Back to Journals » Patient Preference and Adherence » Volume 14
Patient Preferences for Anti-Vascular Endothelial Growth Factor Treatment for Wet Age-Related Macular Degeneration in Japan: A Discrete Choice Experiment
Authors Joko T, Nagai Y, Mori R, Tanaka K ![]() , Oshima Y, Hikichi Y
, Oshima Y, Hikichi Y ![]() , Komori T
, Komori T ![]() , Carrasco J
, Carrasco J ![]() , Maculaitis MC, Will O, Beusterien K, Takahashi K
, Maculaitis MC, Will O, Beusterien K, Takahashi K ![]()
Received 27 August 2019
Accepted for publication 28 December 2019
Published 12 March 2020 Volume 2020:14 Pages 553—567
DOI https://doi.org/10.2147/PPA.S228890
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Takeshi Joko,1 Yoshimi Nagai,2 Ryusaburo Mori,3 Koji Tanaka,3 Yuji Oshima,4 Yusuke Hikichi,5 Tetsushi Komori,6 Joao Carrasco,7 Martine C Maculaitis,8 Oliver Will,8 Kathleen Beusterien,8 Kanji Takahashi2
1Department of Ophthalmology, Matsuyama Red Cross Hospital, Matsuyama, Ehime, Japan; 2Department of Ophthalmology, Kansai Medical University, Hirakata, Osaka, Japan; 3Division of Ophthalmology, Department of Visual Sciences, Nihon University of School of Medicine, Chiyoda-ku, Tokyo, Japan; 4Department of Ophthalmology, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan; 5Department of Market Access, Bayer Yakuhin, Ltd., Chiyoda-ku, Tokyo, Japan; 6Department of Research & Product Development, Bayer Yakuhin, Ltd., Kita-Ku, Osaka, Japan; 7Department of Market Access, Bayer Consumer Care AG, Basel, Canton of Basel-Stadt, Switzerland; 8Health Division, Kantar, New York, NY, USA
Correspondence: Takeshi Joko
Department of Ophthalmology, Matsuyama Red Cross Hospital, 1 Bunkyocho, Matsuyama, Ehime 790-8524, Japan
Tel +81 89 924 1111
Email [email protected]
Background: In Japan, intravitreal anti-vascular endothelial growth factor (anti-VEGF) dosing regimens for wet age-related macular degeneration (wAMD) include pro re nata, every 2 months, and treat-and-extend, resulting in different outcomes and patient burden. Although reflecting patient preferences in treatment decision-making is desirable, few studies have examined this in Japan. This study assessed the patients willingness to trade-off between different dosing regimens.
Patients and Methods: Patients with wAMD were recruited from four Japanese university hospitals to complete a face-to-face cross-sectional survey. In a discrete choice experiment, patients were asked to choose their preferred option from two anti-VEGF treatment profiles shown side-by-side across a series of choice tasks. The profiles varied on four attributes: number of injections in 12 months, number of physician consultations in 12 months, chance of 1-year visual acuity (VA) improvement, and chance of 2-year VA maintenance. Preference weights were estimated using hierarchical Bayes’ models.
Results: Overall, 120 patients (30 treatment naïve and 90 anti-VEGF experienced) completed the survey. Patients were willing to accept an increase from three to approximately eight injections in 12 months to increase the chance of 1-year VA improvement from 25% to 40%. They would be willing to accept 11 injections in 12 months if the chance of 2-year VA maintenance increased from 80% to 96%. The most valued attributes were increasing the chance of 2-year VA maintenance and reducing the number of injections in 12 months, which were each about twice as important as decreasing physician consultations in 12 months and increasing the chance of 1-year VA improvement (p< 0.001). Among the dosing regimens, patients most preferred treat-and-extend because of its higher chance of 2-year VA maintenance.
Conclusion: Informing patients with wAMD about the likelihood of long-term VA maintenance when selecting treatment may increase the acceptance of an optimal treatment regimen and number of injections.
Keywords: wet age-related macular degeneration, patient preference, anti-vascular endothelial growth factor treatment, dosing regimen, treat-and-extend
Introduction
Age-related macular degeneration is a leading cause of blindness in adults in developed countries.1 Wet age-related macular degeneration (wAMD) occurs when abnormal blood vessel growth leaks fluid (or blood) into the macula distorting central vision.2 Global meta-analyses have estimated the prevalence of wAMD to be 0.46%;3 however, the prevalence in Japan has been estimated to be 0.67%.4
The Japanese Ministry of Health, Labor, and Welfare has recommended vascular endothelial growth factor inhibitors (anti-VEGFs) for patients with wAMD.5 Anti-VEGFs, such as pegaptanib, ranibizumab, and intravitreal aflibercept (IVT-AFL),6 are the currently available licensed treatments for wAMD in Japan, but they differ with respect to their associated dosing regimens, which has substantial implications for visual outcomes and healthcare resource use. An early approach for anti-VEGF therapy for wAMD, which was introduced in two pivotal Phase 3 clinical trials, MARINA7 and ANCHOR,8 involved monthly intravitreal injections of ranibizumab, resulting in substantial and sustained increases in best-corrected visual acuity (BCVA) between 7.2 and 11.3 letters.7,8 This treatment required, on average, 13 injections administered annually,9 resulting in substantial burden for physicians and patients.
Consequently, an individualized dosing regimen—pro re nata (PRN)—was evaluated in the PrONTO study,10 Comparison of AMD Treatment trials,11 the IVAN trial,12 and the HARBOR trial.13 The PRN dosing regimen entails monthly clinical examination using optical tomography, and treatment is determined based on evidence of exudation. This approach subsequently reduced the injection frequency with ranibizumab to an average of between 5 and 7.7 injections, with an average gain of 11.1 letters at 24 months and 8.2 to 8.6 letters at 12 months reported in the PrONTO and HARBOR trials, respectively.10,14 Other observational studies investigating the PRN dosing regimen have reported reduced effectiveness, relative to clinical studies, with an average gain of 4.4 letters15 and a concomitant decrease in the number of injections to 4.9 in the first 12 months.16
Because the PRN dosing regimen requires monthly visits, there may be a heavy burden on institutional resources, as well as on patients, who may not present for examination.17 These factors may result in under-treatment and preclude vision improvement.18 To address these issues, researchers investigated an alternative dosing regimen (every 2 months; q8) that decreased injection and monitoring frequency to three initial monthly doses of IVT-AFL, followed by subsequent doses every 2 months. This resulted in an average BCVA gain of 7.9 letters after the first 12 months of treatment.19 In addition to the good visual prognosis associated with q8, this dosing regimen may potentially reduce psychological burden on patients, as they know in advance when they can anticipate receiving treatment. Nevertheless, while the q8 dosing regimen entails a lower number of injections, compared with monthly regimens, it may also lead to patients receiving unnecessary treatment, as injections are administered based on a set time period, rather than on evidence of exudative activity.
A more recently implemented dosing regimen, treat-and-extend (T&E), individualizes wAMD treatment by sequentially lengthening treatment intervals by 2 weeks until there is evidence of choroidal neovascularization.6 The clinical outcomes of T&E, initially investigated with ranibizumab due to its earlier availability, have been reported to be comparable to or better than other dosing regimens, with BCVA gains varying from an average of 8 to 11.6 letters in the first 12 months.20,21 Recent evidence indicates that T&E therapy with IVT-AFL can also produce good outcomes over 2 years while reducing treatment burden.22–24 Recent consensus guidelines recommend the use of IVT-AFL with a T&E dosing regimen for wAMD management in the Asia-Pacific region,25 but there is no clear consensus on the most efficacious and cost-effective anti-VEGF treatment regimen.
In Japan, the PRN dosing regimen became the standard approach for anti-VEGF therapy in wAMD after the introduction of ranibizumab in 2009,26 in contrast with the general recommendations for the Asia-Pacific region, at large. Alternative proactive treatment strategies (ie, q8 and T&E) were not introduced until 2012 when IVT-AFL was launched in Japan.27
A recent study by Iida et al26 showed that, despite evidence of better clinical outcomes with proactive regimens, Japanese ophthalmologists cite challenges in communicating those benefits to their patients. Specifically, ophthalmologists perceived that the high number of injections may impose a treatment-related and economic burden on their elderly patients, which hindered ophthalmologists’ effective communication with them. This has important implications, as shared decision-making can increase treatment satisfaction and may result in better adherence and follow-up care, while reducing the risk of discontinuation, thereby increasing the likelihood of better clinical outcomes.28–31
Although some research has examined patient preferences for wAMD treatments, these studies have been conducted in the West and have not included the T&E dosing regimen.32–34 Moreover, no study has examined how patients in Japan value differences in the characteristics of wAMD treatment options. This study was designed to inform physicians of patient preferences to facilitate shared decision-making for anti-VEGF treatment. Additionally, this study sought to understand and quantify the trade-offs that patients with wAMD in Japan are willing to make between different dosing regimens of anti-VEGFs, specifically, PRN, q8, and T&E.
