Back to Journals » Open Access Emergency Medicine » Volume 13
Pattern and Outcomes of Fall Injuries and Associated Factors in Emergency Department at Addis Ababa Burn, Emergency and Trauma Hospital
Authors Fikadu A ![]() , Sultan M, Michael M, Workina A
, Sultan M, Michael M, Workina A ![]()
Received 13 April 2021
Accepted for publication 4 August 2021
Published 19 August 2021 Volume 2021:13 Pages 381—389
DOI https://doi.org/10.2147/OAEM.S315546
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Hans-Christoph Pape
Ayele Fikadu,1 Menbou Sultan,1 Mebrat Michael,2 Abdata Workina3
1Department of Emergency and Critical Care, Saint Paul Hospital Millennium Medical College, Addis Ababa, Ethiopia; 2Department of Emergency Medicine, Addis Ababa University, Addis Ababa, Ethiopia; 3School of Nursing, Jimma University, Jimma, Oromia, Ethiopia
Correspondence: Abdata Workina
School of Nursing, Jimma University, P.O. Box-378, Jimma, Oromia Region, Ethiopia
Tel +251923643857
Email [email protected]
Introduction: Fall injuries are an important public health concern and remain a growing health problem globally. Falls are predicted to rise in rank compared to other causes of death, to become the 17th leading cause of death by 2030 unless necessary intervention is given.
Purpose: This study was aimed to assess the pattern, outcomes of fall injuries, and associated factors.
Methods: A cross-sectional study design was employed to review a patient’s registration chart from January 1, 2019 to December 31, 2019. Data were collected using a structured checklist developed from previous similar studies. The checked data were entered into Epi data 4.1 versions. Then, it was exported to SPSS 25 versions for analysis. Data were analyzed using descriptive statistics and logistic regression. In the multivariate logistic regression predictors having a P-value < 0.05 were considered to be statistically associated.
Results: A total of 331 patients’ charts were reviewed. The most common outcome of falling injury was alive 284 (85.8%) while death accounts for 47 (14.2%). Among injured body parts, extremity accounts for around one-fourth, 88 (26.6%), followed by head injury 68 (20.5%). In multivariate logistic regression, those patients aged ≥ 65 years had 6.15 times more likely to die than those patients aged between 15 and 30 years (AOR 6.15; 95% CI 2.82– 14.37, P=0.015), and participants with comorbidity were 1.6 times more likely to die than to be discharged (AOR 1.60; 95% CI, 1.01– 5.09, P=0.005) due to falling injury, whereas patient’s occupation, marital status, and sex had no significant association with outcomes of a fall injury.
Conclusion: The most common outcomes of fall injury were discharged with improvement even though there was a high death rate. Extremity injuries were the most common pattern of injury. Fall is high-risk mortality in the older age group. Furthermore, patient with comorbidity, fall from height and injury to spinal cord and poly-trauma is more likely to die relative to other patients.
Keywords: pattern, injuries, outcome, fall, emergency department
Introduction
Fall injuries are an important public health concern and remain a growing health problem worldwide.1–3 Globally, falls are the second leading cause of unintentional injury deaths, with 80% occurring in low- and middle-income countries.4,5 More than 5 million people die each year as a result of injuries, of which fall injuries account for 14% of it. This accounts for 9% of the world’s deaths, almost 1.7 times the number of fatalities that result from HIV/AIDS, tuberculosis, and malaria combined. Two of the three leading causes of injury deaths road traffic injuries and falls – are predicted to rise in rank compared to other causes of death, with falls rising to become the 17th leading cause of death by 2030 unless necessary intervention is given.1 A five years survey study conducted in Ethiopia shows that a total of 136 (21.8%) of accidental fall-related death was reported.6 From 2005 to 2015, global deaths due to falling increased by about 21%, and a major contributor to this were population growth and aging. If the problem was left unaddressed, the burden of fall injuries is projected to increase by 100% by the year 2030.4
The mechanism of fall injury category contains many different types of events, including falls from height, falls from the same level such as fall due to slipping, tripping, or pushing, and collisions due to pushing by another person.6,7
Many factors affect the mortality and morbidity of falls, such as patient age, gender, the co-morbidity associated with chronic illnesses, fall height, cause of fall, type of ground on which the patient fell, and body parts injured and risky behavior such as the intake of multiple medications, excess alcohol use, and sedentary behavior can increase risk fall and its consequences.8,9 Moreover, exposure to environmental risk factors such as narrow steps, slippery surfaces of stairs, looser rugs, Poor building design, cracked or uneven sidewalks, and poor lighting in public places are such hazards that might result in a fall injury.10
Hence, to decrease fall injuries and their consequences there should be preventive strategies that focus on education, training, creating safer environments, prioritizing fall-related research, and establishing effective policies to reduce risk.1
Generally, a different study was conducted worldwide regarding fall injuries with many recommendations to reduce its burden even though some recent reports show the consequence and health burden of fall injuries are increasing.6,10–14 However, there is a lack of data in Ethiopia in line with pattern and outcomes of fall injuries and its associated factors these might be important for health workers and managers to show the gap-related with fall injuries and its health burden and provide a direction on how to prevent fall injuries in the country. Additionally, this study might add whether problems related to falling injuries are universal to low-income countries since the study site represent it. So, this study aims to identify the pattern, outcomes, and associated factors of a fall injury.
