Back to Journals » Patient Preference and Adherence » Volume 11
Patient preferences for antiretroviral therapy: effectiveness, quality of life, access and novel delivery methods
Authors Eaton EF, McDavid C, Banasiewicz MK ![]() , Mugavero MJ, Knight SJ
, Mugavero MJ, Knight SJ
Received 26 May 2017
Accepted for publication 8 August 2017
Published 18 September 2017 Volume 2017:11 Pages 1585—1590
DOI https://doi.org/10.2147/PPA.S142643
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Ellen F Eaton,1 Chastity McDavid,1 Mary Katy Banasiewicz,1 Michael J Mugavero,1 Sara J Knight2
1Division of Infectious Diseases, Department of Medicine, University of Alabama at Birmingham, Birmingham, AL, USA; 2Division of Preventive Medicine, Department of Medicine, University of Alabama at Birmingham, Birmingham, AL, USA
Objective: The objective of this study was to understand patient preferences for contemporary antiretroviral therapy (ART) by focusing on three areas that have been understudied: minority patients (racial/ethnic and sexual minorities), experience with novel single-tablet regimens made available in the last 10 years, and patient concerns related to ART. The rationale was that identifying ART characteristics that are most desirable could inform provider prescribing practices, increase the use of patient-centered ART, maximize durability and ART adherence, and ultimately improve HIV outcomes, such as viral suppression and AIDS-related comorbidities.
Methods: We recruited English- and Spanish-speaking persons living with HIV (PLWH) who were ≥19 years of age or older and had initiated ART after January 1, 2006, until saturation was reached (n=28). We excluded patients who had started on ART more than 10 years earlier, in order to ensure responses were relevant to more contemporary ART regimens. We recruited racial/ethnic and sexual minorities, including men who have sex with men and transgender participants, to reflect the current HIV epidemic. Nominal group technique was used to identify and prioritize preferences and concerns. Multi-voting analysis was used to quantify responses from most important (5 points) to least important (1 point).
Results: For 28 diverse participants, clinical outcomes (162 points) and quality of life (120 points) were preferred. Hispanic participants were more concerned about accessibility than non-Hispanic (3.8 vs 1.9 average points/participant).
Discussion: HIV-infected persons prioritize access, clinical outcomes, and quality of life when considering contemporary ART treatment. Providers, insurers and policy makers should incorporate these preferences when making decisions about ART.
Keywords: HIV, preferences, immigrant, Hispanic, access to care
Background
The superiority of contemporary antiretroviral therapy (ART) in clinical trials relative to the real-world effectiveness of ART in routine care underscores the challenges in achieving and maintaining HIV suppression for diverse patients in real-world settings.1 This is a major barrier to the ambitious goal of 90:90:90 set by the UNAIDS Scientific and Technical Advisory Committee in 2014; reaching this goal would require diagnosis of 90% of HIV infected persons, HIV treatment of 90% with a diagnosis, and a suppressed viral load in 90% on treatment by 2020. Prescribing ART that is tolerable and convenient as a part of routine care is critical in order to make treatment more durable, and adherence less complicated.2 Prior research has focused on patient preferences related to ART therapy in order to identify the regimen(s) that persons living with HIV (PLWH) will most likely adhere to and subsequently obtain optimal clinical outcomes like viral load suppression. Several studies have shown that ART potency and durability are prioritized by patients over the avoidance of side effects and simplified pill regimen.3,4 However, these studies are outdated because most participants in these studies were receiving older, less effective ART regimens, which are no longer routinely prescribed or recommended by national guidelines.5 Specifically, work by Miller et al3 and Sherer et al4 occurred prior to 2007 before the advent of single-tablet regimens. At that time, ART therapy usually consisted of three or more individual tablets and included less effective, less tolerable drugs including zidovudine and atazanavir.6 Whereas, in more recent years, PLWH are most likely to be receiving a once daily regimen including entirely newer drug classes like non-nucleoside reverse transcriptase inhibitors and integrase strand transfer inhibitors.5
More recently, novel work has used choice-based conjoint surveys, which allow patients to consider the value of ART characteristics (eg, efficacy, side effects, pill burden) relative to other factors that they feel are less important, to prioritize patient preferences for ART.7,8 Results demonstrate that quality of life, specifically emotional quality of life, and avoidance of side effects and long-term complications have become important considerations for PLWH in the last decade.7,8 Since these studies were published, the treatment landscape for PLWH has continued to evolve with the introduction of new drugs and annual changes to treatment guidelines. Since 2007, the number of available single-tablet ART regimens has gone from one option to five options, and newer options are thought to be more tolerable with fewer side effects. Assessing patient preferences for ART, therefore, must be re-evaluated to include experiences with current treatments rather than reflections on ART that is no longer in use.5 Studies should also evaluate patient concerns in addition to preferences to shed light on barriers to ART adherence. Furthermore, the HIV epidemic has changed with young, gay males of racial/ethnic minority status and transgender females representing a disproportionate number of new infections.9 Thus, incorporating the preferences of racial/ethnic and sexual minorities is essential to respond to the dynamic epidemiology of HIV.
