Back to Journals » Patient Preference and Adherence » Volume 19
Patient Preference and Time Allocation Associated with Transition from Intravenous to Subcutaneous Administration of Natalizumab (Tysabri) in Patients with Relapsing Remitting MS – A Questionnaire Study
Authors Almroth A, Söderbärg K, Sjöblom I
Received 27 June 2025
Accepted for publication 26 November 2025
Published 23 December 2025 Volume 2025:19 Pages 4233—4244
DOI https://doi.org/10.2147/PPA.S549951
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Anna Almroth,1 Karin Söderbärg,1 Irina Sjöblom2
1Biogen Sweden AB, Stockholm, Sweden; 2Neurology Department, Uppsala University Hospital, Uppsala, Sweden
Correspondence: Anna Almroth, Email [email protected]
Introduction: Natalizumab (NTZ, Tysabri, Biogen) is an established treatment for highly active relapsing-remitting multiple sclerosis (RRMS), administered either intravenously (IV) in hospital settings or subcutaneously (SC), the latter of which can be administered in primary care. This study investigated self-reported preferences, satisfaction, and time allocation of patients and healthcare professionals (HCPs).
Methods: A total of 83 patients with RRMS and 14 HCPs participated and completed questionnaires across five Swedish hospitals. Participants had experience with both NTZ IV and SC administration, and data collection focused on time efficiency, impact on daily activities, satisfaction, and the ease of transitioning to SC.
Results: SC administration was reported as more time-efficient, with 72% of patients spending ≤ 30 min at the hospital vs 83% reporting 1– 2 h for IV. In primary care, 75% of patients reported that SC treatments required less than 15 minutes. The setting of the SC administration had an effect on work disruption according to patients; 60% of patients in primary care reported no impact on work, compared to 35% for SC treatments in hospitals. Regarding preference, 80% of patients favoured SC over IV. Among patients offered SC in primary care, 75% preferred it over hospital treatment. HCPs reported shorter preparation times and improved workflow efficiency with SC, with 93% completing SC treatments within 30 minutes. Both patients and HCPs found the transition from IV to SC manageable, and 86% of HCPs expressed confidence in their ability to inform patients about SC administration.
Discussion: The results align with previous studies, showing SC NTZ provides time savings, less disruption to daily life, and high satisfaction for patients and HCPs. Its feasibility in primary care supports broader adoption, with implications for improving healthcare resource allocation and patient adherence. Future research should focus on long-term outcomes and global implementation.
Keywords: natalizumab, adherence, subcutaneous, preference
Introduction
Highly active relapsing-remitting multiple sclerosis (RRMS) is a form of MS characterized by frequent and severe relapses with incomplete recovery.1 It is associated with active inflammation in the central nervous system, visible as new or enlarging lesions on MRI scans. Symptoms may include vision problems, muscle weakness, numbness, and difficulty with coordination or balance.
Natalizumab (NTZ, Tysabri, Biogen) is a monoclonal antibody and is an established treatment for highly active RRMS. There are two methods of administering NTZ: intravenous infusion (NTZ IV), which has been the standard, and subcutaneous injection (NTZ SC), a more recently available option. NTZ IV requires administration in a hospital setting. Following a label update in 2024, NTZ SC is now approved for use outside hospital settings.2 This form of administration (NTZ SC) allows for easier and faster dosing, potentially improving convenience and accessibility for patients.
The SC version maintains similar efficacy and safety profiles to the infusion, making it a valuable option for managing relapsing forms of MS.3–5 A recent study published in the Multiple Sclerosis and Related Disorders journal assessed the non-inferiority of SC versus IV administration of natalizumab, each administered once every four weeks, in RRMS patients. The findings supported that SC administration was not inferior to IV administration concerning efficacy, providing an alternative route that may offer greater convenience for patient.6 The transition from NTZ IV to SC administration may also carry important economic and organizational implications.7 IV infusions typically require more healthcare resources, including dedicated infusion facilities, specialized staff, and longer appointment times. SC administration, on the other hand, may be performed in shorter visits and even has the potential for home administration in some healthcare systems, thereby reducing the overall burden on infusion units and freeing up capacity for other treatments. For patients, reduced travel time, shorter visits, and increased flexibility may translate into improved quality of life, greater adherence, and reduced indirect costs such as time away from work or caregiving responsibilities. However, potential barriers to wider SC adoption, including safety perceptions and healthcare system constraints, may be considered.
