Back to Journals » Clinical and Experimental Gastroenterology » Volume 14
Patients’ Experiences and Challenges in Living with Inflammatory Bowel Disease: A Qualitative Approach
Authors Popov J ![]() , Farbod Y, Chauhan U, Kalantar M, Hill L, Armstrong D
, Farbod Y, Chauhan U, Kalantar M, Hill L, Armstrong D ![]() , Halder S
, Halder S ![]() , Marshall JK
, Marshall JK ![]() , Moayyedi P
, Moayyedi P ![]() , Kaasalainen S
, Kaasalainen S
Received 5 February 2021
Accepted for publication 26 March 2021
Published 28 April 2021 Volume 2021:14 Pages 123—131
DOI https://doi.org/10.2147/CEG.S303688
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Wing-Kin Syn
Jelena Popov,1,2 Yasamin Farbod,1 Usha Chauhan,1 Mona Kalantar,1,2 Lee Hill,3 David Armstrong,4 Smita Halder,4 John K Marshall,4 Paul Moayyedi,4 Sharon Kaasalainen5
1Hamilton Health Sciences, Adult Digestive Diseases, Hamilton, Ontario, Canada; 2University College Cork, College of Medicine and Health, Cork, Ireland; 3Department of Pediatrics, McMaster University Medical Centre, Hamilton, Ontario, Canada; 4Department of Medicine (Division of Gastroenterology) and Farncombe Family Digestive Health Research Institute, McMaster University, Hamilton, Ontario, Canada; 5School of Nursing, McMaster University, Hamilton, Ontario, Canada
Correspondence: Jelena Popov
Hamilton Health Sciences, Adult Digestive Diseases, 1280 Main Street West, HSC 3N51H, Ontario, L8S 4K1, Canada
Tel +1-905-521-2100 ext. 73543
Fax +1-905-570-8962
Email [email protected]
Purpose: Inflammatory bowel disease (IBD) significantly impacts patients’ quality of life and imposes a considerable psychological, social, and financial burden. While the relationship between disease activity and quality of life is well established, the subjective challenges of living with IBD are more difficult to assess, and suggestions for improving patient experiences are lacking. The aim of this paper was to explore the various challenges patients encounter in living with IBD and to propose suggestions for overcoming them.
Patients and Methods: This study utilized a qualitative descriptive design with thematic content analysis. Patients were recruited from the Gastroenterology Clinic at McMaster University Medical Centre from December 2014 to April 2015. Data were collected over the course of 5 focus group interviews using a semi-structured interview guide.
Results: Seventeen patients aged 25 to 77 years old (mean age 43 years, SD 17 years) were interviewed. Fifteen patients were diagnosed with Crohn’s disease and 2 patients were diagnosed with ulcerative colitis. Findings were categorized into 18 subthemes which were grouped into 4 broader themes: awareness factor, psychosocial impacts, financial burden, and quality of care.
Conclusion: IBD is associated with complex personal challenges across various demographics. Identifying and meeting the unique needs of individual patients may be achieved through improving communication between patients and their healthcare providers. Family-based education approaches, individualized psychotherapy with therapists familiar with IBD, awareness initiatives addressed to important stakeholders, and patient involvement in community support groups may improve overall IBD care.
Keywords: Crohn’s disease, ulcerative colitis, qualitative, patient burden, psychosocial, quality of care
Introduction
Inflammatory bowel disease (IBD) is a chronic, immune-mediated disorder characterized by recurrent remission and relapse, consisting of Crohn’s disease (CD) and ulcerative colitis (UC).1 This lifelong disease has major impacts on physical and emotional well–being and imposes considerable challenges on managing daily activities.2
The influence of stress on gastrointestinal symptoms was first identified in the 1930s.3 Later research uncovered the association between psychological distress and severity of IBD activity.4 IBD patients have an increased incidence of psychiatric disorders, particularly anxiety and depression.5 Depression is more than twice as common in IBD individuals compared to healthy counterparts6 and significantly impairs quality of life.7 The unpredictable nature of IBD and frequent relapses may further exacerbate the psychological and emotional burden of the disease. Thus, to effectively control disease activity, patients must find enduring coping strategies and make significant lifestyle adjustments.
Considerable financial burdens also accompany this condition.8 The cost burden of IBD has drastically increased over the past two decades as a direct result of new treatment paradigms involving biologics.9 With the growing prevalence of IBD worldwide,10 these psychosocial and financial burdens become a particularly pertinent issue to address.
