Back to Journals » Patient Preference and Adherence » Volume 19
Patient Experience and Improvement Opportunities in Self-Administered, Large-Volume Subcutaneous Infusions at Home
Authors Franzese C ![]() , Hawthorne J
, Hawthorne J ![]() , Katsaros D, Coyne M
, Katsaros D, Coyne M
Received 6 February 2025
Accepted for publication 22 May 2025
Published 13 August 2025 Volume 2025:19 Pages 2459—2491
DOI https://doi.org/10.2147/PPA.S515565
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Chris Franzese,1,2 James Hawthorne,1,3 Dimos Katsaros,1,4 Marty Coyne1,2
1Matchstick LLC, Boonton, NJ, USA; 2University of Rhode Island College of Pharmacy, Kingston, RI, USA; 3Sobi North America, Waltham, MA, USA; 4Kiniksa Pharmaceuticals, Lexington, MA, USA
Correspondence: Chris Franzese, Matchstick LLC, 141 Hawkins Place #122, Boonton, NJ, 07005, USA, Tel +1 516 993 3124, Email [email protected]
Purpose: Subcutaneous (SC) administration is largely established as the preferred route to deliver biotherapeutics. Although the majority of approved SC products are limited to dose volumes ≤ 2.25 mL, there has been increasing industry focus on large-volume SC (LVSC) development. To date, however, there are few LVSC biotherapeutics available for self-administration, and subcutaneous immunoglobulin (SCIg) remains the most established example. As a result, there is limited published literature on real-world practices with LVSC therapies to inform user needs and preferences for delivery device design attributes.
Patients and Methods: This was a remote ethnography study of patients self-administering SCIg at home for treatment of primary immunodeficiency diseases (PIDD). Participants passively video recorded their preparation and infusion processes, took photos, and provided open responses to illustrate their overall experiences with their disease, infusions, and delivery devices. Qualitative data were compiled, analyzed, and grouped into themes and subthemes that represented participant responses and sentiments.
Results: A total of 11 patients completed the remote study, all of whom were diagnosed with PIDD. Enrolled participants were currently infusing SCIg with one of five delivery devices and most also had previous experience with another delivery device. Emerging themes included universal preference for SC administration and pain points associated with managing medication/supply orders, storing medications/supplies, troubleshooting device issues, performing burdensome medication preparations, priming tubing/needles, inserting/securing needles, programming devices, adapting to device volume constraints, and loading reservoirs or tubing into delivery devices.
Conclusion: Although patients prefer LVSC administration at home compared to the alternatives, the current SCIg use process presents a variety of challenges. While not all of these factors will apply to every LVSC scenario, these insights, along with their corresponding implications for device design, provide a framework to inform user needs for LVSC self-administration, anticipate obstacles during development of new LVSC therapies, and improve existing delivery devices.
Keywords: large-volume subcutaneous drug delivery, self-administration, drug delivery devices, home infusion, primary immunodeficiency diseases, subcutaneous immunoglobulin
Introduction
Intravenous (IV) administration has historically been the standard of care to deliver many biotherapeutics, including monoclonal antibodies (mAbs).1 Despite efficacy and predictable bioavailability, IV delivery has practical limitations in that it requires invasive access, healthcare professional (HCP) services, potentially complex administration procedures, and typically travel to a healthcare facility, all of which can burden patients and the healthcare system.2–8 To address these constraints, subcutaneous (SC) administration has emerged as the preferred route to deliver biotherapeutics, as it offers numerous and well-established benefits compared to IV administration.9 For HCPs and the broader healthcare system, these include increased operational efficiency and decreased overall treatment costs.10,11 For patients, they include reduced treatment burden, decreased infusion-related adverse effects, increased convenience, and improved quality of life.12–14 Although not exclusively, many of these patient-centered benefits can be attributed to the ability to self-administer SC treatments outside of traditional healthcare settings, namely at home.
