Back to Journals » Psychology Research and Behavior Management » Volume 15
Patient Toward Physician Occupational Stigma Scale: Development of the Chinese Version
Authors Fan Z ![]() , Chen H
, Chen H ![]() , Wu H
, Wu H ![]() , Zhang X
, Zhang X
Received 24 May 2022
Accepted for publication 31 July 2022
Published 11 August 2022 Volume 2022:15 Pages 2117—2127
DOI https://doi.org/10.2147/PRBM.S375032
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Zhiguang Fan,1,2 Hongyan Chen,3 Hanwei Wu,4 Xinghai Zhang2
1Department of Education, Jilin International Studies University, Changchun City, Jilin Province, People’s Republic of China; 2Department of Marxism, Changchun University of Chinese Medicine, Changchun City, Jilin Province, People’s Republic of China; 3Department of Chinese Medicine, Changchun University of Chinese Medicine, Changchun City, Jilin Province, People’s Republic of China; 4Department of English, Jilin International Studies University, Changchun City, Jilin Province, People’s Republic of China
Correspondence: Xinghai Zhang, Department of Marxism, Changchun University of Chinese Medicine, Boshuo Street 1035, Changchun City, Jilin Province, 130117, People’s Republic of China, Tel +86-431-84924101, Fax +86 1 594-831-4623, Email [email protected]
Background/Objective: Physicians’ occupational stigma could eradicate physician-patient trust, threatening physicians’ social status and occupational reputation. Hitherto, there has been no scale obtaining good psychometric properties to assess patients’ stigma toward physicians. The present study aimed to develop the Patient toward Physician Occupational Stigma Scale (PPOSS) and examine its reliability and validity.
Methods: The questionnaire comprising sociodemographic information and the PPOSS were employed to survey 645 Chinese patients in two phases. In Sample 2, the Wake Forest Physician Trust Scale (WFOTS), the Intolerance of Uncertainty Scale-12 (IUS-12), and the Brief Illness Perception Questionnaire (BIPQ) were tested.
Results: The PPOSS includes 19 items subsumed into three dimensions of stereotype, discrimination, and prejudice. According to the results of confirmatory factor analysis (CFA), the three-factor model fitted well (χ2/df=2.065, RMSEA=0.057, SRMR=0.045, RFI=0.904, CFI=0.956, IFI=0.956, PNFI=0.779, PCFI=0.811). The PPOSS was significantly negatively correlated with the WFOTS, and significantly positively correlated with the IUS-12 and the BIPQ. The Cronbach’s alpha coefficients for the total scale and each dimension were between 0.87 and 0.94, and the split-half reliability coefficients were between 0.84 and 0.93. Besides, the PPOSS had the measurement invariance across gender.
Conclusion: With its satisfactory psychometric properties, the PPOSS can be used as an effective instrument to assess patients’ stigma toward physicians.
Keywords: physicians, occupational stigma, reliability, validity
Based on blood and geographic relations, Chinese traditional society was a society of acquaintances.1 The shape, maintenance, and spread of physicians’ image were mainly through word-of-mouth communication between relatives, friends, neighbors, and colleagues.2 Under the circumstances, patients regarded physicians as familiar and trustworthy, showing more treatment compliance. Also, physicians would usually comply with professional ethics. Therefore, acquaintance could be binding on both physicians’ and patients’ behaviors, which was conducive to the establishment of a harmonious physician-patient relationship. In most cases, physicians’ image was positive and respectable.3 Nevertheless, it should not be neglected that physicians’ stigma has existed in different periods of history. For instance, Sun Simiao, the famed Chinese ancient physician mentioned in Qian Jin Yao Fang (a medical book) “Both aristocrats and commoners are ashamed of being healthcare workers”.
Physicians’ occupational stigma refers to the negative and biased cognitive belief that patients hold toward physicians, as well as the subsequent negative emotional reactions and behavioral patterns.4 As a tainted identity, stigma is generally related to the negative results of social exclusion, social devaluation, and interpersonal avoidance.5–7 Patients with a high perceived stigma toward physicians might conceal their medical records, break physicians’ advice, and even threaten or attack medical staff.8,9 Stigma can increase patients’ inter-group anxiety and destruct physician-patient relationships, which is especially obvious among the people who once had conflicts with physicians.10
Devoid of scientific research instruments, previous studies generally focused on a specific theme of physicians’ occupational stigma through qualitative analysis. For instance, Riley et al found that physicians had a relatively high stigma toward mental illness, work-related stress, and burnout, showing the intolerance of their vulnerability, so that they would continue their work although they feel uncomfortable.11 Because of the limitations in the research method, the results of different qualitative studies cannot be compared directly. To enhance the objectivity of studies’ conclusions, support from quantitative data is still needed. However, non-standardized assessment instruments are commonly employed in the existing quantitative studies, which might affect the stability and accuracy of research results. Wijeratne et al found that physicians suffering from depression or anxiety are often considered less reliable.12 However, the reliability and validity of the questionnaire used in their study failed to be strictly tested. Only the Cronbach’s alpha coefficient was reported. Adopting a self-developed Discriminative Attitude Questionnaire, Zarzycki et al investigated the stigma of physicians with mental health disorders.13 The questionnaire is composed of only 3 non-standardized items and is not applicable to the whole group of physicians. Employing the Physical Distance and Discrimination Questionnaire (PDDQ), Kumar et al probed medical staff- and COVID 19-related stigma and discrimination.14 The PDDQ includes 4 items, such as “I would not shake hands with health-care workers involved in taking care of COVID-19 patients”. The PDDQ, assessing public alienation and avoidance of physicians, can reflect people’s stigma and discrimination toward physicians to a certain extent. Nonetheless, the reliability and validity of the PDDQ were not tested.
