Back to Journals » Risk Management and Healthcare Policy » Volume 18
Pattern of Pharmaceutical Poisoning in the Perak Population with Special Reference to the Age and Poisoning Mode Impact
Authors Gatera VA ![]() , Mat Rani NNI, Bin Ismail MF, Mohamed Khan HR, Nor Afendi NSH, Samsudin S, Mohd Samin AS
, Mat Rani NNI, Bin Ismail MF, Mohamed Khan HR, Nor Afendi NSH, Samsudin S, Mohd Samin AS ![]() , Rani NAA, Kamaruzaman NA
, Rani NAA, Kamaruzaman NA
Received 9 January 2025
Accepted for publication 7 November 2025
Published 18 November 2025 Volume 2025:18 Pages 3665—3674
DOI https://doi.org/10.2147/RMHP.S413695
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mecit Can Emre Simsekler
Vesara Ardhe Gatera,1 Nur Najihah Izzati Mat Rani,2 Muhammad Firdaus Bin Ismail,2 Halilol Rahman Mohamed Khan,2 Nor Safwan Hadi Nor Afendi,2 Sulastri Samsudin,3 Ahmad Shalihin Mohd Samin,3 Noor Afiza Abdul Rani,3 Nur Azzalia Kamaruzaman3
1Department of Biological Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jatinangor, West Java, Indonesia; 2Faculty of Pharmacy and Health Sciences, Universiti Kuala Lumpur – Royal College of Medicine Perak, Ipoh, Perak, Malaysia; 3Malaysia National Poison Centre, Universiti Sains Malaysia, Gelugor, Penang, Malaysia
Correspondence: Vesara Ardhe Gatera, Department of Biological Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jatinangor, West Java, Indonesia, Tel +62 22 84288828, Email [email protected] Nur Najihah Izzati Mat Rani, Faculty of Pharmacy and Health Sciences, Royal College of Medicine Perak, Universiti Kuala Lumpur - Royal College of Medicine, Ipoh, Perak, Malaysia, Tel +60 52432635, Email [email protected]
Introduction: Exposure to pharmaceutical poisoning affects people of all ages around the globe, and this is a serious emergency and a major problem. The unsafe medication disposal, such as keeping it at home until it expires, throwing it away in household garbage, giving it to friends/relatives, and flushing it down the toilet, has the consequences of this accidental, homicidal, or suicidal pharmaceutical poisoning toward international communities that range from short-term illness to long-term complications. However, the impact of pharmaceutical poisoning on the Malaysian population is a regular and frequent practice of disposal methods for pharmaceutical waste, and the awareness of pharmaceutical waste can have an adverse impact.
Purpose: : This study aimed to investigate the exposure to and association between pharmaceutical poisoning and intentional and accidental factors in the population from Perak, 2019 to 2021.
Patients and Methods: : This retrospective study evaluated reports from 348 patients with pharmaceutical poisoning in Perak, submitted to the National Poison Center (NPC) from 2019 to 2021. Initially, patient characteristics and clinical presentations were determined for pharmaceutical poisoning exposure, and their association with intentional and unintentional factors was analyzed.
Results: : This study found that the working-age group (48.28%) was the most represented age group. Psychiatric (23.0%) was the most frequent cause of poisoning. Quetiapine (2.9%) and calamine lotion (2.3%) were marked as the most common causes. Female sex (p < 0.001), working age (p < 0.001), and psychiatric agents (p < 0.001) were significantly associated with intentional poisoning, whereas male sex (p < 0.001), young age (p < 0.001), and topical agents (p < 0.001) were significantly associated with accidental poisoning.
Conclusion: : The exposure to pharmaceutical poisoning was associated with age, sex, psychiatric agents, and topical agents.
Keywords: pharmaceutical poisoning exposure, intentional and unintentional factors, Malaysia National Poison Center
Introduction
Nowadays, pharmaceutical poisoning affects people of all ages around the globe, and this exposure is a serious emergency and has become a major problem.1 Young age, female gender, low education level of patients and family members, and low socioeconomic status are identified by epidemiological studies on poisoning as the most common risk factors for pharmaceutical poisoning exposure.2 In Asia, according to data from Global Burden of Disease Study from 1990 to 2019, the pharmaceutical poisoning caters accidental poisoning trends in mortality disability-adjusted life- years (DALYs), years of life lost, years of lived with disability (YLDs) and causative agents in South Asian countries that decreased (32.6%) with the total number of deaths which is from 10.558 deaths in 1990 to 7112 deaths in 2019 (Khan et al, 2023). Based on statistics from the Malaysian National Poison Centre (NPC) database, intentional poisoning accounted for 60% of cases in Malaysia between 2006 and 2015. The majority of these instances occurred at home, and 93.6% of the purposeful cases involved attempted suicides. For instance, a massive number of 11,087 pesticide poisoning cases were recorded, with 60% intentional in nature found among male individuals.3
In addition, the negative consequences of this accidental, homicidal, or suicidal pharmaceutical poisoning toward the international community range from short-term illnesses such as nausea, dilated pupils, seizures, diarrhea, and rash to long-term complications such as organ damage, coma, moderate-to-severe depressive disorder, or even death.4 These consequences might be due to short-term exposure to poisoning, which leads to acute poisoning, or long-term or continuous exposure to poisoning, which leads to chronic poisoning. Depending on the dose, almost every class of medicine can have a hazardous impact, and thus, overuse of any medicine can result in poisoning.5 Predicting impacts in pharmaceutical and non-pharmaceutical poisoning is frequently challenging, particularly with the unclear profile and asymptomatic.6 The predictive impact of pharmaceutical poisoning is worsened because some are probable poisons and might cause severe consequences.7
According to poisoning cases that were retrospectively evaluated using consecutive sampling and admitted to Hospital Serdang between January 2007 and December 2016, pharmaceutical poisoning can have fatal consequences in Malaysia. During the study period, the prevalence of poisoning cases was 0.22% and the fatality rate was 1.8%. Young adults between the ages of 18 and 29 accounted for the majority of poisoning cases (44.2%), with females accounting for 59.7% of admissions compared to males. Overall, 74.5% consists of intentional poisoning cases, and 34.5% consists of non-opioid analgesics usage.8 In this study, we have determined and analyzed the societal characteristics, pharmaceutical categories, and association of pharmaceutical poisoning with intentional and accidental factors in Perak, Malaysia.