From a health economic perspective, the cost-effectiveness of SC versus IV administration is not solely dependent on the drug cost but also on time allocation, healthcare utilization, and patient preferences.8 As healthcare systems aim to optimize both clinical outcomes and resource use, understanding how patients perceive and value different modes of administration becomes essential.
Despite the growing availability of SC natalizumab, limited real-world data exist on how patients experience this transition, and how it affects their time, daily life, and treatment satisfaction. Furthermore, little is known about whether patients perceive the SC option as more convenient, more flexible, or potentially less safe compared to the traditional IV route. The purpose of this study was to investigate general satisfaction and impact on time allocation, for HCPs and patients with experience of both IV and SC administration of NTZ. Moreover, this study specifically explored the use of NTZ SC in a primary care setting.
Part 1. Administration in hospital (IV and SC).
Part 2. Administration in primary care (SC).
Materials and Methods
This observational, prospective, non-interventional study was based on questionnaires completed by adult patients with relapsing-remitting multiple sclerosis (RRMS) and their healthcare professionals (HCPs) to evaluate preferences, satisfaction, and time allocation for subcutaneous (SC) versus intravenous (IV) administration of natalizumab (NTZ, Tysabri, Biogen). The study further assessed the ease of transitioning from IV to SC administration, as perceived by HCPs. The surveys consisted of two questionnaires. Both questionnaires were completed by HCPs and patients with RRMS to capture time allocation and general satisfaction with each route of NTZ administration. Questionnaire 1 focused on NTZ administration in a hospital setting, while questionnaire 2 addressed NTZ administration in a primary care setting.
The study was conducted across five hospitals in Sweden between February 2022 (first patient in) and June 2023 (last patient out). Patients with RRMS who were currently receiving NTZ treatment and HCPs involved in its administration were included in the study.
Patients were recruited by their treating HCPs during routine care visits. Eligible patients were adults aged 18–65 years with RRMS, having at least six months of NTZ treatment experience, and having received at least one prior administration of both SC and IV NTZ. Additionally, HCPs involved in NTZ administration, such as nurses and physicians, were invited to complete a survey assessing their perspectives on SC and IV methods. The study aimed to include at least 50 patients and 15 HCPs. Recruitment continued until the target sample size was achieved or for a maximum of six months.
The patient survey was structured into two parts (see Appendix). The first part focused on IV administration, capturing patient experiences related to time spent at the hospital, the impact of treatment on daily activities, and opportunities for communication with healthcare professionals during IV treatment. The second part addressed SC administration, assessing similar metrics while also including additional questions about patient preferences, the ease of transitioning from IV to SC, and the reasons for choosing SC administration.
The HCP survey explored various aspects of NTZ administration. It assessed the time required for preparation and administration of both IV and SC methods, the perceived benefits and challenges of SC administration, and the ease of transition for patients. Additionally, the survey examined overall satisfaction with SC administration from a clinical perspective and the role of HCPs in facilitating the transition to SC.
The patient survey included both ordinal and nominal response options, with Likert scale questions to evaluate satisfaction, communication, and the perceived burden of treatment. The HCP survey included categorical questions addressing preparation time, workflow impact, and patient engagement.
Quantitative data from the surveys were summarized using descriptive statistics. Proportions and percentages were calculated to compare responses between SC and IV administration for both patients and HCPs. Comparative descriptive analysis focused on time efficiency, satisfaction, and reasons for preferences. Qualitative responses from open-ended questions were thematically analysed to identify key drivers of preferences and perceived barriers. As this was a cross-sectional survey study with a descriptive aim and no pre-specified hypothesis, inferential statistical testing (eg, p-values) was not performed. Ethical approval for the study was obtained on February 9, 2022 (Dnr 2021–06786-01) from the Swedish Ethical Review Authority. All participants provided informed consent, and data were anonymized to ensure confidentiality. The study adhered to national and international guidelines for the ethical conduct of research involving human subjects. The study complies with the Declaration of Helsinki.