Social supports play an important role in influencing patients’ perceptions of emotional and psychological stress.11 A previous study assessing patient perspectives of IBD care highlighted the need for increasing public awareness and psychological support in IBD management.12 However, several studies which investigated the efficacy of psychotherapy in improving anxiety, depression, and overall disease course have reported conflicting results.13–15 Despite these findings, follow-up work showed modest patient-perceived improvements in quality of life and mental health, as well as significant interest in pursuing psychotherapy in the future.16 These findings highlight the need to explore more individualized interventions for patients and to integrate these practices into the standard treatment algorithm for IBD.
The purpose of this study was to explore patient experiences in living with IBD and uncover factors that contribute to psychological distress. We also provide suggestions for addressing these challenges and improving overall IBD management.
Patients and Methods
Study Design
This study was conducted in the Gastroenterology Clinic at McMaster University Medical Centre from December 2014 to April 2015 as part of a larger study assessing the feasibility of telemedicine follow–up appointments. Patients who were enrolled in the clinical trial were invited to participate in the focus groups. Purposeful sampling was performed to ensure diversity in participant demographics. Informed consent was obtained by a member of the research team. Patients were provided with parking passes and refreshments on the day of the interview. Full ethics approval was obtained from the Hamilton Integrative Research Ethics Board (Project Number 14-082). Participants consented to the publication of anonymized responses. This study was conducted in accordance with the Declaration of Helsinki.
Qualitative Approach
The study utilized a Qualitative Descriptive (QD) design,17 a method that has been widely used in health care and nursing in order to investigate related phenomena.18 QD design is a particularly important tool for determining key themes in events and experiences, and to gain insights from informants regarding poorly understood phenomena.19 This approach allows researchers to draw from a naturalistic perspective and to examine a phenomenon in its natural state.20
Theoretical Framework
This study utilized two conceptual models to inform the interview question relating to the experiences and perspectives of patients living with IBD. The first model, the Health Belief Model, has been widely used in several contexts for eliciting information on health behaviors relative to an individual’s attitudes and general behaviors.21 It proposes that a person will accept or adopt a certain behavior if they believe that this behavior will result in either a positive consequence or help to prevent a negative one.21 Secondly, we utilized Kleinman’s Explanatory Models22 to provide a framework for exploring the various beliefs used to identify, understand, and react to a health problem, specifically in patients living with IBD.
Data Collection and Analysis
A focus group method was used to capitalize on group interactions and explore patients’ experiences in living with IBD. A total of 5 sessions were led by a trained nursing professor (S.K.) and facilitated by two members of the research team (J.P., Y.F.). To minimize bias, the researchers who were involved in gathering interview data were not involved in the participants’ care. All members involved in conducting the interviews were trained and experienced in qualitative research design. A semi–structured interview guide was used. Available literature at the time of the study was used to inform key areas of questioning which also addressed our research question. The interview guide was modified across the focus groups to better capture patients’ experiences. The following were standard questions for all interviews:
- What has it been like for you to have IBD?
- Sometimes, having IBD can affect an individual emotionally. How does it affect you?
- What are some financial problems you have experienced since your diagnosis?
The duration of the interviews ranged from 60–90 minutes. Interviews were audiotaped, transcribed verbatim, and coded for analysis in NVivo10 QRS International Qualitative Data Management Software.23 Data were coded independently by two members of the research team (J.P., Y.F.), and analysed using qualitative descriptive design with thematic content analysis. Regular meetings were conducted among the investigatory team throughout the analysis phase to review progress iteratively and to ensure non-biased interpretation of the data. In instances of disparity, a consensus was reached through collaborative analysis with four investigators (J.P., Y.F., U.C., S.K.). All members involved in analyzing the interview data were trained and experienced in qualitative research design. Changes were made to the interview guide and codebook to reflect emerging themes throughout the analysis phase. Memoing was performed during each interview and throughout the coding phase to establish unique codes and emerging themes. Upon conclusion of each session, recycling interpretation24 was performed, whereby participants were asked to review a two-page summary of key findings and provide comments relating to the accuracy of the investigators’ interpretations of the interview data.
Demographic data were captured using standardized questionnaires completed by patients on iPads (Apple, Cupertino, CA USA) using LimeSurvey online survey application.25 Demographic data were studied using descriptive analysis and analyzed in SPSS.26
Results
A total of 17 patients ages 25 to 77 (mean 43 years, SD 17 years) were interviewed (Table 1). The mean disease duration was 15 years (SD 8 years). 15 patients were diagnosed with CD and 2 with UC (8 female, 9 male). Most patients (n=15) were on biologics (infliximab, adalimumab), alone (59%) or in combination with other therapies (29%). The most common occupation status was currently employed, constituting less than half of the patient population (41%). The second and third most common occupation statuses included retirement (24%) and disability (18%). More than a third of the patients (41%) had an annual household income of less than $20,000.