Materials and Methods
Study Design
Medical experts from healthcare facilities around Malaysia reported incidences of poisoning exposure related to pharmaceuticals from 2019 to 2021, and complete details of pharmaceutical cases were entered into the poison case report form (PCRF). All cases of pharmaceutical poisoning involved individuals aged 0–74 years old. An ethical issue considered in this research was the protection of participants’ confidential information, as their reports in the database were examined to gather information. Participants’ names and identity numbers were not recorded in this study to preserve participant confidentiality and privacy. The study protocol was approved by the Human Ethical Committee USM (HREC). The principles outlined in the research align with the principles outlined in the Declaration of Helsinki guidelines.
Study Setting and Population
This retrospective study was conducted in the total population of patients with Perak. This study was designed to determine the exposure to pharmaceutical poisoning and its association with intentional and accidental factors in the Perak population by analyzing the database of the National Poison Centre, Malaysia. All respondent reports were obtained from the National Poison Center during 2019–2021, and the population involved in this study was from the State of Perak, Malaysia. The sample size was based on reports by the National Poison Center from 2019 to 2021, and the calculated sample size was 348 from Perak. Calls related to poisoning by the general public and medical professionals. The telephone calls were recorded on a standardized Poison Case Report Form (PCRF), adapted from the WHO IPCS INTOX system, and then inserted into a database.
Inclusion and Exclusion Criteria
The details of the call included the name, address, product/poison information (drug/medicine), age, sex, categories of pharmaceuticals, clinical presentation, location of poison exposure, and reasons for poisoning exposure (intentional or accidental). All information relating to the call was documented. Each PCRF was manually extracted and reviewed to determine its inclusion criteria. The exclusion criteria included incomplete details of exposure and other types of poisoning, such as pesticide and household cases.
Data Analysis
All reported data obtained from the NPC were kept private and confidential. The data obtained in this study were analyzed using IBM Statistical Package for Social Sciences (SPSS) version 29.0.1.0 (171). Initially, the data outcomes for specific objective 1 were analyzed, involving independent variables such as age, sex, categories of pharmaceuticals, clinical presentation, location of poison exposure, and reasons for poison exposure (intentional or accidental), and reported as percentages. The outcomes of specific objectives 2 and 3, which are the factors that might be associated with intentional and accidental poisoning exposure, were analyzed using the Pearson X2 test, also known as the Chi-square test, which involved independent variables (age, sex, location of poison exposure, clinical presentations, and categories of pharmaceutical) and dependent variables (intentional and accidental factors of poison exposure). In addition, the reasons for poison exposure and sex were analyzed across different age groups using the Pearson χ2 test. Furthermore, statistical significance was set at p < 0.05.9
Results
Patient Characteristics and Clinical Presentation
Exposure to pharmaceutical poisoning in Perak accounted for 348% of the total population (n=348) between 2019 and 2021. All 348 patients with different pharmaceutical poisonings were analyzed in this study. Additionally, Table 1 presents their demographics, comprising 10 males (48.9%) and 174 females (50%). Next, there were three major races involved, with Malays accounting for 52.4% (n= 183). In this context, the age group of working individuals (15–64 years old) had the greatest representation (48.28%), with a frequency of 168 participants, and a mean age of 1.60 ± 0.597 years. Moreover, the most common location of poison exposure was reported at home (97.7%), with 340 cases. The major reason for poisoning exposure was accidental (52.0%), accounting for 181 cases, and most of the populations were exposed through the oral route (n=340). Additionally, the intentional reason for poison exposure accounted for 46.8% (n = 163). In addition to the 348 populations in Perak, 227 populations exhibited symptoms (65.2%), while 121 populations were asymptomatic (34.8%). The most common clinical presentation of symptoms, such as vomiting, was reported in 34 patients (9.8%).