The objective of this study was to understand patient preferences for contemporary ART by focusing on three areas that have been understudied: minority patients (racial/ethnic and sexual minorities), experience with novel single-tablet regimens made available in the last 10 years, and concerns related to ART. The rationale was that identifying ART characteristics that are most desirable could inform provider prescribing practices, increase the use of patient-centered ART, maximize durability and ART adherence, and ultimately improve HIV outcomes like viral suppression and AIDS-related comorbidities.9
Methods
This study was approved by the Institutional Review Board at the University of Alabama Birmingham (protocol number 160824010).
Study sample and procedures
Nominal group technique (NGT) was used to identify domains of preferences and to formally develop priorities about what patients like and dislike about ART regimens.11 NGT allows key stakeholders (ie, patients) to discuss differing opinions on matters of shared interest, and then formally and anonymously vote on these opinions, which allows quantitative analysis in order to establish priorities. We included English- and Spanish-speaking PLWH ≥19 years old who initiated ART since January 1, 2006. We excluded patients started on ART more than 10 years ago (before 2006) in order to ensure responses were relevant to more contemporary ART regimens. Participants were recruited at an academic HIV clinic in the southeastern US (using flyers, staff referrals, and electronic screens) and at a community-based partner organization serving the Hispanic HIV-positive community (using staff referrals). The consent process was conducted in English or Spanish, depending on the participants preferred language, and participants were enrolled if they provided written informed consent. Participants were notified that sessions, including important quotes, would be audio recorded without any identifying information such as names. We conducted four nominal groups: two for English speakers and two for Spanish speakers. Participants were heterogeneous in content with varying ages, gender, sexual orientation, time since diagnosis, and years on ART. Participants were recruited until saturation was achieved.10
During each NGT group, participants were assigned a number by which they were addressed during the discussion to protect their confidentiality. After an introduction and orientation to the study objectives, a skilled moderator asked participants to consider question 1 (Q1): “What do you want this medicine to do for you?” Participants had time to consider this question silently and write their responses on a sheet of paper numbered one through ten. Then, participants were encouraged to share their individual responses in a structured, “round robin” format, and responses were recorded legibly on a large display board.11 This process continued until each participant had shared all responses to Q1. Participants then had time to independently and anonymously rank the most important responses written on the display board from one to five, with one being least important and five being most important. This process was then repeated for question 2 (Q2) “What are your concerns about taking this medicine?”
Analysis
Multi-voting technique was used to weight each patient preference (Q1) and concern (Q2) from one to five points according to the importance of the response: one point was assigned for least important, five points for most important.12 For example, a participant who rated preferences as follows would have responses weighted accordingly: 1) control virus (5 points); 2) minimize side effects (4 points); 3) feel better (3 points); 4) long lasting medication (2 points); 5) minimize organ damage (1 point). Results were compared by race and gender. Results were not compared according to the recruitment method because staff referrals occurred largely in the Hispanic cohort (Table 1). Thus, stratifying by recruitment method would be confounded by race/ethnicity, which was evaluated separately.