To our knowledge, there has been no standardized instrument designed for assessing public stigma toward physicians to date, and only several scales meeting psychometric criteria have involved stigma-related content. For instance, in the Trust in Doctors in General (T-DiG) and the Trust in the Health Care Team scales (THCT) both developed by Richmond et al, there are 29 items divided into 7 dimensions of Stigma-based Discrimination, Communication Competency, Fidelity, Systems Trust, Confidentiality, Fairness, and Global Trust.15 Among them, Stigma-based Discrimination only consists of 3 items, and the contents are all about public opinion on physicians or health care teams’ unfair treatment of patients. The T-DiG and the THCT cannot incorporate the rich connotation of stigma, although they can reflect public stigma toward physicians to a certain extent. Besides, there have been studies employing the adapted Social Distance Scale (SDS) as an instrument to assess physicians’ occupational stigma.16 However, the SDS was initially used to assess the behavioral disposition, discrimination, and exclusion of the public when they have interactions with psychotic patients. Therefore, when it is used to assess physicians’ occupational stigma, its applicability, reliability, and validity need to be further confirmed. Developed by Mostafa, the COVID-19 stigma scale (E16-COVID19-S) comprises 3 dimensions of Personalized Stigma, Concerns of Disclosure and Public Attitudes, and Negative Experiences.17 But the E16-COVID19-S is used to assess physicians’ perceived stigma rather than public stigma.
Stigma, first put forward by Goffman, is defined as a sort of derogatory and insulting label that represents stigmatized people’s untrustworthy and unpopular features. Scholars in psychology, sociology, and other fields give different theories to explain the structure, formation, and development of stigma. Among the theories, individual cognitive models, the most widely used theory, divides stigma into stereotype, prejudice, and discrimination.4 Stereotype pertains to the cognitive factors of stigma, reflecting most of the public’s knowledge structures of physicians. Prejudice is about the recognition of negative comments, generally along with negative emotional reactions. Discrimination refers to behavioral factors. Specific cognition and emotions might lead to negative behavioral reactions. For instance, anger at physicians probably induces criticisms of physicians from patients.
To summarize, based on the gap in existing literature, developing an instrument specifically used for assessing patients’ stigma toward physicians has great value. According to individual cognitive models, the present study, meeting the psychometric requirements, aimed to develop the PPOSS and test its reliability and validity with the hopes to provide an effective instrument for assessing patients’ stigma toward physicians, so contributing to the improvement of physicians’ image and the establishment of harmonious physician-patient relationships.
In the present study, the Wake Forest Physician Trust Scale (WFOTS), the Intolerance of Uncertainty Scale-12 (IUS-12), and the Brief Illness Perception Questionnaire (BIPQ) were selected to test the criterion validity of the PPOSS. Patients’ negative stereotypes of physicians can increase individuals’ intergroup anxiety and decrease their trust in physicians.18 Uncertainty is one of the typical characteristics of medicine. In most medical situations, decisions need to be made by physicians and patients in uncertainty.19 Individuals with high intolerance of uncertainty (IU) tend to appraise all situation types as more disconcerting, exaggerate the condition, doubt the authenticity of the medical diagnosis, question physicians’ decisions, and even avoid or refuse to communicate with physicians.20,21 Moreover, patients’ perception, cognition, and interpretation of the causes, timeline, consequences, and control of illness could affect their medical advice seeking and treatment compliance.22 For patients, the more perception of illness, the more serious perceived illness, and the more negative attitude toward physicians.23 Therefore, we hypothesized that the PPOSS was negatively correlated with the WFOTS, and positively correlated with the IUS-12 and the BIPQ.
Methods
Item Development
To form the initial items of the scale, a semi-structured interview was conducted by two trained postgraduates among 73 patients from two hospitals in Jilin, China. Research questions comprised: “When it comes to physicians, what negative comments would cross your mind?”; “What negative emotional reactions patients would have when getting along with physicians?”; and “Influenced by negative comments and emotions, what behavioral reactions do you think patients might have?”.
After the interview, the results were sorted and analyzed by three postgraduates in psychology to extract highly quoted phrases. The phrases not in line with the theme, semantically unclear, and ambiguous were deleted. Finally, 485 semantically independent phrases were obtained. After that, these valid phrases were merged and simplified. Among them, ten phrases were quoted most, including poor professional competence (67), red envelope (59), unnecessary checks and prescriptions (46), devoid of medical ethics (44), fear (39), irresponsibility (37), getting a kickback (33), apathy (26), violence (21) and caution (19).
According to the extracted phrases, the items of the initial scale were developed by two doctors in medical psychology. Two professors in psychology and three postgraduates in psychology were invited to evaluate and discuss the items and then modify or drop the inappropriate items. Eventually, the initial scale was composed of 23 items divided into three dimensions of stereotype, prejudice, and discrimination. A 5-point Likert-type scale was adopted (1=strongly disagree, 5=strongly agree).
Sample Size
Insufficient samples might lead to the unstable results of factor analysis. Generally, the sample size should be 10 times the number of items and no fewer than 300.24,25 After considering comprehensively, we set 300 as the minimum sample size. All participants were surveyed by systematically trained researchers on a one-to-one basis.
Inclusion Criteria
Criteria for inclusion of participants: (1) 18≤age≤70. (2) Participants were able to understand and communicate. (3) Participants had no mental illness or consciousness disorder. (4) Participants volunteered for the study and signed the informed consent form.
Participants
With the adoption of convenience sampling, questionnaire surveys were conducted among 645 patients from ten hospitals in two phases.
