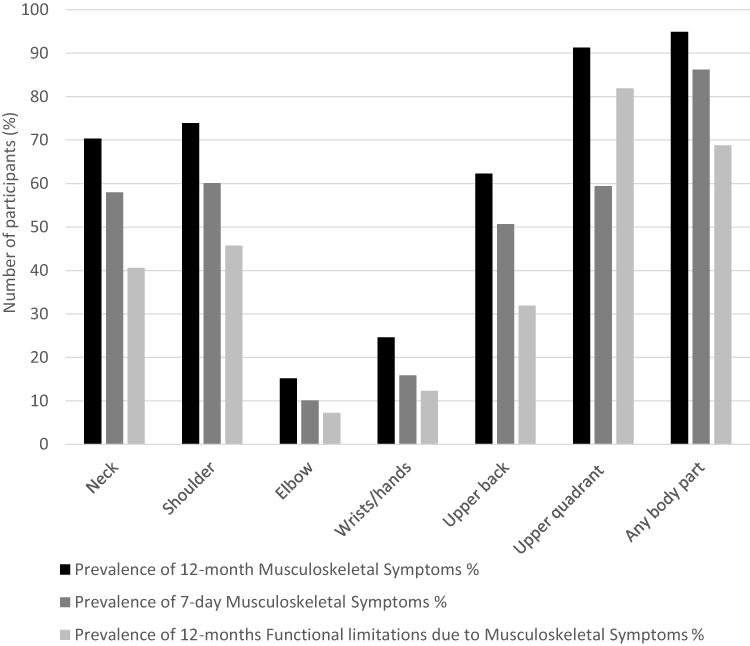 |
Figure 1 Musculoskeletal Symptoms Prevalence Across Body Sites. |
Associated Factors of the Upper Quadrant 12-month WMSDs
Predictors of Neck WMSDs
The multiple variable model successfully identified significant predictors of neck WMSDs (r2=0.317, Chi=52.637, p <0.001). The model demonstrated good fit as suggested by Hosmer–Lemeshow test, p = 0.930. Being married, writing and typing while working, discomfort while doing subjective test and average pain in body during the past week were found as significant associated factors for increased neck WMSDs. Whereas, decreased neck WMSDs was significantly associated with increased years of experience and work province in the middle and north of Jordan compared to working in the south. Details are shown in Table 3.
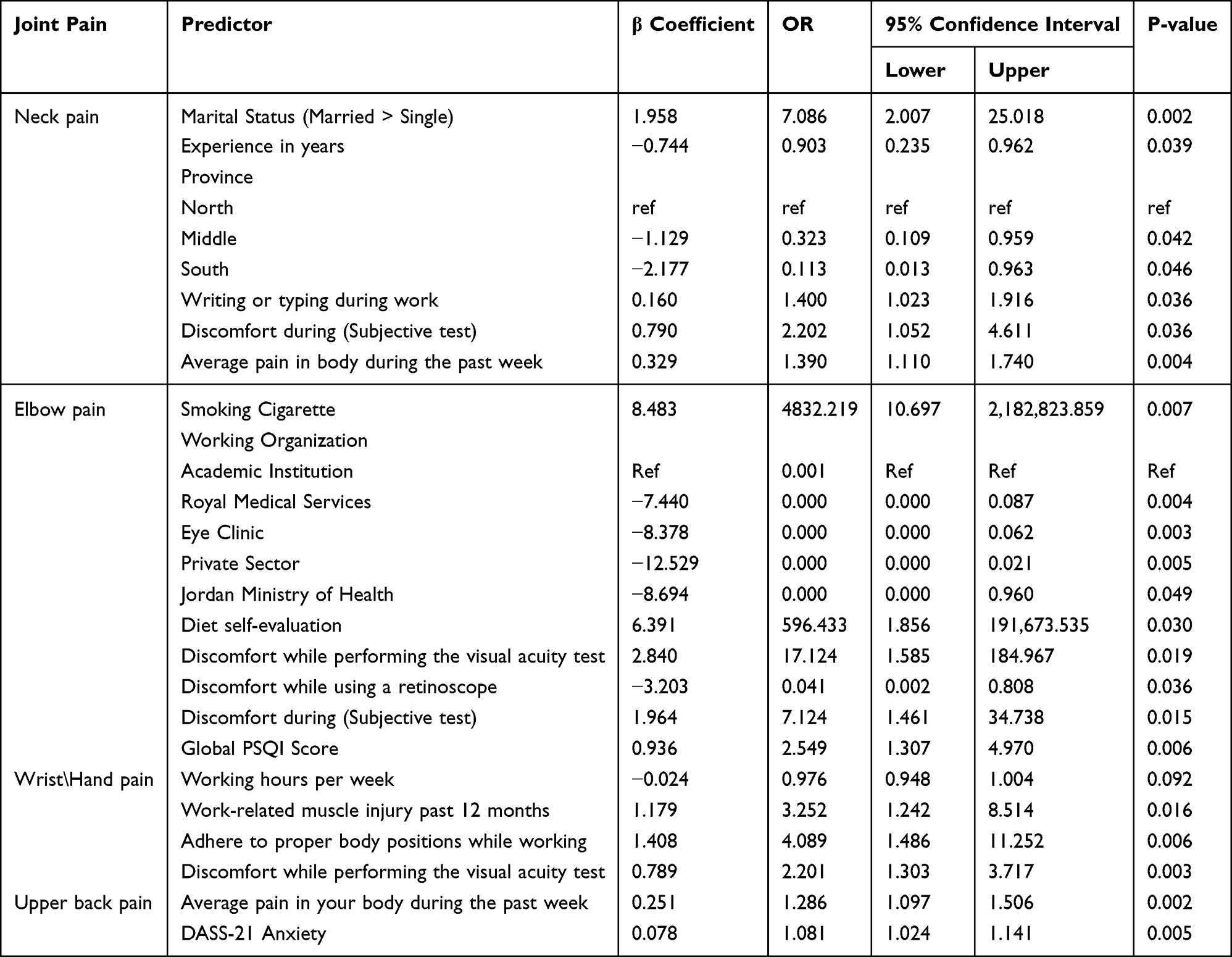 |
Table 3 Multiple Variable Analysis of Factors Associated with Upper Quadrant NQM Musculoskeletal Pain |
Predictors of Elbow WMSDs
The regression model successfully identified significant predictors of elbow WMSDs (r2=0.439, Chi=79.721, p <0.001). The model demonstrated good fit ass suggested by Hosmer–Lemeshow test, p = 0.881. Smoking cigarettes, discomfort while doing the visual acuity test, discomfort during Subjective test, diet self-evaluation, and PSQI global score were significantly associated with increased elbow WMSDs. Whereas, working in Royal Medical Services, eye Clinic, private Sector and hospitals of the ministry of health compared to working in an academic institution, alongside discomfort while using the retinoscope were all significantly associated with decreased elbow WMSDs (see Table 3).
Predictors of Wrist and Hands WMSDs
The multiple variable model also successfully identified significant predictors of wrist and hands WMSDs (r2=0.185, Chi=28.146, p <0.001). The model demonstrated good fit suggested by Hosmer–Lemeshow test, p = 0.885. Increased WMSDs in wrists and hands were significantly associated with work-related muscle injury in the past 12 months, adhering to proper body positions while working, and discomfort while performing the visual acuity test. On the other hand, decreased WMSDs in wrists and hands were associated with working hours per week (Table 3).
Predictors of Upper Back WMSDs
Significant predictors of upper back WMSDs (r2=0.157, Chi=23.526, p <0.001) were also found. The model demonstrated good fit supported by (Hosmer–Lemeshow test, p = 0.801. These include, average pain in the body during the past week and DASS-21 Anxiety were significantly associated with increased WMSDs in the upper back. WMSDs in the shoulders were not linked or associated with any of the variables investigated in this study.
Notably, certain predictors are closely linked to optometry-specific tasks, such as prolonged near work and sustained head and neck postures during refraction and slit-lamp examination, which may contribute to the high prevalence of neck and upper limb symptoms.