Methods and Materials
A cross-sectional study design was conducted from the patient chart at Addis Ababa burn emergency and trauma (AaBET) hospital. The patient population included in the study was between January 1, 2019 and December 31, 2019. There are four trauma centers found in Addis Ababa Ethiopia. Of which two of them are major trauma centers (Alert Trauma Centre and AaBET hospital). AaBET hospital currently provides health care services in specialties namely; orthopedics, neurosurgery, plastic and reconstructive surgery, and emergency and critical care with more than 200 beds. It serves approximately 20–30,000 patients at ED per year.15
Study Population
Fall injury patient’s chart who had visited ED of AaBET hospital from 1st January 2019–31st December 2019.
Sample Size Determination and Sampling Procedure
Due to logistics and resources constraints to include all the study population for study, the sample size was determined using single population formula with confidence level 95%, 5% margin of error, p (proportion of patients who had alive outcome from fall injury) =50%, ni (initial sample size) =  Since the sample size was taken from less than 10,000 populations adjusted correctional formula was used. nf= ni(N)/ni±N = 310 Where N=1609, is the total number of fall injuries patients admitted at AaBET hospital from 1st January 2019–31st December 2019.
Since the sample size was taken from less than 10,000 populations adjusted correctional formula was used. nf= ni(N)/ni±N = 310 Where N=1609, is the total number of fall injuries patients admitted at AaBET hospital from 1st January 2019–31st December 2019.
Finally, after adding 10% contingency for incomplete data, a total of 341 patient charts were targeted for the study. To select each study unit, systematic random sampling technique was used using order of chart review by sampling fraction (k)= N/nf =1609/384=5 the first chart review was selected using the lottery method, then the subsequent patient’s chart review was obtained by adding the sample fraction (5).
Eligibility Criteria
All patients’ registration charts with fall injuries with complete data were included in the study while charts of patients with fall injuries aged < 14 years were excluded from the study.
Data Collection Tool and Procedures
A checklist was developed from previous similar studies which contain socio-demographic characteristics, the pattern of falling injury, outcomes, and factors associated with fall injury.2,16–20
Data were collected through chart review based on inclusion criteria by trained 5BSc Nurses.
Data Quality Assurance
The chart review instrument was pilot tested at Black Lion hospital on 5% of sample size and reliability statistics were computed with Cronbach’s alpha of 0.78 to check the consistency of the Checklist. Training about the contents of the checklist was given for data collectors three days before the data collection period. During the period of data collection, the supervisor was provided on-site close supervision, technical support, and all filled checklists were checked daily for completeness, accuracy, and consistency, and charts with incomplete information were excluded from the study.
Data Processing and Analysis
Checked data were entered into Epi data 4.1 versions. Then, cleaned data were exported and analyzed using SPSS 25.0 versions. Descriptive statistics were used to summarize categorical variables of patients’ characteristics and patterns, outcomes of fall injuries. The outcomes of fall injury were dichotomized into death and alive then, it was analyzed using binary logistic regression. The fitness of the model was checked by the Hosmer-Lemeshow goodness-of-fit test. In the binary logistic regression, predictors with p-value < 0.25 at 95% CI were candidates for multivariate logistic regression. In the multivariate logistic regression predictors with a probability value of < 0.05 were considered statistically significant.