The data from Sample 1 in the first phase was used for item analysis and exploratory factor analysis (EFA). A total of 346 patients were surveyed, and 320 questionnaires were valid. The validity rate was 92.49%. Concerning gender, there were 166 males (51.88%), and 154 females (48.12%). Regarding marital status, a total of 202 were unmarried (63.13%), 107 were married (33.43%), and 11 were divorced or widowed (3.44%). Respecting educational background, a total of 39 (12.19%) received junior high school education or below, 87 (27.19%) received senior high school education, and 194 (60.62%) received college education or above. The mean age of participants in this phase was 29.88 (standard deviation=13.53, range: 18–70).
The data from Sample 2 in the second phase was used for CFA, criterion validity, reliability, and cross-group consistency tests. A total of 347 participants were surveyed, and 325 questionnaires were valid. The validity rate was 91.04%. In terms of gender, there were 128 (39.38%) males and 197 (60.62%) females. As regards marital status, a total of 137 were unmarried (42.15%), 173 were married (53.23%), and 15 were divorced and widowed (4.62%). With reference to educational background, a total of 64 (19.69%) received junior high school education or below, 56 (17.23%) received junior high school education, and 205 (63.08%) received college education or above. The mean age of participants in this phase was 32.97 (standard deviation=13.43, range: 18–70).
Instruments
The Patient toward Physician Occupational Stigma Scale (PPOSS) is a self-developed scale. The initial scale consists of 23 items divided into three dimensions of stereotype, prejudice, and discrimination. A 5-point Likert-type scale is adopted. Participants rate each item according to the degree they are in line with the description from 1 (strongly disagree) to 5 (strongly agree). The sum of the scores of all items is the total score. A higher total score shows patients’ higher stigma toward physicians.
Developed by Hall et al, the WFOTS can be used to assess how much patients trust physicians.26 The Wake Forest Physician Trust Scale (WFOTS) consists of 10 items, and each item is rated on a Likert scale from 1 (strongly disagree) to 5 (strongly agree). The sum of the scores of all items is the total score. A higher total score indicates patients’ higher trust in physicians. The Cronbach’s alpha coefficient of the scale was 0.76 in the present study.
Developed by Carleton et al in 2007, the Intolerance of Uncertainty Scale-12 (IUS-12) can be used to assess how individuals perceive, interpret, and handle uncertain situations.27 The IUS-12 is composed of 12 items divided into two dimensions of Prospective Anxiety and Inhibitory Anxiety. Each item is rated on a Likert scale from 1 (strongly disagree) to 5 (strongly agree). The sum of the scores of all items is the total score. A higher total score represents patients’ higher intolerance of uncertainty (IU). The Cronbach’s alpha coefficient of the scale was 0.89 in the present study.
Developed by Broadbent et al in 2006, the Brief Illness Perception Questionnaire (BIPQ) was adopted in the present study to assess patients’ cognitive and emotional representations of illness.28 Consisting of 9 items, the BIPQ can be divided into three dimensions of cognitive illness representation, emotional illness representation, and illness comprehensibility representation. Item examples are “How long do you think your illness will continue?” and “How much control do you feel you have over your illness?”. Item 9 is an open question, asking patients to list 3 major factors that cause their illness. This item would not be scored. The sum of the scores of the other eight items is the total score. A higher total score indicates patients’ higher negative perception and more serious perceived illness. The Cronbach’s alpha coefficient of the Chinese version was 0.80 in the present study.
Procedure
The present study was approved by the Ethics Committee of Jilin International Studies University (Project Number: JY202111001) and complied with Helsinki declaration. Participants were selected according to convenience sampling. Patients in the hospital were surveyed by systematically trained researchers on a one-to-one basis. Before the survey, participants were informed by researchers of the purpose, anonymity, procedures, and needed time and confidentiality of the present study. Besides, researchers also explained to participants that the data were only used for scientific studies. Researchers sent the link for the survey to the patients after their permission was given, and the informed consent form was signed. Patients were from departments of gastroenterology, cardiology, orthopedics, gynecology and so on.
Firstly, in Nov. 2021, a semi-structured interview was conducted among 73 patients to develop the items of the initial PPOSS. Secondly, in Jan. 2022, a questionnaire survey was conducted among 320 patients (Sample 1), and sociodemographic information and the initial PPOSS were included in the questionnaire. Item analysis and EFA were performed on the obtained data, and then the formal PPOSS was developed. Thirdly, in Mar. 2022, another questionnaire survey was conducted among 325 patients (Sample 2). Sociodemographic information, the formal PPOSS, the WFOTS, the IUS-12, and the BIPQ were comprised in the questionnaire. The surveys on both Sample 1 and Sample 2 were completed on the Internet platforms. All the collected data were reviewed by the researchers. The data with too short response time (less than 130 seconds), the same response (respond to both positive and negative items), and repeated response (from the same IP address) were deleted.