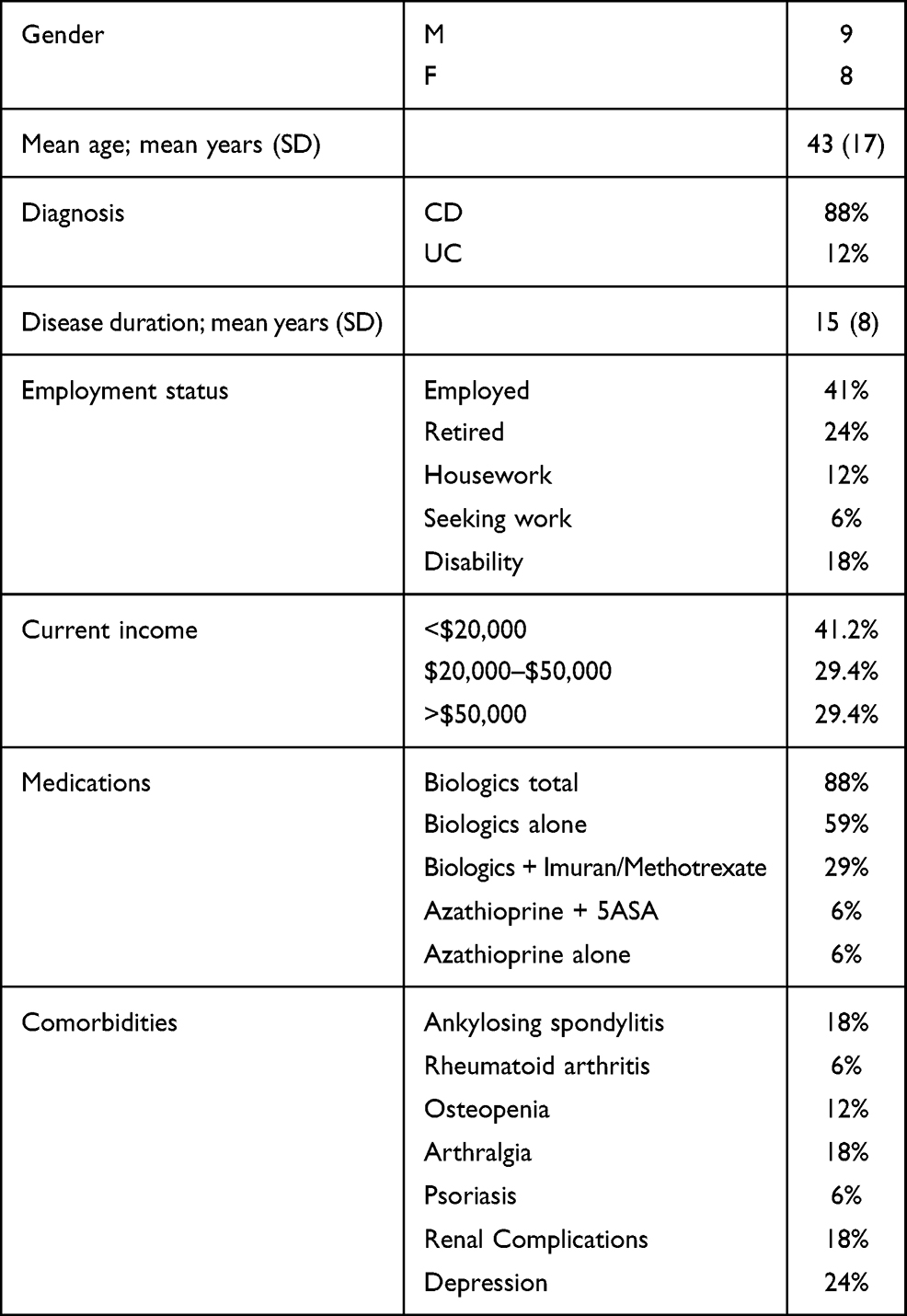 |
Table 1 Participant Demographics |
Participants identified 18 subthemes which were categorized into 4 broader themes: awareness factor, psychosocial impacts, financial burden, and quality of care (Table 2).