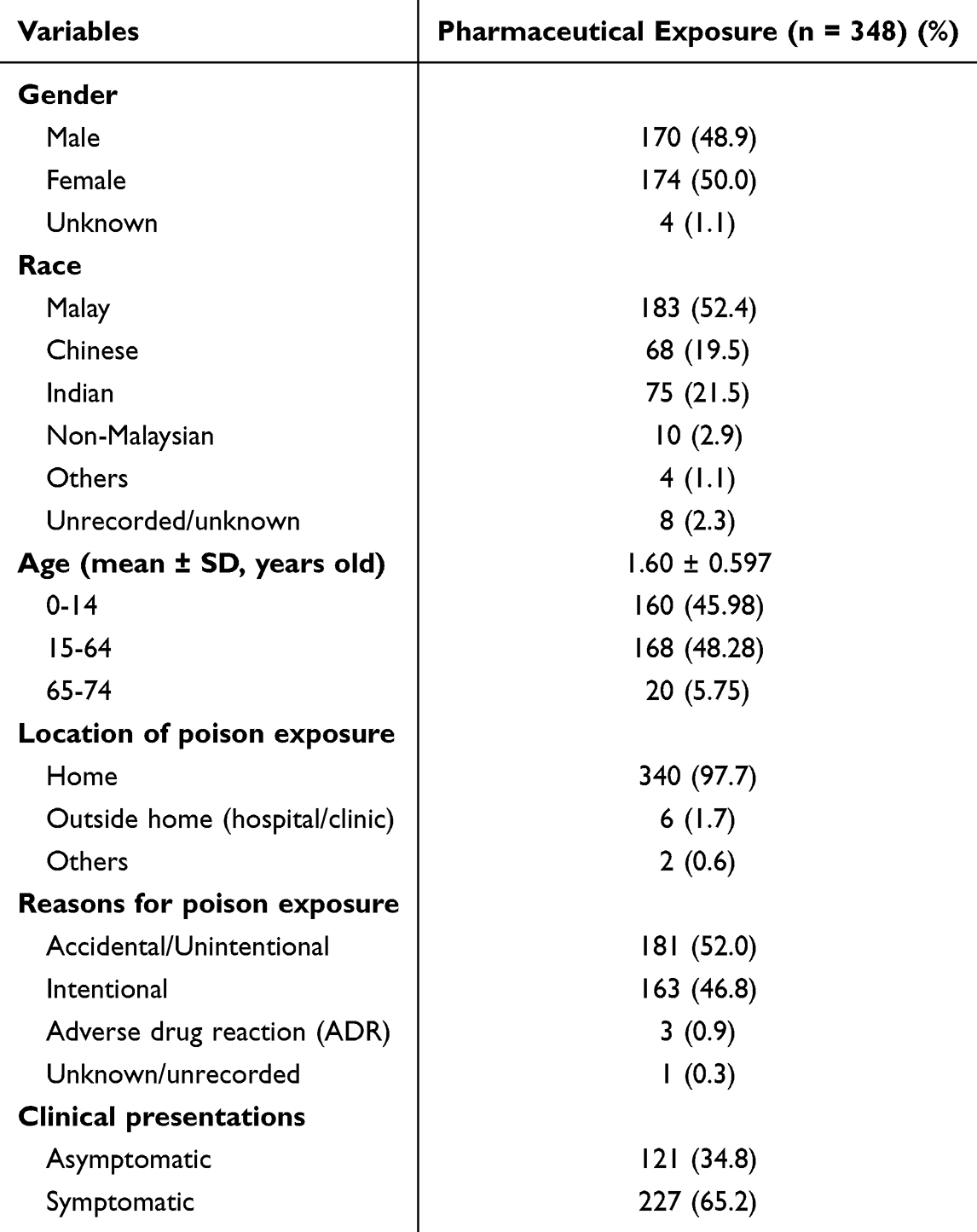 |
Table 1 Patient Characteristics and Clinical Presentations for Pharmaceutical Poisoning Exposure |
Pharmaceutical Categories
Pharmaceuticals are causing poisoning in the Perak population. In this context, Psychiatric agents were reported as the most common category of pharmaceutical poisoning (23.0%). Moreover, Topical agents have been recorded as the second most common pharmaceutical poisoning (15.8%) (Table 2).
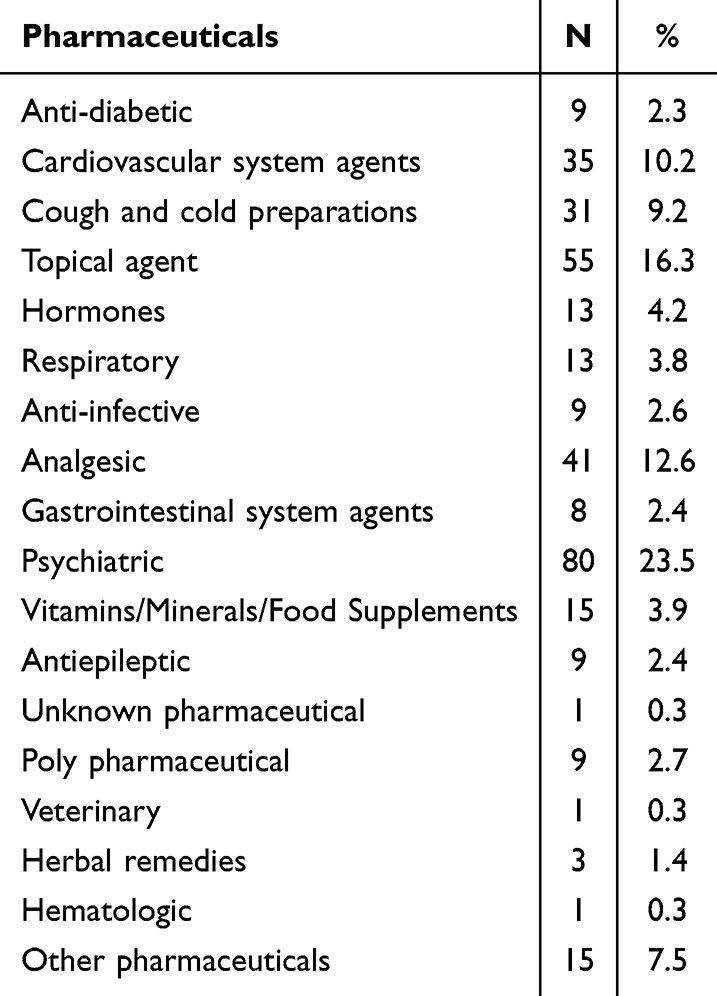 |
Table 2 Detailed Information on Pharmaceuticals |
Categories Pharmaceutical Poisoning Exposure
However, the outcomes in the Perak population were affected by different categories of exposure to pharmaceutical poisoning. In this context, hormones and herbal remedies were significantly associated with the young age group involved (1.00 ± 0.000 years) (p < 0.001). In addition, psychiatric agents were associated with the highest number of individuals in the 15–64 years old group involved (1.96 ± 0.434 years). Moreover, anti-diabetic agents have affected 8 (88.9%) patients in the working-age group (1.89 ± 0.33 years). Besides, the younger age group has been exposed more to pharmaceutical poisoning by cardiovascular system agents (62.9%) than working (22.9%) and post-working age groups (14.3%). Next, 19 patients (61.3%) were in the young age group, 11 patients (35.5%) were in the working age group, and 1 patient (3.2%) was in the post-working age group, all of whom were associated with pharmaceutical poisoning exposure related to cough and cold preparations (1.42 ± 0.564 years) (Table 3).
