Back to Journals » Risk Management and Healthcare Policy » Volume 13
Patient Safety Culture in Handling Prescriptions and Interprofessional Collaboration Practices Amongst Community Pharmacists: An Investigative Simulated Patient Study from the United Arab Emirates
Authors Palaian S ![]() , Buabeid M
, Buabeid M ![]() , Ashames A
, Ashames A ![]()
Received 17 September 2020
Accepted for publication 22 November 2020
Published 31 December 2020 Volume 2020:13 Pages 3201—3209
DOI https://doi.org/10.2147/RMHP.S282571
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Marco Carotenuto
Subish Palaian,1 Manal Buabeid,1 Akram Ashames2
1Department of Clinical Sciences, College of Pharmacy and Health Sciences, Ajman University, Ajman, United Arab Emirates; 2Department of Pharmaceutical Sciences, College of Pharmacy and Health Sciences, Ajman University, Ajman, United Arab Emirates
Correspondence: Subish Palaian Email [email protected]
Background: Community pharmacists are in a unique position to identify drug therapy-related problems (DTRPs) in prescriptions and mitigate them by communicating with prescriber. This study assessed the ability of community pharmacists (CPs) to identify DTRPs in prescriptions, the level of interprofessional collaboration among physician and CPs in mitigating the identified DTRPs, and the existing safety culture practices among CPs.
Methods: Trained simulated patients (SPs), five final-year BSc Pharm female students, visited conveniently selected community pharmacies (n = 50) in Ajman emirate of the United Arab Emirates, with dummy prescriptions containing DTRPs (total 50 prescriptions with five different types of DTRPs categorized per the Pharmaceutical Care Network Europe Version 8) and assessed the DTRP-identifying ability of the CPs. SPs also observed the steps taken by the CPs to mitigate identified DTRPs and existing (if any) collaborative practices between CPs and physician. SPs documented their observations in a checklist immediately after leaving the pharmacy premises, which served as the data source. Statistical analyses were performed with chi-square at alpha = 0.05.
Results: Of the 50 respondents, 44% (n = 22) were able to identify the DTRPs. DTRP identification by pharmacists was associated with labeling [chi-square = 7.879, p value = 0.019], reconciliation [chi-square = 10.359, p value = 0.001], counseling standard [chi-square = 19.09, p = 0.000] and physician visit suggestion [chi-square = 31.15, p = 0.000]. The labeling standards for prescriptions with DTRPs were “low” in five (50%), “average“ in three (30%) and “good” in two (20%) of the cases with wrong dose. Average counseling time of the CPs was 80.38 ± 71.61 seconds. The counseling standard had no significant association with counseling time [chi-square = 34.79, p = 0.250] and use of drug information sources [chi-square = 2.86, p = 0.243]. Average time spent in dispensing is 74.4 ± 73.05 seconds. None (n = 0) of the CPs communicated with the physician, and only five out of 50 (10%) of CPs checked any DI sources. However, in 19 (38%) cases, the CPs recommended the SPs to consult their physician prior to taking the medications.
Conclusion: CPs were generally able to identify DTRPs and mitigate DTRPs by recommending physician consultation. Nevertheless, there were no professional collaborations between the SPs and physicians. The dispensing and counseling standards were not appreciable.
Keywords: community pharmacists, drug therapy related problems, simulated patient, United Arab Emirates
Introduction
According to The Pharmaceutical Care Network Europe (PCNE), a drug therapy-related problem (DTRP) can be defined as a condition involving drug therapy that interferes with desired health outcomes.1 DTRPs are the crucial domain of the pharmaceutical care practitioner; and any pharmacy practitioner is expected to be knowledgeable and able to identify and resolve DTRPs encountered in daily pharmacy practice. The purpose of minimizing DTRPs is to improve patients’ quality of life and help patients achieve their goals of therapy to recognize the optimal outcomes from pharmacotherapy. Identifying a DTRP is a clinical decision that requires the healthcare giver to recognize a relationship between the patient’s medical condition and the patient’s pharmacotherapy. Being the last prescription scanner, community pharmacists should be able to identify DTRPs in the prescriptions and recommend interventions that are able to resolve these problems.2,3 Several DTRP classifications have been mentioned in the literature.1,4 The classification provided by PCNE describes eight primary domains of causes for DTRPS, which include drug selection, drug form, dose selection, treatment duration, dispensing, drug use process, patient-related and others.1 These classifications provide scope for research aiming at the presence of these DTRPs in prescriptions.
Since the causes of DTRPs can originate from multiple levels such a physicians, pharmacists and patients, it is mandatory that healthcare workers collaborate among each other in detecting and mitigating DTRPs. Similarly, good counseling to the patient is also an indispensable step in mitigating DTRPs. Interprofessional communication and collaboration between health professionals has proven beneficial, resulting in better patient outcomes.5 Considering that medications are prescribed by physicians in order for pharmacists to have them dispensed to patients, pharmacists' views on such collaboration give a clear illustration of what provides a well-functioning team result to help the patients.6 Therefore, the implementation of pharmaceutical care and collaborative healthcare practices is mandatory to identify, prevent and resolve any type of DTRP for a given patient.