Materials and Methods
Sample and Procedure
In this cross-sectional observational study, patients with wAMD completed a paper-based survey in a face-to-face interview, which lasted approximately 60 mins. Patient preferences were assessed using a discrete choice experiment (DCE), a stated preference methodology that enables the assessment of patients’ willingness to accept trade-offs among different features and outcomes, called attributes, that are associated with wAMD treatment regimens. A DCE was utilized, as it is the optimal preference elicitation technique for evaluating trade-offs among different treatment attributes, as opposed to obtaining a simple ranking of each attribute. As it requires respondents to state their preference from among multiple hypothetical alternatives and not rank or rate them, the DCE presents an uncomplicated task that mirrors a respondent’s real-world choice.35 The study design and procedures followed the practice guidelines for conjoint analysis developed by the International Society of Pharmacoeconomics and Outcomes Research.36
Participants were recruited by convenience sampling via physician referrals from four hospitals throughout Japan from November 2017 to June 2018. The inclusion criteria were: (1) aged 50 years or older, (2) physician-confirmed wAMD diagnosis (treated/untreated with anti-VEGF agents), (3) able to read and understand Japanese and complete the survey, and (4) BCVA of the better-seeing eye more than a decimal notation of 0.5 (approximately 20/40 at Snellen equivalent), as determined by the referring physician (to ensure the patient had at least a minimal level of visual acuity to be able to complete the questionnaire). Patients were excluded if they were currently participating in a clinical trial, ever experienced a vitrectomy, discontinued an anti-VEGF agent due to an adverse effect (patients with possible disease reoccurrence that could be treated with an anti-VEGF agent were not excluded), had BCVA in the better-seeing eye less than a decimal notation of 0.5, were unable to participate in the interview due to physical or psychological reasons, or were otherwise deemed ineligible by the referring physician.
The study adhered to the Declaration of Helsinki and Ethical Guidelines for Medical and Health Research Involving Human Subjects.37 Prior to data collection, the study protocol was reviewed and approved by the Institutional Review Board at each participating site: Kansai Medical University, Ehime University, Kyushu University, and Nihon University. Written informed consent was obtained from all participants.
Study Survey
The survey was pre-tested via cognitive interviews to ensure patient comprehension of survey content, as well as to pilot the study procedures. These 60-min face-to-face interviews were conducted at Ehime University hospital (Sitsukawa Toon, Ehime, Japan) with nine patients with wAMD to help refine the definitions, instructions, and injection plan schema and to confirm that patients were able to understand the treatment choice questions. For the quantitative study, patients’ responses and clinical data were recorded and entered into an electronic database. The survey was comprised of three parts: (1) explanations of PRN, q8, and T&E dosing regimens, (2) DCE exercise, and (3) patient demographic questions. An interviewer read aloud a standardized injection plan script to patients using a schema that explained and helped patients understand the PRN, q8, and T&E dosing regimens and their characteristics. The injection plan script and schema, as well as the patient questionnaire for the quantitative study, are shown in Appendix 1 and Appendix 2, respectively.
The DCE exercise included eight preference-elicitation questions that asked patients to choose between two hypothetical treatment profiles, “Injection A” and “Injection B” that varied with respect to the attributes shown. Each hypothetical treatment profile was defined by four key attributes of dosing regimens and visual acuity outcomes, each of which were identified through a literature search of randomized controlled trials, guidelines, systematic literature reviews, and meta-analyses. The four attributes included: number of injections required in the first 12 months of treatment, number of physician consultations in the first 12 months of treatment, chance of visual acuity markedly improving after 12 months of treatment (defined as the percentage of patients who gained ≥15 letters after 12 months of treatment), and chance of visual acuity maintenance after 2 years of treatment (defined as the percentage of patients who avoided a loss of ≥15 letters after 24 months of treatment), which appeared with a description of its corresponding dosing regimen (ie, PRN, q8, and T&E). The attributes and levels included in the study are shown in Table 1. Figure 1 shows an example DCE choice task; to enable easier comprehension, the profiles in each choice task showed the description of the dosing regimen on top, and the chance of visual acuity maintenance after 2 years of treatment on the bottom.
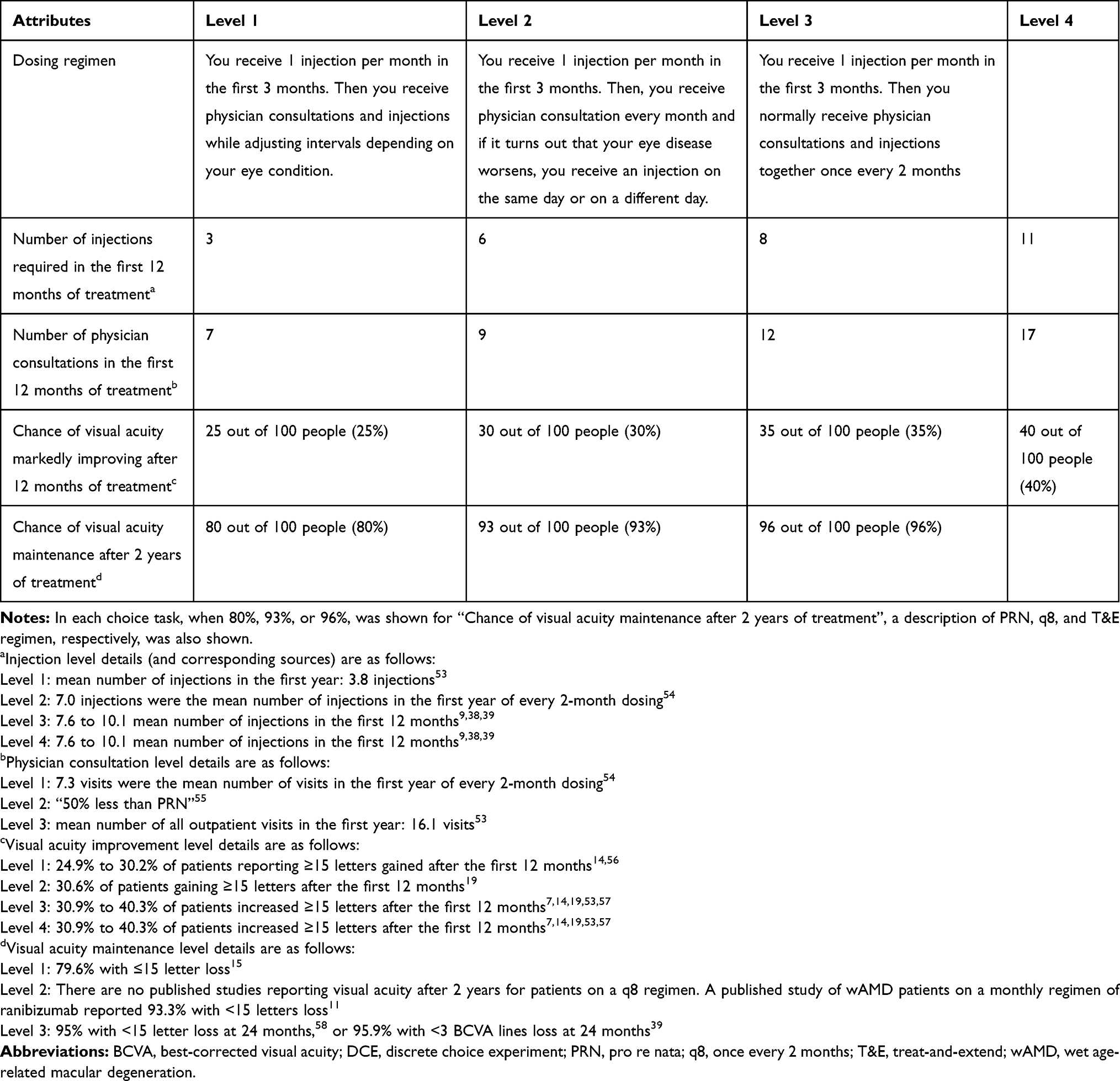 |
Table 1 Attributes and Levels Included in the DCE Exercise |
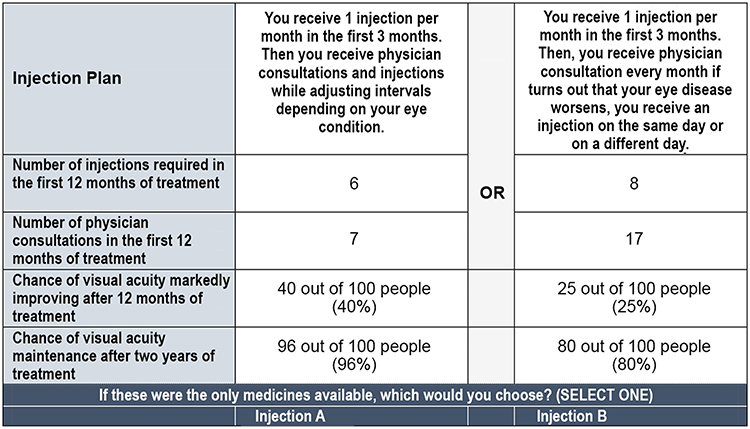 |
Figure 1 Example choice task. |
The literature review, which informed the development of the attributes and levels shown in Table 1, was conducted from January to June of 2016. In particular, the attributes and levels for the T&E dosing regimen in the current study reflect the clinical data that were available at the time the literature review was conducted.38,39
Demographic characteristics self-reported by patients included age, gender, education, marital status, income, employment status, and region. Clinical characteristics data, which were collected from patients’ medical records, included disease duration, number of eyes with wAMD, BCVA at enrollment in the better- and worse-seeing eye, BCVA at 12 months ago in the better- and worse-seeing eye, change in BCVA from 12 months ago to enrollment in the better- and worse-seeing eye, anti-VEGF treatment status (ie, whether the patient was treatment naïve or experienced), current anti-VEGF dosing regimen (anti-VEGF experienced patients only), and duration of anti-VEGF treatment (anti-VEGF experienced patients only); patients self-reported on their round-trip travel time to the hospital. Comorbidity data assessed from medical records included non-ocular comorbidities (used to calculate comorbidity burden via Charlson Comorbidity Index [CCI] scores40,41 and ocular comorbidities.