Results
Participant Characteristics
A total of 83 patients with relapsing-remitting multiple sclerosis (RRMS) and 14 healthcare professionals (HCPs) participated in in the first questionnaire (Table 1). Among the patients, 83% were female, reflecting the known higher prevalence of RRMS among women. Sixty percent of patients were between 36 and 55 years old, 23% were aged 26–35 years, 13% were aged 56–65 years, and 4% were aged 18–25 years. No patients were over 65 years of age. (Table 1). All patients had at least six months of natalizumab (NTZ, Tysabri, Biogen) treatment experience and had received at least one administration of both intravenous (IV) and subcutaneous (SC) NTZ. The 14 participating HCPs included nurses and physicians actively involved in administering NTZ. These professionals had substantial experience with both IV and SC administration and were recruited from the same clinics where the patient data were collected. In the second questionnaire, a total of 12 patients from four primary care sites were included (Table 1).
 |
Table 1 Study Participant Characteristics by Survey. A Total of 83 Patients with Relapsing-Remitting Multiple Sclerosis (RRMS) and 14 Healthcare Professionals (HCPs) Participated in the First Survey |
Time Efficiency
Both patients and HCPs identified SC administration as a more time-efficient method of administration compared to IV. The perceived time efficiency results are presented in Figure 1. Among patients, 72% spent ≤30 minutes in the hospital for SC treatment, as compared to 83% who reported spending 1–2 hours for IV treatment. Additionally, SC administration reduced time away from work, with 73% of patients reporting ≤2 work hours lost for SC. On the contrary, 57% of patients receiving NTZ IV reported to spend more than 2 hours in the hospital (Figure 2). For SC treatment administered in a primary care setting, 75% of patients reported that the process required less than 15 minutes, while 25% indicated it required 15–30 minutes. No patients reported spending more than 30 minutes for NTZ SC treatment in a primary care setting.
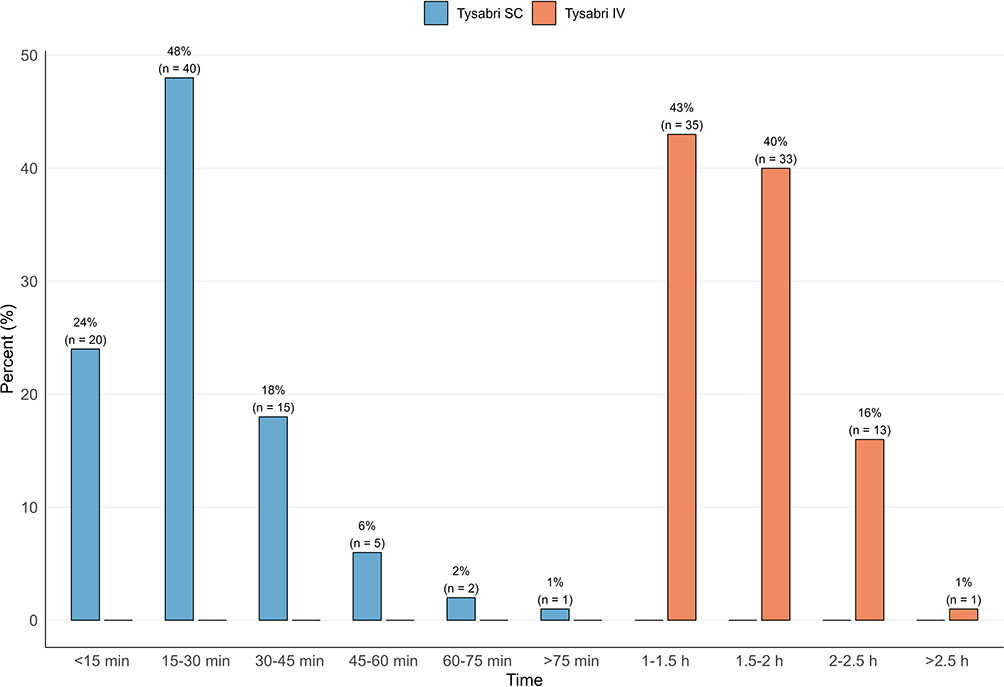 |
Figure 1 Total time spent at the hospital, patient reported. 72% spent ≤30 minutes in the hospital for SC treatment, as compared to 83% who reported spending 1–2 hours for IV treatment. |
 |
Figure 2 Time away from work in connection to treatment, patient reported. The majority of the patients (57%) receiving NTZ IV reported to spend more than 2 hours in the hospital. |