In the UAE, community pharmacists often perform pharmaceutical care and encounter multiple barriers.7 Data from UAE showed that a vast majority of the community pharmacists do not provide enhanced professional services, less than one-third counseled patients on a regular basis and 92% of them did not maintain patient records.8 Based on these observations one can assume community pharmacists in UAE may not be actively looking for DTRPs in the prescriptions filled by them. In fact, pharmacists are the last line of defense between the patient and medication error. Hence, ensuring comprehensive knowledge regarding drug therapy-related problems is essential to achieve the therapy target. Further, the lack of knowledge may lead to serious outcomes. The majority of community pharmacists in UAE are from diverse educational and cultural backgrounds. Although identification of DTRPs is a primary responsibility of community pharmacists, data in this regard are lacking in the UAE. Understanding community pharmacists' ability to identify and resolve DTRPs can add valuable information to further enhance the community pharmacy practice in the country.
Knowing the existing professional collaboration between pharmacists and physicians also throws light on the prevailing safety culture existing in community pharmacy practice settings. With this in view, it is important to employ a suitable method to assess the real practice; this can be largely achieved using simulated patient research. The simulated patient method is a valuable research method to uncover real practice issues and is widely used in the UAE9,10 and other countries in the region.11–14 This method of research is often able to identify real practice challenges and lacunae in community pharmacy practice15–17 and hence is employed more commonly these days.
Objectives
The aim of this study is to assess the ability of community pharmacists to identify DTRPs in prescriptions, to analyze their dispensing, counseling and labeling practices and to assess the level of interprofessional collaboration among community pharmacists and physicians to mitigate identified DTRPs.
Methods
Study Design
This research made use of a simulated-patient method in which trained simulated patients (final- year BSc Pharm students) visited community pharmacies (n = 50) with dummy prescriptions containing DTRPs (Figure 1). Simulated patient research is often used to unrcover real-life practices and can report the real practices, eliminating potential biases. In this research this method was chosen so as to identify the real practice trends of community pharmacists in identifying DTRPs in prescriptions and their collaboration with prescribers.
 |
Figure 1 Study design of the simulated patient research. |
Ethical Approval
This research was approved by the Undergraduate Research Ethical Committee, College of Pharmacy and Health Sciences, Ajman University with ethical approval number PHA-UH-20-03-30. The community pharmacists were not informed about the data collection process since scientific validity of the research is a major concern and this is possible only when the respondents (the community pharmacists) are completely unaware of the fact that they are being investigated. Moreover, this research caused no any damage to the respondents/subjects, confidentiality was maintained and policy-relevant data were gathered with potential to generate socially valuable knowledge.18 The method of data collection followed in this research was reviewed by the ethical committee and approved. Further, strict anonymity was maintained throughout the research process, and the data collectors took a self-pledge on maintaining the confidentiality of the information.
Study Setting
Community pharmacists practicing in various community pharmacies in the emirate of Ajman, UAE were enrolled in the research. The study was conducted during February 2020, prior to the start of the Covid-19 pandemic in the country.
Selection of Community Pharmacies
Fifty community pharmacies were selected based on easy accessibility for the research purpose. These 50 community pharmacists were selected conveniently based on ease of access to data collection, avoiding overcrowded pharmacies and geographically covering different places within the study area. A detailed stratification of study sites was not performed since that was beyond the scope of the research.
Training of Simulated Patients
Five final-year BSc Pharm female students from Ajman University served as simulated patients. They were trained by the researchers to act as patients’ relatives asking for medications. The researchers trained the simulated patients on aspects related to presentation of prescriptions, carefully listening to pharmacists and filling the checklist used as data collection form. The pilot study conducted with one prescription for each simulated patient further provided them with more familiarity in the data collection process.
Simulated Patient Scenarios
A total of five dummy prescriptions covering five different aspects of drug therapy-related problems, categorized as per the PCNE Version 8 (wrong drug dose, wrong dosage form, wrong duration of treatment, wrong indication, treatment not indicated) were developed.1
Development of the Scenarios
Dummy prescriptions with five DTRP scenarios were developed by the researchers (Table 1). Medicines used in the prescriptions and patient conditions selected were the most common ones seen in community pharmacy practices. The content validity of the developed scenarios was ensured by sharing the prescriptions with other pharmacist experts and physicians. Dummy prescriptions were in the proper format of a standard prescription with the necessary information. The telephone number on the prescription was the controlled telephone number of a researcher in this study.