In order to help facilitate at-home administration, a variety of delivery systems, including prefilled syringe (PFS), autoinjector (AI), on-body injector (OBI), and portable infusion pump (PIP) devices have evolved alongside SC biotherapeutic development.15,16 This device innovation has resulted in the approval of over sixty biologic-device combination products,17 where the medication and delivery device are intrinsically linked, and 510(k) clearance of several general-purpose PIP devices for biotherapeutic delivery.18,19 Despite clear progress, SC delivery of larger dose volumes (ie, >3 mL) has presented well-known and intertwined formulation, clinical development, and device challenges, including protein stability concerns at high concentrations, formulation viscosity constraints, potential pharmacokinetic bridging complexities, and lack of timely device availability for pivotal trials.20–25 Amid these challenges, the vast majority of approved SC products are still limited to dose volumes ≤2.25 mL.17 However, the recent IV-to-SC transition of mAbs used to treat cancer has particularly accelerated focus on large-volume SC (LVSC) development, as these products often require comparably higher doses to achieve their therapeutic effects.25 While all approved SC oncology mAbs are currently supplied in conventional vials to be prepared and administered by HCPs in healthcare settings,26–30 at-home and self-administration is being actively explored,31–40 which may inevitably increase the demand for more patient-centric delivery devices.41
To date, however, there are very few LVSC therapies available for self-administration that have dose volumes similar to those of SC oncology mAbs, which are on the order of 5–15 mL for approved products.23 Four biotherapeutics have been approved for delivery via OBI42–45 with other devices in development,20 although one product was recently withdrawn from the market,46 another will seemingly be discontinued,47 and not all can achieve these dose volumes with a single device. The most established LVSC example is subcutaneous immunoglobulin (SCIg), a purified immune globulin derived from pooled human plasma that is the mainstay of treatment for primary immunodeficiency diseases (PIDD) and other diseases affecting the humoral immune system.48 A variety of SCIg products