Ethical Consideration
Before starting data collection, a letter of permission was obtained from the Addis Ababa university department of emergency medicine’s ethical review committee with Ref No. EM/SM/337/2012 and was given to the AaBET hospital administrator. Permission was taken to review patients’ registration charts. The patient’s names were omitted from the Checklist. Confidentiality of all the documents reviewed was highly secured throughout the data collection of the research process. This study was conducted in accordance with the Declaration of Helsinki. The patient informed consent was waived due to the anonymized data.
Results
Socio-Demographic Characteristics
A total of 331 participants were included in the study giving a completion rate of 97.1%. The mean age of respondents was 40.87 ± 19.5 years. Regarding the sex of participants, 207 (62.5%) were males. The most common occupational status of participants was governmental employees which accounts for 65 (19.6%) and 46 (13.9%) of them were daily laborers. The majority of participants’ residence area was urban which accounts for 253 (76.4%) (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Patients with Fall Injury at AaBET Hospital (n=331) from January 1, 2019 to December 31, 2019 |
Outcomes and Factors Associated with Fall Injuries
Among the study participants with fall injuries more than three-fourth, 284 (85.8%), had alive outcomes from fall injuries whereas the 47 (14.2%) of them had died due to fall injuries. Of which factors related to fall injuries Comorbidity was a common factor 92 (71.3%), then Alcohol intoxicated accounts 29 (22.5%) (Table 2).
 |
Table 2 Outcomes and Factors Related to Fall Injuries Among Patients Admitted at AaBET Hospital from January 1, 2019 to December 31, 2019 |
Types of Comorbidities Related to Fall Injury
The most common types of types of comorbidities related to fall injuries diabetes mellitus accounts for 23 (25.0%), followed by hypertension 20 (21.7%), then heart disease 14 (15.2%) whereas postural hypotension was the least comorbidity related with fall injuries (Table 3).
 |
Table 3 Types of Comorbidities in a Patient with Fall Injuries at AaBET Hospital from January 1, 2019 to December 31, 2019 |
Pattern and Mechanisms of Fall Injuries
Among injured body parts extremities injury accounts for around half of the fall injuries, 156 (47.1%), followed by head injury 78 (23.6%), whereas chest injury 18 (5.4%) was the least injured body part due to fall injury. The common cause of falling injuries was fall from the ground which accounts for 177 (53.47%), followed by fall from height 86 (26.0%), while the least cause of fall injuries was fall from stair 28 (8.46%) (Table 4).
 |
Table 4 Pattern and Mechanisms of Fall Injuries Among Patients Admitted at AaBET Hospital (n=331) from January 1, 2019 to December 31, 2019 |
Factors Associated with Outcomes of Fall Injuries
Before computing logistic regression, a cross tab was performed to identify whether the variables were a candidate for bivariate logistic regression. Then, in the crude binary logistic regression model, fitness was checked using Hosmer Lemeshow’s goodness-of-fit test. In this regression predictor variable with p-value of < 0.25 were a candidate for adjusted multivariate logistic regression. In this multivariate logistic regression, the method backward likelihood ratio (Backward LR) was used and those predictors with no association were removed in stepwise and the predictors in the last step in the model were considered to identify the association. Note: In the table of binary and multivariate logistic regression some variables were combined due to its small numbers.
In binary logistic regression age, comorbidity, occupation, injured site, and mechanisms of injury were found to be associated factors for the outcome of fall injuries with a P-value of <0.25, 95% CI. Those patients aged ≥65 years old were 1.5 times more likely than patients with the age of 15–30 years to die than to be discharged after improve (COR 1.51; 95% CI 0.68–3.32, P=0.025), daily laborer patients had 2.9 times probability of die than government employee (COR 2.92; 95% CI 0.91–9.38, P=0.032). Additionally, patients who had fallen from height were 4.3 times more likely to die than patients who fall from a stair (COR 4.33; 95% CI 1.54–12.15, P=0.002) and those patients who had comorbidity was 1.35 times more likely to die than to be improved (COR 1.35; 95% CI 0.55–3.35, P=0.014*) (Table 5).