From the HCP perspective, SC preparation times were notably shorter compared to IV administration. For SC treatments, 93% of HCPs reported that they required less than 5 minutes for preparation, and 7% that they required between 5 and 10 minutes. In contrast, for IV treatments, 64% required less than 10 minutes, 29% used 10–15 minutes, and 7% used 16–20 minutes. SC treatments also required considerably less total time at the hospital, with 93% of SC treatments completed within 30 minutes and the remaining 7% completed within 31–45 minutes. In comparison, only 14% of IV treatments were reported to be completed within 60–80 minutes, 71% required 81–100 minutes, and 14% required 121–140 minutes, according to the respondents.
Additionally, all HCPs noted that transitioning from IV to SC administration resulted in some degree of time savings, with 46% reporting that SC administration provided significant time savings, enabling a more streamlined workflow. HCPs also supported moving NTZ SC administration to primary care, with three out of four agreeing that administering NTZ SC in primary care offered additional benefits beyond time savings. Specifically, 50% of HCPs agreed completely, 25% largely agreed, and 25% agreed to some extent. Notably, no HCPs expressed disagreement.
Impact on Daily Activities
SC administration was reported to have lower impact on patients’ daily activities compared to IV administration. A total of 63% of patients indicated that SC had no limitations on their daily routines, compared to 46% for IV. Only 1% of patients found SC treatment to be sometimes limiting, compared to 7% for IV, and 2% reported SC treatment to be always limiting, compared to 6% for IV (Figure 3).
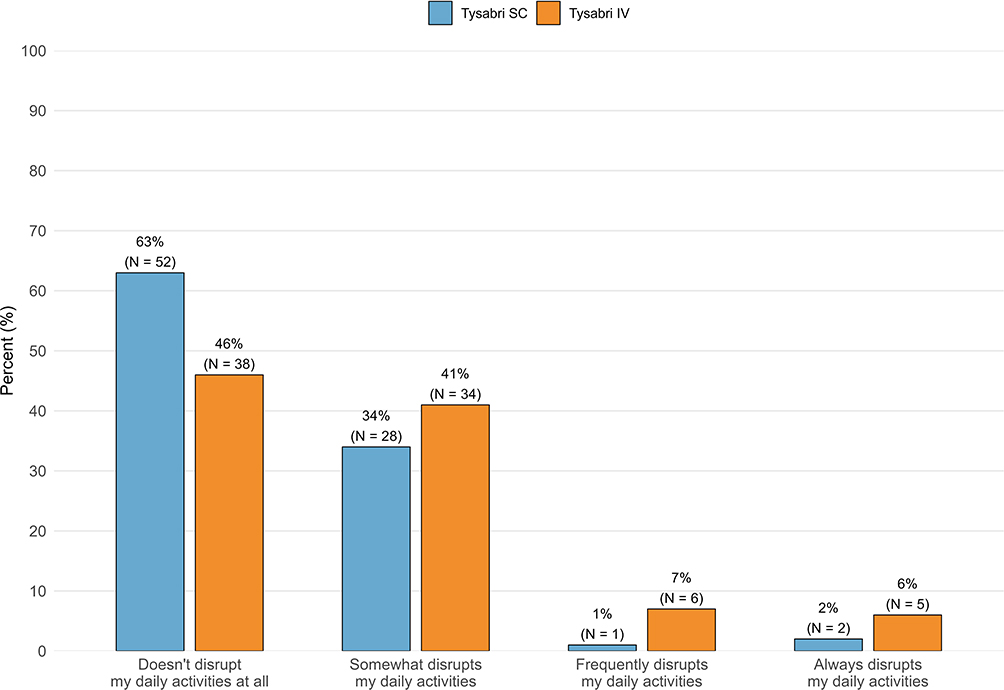 |
Figure 3 Perceived impact of NTZ administration route on patients’ daily activities. Eg a total of 63% of patients indicated that SC had no limitations on their daily routines, compared to 46% for IV. |
Among patients receiving NTZ SC in primary care, 83% reported no limitations on their daily routines, highlighting the additional benefit of primary care settings. The option of administering NTZ SC in a primary care setting also resulted in a reduced impact on patients’ work, with 60% stating it never affected their work-, compared to 35% for SC administration at the hospital (Figure 4).