Data Analysis
Drawing on SPSS 20.0, item analysis and EFA were performed on the data from Sample 1. First, in terms of item analysis, total scores were ranked from low to high, and the upper 27% and the lower 27% were taken as high- and low-score groups. Then independent samples t-test was performed on the two groups, and the items with statistically insignificant critical ratio were deleted. The correlation coefficients between the scores of each item and the total scores of the scale were calculated using Pearson correlation analysis, and the items whose correlation coefficient was less than 0.30 were deleted. Besides, the Cronbach’s alpha coefficient of the initial scale was calculated, and if the Cronbach’s alpha coefficient got higher with the deletion of any item, that item should be deleted. Second, the value of Kaiser–Meyer–Olkin (KMO) higher than 0.60 and the p-value of Bartlett’s chi-square lower than 0.05 were set as the prerequisite for EFA.25 Maximum likelihood estimation (MLE) was performed for factor extraction.24 Promax oblique rotation and the Kaiser rule (eigenvalues > 1) were used to determine the number of factors.29,30 Items would be deleted according to the following criteria: (1) Factor item loadings<0.40. (2) Cross-loadings existed. (3) Communalities<0.20. (4) A single factor was made up of less than 3 items. (5) Items did not have theoretical links to other items in the factor.25
The data from Sample 2 was used for CFA, criterion validity, reliability, and cross-group invariance tests. First, drawing on AMOS 24.0, CFA was performed. The criteria for a good model fit were: (1) χ2/df<3.00, (2) RMSEA<0.08, (3) SRMR<0.05, (4) RFI, CFI, and IFI>0.90, (5) PNFI and PCFI>0.50.31 Second, using Pearson correlation analysis, the correlation coefficients between the PPOSS and the WFOTS, the IUS-12, the BIPQ, as well as that between its factors and the WFOTS, the IUS-12, and the BIPQ were calculated to examine the criterion validity. Third, Cronbach’s alpha coefficient and split-half reliability were used to assess the reliability of the scale. The items were equally divided into odd and even ones, and the Spearman-Brown formula was used to calculate the split-half reliability. If the reliability coefficient is higher than 0.70, the scale will be regarded to have great reliability.32 Forth, measurement invariance across gender was tested using AMOS 24.0.
The configural (M1), weak (M2), strong (M3), and strict (M4) invariance models were constructed in order. M1 was constructed by setting the same factor dimensions. Under the premise that M1 held, M2 was constructed by setting the same factor loadings. Under the prerequisite that M1 held, M3 was constructed by setting the same intercepts. Under the condition that M3 held, M4 was constructed by setting the same residual variances. ΔCFI higher than 0.01 and ΔRMSEA lower than 0.01 were set as the criteria for the acceptable invariance.33
Results
Item Analysis