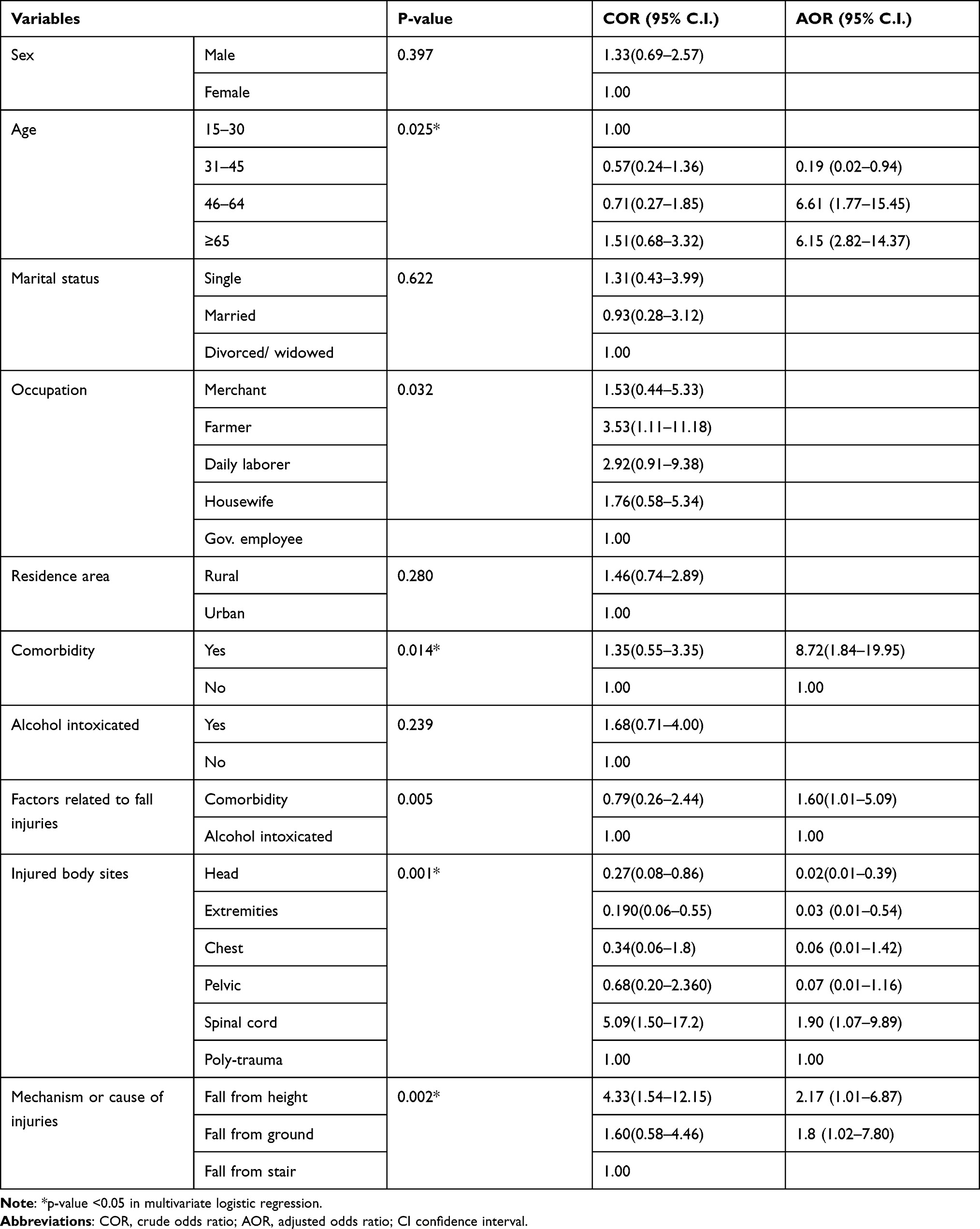 |
Table 5 Binary and Multivariate Logistic Regression of Factors Associated with Outcomes of Fall Injuries Among Participants at AaBET Hospital from January 1, 2019 to December 31, 2019 |
Based on multivariate logistic regression those patients aged ≥65 years old had 6.15 times more likely to die than those patients aged between 15 and 30 years (AOR 6.15; 95% CI 2.82–14.37, P=0.015). Those patients with comorbidity were 8.7 times more likely to die due to fall injury than those patients who had no comorbidity (AOR 8.72; 95% CI, 1.84–19.95, P= 0.014). Patients with comorbidity were 1.6 times more likely to die than alcohol-intoxicated patients due to fall injury (AOR 1.60; 95% CI, 1.01–5.0 9, P=0.005). Additionally, injured body sites and mechanism/cause of fall injury were significant associations at 95% CI with a p-value < 0.05. While variables like, sex, residence area, marital status, and occupations of the patients had no significant association with the outcomes of a fall injury (Table 5).
