Back to Journals » Patient Preference and Adherence » Volume 10
Patients' management of type 2 diabetes in Middle Eastern countries: review of studies
Authors Alsairafi ZK, Taylor KM ![]() , Smith FJ, Alattar AT
, Smith FJ, Alattar AT
Received 15 January 2016
Accepted for publication 24 March 2016
Published 10 June 2016 Volume 2016:10 Pages 1051—1062
DOI https://doi.org/10.2147/PPA.S104335
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Zahra Khalil Alsairafi,1 Kevin Michael Geoffrey Taylor,2 Felicity J Smith,1 Abdulnabi T Alattar3
1Research Department of Practice and Policy, 2Department of Pharmaceutics, School of Pharmacy, University College of London, London, UK; 3Diabetes Unit, Al-Amiri Hospital, Ministry of Health, Safat, Kuwait
Abstract: The increased prevalence of diabetes in Middle Eastern countries is a health policy priority. Important risk factors for diabetes have been identified. Lifestyle interventions and adherence to medications are central to disease prevention and management. This review focuses on the management of type 2 diabetes mellitus in Middle Eastern countries. The aim is to identify the ways in which knowledge, health beliefs, and social and cultural factors influence adherence to medication and lifestyle measures. Thirty-four studies were identified following a systematic search of the literature. The studies describe the influence of knowledge, health beliefs, culture, and lifestyle on the management of type 2 diabetes mellitus in the Middle East. Findings indicate a lack of health knowledge about diabetes among populations, which has implications for health behaviors, medication adherence, and treatment outcomes. Many identified health beliefs and cultural lifestyle factors, such as religious beliefs, beliefs about fasting during Ramadan, and sedentary lifestyles played a role in patients’ decisions. For better management of this disease, a collaborative approach between patients, their families, health care professionals, and governments should be adopted. Implementing behavioral strategies and psychological interventions that incorporate all health care professionals in the management process have been shown to be effective methods. Such services help patients change their behavior. However, the utilization of such services and interventions is still limited in Arabian countries. Physicians in the Middle East are the health care professionals most involved in the care process.
Keywords: type 2 diabetes mellitus, adherence, health beliefs, lifestyle, Ramadan, diet
Introduction
Diabetes mellitus (DM) is a leading cause of death in industrialized and developing countries. In the Middle East, DM is a rapidly growing chronic disease. Saudi Arabia, Kuwait, Qatar, and Egypt are among the ten countries in the world with the highest prevalence of DM. Major contributory factors for type 2 diabetes mellitus (T2DM), which is most prevalent in Middle Eastern countries, include low activity levels, poor diet, and excess body weight.1 Lack of health awareness, health beliefs, attitudes, and lifestyle are all contributing to the rising prevalence of obesity and DM in the Middle East.2 In particular, lack of awareness about nutritional information and the significance of healthy eating have led to adoption of a poor diet.3,4 Social and economic changes are also important. These include changing lifestyles in terms of urbanization and changing dietary habits. Increased wealth resulting from oil production has enabled widespread car ownership. As a consequence, there is decreased physical activity along with rising levels of obesity and smoking.5–9
Many people in the Middle East have been found not to appreciate the potential seriousness of diabetes, its complications, or early detection signs.10 Patients’ beliefs influence their uptake of lifestyle measures and their use of medicines. Adherence refers to “the extent to which a person’s behavior: taking medication, eating a suitable diet, and/or executing lifestyle changes correspond with agreed recommendations from a healthcare provider”.11 Adherence was found to be low among Middle Eastern populations. In particular, studies have estimated medication nonadherence rates for diabetes to be 68% or lower.12–14 The main reasons for patients’ nonadherence were forgetfulness, confusion about the required duration for using medication, and disbelief about the overall effectiveness of the medication.15
The aim of this review is to identify ways in which knowledge, health beliefs, and culture influence adherence to medication and lifestyle measures for T2DM patients in Middle Eastern countries. In addition, this review aims to outline all the determinants of patients’ behavior to assist researchers to further investigate further the issues identified or to identify new ones. In addition, this review will assist in identifying policy implications and propose recommendations to enhance the management of this disease in the region and subsequently improve health outcomes.
Methods
Search terms and search strategy
A systematic search of studies relating to medicines use and medication adherence in diabetes in the Middle East was performed using the following databases: EMBASE, PubMed, Web of Science, and Index Medicus for the Eastern Mediterranean Region; the search was selected for the period from 1990 to 2015. The search terms were (diabetes AND adherence or compliance AND medicine use AND Middle East OR Kuwait OR United Arab Emirates OR Saudi Arabia OR Bahrain OR Qatar OR Oman OR Jordan OR Egypt OR Lebanon OR Syria OR Iraq OR Iran OR Palestine OR Israel OR Turkey OR Libya), with or without the combination of the search terms (health beliefs, lifestyle, patient behavior, insulin). Studies that discussed medicine use during the holy month of Ramadan were searched using the search terms (Ramadan fasting AND diabetes mellitus). In addition, the Google search engine was used to identify clinical journals in Middle Eastern areas. These journals were searched for relevant papers, and the bibliographies of relevant papers were hand searched for further articles. In addition, an expert in diabetes in the area was contacted to help in identifying relevant articles.