Discussion
This is the first study reporting Work-Related Musculoskeletal Disorders (WMSDs) among Jordanian and Middle Eastern optometrists, and one of the limited studies done uniquely among optometrists worldwide. This study provides novel data on the prevalence and predictors of WMSDs among optometrists in Jordan, addressing a significant gap in regional occupational health literature.
Prevalence of Upper Quadrant 12-month WMSDs
Jordanian optometrists reported a high prevalence (94.9%) of WMSDs at anybody site, as measured by NMQ. This very high prevalence might reflect on professionals’ productivity and their quality of life (QoL). The worldwide prevalence of WMSDs among optometrists is not well reported. Most of the studies in the literature explored the prevalence and the associated risk factors among eye care professionals collectively. A survey study done among Australian optometrists in 2012 reported WMSDs prevalence of up to 82%.15 On the other hand, a survey study done among Canadian eye care professionals in 2019 reported a WMSDs prevalence of 61% among the participating optometrists.26 Among Arab and Middle Eastern countries, a study done in Saudi Arabia in 2023 showed that about 66.7% of eye care professionals had WMSDs.27 However, none of these studies used the standardized NMQ to report WMSDs; most of them used an author-designed non-standardized questionnaire influenced by NMQ, but they did not cite or validate their data collection tools. This work has shown that the highest prevalence for the upper quadrant was for the shoulders (73.9%), neck (70.3%), and the upper back (62.3%). The lowest prevalence was for elbows (15.2%), and wrists/hands (24.6%). These results were consistent with the previously mentioned studies. WMSDs prevalence among Jordanian optometrists is comparable to global reports, yet remains among the highest worldwide. This may be attributed to poor ergonomic conditions, limited handling equipment, insufficient training in safe practices, high workloads, and inadequate awareness of proper body mechanics.
Associated Factor of the Upper Quadrant 12-month WMSDs
In this study, an extensive set of factors potentially associated with WMSDs were investigated, these might be divided into two parts:
Participants’ Sociodemographic, Health, and Lifestyle WMSDs Associated Factors
Being married arose as a significant positive factor for neck WMSDs. This suggests that being married increases the risk of neck WMSDs. This finding agrees with that reported by Zahrawi et al 2024, among Syrian healthcare professionals, which showed that being married was correlated with a higher prevalence of having WMSDs.28 Being married often involves taking on many physical responsibilities, such as household chores, and child care, on top of a professional workload. These activities frequently involve repetitive bending, prolonged standing, and inappropriate postures. The combination of work-related physical stress and household responsibilities might increase total musculoskeletal load, leading to musculoskeletal problems. Additionally, Marriage can introduce new psychosocial demands, such as managing family responsibilities, household budgeting.29,30 This may increase muscle tension, pain perception via central nervous system sensitization and reduce pain tolerance.
Smoking cigarettes appeared to be a significant positive associated factor with increased elbow WMSDs. Previous studies reported a higher prevalence of musculoskeletal pain and disorders among smokers in comparison with non-smoker individuals. In the upper extremities, smoking was linked with rotator cuff tendinopathy, carpal tunnel syndrome, and epicondylitis.31,32 These results support our study’s results. Nicotine causes vasoconstriction, decreasing blood flow to muscles, tendons, and joints. This might impair tissue healing in overused areas like the elbow. Additionally, smoking could interfere with collagen synthesis, weakening tendons and ligaments around the elbow. This makes conditions like lateral epicondylitis (tennis elbow) or medial epicondylitis (golfer’s elbow) more likely to occur.31,32 Moreover, cigarette smoking elevates systemic inflammation, which may worsen musculoskeletal pain. However, Smoking does not act alone; it may interact with physical workload.33 Repetitive motions, forceful gripping, and awkward elbow postures already predispose to elbow WRMSDs. Smoking reduces healing capacity, turning microtrauma into a chronic injury.