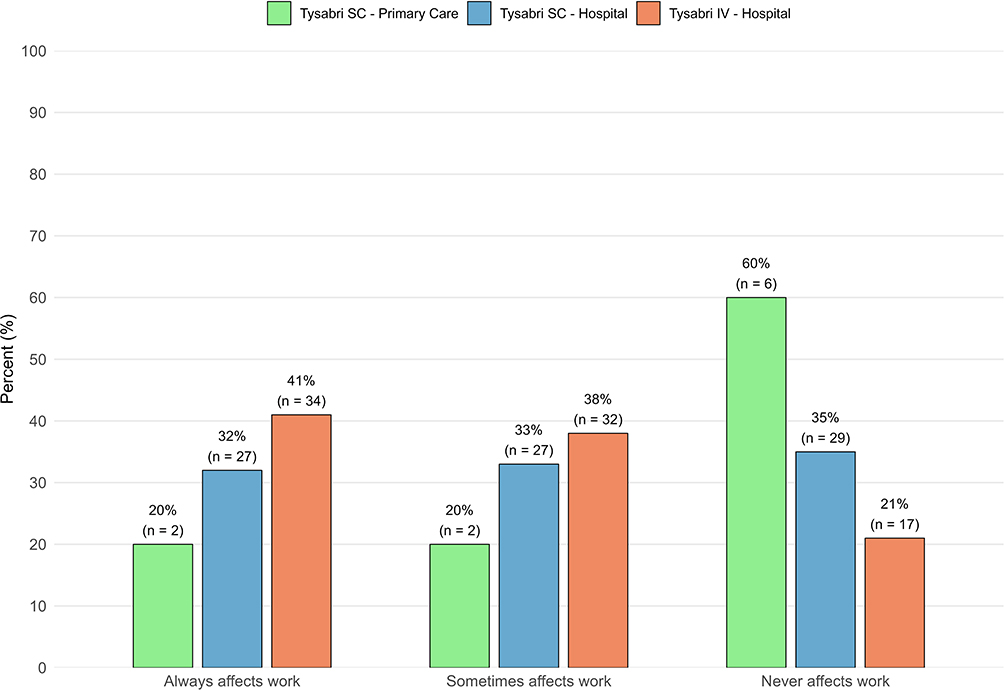 |
Figure 4 Patient-reported impact of NTZ treatment on work. The option of administering NTZ SC in a primary care setting also resulted in a reduced impact on patients’ work, with 60% stating it never affected their work-, compared to 35% for SC administration at the hospital. |
HCPs also highlighted that the reduced time commitment and flexibility of SC administration not only minimized disruptions to patients’ daily lives but also provided additional benefits, such as improved patient satisfaction and enhanced workflow efficiency.