Inclusion or exclusion criteria
The electronic database search yielded 834 studies, and further studies were identified from other sources, such as contact with an expert (n=1), searching reference list (n=3), and using Google search engine (n=10). Removing duplicates resulted in a total of 822 studies. Titles and abstracts were evaluated to determine eligibility for full screening. Studies that employed acceptable quantitative and/or qualitative methods, including randomized controlled trials, observational studies (eg, cross-sectional, experimental, and interventional), and review articles were included. All studies wherein adherence to medicines and/or other management behaviors and/or lifestyle measures among adults with diabetes in Middle Eastern countries were explored were eligible for inclusion. In addition, studies that focused on prevention and/or management of the condition in the region and associated factors were eligible. The inclusion criteria required that the study population be adults (18 years and older) with diabetes and from a Middle Eastern country. Studies that involved all sexes and ethnicities, urban and rural, residents and expatriates, and all socioeconomic and educational backgrounds were included. In addition, the review included studies at different health care levels. Overall, 34 studies were classified as appropriate for full review. Eight studies were excluded due to unavailability of full access to the study (n=3), the quality of the study (n=3), or due to inclusion of irrelevant subjects, eg, pregnant women, who have distinct needs (n=2). The summary of the literature search procedure is illustrated in Figure 1.
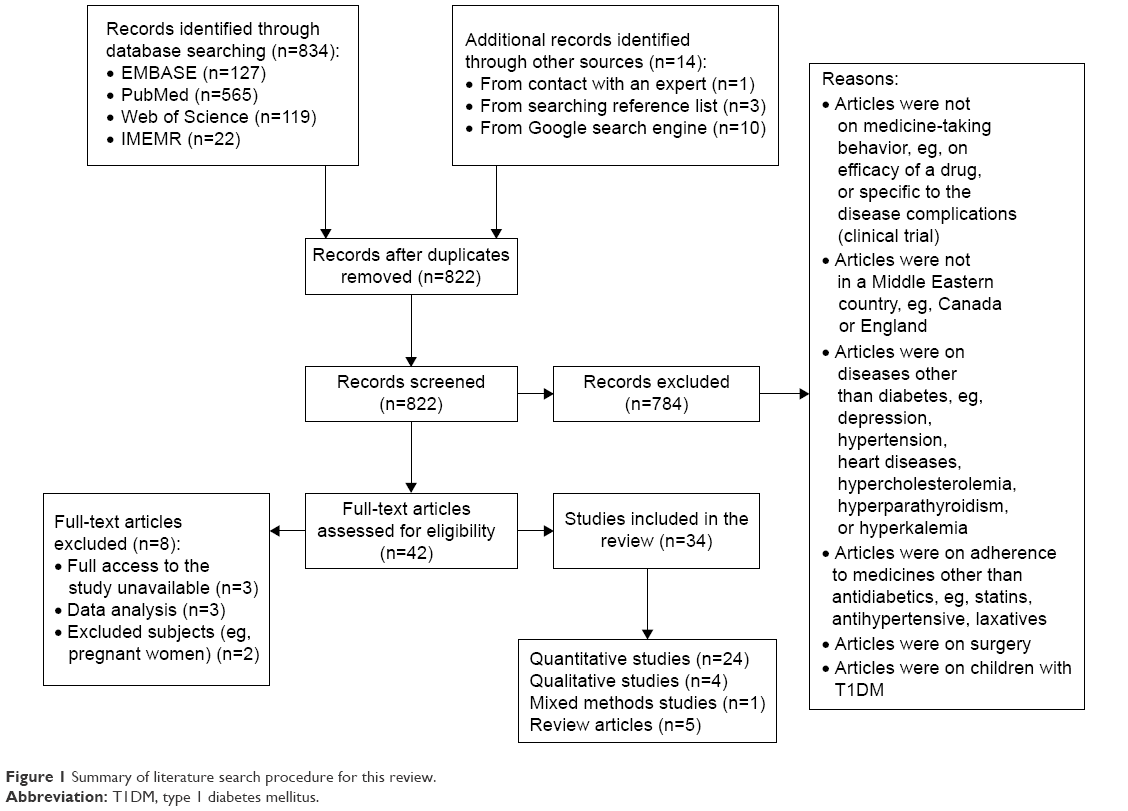 | Figure 1 Summary of literature search procedure for this review. |
Data extraction or quality assessment processes
Once all relevant studies had been identified, full-text manuscripts were retrieved in hard copy for assessment. Information was extracted into a pro forma that included primary author’s name, date of publication, setting, country of study, number of participants, study design and the main study findings regarding the possible determinants of medicine-taking behavior among patients with DM in the Middle East, and sociocultural factors relevant to the prevalence and management of T2DM in the region (Table 1). This enabled identification of papers that addressed specific topics and issues relevant to the study objectives, and facilitated the retrieval of information.
