Back to Journals » Open Access Emergency Medicine » Volume 13
Pattern and Outcome of Acute Appendicitis: Observational Prospective Study from a Teaching Hospital, Addis Ababa, Ethiopia
Authors Gebre Selassie H, Tekle Selassie H, Ashebir D
Received 19 April 2021
Accepted for publication 25 May 2021
Published 22 June 2021 Volume 2021:13 Pages 265—271
DOI https://doi.org/10.2147/OAEM.S315228
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Hana Gebre Selassie,1 Henok Tekle Selassie,2 Daniel Ashebir2
1Department of Surgery, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia; 2Department of Surgery, Addis Ababa University, College of Health Sciences, Addis Ababa, Ethiopia
Correspondence: Hana Gebre Selassie
Department of Surgery, St. Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Tel +251913766868
Email [email protected]
Background: Acute appendicitis is the most common cause of acute abdomen surgery. Despite its commonness and the abundance of literature on the subject, its diagnosis remains challenging. Delay in intervention results in complications of the process leading to increased morbidity and mortality.
Methodology: An observational prospective cohort study was conducted, and all patients who had undergone appendectomy for a clinical diagnosis of appendicitis were included in the study. Data were analysed using Statistical Package for Social Sciences (SPSS) version 23.
Results: Half of the study participants were in the age range of 18– 25 years with male preponderance (63.9%). The mean duration of symptoms was 51.3 hours. The most common presenting symptom was abdominal pain (98.2%), while right lower quadrant tenderness was the most common sign (93.4%). Abdominal ultrasound was done in 81% of the study population with a sensitivity and specificity of 95.7% and 33.3%, respectively. Three-quarters (74.4%) of the patients had uncomplicated appendicitis, while 1.8% had a grossly normal appendix. None of the appendectomy specimens were sent for pathology. The mean hospital stay was 3.2 days. The morbidity and mortality rate were 3.8% and 0.4%, respectively.
Conclusion: Acute appendicitis was the most common emergency surgical procedure in the study period. Abdominal ultrasound was used in the majority of the patients as supplementary imaging for the diagnosis of acute appendicitis. Uncomplicated appendicitis took the major share of the intraoperative finding leading to acceptable morbidity and mortality rates.
Keywords: acute appendicitis, simple appendicitis, complicated appendicitis, morbidity, mortality
Introduction
Acute appendicitis is the most common cause of acute abdomen surgery with an incidence of 86.2–106 per 100,000 population.1 Once thought to be a disease of Western countries, its incidence is on the rise in the developing world.2 For instance, a recent global review showed that in the 21st century the incidence of acute appendicitis has increased in some of the newly industrialized countries in Asia, SouthAmerica, and the Middle East.3 Although population-based data are lacking in Ethiopia, appendectomy was reported as the most common emergency surgical procedure in several facility-based reports.4–8
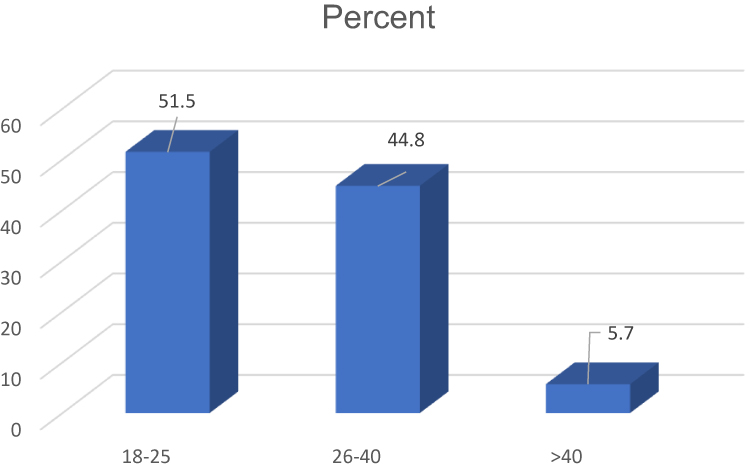 |
Figure 1 Age distribution of the study population. |
The diagnosis of acute appendicitis remains challengingand it was shown that on a population level, diagnosis of appendicitis has not improved with the availability of advanced diagnostic testing.9,10 Hence, some authors still follow the classic teaching that recommends the diagnosis of acute appendicitis to be guided by clinical parameters.11,12 Supplementary imaging modalities should be considered in cases of atypical presentation, children and females of reproductive age since clinical evaluation only may not be adequate to differentiate acute appendicitis from other abdominopelvic pathologies in these groups of patients.