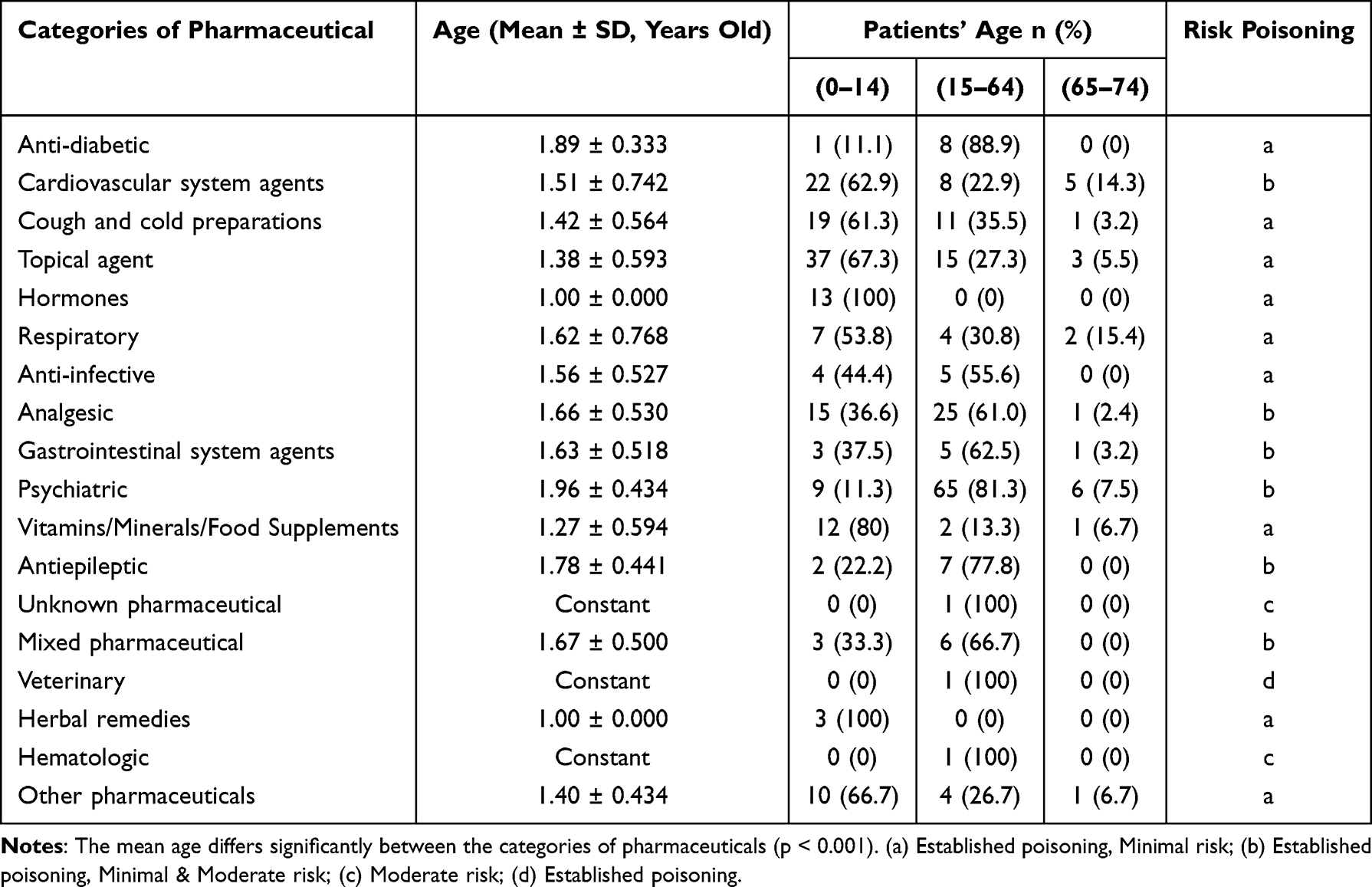 |
Table 3 The Outcomes of Patients Who Suffered Different Categories of Pharmaceutical Poisoning Exposure |
Differences Between Intentional and Accidental Pharmaceutical Poisoning Exposure
In this study, the reasons for pharmaceutical poisoning in the Perak population were classified as intentional or accidental. The differences between the two factors are demonstrated in Table 4, which shows the significant differences between intentional and accidental poison exposure, as more patients were exposed to pharmaceutical poisoning with accidental factors (n= 185) than with intentional factors (n= 163). In this context, the age groups of patients were significantly different between intentional and accidental factors (p < 0.001), as the mean ages of patients associated with intentional factors (1.22 ± 0.552 years) varied from those associated with accidental factors (2.01 ± 0.290 years). In terms of sex, males are more commonly gender to be exposed to pharmaceutical poisoning accidentally (64.3%) than intentionally (32.3%). Meanwhile, females were more commonly exposed to pharmaceutical poisoning intentionally (66.9%) than accidentally (35.1%). Thus, patient sex differed significantly between the two factors of exposure to pharmaceutical poisoning (p < 0.001).