Discussion
Fall was the leading cause of unintentional injury which occurs both in low- and middle-income countries and it might occur due to some risk factors like aging, comorbidity, and occupational status.5,14 There is a lack of data in Ethiopia in line with pattern and outcomes of fall injuries and its associated factors this study might be important for health workers and managers to show the gap-related with falls injuries and its health burden and provide a direction on how to prevent fall injuries in the country. So, this study aimed to identify the common cause, the outcome of fall injuries, and its associated factors.
This study shows that most patients, 284 (85.8%) with fall injury had improved outcome even though, death accounts for 47 (14.2%) among patients with fall injury, of which 10 (68%) of them were found, 65 age groups. This study finding was higher than a study conducted in Europe by the institute of global health shows that falls are 5.7% of the patients with fall injuries were dead.21 Furthermore, a retrospective study was done in Iran and the USA showed 5.6% of patients died and the majority of them were in equal or greater than 62 years old group and a total, of 853 (2.7%) died among patients who visit emergency departments due to falling injuries from all trauma cases, respectively.22,23 This inconsistency might have occurred due to early health care accessibility and quality of health care differences among developing and developed countries. Our study was comparable to a 2015 national safety council report that revealed 2016, 697 (11.5%) patients died due to fall injury.24 Additionally, a retrospective study conducted in Ethiopia was relatively comparable with this study finding that showed the majority, 92.5%, of the cases of fall injuries were discharged with improvement and follow-up.25 This study is also supported by another study conducted in Taiwan that shows elderly patients in fall accidents tend to experience a higher mortality rate compared to adult patients.26 The possible reason for this comparability might be due to identical study design, selecting study participants, and related socio-demographic characteristics of study participants.
Among injured body parts lower extremity accounts for around half of the fall injuries, 156 (47.1%), followed by head injury 78 (23.6%), whereas chest injury 18 (5.4%) was the least injured body part due to fall injury. And the common cause of falling injuries was fall from the ground which accounts for 177 (53.47%), followed by fall from height 86 (26.0%), while the least cause of fall injuries was fall from stair 28 (8.46%). This study finding is consistent with a retrospective review in Sweden that shows extremity skeletal injuries (ranging from 20% to 77%) in high falls, where brain and spine injuries were seen in 25% of the fall from ground fallers.16 This study is also comparable with a retrospective study conducted in Pakistan that shows among injured body parts about 56.6% of fall injuries involved extremities, followed by head/neck 25.4% whereas study finding of a study showing 56.6% of fall injuries was due to slipping while about 28.5% were from height, and 15% were from tripping,19 which is contrary to our study finding. This might be due to the nature of geographic landmarks and living areas. Additionally, this study was relatively comparable with a one-year retrospective study conducted in Kenya among elderly patient’s shows that the major anatomical region affected was the extremity 63.9% and injuries to the head/neck instituted 26.4% of all injuries.27 This study finding is inconsistent with a study conducted in Taiwan that shows among patients who had fallen from a height, the most frequently affected body part was the head 91%, followed by the thorax 54%, abdomen 37%, extremities 36%, and neck 17%,26 and it was also in contrast with another retrospective study, conducted in India that shows 36% of them had a head injury and the second most common site of injury was the face, followed by the spine and lower limbs.27 The possible explanation for this incomparability was due to different mechanisms/causes of fall injuries resulting in differences in the site of injured body parts.
In multivariate logistic regression, those patients aged ≥65 years old had 6.15 times more likely to die than those patients aged between 15 and 30 years, AOR 6.15 (95% CI 2.82–14.37). Patients with comorbidity were 1.6 times more likely to die than alcohol-intoxicated patients due to fall injury, AOR1.60 (95% CI, 1.01–5.09). Additionally, injured body sites and mechanism/cause of fall injury were significant associations at 95% CI with a p-value < 0.05. These study findings were consistent with a seven-year retrospective study finding conducted in the United States shows that the death rate for fall injuries among people age ≥ 65 increased from 60.4 to 68.8 per 1000 populations.28 Similarly, a study conducted in Taiwan revealed that comorbidities are associated with outcomes of fall injuries (p value=0.03).26 Furthermore, a three-year retrospective study conducted in the United Kingdom had relative similarity showing, following a fall down a from height shows that older patients were more likely to suffer injuries to all body regions and sustained more severe injuries to the spine 23.6%.29 This consistency might be due to an identical study design.