Although conservative management is described to be effective in some centers, the gold standard management for acute appendicitis remains appendectomy.13,14 Open appendectomy has largely been replaced by laparoscopic appendectomyin many institutions in middle- and high-income countries. As an institution in a low-income country, our hospital has no facility for laparoscopic appendectomy and hence all procedures included in this study were open procedures.
The complications associated with acute appendicitis have been shown to be increased in cases of delayed presentation, elderly patients and intraoperative finding of complicated appendicitis.15–18 The overall complication rate post appendectomy is estimated to be 8.2–31.4%. In a report by the Lancet, the mortality rate was found to be higher in low-income and middle-income countries (1–4%) compared with developed countries (0.09–0.24%), reflecting the impact of health-care development on the outcome.19
This study aimed to determine the pattern of acute appendicitis in a referral hospital in Addis Ababa in terms of socio-demographic data, clinical presentation, diagnostic modalities and outcome. To our knowledge there is no prospective cohort study done in Ethiopia on this subject.
Materials and Methods
Study Setting
This study was conducted in Menelik II Referral Hospital which is located in Addis Ababa. This hospital was the first public hospital in Ethiopia and was established by Emperor Menelik the second in 1910. The hospital serves many patients from the capital city and surrounding towns. It also serves as a teaching hospital as its surgical department is affiliated with Tikur Anbessa Specialized Hospital of Addis Ababa University.
Study Design and Participants
A prospective observational study was conducted and patients were followed from the time of evaluation at the adult emergency department to the day of discharge from the hospital. Inclusion criteria were all adult patients aged 18 years and above who were operated on for the impression of acute appendicitis, while pediatric patients were excluded from the study.
Data Collection Instruments and Procedures
Data were collected by trained surgical residents using a questionnaire developed for the purpose of this study after they received a day of training. Informed written consent was obtained from all individual participants included in the present study. This study was conducted in accordance with the ethical standards of the institution and with the 1964 Declaration of Helsinki and its later amendments. Ethical clearance was also obtained from the research and ethical board of College of Health Sciences of Addis Ababa University.
Clinical Patient Evaluation Parameters
Patients were initially evaluated at the adult emergency department by trained surgical residents using several pre-defined clinical parameters including history and physical examination. Physical examination consists of measurement of the vital signs (temperature, blood pressure, pulse rate and respiratory rate) and abdominal examination.
Normal vital signs were defined as follows: temperature: morning temperature of <37.2°C or afternoon temperature of <37.7°C, axillary; blood pressure systolic 90–130 mmHg and diastolic 60–85 mmHg, pulse rate 60–100 beats per minute, respiratory rate 14–22 breaths per minute.20,21 Abdominal examination findings which were looked for were direct and rebound tenderness, guarding and palpable right lower quadrant mass.
Blood Work Up
Complete blood count was done in all patients to look for leucocytosis which was defined as a white cell count of >10,000/mL and left shift was considered if neutrophil percentage was > 70% as defined by Alvarado.22
Abdominal Ultrasound
Ultrasound parameters used for the diagnosis of acute appendicitis were the presence of oedematous appendiceal wall measuring > 6 mm, aperistaltic appendix, non-compressible appendix, appendiceal fat stranding, the presence of right lower quadrant free fluid, sonography tenderness at McBurney’s point and visualization of appendicolith. Except for the visualization of appendicolith which was considered definitive, the presence of only one parameter constituted probable acute appendicitis while the presence of two or more parameters was considered definite acute appendicitis. In the absence of all the above parameters and without other alternative diagnosis, a normal or unremarkable finding was reported.
Intraoperative Assessment
The appendix was grossly evaluated by the surgeon intraoperatively. The parameters used were as follows: the presence of erythema, size of the appendix, characteristics of the wall of the appendix, i.e. whether it is oedematous, compressible, any greyish or dark discolouration, fragility, presence of perforation, presence of fecalith. After gross assessment of the above parameters, the appendix was labelled into the following categories: grossly normal, inflamed, with phlegmon, mass, gangrenous, perforated with or without abscess.