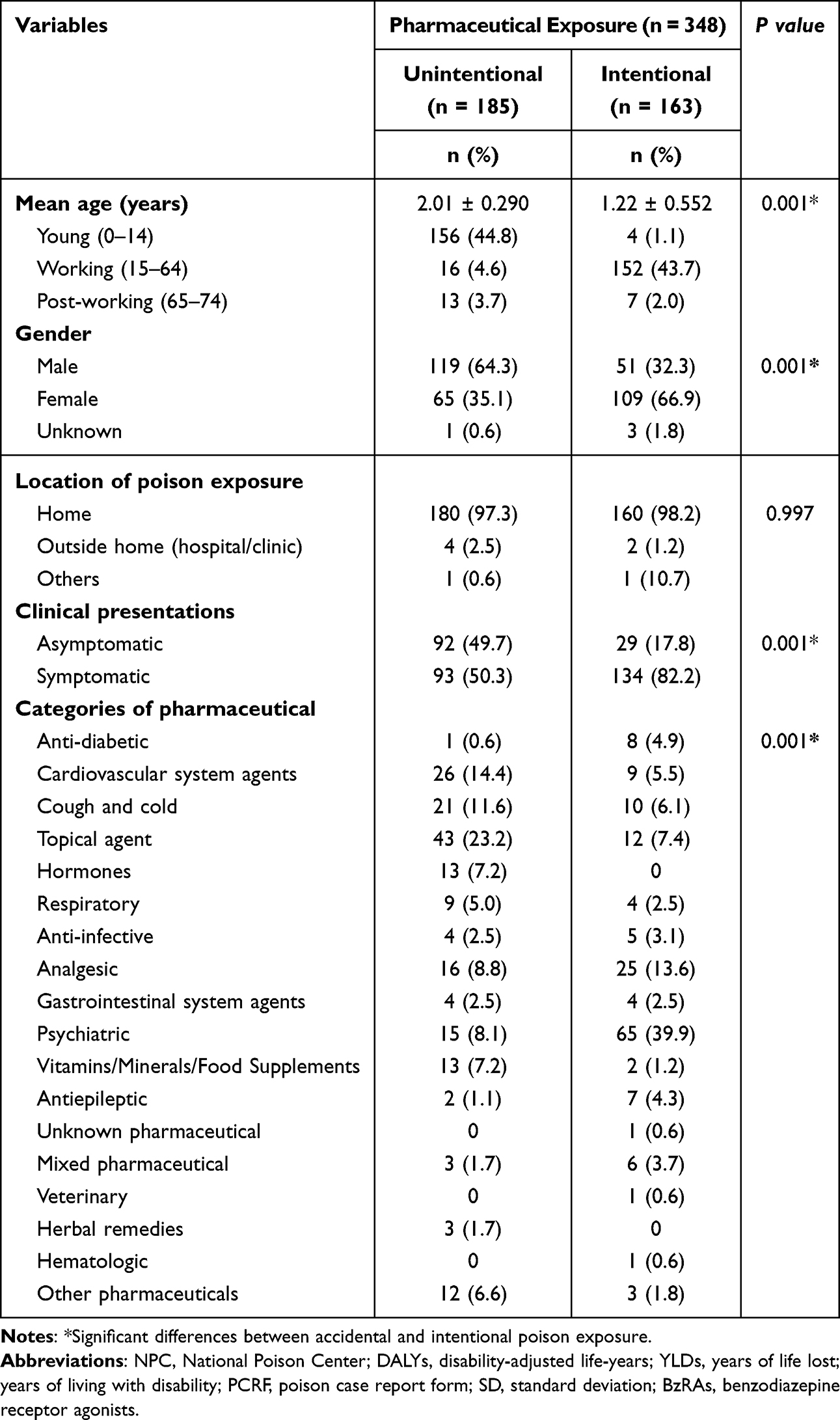 |
Table 4 Significant Differences Between Unintentional and Intentional Poisoning Exposure |
Next, the clinical presentation was significantly different between the intentional and accidental factors (p < 0.001). In this context, the majority of patients in Perak were having symptoms when exposed to pharmaceutical poisoning intentionally (82.2%), whereas some of them were asymptomatic as well (17.8%). Meanwhile, Accidental exposure to pharmaceutical poisoning with symptoms (50.3%) was recorded almost an equal number of patients without symptoms (49.7%). In addition, the categories of pharmaceuticals differed significantly between intentional and accidental factors (p < 0.001). For instance, psychiatric agents had the highest pharmaceutical poisoning exposure by intentional (39.9%). Meanwhile, Topical agents were the most common pharmaceutical poisoning exposure by accident (23.2) (Table 4).