Communication with Healthcare Professional
SC administration did not negatively affect communication opportunities between patients and HCPs. A majority (74%) of patients reported that SC administration did not reduce their ability to discuss relevant issues regarding their disease and treatment with healthcare staff. Specifically, 69% indicated that communication opportunities remained unchanged, and 5% reported that SC administration even improved their perception of the quality of the communication with the HCP. 23% reported slightly reduced opportunities compared to IV. All HCPs agreed that it was easy to provide information about the switch from IV to SC administration, with 29% strongly agreeing. (Figure 5).
 |
Figure 5 HCP opinion on ease of providing information to patients about the switch from IV to SC administration. All HCPs agreed that it was easy to provide information about the switch from IV to SC administration, with 29% strongly agreeing. |
Preference and Satisfaction
The majority of the patients expressed a strong preference for SC administration over IV overall. A total of 80% preferred SC over IV, 9% preferred IV over SC and 11% had no opinion regarding the type of administration. With regards to time consumption, all patients favoured SC over IV, with 55% describing SC as a “big improvement” and 33% as “an improvement” and 12% as “some improvement” compared to IV (Figure 6).
 |
Figure 6 Patient opinions on time consumption of NTZ SC versus IV administration. All patients favoured SC over IV, with 55% describing SC as a “big advantage” and 33% as “an advantage” and 12% as “some advantage” compared to IV. |
When comparing primary care settings to hospital-based administration, 75% of patients preferred SC administration in a primary care setting, 17% preferred SC administration in a hospital setting, and 8% had no preference (Figure 7).
 |
Figure 7 Patient-preferred administration setting of NTZ SC. Three out of four (75%) of patients preferred SC administration in a primary care setting, 17% preferred SC administration in a hospital setting, and 8% had no preference. |
The transition from IV to SC administration was reported to be smooth by both patients and HCPs. Patients found the transition process manageable, with more than 80% accepting the switch to SC. HCPs similarly endorsed the transition process, with all HCPs finding it easy to provide information about the switch from IV to SC, and 86% expressing confidence in their knowledge and ability to inform patients about SC administration.
Discussion
Summary of Findings
This study investigated the preferences, satisfaction, and time efficiency of subcutaneous (SC) versus intravenous (IV) administration of natalizumab (NTZ, Tysabri, Biogen) in patients with relapsing-remitting multiple sclerosis (RRMS) and healthcare professionals (HCPs). The findings demonstrated that SC administration was preferred by both patients and HCPs due to its reported time savings, reduced impact on daily activities, and increased perceived practicality. Among patients, 80% favoured SC over IV administration, and 75% preferred receiving SC treatment in a primary care setting compared to a hospital. SC administration was also reported to have a lower impact on patients’ daily activities, with 83% of patients in primary care reporting that their treatment posed no limitations on their everyday routines compared to 46% for IV. Notably, HCPs reported pronounced workflow benefits with SC, with 93% of treatments completed within 30 minutes and shorter preparation times compared to IV. The transition from IV to SC was perceived as smooth, with both patients and HCPs expressing confidence in the process.