Simple or uncomplicated appendicitis was diagnosed if the intraoperative finding was inflamed or appendix with phlegmon while complicated appendicitis implies a stage in which the appendix was found to be gangrenous, perforated or associated with abscess and local/generalized peritonitis. Gangrenous appendix was defined as the presence of darkened, aperistaltic and fragile appendiceal wall without perforation. The above definitions were taken from similar literature on the subject.23–26
Post Appendectomy Outcome Assessment
Outcome was assessed in terms of development of complications and mortality. Intra-operative complications which were looked for include excessive bleeding and iatrogenic bowel or bladder injury while post-operative complications include surgical site infection, post-operative abdominal collection, wound dehiscence and respiratory complications.
Data Analysis and Presentation
Data coding and analysis was done using SPSS 23 (Statistical Packages for Social Sciences). Data are presented as both frequency and percentage for discrete variables and as a mean and standard deviation for continuous variables. The presence of association between several independent patient variables and the development of complications was assessed by a chi square analysis considering a confidence interval of 95% and a P value of <0.05 was considered significant in all computations.
Result
A total of 227 patients were evaluated at the adult emergency department of Menelik II Referral Hospital with a diagnosis of acute appendicitis based on clinical, laboratory and imaging parameters in the study period and all underwent surgery. Acute appendicitis was the most common emergency surgical procedure accounting for 46.4% of the emergency operations in the study period.
Socio-demographic Characteristics
Males took the major share of the study population accounting for 63.9% and with a male to female ratio of 1.8:1. The mean age was 27.62 ± 8.6 years with a range of 18–70 years. Half of the study participants belong to the age group of 18–25 years (Figure 1). As to the place of residence, the majority of the patients (88.5%) came from the capital city.
Clinical Presentation
The mean duration of symptoms was 51.34 ± 100.5 hours with a range of 4 hours to 10 days while the median and the mode were 29 hours and 24 hours, respectively. The most common presenting symptom was abdominal pain, 223 (98.2%), followed by migration of abdominal pain, 186 (81.9%), and anorexia, 159 (70%), while the most common physical sign was right lower abdominal tenderness, 212 (93.4%). At initial evaluation in the emergency department, 72 (31.7%) of the patients were tachycardic while 39 (17%) were febrile and 2 (0.9%) were hypotensive.
Investigations
Leucocytosis was seen in 69 (30.1%) patients while 164 (72.2%) had left shift. Abdominal ultrasound was done in 184 (81%) patients as part of the preoperative assessment (Table 1). Among patients for whom abdominal ultrasound was done, 9 (4.9%) were reported to have another pathology: 1 (0.5%) nephrolithiasis, 2 (1.1%) ileocolic intussusception, 2 (1.1%) pelvic inflammatory disease, 2 (1.1%) ovarian cyst and 2 (1.1%) mesenteric adenitis. Among patients who had simple/uncomplicated appendicitis intraoperatively, 8 (5.8%) patients were reported to have normal abdominal ultrasound preoperatively while no patient with complicated appendicitis was reported to have normal ultrasound (figure 1, Table 2). The sensitivity of abdominal ultrasound in this study was 95.7% while the specificity was 33.3%.
 |
Table 1 Abdominal Ultrasound Report versus Intra-operative Stage of Appendicitis |
 |
Table 2 Stage of Appendicitis versus Duration of Symptoms |
Operative Findings
The most common abdominal incision used was right lower quadrant transverse incision, in 195 (85.9%) of the patients, followed by midline sub-umbilical vertical incision 17 (7.5%). The type of incision was selected based on the findings of abdominal examination. Right lower quadrant transverse incision was used in patients who had localized tenderness at the right lower quadrant of the abdomen while midline sub-umbilical vertical incision was used for patients with diffuse abdominal tenderness.
Simple/uncomplicated appendicitis accounted for three-quarters of the cases, 169 (74.4%), while 54 (23%) were at a complicated stage. The majority of patients who presented within 48 hours of the onset of symptoms had simple/uncomplicated appendicitis (Table 2).
