Back to Journals » Patient Preference and Adherence » Volume 16
Patient Trust in Primary Care Physicians: A Mixed Methods Study of Persons with Diabetes at University- Based Clinics in the Eastern Province of Saudi Arabia
Authors Boubshait LA ![]() , AlShamlan NA
, AlShamlan NA ![]() , AlShammari RZ, Alamrah SA, Fallatah BA, Abdel Wahab MM, Alreedy AH
, AlShammari RZ, Alamrah SA, Fallatah BA, Abdel Wahab MM, Alreedy AH
Received 25 July 2022
Accepted for publication 18 November 2022
Published 13 December 2022 Volume 2022:16 Pages 3241—3255
DOI https://doi.org/10.2147/PPA.S377500
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Leila A Boubshait,1 Nouf A AlShamlan,1 Razan Z AlShammari,2,3 Shadin A Alamrah,2,4 Bashaer A Fallatah,2 Moataza M Abdel Wahab,1 Abdullah H Alreedy1
1Department of Family and Community Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2College of Medicine, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia; 3Department of Family Medicine, King Fahd Military Medical Complex, Dhahran, Saudi Arabia; 4Department of Pediatric, King Fahd Military Medical Complex, Dhahran, Saudi Arabia
Correspondence: Leila A Boubshait, Department of Family and Community Medicine, College of Medicine, Imam Abdulrahman Bin Faisal University, P.O. Box 1982, Dammam, 34224, Saudi Arabia, Email [email protected]
Background: The establishment of patient trust in physicians is becoming increasingly valuable. Trust can be fundamental to successful patient care, favorable patient outcomes and improved financial savings for healthcare organizations. This study aims to explore patients’ perceptions of trust in physicians, determine factors that play a role in this relationship, and to identify ways to improve patient trust.
Methods: The study was conducted via a mixed-method design using semi-structured in-depth interviews until data saturation was reached (n=24), followed by a cross sectional survey of consecutive sampling until the number of participants (n=256) exceeded the required sample size. Adult patients with diabetes, aged 18– 65, attending internal medicine (IM) or family medicine (FM) clinics of King Fahd Hospital of the University, Saudi Arabia were included in the interviews and surveys. Patients’ interview transcripts were analyzed into trust dimensions resulting in a 51-item scale. Quality function deployment (QFD) was used to define the highest priority patient requirements. Overall satisfaction was calculated as a satisfaction percent, and factors related to satisfaction were tested using independent samples t-test and ANOVA.
Results: Significant domains for establishing patient trust in physicians were the perceived physician’s competency level, comprehensiveness of care, morals, personal traits, and establishing continuity of care. The trust score ranged from 42.0% to 100% with an average of 90.4%. There was no difference between the FM and IM setting, nor between the sociodemographic factors and the patients’ satisfaction level. No statistically significant results were found between diabetes type, years of diagnoses, achieving the target HbA1c with patients’ satisfaction level and trust. Patients reporting hypo or hyperglycemic symptoms had lower levels of satisfaction than those who did not.
Conclusion: Persons with diabetes were more trustful of primary care physicians if they displayed satisfactory communication skills, experience, and a caring attitude.
Keywords: patient-centered care, patient–physician relationship, patient satisfaction, primary care
Introduction
Research that explores the components contributing to patient trust in physicians is becoming increasingly valuable as institutions aim to strengthen their primary care services and achieve international accreditation standards.1 Patient trust in physicians is fundamental to successful patient care and often leads to positive patient outcomes, institutional financial revenue, and cost savings.2,3 The patient–physician relationship depends on a number of factors, including community culture, population demographics, and individual patients’ experiences. As a result, research has struggled to reach a consensus on a measurable definition of patient trust in physicians.4
Despite this challenge, many countries have examined the factors that strengthen trust between patients and physicians based on local perceptions, including studies in the United States (US), the United Kingdom (UK), India, China, South Korea, and Lebanon.5–12 Others have identified that certain communication skills and interactions with patients yield a high level of trust in physicians.1 Thom and Campbell (1997) categorized the doctor-patient relationship into seven dimensions: two are related to technical competence, (thoroughness in evaluation and providing appropriate and effective treatment) and five are interpersonal (understanding the patient’s individual experience, expressing caring, communicating clearly and completely, building a partnership/sharing power, and honesty/respect for the patient).5
As the Kingdom of Saudi Arabia works towards realizing its healthcare transformation under its 2030 vision, primary care and public health services are at the core of this transformation. There is now greater emphasis on disease prevention, health promotion, and population health management, all of which may be related to physician trust. This movement has pushed primary care practices to seek accreditation standards, which are anchored in patient centeredness and in enhancing trusting relationships between patients and their physician.13
Despite its lofty healthcare vision, little research has been done in Saudi Arabia to explicitly address factors related to patient trust in physicians. Much of the transformation’s emphasis is on chronic disease management, including diabetes, as the burden of this particular disease is high. Therefore, we wish to explore the area of trust among persons with diabetes with the understanding that they frequent clinics regularly and would have developed the need for a trusting relationship. One research study in Saudi Arabia examined the influence of the healthcare system on patient trust and found that physicians working in public hospitals received a greater level of patient trust than those employed in private hospitals.6
This study aims to explore persons with diabetes’ perceptions of trust and evaluate factors that could be related to patient trust in physicians in primary care settings. It also seeks to identify the priority requirements that strengthen patient–physician trust from the view of Saudi culture.
Materials and Methods
Study Design
This study was conducted between August 2020 and May 2021 and employed a mixed-method design consisting of two phases: in-depth interviews followed by a cross sectional survey.
Recruitment and Setting
The study was conducted on adult patients with diabetes of both genders between the ages of 18 and 65 who were attending the internal medicine (IM) or family medicine (FM) clinics at King Fahd Hospital of the University (KFHU) or its Family and Community Medicine Center clinics in Eastern province of Saudi Arabia.
KFHU is the teaching hospital of Imam Abdulrahman Bin Faisal University (IAU). As a large tertiary center, it serves IAU employees and residents from the Eastern region. The affiliated department of family and community medicine center at IAU provides care to all university staff, students, and their families, who are also eligible to receive care from KFHU. Both settings share the same electronic medical record system. Both IM and FM physicians have comparable clinical approaches and similar staff training and both contribute to undergraduate and postgraduate education. The hospital also discharges eligible patients from their inpatient and outpatient services to the family medicine outpatient services, including patients with diabetes.