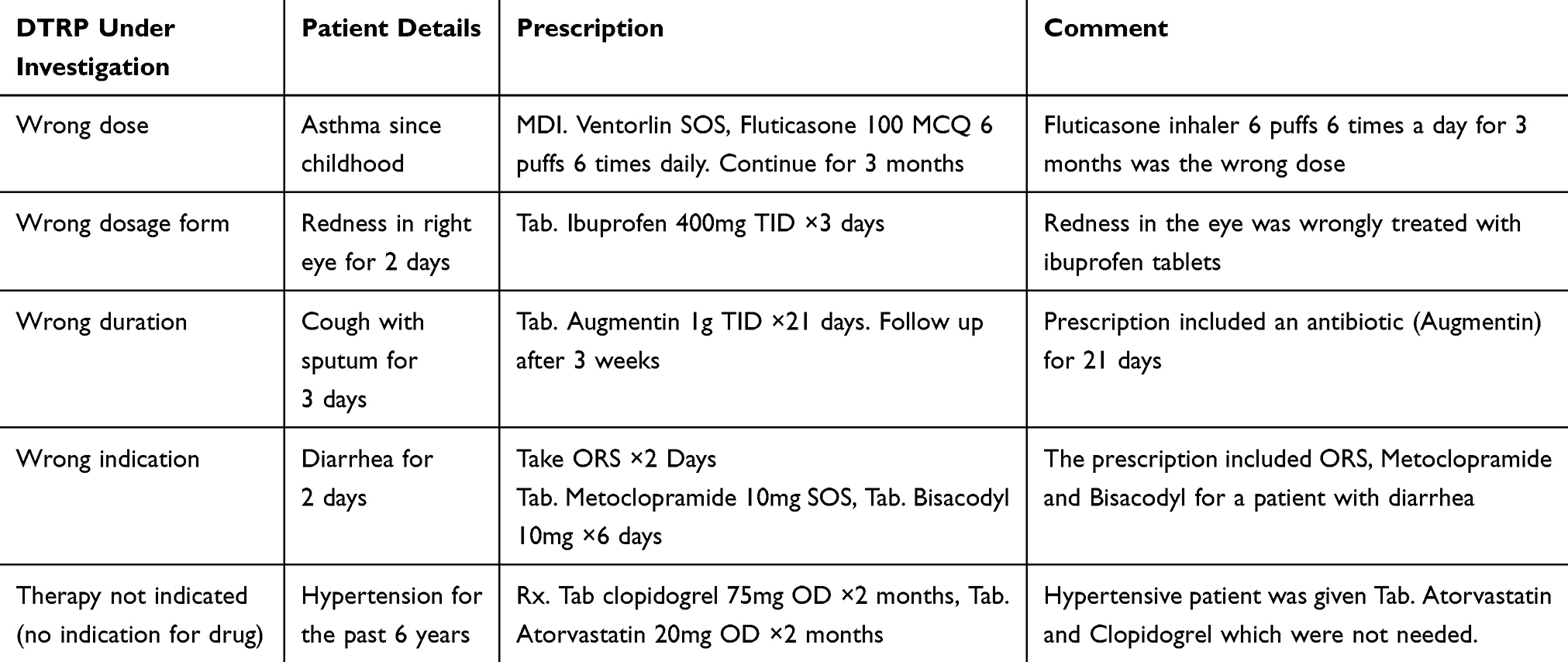 |
Table 1 DTRP Scenarios Assessed in the Study |
Data Collection
In this research, data collection was performed through face-to-face interaction by the SPs with the community pharmacists. Each SP visited ten different pharmacies and role-played the designated role with the allocated dummy prescriptions and asked for their prescriptions to be filled as predefined by the researchers in the study protocol. The researchers ensured that the study data collection was short, and pharmacies were approached only when the counters were empty and the simulated patients did not in any way crowd the counters.
Data Analysis
The students immediately after leaving the community pharmacy premises entered the information collected by them, such as ability of the pharmacists to identify the DTRP, their dispensing, counselling and labelling practices etc in a checklist designed as per the study objectives. Data were then organized and analyzed for the demography of the respondents, including history taking and reconciliation by the pharmacists, identification of DTRPs by the pharmacists and action taken by them in handling the identified DTRPs, labeling and counseling standards by the pharmacists and the practice of referring to DI sources by the pharmacists while checking for DTRPs in the prescriptions. Counseling and dispensing standards were further categorized as “low“, “average” and “high” as per a previously published study.12 Inferential statistics was performed using SPSS Version 26. Chi-square test was performed with alpha = 0.05.
Pilot Testing
Prior to starting the research, pilot testing was performed with one dummy prescription for each of the five scenarios, including changes made in the prescriptions as needed. The pilot study also served as a practice session for the simulated patients and improved their professional practice while performing as simulated patients in the main study.
Results
Demography of the Community Pharmacists
A total of 50 prescriptions with five different types of DTRPs were provided to participating students (simulated patients), and they in turn tested the ability of community pharmacists to identify the DTRPs and observed the actions taken accordingly. Of these 50 pharmacists, 39 (78%) were males and the remaining 11 (22%) females. Thirty-four (68%) were non-Arabs, and the remaining 16 (32%) were Arabs.
History Taking and Reconciliation by the Pharmacists
Of these 50 community pharmacists, seven (14%) took the medication history of the visiting simulated patients, one took medical history and none of them took history on allergy. Seven (14%) performed at least a few of the medication reconciliation steps.
Identification of DTRPs by the Pharmacists
Of the 50 pharmacists, 22 (44%) of them were able to identify the presence of DTRPs in the prescriptions produced by the simulated patients. Further details on the ability of the pharmacists in identifying the DTRPs are listed in Table 2.