The results of item analysis are shown in Table 1. Each critical ratio of the initial PPOSS was between 9.35 and 30.63. The results of correlation analysis indicated that the correlation coefficients between each item and the total scores were between 0.52 and 0.87 (p<0.01). The Cronbach’s alpha coefficient of the initial scale was 0.931. When any item was deleted, the Cronbach’s alpha coefficient did not get significantly higher. Therefore, no item was deleted in this phase.
 |
Table 1 Item Analysis of the PPOSS |
Exploratory Factor Analysis
In the initial scale, the value of KMO was 0.930, and the value of Bartlett’s test of sphericity was 3890.87 (df=253, p<0.001). According to EFA, three factors (eigenvalues>1) were extracted with 56.43% of the total variance. The items not conforming to the retention criteria were deleted. When one item was deleted, EFA would be performed again. Item 7, 16, and 19 were dropped for their factor loadings lower than 0.40. Item 22 was deleted, as it did not have theoretical links to other items in the factor. After EFA was performed again on the rest 19 items, three factors (eigenvalues>1) were extracted with 58.51% of the total variance. For each factor, the loading was between 0.49 and 0.89, and the communality was between 0.26 and 0.73 (see Table 2). According to our theoretical conceptualization and the items contained in the dimensions, factor 1 was named stereotype; factor 2 was named prejudice; and factor 3 was named discrimination.
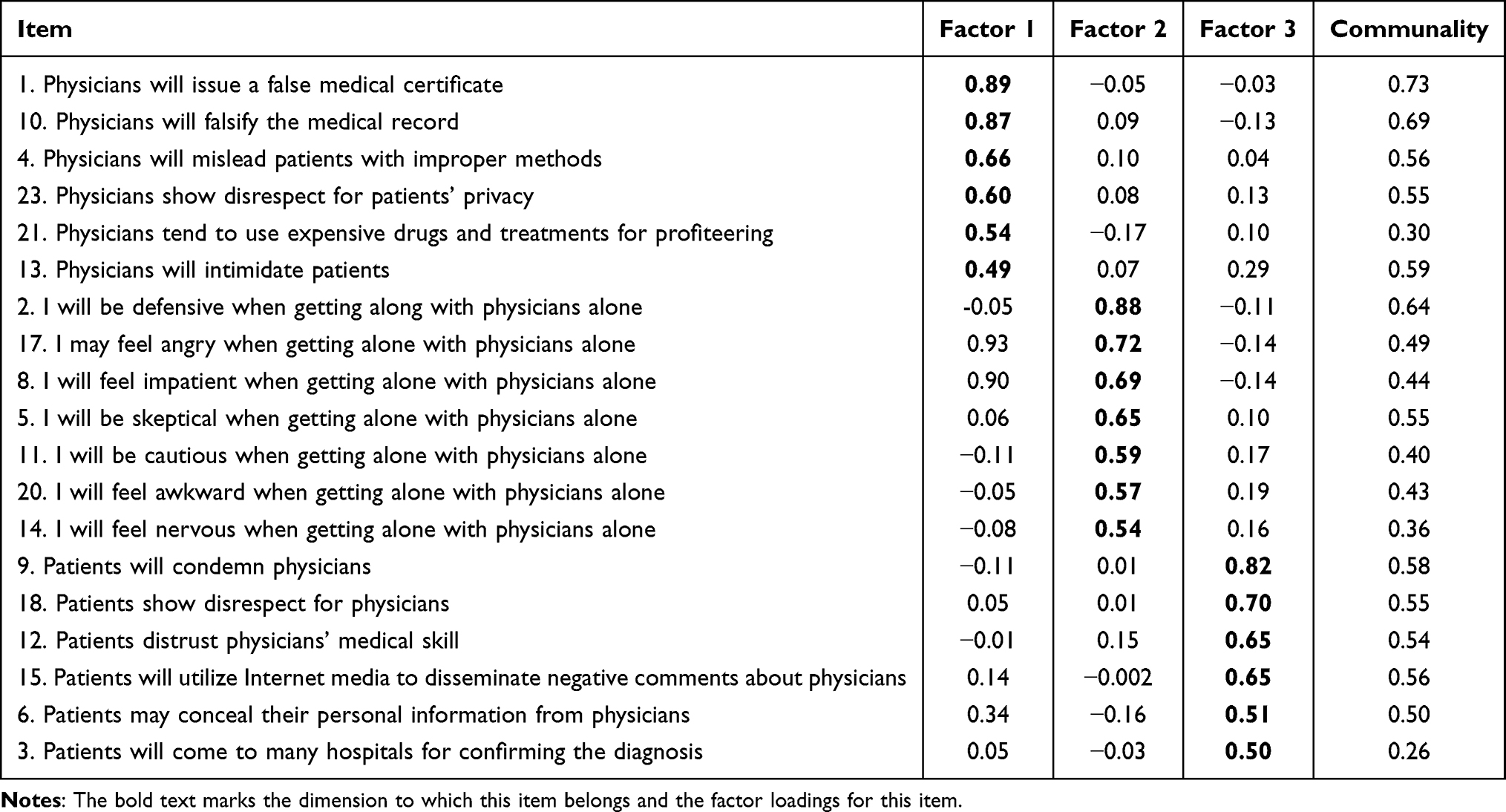 |
Table 2 Factor Loadings and Communalities of the PPOSS (N=320) |
Confirmatory Factor Analysis
CFA was performed on Sample 2 to examine the fit of three-factor structured PPOSS. The results indicated that all fit indices were adequate (χ2/df=2.065, RMSEA=0.057, SRMR=0.045, RFI= 0.904, CFI= 0.956, IFI= 0.956, PNFI= 0.779, PCFI= 0.811).
Criterion Validity Testing
Table 3 indicated the results of criterion validity testing of the PPOSS. The PPOSS, as well as its every factor was significantly negatively correlated with the WFOTS, and significantly positively correlated with the IUS-12 and the BIPQ.
 |
Table 3 Criterion Validity of the PPOSS (N=320) |
Reliability Testing
The Cronbach’s alpha coefficients of the PPOSS and each factor were between 0.87 and 0.94, and the split-half reliability coefficients were between 0.84 and 0.93 (see Table 4), which were both higher than 0.70.
 |
Table 4 Reliability of the PPOSS (N=325) |
Cross-Gender Invariance Testing
The measurement invariance of the PPOSS across gender was tested using multi-group CFA. The results (see Table 5) indicated that in M1 (configural invariance model), M2 (weak invariance model), and M3 (strong invariance model), all fit indices reached the metrological requirements, thus meeting the criteria for testing the invariance further, except SRMR was slightly higher than 0.05. The results showed when comparing M1 to M2, M2 to M3, and M3 to M4, both ∆CFI and ∆CFI were lower than 0.01 (see Table 5), suggesting that the PPOSS had measurement invariance across gender.
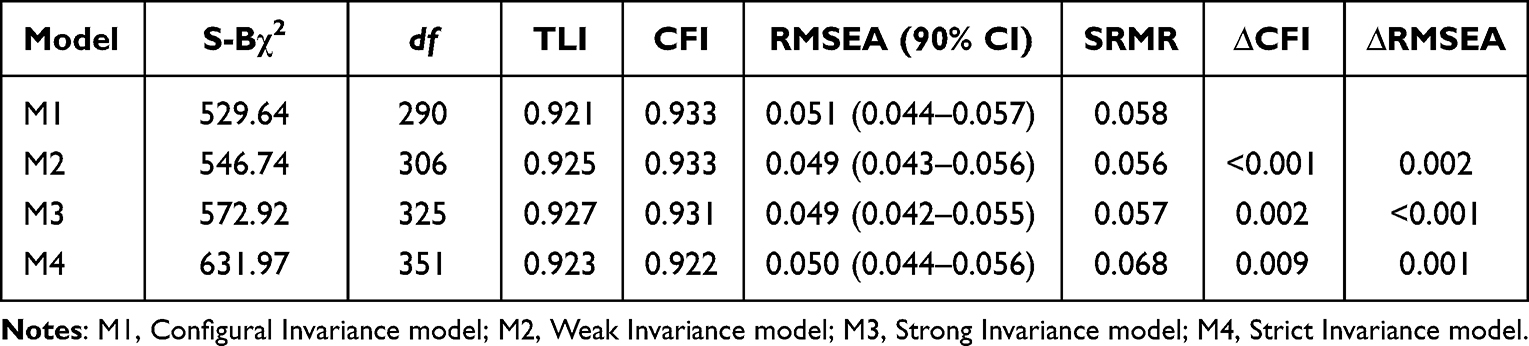 |
Table 5 Measurement Invariance Across Gender of the NOSS (N=325) |
The results of the independent samples t-test indicated that the total score of males in the PPOSS (t=2.54, p=0.011), stereotype (t=2.35, p=0.019), and prejudice (t=2.57, p=0.011) were significantly higher than females.