In addition to smoking, the PSQI global score (sleep quality) appeared in this study as a significant positive associated factor linked with increased elbow WMSDs. PSQI global score reports poor for scores greater than 5 and normal for scores 5 and less, indicating that poor sleep (higher scores) is associated with a higher level of elbow WMSDs. This finding aligns with previous report by Almhdawi et al34 among registered nurses in Jordan, demonstrating a positive association between poor sleep quality and WMSDs.
Anxiety appeared in this study as a significant positive associated factor for increased upper back WMSDs. Previous studies among healthcare professionals investigated and reported the relation between psychological factors, including anxiety, stress, and depression, and the WMSDs.34,35 It is speculated that chronic muscle tension can lead to muscle fatigue, converting microtrauma in the workplace into chronic muscle disease, and increasing pain sensitivity. Moreover, Anxiety is linked to increased hormonal secretion such as cortisol and catecholamines. These hormones may increase muscle inflammation and decrease the muscle’s recovery process.36
Work-Related and Ergonomic WMSDs Associated Factors
Although several predictors were identified, some associations should be interpreted with caution due to relatively wide confidence intervals, suggesting limited precision. These findings may therefore be considered indicative signals rather than definitive predictors and warrant further investigation in larger studies.
Years of work experience and working in the Middle and South of Jordan (compared to the North) in this study appeared as a significant negative associated factor for Neck WMSDs. This means optometrists with higher experience and who work in the Middle and South of Jordan experienced lower levels of neck WMSDs. This agrees with a study done among medical and health sciences workers which showed that increased years of experience were associated with decreased WMSDs in different body sites. This could be attributed to the use of better ergonomic practices or adopting less physically demanding work tasks among experienced.37 Working in Amman (Middle), the capital of Jordan, was associated with a lower prevalence of neck WMSDs. The higher quality of healthcare services and availability of modern, ergonomically designed equipment in Amman may facilitate better management and prevention of WMSDs among optometrists. In the south of Jordan, the lower population density could have reduced work demand, which may have contributed to a decreased prevalence of neck WMSDs.
Working in all types of working organization appeared significant negative WMSDs associated factors in comparison with working in academia, with increased the risk of elbow WMSDs. This suggest that all workers in various types of organizations, including those in Royal Medical Services, eye clinics, the private sector, non-profit institutions, and the Jordan Ministry of Health, were associated with a decreased risk of elbow WMSDs compared to working in an academic institution. When compared with academic institutions, other organizational types may present a lower risk of WMSDs. The increased risk of elbow WMSDs may be associated with academic tasks involving prolonged typing, repetitive mouse use, and handwriting, which place mechanical load on the forearm muscles. Non-neutral wrist–elbow postures, static loading during computer work, and frequent fine motor tasks have all been identified as key ergonomic mechanisms contributing to elbow musculoskeletal disorders. In contrast, clinical or organizational settings may involve less academic-related tasks and better ergonomic and therapeutic support. Zhou et al investigated the risk factors related to elbow musculoskeletal diseases. They reported that the prevalence of elbow WMSDs was high in industries with repetitive operations, forceful upper limb tasks, awkward posture, and vibrating tools (similar to those of optometrists).38
Interestingly, working hours per week emerged as a significant negative associated factor with wrist/hand WMSDs in this study. Previous studies suggested that increased working hours were associated with increased WMSDs.39 This lack of agreement with previous studies may be explained by the “healthy worker effect”. Workers with WMSDs may reduce their hours or leave physically demanding positions, leaving behind a more resilient and healthier workforce. Longer hours are also frequently associated with greater experience, probably improved ergonomics, and a higher likelihood of working for organizations that have better designed equipment. Despite longer workdays, these factors could have worked together to reduce the risk of WMSDs.