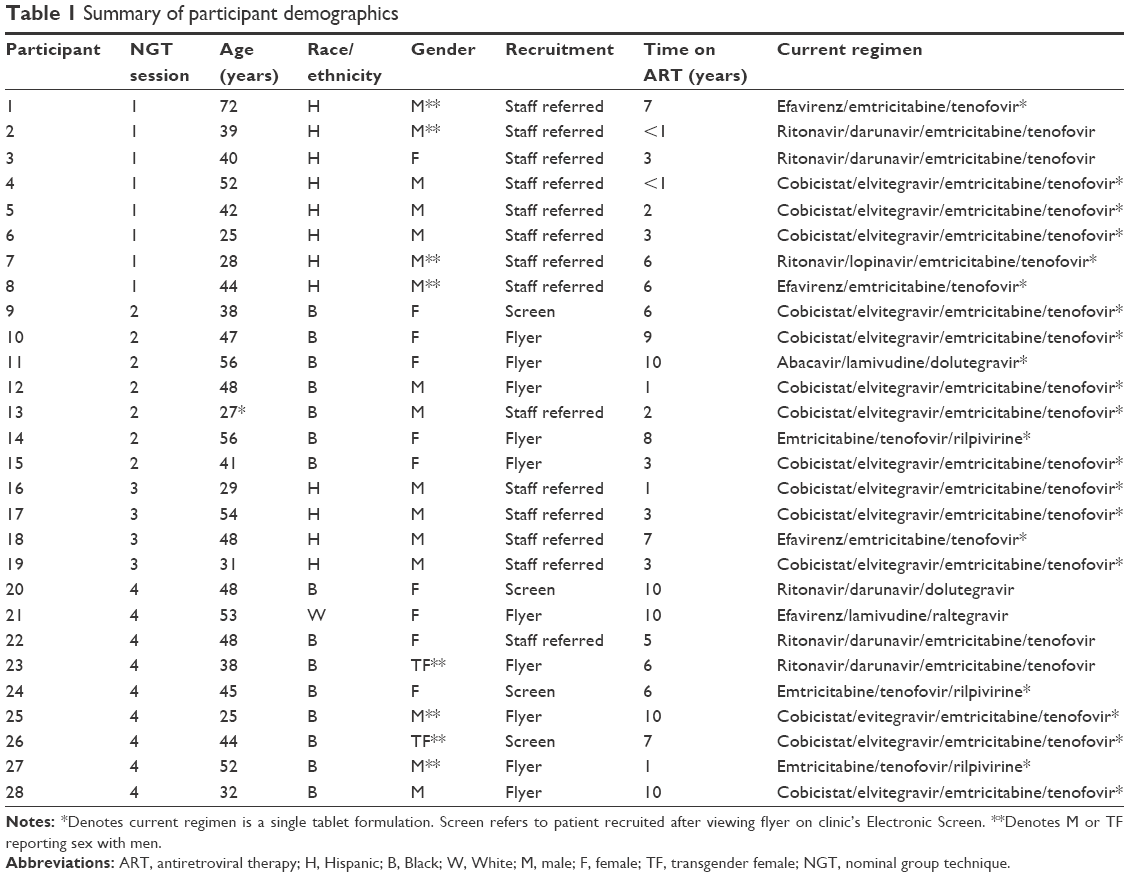 | Table 1 Summary of participant demographics |
For each response, scores were averaged across groups to compare the importance that an Hispanic participant, for example, placed on a preference relative to a non-Hispanic participant. Quotes were recorded and categorized according to which of the above categories they addressed. Results were analyzed following each session in order to determine if saturation had been met and, if not, additional recruitment and session were conducted.
