Back to Journals » Clinical Ophthalmology » Volume 20
Patient Reported Outcomes and Visual Acuity After Bilateral Implantation of a Next Generation Presbyopia Correcting Intraocular Lens
Authors Hacopian AG, Brunson PB, Hall B ![]()
Received 8 October 2025
Accepted for publication 27 January 2026
Published 5 February 2026 Volume 2026:20 572703
DOI https://doi.org/10.2147/OPTH.S572703
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Bharat Gurnani
Alexander G Hacopian,1 Phillip B Brunson,1 Brad Hall2
1Mann Eye Institute, Houston, TX, USA; 2Sengi, Penniac, NB, Canada
Correspondence: Phillip B Brunson, Mann Eye Institute, 5115 Fannin St Suite 1000, Houston, TX, 77004, USA, Tel +1-713-580-2500, Email [email protected]
Purpose: To evaluate 3-month postoperative outcomes for bilateral implantation of a next generation presbyopia correcting intraocular lens (IOL).
Methods: This was a single center, ambispective study of visual outcomes after successful bilateral cataract surgery (with presbyopia-correcting intent) and TECNIS Odyssey implantation. Subjects were assessed 3 months postoperatively during a single visit. Clinical evaluations included measurement of visual acuities at distance, intermediate, near, and extreme near, and administration of the assessment of intraocular lens implant symptoms (AIOLIS) and ocular surface disease index (OSDI) questionnaires.
Results: A total of 40 subjects completed the study. Mean photopic binocular uncorrected visual acuities at 6 m, 66 cm, 40 cm, and 33 cm were − 0.05 ± 0.06, 0.02 ± 0.12, 0.04 ± 0.10, and − 0.02 ± 0.07 logMAR, respectively. The most commonly reported dysphotopsias (percentage of subjects experiencing them “Always”) were halos at 32% (13/40), glare at night at 30% (12/40), and rings or spiderwebs at 18% (7/40). However, only 0% (0/40), 5% (2/40), and 2% (1/40) of subjects were “Extremely” bothered by halos, glare at night, and rings or spiderwebs, respectively. In addition, 80% (36/40) of subjects reported needing glasses “Not at all” or “A little of the time”, and 100% (40/40) of subjects were satisfied with their vision.
Conclusion: The results of this study suggest excellent visual outcomes at distance, intermediate, near, and extreme near, high spectacle independence, and high patient satisfaction with bilateral Odyssey implantation.
Keywords: cataract, odyssey, continuous range of vision
Introduction
Many cataract surgery patients desire clear vision at all ranges including distance, intermediate, near, and extreme near. There are a variety of intraocular lenses (IOLs) designed to fill this need; however, each type makes particular compromises. The most commonly implanted IOL is the monofocal IOL, which provides clear vision for distant objects, but patients still require spectacles to see objects at arm’s length or closer. The optic design of traditional monofocals can be modified to achieve functional vision at intermediate.1 However, there are reports that the functional intermediate vision provided by enhanced monofocal IOLs is not superior to that of traditional monofocal IOLs.2
Multifocal IOLs aim to split incoming light into more than one distinct focal points, enabling clear vision at distance, intermediate, near, and extreme near.3,4 However, patients may experience unwanted visual disturbances.5 Extended depth of focus (EDOF) IOLs are designed to provide a single continuous focal point for clear vision at distance, intermediate, and near.6 Although there may be fewer visual disturbances and better contrast sensitivity compared to multifocal IOLs, EDOF IOLs may not provide as clear vision when viewing near objects.7
The TECNIS Odyssey IOL (Johnson & Johnson Vision) is a presbyopia correcting IOL that combines multifocal and EDOF technologies.8 The posterior optic of the lens is a derivative of the posterior optic in the TECNIS Synergy IOL (Johnson & Johnson Vision), but it uses different ring diameters and step heights. The anterior optics of the Odyssey and Synergy IOLs are similar and incorporate diffractive designs. The optic diameters of both the Odyssey and Synergy IOLs are 6 mm with the same overall IOL length of 13 mm. The Synergy IOL has been observed to provide good visual outcomes for patients at all ranges of vision,3,9–11 Including extreme near (33 cm), which is increasingly important for viewing handheld devices such as smartphones. However, there are minimal data reported regarding the performance of the Odyssey IOL.
Patients experience a variety of lighting conditions day-to-day. Fluctuations in illumination affect pupil size, which in turn influences the effective optical zone of the IOL, the distribution of the incoming light, and the magnitude of optical aberrations. Evaluating visual outcomes under different lighting levels can give a clearer understanding of overall IOL performance. In particular, testing under mesopic conditions provides insights into IOL performance in low-light environments, where pupil dilation may reduce contrast sensitivity and increase dysphotopsias.