Experimental Design
A full profile, fractional, factorial, balanced, incomplete block design was used to identify the different combinations of attributes and levels to be shown in each DCE task. The design was selected to maximize the observed combinations for analysis and the orthogonality of the levels (ie, the ability to isolate the effect of a particular level), as well as choosing the fewest choice tasks possible per patient to decrease fatigue. Level combinations that could not appear in practice (ie, violations) were excluded a priori. The choice tasks were blocked into four sets so that any two-way attribute and level combination would not be repeated. A design with 24 choice tasks in 4 blocks was chosen based on these criteria. Two additional fixed-choice tasks were added into all the blocks. These fixed-choice tasks showed a hypothetical profile with the most desirable treatment features versus one with the least desirable treatment features to determine the patient’s capability to recognize the profile with dominant (ie, the most desirable) characteristics.
The design of 24-choice tasks in 4 blocks achieved a D-efficiency of 99.1 out of 100. D-efficiency is a measure of balance and orthogonality, and a value of 100 means that the design is perfectly balanced and orthogonal and will minimize the errors in a model of preference weights. Potential designs were evaluated using Warren Kuhfeld’s macro %MktRuns. Kuhfeld’s macro %MktEx was further used to analyze the potential designs and determine a final design for use in the current study.42
Statistical Analysis
Descriptive statistics were computed for all study variables and included means and standard deviations (SDs) for continuous variables, as well as frequencies and percentages for categorical variables. Preference weights (also called utilities) are coefficients derived from a hierarchical Bayesian (HB) regression model. To estimate preference weights for each attribute level, a HB model was fitted to the choice data.43 The underlying choice-probability model in HB was conditional logit and used effects coding for the attribute levels. Preference weights measure relative preference, which means that only changes between attribute-level estimates and the relative size of those changes across attributes have meaningful interpretations. Specifically, differences between these weights across levels of an attribute (eg, reducing the number of injections in 12 months from 8 to 3) represent the strength of preference for the respective change. The magnitude of the changes from one level to another level within an attribute, compared with the changes from one level to another level within another attribute, enable us to assess trade-offs that respondents are willing to make when choosing a treatment. For example, if the difference in preference weights between two levels of an efficacy attribute is equal to 2 points, and the difference between two levels of an attribute for number of physician consultations is equal to 2 points, then one can conclude that respondents are willing to accept an increase in the number of physician consultations specified by the two levels of the “number of physician consultations in the first 12 months of treatment” attribute for an increase in efficacy specified by the two levels of the “chance of visual acuity markedly improving after 12 months of treatment” attribute.
Relative preference weights for each attribute level are reported using point estimates of model coefficients, standard errors (SEs), and 95% confidence intervals (CIs) comparing the level to the mean level of each attribute. The conditional relative importance was calculated for each attribute at the respondent level by dividing the range of each attribute (ie, the preference weights of the best level minus the preference weights of the worst level) by the sum of the ranges of all attributes and then multiplying by 100 to convert to a percentage. The prediction of treatment choice was computed by summing the preference weights matching to each attribute level for the best and worst treatment profiles for each dosing regimen. The best and worst treatment profiles reflected the most favorable levels and least favorable levels, respectively, across all attributes for each dosing regimen. The preference weights were summed at the individual level, resulting in a mean summed preference weight and 95% CI. The summed weights indicate patients’ relative preference for each profile assessed.
Patients who failed to choose the characteristically dominant profile in one or both fixed tasks were flagged, and their effect on the final preference weights was evaluated. Subgroup comparisons of relative preference weights were performed using one-way analysis of variance (ANOVA) tests or independent-samples t-tests, depending upon the number of levels of the subgroup variable. The subgroups compared included age (50 to <70 years or ≥70 years), gender (male or female), income level (<¥2,500,000 [<$23,500], ¥2,500,000 [$23,500] to ¥4,999,999 [<$47,000], or ≥¥5,000,000 [≥$47,000]), BCVA at enrollment in the better- and worse-seeing eye (categories adapted with slight modification from Brown et al;44 Group 1 [>20/20, >1.0 in decimal unit], Group 2 [20/20-20/25, 0.8–1.0 in decimal unit], Group 3 [20/30-20/40, 0.5–0.7 in decimal unit], Group 4 [20/50-20/100, 0.2–0.4 in decimal unit], and Group 5 [≤20/200, ≤0.1 in decimal unit]), anti-VEGF treatment status (anti-VEGF experienced or anti-VEGF naïve), current anti-VEGF dosing regimen (PRN, fixed dosing, T&E, or modified T&E [mT&E]), region (as determined by location of the hospital site; rural: Ehime University; urban: Kansai Medical University, Kyushu University, and Nihon University), and round-trip travel time to the hospital (<60 mins, ≥60 to <120 mins, or ≥120 mins). Due to the exploratory nature of the study, formal statistical tests were not planned. All p-values are nominal and not adjusted for multiplicity.
Analyses were conducted using Sawtooth’s Software Lighthouse Studio, 2018 and SPSS version 23.0.
Results
A total of 122 patients were recruited to participate in this study; two patients withdrew, resulting in an effective sample size of 120 patients. The average age of the patients was 75.9 (SD=8.0) years, 59.2% were male, and 30.0% had at least some college education. Most were married or living with a partner (77.5%) and currently not employed (87.5%); a majority reported an income of <¥5,000,000 (<$47,000) per year (65.8%). The most commonly reported comorbidity was cataracts (70.8%); mean CCI score was 0.07 (SD=0.42), indicating a low overall comorbidity burden (Table 2).