Results
A total of 28 participants were recruited: 42% Hispanic (n=12), 57% male (n=16), 38% of the men (n=6) were self-reported men who have sex with men (MSM), 4% transgender female (n=2), and 79% (n=22) were receiving a single tablet ART (Table 1). The mean age was 43 years. A majority (57%) were receiving ART containing one or more drugs that was US Food and Drug Administration (FDA)-approved in the last 5 years. Due to a large number of responses to Q1 and Q2 receiving ≤10 points, only responses receiving more than 10 points were included in the analysis. Based on common themes, responses were categorized into four groups: clinical (eg, control virus, minimize organ damage), pharmacologic (eg, long acting, once daily), quality of life (eg, feel better, reduce side effects), and access to care (eg, insurance, cost). Notably, some participants had multiple responses pertaining to the same category. For example, one participant desired that ART regimen 1) cure their virus (assigned 5 points); 2) improve their immune system (4 points); and 3) control their virus (3 points) – therefore this participant’s first three priorities were all counted toward the clinical outcome category (12 points).
Overall, the most heavily weighted responses to Q1 were clinical outcomes like viral control, cure and improved CD4 cell count (162 points) and improved quality of life (120 points). Patients desired that medications “maintain the levels of HIV in control” and “to help me feel better … even on bad days”. Pharmacologic features such as dosing and pill burden were less important (52 points). The most heavily weighted responses to Q2 were clinical outcomes (149 points) like viral control and accessibility of ART and out of pocket costs (78 points). One participant expressed: “My major concern is that I will not be able to get access, or to get it for free more, because of the change of the government.” Another said:
Some people, I mean, you have, it’s affordable. Then you have some to where the insurance will pay so much and then you have a copay. And that’s still expensive for some people.
The most heavily weighted responses are summarized in Table 2.
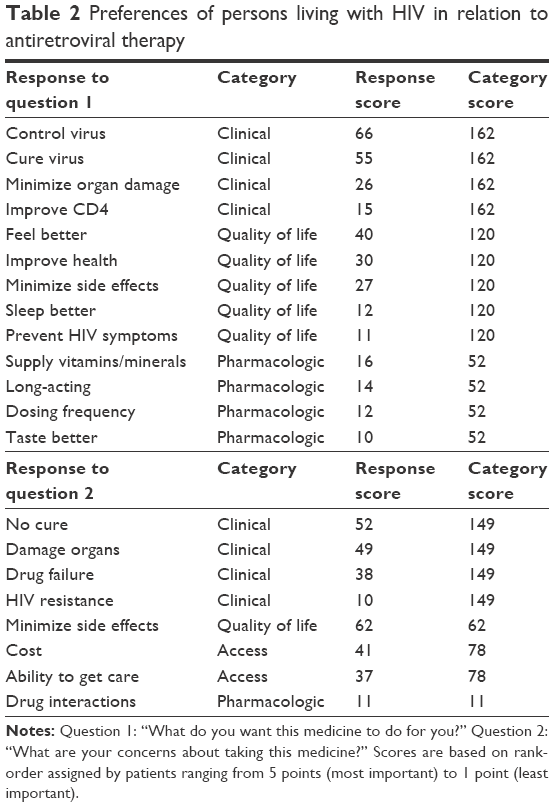 | Table 2 Preferences of persons living with HIV in relation to antiretroviral therapy |
Although patient preferences were similar across race/ethnicity and gender, concerns were unique for some groups. Hispanic participants were more concerned about accessibility including insurance coverage (3.8 average points/participant) than non-Hispanic (1.9 points/participant). Responses highlighted unique challenges for this population: “If I need to go back to Mexico, how will I get it?” Another commented:
For us, as Latino’s, it’s important that the information could be in Spanish so we can understand … instructions could be translated in Spanish.
Women expressed more pharmacologic concerns in the nominal groups (12 quotes) relative to men (8 quotes), including:
My major concern is the interaction between other medicines, because I have other conditions. I take other medicines. And they’re very strong, and I think that in the long-run, I can have a lot of complications.
However, when ranking these pharmacologic concerns, both men and women placed minimal priority on these issues (Table 2). Patients also desire novel ART delivery methods including long acting medications and coformulation with vitamins and/or other medications (eg, high blood pressure medications): “The other thing is I would like for or want this medicine to be in a convenient 3, 6, or 12 month injection.” Several patients expressed a desire to co-formulate their ART with a medication for another chronic illness like high blood pressure:
I am wondering since high blood pressure is prevalent in the African American community, if they can have an antiviral medication that also helps with high blood pressure.