The purpose of this study was to evaluate 3-month postoperative outcomes for bilateral implantation of the Odyssey IOL in photopic and mesopic conditions.
Methods
This was a single site, single arm, ambispective study conducted in private practice. An independent institutional review board (Advarra IRB) reviewed and approved the study (approval Pro00081194). All participants gave written informed consent. The study was conducted in compliance with the tenets of the Declaration of Helsinki, Good Clinical Practice (GCP), and International Harmonization (ICH) guidelines, and was registered on clinicaltrials.gov (NCT06550375). Data are not available for sharing.
The study included subjects 50 years and older who had bilateral cataract surgery with presbyopia-correcting intent and TECNIS Odyssey IOL implantation. Subjects were excluded who had significant ocular comorbidities (eg, macular degeneration, glaucoma), were less than 2 weeks post YAG capsulotomy, or had best corrected distance visual acuity worse than 20/25.
Preoperative biometry was performed using the IOLMaster 700 (Carl Zeiss Meditec AG) and corneal tomography and anterior-segment optical coherence tomography (OCT) were performed using the Pentacam Cornea OCT (OCULUS Optikgeräte GmbH). The Barrett True K formula was used for preoperative planning. All subjects underwent femtosecond laser assisted cataract surgery with the Catalys Precision Laser System (Johnson & Johnson Vision). Eye with ≥ 1.0 D of astigmatism were implanted with a toric IOL, while eyes with < 1.0 D of astigmatism received limbal relaxing incisions.
Subjects were evaluated at least 3 months postoperative at a single visit. Monocular and binocular uncorrected and distance-corrected visual acuities distance (UDVA, CDVA; 6 m), intermediate (UIVA, DCIVA; 66 cm), and near (UNVA, DCNVA; 40 cm and 33 cm) were evaluated under photopic (85 cd/m2) and mesopic (3 cd/m2) conditions using a fixed sequence. Distance visual acuities were measured in a mirrored testing lane using a standard Early Treatment Diabetic Retinopathy (ETDRS) chart and recorded in logMAR. A manifest refraction was performed, and subjects were administered the Assessment of Intraocular Lens Implant Symptoms Questionnaire (AIOLIS) and Ocular Surface Disease Index (OSDI) questionnaires. The AIOLIS questionnaire asks subjects to rate the frequency and bothersomeness of common dysphotopsias, rate their spectacle independence, and rate their vision. The OSDI questionnaire is a tool to assess dry eye symptoms and their visual impact.
The software R (version 4.4.2; The R Foundation for Statistical Computing, Vienna, Austria) was used for all statistical analysis. Comparisons of photopic and mesopic visual acuities were done using linear mixed effects models. A p-value ≤ 0.05 was considered significant. Using sample sizes from other single arm studies,12–14 it was estimated that 35 subjects (70 eyes) would provide sufficient data to characterize the clinical performance of the lens. To allow for dropout, 40 subjects (80 eyes) were targeted.
Results
A total of 40 subjects (80 eyes) completed the study. The average age of subjects was 63.6 ± 6.9 years, and there were 30 female participants (75%). Mean mesopic pupil size was 4.1 ± 1.1 mm.