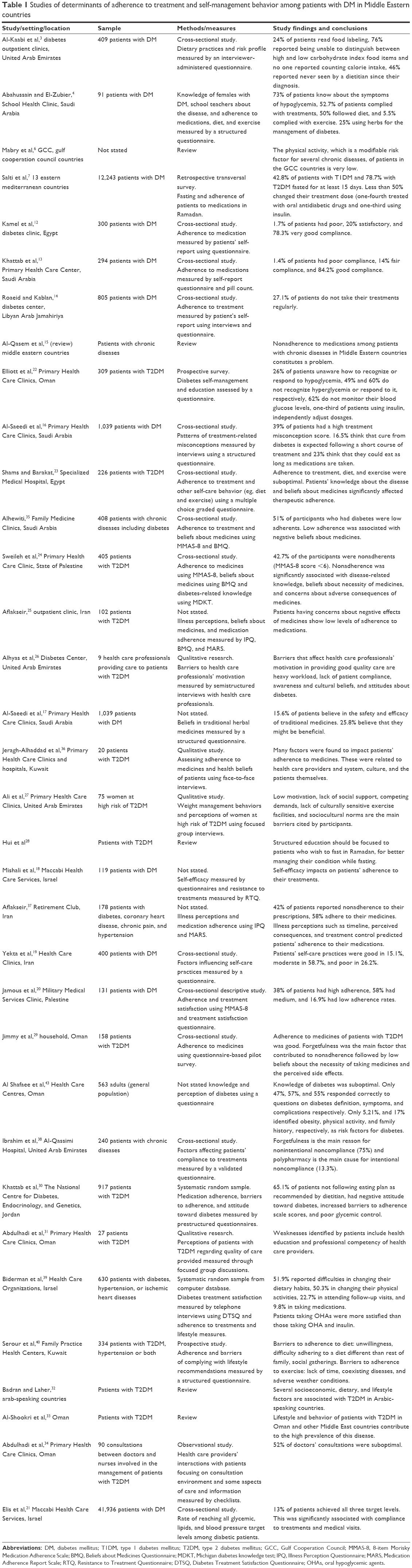 | Table 1 Studies of determinants of adherence to treatment and self-management behavior among patients with DM in Middle Eastern countries |
The quality of each study was assessed using checklists adapted from the Critical Appraisal Skills Program. The authors of this article undertook all stages of identification, review of papers, and analysis. Any disagreements were resolved through regular meetings and discussions.
Results
A total of 34 studies were identified from all regions of the Middle East: Kuwait (two studies), Iran (three), Saudi Arabia (five), Turkey (one), Palestine (two), Israel (three), Jordan (one), Oman (five), Libyan Arab Jamahiriya (one), Egypt (two), and United Arab Emirates (four). Three studies were across Middle Eastern countries, and one study focused on the Gulf Cooperation Council countries.
Of these 34 studies, 13 discussed issues related to T1DM and T2DM,3,4,7,12–14,16–21,43 while 14 focused on T2DM only.22–34,36 Six of the studies addressed other long-term diseases alongside diabetes,15,35,37–40 and one focused on lifestyle issues and obesity.6 All the studies were conducted among adult populations (≥18 years of age). The settings of the research studies were primary health care centers (n=8), hospitals (n=4), diabetes centers/clinics (n=10), a retirement club (n=1), household (n=1) and a school health clinic (n=1). Settings of some studies (n=5), other than the reviews (n=5), were not stated (n=1). The sample sizes of the reviewed studies ranged from 91 to 41,936 participants for the quantitative studies and from 9 to 75 participants for the qualitative studies (Table 1).
Most studies (n=24) employed survey methods to collect data and applied quantitative analytical procedures to explore the determinants of patients’ medicine-taking behavior, such as health awareness and beliefs. Only four studies applied qualitative methods (focus groups and interviews).26,27,31,36 These studies investigated factors that affected patients’ management behaviors from the perspectives of patients themselves (n=2) and from the perspectives of health care professionals (n=2). One study combined quantitative and qualitative methods (questionnaires and interviews).12 All of the studies were original articles except five, which were reviews.6,15,28,32,33
Lack of health awareness about diabetes and its management
Knowledge is a prerequisite of preventive health behavior and may motivate patients to take actions for treating their diabetes.12,22,41 Patients with T2DM need to understand their disease and how to treat it, as they are responsible for their daily control behavior.42 Many studies have discussed the knowledge of patients with diabetes in the Middle East. Poor knowledge and lack of health awareness about the proper management of the disease, and its seriousness, were reported in all studies. For example, one study reported that patients had poor knowledge about the effects of diabetes on the eye and kidney. Also, it has been found that patients lack the awareness about the symptoms of hypoglycemia and its treatment.14 Another study revealed that a significant proportion of people had no information regarding preventive measures needed to cope with diabetes.43 One study noted that a substantial proportion of patients did not mention any signs of abnormal glucose levels, nor knew how to detect hypoglycemia.22 Kamel et al,12 in Egypt, found the majority of patients had poor knowledge about diabetes, its complications, and how to control it. Another study reported that patients believed that diabetes would be cured after a short course of treatment. In that study, the patients believed that they could eat whatever they wanted as long as medicines were taken.16
Health awareness and medicines use
In five studies, patients demonstrated better adherence to treatment when they received sufficient information about the disease and its complications, medicines, and dosage.12,16,23,24,35 Moreover, patients who believed that diabetes would last a long time had better medication adherence.25
Some studies have shown that poor knowledge of diabetes and its potential consequences discourages patients from adhering to their therapeutic regimens. Such studies found that patients may use herbs to control their diabetes while abstaining from their conventional treatment.4,17,26–36 In addition to the use of herbs, poor awareness about how to manage the disease led to actions that potentially affected glycemic control. For example, Roaeid and Kablan14 reported that some patients omitted their evening insulin doses, did not store insulin in a refrigerator or did not shake it before use, did not routinely change the injection site, and used insulin syringes more than once.