Discussion
In the current ART treatment era, there are many single-tablet, tolerable, effective regimens available, and yet only 30% of HIV infected persons in the US have achieved appropriate HIV control.13 This study sought to identify factors that have the potential to increase ART adherence, evaluating the preferences and concerns of diverse PLWH related to contemporary ART. Our findings demonstrate that PLWH prioritize ART efficacy, similar to prior studies,7,8 and also consider an HIV cure, quality of life, and cost of great importance. Patients’ interest in ART cost and access has not previously been described and likely reflects the changing political climate, uncertainty regarding the future of the Affordable Care Act and Ryan White Program, and the concerns of many immigrants living with HIV in the US, based on the weight that Latino participants placed on these considerations relative to their non-Latino counterparts.
Our study captured a diverse socio-demographic sample including Hispanic, African American, MSM and transgendered PLWH. Only one participant was white (4%), which is consistent with the current HIV epidemic wherein black and Hispanic men are disproportionately affected.14 A majority were receiving new ART agents (<5 years since FDA approval) as part of their ART regimen, including newer single-tablet regimens, which makes the results unique and germane. Overall, patient preferences and concerns focused on clinical outcomes such as viral control and improved immunity (ie, CD4 count) and avoidance of organ damage. Patients commented that kidney, liver and cognitive damage were especially concerning. This is likely reflective of an aging population who is now struggling with comorbidities such as chronic kidney and liver disease that are more prevalent and often more progressive in HIV infected cohorts.15 Patients’ interest in an improved CD4 cell count is noteworthy because experts no longer recommend frequent CD4 cell count testing for those with well-controlled HIV.16 The discrepancy between patient preferences and evidence-based medicine deserves further study to ensure contemporary HIV care is patient-centered.
Discussion of pharmacologic factors revealed that patients are interested in novel ART delivery forms. Participants, especially women participants, shared several drug-related ideas and concerns in nominal group sessions although they did not prioritize pharmacologic preferences over clinical factors and quality of life when asked to order them according to importance. For example, female participants expressed a desire for long-acting ART that is injectable or in pill format that lasts for months or longer. Female participants also discussed a desire to have their ART co-formulated with other medications (eg, antihypertensive medication) and supplements (eg, vitamins and minerals) in order to jointly receive these therapies in a single tablet with their ART. Pharmaceutical developers should consider these patient preferences when designing new regimens. Interestingly, females had more pharmacologic concerns than men (12 quotes vs 8 quotes) even though they made up a smaller percentage of participants (43%). This may also reflect an aging cohort dealing with multiple medications required for comorbidities like diabetes and high blood pressure and underscores that drug factors, like simplicity and tolerability, should be considered in decisions related to ART for women.
Lastly, the two Hispanic groups, which represented 42% of our sample, expressed significant concerns related to ART barriers including insurance, out of pocket costs, and visa issues. Some patients were receiving short-term visas, which requires that they return to their country of origin annually for prolonged periods. During this time, these HIV positive immigrants may not have access to their current ART in which case they would have to modify their regimen based on ART availability in another country. Others were generally fearful of recent trends in the social and political climate in the US and how this would impact access to medical care, access to ART, and issues with deportation. The emphasis on access to care is noteworthy and should be considered when caring for patients with HIV as it will have unpredictable implications for uninsured and underinsured persons in the changing health care environment.
Conclusion
Despite a dramatically changing treatment landscape, traditional patient preferences for clinical potency, quality of life, and avoidance of side effects persist in the current ART era. However, contemporary themes have emerged including an interest in novel pharmacologic delivery methods like injectable ART and an increased awareness of long-term toxicity and complications like organ failure. Moreover, concerns regarding treatment access have become a prominent concern for Latinos, reflecting political, immigration and health policy uncertainties. Providers should consider these enduring priorities as well as novel pharmacologic considerations and barriers to health care access for all PLWH, especially Hispanic patients, when making decisions with patients about ART selection.