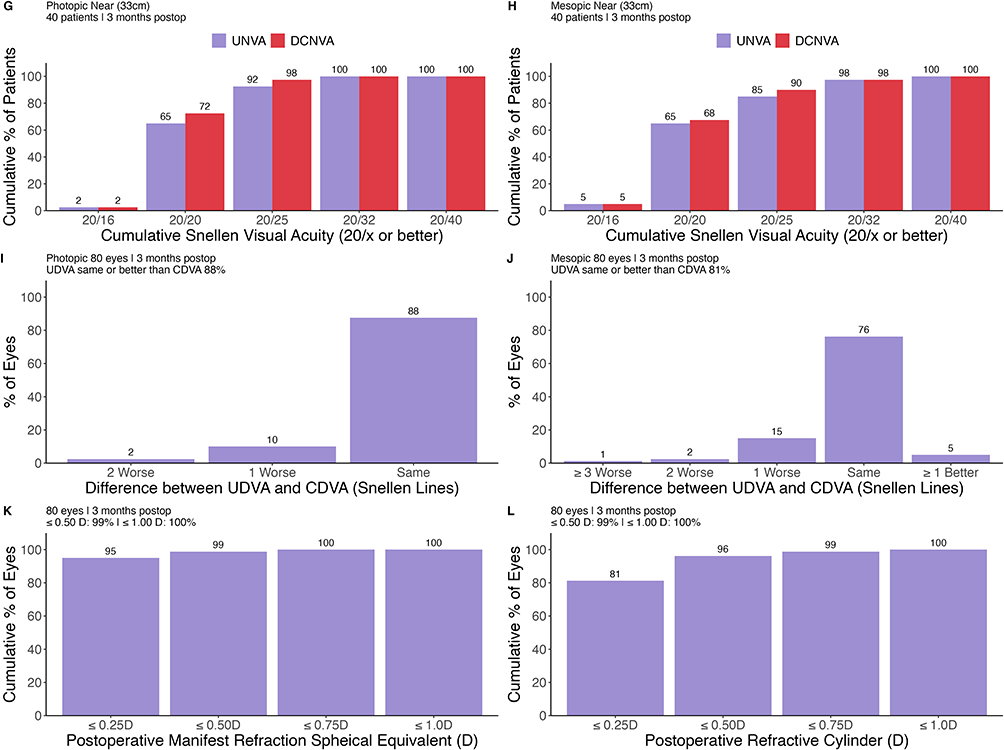
Standard efficacy plots for presbyopia correcting IOLs are shown in Figure 1. Under photopic and mesopic conditions, postoperative monocular UDVA and CDVA were within 1 line in 98% and 96% of eyes, respectively. The percentages of eyes with ≤ 0.5 D of manifest refraction spherical equivalent (MRSE) and residual astigmatism were 99% (79/80) and 96% (77/80), respectively.
Figure 1 continued. Figure 1 Standard efficacy plots for presbyopia correcting intraocular lenses. Cumulative percentage of patients achieving binocular uncorrected and distance corrected visual acuities, under photopic conditions at (A) far, (C) intermediate, (E) near, and (G) extreme near distances. Cumulative percentage of patients achieving binocular uncorrected and distance corrected visual acuities, under mesopic conditions at (B) far, (D) intermediate, (F) near, and (H) extreme near distances. Difference in lines between postoperative UDVA and CDVA under (I) Photopic and (J) Mesopic conditions. (K) Postoperative manifest refraction spherical equivalent distribution and (L) postoperative refractive cylinder distribution.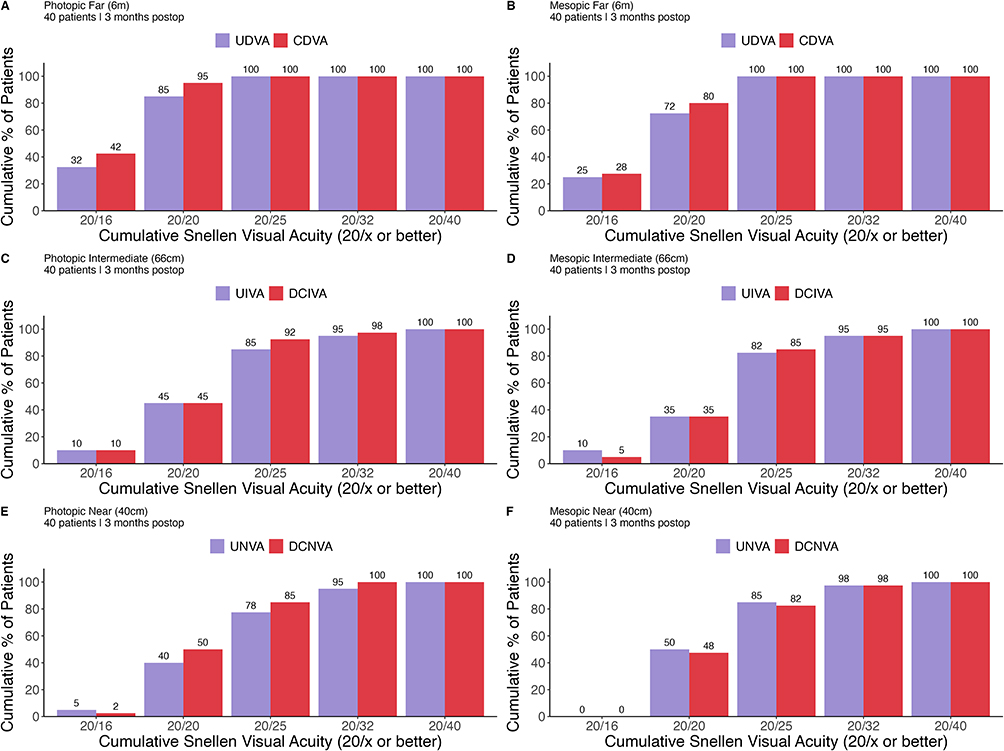
Visual outcomes are summarized in Table 1. Binocular visual acuities were 20/25 or better, under photopic conditions, for 100% (40/40) subjects at distance, 85% (34/40) at Intermediate, 78% (31/40) at near, and 92% (37/40) at extreme near. Likewise, binocular visual acuities under mesopic conditions were 20/25 or better in 100% (40/40) of subjects at distance, 82% (33/40) at intermediate, 85% (34/40) at near, and 85% (34/40) at extreme near. Figure 2 summarizes the linear mixed effects model-based estimated marginal means and 95% confidence intervals. There were minimal differences between visual acuities under photopic and mesopic conditions. Although there was a statistically significant difference was for UDVA (p = 0.032).