are available that vary in formulation concentration and composition, packaging configuration, recommended infusion volumes and rates, pharmacokinetic profiles, and typical dosing frequencies.49 Table 1 provides a brief overview of SCIg products available in the US market with their relevant administration-related characteristics, adapted from a recent and comprehensive review by Mathias et al50 and supplemented with additional information from product labeling.51–56 Regardless of the product selected, SCIg treatment decisions such as dose, dosing frequency, administration method and equipment, number of infusion sites, and infusion parameters are highly individualized to each patient based on a combination of pharmacokinetic monitoring (ie, immune globulin trough levels), clinical response (ie, frequency of infections), tolerability, and preference.48
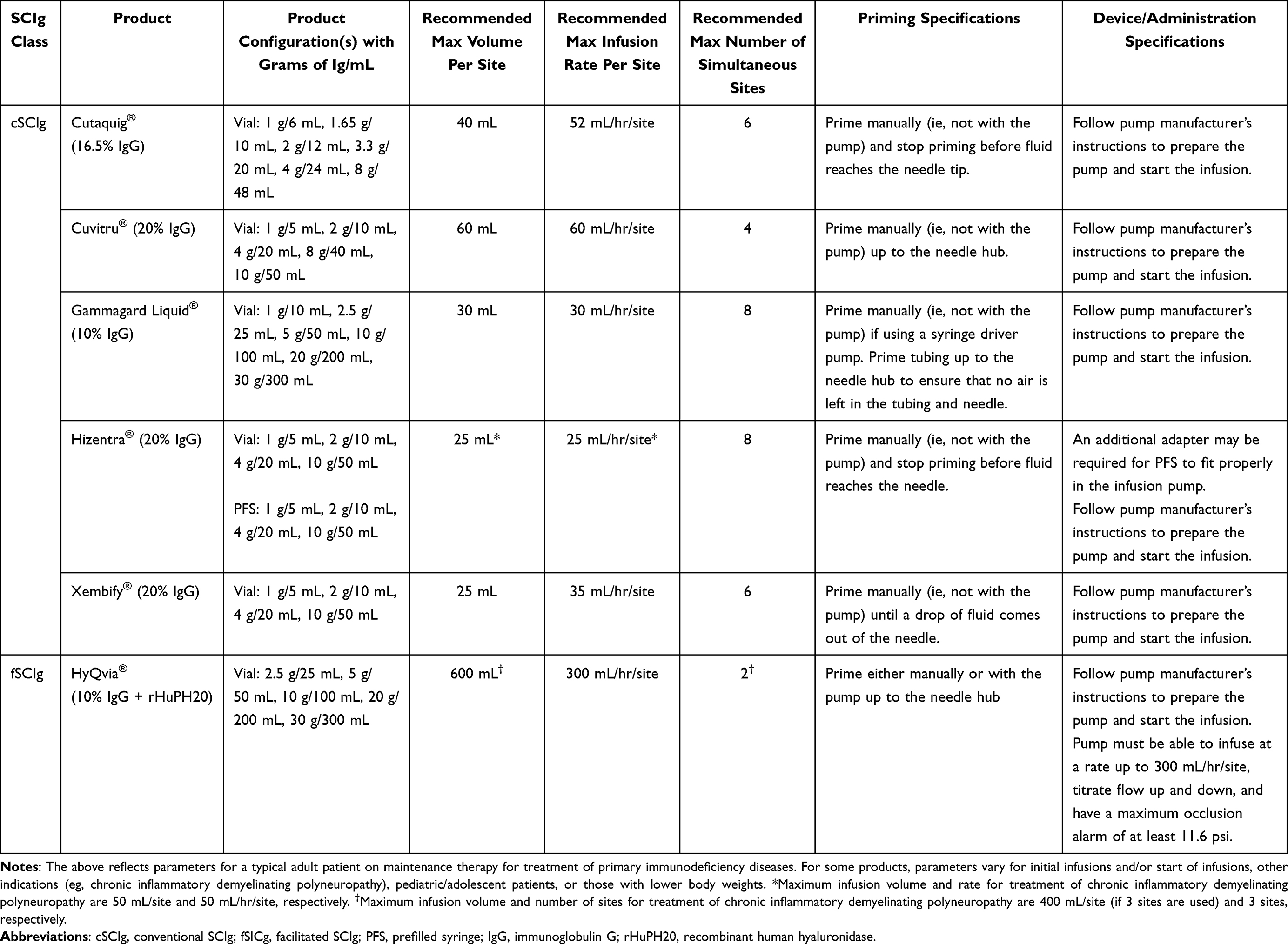 |
Table 1 Overview of SCIg Products Available in the US Market |
As no biologic-device combination products currently exist for SCIg, available treatments are administered using one of several general-purpose PIP devices.57 Each of these devices has a corresponding set of supplies and accessories that are intended to be used with their respective PIP.58–60 Table 2 summarizes key attributes of a subset of commonly used PIP systems, including device features and associated supplies according to product labeling.61–65 With one exception, SCIg products are supplied in vials and require patient manipulation steps prior to administration, which may include withdrawing dose volumes into conventional (eg, polypropylene) syringes, pooling multiple vials, and “nose-to-nose” transfer to appropriate syringes for loading into PIPs.66 Depending on the delivery method, additional administration-related steps may include inserting and securing needles, priming infusion sets, programming PIPs, initiating/manually administering infusions, and disposing of supplies.67 Ancillary supplies, such as syringes, needles, vial adaptors or transfer spikes, tubing sets, pooling bags, alcohol wipes, tape or bandages, gloves, and sharps containers are typically provided by the dispensing pharmacy or home infusion provider to facilitate patient preparation and administration.49 Still, current guidelines stress that providers must be able to offer adequate education, training, and support for patients to ensure they have the necessary tools and guidance to prepare and self-administer SCIg.48