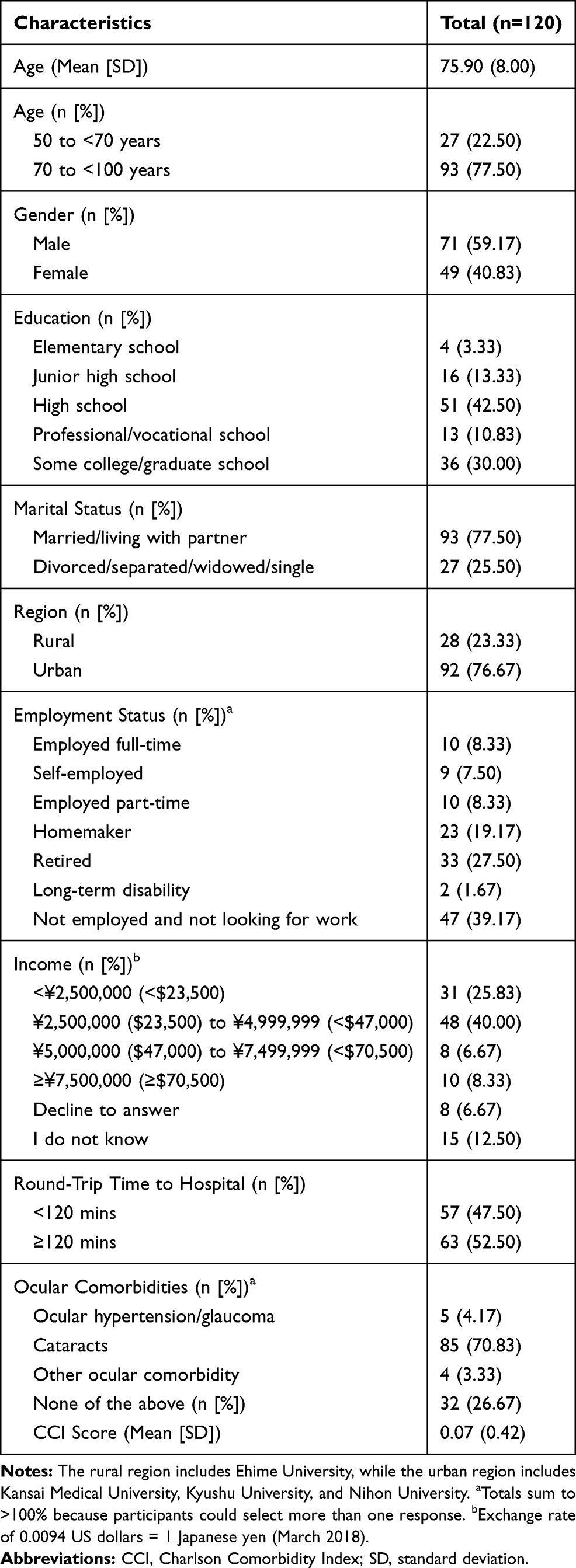 |
Table 2 Demographic and Clinical Characteristics |
At enrollment, 55.8% had a BCVA of >20/20 (>1.0 in decimal unit) for the better-seeing eye, wheras, for worse-seeing eye, this was the case for only 8.3% of the patients. Mean BCVA at enrollment for the better- and worse-seeing eyes were 1.10 (SD=0.26) and 0.61 (SD=0.37) in decimal unit, respectively. The mean change in BCVA from 12 months ago to enrollment was 0.05 (SD=0.26) in decimal unit for the better-seeing eye and -0.02 (SD=0.23) in the decimal unit for the worse-seeing eye. The majority of patients (90.8%) had unilateral wAMD, with an average disease duration of 39.3 (SD=48.2) months. The majority of patients (75.0%) were anti-VEGF experienced, with a mean anti-VEGF treatment duration of 35.6 (SD=28.6) months; PRN was the most commonly received dosing regimen (72.4%; Table 3).
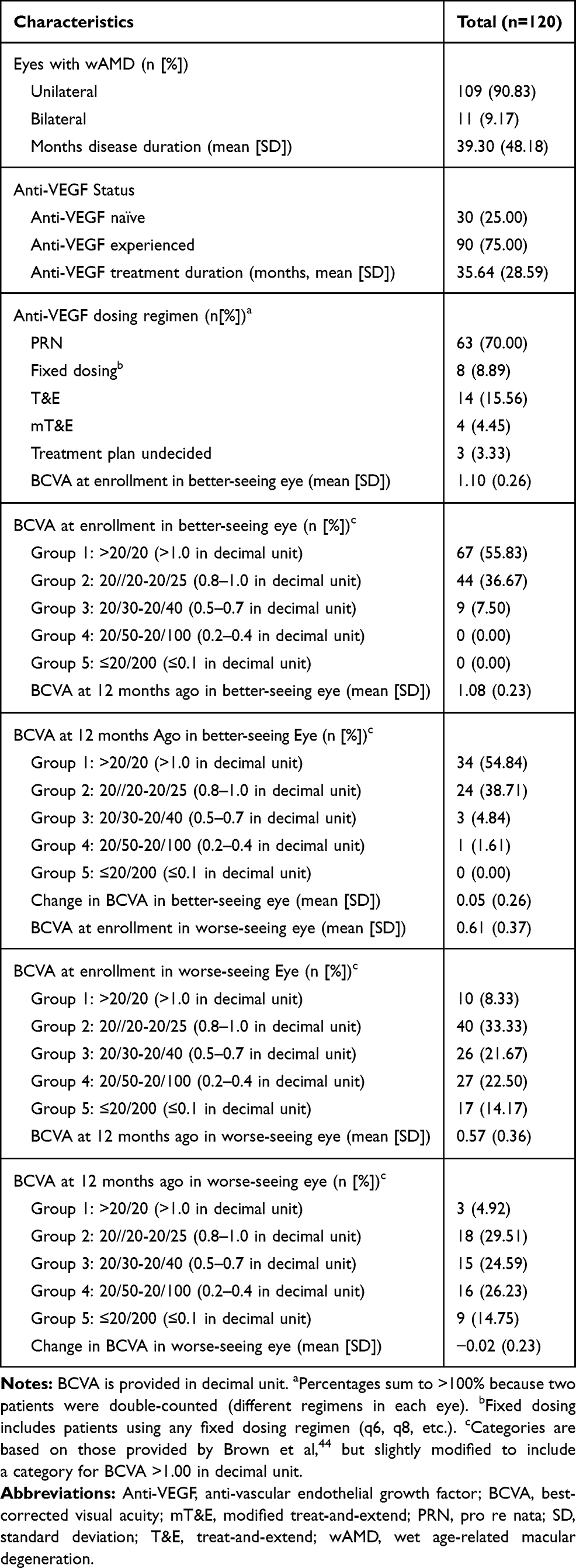 |
Table 3 Clinical and Treatment Characteristics |
Attribute Preferences
Overall, patients most preferred three (compared with 6, 8, or 11) injections required in the first 12 months of treatment, nine (compared with 7, 11, or 12) physician consultations in the first 12 months of treatment, 40% (compared with 25%, 30%, or 35%) chance of visual acuity markedly improving after 12 months of treatment, and 96% (compared with 80% or 93%) chance of visual acuity maintenance after 2 years of treatment (Figure 2). A trade-off is defined as the compromise made by patients between selecting the expected beneficial visual outcome and patient inconvenience. For example, patients were willing to accept: a) an increase in the number of injections required in the first 12 months of treatment from 3 to approximately 11 (difference in preference weights: 2.58 – [−2.63] = 5.21) in exchange for increasing the percentage chance of visual acuity maintenance after 2 years of treatment from 80% to 96% (difference in preference weights: 3.03 – [−2.10] = 5.13), and b) an increase from 9 to 12 physician consultations in the first 12 months of treatment (difference in preference weights: 1.54 – [−0.63] = 2.17) in exchange for increasing the percentage chance of visual acuity markedly improving after 12 months of treatment from 25% to 40%.
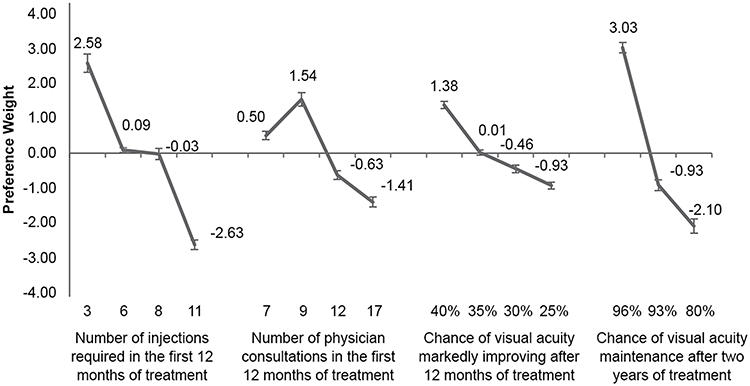 |
Figure 2 Attribute-level preference weights: overall sample. Notes: The error bars represent the 95% confidence intervals. Preference weights are not interpreted by themselves. Instead, the magnitude of change within one attribute is compared to change within another attribute.Abbreviation: VA, visual acuity. |
With respect to relative attribute importance, patients valued increasing the chance of visual acuity maintenance after 2 years of treatment (34%; 95% CI: 32%-36%), followed by reducing the number of injections required in the first 12 months of treatment (31%; 95% CI: 29%-33%). These changes were almost twice as important as decreasing the number of physician consultations in the first 12 months of treatment (19%; 95% CI: 18%-20%) and increasing the chance of visual acuity markedly improving after 12 months of treatment (16%; 95% CI: 15%-17%) (p<0.001; Figure 3).
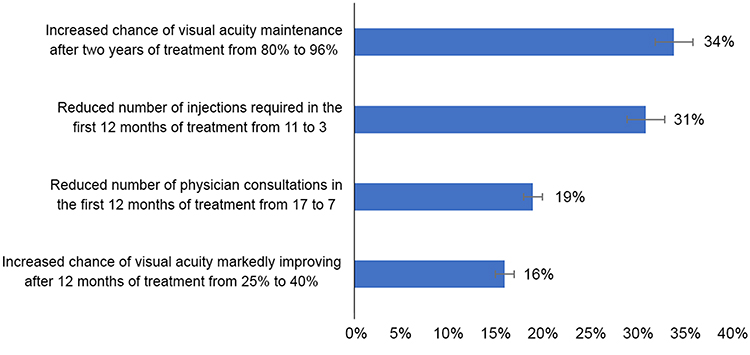 |
Figure 3 Relative importance of treatment attributes: overall sample. Notes: The error bars represent 95% confidence intervals. |
The best profile for each treatment regimen involved the fewest number of injections required in the first 12 months of treatment and physician consultations in the first 12 months of treatment, coupled with greater chances of visual acuity markedly improving after 12 months of treatment and visual acuity maintenance after 2 years of treatment. In contrast, the worst profiles for each treatment profile had the highest number of injections required in the first 12 months of treatment and physician consultations in the first 12 months of treatment, with lower chances of visual acuity markedly improving after 12 months of treatment and visual acuity maintenance after 2 years of treatment. The summed preference weights matching to selected treatment profiles showed that patients have the strongest preference for the best T&E profile; they least preferred the worst PRN profile. The best PRN profile was preferred more than the worst T&E profile, which was, in turn, preferred over the worst PRN profile (both, p<0.001). A trend was observed in which the worst q8 profile was preferred over the worst PRN and worst T&E profiles (Table 4 and Figure 4).