Discussion
The present study aimed to develop the PPOSS and examine its psychometric properties with the hopes to provide a reliable and effective instrument for assessing patients’ stigma toward physicians. Therefore, based on individual cognitive models, we constructed the theoretical structure of the PPOSS based on the results of the semi-structured interview and the suggestions of experts. Then, we formed the items of the initial scale. After that, we developed the three-factor structured PPOSS using item analysis and EFA. We further examined the construct validity, criterion validity, internal consistency, and split-half reliability, demonstrating that the PPOSS had satisfactory reliability and validity. In addition, we also tested the cross-gender invariance of the PPOSS, finding that the PPOSS had measurement invariance across gender.
The PPOSS comprises 19 items divided into three dimensions of stereotype, prejudice, and discrimination. The three-factor structure from EFA was in line with the theoretical framework, and CFA validated this framework. Consisting of 6 items, stereotype refers to patients’ negative labels and cognitive bias toward physicians. People with high scores tend to have a subjectively negative attitude toward physicians, connecting physicians to negative characteristics like exploitation, avarice, horror, and dominance. Composed of 7 items, prejudice refers to patients’ negative emotional reactions formed by their negative perceptions of physicians. People with high scores are inclined to experience negative emotions like anger, impatience, embarrassment, and anxiety when getting along with physicians. Comprised of 6 items, discrimination refers to patients’ behavioral reactions triggered by their negative perceptions of physicians and negative emotional experiences. People with high scores are prone to doubt and condemn physicians, and probably disseminate negative comments about physicians. In the Health Care Provider HIV/AIDS Stigma Scale (HPASS) and the COVID-19 Public Stigma Scale (COVID-PSS), public stigma is divided into three dimensions of stereotype, prejudice, and discrimination.34,35 Consistent with previous studies, it was also found in the present study that the three-factor model was applicable to the research on patients’ stigma toward physicians.
According to the results of correlation analysis, the PPOSS was significantly negatively correlated with the WFOTS, and significantly positively correlated with the IUS-12 and the BIPQ, which was consistent with our hypotheses. On the one hand, it suggested that the PPOSS had good criterion validity. On the other hand, the present study further demonstrated the close association between physicians’ occupational stigma and the physician-patient relationship, since patient trust, intolerance of uncertainty, and illness perceptions are crucial indicators of a physician-patient relationship.36–38 It implied that effacing the stigma is the prerequisite of establishing a harmonious physician-patient relationship. Based on previous studies, males showed significantly higher stigma toward mentally ill patients, dementia patients, and drug addicts than females,39–41 suggesting that gender differences might exist in the PPOSS. Measurement invariance across gender is the premise of comparing group differences. Hence if gender differences surely exist in the PPOSS, its cross-gender invariance o needs to be examined first. The results of multi-group CFA indicated that the PPOSS’s configural, weak, strong, and strict invariance were all acceptable, suggesting that the PPOSS had measurement invariance across gender. Gender differences in the PPOSS could be attributed to the actual differences between males and females. According to the further analysis, males got a higher score in the PPOSS, stereotype, and prejudice than females, which was in line with the previous study.
The present study has certain theoretical significance. Based on individual cognitive models, the dimensions of patients’ stigma toward physicians were constructed in the present study. Previously, individual cognitive models were mainly used to account for the formation of mental illness. The present study further enriched and confirmed the models in the occupational stigma field. The present study also has certain practical significance. Patients’ stigma toward physicians can destruct patient-physician trust, break physician-patient relationships and even trigger violence against physicians. Therefore, it is of great significance for medical practice to reduce stigma and reshape the image of physicians. Hence, the PPOSS developed in the present study, with its good psychometric properties, can be used as an instrument for accurately recognizing and assessing stigma, and for measuring the effectiveness of interventions. Besides, during the COVID-19 pandemic, healthcare workers played a pivotal role and made a great sacrifice in preventing, diagnosing, and curing illness. Nevertheless, many people still tended to avoid, exclude, and discriminate against physicians out of their fear of the virus, since physicians had a greater risk of getting infected with coronavirus for their constant contact with patients.42,43 During this special period, patients held an ambivalent attitude toward physicians—on the one hand, they showed understanding of and appreciation for physicians, but on the other hand, they also had stigmatizing remarks and behaviors against physicians.44 An epidemic of stigma can lead to frequent medical violence, resulting in the strong worry of medical staff.45 Therefore, it’s urgent for governments to take immediate interventions to reduce physicians’ stigma and physician-patient conflicts. The PPOSS can provide empirical evidence for the government to formulate policies against stigma.
The present study also has several limitations. Firstly, with convenience sampling, all participants were outpatients. Because of limited medical resources, physicians may spend only several minutes on outpatients, while outpatients need to spend lots of time waiting. By contrast, inpatients have more communication with physicians, so that physicians have a deeper understanding of their conditions,46 which probably causes differences in satisfaction with and stigma toward physicians between inpatients and outpatients. Therefore, more empirical evidence for the applicability of the PPOSS in inpatients, especially in inpatients with different illnesses is needed. Secondly, the dimensions of the PPOSS also need to be further demonstrated. The present study was based on individual cognitive models, but no theory of occupational stigma has been widely acknowledged since different theories have different advantages and emphases. Hence, more studies are needed to examine the structure of the PPOSS. Thirdly, the present study failed to examine the test-retest reliability, so the scale’s stability and consistency over time can hardly be explained. Fourthly, no item with reverse scoring was included in the PPOSS, and all items were related to physicians’ occupational stigma, which may negatively affect participants’ response, and exaggerate stigma.
Conclusion
Based on individual cognitive models, the PPOSS strictly followed the steps of scale development. The PPOSS is composed of 19 items divided into three dimensions of stereotype, discrimination, and prejudice. According to the present study, the PPOSS, with its satisfactory reliability and validity, can be a reliable and effective instrument to assess patients’ stigma toward physicians.