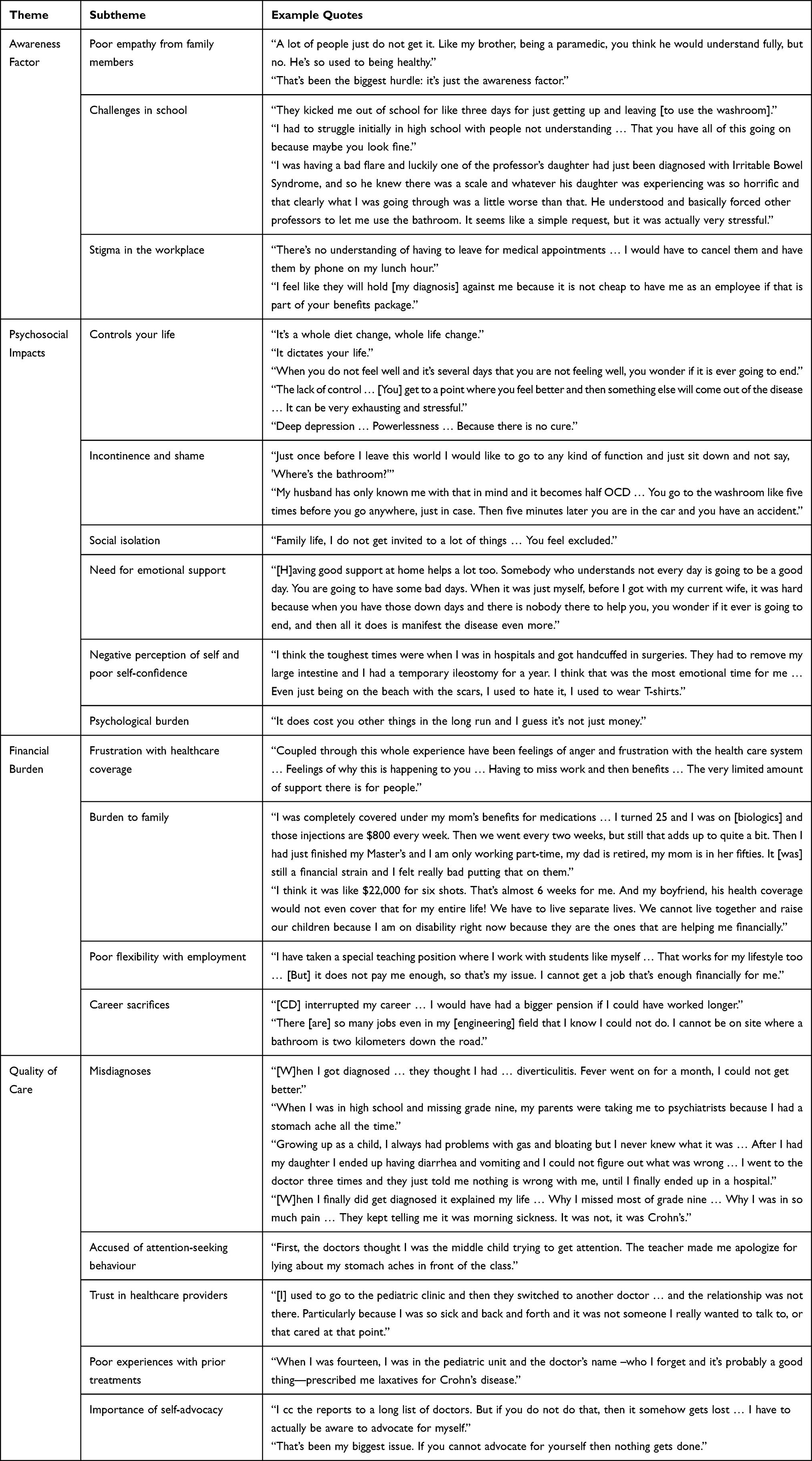 |
Table 2 Emerging Themes from Interviews |
Awareness Factor
The awareness factor was cited by participants as “the biggest hurdle” in living with IBD. This encompassed eliciting empathy and understanding from family members, teachers, and employers. Several participants reported that their family members could not appreciate the extent of their physical pain and fatigue during disease flares. This lack of understanding was cited as an important source of contention within families.
Arranging special accommodations with school and work for frequent restroom access and clinic appointments were also an important source of difficulty. Those who were diagnosed in pediatric ages described challenges in obtaining permission to access restrooms during teaching sessions which caused considerable stress with attending school. In the workplace, several participants described difficulties with employers granting sick days for the purposes of attending clinic appointments. Thus, some participants reported resorting to telephone follow-up appointments during work hours.
Finally, several participants described a fear of disclosing their valuable contributions to community support programs for IBD in job interviews. This was attributed to concerns for raising suspicions of their diagnosis. Most participants felt strongly against disclosing their diagnosis to potential employers as they felt this could negatively impact their ability to be hired due to the cost burden on employee benefits.
Psychosocial Impacts
Psychosocial impacts were the second challenge and referred to feelings of being controlled by the disease, incontinence and shame, social isolation, need for emotional support, poor self-esteem, and the overall psychological burden of the disease.