Sampling and Sample Size
For Phase I, a convenience sampling technique was used. Participants were recruited until data saturation was reached.
For Phase II, consecutive enrolment was performed until the number of participants (256) exceeded the required sample size. (The minimum required sample size was calculated by STATA 11.0 software to be 224 at 95% CL, power 80%, assuming 75.7± 16 patient trust score percent in the physicians14 with a margin of error = 3).
Data Collection Plan, Technique, and Tools
Phase I
Initially, the study team conducted in-depth interviews to explore patients with diabetes’ perceptions of trust according to their experiences. Patients were invited to participate in the study after completing their consultations. Interviews were conducted in the patients’ preferred language, mostly in Arabic. The demographic data of the interviewed individuals, such as the age, sex, nationality, and level of education were obtained, followed by several open-ended questions as follows: Can you describe patient trust in physicians from your own perception? What are other factors that would potentially affect your trust in physicians from your point of view? The former answers were perceived as factors of a major impact on patient trust and the latter were perceived as factors of a lesser impact. Participants were also asked to describe a situation that made them establish or lose trust in a physician. The interviewers asked more questions when needed to verify the patient’s point of view. The interviews were conducted and audio recorded via Zoom Application version 5.2.1 after receiving the participants’ consent.13 The interviews ranged from 11 (min) to 50 (max) minutes with an average duration of 27.78 minutes.
Phase II
For the second phase of the study, the perception of trust dimensions and determinants derived from the first phase and items obtained from existing scales we obtained from the extant literature, were used to construct the questionnaire.15–19 The questionnaire was distributed initially by data collectors in the outpatient department of the FM and IM clinics. Then, due to the low number of patients visiting the hospital because of the COVID-19 pandemic (at that time the clinics were partially operating in a virtual format) the survey was designed via QuestionPro software and distributed online through WhatsApp.20 The questionnaire of patient trust in physicians (PTPS-51) contains 51 required items; it measures the importance of each item (on a scale of 1–5) and investigates patient satisfaction with each item studied (on a scale of 1–5) in either the FM or IM setting. The survey also includes questions about participants’ sociodemographic characteristics and diabetes history, such as diabetes type, years of diagnosis, last Hemoglobin A1C (HbA1C), and the patients’ self-reported episodes of hypo or hyperglycemic symptoms.
Informed consent was obtained from all study participants prior to data collection. They were reassured that all data would be kept confidential and that they have the right to withdraw from the study at any time.
Data Processing and Analysis
Qualitative Analysis
Interviews were anonymously transcribed, coded, and then categorized into different trust dimensions using the Max Weber Qualitative Data Analysis program version 18.2.4 (MAXQDA).21,22 The responses to the question “From your personal perspective, what are the determining characteristics of a physician that make him/her a trustworthy?” were perceived as factors of a major impact, whereas responses to the question “What are other factors that may potentially affect your trust?” were perceived as factors of a lesser impact on trust. Triangulation was performed by two investigators who coded the data separately without prior discussion, followed by a third investigator who compared and finalized the data interpretation. The entire team participated in the final review of themes, categories, and codes. All data were translated from Arabic to English language via the double translation method.
Quantitative Analyses
The constructed questionnaire was validated by three experts who have experience in statistics, family, and community medicine (face validity) and was distributed to 30 patients to calculate its reliability. Cronbach’s alpha was 0.923 for importance and 0.967 for satisfaction of patient’s trust in physicians. Using the IBM Statistical Package for the Social Sciences (SPSS) Statistics for Windows, version 26.0 program, overall satisfaction was calculated as a satisfaction percent (average scores *100/highest possible score) and presented as the minimum, maximum, mean, and standard deviation. The different factors related to satisfaction were tested using the independent samples t-test and analysis of variance (ANOVA).14
Quality function deployment (QFD) was used to effectively define the highest priority patient requirements and translate their voices into specific service recommendations. This was done through calculating the gap of satisfaction of each item (5 = the mean satisfaction score of the item) and multiplying it by the mean importance score obtained for the item, then arranging the requirements in descending order according to the obtained values ((5 = satisfaction score) *importance).
We used the independent sample t-test to compare the total satisfaction score and the individual satisfaction score requirements between the IM and FM settings. We also compared the scores between the two categories. Additionally, one way ANOVA was used to compare satisfaction scores among factors of three or more categories.
Results
A total of 280 patients with diabetes participated in the study; 24 patients were interviewed in the qualitative interviews, and 256 patients completed the survey. Their ages ranged from 20 to 77 with an average of 47.25±13.3 years. The majority of participants had a bachelor’s degree (see Table 1).