Disclosure
EF Eaton is supported by grant K12HS023009 from the Agency for Health Research and Quality and has received funds (to University of Alabama at Birmingham) from the Bristol Myers Squibb Virology Fellowship, Merck, and the University of Alabama at Birmingham Center for AIDS Research (CFAR; P30-A1027767). MJ Mugavero has received grant support (to University of Alabama at Birmingham) from Bristol Myers Squibb Virology Fellows Research Training Program and consulting fees from Gilead Sciences. SJ Knight receives support from the Department of Veterans Affairs (VA) Health Services Research and Development Service (1I01HX002315-01) and from the Agency for Healthcare Research and Quality (T32HS023009). The other authors report no conflicts of interest in this work.
References
Kanters S, Vitoria M, Doherty M, et al. Comparative efficacy and safety of first-line antiretroviral therapy for the treatment of HIV infection: a systematic review and network meta-analysis. Lancet HIV. 2016;3(11):e510–e520. | ||
Trottier B, Machouf N, Huchet E, et al. Tolerability is more important than simplicity for treatment durability. J Int AIDS Soc. 2014;17(4 Suppl 3):19765. | ||
Miller LG, Huffman HB, Weidmer BA, Hays RD. Patient preferences regarding antiretroviral therapy. Int J STD AIDS. 2002;13(9):593–601. | ||
Sherer RD Jr, Fath MJ, Da Silva BA, Nicolau AM, Miller NL. The importance of potency and durability in HIV patient antiretroviral therapy preferences: a telephone survey. AIDS patient Care STDs. 2005;19(12):794–802. | ||
Eaton EF, Tamhane A, Burkholder G, Willig J, Saag M, Mugavero MJ. Unanticipated effects of new drug availability on antiretroviral durability: implications for comparative effectiveness research. Open Forum Infect Dis. 2016;3(2):ofw109. | ||
McKinnell JA, Willig JH, Westfall AO, et al. Antiretroviral prescribing patterns in treatment-naive patients in the United States. AIDS patient Care STDs. 2010;24(2):79–85. | ||
Muhlbacher AC, Stoll M, Mahlich J, Nubling M. Patient preferences for HIV/AIDS therapy – a discrete choice experiment. Health Econ Rev. 2013;3(1):14. | ||
Gazzard B, Ali S, Muhlbacher A, et al. Patient preferences for characteristics of antiretroviral therapies: results from five European countries. J Int AIDS Soc. 2014;17(4 Suppl 3):19540. | ||
The Centers for Disease Control. HIV in the United States: At A Glance. Available from http://www.cdc.gov/hiv/pdf/statistics_basics_ataglance_factsheet.pdf. Accessed February 26, 2016. | ||
Walker JL. The use of saturation in qualitative research. Can J Cardiovasc Nurs. 2012;22(2):37–46. | ||
Harvey N, Holmes CA. Nominal group technique: an effective method for obtaining group consensus. Int J Nurs Pract. 2012;18(2):188–194. | ||
Lucas AG, Primus K, Kovach JV, Fredendall LD. Rethinking behavioral health processes by using design for six sigma. Psychiatr Serv. 2015;66(2):112–114. | ||
Mugavero MJ, Amico KR, Horn T, Thompson MA. The state of engagement in HIV care in the United States: from cascade to continuum to control. Clin Infect Dis. 2013;57(8):1164–1171. | ||
Centers for Disease Control and Prevention. Lifetime Risk of HIV Diagnosis. Available from http://www.cdc.gov/nchhstp/newsroom/2016/croi-press-release-risk.html. Accessed March 7, 2016. | ||
Deeks SG, Phillips AN. HIV infection, antiretroviral treatment, ageing, and non-AIDS related morbidity. BMJ. 2009;338:a3172. | ||
Duncan CJ, Schmid ML, Schwab U, Price DA, Ong E. Futility of CD4+ monitoring in HIV-1 patients with CD4+ cell count above 350 cells/mul on suppressive antiretroviral therapy. AIDS (London, England). 2014;28(17):2638–2639. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.