Psychosocial impacts were often associated with the inability to travel and attend social events due to a fear of incontinence and subsequent embarrassment. Physical pain and persistent fatigue were also cited as important barriers to engaging in social activities. These led to feelings of “powerlessness,” “deep depression,” and alienation from family and friends.
Negative perceptions of self and poor confidence were expressed by most participants. Teenage years were a particularly challenging time as several participants reported developing insecurities from surgical scars and ostomies. These insecurities manifested in the form of avoiding beaches and covering up with clothing.
Emotional supports in the form of family, friends, and intimate partners were endorsed as important factors in managing the overall psychosocial impacts of the disease. Participants who were diagnosed in childhood reported feeling better supported in pediatric clinics due to increased access to social workers and child support workers. Furthermore, most participants reported benefits in participating in community support groups for IBD. However, concerns were raised regarding insufficient access to such resources for adult patients. These personal and community supports were found to be particularly important during initial diagnosis and disease flares.
Financial Burden
Financial burden was the third theme and included frustration with healthcare coverage, guilt associated with costly treatments, poor schedule flexibility with employment, and career sacrifices. The inability to hold fulltime employment, early retirement, and out of pocket expenses gave rise to financial strain. Subsequent strain on marriage and family life were also reported. Participants commonly expressed guilt with their diagnosis and viewed themselves as financial burdens for their families.
Participants also described considerable challenges with pursuing appropriate career paths which met the unique needs of managing their disease. Several participants felt restricted by the limited employment options available which would enable flexible scheduling for clinic appointments and ease of access to restrooms. For most participants, such employment options were part-time and low income. This profoundly affected career choices and instilled feelings of regret due to the inability to actualize preferred career paths.
Feelings of frustration towards the high cost of healthcare and pharmacotherapy were common. For some, the cost of medication came at the expense of living separately from their intimate partners in order to qualify for coverage. Moreover, finding and maintaining fulltime employment with benefits became increasingly difficult with age, long duration of disease, and development of multiple IBD-related comorbidities. Some participants described being forced into early retirement with smaller pensions due to the inability to cope with disease activity, which further increased the financial strain.
Quality of Care
Quality of care was the fourth theme and referred to misdiagnoses, accusations of attention-seeking behaviour, trust in healthcare providers, poor experiences with prior treatments, and the importance of self-advocacy.
A common problem for participants was a long duration from the onset of symptoms to receiving the correct diagnosis. These delays were attributed to accusations of attention-seeking behaviour and poor acknowledgement of symptoms by family members and providers during the initial disease presentation. Most participants reported frustration with frequent initial misdiagnoses and delays in initiating treatment. These experiences instilled feelings of isolation from family, mistrust in providers, and the belief that patients must advocate for themselves in order to receive adequate treatment.
Upon receiving their diagnoses, participants unanimously expressed a sense of relief for having an explanation for their symptoms. Nevertheless, participants felt that most of their challenges in interpersonal relationships stemmed from a lack of understanding among providers and the general public for the difficulties imposed by this chronic condition. Thus, participants continued to be burdened by the ongoing need to self-advocate.
Discussion
The aim of this qualitative study was to explore the impact of IBD on various facets of patients’ lives. The open-ended nature of focus group interviews promoted exploration of opinions and attitudes27,28 relating to the challenges imposed on daily living throughout different stages of life. The greatest challenge in living with IBD was cited by participants as the “awareness factor.” This pertained to a poor understanding of the special needs required by IBD patients. Patients described feelings of “powerlessness,” “deep depression,” shame, and alienation from family and friends. The importance of strong interpersonal supports in managing the psychosocial impacts of the disease were positively endorsed. Feelings of frustration with the financial strain imparted by the disease were common. Finally, participants emphasized the burden and importance of lifelong self-advocacy to ensure satisfactory patient care.
In line with our findings, IBD has been shown to affect patients financially, emotionally, and psychologically.29 The chronic course of the disease imposes difficulties on finding flexible employment, earning livable wages, and obtaining healthcare benefits. Notably, more than a third of the participants in this study had an annual household income of less than $20,000 which was below the poverty line for a three-person household in 2014.30 An association between financial and work-related stress and increased frequency and severity of IBD relapses has previously been reported.31 Thus, patients are often affected by the inability to achieve financial independence.
Previously reported challenges and concerns in living with IBD include fear of treatment side-effects, lack of control over the condition, fear of incontinence, fatigue, low self-esteem, unsatisfactory translation of information between healthcare professionals and patients, poor public knowledge, and fear of stigma.32,33 These findings reflect our own. These lifelong challenges contribute to poorer outcomes, including increased anxiety and depression.34 Thus, increasing IBD awareness and improving educational resources for patients, families, and the general public are clearly needed.