A study by Elliott et al22 found that some patients were unable to distinguish between hypo- and hyperglycemic attacks and consequently were practicing potentially problematic actions such as increasing their doses of oral antidiabetic medicines or insulin or going to sleep when experiencing hypoglycemia and drinking juice or eating sour food when having hyperglycemia.
Health awareness and self-care behavior
In patients with diabetes, health awareness is an important determinant of health behavior.12 For example, patients’ understanding of hypertension as a diabetic complication motivated them to have regular blood pressure checks. Knowledge about retinopathy and foot ulcers was associated with patients’ attendance at eye screenings and foot checkups.14
Self-monitoring of blood glucose levels and responding to hypo- and hyperglycemic episodes are an integral part of the management of diabetes by insulin. Only a small proportion of patients have been found regularly to monitor their blood glucose levels. Reasons included not understanding its importance, not knowing how to do it, or lacking the desire to do so. In addition, it was found that some patients did not know that they could buy monitoring devices themselves and believed that these were only sold to health care professionals.22,23 A study by Elliott et al22 revealed hazardous practices undertaken by patients in controlling their disease, by responding poorly to its complications. For example, the authors reported that patients used to drink juice or eat sour food to counteract their hyperglycemia. Other practices that could be hazardous were not being able to recognize hypoglycemia, ignoring and not responding to it once detected, or going to sleep.
Health awareness and lifestyle
Ali et al27 in their qualitative study reported that some participants did not know how to cook healthy food. Others needed a program that helped them lose and maintain weight.27 Al-Kaabi et al3 reported that patients with DM could not count their calorie intake, and only a small proportion of them read food labeling. The majority of patients were also unable to distinguish between low and high carbohydrate index food items.3 In Saudi Arabia, most women with DM were unaware of the importance of diet and exercise to control their disease, and they were overweight or obese.4
Health beliefs and their impact on patients’ behavior
Patient adherence to treatment is significantly affected by health beliefs. It is postulated that there is a relationship between beliefs and behavior.26 Psychologists have studied this relationship extensively. The use of sociopsychological approaches has revealed that health beliefs impact on patients’ medicine-taking behavior.44 Vermeire et al45 have noted that patients with DM might deliberately choose not to adhere to their medicines as a result of their beliefs. An explanation for some of these beliefs, which are specific to the Middle Eastern population, will now be discussed.
Religious beliefs
Despite the cultural diversity among the population of Middle Eastern countries, Islam is the most practiced religion in the region. Since Muslims comprise the dominant portion of the Middle Eastern population, medical practices are based on Islamic beliefs. Religious beliefs hold that death is part of God’s plan. Consequently, ensuring patients appreciate the seriousness and urgency of making lifestyle changes and taking appropriate actions is challenging. Patients’ management of their diabetes will be influenced by their religious beliefs, including “fatalism”. Fatalism refers to a belief that “events are controlled and predetermined by Allah and that humans have little, if any, control over their destinies”. Severe untreated cases of diabetes can lead to death, and there are verses of the Holy Quran and prophet’s sayings that stress disease prevention and treatment. Despite this fact, religious beliefs and strong faith in God’s control may discourage patients from engaging in activities that are against God’s will.17 In this regard, Jeragh-Alhaddad et al36 found that many patients believed that only God can cure diabetes and not doctors or medicines.
Beliefs about fasting during Ramadan
In Ramadan, when people are obliged to abstain from eating and drinking between sunrise and sunset, patients with diabetes change their medicine-taking behavior without consulting their doctors.28,46 A study by Salti et al7 revealed that 20% of patients using oral antidiabetic medicines and 37% of patients using insulin changed their doses during Ramadan. Patients reported that they reduced their oral doses because they believed that while they were not eating traditional foodstuffs, they did not need to take their medicines.7 Lawton et al47 reported that some patients believed that taking their medicines without eating several large meals would further reduce their blood glucose levels and expose them to more side effects.