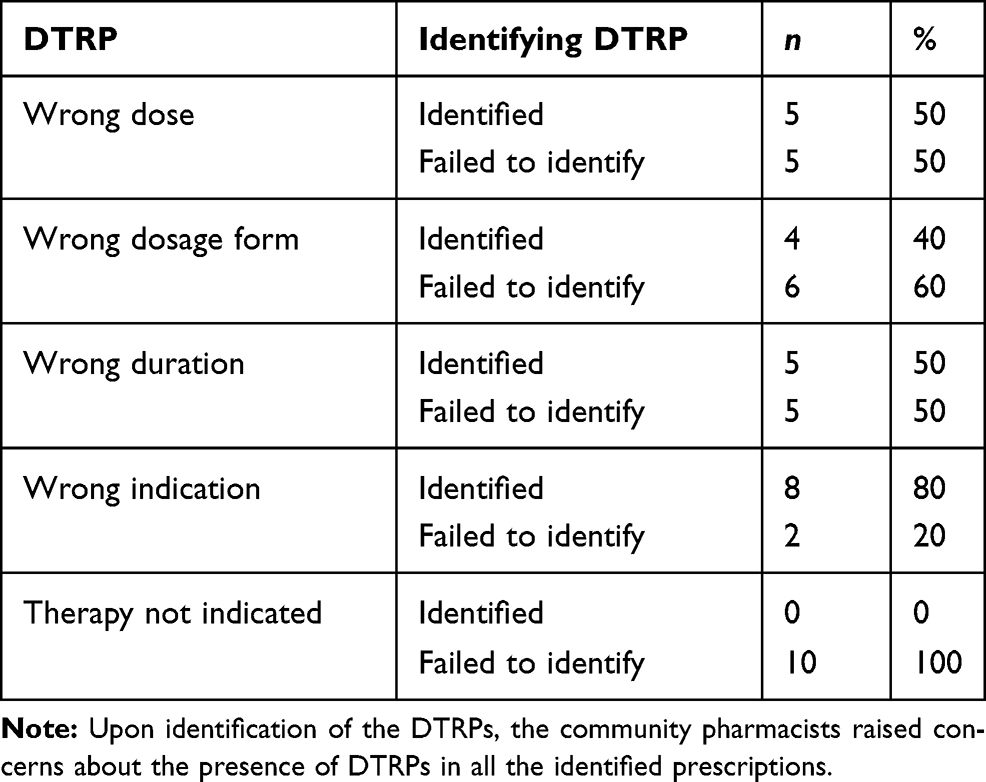 |
Table 2 Identification of DTRPs by the Pharmacists |
There was a statistically significant association between DTRP identification by pharmacists and labeling [chi-square = 7.879, p value = 0.019], reconciliation [chi-square = 10.359, p value = 0.001], counseling standard [chi-square = 19.0, p = 0.000] and physician visit suggestion [chi-square = 31.15, p = 0.000].
Action Taken by Pharmacists in Handling DTRPs
When the simulated patients presented to the pharmacies, six pharmacists (60%) dispensed the prescription with wrong medications, and eight (80%) dispensed the wrong dosage form. However, nine (90%) refused to dispense medications for wrong indications (Table 3).
 |
Table 3 Action Taken by Pharmacists for the DTRPs |
Labeling Standards
The assessment of labeling standards of the pharmacists while dispensing the medications for prescriptions with DTRPs indicated that labeling standards for prescriptions with the wrong dose were “low” in five (50%), “average“ in three (30%) and “good“ in two (20%) of the cases. Similarly, for the wrong dosage form, we found “low” standard in four (40%), “average” in two (20%) and “good” in four (40%) of the cases. For the wrong duration, the standards were “low” in three (30%), “average” in six (60%) and “good” in one (10%) of the cases. For prescriptions with “wrong indication”, the standards were “low” in one (10%), “average” in four (40%) and “good” in five (50%) of the cases. For prescriptions with therapy not indicated, the standards were “low” in six (60%) cases, “average” in three (30%) and “good” in one (10%) of the cases.
Patient Counseling Standards
The details on the counselling standards practiced by the pharmacists while counseling the patients with prescriptions containing DTRP are presented in Table 4.