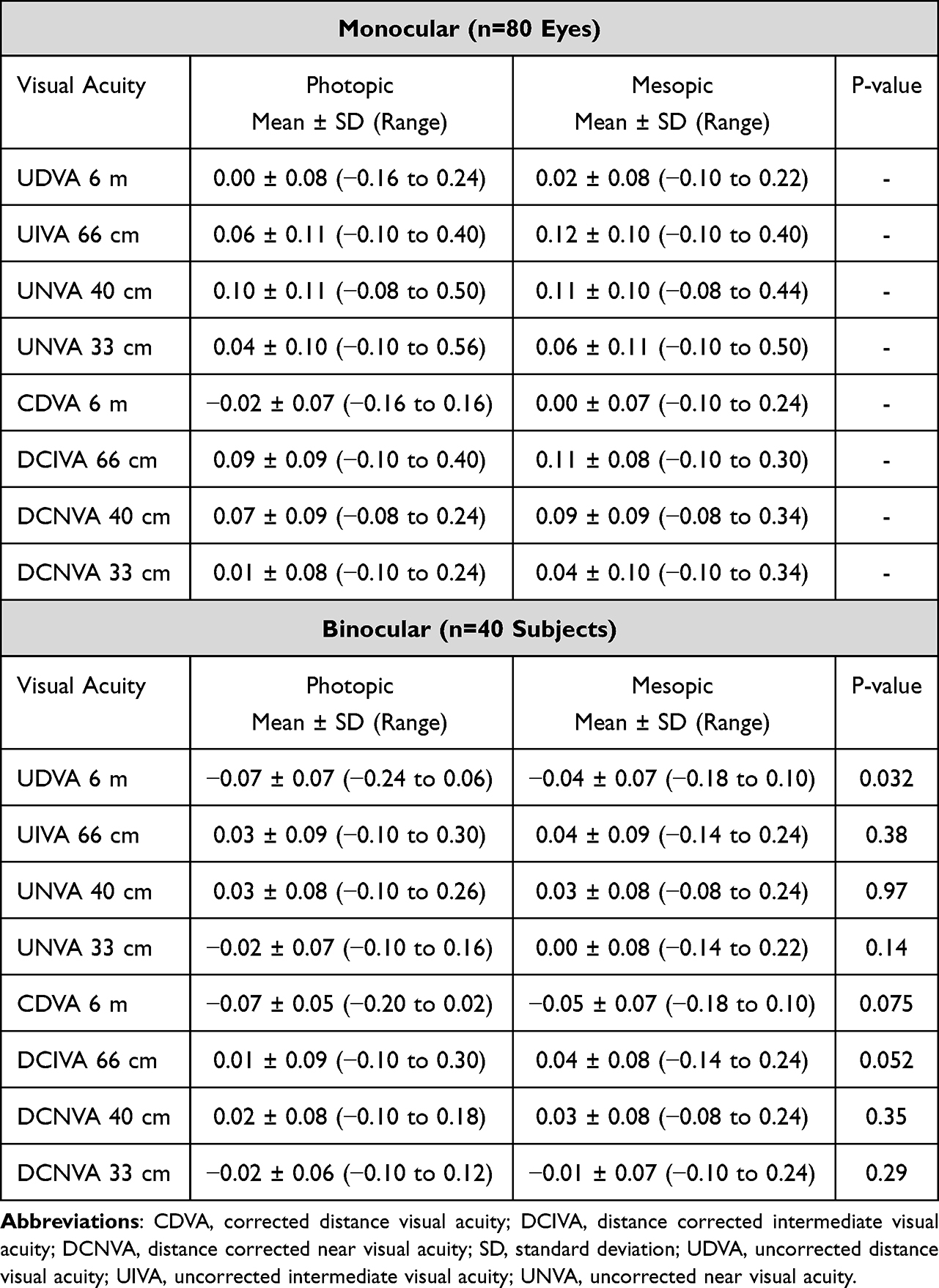 |
Table 1 Visual Outcomes Under Photopic and Mesopic Conditions |
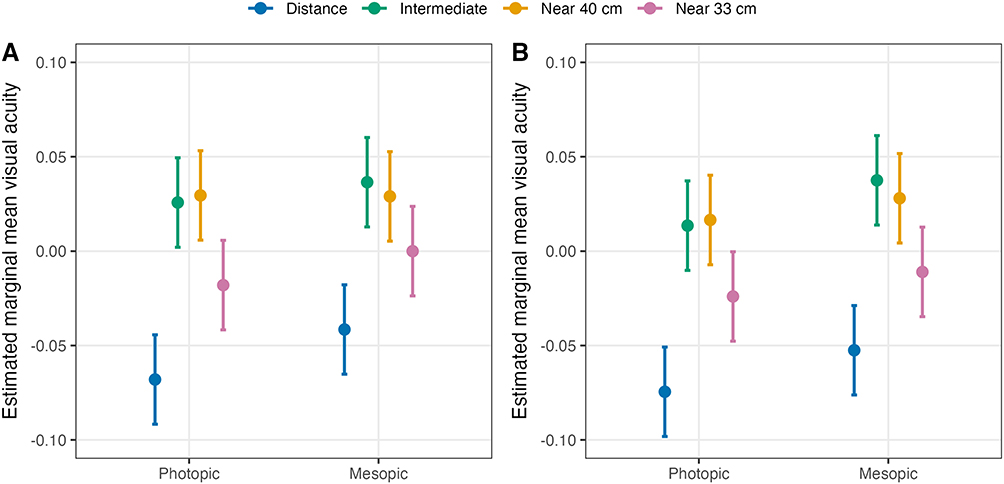 |
Figure 2 Model-based estimated marginal means (± 95% confidence intervals) for photopic and mesopic (A) uncorrected and (B) distance-corrected visual acuities. |
The percentages of subject responses when asked about the frequency and bothersomeness of each dysphotopsia are summarized in Table 2. The highest percentage of subjects reported experiencing halos, glare at night, and rings or spiderwebs “Always”. However, very few subjects reported that they were “Extremely” bothered by halos, glare at night, or rings or spiderwebs.
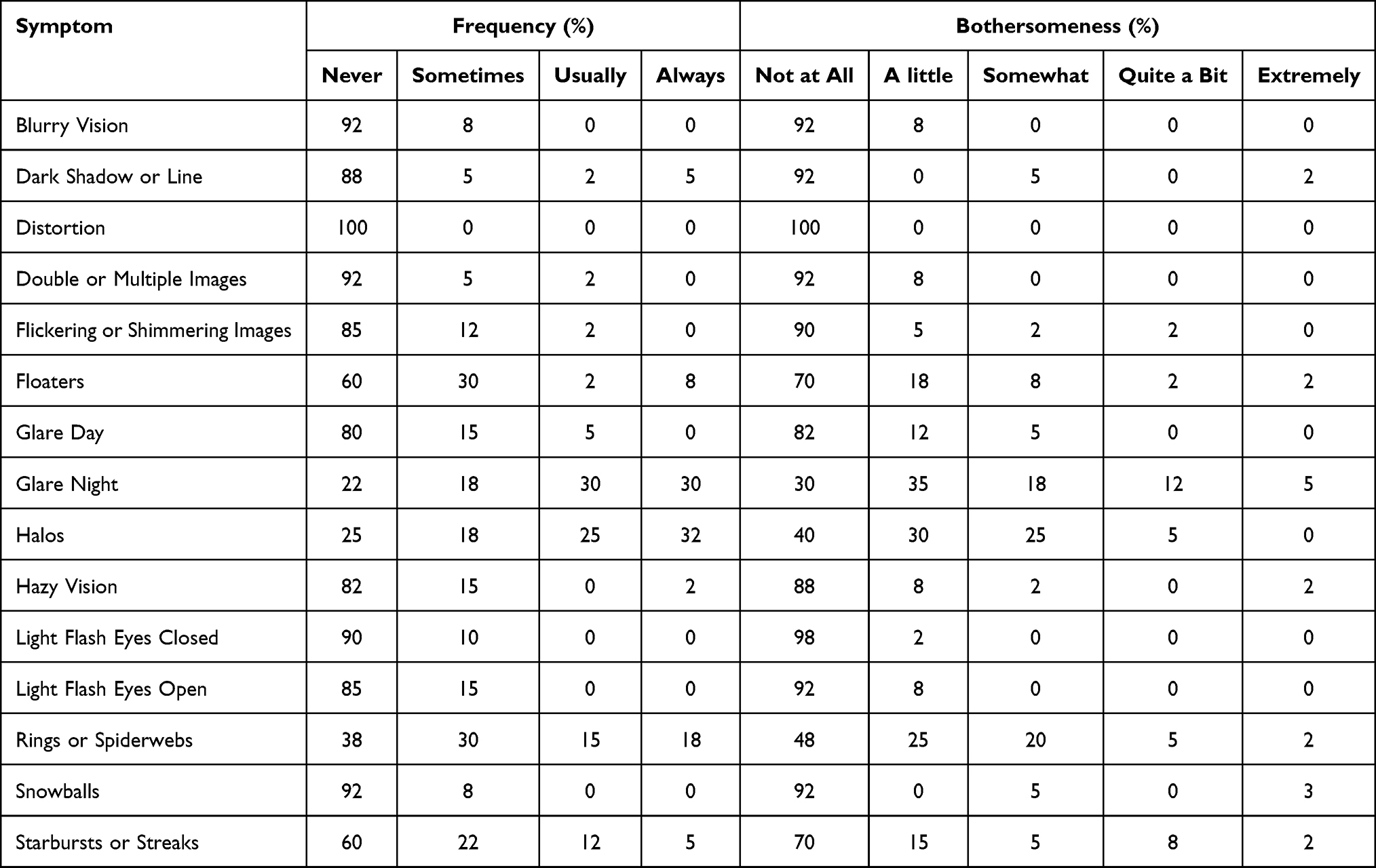 |
Table 2 Responses About Visual Disturbances on the AIOLIS Questionnaire (n=40) |
Table 3 summarizes how subjects rated their vision using the AIOLIS questionnaire. The percentage of subjects that rated their vision as “Excellent” or “Very Good” was 85% (34/40) overall, 100% (40/40) at distance, 88% (35/40) at intermediate, and 77% (31/40) at near. In addition, 100% (40/40) indicated that they were completely, very, or somewhat satisfied with their vision and 100% (40/40) reported seeing perfectly, very, or pretty well. Finally, 85% (34/40) indicated that they were completely spectacle independent (responding “Not at all” when asked about spectacle or contact lens wear in the last 7 days). As an exploratory outcome measure, we observed a weak Spearman correlation (ρ = 0.28) between pupil size (average across both eyes) and satisfaction, with smaller pupil sizes associated with greater satisfaction. Mean score on the OSDI questionnaire was 14.6 ± 11.7.
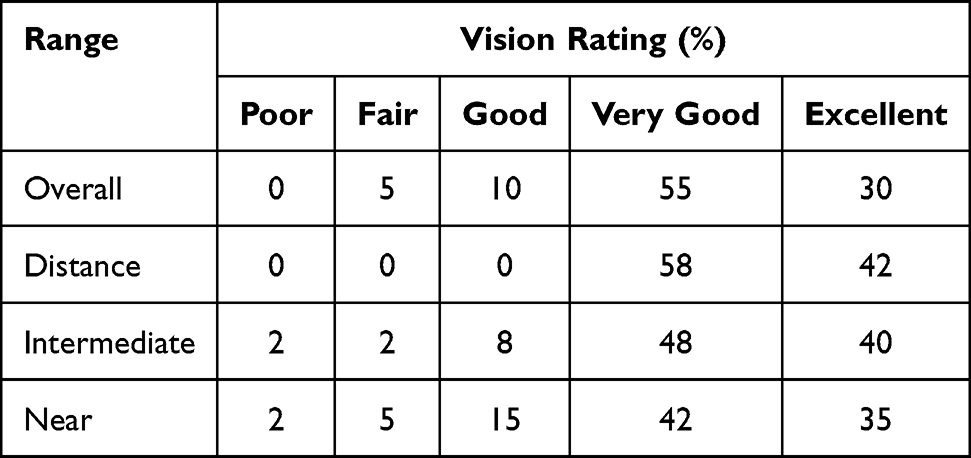 |