Four patients were found to have grossly normal appendix by operating surgeon’s assessment. None of the specimens were sent for histo-pathological analysis as this service is not available in our hospital. All these patients had abdominal ultrasound done and half, 2 (50%), were reported to have definite acute appendicitis while 1 (25%) had unremarkable ultrasound report and 1 (25%) was reported to have mesenteric adenitis without sonographic signs of acute appendicitis (Table 2).
The great majority of the appendectomies were performed by general surgery residents, in 225 (99.1%) of the cases. The mean duration of surgery was 54.58±24.3 minutes while the mean hospital stay was 3.2±1.9 days.
Outcomes After Appendectomy
Complications developed in 9 (3.8%) of patients in the post-operative period, the most common being superficial surgical site infection, in 4 (1.8%) (Table 3).
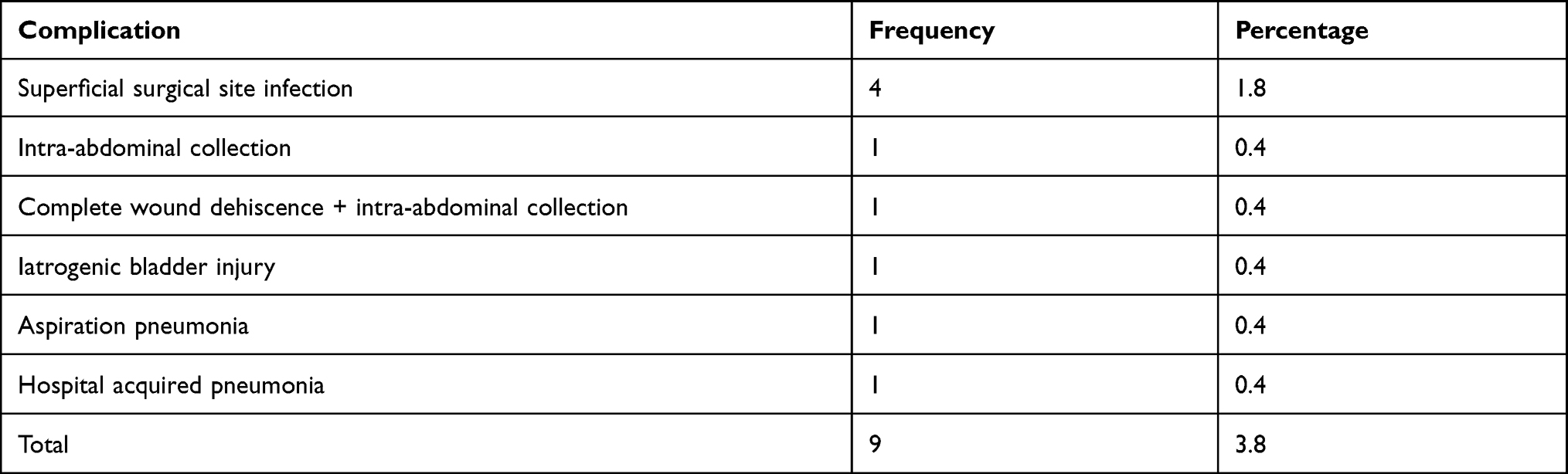 |
Table 3 Complications Post Appendectomy |
Relaparotomy was required in 2 patients (0.8%) with intra-abdominal collection. One patient who was initially operated on for complicated acute appendicitis with generalized peritonitis, developed complete wound dehiscence and intra-abdominal collection postoperatively and died subsequently due to sepsis. Hence, the mortality rate in this study was 0.4%.
Associations
The association between duration of symptoms of more than 48 hours and presence of complicated appendicitis was found to be significant by a chi square analysis considering a confidence interval of 95% with p = 0.000. Age, sex and place of residence were not found to have any significant association with complications and mortality by a chi square analysis. In addition, the association between the type of abdominal incision used and the development of surgical site infection was found to be significant by a chi square analysis considering a confidence interval of 95% with p = 0.028.