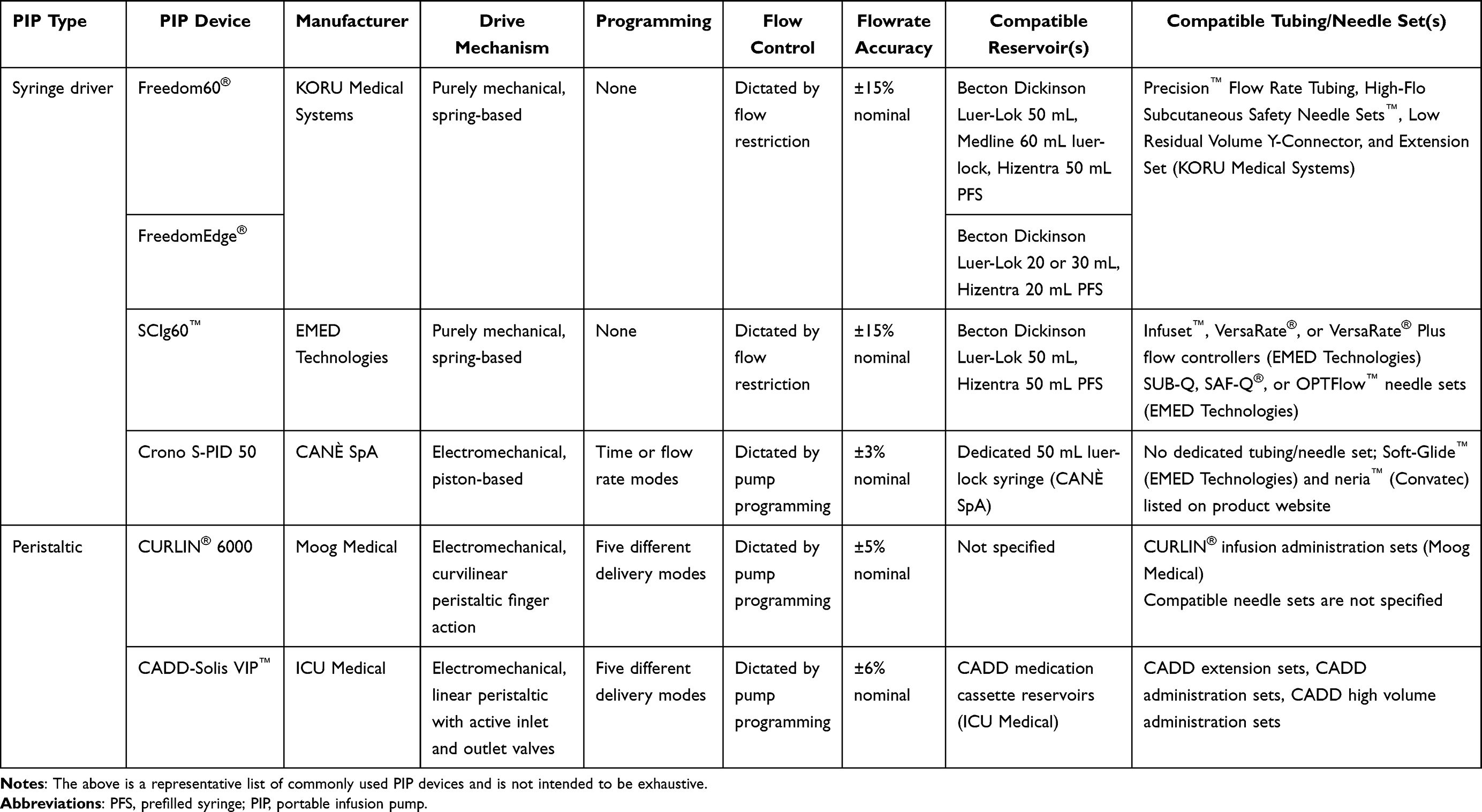 |
Table 2 Attributes and Supplies of Commonly Used PIP Devices |
Although SCIg is a cornerstone treatment, its use is still comparatively rare, given that the estimated prevalence of PIDD is between 1 in 1000 and 1 in 5000.68,69 As a result, while studies have evaluated some elements of the SCIg use process such as treatment preferences,70–72 packaging configurations,66 administration methods,73–77 training impacts,78 treatment burden,79,80 and overall lived experience with PIDD,81–83 to our knowledge, no study has specifically explored real-world practices with self-administered SCIg or other LVSC therapies through a delivery device lens. Clear gaps in this area have been reinforced by a recent systematic survey conducted by the Subcutaneous Drug Development & Delivery Consortium that centered on high-dose/high-volume SC technology development and patient preference for SC design attributes.84 Briefly, 20 subject matter experts currently working in/on developing SC-administered products were asked to rank the importance of 33 parameters in terms of their impact on patient experience around the SC drug development/delivery process and the need for additional data/knowledge surrounding each parameter. The authors found that despite being ranked as the most important factors by the subject matter experts for impact on patient experience, the parameters “complexity of user steps”, “form factor/human factors considerations”, and “number of use steps to administer dose” were identified among those with the largest data gaps.
To help address these and related knowledge gaps, we conducted a remote ethnography study specifically designed to characterize the full patient use process with SCIg, including treatment decisions, medication procurement, storage, preparation, and administration with various delivery devices. The primary goals of this study were to: (1) document real-world practices and challenges experienced by patients self-administering SCIg at home, with particular focus on the use of delivery devices; (2) identify opportunities to improve the current use process through qualitative thematic analysis; and (3) inform user needs for future devices designed to deliver SCIg and LVSC treatments more broadly as this landscape expands to other disease areas.