In our study sex, residence area, marital status, and occupations of the patients had no association with the outcomes of a fall injury. This study was consistent with other studies conducted in the United Kingdom which reveal marital status and residential area of patients were no significant association.29 And also with study in Taiwan,26 and the USA which states sex of participants had no significant association.28 While, it was inconsistent with Bangladesh in 2017 regarding fall injuries shows that the risk of falls was higher at extremes of age.4 This inconsistent might be due to the socio-demographic difference of study respondents and among study regions.
Strengths and Limitations of the Study
The strengths of this study were; it generates valid information for the organization to establish or strengthen the health service and this finding is an original study in this particular study area that gives away and expects to formulate baseline information for the one who needs to conduct another assessment. The limitation of this study was since the study was conducted at a single facility-based it might affect the finding conclusion. Additionally, this study might have been a selection or measurement biases that may not have been avoidable.
Conclusion
The most common outcomes of fall injury were discharged with improvement even though there was a high death rate. Extremity injuries were the most common pattern of injury, followed by head injuries. The common cause of falling injuries was fall from the ground while the least cause of fall injury was fall from stairs. Fall is high-risk mortality in the older age group. Furthermore, patients with comorbidity, fall from height and injury to spinal cord and polytrauma has more likely to die relative to other patients. While predictors like sex, residence area, marital status, and occupation of the patients had no association with the outcome of falling injury (p-value > 0.05).
Acknowledgments
We would like to thank Addis Ababa Burn, Emergency, and Trauma Hospital for technical support during data collection.
Disclosure
We disclose that this manuscript was based on Ayele Fikadu’s Master’s thesis. The authors declare no conflicts of interest in this research work.
References
1. World Health Organization. Injuries and violence: the facts 2014. World Health Organization. Available from: https://www.who.int/violence_injury_prevention/media/news/2015/Injury_violence_facts_2014/en/.
2. Saidi H, Mutiso B. Injury outcomes in elderly patients admitted at an urban African hospital. Surgical Science. 2013;4(6):292–297. doi:10.4236/ss.2013.46057
3. CDC Injury Center. Important facts about falls | home and recreational safety. Available from: https://www.cdc.gov/homeandrecreationalsafety/falls/adultfalls.html.
4. Wadhwaniya S, Alonge O, Baset K, Chowdhury S, Bhuiyan MAA, Hyder A. Epidemiology of fall injury in rural Bangladesh. Int J Environ Res Public Health. 2017;14:900. doi:10.3390/ijerph14080900
5. Morello RT, Soh S-E, Behm K, et al. Multifactorial falls prevention programmes for older adults presenting to the emergency department with a fall: systematic review and meta-analysis. Inj Prev J Int Soc Child Adolesc Inj Prev. 2019;25(6):557–564. doi:10.1136/injuryprev-2019-043214
6. Gelaye KA, Tessema F, Tariku B, et al. Injury-related gaining momentum as external causes of deaths in Ethiopian health and demographic surveillance sites: evidence from verbal autopsy study. Glob Health Action. 2018;11(1):1430669. doi:10.1080/16549716.2018.1430669
7. Mekkodathil A, El-Menyar A, Kanbar A, et al. Epidemiological and clinical characteristics of fall-related injuries: a retrospective study. BMC Public Health. 2020;20(1):1–9.
8. Dr | Semantic Scholar. Biological, medical and behavioral risk factors on falls. Available from: https://www.semanticscholar.org/paper/Biological-%2C-Medical-and-Behavioral-Risk-Factors-on-Kronfol/632bc792e8bf38ade7b0fbf142bfdc48e52f582c#paper-header.
9. Morello RT, Soh SE, Behm K, et al. Multifactorial falls prevention programmes for older adults presenting to the emergency department with a fall: systematic review and meta-analysis. Injury Prevention. 2019;25(6):557–564. doi:10.1136/injuryprev-2019-043214
10. World Health Organization. WHO Global Report on Falls Prevention in Older Age. Geneva, Switzerland: World Health Organization; 2008:47.