Discussion
Acute appendicitis is a disease of the young with a peak incidence at the second and third decade of life. This was also seen in our study in which half of the patients belonged to the age group of 18–25 years. The same pattern was observed in other studies from Africa.5,27–34 There is also a known male preponderance which was also reflected in our study as well as other reports.4–8,35–37
The mean duration of symptoms was more than 2 days in this study which is in line with similar studies done locally and from South Africa.5,27,30,37 Almost all patients presented with abdominal pain as in other reports in Ethiopia, Nigeria and South Africa.5,27,31,33 The typical migratory type of abdominal pain was present in a great majority of patients (81.9%) in this study which is a higher figure compared with a study from South Africa in which it was seen only in one-third of the patients and a study in India that reported it in 52% of the patients.35,36
The most common physical finding was right lower quadrant tenderness which was demonstrated in 93.4% of patients, which was also true in other studies.7,27,33,36 Leucocytosis was seen in only one third of our patients which is a lower figure compared with other studies from Zewditu Memorial Hospital, Ethiopia and India in which 50.7% and 70% of the patients had leucocytosis, respectively.7,36
Supplementary imaging study (abdominal ultrasound) was done in 81% of our patients. Although the proportion of patients for whom imaging was done for the diagnosis of acute appendicitis was not mentioned in similar local studies, from our observations our figure may be quite high. This may be in part explained by the fact that our institution is a referral hospital and most of our patients will be evaluated and investigated at a primary health-care facility prior to their referral to our institution. Hence, most patients have ultrasound done when they arrive to the emergency department of our hospital. The other fact may be the increased tendency to use imaging modalities by physicians nowadays, which is also observed in other studies.37,38 In some of these reports it was even described that the increasing trend in the use of preoperative imaging has decreased the negative appendectomy rate and it is a practice to be encouraged.38,39
The most common incision used for appendectomy in this study was right lower quadrant transverse incision as three-quarters of the patients had simple appendicitis. Complicated appendicitis was found in 23% of the patients which is comparable with some reports7,15,29,33 while it was found to be lower than some reports.27,35 Grossly normal-looking appendix was the finding in 1.8% of the patients by operating surgeon’s assessment. The correlation rate of intra-operative finding with histopathological reports is debatable with a mentioned similarity of between 46.6% and 93.5% in different literatures.40–44
The complication rate in this study was found to be 3.8%, which was significantly lower than similar studies.29,35,37 The most common postoperative complication was superficial surgical site infection which is in line with other studies but with much less magnitude.27,33,35 Intra-abdominal collection was the second most common complication and was the indication for re-exploration.
The relaparotomy rate of this study is 1.85% and was comparable with one report from Sweden while it was significantly lower compared with a study done in a rural part of South Africa. The lower post-operative intra-abdominal collection rate might be due to the fact that the majority of the patients have simple appendicitis. The mortality rate in this study was found to be lower compared with studies done locally but in earlier years, which may reflect an improved health-seeking behaviour of the society or better surgical care.7,27,44 The mean hospital stay was found to be shorter than in other reports.27,29,34,35,45,46
Disclosure
The authors report no conflicts of interest in this work.
References
1. Golz RA, Flum DR, Sanchez SE, Liu X, Donovan C, Drake FT. Geographig association between incidence of acute appendicitis and socia economic status. JAMA Surg. 2020;155(4):330–338. doi:10.1001/jamasurg.2019.6030
2. Reiter AJ, Schlottmann F, Kajombo C, Gallaher J, Charles AG. Surgical outcomes of acute appendicitis in high-middle- and low-income countries. Am Surg. 2019;85(2):97–99. doi:10.1177/000313481908500210
3. Ferris M, Quan S, Kaplan BS, et al. The global incidence of appendicitis, a systematic review of population-based studies. Ann Surg. 2017;266(2).
4. Kotiso B, Abdurahman Z. Pattern of acute abdomen in adult patients in Tikur Anbessa Teaching Hospital, Addis Ababa, Ethiopia. East Central Afri J Surg. 2007;12(1):47–52.
5. Hagos M. Acute abdomen in adults: a two-year experience in Mekelle, Ethiopia. Ethiop Med J. 2015;53(1):19–24.
6. Melkie A, Alemayehu T, Tarekegn E. Pattern of acute abdomen in Dil Chora Referral Hospital, Eastern Ethiopia. Int J Collab Res Intern Med Public Health. 2016;8(11):607–615.