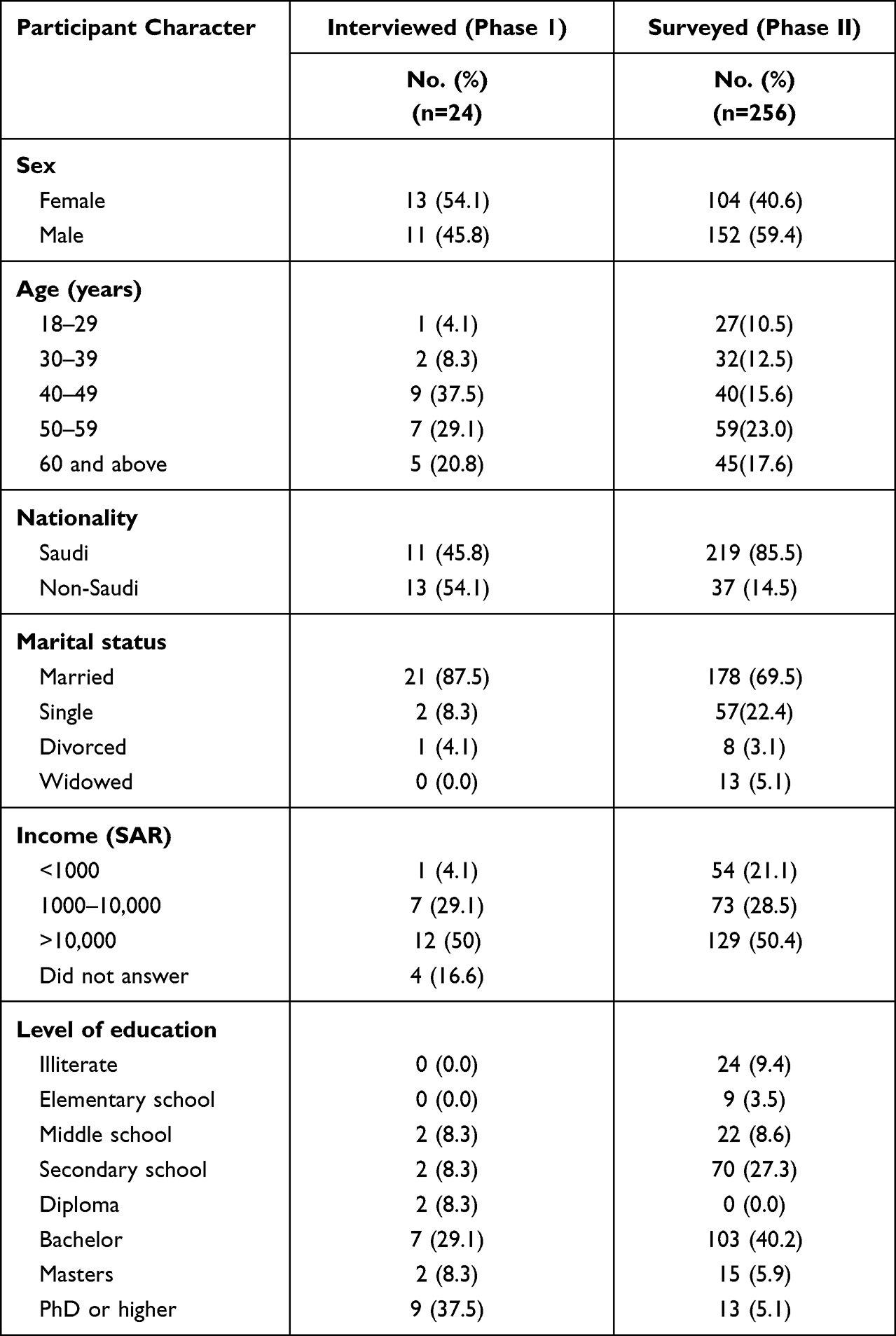 |
Table 1 Sociodemographic Characteristics of Persons with Diabetes Attending Family Medicine and Internal Medicine Clinics |
In-Depth Interviews
Factors that determine patient trust were sorted into three themes: physician competence, physician personal characteristics, and patient factors. Each theme represents multiple sub-themes. Based on patients’ perceptions of trust, Table 2 lists the factors that were perceived to have a major impact on patient’s trust. For example, the respondents considered good listening skills and providing satisfactory explanations to be the most important physician competency impacting trust, followed by level of experience, and then having a caring disposition. Notably, the physician’s professional appearance also affected patient trust. Table 3 lists the frequencies of factors that were perceived to have a lesser impact on patient trust.
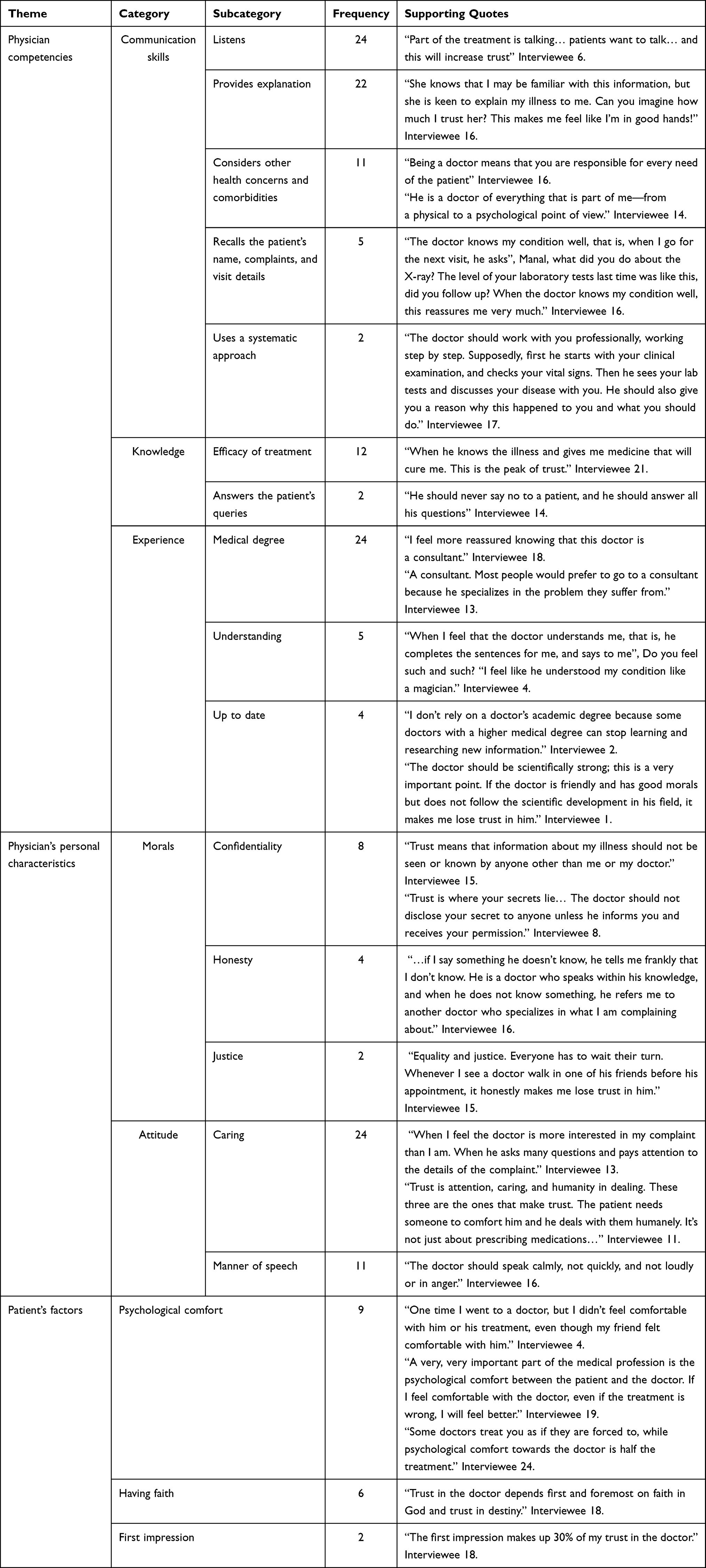 |
Table 2 Factors of Major Impact on Patient Trust and Relevant Quotes. (n=24) |