Performing subjective eye test, visual acuity testing, and retinoscopy in this study was associated with more upper quadrant WMSDs. These procedures require optometrists to maintain static, forward-leaning postures, prolonged visual focus, and repetitive fine motor movements, all of which might increase strain across the upper quadrant.27,40 Repetitive adjustments of trial frames and lenses during subjective testing, combined with sustained arm and hand positions during retinoscopy, can also contribute to cumulative stress in the elbows, hands, and wrists. Ergonomic assessments have highlighted high-risk postures in optometry, including prolonged shoulder elevation, unsupported arms, and non-adjustable equipment, which may exacerbate musculoskeletal load across the neck, shoulders, and upper back.40 These findings are consistent with previous reports indicating that sustained near work, repetitive fine motor tasks, and poor ergonomic design were significant contributors to upper quadrant WMSDs among eye-care professionals.27
Study Limitations
This study implemented a cross-sectional design, which decreases the ability to generalize and generate causality conclusions. Longitudinal studies in the future should be adopted to enhance the understanding of nature and progress of the WMSDs. Moreover, the relatively modest sample size and the use of a convenience sampling approach, may limit the generalizability of the results. Additionally, this study used few self-evaluation and non-standardized assessments. The reliance on self-reported measures for both exposures and outcomes may introduce common-method bias, whereby participants’ perception of pain could influence the reporting of ergonomic risk factors. So, using a more objective and standardized assessment could have given this study better investigation accuracy. Moreover, as the NMQ is regarded as a subjective assessment tool, variability in optometrists’ interpretations of pain and musculoskeletal disorders may introduce inconsistencies. Future research and clinical screening should incorporate objective assessments (eg. posture analysis, electromyography, or range-of-motion testing) to improve diagnostic accuracy and monitoring. In this study, shoulder WMSDs were not associated with any of the investigated factors, despite its high prevalence among our optometrist participants. This may indicate the presence of unmeasured ergonomic or task-specific factors that were not captured in the current study. Further studies should explore more and varied factors, and with a larger sample size. Collectively, Future studies are needed to evaluate the efficacy of various interventional techniques in reducing the level of WMSDs among optometrists in Jordan. Future research should also consider incorporating a broader range of psychosocial factors, such as job stress and job satisfaction, to provide a more comprehensive understanding of the determinants of WMSDs among optometrists.
Conclusion
Upper quadrant work-related musculoskeletal disorders (WMSDs) are highly prevalent among practicing optometrists in Jordan. Several factors were found to be significantly associated with these disorders; however, due to the cross-sectional design of the study, causal relationships cannot be established.
The findings of this work highlight the urgent need for ergonomic guidelines and workplace interventions tailored to optometry practice in Jordan. Practical measures such as optimizing workstation design, promoting proper posture during clinical procedures, and implementing structured ergonomic training programs are recommended. Furthermore, regulatory and professional bodies have an important role in developing and enforcing occupational health standards, raising awareness, and supporting preventive strategies aimed at reducing the burden of WMSDs. Such efforts may contribute to improving practitioner well-being, enhancing productivity, and ensuring high-quality patient care.
Acknowledgments
This study was approved and sponsored by the Deanship of Research at Jordan University of Science and Technology. The authors would like to thank all participants who participated in this study.
Disclosure
None of the authors has conflicts of interest in the present work.
References
1. Punnett L, Wegman DH. Work-related musculoskeletal disorders: the epidemiologic evidence and the debate. J Electromyogr Kinesiol. 2004;14(1):13–12. doi:10.1016/j.jelekin.2003.09.015
2. World Health Organization.Identification and control of work-related diseases.1985;(Technical Report Series
3. Lozano R, Gomez-Dantes H, Garrido-Latorre F, et al. Burden of disease, injuries, risk factors and challenges for the health system in Mexico. Salud Publica Mex. 2013;55(6):580–594. doi:10.21149/spm.v55i6.7304
4. Sivak-Callcott JA, Diaz SR, Ducatman AM, Rosen CL, Nimbarte AD, Sedgeman JA. A survey study of occupational pain and injury in ophthalmic plastic surgeons. Ophthalmic Plast Reconstr Surg. 2011;27(1):28–32. doi:10.1097/IOP.0b013e3181e99cc8
5. Kaur H, Xie JS, Lusterio A, et al. A scoping review of ergonomics in ophthalmology: working in pain. Am J Ophthalmol. 2026;282:433–457. doi:10.1016/j.ajo.2025.11.005
6. Bernal D, Campos-Serna J, Tobias A, Vargas-Prada S, Benavides FG, Serra C. Work-related psychosocial risk factors and musculoskeletal disorders in hospital nurses and nursing aides: a systematic review and meta-analysis. Int J Nurs Stud. 2015;52(2):635–648. doi:10.1016/j.ijnurstu.2014.11.003
7. Vieira ER, Schneider P, Guidera C, Gadotti IC, Brunt D. Work-related musculoskeletal disorders among physical therapists: a systematic review. J Back Musculoskelet Rehabil. 29(3):417–428. doi:10.3233/BMR-150649
8. Hanson H, Wagner M, Monopoli V, Keysor J. Low back pain in physical therapists: a cultural approach to analysis and intervention. Work. 2007;28(2):145–151.