7. Deneke A, Tadesse B. Pattern and clinical presentation of acute appendicitis in adults in Zewditu memorial hospital. Ethiop J Health Sci. 2003;13(2).
8. Hanks L, Lin CP, Tefera G, Seyoum N. Abdominal surgical emergencies at Tikur Anbessa Specialized Hospital in Ethiopia; a shifting paradigm. East Central Afri J Surg. 2014;19(1).
9. Wagner JM, McKinney WP, Carpenter JL. Does this patient have appendicitis? JAMA. 1996;276:19.
10. Snyder MJ, Guthrie M, Cagle S. Acute appendicitis: efficient diagnosis and management. Am Fam Physician. 2018;98(1):25–33.
11. Petroianu A. Diagnosis of acute appendicitis. Int J Surg. 2012;10:115e119. doi:10.1016/j.ijsu.2012.02.006
12. Baird DLH, Simillis C, Kontovounisios C, Rasheed S, Tekkis PP. Acute appendicitis. BMJ. 2017;357:j1703. doi:10.1136/bmj.j1703
13. Flum DR, Morris A, Koepsell T, Dellinger EP. Has misdiagnosis of appendicitis decreased over time? A population-based analysis. JAMA. 2001;286(14):1748–1753. doi:10.1001/jama.286.14.1748
14. Di Saverio S, Birindelli A, Kelly MD. WSES Jerusalem guidelines for diagnosis and treatment of acute appendicitis. World J Emerg Surg. 2016;11:34. doi:10.1186/s13017-016-0090-5
15. Kim JW, Shin DW, Kim DJ, Kim JY, Park SG, Park JH. Effects of timing of appendectomy on the risks of perforation and postoperative complications of acute appendicitis. World J Surg. 2018;42:1295–1303. doi:10.1007/s00268-017-4280-4
16. Kidwai R, Sharma A. Acute perforated appendicitis: clinical profile and analysis of risk factors. J Nepalgunj Med Coll. 2018;16:13–15. doi:10.3126/jngmc.v16i2.24865
17. Khan J, Ali A, Sarwar B. Causes of delayed presentation of acute appendicitis and how it affects morbidity and mortality. J Saidu Med Coll. 2018;8(1).
18. Calis H. Morbidity AND MORTALITY IN APPENDICITIS IN THE ELDERLY. J Coll Physicians Surg Pak. 2018;28(11):875–878. doi:10.29271/jcpsp.2018.11.875
19. Bhangu A, Søreide K, Di Saverio S, Assarsson JH, Drake FT. Acute appendicitis: modern understanding of pathogenesis, diagnosis, and management. Lancet. 2015;386:1278–1287. doi:10.1016/S0140-6736(15)00275-5
20. Bickley L, Szilagyi PG. Bates’ Guide to Physical Examination and History Taking.
21. Longo DL, Kasper DL, Larry Jameson J, Fauci AS, Hauser SL, Loscalzo J. Harrison’s Principles of Internal Medicine.
22. Alvarado A. A practical score for the early diagnosis of acute appendicitis. Ann Emerg Med. 1986;15:557–564. doi:10.1016/S0196-0644(86)80993-3
23. Kim HY, Park JH, Lee SS, Jeon JJ, Yoon CJ, Lee KH. Differentiation between complicated and uncomplicated appendicitis: diagnostic model development and validation study. Abdom Radiol. 2020. doi:10.1007/s00261-020-02737-7
24. García-Marín A, Pérez-López M, Martínez-Guerrero E, Rodríguez-Cazalla L, Compañ-Rosique A. Microbiologic analysis of complicated and uncomplicated acute appendicitis. Surg Infect (Larchmt). 2018;19(1). doi:10.1089/sur.2017.210
25. Bom WJ, Scheijmans JCG, Salminen P, Boermeester MA. Diagnosis of uncomplicated and complicated appendicitis in adults. Scand J Surg. 2021;1–10. doi:10.1177/14574969211008330
26. Mariage M, Sabbagh C, Grelpois G, Prevot F, Darmon I, Regimbeau JM. Surgeon’s definition of complicated appendicitis: a prospective video survey study. Eur J Hepato Gastroenterol. 2019;9(1).