Discussion and Comparison to Other Studies
The preference for SC administration observed in this study aligns with findings from previous research on SC versus IV treatments in chronic conditions, including multiple sclerosis.8–12 Time efficiency and reduced burden on daily activities have consistently been highlighted as key drivers of preference for SC administration in similar studies.12 The high acceptance rate of SC administration (90% of patients) observed in this study aligns with findings from other studies reporting similarly positive experiences among patients and HCPs, as well as significant time savings during transitions from IV to SC administration across various therapeutic areas.9,10 The observational SISTER study provides real-world evidence supporting SC administration of natalizumab in RRMS patients.12 A high proportion of patients favoured SC over IV administration, with over 90% of those starting on SC expressing continued preference. Many patients on IV also reported interest in switching to SC, highlighting its perceived convenience. Treatment satisfaction remained high across both groups and improved over time, particularly after switching from IV to SC. SC administration was also associated with shorter clinic visits, offering practical time savings for both patients and healthcare providers. In the NOVA Phase IIIb extension study, 87.8% of patients with RRMS preferred NTZ SC administration over IV.8 Additionally, the EASIER study, a multicentre observational study conducted across nine Italian MS canters, reported that NTZ SC administration led to a 50% reduction in patient procedure time and a 55% decrease in active working time for healthcare professionals compared to IV administration.11 In a recent cost-analysis study, they demonstrated that NTZ SC significantly reduced healthcare resource utilization and overall treatment costs compared to IV administration.7 These findings underscore the economic advantage of SC administration, particularly when considering streamlined patient care pathways and reduced time demands on both patients and healthcare providers. Also, the improved communication opportunities reported by some patients and the perceived ease of providing information by HCPs in this study underscore the importance of adequate education and support during transitions to SC administration. These findings align with prior research emphasizing that effective communication and patient education are essential not only for maintaining satisfaction during changes in treatment modality but also for fostering adherence to treatment over time.13,14 Collectively, these studies suggest that SC administration of natalizumab is as effective as the traditional IV route for RRMS patients. Additionally, SC administration may offer advantages in terms of reduced healthcare resource utilization and increased patient preference, potentially leading to improved adherence and quality of life.
Strengths and Limitations
A major strength of this study is its observational, prospective design, which allowed for the collection of real-world data from patients and HCPs with direct experience of both SC and IV administration. In Sweden, RRMS is diagnosed according to uniform national guidelines. Therefore, the participating sites are not expected to differ from other clinics in the country. The inclusion of perspectives from both patients and HCPs provides a comprehensive understanding of the practical and personal implications of transitioning to SC administration, from both a clinical and a patient perspective. Furthermore, the focus of the study on primary care settings is particularly relevant, as healthcare systems increasingly shift toward decentralized models of care. However, this study has some limitations. The sample size, while sufficient to identify key trends, may not capture the full diversity of experiences among RRMS patients and HCPs, and is not sufficient for statistical analysis. Additionally, the study was conducted in one country only, whereas healthcare practices and patient preferences may differ from country to country. A limitation of this study is that no validated questionnaires were available for the constructs of interest; despite a thorough literature review, no suitable instruments were identified.
As SC administration becomes more widely adopted following the 2024 label update for Tysabri (Natalizumab, NTZ, Biogen (2)), further studies across diverse healthcare systems will be important to validate these findings. Lastly, the use of self-reported surveys introduces the potential for recall bias, though efforts were made to minimize this by collecting data prospectively. In addition, as this was an observational study, no clear hypothesis was defined, and no inferential statistics such as p-values were calculated.
Implications for Practice
The results of this study suggest that SC administration of NTZ may reduce burden for both patients and healthcare systems. The shorter treatment times and ability to administer SC NTZ in primary care settings could alleviate hospital workloads, making specialized care more accessible for other patients requiring in-hospital treatments. Additionally, primary care-based SC administration may improve convenience for patients living in rural or underserved areas, thereby increasing adherence to treatment. HCPs also reported that SC administration streamlined workflows and allowed for more efficient use of healthcare resources, supporting the feasibility of broader adoption of SC NTZ administration in clinical practice. Although our findings support the benefits of SC administration, potential barriers to adoption should be acknowledged, including patient and physician safety perceptions as well as healthcare system constraints.
Conclusion
This study highlights the advantages of SC administration of natalizumab over IV administration, as perceived by both patients and HCPs. SC administration was associated with substantial time savings for both patients and healthcare systems, along with high levels of general satisfaction reported by both groups. The switch from IV to SC was perceived as easy by both HCPs and patients, with majority of patients expressing a preference for SC over IV administration. Among patients offered the possibility of receiving SC administration in a primary care setting, most were positive about this alternative, and a majority preferred it over hospital-based administration. These findings support the broader adoption of SC administration in clinical practice, especially in decentralized care models. Future research should focus on larger multi centre studies, long-term outcomes, patient adherence, and the impact on healthcare resource utilization, and cost-effectiveness studies.