An important suggestion brought forth by our participants was the need to implement more extensive support systems for adults living with IBD. A recent meta-analysis emphasized the current gap in research for assessing patients’ perceptions of the degree of support they receive from healthcare professionals.35 These findings are particularly relevant as physician-patient relational empathy has been shown to correlate with patient anxiety, sleep quality, and inflammatory markers.36 Thus, more research is warranted to determine IBD patients’ perceived levels of support from medical staff and the resulting influence on disease outcomes. This may be particularly relevant in the adult IBD population, as access to social workers and child support workers dwindles upon transitioning from pediatric to adult clinics. Community-based support groups are also useful in alleviating distress associated with initial diagnosis, providing advice on coping strategies, and promoting overall psychosocial benefits through social activities in the form of fundraisers which may provide patients with a sense of purpose.37 Thus, greater emphasis should be placed on promoting patient engagement in support groups and increasing referrals to counsellors as an integral component of the multidisciplinary model of IBD care.
Recent research supported patient interest in pursuing psychotherapy, but cited high out-of-pocket expenses, lack of referral to mental health services by providers, and inadequate familiarity with IBD among therapists as important barriers to such interventions.16 Interestingly, patients of lower socioeconomic standing appear to be more likely to positively endorse psychotherapy.16 This may also reflect our participants’ favorable perception of psychotherapy as more than a third of our patients had an annual income of less than $20,000. Together, these findings may highlight an increased need for counselling services in a subset of patients with a lower annual income.
In response to the concerns raised by our participants, we provide the following suggestions according to their respective themes:
- Awareness Factor: Promoting family-based counselling and IBD education may be particularly important at the time of initial diagnosis. These should include family education, written manuals, and visual materials translated into common languages. This education-based approach may reduce distress associated with the disease, prepare patients and families for unexpected flares in the future, and impart patients with a better knowledge of symptoms to promote early intervention. It may alleviate patients’ anxieties with treatment options, promote active patient engagement in developing a treatment plan, and explore healthcare coverage options through work benefits and government assistance programs. Such endeavors may also increase families’ awareness of the condition and decrease the associated stigma and fear of discrimination among patients.
- Psychological Impacts: Individualized psychotherapeutic interventions may be improved by increasing familiarity among therapists of the unique needs of IBD patients. Therapy sessions should strive to explore individual patient challenges in school, the workplace, and personal life. Interventions may include arranging special accommodations in the form of written letters or direct communication with teachers and employers of affected patients. Establishing enduring coping skills would also be an important component. Finally, providers would need to incorporate referrals to such services as a standard component of IBD care.
- Financial Burden: Increasing public awareness of the disease through various support groups and community fundraisers may reduce stigma associated with the disease, provide financial resources to subsidize costly treatments, and reduce patients’ feelings of guilt associated with financial strain. Education and awareness initiatives may also be addressed to employers, insurance companies, and ministries of health.
- Quality of Care: Improving interactions between patients and healthcare providers may be achieved through increasing awareness and education among physicians, nurses, and allied health professionals. The importance of patient support systems should be emphasized at all levels of patient care.
Limitations to this study included a small sample size compared to previous qualitative IBD studies as we were limited by the number of patients enrolled in the larger trial. Nevertheless, we were able to achieve data saturation for the themes reported in this manuscript.38 Our study population was disproportionately more affected by CD than UC. Thus, we were unable to make inferences based on disease phenotype. Finally, while focus groups are the preferred interview design for facilitating in-depth exploration of particular phenomena, generating group debate, and ensuring accurate interpretation of data through group feedback, they are not suitable formats for performing statistical analyses or generating frequencies of emerging subthemes.39 Thus, we were unable to organize our themes according to frequency of participant citation. However, the goal of this study was not to achieve consensus but rather diversity of patient perspectives and experiences.
Strengths included purposeful sampling of our study population which ensured an equal sex distribution, a broad range of ages, a long duration of diagnosis, various employment statuses, and multiple comorbidities. Despite more than a third of our participants having less than $20,000 annual income, other income brackets were also represented. Thus, our findings are unlikely to be biased by particular socio-cultural circumstances or influenced by gender-based constraints.
The challenges associated with living with IBD reported herein underscore the need for increasing patient supports. Improvements should be made to increase educational resources for patients and their families in order to facilitate the implementation of suitable lifestyle adjustments and to provide appropriate supports. Healthcare providers must strive to incorporate methods of effectively addressing the restraints imposed by the disease with school boards and employers by seeking flexibility from such institutions as necessitated by flares and follow-up appointments. Family-based education approaches, individualized psychotherapy, education and awareness initiatives addressed to the aforementioned stakeholders, and expansion of community support groups are required for improving overall IBD care.