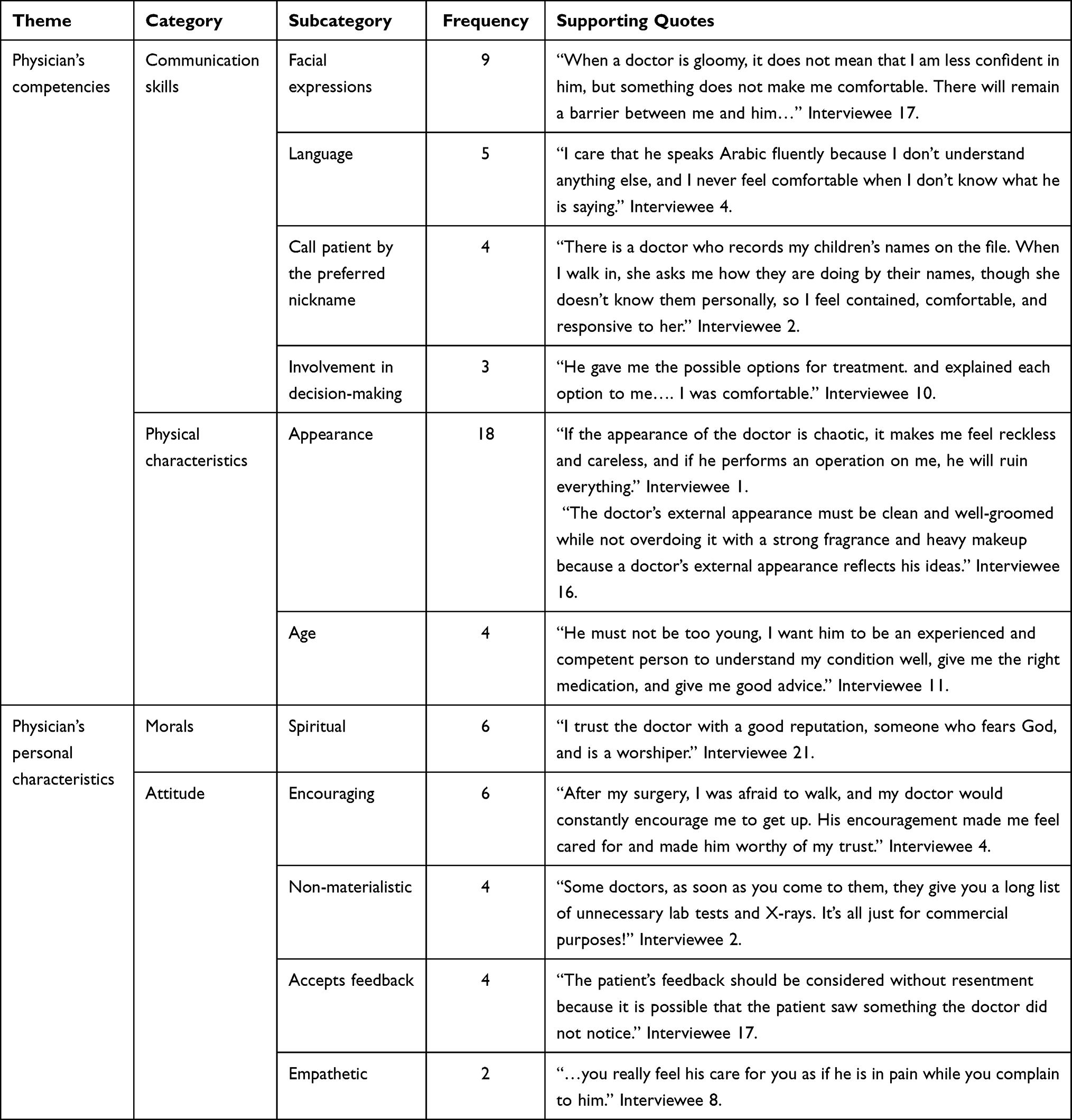 |
Table 3 Important Factors of Lesser Impact on Patient Trust and Relevant Quotes. (n=24) |
Cross-Sectional Survey
Required Items of the Highest Importance for Establishing Patient Trust in Physicians
Table 4 shows the mean importance and satisfaction rates of all studied items (patient voices) in both the FM and IM settings. The most important requirements for patient–physician trust are to have a doctor who is respectful, committed, and clarifies, engages, and informs the patient of the management plan. In addition, patients desire physicians who provide continuity of care, explain the disease clearly, take early preventative measures, ensure their privacy, and encourage them. They wish their medical record was accessible to all their healthcare providers (mean= 4.9). On the other hand, the less important requirements were the physician’s religious exterior profile and being treated by a physician of the same gender (mean= 3.1).