Self-beliefs
Self-efficacy, which refers to patients’ beliefs in their ability to change and succeed, has been described in two studies. In one study, it was noted that self-efficacy was significantly associated with patients’ adherence to treatment recommendations. Patients who had lower self-efficacy showed higher resistance to treatment recommendations and consequently lower adherence to oral medications.28 Patients who perceived that they had control over their condition and medicines better adhered to their therapeutic regimens.37 On the other hand, beliefs in the efficacy of self-care practices, such as undertaking sufficient levels of physical activity and controlling dietary intake, encouraged patients not to adhere to medicines.19
Beliefs about efficacy and necessity
Jamous et al20 and Alhyas et al26 concluded that beliefs regarding the balance of necessity and efficacy against costs and risks were influential. Patients who believed in the necessity of taking medicines were more likely to be adherents.23,24,35,29 On the other hand, patients who perceived medicines to be ineffective and those with longer duration of diabetes and more complications were least likely to adhere to their treatments.13,25,30,37,38 Consequently, low cure beliefs affected patients’ health outcomes, such as psychological well-being, recovery, survival, and treatment-related behavior (eg, adherence).48 Conversely, some studies have described ways in which confidence about the efficacy of medicines may negatively impact on other aspects of diabetes management. For example, patients who believed that T2DM could be managed with drugs did not spend time with their health care professionals to discuss other important management behaviors.26
Belief in the health care provider
A study by Abdulhadi et al31 highlighted some weaknesses in the patient–provider interaction from the perspectives of patients. The weaknesses were mainly related to the communication skills of the health care providers. Patients were hindered from participating in the management process, which resulted in their dissatisfaction with the services provided. The patients reported some barriers to good diabetes management, such as a lack of continuity of care and inexperienced health care providers. The study has revealed that patients who continued their care with one primary care provider had better adherence to appointments and treatments. Consequently, these patients achieved glycemic control. Patients preferred to be seen by the same doctor because they believed that they would get better advice regarding their problems. Moreover, some patients perceived that continuity of care with the same health care provider was a salient element in building their confidence and improving their relationship with doctors.31 Another study reported that some patients lacked trust in the government health care system, turning to the private sector to receive better care. In this study, patients reported unavailability of medicines, discontinuity of care, doctors’ paternalism, and inequalities of services provided as barriers to better management of diabetes.36 Aflakseir37 concluded that a weak relationship between doctor and patient was associated with medication nonadherence. Patients’ lack of belief in the competence of doctors and nurses also significantly impacted health outcomes.37 Reduced levels of trust in the scientific medical knowledge of health care professionals other than specialists led to poor adherence to appointments and oral antidiabetic medication.26,31,39
Lifestyle and diabetes
Physical activity
Several social environmental barriers have been identified as contributing to low physical activity levels. For example, households in the Middle East (especially Saudi Arabia, Qatar, and Kuwait) have a common practice of employing maids, which reduces physical activity expended for domestic chores.39 This was highlighted in a qualitative study, where participants attributed their increased weight to their dependence on housemaids.27 Patients with T2DM in Kuwait identified lack of time, coexisting diseases, extreme weather conditions, the abundance of maids, and excessive use of cars as barriers to engagement in recommended levels of physical activity.40 Badran and Laher32 noted that after marriage, couples become less active and consume more food during cultural joint meals. Also, it has been claimed that cultural barriers restrict women’s access to outdoor activities; the availability of culturally acceptable exercise facilities is limited and expensive.2,27 There are also some traditional cultural expectations that couples will have a high number of children, which means high fertility rates in women and short periods between pregnancies. This may further limit their opportunities for physical activity and increases their chances of obesity.2
Dietary habits
Dietary habits have undergone dramatic changes in the last 30 years, with low dietary fiber and high-fat intake leading to obesity and DM in the Middle East.32 Serour et al40 reported barriers to following a healthy diet. These include lack of desire, stress, type of traditional food, difficulty in adhering to a diet that is different from other family members, and the high frequency of social gatherings.40 In addition, in Arab-speaking countries, the social processes of gatherings require consumption of mainly meat, fat, rice, and carbohydrates.32 Hospitality and generosity are important Islamic values, whereby individuals wish to serve and encourage guests to consume large amounts of food as a sign of friendliness and demonstration of honor. Guests may find it difficult to refuse food, which might be interpreted as a sign of illness or low ingratitude.27,49 Additionally, in some Middle Eastern countries, especially the Gulf Cooperation Council countries, people strongly believe in the nutritional and economic value of dates. Consequently, they consume dates frequently with coffee during the day as part of their culture. Consumption of large quantities of dates may affect glycemic control of patients with DM due to their high sugar content.26,31,33
Discussion
The findings of this review indicate that the problem of nonadherence to treatment is prevalent among patients with T2DM in the Middle East. This review has investigated the determinants of such patients’ behavior in order to propose services and recommendations targeted at those determinants. This should help in counteracting such behavior and lead to improved health outcomes in the region. The review revealed that lack of health awareness, health beliefs, and culture have a significant influence on patients’ adherence to treatment and lifestyle measures. Different methodologies were employed to obtain the results of the reviewed studies. Most studies used questionnaires to collect data, whereas few studies applied interviews and focus groups. All the reviewed studies were conducted with adult patients with DM (predominantly T2DM). One study was conducted with participants at high risk of T2DM and two studies were conducted with health care professionals.