Conclusion
This study informs the multifaceted impact of IBD on daily living. Several themes were common among our patients irrespective of age, gender, or other demographic differences. Main challenges were associated with a lack of public awareness of the disease, psychosocial impacts in the form of social isolation and shame, financial burdens and career sacrifices, and room for improving the quality of IBD care. With the identification of these burdens, more focused interventions may be implemented to improve patient quality of life and overall IBD management.
Disclosure
This study was supported by the Health Professional Investigator (HPI) operating grant from Hamilton Health Sciences (Grant # HPI-12009). Mrs Usha Chauhan reports grants from Hamilton Health Sciences, during the conduct of the study; personal fees from Pfizer, personal fees from Janssen, personal fees from AbbVie, personal fees from Takada, outside the submitted work. The authors declare that they have no other conflicts of interest.
References
1. Cooper J, Collier J, James V, Hawkey C. Beliefs about personal control and self-management in 30–40 year olds living with inflammatory bowel disease: a qualitative study. Int J Nurs Stud. 2010;47(12):1500–1509. doi:10.1016/j.ijnurstu.2010.05.008
2. Farrell D, McCarthy G, Savage E. Self-reported symptom burden in individuals with inflammatory bowel disease. J Crohns Colitis. 2016;10(3):315–322. doi:10.1093/ecco-jcc/jjv218
3. Sajadinejad M, Asgari K, Molavi H, Kalantari M, Adibi P. Psychological issues in inflammatory bowel disease: an overview. Gastroenterol Res Pract. 2012;2012:106502. doi:10.1155/2012/106502
4. Marrie R, Graff L, Fisk J, Patten S, Bernstein C. The relationship between symptoms of depression and anxiety and disease activity in IBD over time. Inflamm Bowel Dis. 2021;izaa349. doi:10.1093/ibd/izaa349
5. Bannaga A, Selinger C. Inflammatory bowel disease and anxiety: links, risks, and challenges faced. Clin Exp Gastroenterol. 2015;8:111–117. doi:10.2147/CEG.S57982
6. Mikocka-Walus A, Turnbull D, Moulding N, Wilson I, Andrews J, Holtmann G. Controversies surrounding the comorbidity of depression and anxiety in inflammatory bowel disease patients: a literature review. Inflamm Bowel Dis. 2007;13(2):225–234. doi:10.1002/ibd.20062
7. Zhang C, Hewett J, Hemming J, et al. The influence of depression on quality of life in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2013;19(8):1732–1739. doi:10.1097/MIB.0b013e318281f395
8. Bloomfeld R, Bickston S. Financial toxicity in people with inflammatory bowel disease. Inflamm Bowel Dis. 2020;izaa267. doi:10.1093/ibd/izaa267
9. Jonathan B, Benjamin C. The burden of cost in inflammatory bowel disease: a medical economic perspective. Curr Opin Gastroenterol. 2020;36(4):310–316. doi:10.1097/MOG.0000000000000642
10. Kaplan G, Ng S. Understanding and preventing the global increase of inflammatory bowel disease. Gastroenterol. 2017;152(2):313–321. doi:10.1053/j.gastro.2016.10.020
11. Sewitch M, Abrahamowicz M, Bitton A, et al. Psychological distress, social support, and disease activity in patients with inflammatory bowel disease. Am J Gastroenterol. 2001;96(5):1470–1479. doi:10.1111/j.1572-0241.2001.03800.x
12. Vutcovici M, Sewitch M, Kachan N, et al. Patient perspectives of IBD care and services: an integral part of a pan-Canadian quality improvement initiative. J Can Assoc Gastroenterol;2021. gwaa044. doi:10.1093/jcag/gwaa044
13. Knowles S, Monshat K, Castle D. The efficacy and methodological challenges of psychotherapy for adults with inflammatory bowel disease: a review. Inflamm Bowel Dis. 2013;19(12):2704–2715. doi:10.1097/MIB.0b013e318296ae5a
14. Mikocka-Walus A, Bampton P, Hetzel D, Hughes P, Esterman A, Andrews J. Cognitive-behavioural therapy for inflammatory bowel disease: 24-month data from a randomised controlled trial. Int J Behav Med. 2016;24(1):127–135. doi:10.1007/s12529-016-9580-9
15. McCombie A, Mulder R, Gearry R. Psychotherapy for inflammatory bowel disease: a review and update. J Crohns Colitis. 2013;7(12):935–949. doi:10.1016/j.crohns.2013.02.004