Table 3 Responses About Vision on the AIOLIS Questionnaire (n=40) |
Discussion
Cataract surgery patients increasingly desire clear vision at all ranges (distance, intermediate, and near). In this study, we evaluated the visual outcomes of a new presbyopia correcting IOL that combines multifocal and EDOF technologies. Under photopic conditions, UDVA, UIVA, UNVA 40 cm and UNVA 33 cm were −0.07 logMAR (20/17 Snellen equivalent), 0.03 logMAR (20/21 Snellen equivalent), 0.03 logMAR (20/21 Snellen equivalent), and −0.02 logMAR (20/19 Snellen equivalent), respectively. There are minimal data on outcomes with the Odyssey IOL. However, the Synergy IOL offers a reasonable comparison as the Odyssey IOL is the next generation of the TECNIS platform. A large randomized control trial of the Synergy IOL reported that bilateral UDVA, UIVA, UNVA 40 cm were 0.02 logMAR, 0.02, logMAR, and 0.06 logMAR, respectively, under photopic conditions in 131 subjects.10 Modi et al,15 in a multicenter prospective study of 138 subjects bilaterally implanted with the Synergy IOL, observed that UDVA, UIVA, UNVA 40 cm and UNVA 33 cm were 0.05 logMAR, 0.09, logMAR, 0.14 logMAR, 0.23 logMAR, respectively, under photopic conditions. In an ambispective study of 77 subjects bilaterally implanted with the Synergy IOL, Micheletti et al3 reported that UDVA, UIVA, UNVA 40 cm and UNVA 33 cm were 0.00 logMAR, 0.00, logMAR, 0.03 logMAR, 0.04 logMAR, respectively, under photopic conditions. Other studies have reported similar results to our study following bilateral implantation with the Synergy IOL.11,16