Lack of health awareness is common among patients with DM in the Middle East. It has been found that patients lacked an awareness of the seriousness of diabetes.12,14,16,22–24,35,36,43 In addition, this poor awareness was associated with different practices, such as the use of herbs instead of conventional treatment, and stopping or taking less medication to avoid adverse effects.17,26,36 Also, lack of health awareness of the role of diet and exercise led to difficulties in weight management and obesity.3,4,27 Some specific beliefs of the Middle Eastern population were also identified in this review. Examples of these beliefs are religious beliefs in God’s control and in the “evil eye”, beliefs about fasting in Ramadan, self-belief, and beliefs about necessity of treatment and in health care providers. From the studies that discussed these beliefs, it was conspicuous how these beliefs impacted patients’ behavior and the management of diabetes.7,13,18,19,23–25,29,31,35,39,47–49,50 Cultural factors that were found to influence patients’ behavior were also identified. It was found that culture impacted adherence to lifestyle measures, such as diet and physical activity, and led to high obesity rates in the region and consequent poor health outcomes.2,32,39,40,48
Enhancing educational efforts by health care professionals to improve patients’ health awareness, modify health beliefs, and address sociocultural factors should play a major role in improving patients’ behavior. Improving patients’ medicine use and other management responsibilities will improve the management of T2DM in the region and also improve health outcomes. In addition, enhancing patients’ trust in the quality of the health care services is important. This could be achieved by implementing strategies for assessing and improving the quality of the health care services provided.24,26,51 Also, at the governmental level, reinforcing and strengthening strategies for prevention and early diagnosis of T2DM should be taken into consideration.
Limitations of the review
Identification of papers was through electronic databases and handsearching. All of the reviewed studies were published in English. A limitation of this review was related to the heterogeneity of the reviewed studies. The studies were carried out on different populations (although they were mostly from Eastern Mediterranean countries) from various levels of health care provision and used different methodologies and adherence measurements and follow-up duration. In addition, the studies reported variable outcome measures, eg, some studies covered both T1DM and T2DM, whereas others focused on T2DM only. Due to a lack of published studies, this review did not include data from all Middle Eastern countries. Therefore, the outcomes of the review are of a broad nature, and their relevance to population groups in other countries, societies, and contexts is unclear. However, the strengths of the review were that it incorporated data related to the wider management of diabetes in the region and did not only focus on adherence studies. In addition, data provided here could be considered adequate to comment on the potential implications for T2DM care in the Middle Eastern region.
Practice implications
The increased prevalence of T2DM and the poor glycemic control among the Eastern Mediterranean population calls for further research, particularly to identify the determinants of patients’ behavior. For better management of this disease, a collaborative approach between patients, their families, health care professionals, and the government should be adopted. The health awareness of patients, which is a determinant of their behavior, should be improved by increasing education efforts. This could be achieved by modifying physician–patient communication to accommodate health beliefs and culture.
In a study by Alhyas et al,26 it was found that beliefs and attitudes of some health care professionals might constitute an obstacle to the management of DM in the Middle East. For example, some health care professionals were poorly motivated to get involved in patients’ care. This was due to beliefs that diabetes is a complex disease, needs intensive care, and the complications are hard to control once they have occurred. Some health care professionals perceived the poor compliance of patients to treatment plans and not achieving target goals as barriers to their motivation and contribution to the management process. Also, this reduced their motivation to the provision of high-quality diabetes care. Therefore, stressing the need for continuous education and training for health care professionals and applying a system for credit and qualifications would enhance their responsibility in providing better disease management.
The lack of a multidisciplinary approach in patients’ care has been reported in several studies. Four studies have concluded that health care professionals, such as dietitians, chiropodists, ophthalmologists, or health educators, did not see patients following their diagnosis.3,31,34,42 Another study by Biderman et al39 reported that physicians are the health care providers most involved in diabetes care in all health sectors. However, doctors usually concentrate on the disease rather than the whole person and neglect the importance of patient perceptions and satisfaction. Patient dissatisfaction is a major factor contributing to medicine misuse and nonadherence.11 Competent professionals must cooperate in order to provide patients with the required skills for maintaining untraditional desired behavior. Therefore, implementing behavioral strategies, psychological interventions, and services that incorporate all health care professionals would have a great influence on patients’ behavior and health outcomes. Individualization of care, taking into consideration the patient, and the societal, cultural, and economic variables would also be paramount. This would help patients to initiate and maintain behavioral change, particularly in lifestyle aspects.50
Conclusion
Prevention and management of T2DM is a priority for governments and people in Middle Eastern countries. This review identifies a lack of health knowledge about diabetes among Middle Eastern populations. The lack of awareness impacts on health behaviors and medication adherence and has implications for treatment outcomes. Many health beliefs and social, cultural, and lifestyle factors that are specific to people in Middle Eastern countries have been identified. These have been found to be important for disease patterns at a population level, management strategies at a governmental and health professional level, and health behaviors at the individual level. Knowledge, beliefs, and cultural and lifestyle factors play an important role in patients’ decisions regarding medication adherence and lifestyle interventions.
Disclosure
The authors report no conflicts of interest in this work.