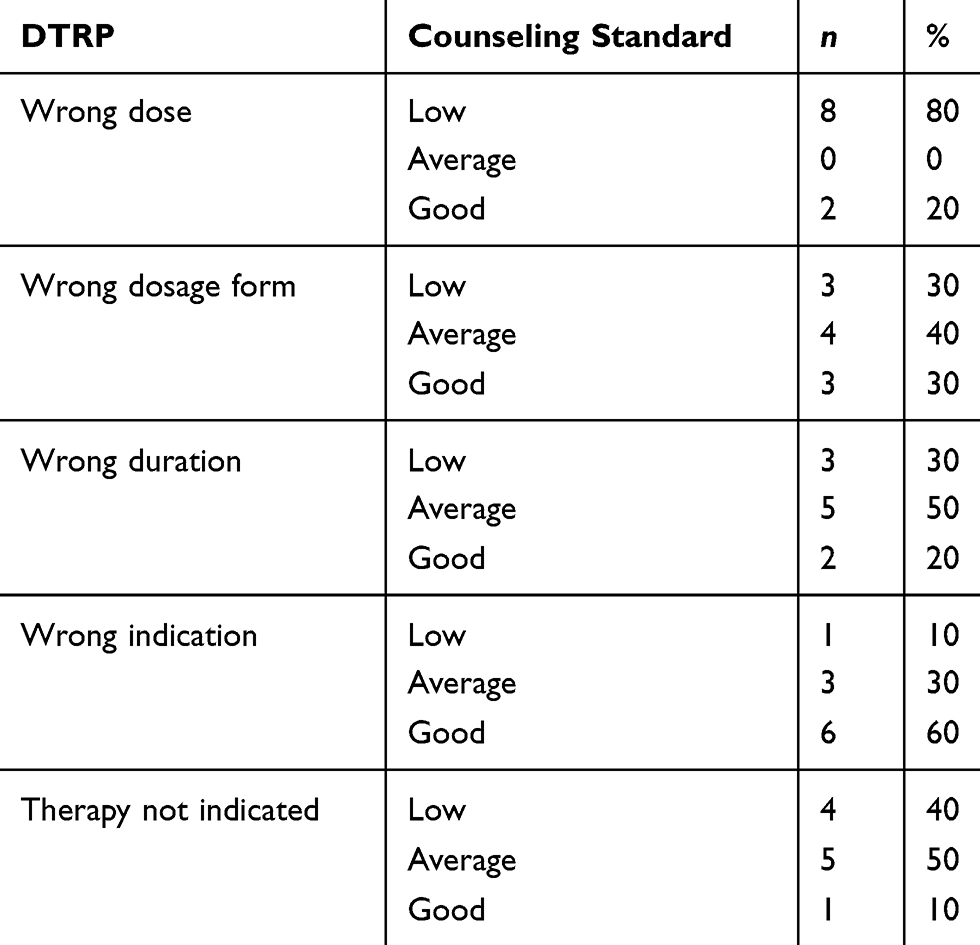 |
Table 4 Counseling Standards Maintained by the Pharmacists with Prescriptions Containing DTRPs |
The average time spent by the pharmacists in counseling was 80.38 ± 71.61 seconds. Further assessment showed that for the wrong dose no time was spent in three (30%) cases, less than one minute in three cases and more than one minute in the remaining four (40%) cases. For the wrong dosage form, five (50%) spent less than one minute and five (50%) more than one minute. A similar observation was noted for wrong duration. For the wrong indication, zero time was spent in one (10%) case, less than one minute in four (40%) cases and more than one minute in five (50%) cases. For prescriptions with therapy not indicated, less than one minute was spent in six (60%) cases, and more than one minute in the remaining four (40%) cases. The counseling standard had no significant association with counseling time [chi-square = 34.79, p = 0.250] and use of DI source [chi-square = 2.86, p = 0.243].
Dispensing Standards
The average time spent by the pharmacists in the dispensing process was 74.4 ± 73.05 seconds. A detailed assessment of dispensing process by the pharmacists is set out in Table 5.
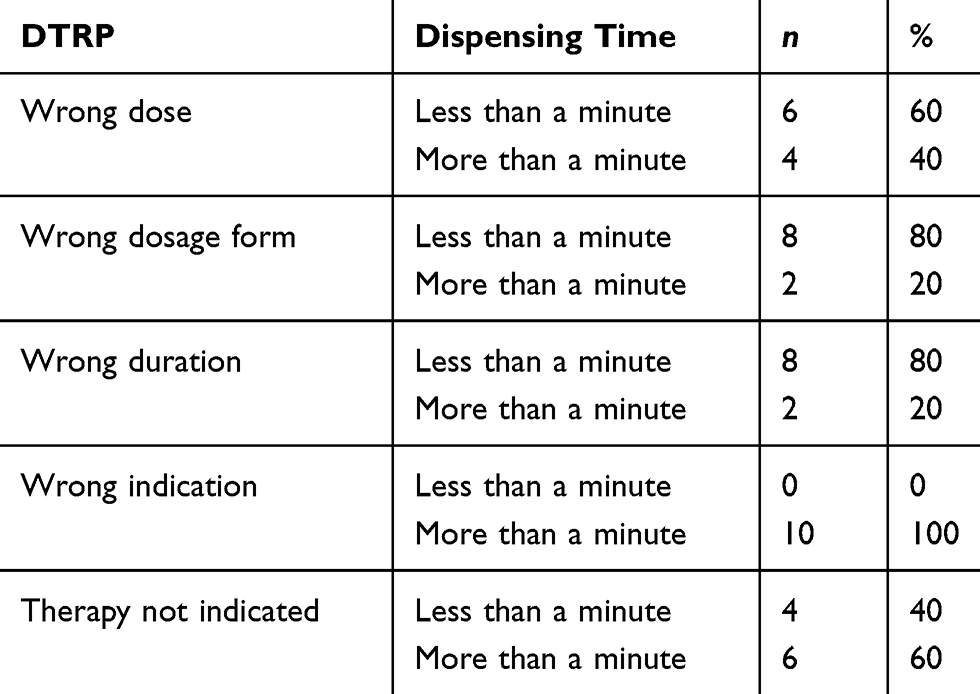 |
Table 5 Time Spent by Pharmacists in Dispensing the Prescriptions with DTRPs |
The instructions for medicine use was mentioned by one (10%) pharmacist among ten for those simulated patients with wrong dose, six (60%) in the wrong dosage form scenario, five (50%) in wrong duration of treatment, six (60%) in wrong indication and five (50%) in therapy not indicated.