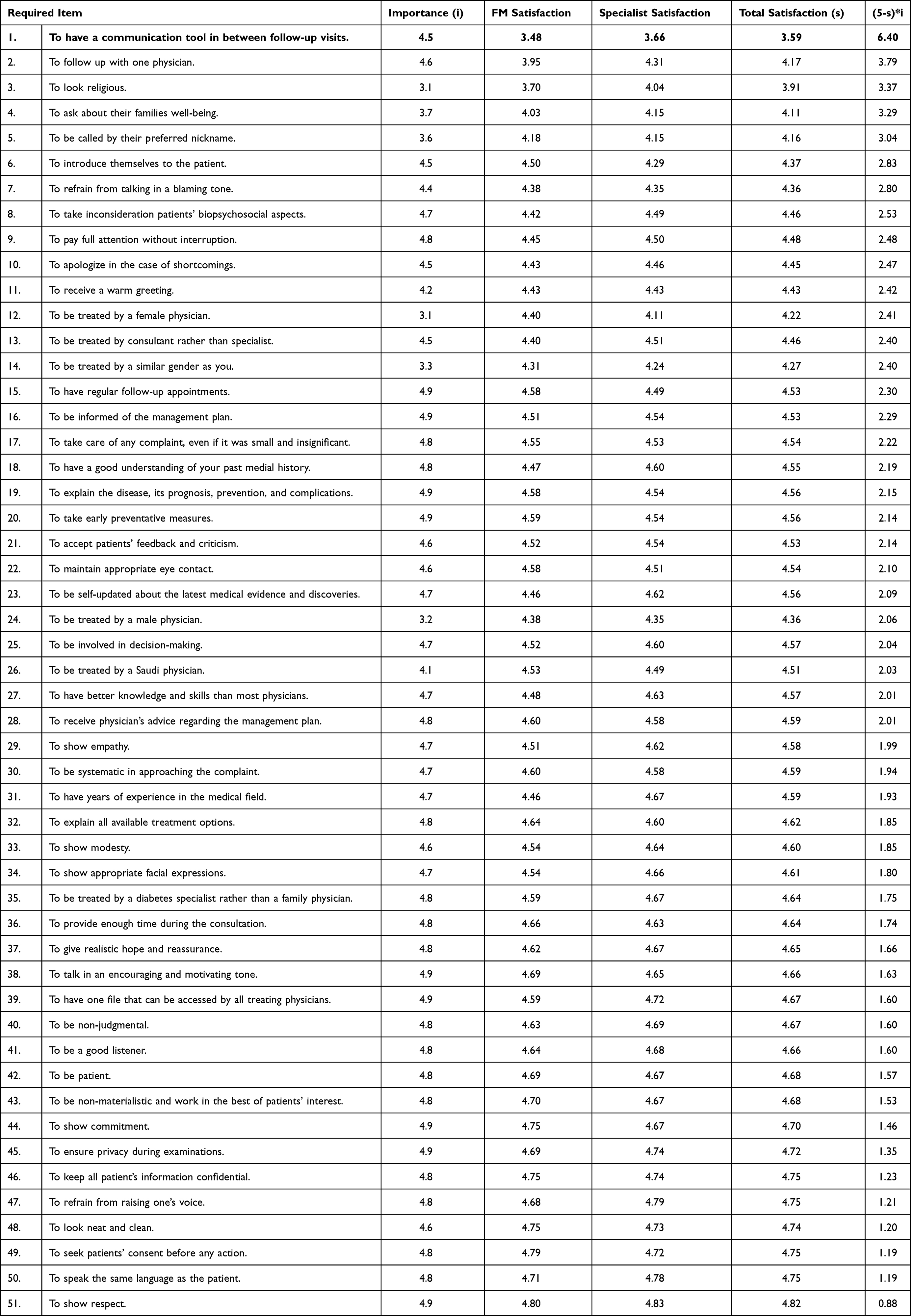 |
Table 4 Trust Requirements’ Level of Importance and Satisfaction by Different Settings. (n=256) |
Difference in Satisfaction Between FM and IM Clinics
The total satisfaction score (trust) ranged from 41.96% to 100%, with an average of 90.4% ±10.7. There was no statistically significant difference between the FM (89.9±9.2) and IM (90.6±11.6) settings (p=0.194). Out of the total sample, 17 (6.6%) scored less than 70% in trust level with no statistical difference in the proportions between the settings (Figure 1).
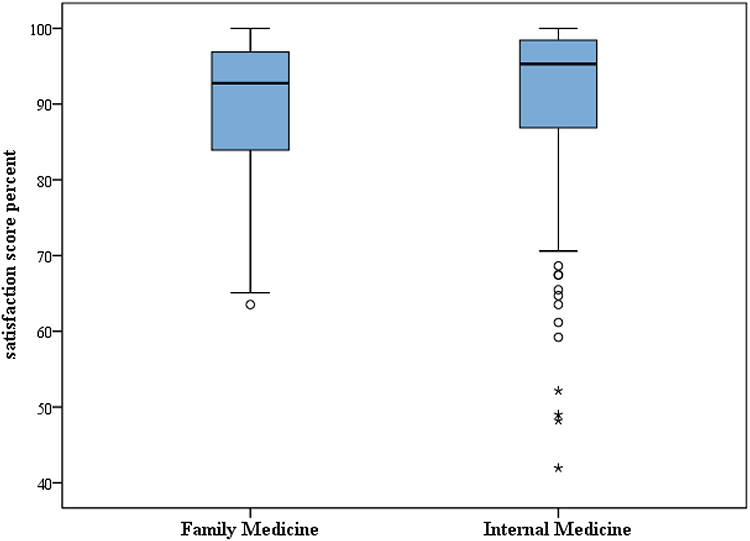 |
Figure 1 Total satisfaction percent of patient trust in family medicine and internal medicine. |
Furthermore, an item analysis revealed that FM patients with diabetes are more satisfied with physicians who introduce themselves, are the same gender as the patient, provide regular follow-up appointments, are committed, seek the patient’s consent before taking any action, maintain appropriate eye contact, and offer early preventative measures (p<0.05). In contrast, IM patients with diabetes were more satisfied with a follow-up with one physician and preferred doctors who looked religious, have years of experience, use a communication tool in between follow-ups, are updated on the latest medical evidence and discoveries, and have better knowledge and skills than most physicians. (Table 4) No statistical difference was observed between age, sex, nationality, or level of education as regards the patients’ satisfaction level.
QFD to Enhance Patient Trust in Physicians
Table 4 also displays the gaps in satisfaction from the maximum score (5) for each trust item weighted by the item importance to the patients, which reveals that the patient requirements that need highest service concentration are as follows: more frequent follow-up channels as a continuous communication tool in between follow-ups and ensuring one physician follows up on the patients’ case after each visit.
Relation Between Patient–Physician Trust Level and Diabetes-Related Parameters
Concerning diabetes history, no statistically significant relationship was found between diabetes type or years of diagnoses with patients’ level of trust. Achieving the target of HbA1c was not associated with patient trust (p=0.294). However, those who had had episodes of perceived symptoms of hypo or hyperglycemic had lower levels of trust than those who had not (88.7± 12.3 vs 91.3±9.6, respectively, p=0.019).