Patients experience a variety of lighting conditions in their everyday lives. Thus, it is crucial to understand the visual outcomes of the Odyssey IOL under mesopic conditions. In our study, binocular UDVA, UIVA, UNVA 40 cm and UNVA 33 cm were −0.04 logMAR, 0.04, logMAR, 0.03 logMAR, 0.00 logMAR, respectively, under mesopic conditions. De Rojas et al11 reported that binocular UIVA, UNVA 40 cm, and UNVA 33 cm were 0.23, logMAR, 0.22 logMAR, 0.23 logMAR, respectively, under mesopic conditions, higher than our study. In addition, Modi et al15 observed that DCIVA, DCNVA 40 cm, and DCNVA 33 cm were 0.33 logMAR, 0.35 logMAR, and 0.41 logMAR, respectively, and under mesopic conditions, compared to 0.04 logMAR, 0.03 logMAR, and −0.01 logMAR, respectively, in our study. Chang et al10 also reported mesopic binocular DCNVA 40 cm of 0.24 logMAR.
An exploratory endpoint of our study was to compare photopic and mesopic conditions using linear mixed effects modelling. The only statistically significant difference was for UDVA (p = 0.032). However, the mean difference was 1.5 letters, suggesting a clinically insignificant difference.17 The results of our study suggest similarly excellent visual acuities under both mesopic and photopic conditions.
Dysphotopsias are a concern with any presbyopia correcting IOL. In our study, glare at night, halos, and rings or spiderwebs were reported by patients as the most frequent and most bothersome visual disturbances on the AIOLIS questionnaire. However, we note that previous studies of the Synergy IOL used a variety of questionnaires, which makes comparisons difficult. Micheletti et al,2 using the Questionnaire for Visual Disturbances, observed that starburst, halos, and glare had the highest frequency and bothersomeness as reported by patients. De Rojas et al11 stated that halos, light sensitivity, and starbursts were the most frequently reported visual disturbance on the Patient Reported Visual Symptoms