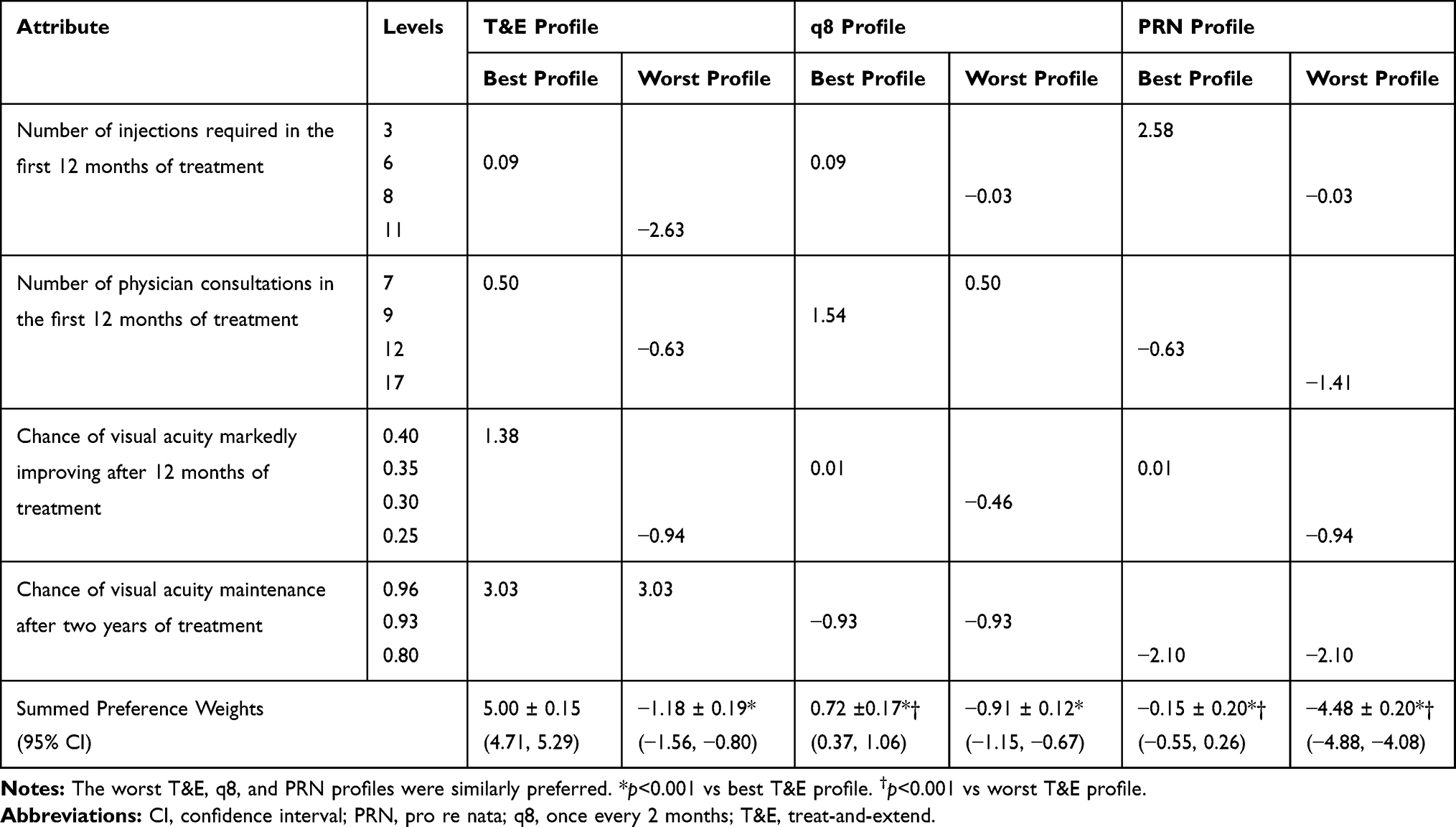 |
Table 4 Preferences for Selected Treatment Profiles: Overall Sample |
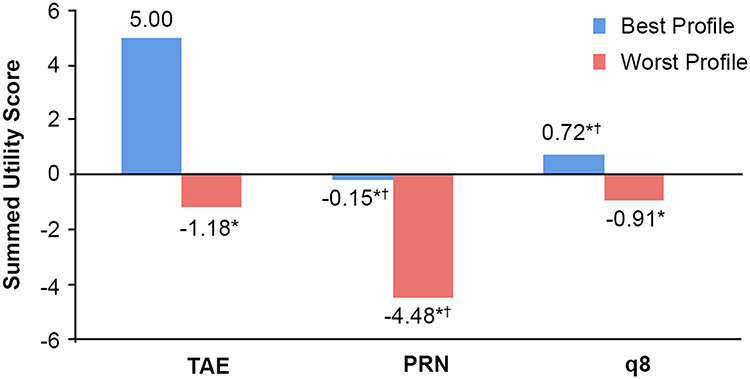 |
Figure 4 Preferences for selected treatment profiles: overall sample. Notes: The worst T&E, q8, and PRN profiles were similarly preferred. *p<0.001 vs best T&E profile. †p<0.001 vs worst T&E profile.Abbreviations: PRN, Pro re nata; q8, once every 2 months; T&E, treat-and-extend. |
Subgroup Analyses
Table 5 reports the subgroup analyses in which the overall trends were similar to those observed for the total sample; nevertheless, results suggested there were differences in preferences among certain subgroups of patients. Females more strongly preferred the best T&E profile than males (12.5 vs 11.8), and males more strongly preferred the best PRN profile, compared with females (7.3 vs 6.4; both p<0.05). Both anti-VEGF naïve and anti-VEGF experienced patients had the strongest preference for the best T&E profile. However, compared with anti-VEGF naïve patients, anti-VEGF experienced patients more strongly preferred the best q8 profile (8.0 vs 7.2) and less strongly preferred the worst T&E profile (2.4 vs 3.2; both, p<0.05). Rural patients more strongly preferred the best q8 profile than urban patients (8.7 vs 7.5; p<0.05).
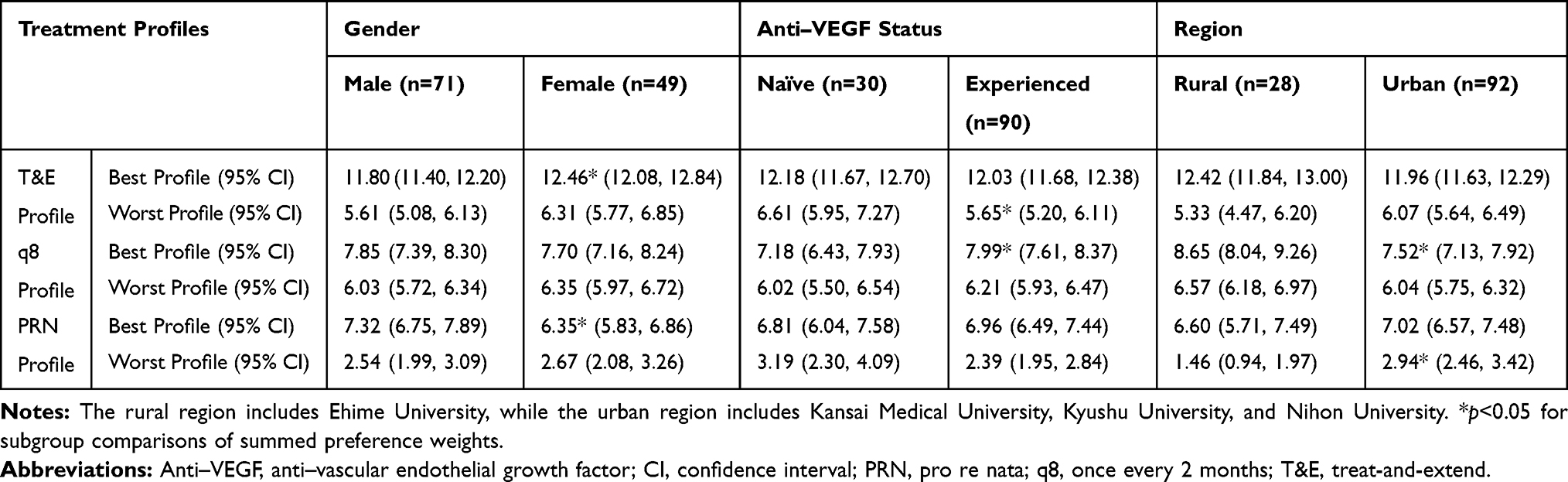 |
Table 5 Preferences for Selected Treatment Profiles: Subgroup Analyses |
A linear association was not observed between income and preferences. Preferences for the different treatment profiles were generally similar by income category. Preferences for the different treatment profiles were similar across groups based on BCVA at enrollment in the better- or the worse-seeing eye, age group, current anti-VEGF dosing regimen, or round-trip travel time to the hospital.