Discussion
The most statistically significant domains accounting for patient trust in this study are physician competence, comprehensiveness of care, physician ethical conduct and personal traits. The total satisfaction score ranged from 41.96% to 100, % with an average of 90.37%, Overall, there were no major differences between the FM and IM settings. The current study revealed that no difference was observed between patients’ satisfaction level and their demographic characteristics and diabetes-related variables such as diabetes type, years of diagnoses, or achieving the target HbA1c. However, those who had perceived symptoms of hypo or hyperglycemia had lower level of satisfaction than those who had not.
The results of this study show that patients with diabetes’ trust in physicians in Saudi Arabia is higher (Wake Forest Physician Trust Scale average of 90.4%) than levels reported in the China, the US, and the Netherlands, where PHC physicians scores average 67%, 77%, and 86%, respectively.12,16,22,23 Moreover, compared to other scales from different studies, the trust level score in this study was found to be higher than reports from the US (87.5%) and specific states: Virginia and California (78.9%), the Commonwealth of Massachusetts (US) (75.7%), and an Iranian study, in which the average score was 82.37% for patient trust in physicians.16,17,19,23 The results of the current study indicate that most individuals were highly satisfied with their physician, which echoes the established idea that the more the patients trust their physician, the better their relationship, and thus the more satisfied they are with their care.24 Furthermore, a comparison between IM and FM attendees revealed no overall differences in patients’ level of satisfaction. This might be attributable to the fact that both settings share the same medical record system and a method to communicate and exchange information on patients is readily available. Additionally, both settings have similar policies, procedures, and practice behaviors, which leads to the implementation of comparable clinical and therapeutic approaches to patient care. However, there were statistically significant differences in the factors that led to a high level of satisfaction in the different settings, which might be explained by the fact that patients in IM and FM clinics have different needs and expect different clinical approaches from the IM and FM physicians.
A systematic review of Saudi Arabia PHC centers found that PHC attendees were satisfied in eight out of the ten studies, with an overall satisfaction rating of 75% or higher.25 The findings from the current study were higher than a report from Abha, Saudi Arabia, which revealed that 43% of diabetic patients who attended PHC were highly satisfied.26 Additionally, a study done in Dammam, Saudi Arabia PHCs reported a 50.5% patient satisfaction rate.27 The higher percentage of trust in this study compared to other Saudi studies could be attributed to differences in methodologies, institutions, and patients and physicians’ backgrounds. KFHU is an academic hospital that is Joint Commission International (JCI) accredited, the practicing physicians are highly qualified, and almost all of them participate in undergraduate or postgraduate education. Being a part of this accreditation journey encourages them to be updated with the latest guidelines, practice medicine efficiently, and serve as a role model for their students and residents.
The patients had more trust in physicians who spoke in an encouraging and motivating tone. In addition, physicians’ personal traits and morals, such as showing respect, fidelity, commitment, and ensuring patient privacy during examinations, had a great influence on patient trust. These findings are consistent with those of another study conducted on the residents of urban and rural areas of southern India.28 To gain a patient’s trust, it is also critical to explain the disease and to offer information about the drug prescribed and any adverse effects it may have. According to the findings of one US study designed to identify factors that build trust, physicians are perceived as competent based on their abilities to explain patients’ conditions, practice comprehensive care, and solve their health concerns.29 As assessed by our results, comprehensive care entails taking preventative measures against future health issues, delaying health deterioration, and maintaining proper follow-up appointments with patients. According to research from the UK and US, there is an association between patient trust and continuity of care, where continuity of care means having a regular physician or place of care or concentrating one’s care with a single physician or location of care.30 These findings may imply the value of knowing patients’ prior health issues to gain their trust.
In our study, access to patients’ past medical history from health records was shown to be important in influencing patient’s level of trust. Our study shows that physicians’ attire had an impact on the patient–physician relationship. As one interviewee explained,
The doctor’s external appearance must be clean and well-groomed while not overdoing it with a strong fragrance and heavy makeup because a doctor’s external appearance reflects his/her ideas.
This finding is in line with those of two studies conducted in Saudi Arabia. In Jeddah, a 2020 study done concluded that physicians should be aware that their attire could affect the patient’s trust and compliance with medical advice or the treatment plan.31 Similarly, 2014 study done in Riyadh showed that the level of patient trust in a physician is related to his/her external appearance.32
Results from the current study demonstrate that some factors, such as the doctor’s gender, religious profile, asking casually about family health, and calling individuals by their preferred nicknames were less important to patients. On the other hand, research in southern India showed that these factors had a statistically significant impact on trust.28 Specifically, the study pointed that they made patients feel more comfortable and familiar with the physicians and that they felt that they had something in common with them.
The result of our analysis shows that two factors were of great importance for patients and received low satisfaction scores in both the IM and FM settings: utilizing a communication tool in between follow-up visits and establishing continuity of care with one physician. These factors can be the focus of future interventions to improve patient satisfaction. These findings are consistent with the results of other studies from China, South Korea, and the US, where it has been found that effective physician communication is positively associated with higher patient satisfaction.33–35 Moreover, physicians are advised to embrace a deeper interpersonal relationship with their patients.35
No significant association was found between the participants’ demographic characteristics, such as age, sex, nationality, income, and level of education, with patient satisfaction in this study. This outcome was similar to the findings of a study performed in PHC centers in the US and UK that explored the effect of having a regular family physician on trust and satisfaction and reported no significant difference in satisfaction levels between male and female physicians.36 On the other hand, another study found that patients of female physicians were more satisfied, attributing this significant difference to female physicians being more patient centered, empathic, and providing longer visits.37 Moreover, another US study concluded that the participant’s age was not significantly related to their satisfaction with the primary care physician.38 Contrary to our findings, previous studies showed a significant relation between patients’ demographic characteristics and the level of satisfaction. For instance, one paper from China found that male participants had greater satisfaction with their family physicians33 Additionally, another study from the US reported that high-income participants were more likely to be completely satisfied with their physicians.38
Concerning the diabetes factors, patient satisfaction was not statistically related to diabetes type or time since diagnosis. In contrast, one study from Italy found that those with Type 1 diabetes appeared to have less trust in family, friends, and healthcare providers than individuals with Type 2 diabetes.39 Moreover, there was no statistically significant association between patient satisfaction and glycemic control. Conversely, a study from Malaysia found that individuals with Type 2 diabetes who received family care showed improvements in glycemic control.40 On the other hand, our data shows that individuals who had frequent low or high blood sugar crises had a significantly lower level of satisfaction with their treating physician. Similarly, one study discovered lower treatment satisfaction in the presence of diabetes-related complications.40
Limitations and Future Research
The current study was conducted in two main settings: KFHU IM clinics and KFHU FM clinics, but both are similarly equipped with physicians of similar qualifications. The similarity between the settings may differ in other Eastern province institutions. The COVID-19 pandemic was another limitation; even though we exceeded the minimum required sample size, a larger sample would have highlighted more factors associated with trust.