9. Anderson SP, Oakman J. Allied health professionals and work-related musculoskeletal disorders: a systematic review. Saf Health Work. 2016;7(4):259–267. doi:10.1016/j.shaw.2016.04.001
10. Zhang H, Liu Y, Liu Y, Luo Y. Musculoskeletal Disorders in COVID-19 surveillance staff members: an analysis of prevalence, risk factors, and coping strategies. Br J Hosp Med. 85(11):1–17. doi:10.12968/hmed.2024.0423
11. Freimann T, Paasuke M, Merisalu E. Work-related psychosocial factors and mental health problems associated with musculoskeletal pain in nurses: a cross-sectional study. Pain Res Manag. 2016;2016:9361016. doi:10.1155/2016/9361016
12. Espin A, Nunez-Cortes R, Irazusta J, et al. Mental health and vitality predict spinal pain in healthcare workers. Occup Med. 2023;73(8):464–469. doi:10.1093/occmed/kqad096.
13. Wasserman JB, Bustos KM, Coombs SD, et al. Effect of slit lamp table design on neck position and the prevalence of neck pain in eye care professionals. Work. 2022;72(1):181–188. doi:10.3233/WOR-205141
14. Kitzmann AS, Fethke NB, Baratz KH, Zimmerman MB, Hackbarth DJ, Gehrs KM. A survey study of musculoskeletal disorders among eye care physicians compared with family medicine physicians. Ophthalmology. 2012;119(2):213–220. doi:10.1016/j.ophtha.2011.06.034
15. Long J, Naduvilath TJ, Hao LE, et al. Risk factors for physical discomfort in Australian optometrists. Optom Vis Sci. 2011;88(2):317–326. doi:10.1097/OPX.0b013e3182045a8e
16. Dhimitri KC, McGwin G Jr, McNeal SF, et al. Symptoms of musculoskeletal disorders in ophthalmologists. Am J Ophthalmol. 2005;139(1):179–181. doi:10.1016/j.ajo.2004.06.091
17. M A-MA-J, Khandekar R, Al-Harby M, Al-Hassan A, Edward DP. Neck and upper back pain among eye care professionals. Occup Med. 2015;65(9):753–757. doi:10.1093/occmed/kqv132
18. Venkatesh R, Kumar S. Back pain in ophthalmology: national survey of Indian ophthalmologists. Indian J Ophthalmol. 2017;65(8):678–682. doi:10.4103/ijo.IJO_344_17
19. Chatterjee A, Ryan WG, Rosen ES. Back pain in ophthalmologists. Eye. 1994;8((Pt 4):473–474. doi:10.1038/eye.1994.112
20. Bertelmann T, Heutelbeck A, Bopp S, et al. Prevalence of back pain among german ophthalmologists. Ophthalmic Res. 2021;64(6):974–982. doi:10.1159/000517574
21. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/BRM.41.4.1149
22. Kuorinka I, Jonsson B, Kilbom A, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18(3):233–237. doi:10.1016/0003-6870(87)90010-x