Checking of DI Sources by the Pharmacists
While assessing the responses, it was found that five out of 50 (10%) pharmacists checked DI sources while handling prescriptions with DTRPs. Further analysis of these five pharmacists indicated that, for wrong dose, two (20%) checked DI sources and similarly for wrong dosage form one (10%), wrong duration none, wrong indication one (10%) and one (10%) for therapy not indicated.
Professional Collaboration Between the Pharmacists and Physician
Of the 50 pharmacists, none of them communicated with the physician who prescribed the medications. However, in 19 (38%) of the cases, the pharmacists recommended the simulated patients to consult their physician prior to taking the medications, Table 6.
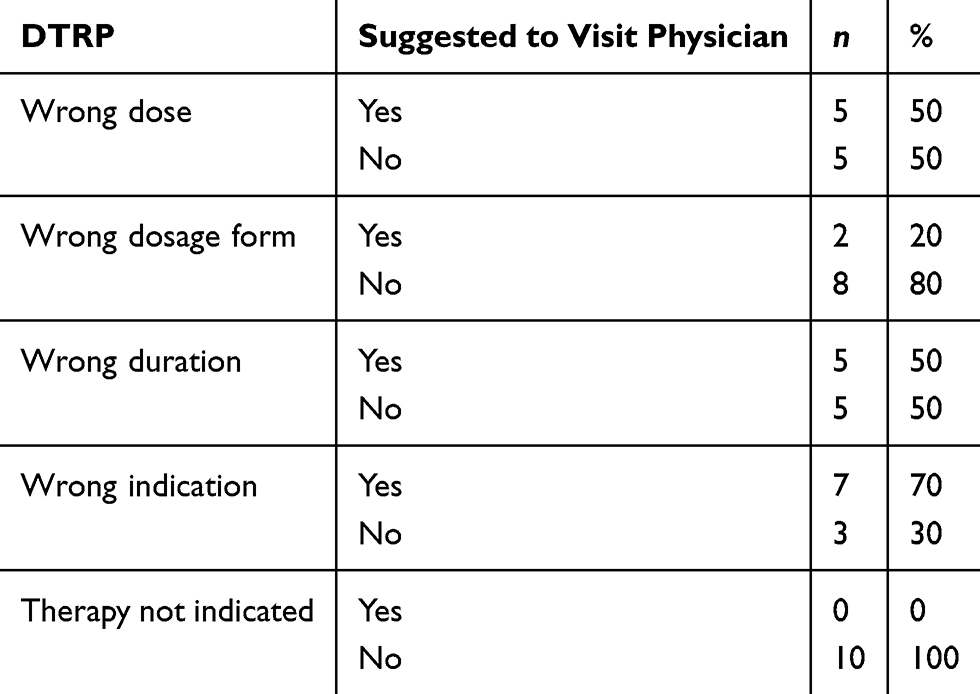 |
Table 6 Physician Visit Suggestion by the Pharmacists |
Discussion
Drug efficacy, safety and quality are essential for achieving the required therapeutic target with minimal side effects. Pharmacists play a crucial role in ensuring the drug efficacy and safety across the continuum of the healthcare process.19 To practice pharmacy in UAE, pharmacists have to pass a licensing exam and fulfill renewal requirements.20 In this study, authors identified the ability of community pharmacists to identify DTRPs in the prescriptions handled by them and their existing practices on collaborating with prescribers in the event of a potential DTRP. Present study findings indicate that more than half (56%) of the studied pharmacists were unable to detect DTRPs in the simulated prescriptions and ended up dispensing inappropriate medications.
Providing patient counseling is an important aspect of community pharmacy practice. Communicating with the patient and taking the proper time to counsel them is essential for several reasons. Proper counseling can simply be when the pharmacist asks the patient about medication and medical history. One common error during consultation is to ignore medication allergic reactions and their consequences on patient health.21 Only 14% of the pharmacists in this study asked about patient medication history before they dispensed the drugs to patients. Over 75% of the studied population spent less than one minute consulting the patient. Consequently, the labeling standard was almost always low, which is confirmed when we noticed that the dispensing time was also around one minute or less. Similar observations were noted in Qatar while dispensing to patients with acute gastroenteritis.12 This finding confirms that the pharmacists should spend more time in labeling the drugs and ensuring that the patient has sufficient knowledge about medications and possible drug–drug interactions and side effects.
The proportion of pharmacists who referred simulated patients to a physician was 38% in the tested population. It is important that community pharmacists refer patients back to the physician if they find any DTRP in the prescriptions.22 Interprofessional collaboration is an important component of pharmaceutical care2,23 and is crucial in minimizing DTRPs. The other 62% did not suggest a revisit to a physician for reassurance, and that can be due to different reasons; a significant reason can be the gap in interprofessional collaboration and communication. Improving collaboration would result in several advantages such as spreading confidence amongst team members, acquiring comprehensive patient-centered care, minimizing referrals and readmission rates or hospitalization needs, and promoting the mentality of equality amongst all levels in the healthcare profession. Undoubtedly one can say that teamwork improves patient care and minimizes harm to patients.