11. Gebru AA, Mosadeghrad AM, Sari AA, Tafesse TB, Kahsay WG. Prevalence, pattern, magnitude and associated factors of trauma in the Emergency Department at Health Institutes in Ethiopia: A systematic review. Human antibodies. 2019;27(S1):1–10. doi:10.3233/HAB-190363
12. Tadesse B, Tekilu S, Nega B, Seyoum N. Pattern of injury and associated variables as seen in the emergency department at tikur anbessa specialized referral hospital, Addis Ababa, Ethiopia. East Cent Afr J Surg. 2014;19(1):73–82.
13. Miller E, Wightman E, Rumbolt K, et al. Management of fall-related injuries in the elderly: a retrospective chart review of patients presenting to the emergency department of a community-based teaching hospital. Physiother Can. 2009;61(1):26–37. doi:10.3138/physio.61.1.26
14. Toluse AM, Idowu OO, Ogundele OO, Egbewole AO. Injury epidemiology at a trauma center in Southwest Nigeria. Afr J Trauma. 2016;5(1):1.
15. Tadesse A. EC emergency medicine and critical care EC emergency medicine and critical care research article assessment of trauma care in Tertiary Center, Addis Ababa Ethiopia: an Observational Study. 2020.
16. Granhed H, Altgärde E, Akyürek LM, David P, Injuries sustained by falls - a review. Trauma Acute Care. 2017;2(2):38.
17. Wong C, Chihuri S, Li G. Risk of fall-related injury in people with lower limb amputations: A prospective cohort study. Journal of Rehabilitation Medicine. 2016;48(1):80–85. doi:10.2340/16501977-2042
18. Gebru AA, Mosadeghrad AM, Sari AA, Tafesse TB, Kahsay WG. Prevalence, pattern, magnitude and associated factors of trauma in the Emergency Department at Health Institutes in Ethiopia: a systematic review. Hum Antibodies. 2019;27(S1):1–10. doi:10.3233/HAB-190363
19. Fayyaz J, Wadhwaniya S, Shahzad H, et al. Pattern of fall injuries in Pakistan: the Pakistan National Emergency Department Surveillance (Pak-NEDS) study. BMC Emerg Med. 2015;15(Suppl 2):S3. doi:10.1186/1471-227X-15-S2-S3
20. Sitota AF. Pattern and outcomes of fall injuries and its associated factors in Emergency Department at Addis Ababa burn, emergency and trauma Hospital, Addis Ababa, Ethiopia, 2020. [Thesis]. Addis Abeba University; 2020. Available from: http://etd.aau.edu.et/handle/123456789/23266.
21. Norton R, Kobusingye O. Injuries. N Engl J Med. 2013;368(18):1723–1730. doi:10.1056/NEJMra1109343
22. Liu B, Zhu Y, Liu S, Chen W, Zhang F, Zhang Y. National incidence of traumatic spinal fractures in China. Medicine (Baltimore). 2018;97(35). Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6393073/.
23. Christopher Kevin W, Li G, Li G. Risk of fall-related injury in people with lower limb amputations: a prospective cohort study. J Rehabil Med. 2016;48(1):80–85. doi:10.2340/16501977-2042
24. Injury Facts; State Data; State Overview. National Safety Council analysis of National Center for Health Statistics (NCHS). Available from: https://injuryfacts.nsc.org/state-data/state-overview/.
25. Hajito K, Bayou N. Magnitude and pattern of injury in Jimma University Specialized Hospital, South West Ethiopia. Ethiop J Health Sci. 2011;21:155–165.
26. Rau C-S, Lin T-S, Wu S-C, et al. Geriatric hospitalizations in fall-related injuries. Scand J Trauma Resusc Emerg Med. 2014;22:63. doi:10.1186/s13049-014-0063-1
27. Jagnoor J, Keay L, Ganguli A, et al. Fall related injuries: a retrospective medical review study in North India. Injury. 2011;43:1996–2000. doi:10.1016/j.injury.2011.08.004
28. Shankar KN, Ganz DA, Liu SW. Trends and characteristics of emergency department visits for fall-related injuries in older adults, 2003–2010. West J Emerg Med Integrating Emerg Care Popul Health. 2017;18(5):785.
29. Chatha H, Sammy IA, Hickey M, Sattout A, Hollingsworth J. Falling down a flight of stairs: the impact of age and intoxication on injury pattern and severity. Trauma. 2017;20:169–174.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.