Questionnaire; however, halos, glare, and starbursts had the highest percentages of patients reporting an extreme degree of bother. Finally, Dick et al9 observed that the most frequently patient-reported visual disturbance was halos (reported by 44.2% of subjects), with most cases having a severity of mild to moderate.
The primary limitation of this study was the lack of a comparator group. We summarized the results from previous studies of the Synergy IOL, however a direct comparison between the Synergy and Odyssey, or the Odyssey and other presbyopia correcting IOLs would allow for more robust conclusions about the performance of the Odyssey IOL. However, given the scarcity of data for the Odyssey IOL, our study is a good indication of the real-world clinical outcomes of this IOL. Another limitation of this study was the relatively short follow-up period, as we are not able to draw long-term conclusions about the performance of the Odyssey IOL. In addition, dysphotopsias may improve over 6 to 12 months compared to 3 months posteroperatively. Although a 3 months postoperative follow-up is typical of an ambispective, single-arm study.
In conclusion, the results of this study suggest excellent photopic and mesopic visual outcomes at distance, intermediate, near, and extreme near, high spectacle independence, and high patient satisfaction with bilateral Odyssey implantation.
Acknowledgment
Melissa Wright from Mann Eye Institute and Laser Centers assisted with data collection and data checking. This paper was presented at the 2025 American Society of Cataract and Refractive Surgery (ASCRS) Annual Meeting as a conference paper.
Funding
This study was supported with an investigator-initiated study grant from Johnson & Johnson, Jacksonville, FL, USA.