Discussion
In Perak, pharmaceutical poisoning exposure in patients of different ages and genders is significantly different from the intentional and accidental factors of pharmaceutical poisoning exposure, as more than half of the exposure was accidental rather than intentional from 2019 to 2021. The primary factor associated with the reason for exposure to pharmaceutical poisoning was the age groups. Based on a previous study, more than half of the participants were exposed intentionally rather than accidentally between 2006 and 2015.10
In terms of age, the young and old groups recorded higher numbers of accidental pharmaceutical poisoning exposures. This report is Similar to Lin et al (2010) and Tangiisuran et al (2018) in Malaysia, where adolescents and adults reported a higher percentage.2,7 Another study by Naseri et al 2023 also showed the rate of pharmaceutical poisoning in patients between 15–35 years was relatively higher than in the other age groups, and with intentional poisoning was noticeable.11 This could be due to the lack of knowledge of caregivers about the toxicity of agents, risks, and lack of supervision, leading to overdosage of pharmaceutical or household products. Inappropriate storage of medicines and cleaning products can also lead to an increased risk of accidental exposure in young people, as their organ systems are still immature in detoxifying poisons, and their greater body surface area enhances the rapid rate of absorption through the skin as well.12 Additionally, this group considers psychological aspects to be the primary parameter.13,14 The capability to generate protection skills seems to be a factor in young adults.15 This study was consistent with the reports of some other findings.16–18 Studies commonly signify that the highest case of intoxication develops in adolescents and accidentally occurs among active workers.19,20
In addition, the old groups recorded the highest intentional poisoning exposure with suicide attempts. According to Jesslin et al (2010), the common reasons or factors for intentional poisoning are emotional disturbances, distress due to loss in business, failure in romance or differences with the intimate partner, failure in examination, and chronic disease.21 However, according to a previous study in Japan, the prevalence of dementia among the elderly increases the risk of accidental poisoning rather than intentional poisoning.22 The findings are consistent with those of previous studies, which might be due to the distribution and excretion of drugs, as well as the sensitivity to drugs changing with age, and the old age group usually uses multiple drugs (polypharmacy). Studies have reported the use of polypharmacy in both intentional and unintentional pharmaceutical deaths, with single-medication deaths being a minority.23–28
Furthermore, in this study, males were involved in accidental poisoning exposure, whereas intentional poisoning exposure was more associated with females. Based on a previous study in the US (2013) and Malaysia (2018), females were found to be more likely than males to be at risk for admissions of self-inflicted poisoning. This might be because a history of sexual trauma and anxiety disorders is usually associated with suicide attempts among females, while for males, it is associated with self-harm, alcohol use disorders, and economic stressors.10,29
In this study, the majority of intentional and accidental poisoning exposure occurred at home. This finding is similar to Yan-Ren et al 2011 in Taiwan; therefore, many intentional poisonings are frequently impulsive. Thus, restricting the compilation of pharmaceutical products stored at home through safe disposal campaigns via pharmacies could be an effective method. Promotions could be shared within healthcare facilities, and social media could be used as a medium to reach large audiences.2,30
This study revealed that intentional and accidental exposure to poisoning differed significantly according to the clinical presentation of symptoms in the Perak population. In this context, intentional poisoning exposure is commonly symptomatic, while accidental poisoning exposure has an equal proportion of clinical presentations in symptomatic and asymptomatic patients. Another study from Yan-Ren et al (2011) has similar findings for intentional and accidental poisoning exposure. Neurological side effects such as drowsiness and dizziness were the most common and consistent with other studies.2,29,31 Other studies reported that most people experienced poisoning events within their home premises, and there was a direct correlation between the quantity consumed and the side effects of many pharmaceutical poisonings.32–34
In Perak, we reported that psychiatric agents, topical agents, analgesics, and cardiovascular medications were the most common drugs associated with pharmaceutical poisoning. A previous study by Haselberger et al showed that analgesics, cardiovascular medications, theophylline preparations, antidepressants, and other psychotropic medications were common pharmaceutical poisonings.35 Then, psychiatric agents were demonstrated to be the most frequent in intentional poisoning, and also the pharmaceutical categories differed significantly between intentional and accidental poisoning. In this context, Haoka et al (2019) reported antihypertensive and antipsychotic agents as the most frequent agents causing intentional poisoning exposure, while benzodiazepine receptor agonists (BzRAs) have been reported as the most common agents causing accidental poisoning exposure.22 Another study reported that psychiatric agents, such as antipsychotics and tranquillizers, are utilized by the majority of suicide attempters in urban areas.10 According to multiple reports from hospitals and poison control centers, over-the-counter medications, such as paracetamol and some analgesics, are the most frequently implicated agents in poisoning cases in developed and developing countries.
Moreover, this study also found that topical agents were the most frequent cause of accidental poisoning, followed by cardiovascular agents. In this context, poisoning with topical agents is frequently reported in young age groups, which may be due to topical agents being readily available in every home and often placed on low shelves that can be quickly and easily accessed by young people, mostly children.36 Meanwhile, based on a previous study, poisoning with cardiovascular system agents commonly results in unstable hemodynamics and/or seizures, and these patients need to be closely monitored and treated with intensive treatment in a hospital, as accidental poisoning generally occurs from the standard dose.22
Limitation Study
The patterns observed in this research may not fully represent all regions and the current situation in Malaysia. During the study period (2019–2021), poisoning exposures may have been more common than the data suggest, as reporting them to the NPC is not compulsory. This study’s data is based on calls from healthcare providers across the country, detailing real or potential substance exposures that needed management at their healthcare facilities. However, not every poisoning or overdose was reported to the NPC, especially if the cases were manageable without needing further advice on treatment. Although this data helps us understand poisoning patterns in Malaysia, other Southeast Asian countries may observe very different trends or impacts due to their sociodemographic and regulatory contexts.