Discussion
The present study assessed patient preferences for attributes associated with PRN, q8, and T&E dosing regimens of anti-VEGF treatments for wAMD in Japan and found that patients are willing to make trade-offs among them. They are willing to accept increases in the number of intraocular injections required in the first 12 months of treatment, as well as increases in the number of physician consults in the first 12 months of treatment, in exchange for better visual acuity outcomes. In particular, they most valued increases in the chance of visual acuity maintenance after 2 years of treatment. These findings are consistent with a previous German study in wAMD, wherein the patients were willing to trade-off a heavier treatment burden, which included an additional 12.7 hrs spent for physician visits, to achieve stable visual acuity and avoid worse visual acuity,33 as well as other previous findings in which patients reported a clear preference for having good visual acuity over any other factor.34,45 Collectively, such findings are important, as good visual outcomes can potentially be maintained as long as the patient is willing to adhere to a regimen over a longer period of time.
The findings of this study suggest that Japanese patients with wAMD value longer-term over shorter-term visual acuity outcomes. Specifically, patients valued visual acuity maintenance after 2 years of treatment more than the chance of visual acuity markedly improving after 12 months of treatment and were willing to accept a higher number of injections required in the first 12 months of treatment for a greater chance of visual acuity maintenance after 2 years of treatment. Even though patients valued the high chance of visual acuity maintenance after 2 years of treatment, relative to the high number of injections required in the first 12 months of treatment, this does not necessarily mean that patients would need to receive a high number of injections in clinical practice. Yet, the optimal number of injections patients should receive may diverge from what they really are willing to accept in exchange for better visual acuity outcomes. Furthermore, the finding that patients are willing to accept a heavier treatment burden, which includes more injections at shorter intervals, as a trade-off for maintaining visual acuity in the longer-term, suggests that patients may fear disease recurrence more than intraocular injections.32
While T&E has more balanced profiles with respect to the chances of visual acuity markedly improving after 12 months of treatment and visual acuity maintenance after 2 years of treatment, as well as the number of injections required in the first 12 months of treatment, patients generally preferred T&E because of its association with the highest chance of visual acuity maintenance after 2 years of treatment. However, PRN or q8 profiles with fewer injections required in the first 12 months of treatment and a greater chance of visual acuity markedly improving after 12 months of treatment were preferred by patients, relative to the worst T&E profile (ie, 11 injections required in the first 12 months of treatment, 12 physician consultations in the first 12 months of treatment, 25% chance of visual acuity markedly improving after 12 months of treatment, and 96% chance of visual acuity maintenance after 2 years of treatment). This finding demonstrates that the negative perceptions of the high number of injections required in the first 12 months of treatment and lower chance of visual acuity markedly improving after 12 months of treatment, taken together, overshadowed patients’ positive perceptions of the high chance for visual acuity maintenance after 2 years of treatment. In a recent meta-analysis, T&E using ranibizumab was shown to be superior to PRN and as effective as monthly dosing in improving visual acuity outcomes,46 with a weighted frequency of 8.6 injections in 1 year.47 The worst T&E profile, which is associated with a high number of injections required in the first 12 months of treatment, is similar to a monthly dosing regimen. The worst T&E profile in this study was based on the available data at the time of the study, which included the Trex-AMD and LUCAS trials.9,38,48 The T&E data using IVT-AFL now available (eg, ALTAIR trial) suggest that approximately 7 injections are needed in the first year49 and 3.6 injections in the second year50 to achieve comparable (or even superior) visual acuity outcomes. Preferences for the worst T&E profile may have been different from what was observed in the current study if this profile had been associated with a less extreme number of injections required in the first 12 months of treatment, such as the number reported in the ALTAIR trial.
Gender differences observed in the current study, in which females more strongly preferred the best T&E regimen than males, and males more strongly preferred the best PRN regimen than females, may be due to variations in perceptions regarding investment, relative to expected outcomes. However, this hypothesis needs to be confirmed through further research. While, overall, the best T&E profile was most preferred by patients, subtle differences by anti-VEGF status were observed, in which anti-VEGF experienced (vs anti-VEGF naïve) patients more strongly preferred the best q8 profile and less strongly preferred the worst T&E profile. It is thus possible that anti-VEGF experienced patients may have an increased sensitivity or higher expectations than anti-VEGF naïve patients regarding treatment performance or outcomes, relative to the investment involved with anti-VEGF treatment. We hypothesized that income may influence patient preferences differentially depending upon age. Specifically, in Japan, copayments generally differ by age, with a higher out-of-pocket cost threshold for those up to 70 years (vs >70 years) old. However, a linear pattern of results was not observed for income groups. Rural patients in the current study more strongly preferred the best q8 profile than urban patients. As the rural region results were driven by a single site, firm conclusions cannot be drawn.
Overall, the findings suggest that, to improve patients’ acceptance of the optimal treatment regimen and number of injections for their wAMD, physicians should place greater emphasis in describing the impact on visual acuity outcomes, particularly the ability of a given treatment regimen to maintain longer-term visual acuity. Physicians should likewise be mindful of potential differences in preference, depending upon patient characteristics, and should adjust their communication with the patient, accordingly. To ensure patients are fully informed about their options, it would be ideal for physicians to first present the different treatment regimen alternatives and clearly explain the benefits and shortcomings of each, followed by a discussion of the costs entailed. An important aspect of healthcare policy in ophthalmology is shared decision-making,51 yet, as prior research shows, physicians may perceive difficulties in discussing dosing regimens with their patients,26 and they may also have little time to do so during the patients' visit. Thus, other health-care providers involved in the patient’s treatment for wAMD, such as nurses, can utilize standardized scripts to facilitate this communication with patients on the behalf of physicians.
Limitations
Due to sample selection during recruitment, respondents who were healthy enough to participate and were interested in research may have been over-represented, hence the possibility of selection bias. However, efforts were made to increase the representativeness of the sample (eg, collecting data at multiple sites, etc.). A further limitation is that only 25% of our study sample was anti-VEGF treatment-naïve; therefore, we cannot exclude the possibility that patients’ preferences may have been biased by their prior experiences with anti-VEGF treatment. Additionally, while the results suggest a specific pattern of preferences among patients in the aggregate study sample, motivation and adherence may potentially differ among individual patients, which may lead to different outcomes; this possibility will need to be addressed in a future research study. The overall patient sample was adequate for estimating fairly precise preference weights. However, subgroup sample sizes were relatively small, and subgroup comparisons may have been underpowered to detect statistically significant differences as a result.
The data collected in the DCE were based on responses to hypothetical anti-VEGF dosing regimen profiles. The choices presented in the DCE were intended to simulate possible treatment decisions, but do not have the same clinical, financial, or emotional consequences of actual decisions. The attributes and levels selected were designed to closely map onto the available clinical data, such as the LUCAS and TREX-AMD trials,49,50,52 at the time the study was conducted. As such, we were unable to consider more recent clinical evidence, such as data on the T&E dosing regimen from the ALTAIR trial, when developing the attributes and levels included in the DCE. Of note, while costs are relevant to treatment decisions, they are typically not included in a DCE. Specifically, costs are often a dominant factor in preferences, and they can greatly overshadow the effects of other attributes in the DCE, which may yield unstable estimates. Hence, the decision was made to exclude costs from the DCE in the current study.
Conclusions
In summary, the T&E dosing regimen was generally most preferred by patients due to its association with a greater chance of visual acuity maintenance after 2 years of treatment. The chance for longer-term visual acuity maintenance should be emphasized by physicians in discussions with patients about treatment, which may help to improve patient acceptance of and adherence to the optimal number of injections. Findings suggest that preferences may differ depending upon certain patient characteristics. Hence, physicians should take these factors into account when communicating with their patients about anti-VEGF treatment for wAMD.