Acknowledgments
We are very much thankful to all the researchers for data collection and processing. We thank all the survey participants in our study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Joint Fund Project of the Educational Department of Jilin Province (project number: JJKH20211005SK).
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Hu Y, Scott J. Family and gender values in China. J Fam Issues. 2014;37(9):1267–1293. doi:10.1177/0192513x14528710
2. Wang Q. Doctor-Patient Communication and Patient Satisfaction: A Cross-Cultural Comparative Study Between China and the U.S. Purdue University; 2012.
3. Zhou M, Zhao L, Campy KS, Wang S. Changing of China׳s health policy and doctor–patient relationship: 1949–2016. Health Policy Technol. 2017;6(3):358–367. doi:10.1016/j.hlpt.2017.05.002
4. Corrigan PW, Kerr A, Knudsen L. The stigma of mental illness: explanatory models and methods for change. Appl Prev Psychol. 2005;11(3):179–190. doi:10.1016/j.appsy.2005.07.001
5. Simeone S, Rea T, Guillari A, Vellone E, Alvaro R, Pucciarelli G. Nurses and stigma at the time of COVID-19: a phenomenological study. Healthcare. 2021;10(1):25. doi:10.3390/healthcare10010025
6. Zwar L, Angermeyer MC, Matschinger H, Riedel-Heller SG, Konig HH, Hajek A. Public stigma towards informal caregiving in Germany: a descriptive study. Aging Ment Health. 2021;25(8):1515–1524. doi:10.1080/13607863.2020.1758913
7. Manchha AV, Way KA, Tann K, Thai M. The social construction of stigma in aged-care work: implications for health professionals’ work intentions. Gerontologist. 2022. doi:10.1093/geront/gnac002
8. Sharma S, Lal Gautam P, Sharma S, et al. Questionnaire-based evaluation of factors leading to patient-physician distrust and violence against healthcare workers. Indian J Crit Care Med. 2019;23(7):302–309. doi:10.5005/jp-journals-10071-23
9. Puhl RM, Gold JA, Luedicke J, DePierre JA. The effect of physicians’ body weight on patient attitudes: implications for physician selection, trust and adherence to medical advice. Int J Obes. 2013;37(11):1415–1421. doi:10.1038/ijo.2013.33
10. He W, Wang X, Zhou X, Xu L. Negative expectations and bad relationships: effects of negative metastereotypes on doctor–patient relationships. Asian J Soc Psychol. 2019;23(1):103–108. doi:10.1111/ajsp.12388
11. Riley R, Buszewicz M, Kokab F, et al. Sources of work-related psychological distress experienced by UK-wide foundation and junior doctors: a qualitative study. BMJ Open. 2021;11(6):e043521. doi:10.1136/bmjopen-2020-043521
12. Wijeratne C, Johnco C, Draper B, Earl J. Doctors’ reporting of mental health stigma and barriers to help-seeking. Occup Med. 2021;71(8):366–374. doi:10.1093/occmed/kqab119
13. Zarzycki MZ, Goetz Z, Flaga-Luczkiewicz M. What do medical students think about medical doctors with mental health issues? Psychol Health Med. 2020;25(5):623–629. doi:10.1080/13548506.2020.1724309
14. Kumar P, Chanpa N, Kotecha I, Tiwari D, Vasavada D, Bhatt R. Stigma and discrimination among doctors toward health-care staff working at COVID-19 sites. Arch Ment Health. 2020;21(2):77–82. doi:10.4103/amh.Amh_48_20
15. Richmond J, Boynton MH, Ozawa S, Muessig KE, Cykert S, Ribisl KM. Development and validation of the trust in my doctor, trust in doctors in general, and trust in the health care team scales. Soc Sci Med. 2022;298:114827. doi:10.1016/j.socscimed.2022.114827
16. Shiu C, Chen WT, Hung CC, Huang EP, Lee TS. COVID-19 stigma associates with burnout among healthcare providers: evidence from Taiwanese physicians and nurses. J Formos Med Assoc. 2021;121(8):1384–1391. doi:10.1016/j.jfma.2021.09.022
17. Mostafa A, Mostafa NS, Ismail N. Validity and reliability of a COVID-19 stigma scale using exploratory and confirmatory factor analysis in a sample of Egyptian physicians: E16-COVID19-S. Int J Environ Res Public Health. 2021;18(10):5451. doi:10.3390/ijerph18105451
18. Xu L, Sun L, Li J, Zhao H, He W. Metastereotypes impairing doctor-patient relations: the roles of intergroup anxiety and patient trust. PsyCh J. 2021;10(2):275–282. doi:10.1002/pchj.408
19. Han PKJ, Strout TD, Gutheil C, et al. How physicians manage medical uncertainty: a qualitative study and conceptual taxonomy. Med Decis Making. 2021;41(3):275–291. doi:10.1177/0272989X21992340
20. Yang Z, Zhao X, Zhu Z, Fu Y, Hu Y. How patients with an uncertain diagnosis experience intolerance of uncertainty: a grounded theory study. Psychol Res Behav Manag. 2021;14:1269–1279. doi:10.2147/PRBM.S318263
21. Koerner N, Dugas MJ. An investigation of appraisals in individuals vulnerable to excessive worry: the role of intolerance of uncertainty. Cognit Ther Res. 2007;32(5):619–638. doi:10.1007/s10608-007-9125-2
22. Huang W, Zhang L, Yan J. Psychometric evaluation of the Chinese version of the revised illness perception questionnaire for breast cancer-related lymphedema. Eur J Cancer Care. 2019;28(1):e12900. doi:10.1111/ecc.12900