References
World Health Organization. Diabetes programme [online]; 2013. Available from: http://who.int/diabetes/en. Accessed July 17, 2013. | ||
Musaiger AO. Overweight and obesity in the Eastern Mediterranean Region: can we control it? East Mediterr Health J. 2004;10(6): 789–793. | ||
Al-Kaabi J, Al-Maskari F, Saadi H, Afandi B, Parkar H, Nagelkerke N. Assessment of dietary practice among diabetic patients in the United Arab Emirates. Rev Diabet Stud. 2008;5(2):110–115. | ||
Abahussain NA, El-Zubier AG. Diabetes knowledge among self-reported diabetic female teachers: Al-khobar, Saudi Arabia. J Family Community Med. 2005;12(1):43–48. | ||
Azab AS. Glycemic control among diabetic patients. Saudi Med J. 2001;22(5):407–409. | ||
Mabry RM, Reeves MM, Eakin EG, Owen N. Evidence of physical activity participation among men and women in the countries of the Gulf cooperation council: a review. Obes Rev. 2010;11(6):457–464. | ||
Salti I, Benard E, Detournay B, et al. A population-based study of diabetes and its characteristics during the fasting month of Ramadan in 13 countries: results of the epidemiology of diabetes and Ramadan 1422/2001 (EPIDIAR) study. Diabetes Care. 2004;27(10):2306–2311. | ||
INSEAD Knowledge. Combatting diabetes: some things money can’t buy [online]; 2012. Available from: http://knowledge.insead.edu/csr/healthcare/combatting-diabetes-some-things-money-cant-buy-583. Accessed July 17, 2013. | ||
World Health Organization. Building the knowledge based on the social determinants of health. Review of seven countries in the Eastern Mediterranean region [online]; 2008. Available from: http://applications.emro.who.int/dsaf/dsa939.pdf. Accessed July 20, 2013. | ||
International Diabetes Federation. Middle East and North Africa (MENA) [online]; 2013. Available from: http://idf.org/diabetesatlas/5e/middle-east-and-north-africa. Accessed July 17, 2013. | ||
World Health Organization. Adherence to long-term therapies: evidence for action [online]; 2003. Available from: http://who.int/chp/knowledge/publications/adherence_report/en/. Accessed July 22, 2013. | ||
Kamel NM, Badawy YA, el-Zeiny NA, Merdan IA. Sociodemographic determinants of management behaviour of diabetic patients. Part I. Behaviour of patients in relation to management of their disease. East Mediterr Health J. 1999;5(5):967–973. | ||
Khattab MS, Aboifotouh MA, Khan MY, Humaidi MA, Al-Kaldi YM. Compliance and control of diabetes in a family practice setting, Saudi Arabia. East Mediterr Health J. 1999;5(4):755–765. | ||
Roaeid RB, Kablan AA. Profile of diabetes health care at Benghazi Diabetes Centre, Libyan Arab Jamahiriya. East Mediterr Health J. 2007;13(1):168–176. | ||
Al-Qasem A, Smith F, Clifford S. Adherence to medication among chronic patients in Middle Eastern countries: review of studies. East Mediterr Health J. 2011;17(4):356–363. | ||
Al-Saeedi M, Elzubier AG, Bahnassy AA, Al-Dawood KM. Treatment-related misconceptions among diabetic patients in Western Saudi Arabia. Saudi Med J. 2002;23(10):1243–1246. | ||
Al-Saeedi M, Elzubier AG, Bahnassi AA, Al-Dawood KM. Patterns of belief and use of traditional remedies by diabetic patients in Mecca, Saudi Arabia. East Mediterr Health J. 2003;9(1–2):99–107. | ||
Mishali M, Omer H, Heymann AD. The importance of measuring self-efficacy in patients with diabetes. Fam Pract. 2011;28(1):82–87. | ||
Yekta Z, Pourali R, Aghassi MR, Ashragh N, Ravanyar L, Rahim Pour MY. Assessment of self-care practice and its associated factors among diabetic patients in urban area of Urmia, Northwest of Iran. J Res Health Sci. 2011;11(1):33–38. | ||
Jamous RM, Sweileh WM, Abu-Taha AS, Sawalha AF, Zyoud SH, Morisky DE. Adherence and satisfaction with oral hypoglycemic medications: a pilot study in Palestine. Int J Clin Pharm. 2011;33(6):942–948. | ||
Elis A, Rosenmann L, Chodick G, Heymann AD, Kokia E, Shalev V. The association between glycemic, lipids and blood pressure control among Israeli diabetic patients. QJM. 2008;101:275–280. | ||
Elliott JA, Abdulhadi NN, Al-Maniri AA, Al-Shafaee MA, Wahlstrom R. Diabetes self-management and education of people living with diabetes: a survey in primary health care in Muscat Oman. PLoS One. 2013;8(2):e57400. | ||
Shams ME, Barakat EA. Measuring the rate of therapeutic adherence among outpatients with T2DM in Egypt. Saudi Pharm J. 2010;18(4):225–232. | ||
Sweileh WM, Zyoud SH, Abu Nab’a RJ, et al. Influence of patients’ disease knowledge and beliefs about medicines on medication adherence: findings from a cross-sectional survey among patients with type 2 diabetes mellitus in Palestine. BMC Public Health. 2014;14:94. | ||
Aflakseir A. Role of illness and medication perceptions on adherence to medication in a group of Iranian patients with type 2 diabetes. J Diabetes. 2012;4(3):243–247. | ||