Abbreviations
ANOVA, Analysis of Variance; Anti-VEGF, Anti-Vascular Endothelial Growth Factor; BCVA, Best-Corrected Visual Acuity; CCI, Charlson Comorbidity Index; CI, Confidence Interval; DCE, Discrete Choice Experiment; HB, Hierarchical Bayesian; IVT-AFL, Intravitreal Aflibercept; mT&E, Modified Treat-and-Extend; PRN, Pro Re Nata; q8, Every Two Months; SD, Standard Deviation; SE, Standard Error; T&E, Treat-and-Extend; wAMD, Wet Age-Related Macular Degeneration.
Data Sharing Statement
Bayer commits to sharing upon request from qualified scientific and medical researchers patient-level clinical trial data, study-level clinical trial data, and protocols from clinical trials in patients for medicines and indications approved in the US and European Union (EU) as necessary for conducting legitimate research. Interested researchers can use www.clinicalstudydatarequest.com to request access to available datasets and supporting documents from clinical studies to conduct further research that can help advance medical science or improve patient care. Information on the Bayer criteria for listing studies and other relevant information is provided in the “Study sponsors” section of the portal. Data access will be granted to available datasets, protocols, and clinical study reports after approval by an independent scientific review panel. Bayer is not involved in the decisions made by the independent review panel. Bayer will take all necessary measures to ensure that patient privacy is safeguarded.
Acknowledgments
The authors would like to thank the patients who participated in the study, the investigators and site coordinators, Junko Chojamori, Yuki Nishiyama, and Nobuyuki Sasaoka at Bayer Yakuhin for site recruitment support, and Leo J. Philip Tharappel and Urmila Rao from Indegene Pvt. Ltd for providing writing and editorial support.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
This study was funded by Bayer Yakuhin, Ltd. The funder was involved in the study design, data collection, data analysis, decision to publish, and preparation of the manuscript. Kantar, LLC. was contracted by Bayer Yakuhin, Ltd, and was involved in data collection, data analysis and medical writing.
Disclosure
TJ has received honorarium from Bayer Yakuhin. YN has received honorarium from Bayer Yakuhin, Santen Pharmaceutical, Alcon Pharmaceuticals, Senju Pharmaceutical, JFC Sales Plan and Kowa Pharmaceutical. RM has received honorarium from Alcon Pharmaceuticals, Bayer Yakuhin, Santen Pharmaceutical, Pfizer, Senju Pharmaceutical, and JFC Sales Plan. K Tanaka has received honorarium from Santen Pharmaceutical, Alcon Pharmaceuticals, Bayer Yakuhin, and Novartis. YO has received honorarium from Alcon Pharmaceutical and Bayer Yakuhin. YH and T Kakahashi are employees of Bayer Yakuhin. JC is an employee of Bayer Consumer Care. MCM, OW, and KB have provided consultancy to Bayer Yakuhin and are employees of Kantar. KT has received grants from Santen Pharmaceutical, Hoya, AMO, Alcon Pharmaceuticals, Pfizer, Senju Pharmaceutical and Sun Contact Lens, and has received honorarium from Novartis, Santen Pharmaceutical, Alcon Pharmaceuticals, Bayer Yakuhin, Pfizer, Otsuka Pharmaceutical and Zeiss.
References
1. Mitchell P, Liew G, Gopinath B, Wong TY. Age-related macular degeneration. Lancet. 2018;392(10153):1147–1159. doi:10.1016/S0140-6736(18)31550-2
2. Mayo Clinic. Wet macular degeneration. Available from: https://www.mayoclinic.org/diseases-conditions/wet-macular-degeneration/symptoms-causes/syc-20351107.
3. Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014;2(2):e106–e116. doi:10.1016/S2214-109X(13)70145-1
4. Oshima Y, Ishibashi T, Murata T, Tahara Y, Kiyohara Y, Kubota T. Prevalence of age related maculopathy in a representative Japanese population: the Hisayama study. Br J Ophthalmol. 2001;85(10):1153–1157. doi:10.1136/bjo.85.10.1153
5. Takahashi K, Ogura Y, Ishibashi T, Shiraga F, Yuzawa M. Treatment guidelines for age-related macular degeneration. Nihon Ganka Gakkai Zasshi. 2012;116(12):1150–1155.
6. Lanzetta P, Loewenstein A. Vision academy steering committee. Fundamental principles of an anti-VEGF treatment regimen: optimal application of intravitreal anti-vascular endothelial growth factor therapy of macular diseases. Graefes Arch Clin Exp Ophthalmol. 2017;255(7):1259–1273. doi:10.1007/s00417-017-3647-4
7. Rosenfeld PJ, Brown DM, Heier JS, et al. Ranibizumab for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1419–1431. doi:10.1056/NEJMoa054481
8. Brown DM, Michels M, Kaiser PK, et al. Ranibizumab versus verteporfin photodynamic therapy for neovascular age-related macular degeneration: two-year results of the ANCHOR study. Ophthalmology. 2009;116(1):57–65.e5. doi:10.1016/j.ophtha.2008.10.018
9. Wykoff CC, Croft DE, Brown DM, et al. Prospective trial of treat-and-extend versus monthly dosing for neovascular age-related macular degeneration: TREX-AMD 1-year results. Ophthalmology. 2015;122(12):2514–2522. doi:10.1016/j.ophtha.2015.08.009
10. Lalwani GA, Rosenfeld PJ, Fung AE, et al. A variable-dosing regimen with intravitreal ranibizumab for neovascular age-related macular degeneration: year 2 of the PrONTO study. Am J Ophthalmol. 2009;148(1):43–58.e1. doi:10.1016/j.ajo.2009.01.024
11. Martin DF, Maguire MG, Fine SL, et al. Ranibizumab and bevacizumab for treatment of neovascular age-related macular degeneration. Ophthalmology. 2012;119(7):1388–1398. doi:10.1016/j.ophtha.2012.03.053
12. Chakravarthy U, Harding SP, Rogers CA, et al. Ranibizumab versus bevacizumab to treat neovascular age-related macular degeneration. Ophthalmology. 2012;119(7):1399–1411. doi:10.1016/j.ophtha.2012.04.015
13. Ho AC, Busbee BG, Regillo CD, et al. Twenty-four-month efficacy and safety of 0.5 mg or 2.0 mg ranibizumab in patients with subfoveal neovascular age-related macular degeneration. Ophthalmology. 2014;121(11):2181–2192. doi:10.1016/j.ophtha.2014.05.009
14. Busbee BG, Ho AC, Brown DM, et al. Twelve-month efficacy and safety of 0.5 mg or 2.0 mg ranibizumab in patients with subfoveal neovascular age-related macular degeneration. Ophthalmology. 2013;120(5):1046–1056. doi:10.1016/j.ophtha.2012.10.014
15. van Asten F, Evers-Birkenkamp KU, van Lith-verhoeven JJC, et al. A prospective, observational, open-label, multicentre study to investigate the daily treatment practice of ranibizumab in patients with neovascular age-related macular degeneration. Acta Ophthalmol. 2015;93(2):126–133. doi:10.1111/aos.12610
16. Ferreira A, Sagkriotis A, Olson M, Lu J, Makin C, Milnes F. Treatment frequency and dosing interval of ranibizumab and aflibercept for neovascular age-related macular degeneration in routine clinical practice in the USA. PLoS One. 2015;10(7):e0133968. doi:10.1371/journal.pone.0133968
17. Mantel I. Optimizing the anti-VEGF treatment strategy for neovascular age-related macular degeneration: from clinical trials to real-life requirements. Transl Vis Sci Technol. 2015;4(3):6. doi:10.1167/tvst.4.3.6
18. Wolf A, Kampik A. Efficacy of treatment with ranibizumab in patients with wet age-related macular degeneration in routine clinical care: data from the COMPASS health services research. Graefes Arch Clin Exp Ophthalmol. 2014;252(4):647–655. doi:10.1007/s00417-013-2562-6
19. Heier JS, Brown DM, Chong V, et al. Intravitreal aflibercept (VEGF trap-eye) in wet age-related macular degeneration. Ophthalmology. 2012;119(12):2537–2548. doi:10.1016/j.ophtha.2012.09.006
20. Oubraham H, Cohen SY, Samimi S, et al. Inject and extend dosing versus dosing as needed. Retina. 2011;31(1):26–30. doi:10.1097/IAE.0b013e3181de5609
21. Silva R, Berta A, Larsen M, et al. Treat-and-extend versus monthly regimen in neovascular age-related macular degeneration. Ophthalmology. 2018;125(1):57–65. doi:10.1016/j.ophtha.2017.07.014
22. Haga A, Kawaji T, Ideta R, Inomata Y, Tanihara H. Treat-and-extend versus every-other-month regimens with aflibercept in age-related macular degeneration. Acta Ophthalmol. 2018;96(3):e393–e398. doi:10.1111/aos.13607
23. DeCroos FC, Reed D, Adam MK, et al. Treat-and-extend therapy using aflibercept for neovascular age-related macular degeneration: a prospective clinical trial. Am J Ophthalmol. 2017;180:142–150. doi:10.1016/j.ajo.2017.06.002
24. Barthelmes D, Nguyen V, Daien V, et al. Two year outcomes of “treat and extend” intravitreal therapy using aflibercept preferentially for neovascular age-related macular degeneration. Retina. 2018;38(1):20–28. doi:10.1097/IAE.0000000000001496
25. Koh A, Lanzetta P, Lee W, Lai -C-C, Chan W-M, Yang C-M. Recommended guidelines for use of intravitreal aflibercept with a treat-and-extend regimen for the management of neovascular age-related macular degeneration in the Asia-Pacific region: report from a consensus panel. Asia-Pac J Ophthalmol (Phila). 2017;6(3):296–302. doi:10.22608/APO.2016125
26. Iida T, Ishii K. Physician, patient, and caregiver experience of different wet age-related macular degeneration anti-VEGF treatment regimens in Japan: a qualitative assessment. Clin Ophthalmol. 2016;10:2505–2513. doi:10.2147/OPTH
27. EYLEA® (aflibercept) injection approved for the treatment of wet age-related macular degeneration in Japan. Available from: https://investor.regeneron.com/news-releases/news-release-details/eylear-aflibercept-injection-approved-treatment-wet-age-0.