The study’s limitation is a lack of information on patient outcomes and poisoning severity, as no standard scoring systems were applied, such as the Poisoning Agitation-Sedation Score (PASS) and the Poisoning Severity Score (PSS), to predict the outcomes of acutely poisoned patients.37,38 It also does not include details on suicidal poisoned patients, clinical and laboratory parameters, and treatments used. Understanding medical outcomes is particularly important, given the high number of intentional exposures, to gauge the actual severity of the cases. Having this kind of data would significantly improve our understanding of the issue; for example, knowing about fatal poisonings could provide a basis for developing better prevention strategies.
Conclusion
The detailed categories of pharmaceuticals that cause intentional and accidental poisoning were analyzed in this study. Psychiatric and topical agents are responsible for most cases of intentional or accidental pharmaceutical poisoning. Hence, this report indicates that attention and care need to be applied to poisoning induced by storage, especially for pharmaceutical products in the home and other locations. Also, educational programs, parental control, community psychiatry campaigns, and psychological consultation are obligatory to prevent and restrain the incidence of pharmaceutical poisoning.
Ethical Approval
This research involves human participants. The study was approved by the Human Ethics Committee of Universiti Sains Malaysia (USM/JEPeM/22030173). Participants provided informed consent to participate in the study and report.
Acknowledgment
We thank the Malaysian National Poison Center for providing data used in this study. The findings and conclusions of this report are those of the authors and do not necessarily represent the views of the National Poison Center.”
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Chukkanakal JL, Kanakareddi B, Kurnool S, Senapathi P. A study of clinical profile and outcome of poisoning among pediatric population in a tertiary care hospital. Int J Health Sci. 2022;6(22):13230–13238. doi:10.53730/ijhs.v6nS2.8517
2. Lin YR, Wu TK, Liu TA, Chou CC, Wu HP. Poison exposure and outcome of children admitted to a pediatric emergency department. World J Pediatrics. 2011;7(2):143–149. doi:10.1007/s12519-011-0267-7
3. Kamaruzaman NA, Leong YH, Jaafar MH, Khan HR, Razali MF, Majid MIA. Epidemiology and risk factors of pesticide poisoning in Malaysia: a retrospective analysis by the National Poison Centre (NPC) from 2006 to 2015. BMJ Open. 2020;10(6):e036048. doi:10.1136/bmjopen-2019-036048
4. El-Sarnagawy G, Hafez A, Amer R. Characteristics of suicidal poisoned patients admitted to tertiary care center during COVID-19 pandemic. Egyptian J Neurol Psychiatry Neurosurg. 2022;58(1). doi:10.1186/s41983-022-00577-4
5. Deshmukh CD, Pawar AT. General principles, types, diagnosis and management of poisoning. Scholars Academic J Pharmacy. 2020;9(5):155–162. doi:10.36347/sajp.2020.v09i05.001
6. Saikia D, Sharma R, Janardhan K. Clinical profile of poisoning due to various poisons in children of age 0–12 years. J Family Med Prim Care. 2020;9(5):2291. doi:10.4103/jfmpc.jfmpc_365_20
7. Moon J, Chun B, Cho Y, Lee S, Jung E. Characteristics of emergency department presentations of pediatric poisoning between 2011 and 2016 A retrospective observational study in South Korea. Pediatr Emerg Care. 2021;37(5):261–268. doi:10.1097/PEC.0000000000001668
8. Leng TH, Ismail HA, Xuan HL, Zheng KL, Lotfi NAA, Taridi NS. Prevalence and mortality incidence of poisoning cases in serdang hospital. ASM Sci J. 2020;13:1–9. doi:10.32802/asmscj.2020.403
9. Kwak S. Are only p-values less than 0.05 significant? A p-value greater than 0.05 is also significant! J Lipid Atheroscler. 2023;12(2):89–95. doi:10.12997/jla.2023.12.2.89
10. Tangiisuran B, Jiva M, Ariff AM, et al. Evaluation of types of poisoning exposure calls managed by the Malaysia national poison centre (2006-2015): a retrospective review. BMJ Open. 2018;8(12):e024162. doi:10.1136/bmjopen-2018-024162
11. Naseri K, Kiani Z, Sajadi ZS, Mehrpour O, Javadmoosavi SY, Sadeghi M. Pharmaceutical toxicity is a common pattern of inpatient acute poisonings in Birjand City, East of Iran. Sci Rep. 2023;13:1312. doi:10.1038/s41598-023-28353-1
12. Vilaça L, Volpe FM, Ladeira RM. Accidental poisoning in children and adolescents admitted to a referral toxicology department of a brazilian emergency hospital. Rev Paulista Pediatria. 2020;25(38):e2018096. doi:10.1590/1984-0462/2020/38/2018096
13. Mackenzie S, Wiegel JR, Mundt M, et al. Depression and suicide ideation among students accessing campus health care. Am J Orthopsych. 2011;81(1):101–107. doi:10.1111/j.1939-0025.2010.01077.x
14. Sohrabi F, Yousefi F, Esfandyari G, Saed G, Abdollahi N, Bakhivushi S. Suicide and its relationship with demographic variables, psychiatric diagnosis and duration of disorders in patients of Ghods psychiatric hospital. Shenakht J Psychol Psychiatry. 2017;4(3):49–57.
15. Fakhari A, Rostami M, Hashemi T, Bvha N. Relationship of family features, coping styles and stressor life events with suicide attempt. J Res Behavioral Sci. 2014;12(2):155–164.