Conclusion
The most important items contributing to patient–physician trust were to have a respectful and committed physician who explains clearly to the patients their health condition, recommends preventative measures, ensures privacy, establishes continuity of care, and engages the patient in the management plan.
The trust scores also showed that two factors were of high level of importance but received low satisfaction levels: having a communication method in between follow-up visits and establishing continuity of care with one physician.
The overall level of patient trust in physicians did not differ between the IM and FM settings.
Therefore, we recommend system level changes by primary care leadership of organizations to establish training programs for primary care physicians regarding the factors our study has shown to strengthen patient trust. Leadership should also work on creating infrastructures that ensure continuity of care for patients.
Family medicine can provide similar care outcomes to internal medicine, as shown by the similar patient– physician trust levels; therefore, referral to IM might not provide more patient satisfaction.
Primary care practices should explore more platforms, such as virtual visits and patient portals, to establish a continuous communication method in between the in-person clinic visits.
Finally, the lowest trust levels were found in patients who reported perceived symptoms of hyperglycemia. With more research, this finding can potentially serve as an indirect indicator for identifying low trust in physicians and can be the focus of targeted efforts aimed at closing the trust gaps.
Key Points for Decision-Makers
- The Arabic version of the Patient Trust in Physician Scale (PTPS-51) is a valid tool for assessing patient- physicians trust in both Primary Care and hospital-based clinical settings in Saudi Arabia.
- Patients’ trust in their physicians depends heavily on the effectiveness of the physicians’ communication skills and the establishment of continuity of care.
Data Sharing Statement
The data sets generated and analyzed for this study are available from the corresponding author upon reasonable request.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Ethical approval was obtained from the Institutional Review Board Committee of Imam Abdulrahman Bin Faisal University (IRB) No. IRB‐UGS‐2020‐01-094, dated March 29, 2020, and informed written consent was obtained from all participants.
Consent to Participate
Participation in this study was voluntary and informed written consent was obtained from all study participants. The participants informed consent included publication of anonymized responses.
Consent for Publication
Obtained from the IRB and participants.
Acknowledgment
We would like to thank Editage for English language editing.
Author Contributions
RZA, SAA, and BAF conducted the field work for data acquisition, analyzed the qualitative portion of the study, and drafted the article. AHA pooled the patients with diabetes data from the health records and cleaned the data. MMA set the study design and analyzed and interpreted the results. LAB, NAS, and AHA participated in the qualitative design and analysis. NAA revised the first draft. LAB contributed to writing and editing the final article. LAB and MMA substantially revised the article. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This study received no funding.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Hall M, Dugan E, Zheng B, Mishra A. Trust in physicians and medical institutions: what is it, can it be measured, and does it matter? Milbank Q. 2001;79(4):613–639. doi:10.1111/1468-0009.00223
2. Kelley J, Kraft-Todd G, Schapira L, Kossowsky J, Riess H, Timmer A. The influence of the patient-clinician relationship on healthcare outcomes: a systematic review and meta-analysis of randomized controlled trials. PLoS One. 2014;9(4):e94207. doi:10.1371/journal.pone.0094207
3. Wilk A, Platt J. Measuring physicians’ trust: a scoping review with implications for public policy. Soc Sci Med. 2016;165:75–81. doi:10.1016/j.socscimed.2016.07.039
4. Pearson S, Raeke L. Patients’ trust in physicians: many theories, few measures, and little data. J Gen Intern Med. 2000;15(7):509–513. doi:10.1046/j.1525-1497.2000.11002.x
5. Thom D, Campbell B. Patient–physician trust: an exploratory study. J Fam Pract. 1997;44(2):169–176.
6. Aljaffary A, AlThumairi A, Almarhoon L, Alsaawi G. Measuring patient trust in public versus private physicians in the kingdom of Saudi Arabia (KSA). J Multidiscip Healthc. 2021;14:151–159. doi:10.2147/JMDH.S286313
7. Croker J, Swancutt D, Roberts M, Abel G, Roland M, Campbell J. Factors affecting patients’ trust and confidence in GPs: evidence from the English national GP patient survey. BMJ Open. 2013;3(5):e002762. doi:10.1136/bmjopen-2013-002762
8. Gopichandran V, Chetlapalli S. Factors influencing trust in doctors: a community segmentation strategy for quality improvement in healthcare. BMJ Open. 2013;3(12):e004115. doi:10.1136/bmjopen-2013-004115
9. Kim A, Bae J, Kang S, Kim Y, Lee J. Patient factors that affect trust in physicians: a cross-sectional study. BMC Fam Pract. 2018;19:1. doi:10.1186/s12875-018-0875-6
10. Shaya B, Al Homsi N, Eid K, et al. Factors associated with the public’s trust in physicians in the context of the Lebanese healthcare system: a qualitative study. BMC Health Serv Res. 2019;19:1. doi:10.1186/s12913-019-4354-0
11. Thom D. Physician behaviors that predict patient trust. J Fam Pract. 2001;50(4):323–328.
12. Wang W, Zhang H, Washburn D, et al. Factors influencing trust towards physicians among patients from 12 hospitals in China. Am J Health Behav. 2018;42(6):19–30. doi:10.5993/AJHB.42.6.3
13. Health sector transformation program. [Internet]. Saudi vision 2030; 2022 [cited January 13, 2022]. Available from: https://www.vision2030.gov.sa/ar/v2030/vrps/%D8%A8%D8%B1%D9%86%D8%A7%D9%85%D8%AC-%D8%AA%D8%AD%D9%88%D9%84-%D8%A7%D9%84%D9%82%D8%B7%D8%A7%D8%B9-%D8%A7%D9%84%D8%B5%D8%AD%D9%8A.