The wrong medication dose may lead to inadequate therapy (if the dose is inadequate) or harmful effects (if the dose is too high). Our findings showed that 60% of pharmacists dispensed the prescription with wrong medications and 80% dispensed using the wrong dosage form. However, the majority of pharmacists in this study (90%) refused to dispense medications for the wrong indication.
Common DTRPs resulting in emergency room visits are adverse drug reactions (ADRs), wrong medication and inappropriate prescribing. Most DTRPs result in the patient ending up in the emergency room due to wrong drug indication, ADRs or wrong dose.24 Presence of DTRPs in prescriptions could result in lower outcomes from the therapy plan, which are often collected by the pharmacist.25 Medications that present risks and are related to lethal drug interactions result in 3.1% of total patients admitted to the hospital, 6.4% of whom die. Three to 14% of total hospital admissions are associated with ADRs, which is one of the DTRPs.24 ADRs are one of the biggest challenges to the healthcare system as they increase the number of hospitalized patients. The goal of the therapy in this case is not reached, which also affects the quality of life.26 As an outcome, ADRs has generated an over-consumption of medical goods and services, which was accompanied by un-economical up-scale of prices within the medical system.26 Delaying the detection and correction of ADRs could lead to horrible outcomes and may even lead to mortality. In addition, drug–drug interactions may lead to extremely dangerous reactions and the need for hospitalization. The eye-catching problem which draws most attention to hospitalized cases is ADRs, even though the other DTRPs are nevertheless important. The benefits of interprofessional medical services such as pharmaceutical care groups can add to a progressively complete program supporting a patient’s medication use.27
Collaborating with the physician is very important for the pharmacist as it is important to be able to identify problems, especially as community pharmacists have some lack in the knowledge of the patient’s history or information, which can lead to dispensing errors. Therefore, communicating with patients would lead to better clinical decisions and treatment outcomes.28 Based on the research findings, the authors would recommend pharmacotherapy and clinical skills training for practicing community pharmacists. More researches on interprofessional collaboration among community pharmacists and physicians should be conducted to identify possible solutions to overcome the barriers.
The study was conducted in 50 pharmacies in one of the seven emirates in the country, and hence the findings cannot be generalized to the entire country’s practice. There is a possibility that the simulated patients might have failed to document/record some information while completing the checklist. This study also did not assess the clinical skills of the community pharmacists under study to identify DTRP, and the authors are unsure whether pharmacists possessed those necessary skills.
Conclusions
Although the community pharmacists were generally able to identify DTPRs, there exists no professional collaboration between CPs and physicians in resolving the identified DTRPs. However, a high percentage of the CPs recommended that SPs visit their physician prior to taking the prescription medications encountered with DTRPs. In general, the dispensing, counseling and labeling practices were below expectation because CPs spent minimal time engaging with the patients.
Acknowledgments
Authors would like to acknowledge Sara Mousa Dahe, Rim Khaled Intabli, Zahraa Mohammed Alkaram, Wafaa Mohammed Ali and Parwin Haseeb from the College of Pharmacy and Health Sciences, Ajman University, for their help in data collection.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
Authors declare no potential conflicts of interest with respect to research, authorship and/or publication of this article.
References
1. DRP classification, now V8.01. The pharmaceutical care network Europe. Available from: https://www.pcne.org/news/60/drp-classification-now-v801.
2. Cipolle R, Strand L. Drug therapy problems. In: Cipolle R, Strand L, Morley P, editors. Pharmaceutical Care Practice: The Clinician’s Guide.
3. Young SW, Bishop LD, Conway A. Interventions performed by community pharmacists in one Canadian province: a cross-sectional study. Ther Clin Risk Manag. 2012;8:415. doi:10.2147/TCRM.S37581
4. Ruths S, Viktil KK, Blix HS. Classification of drug-related problems. Tidsskr nor Laegeforen. 2007;127:3073–3076.
5. Zwarenstein M, Goldman J, Reeves S. Interprofessional collaboration: effects of practice‐based interventions on professional practice and healthcare outcomes. Cochrane Database Syst Rev. 2009;(3). doi:10.1002/14651858.CD000072.pub2
6. Hasan S, Stewart K, Chapman CB, Kong DC. Physicians’ perspectives of pharmacist-physician collaboration in the United Arab Emirates: findings from an exploratory study. J Interprof Care. 2018;32(5):566–574. doi:10.1080/13561820.2018.1452726
7. Ghazal R, Hassan NA, Ghaleb O, Ahdab A, Saliem II. Barriers to the implementation of pharmaceutical care into the UAE community pharmacies. IOSR J Pharm. 2014;4:68–74.