16. Craven M, Quinton S, Taft T. Inflammatory bowel disease patient experiences with psychotherapy in the community. J Clin Psychol Med Settings. 2019;26(2):183–193. doi:10.1007/s10880-018-9576-5
17. Doyle L, McCabe C, Keogh B, Brady A, McCann M. An overview of the qualitative descriptive design within nursing research. J Res Nurs. 2020;25(5):443–455. doi:10.1177/1744987119880234
18. Kim H, Sefcik J, Bradway C. Characteristics of qualitative descriptive studies: a systematic review. Res Nurs Health. 2017;40(1):23–42. doi:10.1002/nur.21768
19. Neergaard M, Olesen F, Andersen R, Sondergaard J. Qualitative description - the poor cousin of health research? BMC Med Res Methodol. 2009;9(1):52. doi:10.1186/1471-2288-9-52
20. Sandelowski M. What’s in a name? Qualitative description revisited. Res Nurs Health. 2010;33(1):77–84. doi:10.1002/nur.20362
21. Janz N, Becker M. The health belief model: a decade later. Health Educ Q. 1984;11(1):1–47. doi:10.1177/109019818401100101
22. McSweeney J, Allan J, Mayo K. Exploring the use of explanatory models in nursing research and practice. Image J Nurs Sch. 1997;29(3):243–248. doi:10.1111/j.1547-5069.1997.tb00992.x
23. QSR International Pty LTD. NVivo qualitative data analysis Software Version 10; 2012.
24. Crabtree B, Miller W. Doing Qualitative Research. Thousand Oaks, Calif.: Sage Publications; 1999:406.
25. Schmitz C; LimeSurvey Project Team. LimeSurvey: an open source survey tool. Germany: LimeSurvey Project Hamburg; 2015.
26. IBM Corp. IBM SPSS statistics for Windows, Version 23.0. Armonk, NY: IBM Corp; Released 2015.
27. Kiltzinger J. Qualitative research: introducing focus groups. BMJ. 1995;311(7000):299–302. doi:10.1136/bmj.311.7000.299
28. Basch C. Focus group interview: an underutilized research technique for improving theory and practice in health education. Health Educ Quart. 1987;14(4):411–448. doi:10.1177/109019818701400404
29. Kemp K, Griffiths J, Lovell K. Understanding the health and social care needs of people living with IBD: a meta-synthesis of the evidence. World J Gastroenterol. 2012;18(43):6240–6249. doi:10.3748/wjg.v18.i43.6240
30. Lammam C, MacIntyre H. An Introduction to the State of Poverty in Canada. Fraser Institute; 2016.
31. Sun Y, Li L, Xie R, Wang B, Jiang K, Cao H. Stress triggers flare of inflammatory bowel disease in children and adults. Front Pediatr. 2019;7:432. doi:10.3389/fped.2019.00432
32. Fourie S, Jackson D, Aveyard H. Living with inflammatory bowel disease: a review of qualitative research studies. Int J Nurs Stud. 2018;87:149–156. doi:10.1016/j.ijnurstu.2018.07.017
33. Kemp K, Griffiths J, Campbell S, Lovell K. An exploration of the follow-up up needs of patients with inflammatory bowel disease. J Crohns Colitis. 2013;7(9):e386–95. doi:10.1016/j.crohns.2013.03.001
34. Mikocka-Walus A, Hanlon I, Dober M, et al. Lived experience in people with inflammatory bowel disease and comorbid anxiety and depression in the United Kingdom and Australia. J Health Psychol. 2020;1359105320911427.
35. Byron C, Cornally N, Burton A, Savage E. Challenges of living with and managing inflammatory bowel disease: a meta-synthesis of patients’ experiences. J Clin Nurs. 2020;29(3–4):305–319. doi:10.1111/jocn.15080
36. Xu X, Zhang Y, Wang W, Zhang Y, Yang N. Effects of patients’ perceptions of physician-patient relational empathy on an inflammation marker in patients with Crohn’s disease: the intermediary roles of anxiety, self-efficacy, and sleep quality. Psychol Res Behav Manag. 2020;13:363–371. doi:10.2147/PRBM.S221435
37. Cable M. The role of patients’ organizations. Int Disabil Stud. 1988;10(4):181–182. doi:10.3109/09638288809164078
38. Guest G, Bunce A, Johnson L. How many interviews are enough?: an experiment with data saturation and variability. Field Methods. 2006;18(1):59–82. doi:10.1177/1525822X05279903
39. Nyumba T, Wilson K, Derrick C, Mukherjee N. The use of focus group discussion methodology: insights from two decades of application in conservation. Methods Ecol Evol. 2018.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.