Acknowledgments
Medical writing support was provided by Hanna Vikman, MSc and Anders Berglund, PhD, of Epistat, and was funded by Biogen. This support was provided in accordance with Good Publication Practice guidelines.
Disclosure
Anna Almroth and Karin Söderbärg were employed at Biogen Sweden when the study was conducted. Irina Sjöblom report no conflicts of interest in this work.
References
1. Lublin FD, Reingold SC, Cohen JA, et al. Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology. 2014;83(3):278–286. doi:10.1212/WNL.0000000000000560
2. Ltd BI. Tysabri 300 mg concentrate for solution for infusion: summary of product characteristics: European Medicines Agency; 2023. Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/tysabri.
3. Plavina T, Fox EJ, Lucas N, Muralidharan KK, Mikol D. A randomized trial evaluating various administration routes of natalizumab in multiple sclerosis. J Clin Pharmacol. 2016;56(10):1254–1262. doi:10.1002/jcph.707
4. Mealli F, Mattei A, Mariottini A, Massacesi L. Non-inferiority analysis of subcutaneous versus intravenous 300 mg monthly natalizumab administration: a post hoc analysis of the REFINE study. Mult Scler. 2024;30(8):1077–1080. doi:10.1177/13524585241238136
5. Trojano M, Ramio-Torrenta L, Grimaldi LM, et al. A randomized study of natalizumab dosing regimens for relapsing-remitting multiple sclerosis. Mult Scler. 2021;27(14):2240–2253. doi:10.1177/13524585211003020
6. Mariottini A, Mealli F, Mattei A, Massacesi L. Comparative efficacy of subcutaneous versus intravenous natalizumab on annualized relapse rate: a post-hoc analysis of the REFINE study. Mult Scler Relat Disord. 2024;91:105852. doi:10.1016/j.msard.2024.105852
7. Alonso Torres AM, Arevalo Bernabe AG, Becerril Rios N, et al. Cost-analysis of subcutaneous vs intravenous administration of natalizumab based on patient care pathway in multiple sclerosis in Spain. Pharmacoecon Open. 2023;7(3):431–441. doi:10.1007/s41669-023-00394-2
8. Wiendl H, Foley J, Defer G, et al. Patient preference for subcutaneous versus intravenous administration with every-6-week Natalizumab (Tysabri((R))) dosing: NOVA phase IIIb extension study (Part 2). Neurol Ther. 2024;13(5):1385–1401. doi:10.1007/s40120-024-00647-0
9. Napolitano D, Settanni CR, Parisio L, et al. Transition from intravenous to subcutaneous biological therapies in inflammatory bowel disease: an online survey of patients. Indian J Gastroenterol. 2024;43(1):215–225. doi:10.1007/s12664-023-01500-2
10. Harvey MJ, Zhong Y, Morris E, Beverage JN, Epstein RS, Chawla AJ. Assessing the transition from intravenous to subcutaneous delivery of rituximab: benefits for payers, health care professionals, and patients with lymphoma. PLoS One. 2022;17(1):e0261336. doi:10.1371/journal.pone.0261336
11. Filippi M, Grimaldi L, Conte A, et al. Intravenous or subcutaneous natalizumab in patients with relapsing-remitting multiple sclerosis: investigation on efficiency and savings-the EASIER study. J Neurol. 2024;271(1):340–354. doi:10.1007/s00415-023-11955-0
12. Gold R, Schmidt S, Deisenhammer F, et al. Real-world evidence and patient preference for subcutaneous versus intravenous natalizumab in the treatment of relapsing-remitting multiple sclerosis - initial results from the observational SISTER study. Ther Adv Neurol Disord. 2024;17:17562864241241382. doi:10.1177/17562864241241382
13. Haskard-Zolnierek KB, Miller TA, DiMatteo MR. Promoting treatment adherence. In: Oxford Textbook of Communication in Oncology and Palliative Care.
14. Martin LR, DiMatteo MR. From communication to healthy behavior and adherence. In: The Oxford Handbook of Health Communication, Behavior Change, and Treatment Adherence.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.