28. Lindhiem O, Bennett CB, Trentacosta CJ, McLear C. Client preferences affect treatment satisfaction, completion, and clinical outcome: a meta-analysis. Clin Psychol Rev. 2014;34(6):506–517. doi:10.1016/j.cpr.2014.06.002
29. Hughes TM, Merath K, Chen Q, et al. Association of shared decision-making on patient-reported health outcomes and healthcare utilization. Am J Surg. 2018;216(1):7–12. doi:10.1016/j.amjsurg.2018.01.011
30. Hack TF, Degner LF, Watson P, Sinha L. Do patients benefit from participating in medical decision making? Longitudinal follow-up of women with breast cancer. Psychooncology. 2006;15(1):9–19. doi:10.1002/(ISSN)1099-1611
31. Schoenthaler A, Rosenthal DM, Butler M, Jacobowitz L. Medication adherence improvement similar for shared decision-making preference or longer patient-provider relationship. J Am Board Fam Med. 2018;31(5):752–760. doi:10.3122/jabfm.2018.05.180009
32. Droege KM, Muether PS, Hermann MM, et al. Adherence to ranibizumab treatment for neovascular age-related macular degeneration in real life. Graefes Arch Clin Exp Ophthalmol. 2013;251(5):1281–1284. doi:10.1007/s00417-012-2177-3
33. Mueller S, Agostini H, Ehlken C, Bauer-Steinhusen U, Hasanbasic Z, Wilke T. Patient preferences in the treatment of neovascular age-related macular degeneration. Ophthalmology. 2016;123(4):876–883. doi:10.1016/j.ophtha.2015.12.001
34. Baxter JM, Fotheringham AJ, Foss AJE. Determining patient preferences in the management of neovascular age-related macular degeneration: a conjoint analysis. Eye (Lond). 2016;30(5):698–704. doi:10.1038/eye.2016.18
35. Mangham LJ, Hanson K, McPake B. How to do (or not to do) … Designing a discrete choice experiment for application in a low-income country. Health Policy Plan. 2009;24(2):151–158. doi:10.1093/heapol/czn047
36. Bridges JFP, Hauber AB, Marshall D, et al. Conjoint analysis applications in health—a checklist: a report of the ISPOR good research practices for conjoint analysis task force. Value Health. 2011;14(4):403–413. doi:10.1016/j.jval.2010.11.013
37. Ministry of Education, Culture, Sports, Science and Technology, and Ministry of Health, Labour and Welfare, Japan. Ethical Guidelines for Medical and Health Research Involving Human Subjects. Tokyo, Japan; 2015.
38. Berg K, Pedersen TR, Sandvik L, Bragadóttir R. Comparison of ranibizumab and bevacizumab for neovascular age-related macular degeneration according to LUCAS treat-and-extend protocol. Ophthalmology. 2015;122(1):146–152. doi:10.1016/j.ophtha.2014.07.041
39. Rayess N, Houston SKS, Gupta OP, Ho AC, Regillo CD. Treatment outcomes after 3 years in neovascular age-related macular degeneration using a treat-and-extend regimen. Am J Ophthalmol. 2015;159(1):3–8.e1. doi:10.1016/j.ajo.2014.09.011
40. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
41. Quan H, Li B, Couris CM, et al. Updating and validating the Charlson Comorbidity Index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am J Epidemiol. 2011;173(6):676–682. doi:10.1093/aje/kwq433
42. Kuhfeld WF. Marketing Research Methods in SAS. Experimental Design, Choice, Conjoint, and Graphical Techniques. Cary, NC, USA; 2010.
43. Hauber AB, González JM, Groothuis-Oudshoorn CGM, et al. Statistical methods for the analysis of discrete choice experiments: a report of the ISPOR conjoint analysis good research practices task force. Value Health. 2016;19(4):300–315. doi:10.1016/j.jval.2016.04.004
44. Brown MM, Brown GC, Sharma S, Landy J, Bakal J. Quality of life with visual acuity loss from diabetic retinopathy and age-related macular degeneration. Arch Ophthalmol. 2002;120(4):481–484. doi:10.1001/archopht.120.4.481
45. Vennedey V, Danner M, Evers SM, et al. Using qualitative research to facilitate the interpretation of quantitative results from a discrete choice experiment: insights from a survey in elderly ophthalmologic patients. Patient Prefer Adherence. 2016;10:993–1002. doi:10.2147/PPA
46. Okada M, Kandasamy R, Chong EW, McGuiness M, Guymer RH. The treat-and-extend injection regimen versus alternate dosing strategies in age-related macular degeneration: a systematic review and meta-analysis. Am J Ophthalmol. 2018;192:184–197. doi:10.1016/j.ajo.2018.05.026
47. Rufai SR, Almuhtaseb H, Paul RM, et al. A systematic review to assess the ‘treat-and-extend’ dosing regimen for neovascular age-related macular degeneration using ranibizumab. Eye. 2017;31(9):1337–1344. doi:10.1038/eye.2017.67
48. Wykoff CC, Ou WC, Brown DM, et al. Randomized trial of treat-and-extend versus monthly dosing for neovascular age-related macular degeneration: 2-year results of the TREX-AMD study. Ophthalmol Retina. 2017;1(4):314–321. doi:10.1016/j.oret.2016.12.004
49. Ohji M, Okada AA, Takahashi K, Kobayashi M, Terano Y. Two different treat-and-extend dosing regimens of intravitreal aflibercept in Japanese patients with wet age-related macular degeneration: 96 week results of the ALTAIR study. In
50. Ohji M, Okada AA, Takahashi K, Kobayashi M, Terano Y. Two different treat and extend dosing regimens of intravitreal aflibercept for wAMD in Japanese patients: 52 weeks results of the ALTAIR study. In
51. Stuart A The whys and hows of shared decision making. EyeNet Magazine. January, 2015:27–28. doi:10.3389/fped.2015.00027
52. Wai KM, Singh RP. Treat and extend dosing regimen with anti-vascular endothelial growth factor agents for neovascular age-related macular degeneration. Am J Ophthalmic Clin Trials. 2018;1(1):1–6. doi:10.25259/AJOCT-2-2018
53. Iida T, Narimatsu A, Adachi K, Wang EC. Anti-vascular endothelial growth factor outpatient treatment patterns in patients with exudative age-related macular degeneration from a Japanese hospital claims database. J Health Econ Outcomes Res. 2014;2(1):41–52.
54. Talks JS, Lotery AJ, Ghanchi F, et al. First-year visual acuity outcomes of providing aflibercept according to the VIEW study protocol for age-related macular degeneration. Ophthalmology. 2016;123(2):337–343. doi:10.1016/j.ophtha.2015.09.039
55. Uemura H, Matsubara N, Kimura G, et al. Patient preferences for treatment of castration-resistant prostate cancer in Japan: a discrete-choice experiment. BMC Urol. 2016;16(1):63. doi:10.1186/s12894-016-0182-2
56. CATT Research Group, Martin DF, Maguire MG, et al. Ranibizumab and bevacizumab for neovascular age-related macular degeneration. N Engl J Med. 2011;364(20):1897–1908.
57. Brown DM, Kaiser PK, Michels M, et al. Ranibizumab versus verteporfin for neovascular age-related macular degeneration. N Engl J Med. 2006;355(14):1432–1444. doi:10.1056/NEJMoa062655
58. Abedi F, Wickremasinghe S, Islam AFM, Inglis KM, Guymer RH. Anti-VEGF treatment in neovascular age-related macular degeneration. Retina. 2014;34(8):1531–1538. doi:10.1097/IAE.0000000000000134
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.