23. Baines T, Wittkowski A. A systematic review of the literature exploring illness perceptions in mental health utilising the self-regulation model. J Clin Psychol Med Settings. 2013;20(3):263–274. doi:10.1007/s10880-012-9337-9
24. Worthington RL, Whittaker TA. Scale development research: a content analysis and recommendations for best practices. Couns Psychol. 2006;34(6):806–838. doi:10.1177/0011000006288127
25. Carpenter S. Ten steps in scale development and reporting: a guide for researchers. Commun Methods Meas. 2018;12(1):25–44. doi:10.1080/19312458.2017.1396583
26. Hall MA, Zheng B, Dugan E, et al. Measuring patients’ trust in their primary care providers. Med Care Res Rev. 2002;59(3):293–318. doi:10.1177/1077558702059003004
27. Carleton RN, Norton MA, Asmundson GJ. Fearing the unknown: a short version of the intolerance of uncertainty scale. J Anxiety Disord. 2007;21(1):105–117. doi:10.1016/j.janxdis.2006.03.014
28. Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res. 2006;60(6):631–637. doi:10.1016/j.jpsychores.2005.10.020
29. Fabrigar LR, Wegener DT, MacCallum RC, Strahan EJ. Evaluating the use of exploratory factor analysis in psychological research. Psychol Methods. 1999;4(3):272–299. doi:10.1037/1082-989X.4.3.272
30. Morrison JT. Evaluating factor analysis decisions for scale design in communication research. Commun Methods Meas. 2009;3(4):195–215. doi:10.1080/19312450903378917
31. Bentler PM, Bonett DG. Significance tests and goodness of fit in the analysis of covariance structures. Psychol Bull. 1980;88(3):588–606. doi:10.1037/0033-2909.88.3.588
32. Viladrich C, Angulo-Brunet A, Doval E. A journey around alpha and omega to estimate internal consistency reliability. An de Psicol. 2017;33(3):755–782. doi:10.6018/analesps.33.3.268401
33. Cheung GW, Rensvold RB. Evaluating goodness-of-fit indexes for testing measurement invariance. Struct Equ Modeling. 2002;9(2):233–255. doi:10.1207/s15328007sem0902_5
34. Wagner AC, Hart TA, McShane KE, Margolese S, Girard TA. Health care provider attitudes and beliefs about people living with HIV: initial validation of the Health Care Provider HIV/AIDS Stigma Scale (HPASS). AIDS Behav. 2014;18(12):2397–2408. doi:10.1007/s10461-014-0834-8
35. Nochaiwong S, Ruengorn C, Awiphan R, et al. COVID-19 public stigma scale (COVID-PSS): development, validation, psychometric analysis and interpretation. BMJ Open. 2021;11(11):e048241. doi:10.1136/bmjopen-2020-048241
36. Wu Q, Jin Z, Wang P. The relationship between the physician-patient relationship, physician empathy, and patient trust. J Gen Intern Med. 2022;37(6):1388–1393. doi:10.1007/s11606-021-07008-9
37. Lyu X, Fu C, Wang X. Effect and underlying mechanism of refutation texts on the trust and moral judgment of patients. Acta Psychol Sin. 2019;51(10):1171–1186. doi:10.3724/sp.J.1041.2019.01171
38. Bridges HA, Smith MA. Mediation by illness perceptions of the association between the doctor-patient relationship and diabetes-related distress. J Health Psychol. 2016;21(9):1956–1965. doi:10.1177/1359105315569094
39. Wong EC, Collins RL, Cerully JL, Yu JW, Seelam R. Effects of contact-based mental illness stigma reduction programs: age, gender, and Asian, Latino, and White American differences. Soc Psychiatry Psychiatr Epidemiol. 2018;53(3):299–308. doi:10.1007/s00127-017-1459-9
40. Werner P, Kim S. A cross-national study of dementia stigma among the general public in Israel and Australia. J Alzheimers Dis. 2021;83(1):103–110. doi:10.3233/JAD-210277
41. Sattler S, Escande A, Racine E, Goritz AS. Public stigma toward people with drug addiction: a factorial survey. J Stud Alcohol Drugs. 2017;78(3):415–425. doi:10.15288/jsad.2017.78.415
42. Dye TD, Alcantara L, Siddiqi S, et al. Risk of COVID-19-related bullying, harassment and stigma among healthcare workers: an analytical cross-sectional global study. BMJ Open. 2020;10(12):e046620. doi:10.1136/bmjopen-2020-046620
43. Taylor S, Landry CA, Rachor GS, Paluszek MM, Asmundson GJG. Fear and avoidance of healthcare workers: an important, under-recognized form of stigmatization during the COVID-19 pandemic. J Anxiety Disord. 2020;75:102289. doi:10.1016/j.janxdis.2020.102289
44. Aguirre S, Jogerst KM, Ginsberg Z, et al. COVID-19 impact on the doctor-patient relationship: patient perspectives on emergency physician empathy and communication. Bull Emerg Trauma. 2021;9(3):125–132. doi:10.30476/BEAT.2021.89058.1216
45. Kumari A, Kaur T, Ranjan P, Chopra S, Sarkar S, Baitha U. Workplace violence against doctors: characteristics, risk factors, and mitigation strategies. J Postgrad Med. 2020;66(3):149–154. doi:10.4103/jpgm.JPGM_96_20
46. Liang H, Xue Y, Zhang ZR. Patient satisfaction in China: a national survey of inpatients and outpatients. BMJ Open. 2021;11(9):e049570. doi:10.1136/bmjopen-2021-049570
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.