Alhyas L, Nielsen JD, Dawoud D, Majeed A. Factors affecting the motivation of healthcare professionals providing care to Emiratis with type 2 diabetes. JRSM Short Rep. 2013;4(2):14. | ||
Ali HI, Baynouna LM, Bernsen RM. Barriers and facilitators of weight management: perspectives of Arab women at risk for type 2 diabetes. Health Soc Care Community. 2010;18(2):219–228. | ||
Hui E, Bravis V, Hassanein M, et al. Management of people with diabetes wanting to fast during Ramadan. BMJ. 2010;340:c3053. | ||
Jimmy B, Jose J, Al-Hinai ZA, Wadair IK, Al-Amri GH. Adherence to medications among type 2 diabetes mellitus patients in three districts of Al Dakhliyah Governorate, Oman: a cross-sectional pilot study. Sultan Qaboos Univ Med J. 2014;14(2):e231–e235. | ||
Khattab M, Khader YS, Al-Khawaldeh A, Ajlouni K. Factors associated with poor glycemic control among patients with type 2 diabetes. J Diabetes Complications. 2010;24(2):84–89. | ||
Abdulhadi N, Al Shafaee M, Freudenthal S, Ostenson CG, Wahlström R. Patient-provider interaction from the perspectives of type 2 diabetes patients in Muscat, Oman: a qualitative study. BMC Health Serv Res. 2007;7:162. | ||
Badran M, Laher I. Type II diabetes mellitus in arabic-speaking countries. Int J Endocrinol. 2012;2012:902873. | ||
Al-Shookri A, Khor GL, Chan YM, Loke SC, Al-Maskari M. Type 2 diabetes in the sultanate of Oman. Malays J Nutr. 2011;17(1):129–141. | ||
Abdulhadi N, Al-Shafaee MA, Ostenson CG, Vernby A, Wahlstrom R. Quality of interaction between primary health-care providers and patients with type 2 diabetes in Muscat, Oman: an observational study. BMC Fam Pract. 2006;7:72. | ||
Alhewiti A. Adherence to long-term therapies and beliefs about medications. Int J Family Med. 2014;2014:479596. | ||
Jeragh-Alhaddad FB, Waheedi M, Barber ND, Brock TP. Barriers to medication taking among Kuwaiti patients with type 2 diabetes: a qualitative study. Patient Prefer Adherence. 2015;9:1491–1503. | ||
Aflakseir A. Predicting medication adherence based on illness perceptions in a sample of Iranian older adults. ME-JAA. 2013;10(3):3–7. | ||
Ibrahim OH, Jirjees F, Mahdi H. Barriers affecting compliance of patients with chronic diseases: a preliminary study in United Arab Emirates (UAE) population. Asian J Pharm Clin Res. 2011;4(2):42–45. | ||
Biderman A, Noff E, Harris SB, Friedman N, Levy A. Treatment satisfaction of diabetic patients: what are the contributing factors? Fam Pract. 2009;26(2):102–108. | ||
Serour M, Alqhenaei H, Al-Saqabi S, Mustafa AR, Ben-Nakhi A. Cultural factors and patients’ adherence to lifestyle measures. Br J Gen Pract. 2007;57(537):291–295. | ||
van den Arend IJM, Stolk RP, Krans HMJ, Grobbee DE, Schrijvers AJP. Management of type 2 diabetes: a challenge for patient and physician. Patient Educ Couns. 2000;40:187–194. | ||
Saadi H, Al-Kaabi J, Benbarka M, et al. Prevalence of undiagnosed diabetes and quality of care in diabetic patients followed at primary and tertiary clinics in Abu Dhabi, United Arab Emirates. Rev Diabet Stud. 2010;7(4):293–302. | ||
Al Shafaee MA, Al-Shukaili S, Rizvi SG, et al. Knowledge and perceptions of diabetes in a semi-urban Omani population. BMC Public Health. 2008;8:249. | ||
Horne R, Weinman J, Barber N, et al. Concordance, Adherence and Compliance in Medicine Taking. Report. NCCSDO R & D; 2005:1–160. | ||
Vermeire E, Royen PV, Coenen S, Wens J, Denekens J. The adherence of type 2 diabetes patients to their therapeutic regimens: a qualitative study from the patients’ perspective. Pract Diabetes Int. 2003;20:209–214. | ||
Mygind A, Kristiansen M, Wittrup I, Nørgaard LS. Patient perspectives on type 2 diabetes and medicine use during Ramadan among Pakistanis in Denmark. Int J Clin Pharm. 2013;35(2):281–288. | ||
Lawton J, Ahmad N, Hallowell N, Hanna L, Douglas M. Perceptions and experiences of taking oral hypoglycaemic agents among people of Pakistani and Indian origin: qualitative study. BMJ. 2005;330(7502):1247. | ||
Petrie KJ, Weinman J. Patients’ perceptions of their illness: the dynamo of volition in health care. Curr Dir Psychol Sci. 2012;21(1):60–65. | ||
Khoury S. A cultural approach to diabetes therapy in the Middle East. Diabetes Voice. 2001;46(1):23–25. | ||
Natureasia.com/en/nmiddleeast [online]. Dealing with mental illness in the Middle East. 2012. Available from: http://nature.com/nmiddleeast/2012/120724/full/nmiddleeast.2012.103.html. Accessed July 20, 2013. | ||
Badawi D, Saleh S, Natafgi N, Mourad Y, Behbehani K. Quality of type II diabetes care in primary health care centers in Kuwait: employment of a diabetes quality indicator set (DQIS). PLoS One. 2015;10(7):e0132883. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.