14. StataCorp. Stata Statistical Software: Release 16. College Station, TX: StataCorp LLC; 2019.
15. Video conferencing, cloud phone, webinars, chat, virtual events | zoom [Internet]. Zoom Video Communications; 2021 [cited September 5, 2021]. Available from: https://zoom.us/.
16. Hall MA, Zheng B, Dugan E, et al. Measuring patients’ trust in their primary care providers. Med Care Res Rev. 2002;59(3):293–318. doi:10.1177/1077558702059003004
17. Safran D, Kosinski M, Tarlov A, et al. The primary care assessment survey. Med Care. 1998;36(5):728–739. doi:10.1097/00005650-199805000-00012
18. Leisen B, Hyman M. An improved scale for assessing patients’ trust in their physician. Health Mark Q. 2001;19(1):23–42. doi:10.1300/J026v19n01_03
19. Anderson LA, Dedrick RF. Development of the trust in physician scale: a measure to assess interpersonal trust in patient-physician relationships. Psychol Rep. 1990;67(8):1091. doi:10.2466/pr0.1990.67.3f.1091
20. Free online survey software and tools | questionPro® [Internet]. Questionpro.com; 2021 [cited September 5, 2021]. Available from: https://www.questionpro.com/.
21. VERBI Software. MAXQDA 2020. Berlin: VERBI Software; 2020.
22. Hillen M, Postma R, Verdam M, Smets E. Development and validation of an abbreviated version of the Trust in Oncologist Scale—The Trust in Oncologist Scale–short form (TiOS-SF). Support Care Cancer. 2016;25(3):855–861. doi:10.1007/s00520-016-3473-y
23. Dehghanfard J, Yazdanpanah A, Mahmoudi G. The level of patient trust in family physicians. Int J Manag Appl Sci. 2016;2(8):2394–7926.
24. Senitan M, Alhaiti A, Gillespie J. Patient satisfaction and experience of primary care in Saudi Arabia: a systematic review. Int J Qual Health Care. 2018;30(10):751–759. doi:10.1093/intqhc/mzy104
25. Ghazwani E, AlJaber O. Study of satisfaction of diabetic patients attending the diabetic clinic at primary health centers in Abha city, Saudi Arabia. Int J Med Sci Public Health. 2014;3(4):436. doi:10.5455/ijmsph.2014.110220141
26. Al Ali A, Elzubair A. Establishing rapport: physicians′ practice and attendees′ satisfaction at a Primary Health Care Center, Dammam, Saudi Arabia, 2013. J Family Community Med. 2016;23(1):12. doi:10.4103/2230-8229.172224
27. Gopichandran V, Chetlapalli S. Trust in the physician–patient relationship in developing healthcare settings: a quantitative exploration. Indian J Med Ethics. 2015;12(3):141. doi:10.20529/IJME.2015.043
28. Greene J, Ramos C. A mixed-methods examination of health care provider behaviors that build patients’ trust. Patient Educ Couns. 2021;104(5):1222–1228. doi:10.1016/j.pec.2020.09.003
29. Mainous A, Baker R, Love M, Gray D, Gill J. Continuity of care and trust in one’s physician: evidence from primary care in the United States and the United Kingdom. Fam Med. 2001;33(1):22–27.
30. Basheikh A, Yasawy M, Magadmi B, et al. The effect of male physicians’ outfits on the general population’s perception in Saudi Arabia. Cureus. 2020. doi:10.7759/cureus.12131
31. Aldrees T, Alsuhaibani R, Alqaryan S, et al. Physicians’ attire. Saudi Med J. 2017;38(4):435–439. doi:10.15537/smj.2017.4.15853
32. Chen W, Feng Y, Fang J, et al. Effect of trust in primary care physicians on patient satisfaction: a cross-sectional study among patients with hypertension in rural China. BMC Fam Pract. 2020;21(1):1–196. doi:10.1186/s12875-020-01268-w
33. Kim SS, Kaplowitz S, Johnston MV. The effects of physician empathy on patient satisfaction and compliance. Eval Health Prof. 2004;27(3):237–251. doi:10.1177/0163278704267037
34. Platonova EA, Kennedy KN, Shewchuk RM. Understanding patient satisfaction, trust, and loyalty to primary care physicians. Med Care Res Rev. 2008;65(6):696–712. doi:10.1177/1077558708322863
35. Baker R, Mainous Iii AG, Gray DP, Love MM. Exploration of the relationship between continuity, trust in regular doctors and patient satisfaction with consultations with family doctors. Scand J Prim Health Care. 2003;21(1):27–32. doi:10.1080/0283430310000528
36. Zandbelt LC, Smets EMA, Oort FJ, Godfried MH, Haes HCJM. Satisfaction with the outpatient encounter - A comparison of patients’ and physicians’ views. J Gen Intern Med. 2004;19(11):1088–U22. doi:10.1111/j.1525-1497.2004.30420.x
37. Blendon RJ, Benson JM, Hero JO. Public trust in physicians — u.S. medicine in an international perspective. N Engl J Med. 2014;371(17):1570–1572. doi:10.1056/NEJMp1407373
38. Trento M, Tomelini M, Basile M, et al. The locus of control in patients with Type 1 and Type 2 diabetes managed by individual and group care. Diabetic Med. 2008;25(1):86–90. doi:10.1111/j.1464-5491.2007.02319.x
39. Nordin N, Mohd Hairon S, Yaacob N, Abdul Hamid A, Hassan N. Effects of family doctor concept and doctor-patient interaction satisfaction on glycaemic control among type 2 diabetes mellitus patients in the northeast region of Peninsular Malaysia. Int J Environ Res Public Health. 2020;17(5):1765. doi:10.3390/ijerph17051765
40. Biderman A, Noff E, Harris S, Friedman N, Levy A. Treatment satisfaction of diabetic patients: what are the contributing factors? Fam Pract. 2009;26(2):102–108. doi:10.1093/fampra/cmp007
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.