23. Lovibond SH, Lovibond PF. Manual for the Depression Anxiety Stress Scales.
24. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
25. van Poppel MN, Chinapaw MJM, Mokkink MJ, et al. Physical activity questionnaires for adults: a systematic review of measurement properties. Sports Med. 40(7):565–600. doi:10.2165/11531930-000000000-00000
26. Diaconita V, Uhlman K, Mao A, Mather R. Survey of occupational musculoskeletal pain and injury in Canadian ophthalmology. Can J Ophthalmol. 2019;54(3):314–322. doi:10.1016/j.jcjo.2018.06.021
27. Al Taisan A, Al Qurainees AE, Al Sowayigh OM, Al Owayfir MA. Musculoskeletal pain among eye care professionals. Cureus. 2023;15(5):e39403. doi:10.7759/cureus.39403
28. Zahrawi H, Asaad SHA, Al Houri AN, et al. The prevalence of work-related musculoskeletal disorder among health care workers in Damascus, Syria. A cross-sectional study. Health Sci Rep. 2024;7(2):e1860. doi:10.1002/hsr2.1860
29. Bezzina A, Austin E, Nguyen H, James C. Workplace psychosocial factors and their association with musculoskeletal disorders: a systematic review of longitudinal studies. Workplace Health Saf. 2023;71(12):578–588. doi:10.1177/21650799231193578
30. Kim SS, Okechukwu CA, Buxton OM, et al. Association between work-family conflict and musculoskeletal pain among hospital patient care workers. Am J Ind Med. 2013;56(4):488–495. doi:10.1002/ajim.22120
31. Michienzi AE, Anderson CP, Vang S, Ward CM. Lateral epicondylitis and tobacco use: a case-control study. Iowa Orthop J. 2015;35:114–118.
32. Sayampanathan AA, Basha M, Mitra AK. Risk factors of lateral epicondylitis: a meta-analysis. Surgeon. 2020;18(2):122–128. doi:10.1016/j.surge.2019.08.003
33. Curti S, Mattioli S, Bonfiglioli R, Farioli A, Violante FS. Elbow tendinopathy and occupational biomechanical overload: a systematic review with best-evidence synthesis. J Occup Health. 2021;63(1):e12186. doi:10.1002/1348-9585.12186
34. Almhdawi KA, Alrabbaie H, Kanaan SF, et al. The prevalence of upper quadrants work-related musculoskeletal disorders and their predictors among registered nurses. Work. 2021;68(4):1035–1047. doi:10.3233/WOR-213434
35. J-h K, S-a C, S-h J. Relationships among sleep quality, postural alignment, muscle strength, and psychological health in healthy adults. J Musculoskelet Sci Technol. 2025;9:72–78. doi:10.29273/jmst.2025.9.1.72
36. Hannibal KE, Bishop MD. Chronic stress, cortisol dysfunction, and pain: a psychoneuroendocrine rationale for stress management in pain rehabilitation. Phys Ther. 2014;94(12):1816–1825. doi:10.2522/ptj.20130597
37. Tembo LN, Munyikwa JP, Musoro C, Majonga G, Mavindidze E. Prevalence of work-related musculoskeletal disorders and associated factors among university of zimbabwe faculty of medicine and health sciences non-academic workers: a cross-sectional study. BMC Musculoskelet Disord. 2023;24(1):792. doi:10.1186/s12891-023-06900-1
38. Zhou Z, Meng P, Jia N, et al. Risk and related factors of elbow musculoskeletal diseases: a nationwide cross-sectional survey in China. J Occup Health. 2024;66(1). doi:10.1093/joccuh/uiae031
39. Garza JL, Ferguson JM, Dugan AG, et al. Investigating the relationship between working time characteristics on musculoskeletal symptoms: a cross sectional study. Arch Environ Occup Health. 2022;77(2):141–148. doi:10.1080/19338244.2020.1860878
40. Das S, Asokan R, Suresh J, Caron P, Subramaniam S. Prevalence of work related musculoskeletal disorders and quantification of ergonomic hazards among optometrists in chennai- a cross sectional study. Int. J. Kinanthrop. 2025;5(2):54–59. doi:10.34256/ijk2527
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.