8. Hasan S, Sulieman H, Chapman CB, Stewart K, Kong DC. Community pharmacy services in the United Arab Emirates. Int J Pharm Pract. 2012;20(4):218–225. doi:10.1111/j.2042-7174.2011.00182.x
9. Mobark DM, Al-Tabakha MM, Hasan S. Assessing hormonal contraceptive dispensing and counseling provided by community pharmacists in the United Arab Emirates: a simulated patient study. Pharm Pract (Granada). 2019;17(2). doi:10.18549/PharmPract.2019.2.1465
10. Alomar MJ, Qandil S, Al-Hilwani HM, Malkat DM, Caroline C. Evaluation of the community pharmacist’s behavior towards a prescription of antidiabetic and antiasthma drugs. Pharm Pract (Granada). 2011;9(1):37. doi:10.4321/s1886-36552011000100006
11. Paravattil B, Kheir N, Yousif A. Utilization of simulated patients to assess diabetes and asthma counseling practices among community pharmacists in Qatar. Int J Clin. 2017;39(4):759–768. doi:10.1007/s11096-017-0469-8
12. Ibrahim MI, Palaian S, Al-Sulaiti F, El-Shami S. Evaluating community pharmacy practice in Qatar using simulated patient method: acute gastroenteritis management. Pharmacy Practice. 2016;14(4):800. doi:10.18549/PharmPract.2016.04.800
13. Mahmoud AA, Althobaiti OA, Althobaiti AE, Althomali AO, Yossef OM. Community pharmacists’ response to acute back pain: a simulated patient study in western region, Saudi Arabia. GSC Biol Pharma Sci. 2018;2(2):25–32. doi:10.30574/gscbps.2018.2.2.0008
14. Abdelaziz AI, Tawfik AG, Rabie KA, et al. Quality of community pharmacy practice in antibiotic self-medication encounters: a simulated patient study in upper Egypt. Antibiotics(Basel). 2019;8(2):35. doi:10.3390/antibiotics8020035
15. Elayeh ER, Hammad EA, Tubeileh RH, Basheti IA. Use of secret simulated patient followed by workshop-based education to assess and improve inhaler counseling in community pharmacy in Jordan. Pharm Pract (Granada). 2019;17(4):1661. doi:10.18549/PharmPract.2019.4.1661
16. Foroutan N, Dabaghzadeh F. Evaluating the practice of Iranian community pharmacists regarding oral contraceptive pills using simulated patients. Pharm Pract (Granada). 2016;14(4):745. doi:10.18549/PharmPract.2016.04.745
17. Surur AS, Getachew E, Teressa E, Hailemeskel B, Getaw NS, Erku DA. Self-reported and actual involvement of community pharmacists in patient counseling: a cross-sectional and simulated patient study in Gondar, Ethiopia. Pharm Pract (Granada). 2017;15(1):890. doi:10.18549/PharmPract.2017.01.890
18. Rhodes KV, Miller FG. Simulated patient studies: an ethical analysis. Milbank Q. 2012;90(4):706–724. doi:10.1111/j.1468-0009.2012.00680.x.
19. Sen S, Bowen JF, Ganetsky VS, et al. Pharmacists implementing transitions of care in inpatient, ambulatory and community practice settings. Pharm Pract (Granada). 2014;12(2).
20. Renewal of a license to practice as a pharmacist. United Arab Emirates: Ministry of Health and Prevention. Available from: https://www.mohap.gov.ae/en/services/Pages/336.aspx.
21. Kalliat R, Smith N, Graham-Clarke E. An audit of the completeness and accuracy of allergy-status documentation. Clin Pharm. 2010.
22. Snyder ME, Zillich AJ, Primack BA, et al. Exploring successful community pharmacist-physician collaborative working relationships using mixed methods. Res Social Adm Pharm. 2010;6(4):307–323. doi:10.1016/j.sapharm.2009.11.008
23. McGivney MS, Meyer SM, Duncan–Hewitt W, Hall DL, Goode JV, Smith RB. Medication therapy management: its relationship to patient counseling, disease management, and pharmaceutical care. J Am Pharm Assoc. 2007;47(5):620–628. doi:10.1331/JAPhA.2007.06129
24. Belayneh YM, Amberbir G, Agalu A. A prospective observational study of drug therapy problems in medical ward of a referral hospital in northeast Ethiopia. BMC Health Serv Res. 2018;18(1):808. doi:10.1186/s12913-018-3612-x
25. Al-Taani GM, Al-Azzam SI, Alzoubi KH, Aldeyab MA. Which drugs cause treatment-related problems? Analysis of 10,672 problems within the outpatient setting. Ther Clin Risk Manag. 2018;14:2273.
26. Niriayo YL, Kumela K, Kassa TD, Angamo MT, Frey R. Drug therapy problems and contributing factors in the management of heart failure patients in Jimma University Specialized Hospital, Southwest Ethiopia. PLoS One. 2018;13(10):e0206120. doi:10.1371/journal.pone.0206120
27. Peterson C, Gustafsson M. Characterisation of drug-related problems and associated factors at a clinical pharmacist service-naive Hospital in Northern Sweden. Drugs Real World Outcomes. 2017;4(2):97–107. doi:10.1007/s40801-017-0108-7.
28. Patel M, Campbell M, Moslem M, Spriggel P, Warholak T. Identifying drug therapy problems through patient consultation at community pharmacies: a quality improvement project. J Patient Saf. 2020;16(1):19–23. doi:10.1097/PTS.0000000000000228
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.