16. Singh DP, Aacharya RP. Pattern of poisoning cases in bir hospital. J Institute Med Nepal. 2006;28(1):3–6. doi:10.59779/jiomnepal.212
17. Ahmadi A, Pakravan N, Ghazizadeh Z. Pattern of acute food, drug, and chemical poisoning in Sari City, Northern Iran. Hum Exp Toxicol. 2010;29(9):731–738. doi:10.1177/0960327110361501
18. Torkashvand F, Sheikh Fathollahi M, Shamsi S, Kamali M, Rezaeian M. Evaluating the pattern of acute poisoning in cases referred to the emergency department of Ali-ebn Abi Taleb Hospital of Rafsanjan from October 2013 to September 2014. J Rafsanjan Univ Med Sci. 2015;14(4):311–324.
19. Cheng TL, Wright JL, Pearson-Fields AS, Brenner RA. The spectrum of intoxication and poisonings among adolescents: surveillance in an urban population. Inj Prev. 2006;12(2):129–132. doi:10.1136/ip.2005.010710
20. Henry KL, McDonald JN, Oetting ER, Walker PS, Walker RD, Beauvais F. Age of onset of first alcohol intoxication and subsequent alcohol use among urban American Indian adolescents. Addict Behav. 2011;25(1):48–56. doi:10.1037/a0021710
21. Jesslin J, Adepu R, Churi S. Assessment of prevalence and mortality incidences due to poisoning in a South Indian tertiary care teaching hospital. Indian J Pharm Sci. 2010;75(5):587–591. doi:10.4103/0250-474X.78525
22. Haoka T, Sakata N, Okamoto H, et al. Intentional or unintentional drug poisoning in elderly people: retrospective observational study in a tertiary care hospital in Japan. Acute Med Surg. 2019;6(3):252–258. doi:10.1002/ams2.403
23. Barocas JA, Wang J, Marshall BDL, et al. Sociodemographic factors and social determinants associated with toxicology confirmed polysubstance opioid-related deaths. Drug Alcohol Depend. 2019;200:59–63. doi:10.1016/j.drugalcdep.2019.03.014
24. Campbell G, Bruno R, Darke S, et al. Prevalence and correlates of suicidal thoughts and suicide attempts in people prescribed pharmaceutical opioids for chronic pain. Clin J Pain. 2016;32(4):292–301. doi:10.1097/AJP.0000000000000283
25. Campbell G, Darke S, Degenhardt L, et al. Prevalence and characteristics associated with chronic noncancer pain in suicide decedents: a national study. Suicide Life Threat Behav. 2020;50(4):778–791. doi:10.1111/sltb.12627
26. Darke S, Duflou J, Torok M. Comparative toxicology of intentional and accidental heroin overdose. J Forensic Sci. 2010;55(4):1015–1018. doi:10.1111/j.1556-4029.2010.01385.x
27. Darke S, Kaye S, Duflou J. Rates, characteristics and circumstances of methamphetamine-related death in Australia: a national 7-year study. Addiction. 2017;112(12):2191–2201. doi:10.1111/add.13897
28. Degenhardt L, Grebely J, Stone J, et al. Global patterns of opioid use and dependence: harms to populations, interventions, and future action. Lancet. 2019;394(10208):1560–1579. doi:10.1016/S0140-6736(19)32229-9
29. Dayasiri K, Jayamanne SF, Jayasinghe CY. Accidental and deliberate self-poisoning with medications and medication errors among children in rural Sri Lanka. Emerg Med Int. 2020;2020:1–8. doi:10.1155/2020/9872821
30. Hamid H, Masood RA, Tariq H, Khalid W, Rashid MA, Munir MU. Current pharmacy practices in low- and middle-income countries; recommendations in response to the COVID-19 pandemic. Drugs Therapy Perspect. 2020;36(8):355–357. doi:10.1007/s40267-020-00745-7
31. Alameli JM, Ezadi N. Frequency distribution of opiate poisoning according to individual characteristics and clinical manifestations. Scientific Inform Database. 2005;10(37):71–80.
32. Dayasiri MBKC, Jayamanne SF, Jayasinghe CY. Patterns and outcome of acute poisoning among children in rural Sri Lanka. BMC Pediatr. 2018;18(18):274. doi:10.1186/s12887-018-1246-0
33. Mowry JB, Spyker DA, Cantilena LR, McMillan N, Ford M. 2013 annual report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 31st annual report. Clin Toxicol. 2014;52(10):1032–1283. doi:10.3109/15563650.2014.987397
34. Anderson BJ, Holford NHG, Armishaw JC, Aicken R. Predicting concentrations in children presenting with Acetaminophen overdose. J Pediatr. 1999;135(3):290–295. doi:10.1016/s0022-3476(99)70122-8
35. Haselberger MB, Kroner BA. Drug Poisoning in Older Patients. Drugs Aging. 1995;7(4):292–297. doi:10.2165/00002512-199507040-00004
36. Alwan IA, Brhaish AS, Awadh AI, et al. Poisoning among children in Malaysia: a 10-years retrospective study. PLoS One. 2022;17(4):e0266767. doi:10.1371/journal.pone.0266767
37. Abd Elghany SA, Lashin HI, El-Sarnagawy GN, Oreby MM, Soliman E. Development and validation of a novel poisoning agitation-sedation score for predicting the need for endotracheal intubation and mechanical ventilation in acutely poisoned patients with disturbed consciousness. Hum Exp Toxicol. 2023;42. doi:10.1177/09603271231222253
38. El-Sarnagawy GN, Ghonem MM, Helal NE. Initial clinical and laboratory parameters triaging non-pharmaceutical acute pediatric poisoned patients for potential adverse outcomes: a three-year retrospective study. Toxicol Res. 2023;12(1):95–106. doi:10.1093/toxres/tfac088
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.