Disclosure
Brad Hall reports independent contractor fees from Topcon Healthcare Inc. The authors report no other conflicts of interest in this work.
References
1. Tognetto D, Cecchini P, Giglio R, Turco G. Surface profiles of new-generation IOLs with improved intermediate vision. J Cataract Refract Surg. 2020;46(6):902–8. doi:10.1097/j.jcrs.0000000000000215
2. Micheletti JM, Duncan NB, Hall B. Head-to-head comparison of intermediate vision of two monofocal intraocular lenses. Clin Ophthalmol. 2023;17:3983–3990. doi:10.2147/OPTH.S444696
3. Micheletti J, Hall B, Smiley H, Langston W. Visual outcomes and patient satisfaction of two continuous range of vision intraocular lenses. Clin Ophthalmol. 2025;19:309–316. doi:10.2147/OPTH.S504090
4. Kohnen T, Herzog M, Hemkeppler E, et al. Visual performance of a quadrifocal (trifocal) intraocular lens following removal of the crystalline lens. Am J Ophthalmol. 2017;184:52–62. doi:10.1016/j.ajo.2017.09.016
5. Hovanesian JA, Jones M, Allen Q. The PanOptix trifocal IOL vs the ReSTOR 2.5 active focus and ReSTOR 3.0-add multifocal lenses: a study of patient satisfaction, visual disturbances, and uncorrected visual performance. Clin Ophthalmol. 2021;15:983–990. doi:10.2147/OPTH.S285628
6. Kohnen T, Suryakumar R. Extended depth-of-focus technology in intraocular lenses. J Cataract Refract Surg. 2020;46(2):298–304. doi:10.1097/j.jcrs.0000000000000109
7. Schallhorn JM. Multifocal and extended depth of focus intraocular lenses: a comparison of data from the United States food and drug administration premarket approval trials. J Refract Surg. 2021;37(2):98–104. doi:10.3928/1081597X-20201111-02
8. JJVCI. TECNIS Odyssey™ IOL with TECNIS SIMPLICITY™ delivery system. Instructions for use. 2024.
9. Dick HB, Ang RE, Corbett D, et al. Comparison of 3-month visual outcomes of a new multifocal intraocular lens vs a trifocal intraocular lens. J Cataract Refract Surg. 2022;48(11):1270–1276. doi:10.1097/j.jcrs.0000000000000971
10. Chang DH, Hu JG, Lehmann RP, Thompson VM, Tsai LH, Thomas EK. Clinical performance of a hybrid presbyopia-correcting intraocular lens in patients undergoing cataract surgery in a multicenter trial. J Cataract Refract Surg. 2023;49(8):840–847. doi:10.1097/j.jcrs.0000000000001205
11. De Rojas JO, Sandoval HP, Potvin R, Solomon KD. Visual outcomes, quality of vision, patient satisfaction and spectacle independence after bilateral implantation of the synergy intraocular lens. Clin Ophthalmol. 2023;17:2277–2285. doi:10.2147/OPTH.S421185
12. Daya S, Espinosa Lagana M. Visual and refractive outcomes of a new hydrophobic trifocal toric intraocular lens. Clin Ophthalmol. 2024;18:997–1007. doi:10.2147/OPTH.S453565
13. Gundersen KG. Rotational stability and visual performance 3 months after bilateral implantation of a new toric extended range of vision intraocular lens. Clin Ophthalmol. 2018;12:1269–1278. doi:10.2147/OPTH.S173120
14. Newsom TH, Potvin R. Evaluation of quality of vision and visual outcomes with bilateral implantation of a non-diffractive extended vision intraocular lens with a target of slight myopia in the non-dominant eye. Clin Ophthalmol. 2022;16:183–190. doi:10.2147/OPTH.S350850
15. Modi SS, Lehmann RP, Fisher BL, Roth RE, Reiser H. Comparison of visual function and patient-reported outcomes between two full range of field intraocular lenses: a randomized controlled study. J Cataract Refract Surg. 2025;51(8):695–702. doi:10.1097/j.jcrs.0000000000001678
16. Benyoussef AA, Reboux N, Cochener B. Comparison of bilateral reading performance among two presbyopia-correcting intraocular lenses. J Refract Surg. 2022;38(7):428–434. doi:10.3928/1081597X-20220516-02
17. Rosser DA, Cousens SN, Murdoch IE, Fitzke FW, Laidlaw DA. How sensitive to clinical change are ETDRS logMAR visual acuity measurements? Invest Ophthalmol Vis Sci. 2003;44(8):3278–3281. doi:10.1167/iovs.02-1100
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.