27. Asefa Z. Acute appendicitis in Yirgalem Hospital, southern Ethiopia. Ethiop Med J. 2002;40(2):155–162.
28. Doumi EA, Abdelrahman IH. Acute appendicitis: still a missed diagnosis in El Obeid, Western Sudan. Sudan JMS. 2007;2(1). doi:10.4314/sjms.v2i1.38459
29. Chavda SK, Hassan S, Magoha GA. Appendicitis at Kenyatta National Hospital, Nairobi. East Afr Med J. 2005;82(10):526–530. doi:10.4314/eamj.v82i10.9351
30. Kong VY, Aldous C, Clarke DL. Understanding the reasons for delay to definitive surgical care of patients with acute appendicitis in rural South Africa. S Afr J Surg. 2014;52(1):2–5.
31. Chamisa I. A clinic pathological review of 324 appendices removed for acute appendicitis in Durban, South Africa: a retrospective analysis. Ann R Coll Surg Engl. 2009;91:688–692. doi:10.1308/003588409X12486167521677
32. Alegbeleye BJ, Adisa CA, Keskin H. Epidemiologic features of acute appendicitis in a Tropical African Population. WW Med. 2019;1(6):202–211.
33. Edino ST, Mohammed AZ, Ochicha O, Anumah M. Appendicitis in Kano, Nigeria: a 5-year review of pattern, morbidity and mortality. Ann Afr Med. 2004;3(1):38–41.
34. Clegg-Lamptey J, Naaeder S. Appendicitis in Accra: a contemporary appraisal. Ghana Med J. 2003;37(2).
35. Kong VY, Sartorius B, Clarke DL. Acute appendicitis in the developing world is a morbid disease. Ann R Coll Surg Engl. 2015;97:390–395. doi:10.1308/003588415X14181254790608
36. Mathew T, Ammanagi AS. Clinicopathological evaluation of acute appendicitis and the role of ultrasound in diagnosis: a prospective study. Int Surg J. 2019;6(5):1471–1476. doi:10.18203/2349-2902.isj20191560
37. Dahlberg MJ, Pieniowski EH, Boström LÅ. Trends in the management of acute appendicitis in a single-center quality register cohort of 5614 patients. Dig Surg. 2018. doi:10.1159/000477269
38. Høydahl Ø, Kørner H, Edna TH. Preoperative imaging in the diagnosis of acute appendicitis is associated with low negative appendectomy rate. Int J Surg Res Pract. 2017;4:3.
39. Daly AB, Cuthbert R, Finnegan D, Arnold C, Craddock C, McMullin MF. Pre-operative imaging can reduce negative appendectomy rate in acute appendicitis. Ulster Med J. 2019;88(3):25–28.
40. Bolmers MD, de Jonge J, van Rossem CC, van Geloven AA, Bemelman WA. Discrepancies between intraoperative and histological evaluation of the appendix in acute appendicitis. J Gastrointest Surg. 2019. doi:10.1007/s11605-019-04345-3
41. Cho J, Lee D, Sung K, Baek J, Lee J. Clinical implication of discrepancies between surgical and pathologic diagnoses of acute appendicitis. Ann Surg Treat Res. 2017;93(1):43–49. doi:10.4174/astr.2017.93.1.43
42. Correa J, Jimeno J, Vallverdu H, et al. Correlation between intraoperative surgical diagnosis of complicated acute appendicitis and the pathology report: clinical implications. Surg Infect (Larchmt). 2015;16(1).
43. Patel MM, Shah RJ. Impact of histopathological examination of appendix in context to clinical management of patients. Ann Pathol Lab Med. 2017;4(6).
44. Kotisso B, Messele G. Acute appendicitis in Ethiopia. East Afr Med J. 1996;73(4):251–252.
45. Ceresoli M, Zucchi A, Allievi N, et al. Acute appendicitis: epidemiology, treatment and outcomes- analysis of 16544 consecutive cases. World J Gastrointest. 2016;8(10).
46. Barlas SU, Günerhan Y, Palanci Y, Işler B, Çağlayan K. Epidemiological and demographic features of appendicitis and influences of several environmental factors. Turk J Trauma Emerg Surg. 2010;16(1):38–42.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.