Materials and Methods
Study Design
This was a US-based, mixed-methods, semi-structured, non-interventional, remote ethnographic study of patients self-administering LVSC biotherapeutics with ≥5 mL dose volumes at home. The 5 mL minimum volume was selected based on the dose volumes of currently marketed LVSC mAbs used to treat cancer (typical range: 5–15 mL), as this represents the most active area of LVSC development.85 As SCIg was the only commercially available biotherapeutic that met these criteria at the time of study execution, all included patients were currently receiving one of several SCIg products. The LVSC oncology mAbs Rituxan Hycela® (rituximab and hyaluronidase human) (Genentech), Herceptin Hylecta® (trastuzumab and hyaluronidase-oysk) (Genentech), Darzalex Faspro® (daratumumab and hyaluronidase-fihj) (Janssen), Phesgo® (pertuzumab, trastuzumab, and hyaluronidase-zzxf) (Genentech), Tecentriq Hybreza® (atezolizumab and hyaluronidase-tqjs) (Genentech), and Opdivo Qvantig™ (nivolumab and hyaluronidase-nvhy) (Bristol-Myers Squibb), and the neonatal Fc receptor (FcRn) inhibitors Vyvgart Hytrulo® (efgartigimod alfa and hyaluronidase-qvfc) (argenx) and Rystiggo® (rozanolixizumab-noli) (UCB) were excluded prospectively, as these agents are not currently FDA-approved for self-administration, most are not administered with a delivery device, and some were not yet approved at all at the time of study enrollment. The complement protein C3 modulator Empaveli® (pegcetacoplan) (Apellis), which has been approved for self-administration of a 20 mL SC dose volume, was only recently commercialized at the time of study initiation, and patient users were unfortunately not yet available for recruitment. Other LVSC biotherapeutics available at the time of study enrollment with dose volumes smaller than the target 5 mL, such as the Repatha® (evolocumab) Pushtronex® System (Amgen), were considered out of scope.
Patients were enrolled from June 2021 to August 2021 and completed a series of activities at their own pace through a moderated, online, remote ethnography platform during the study period. Activities included closed- and open-form questions, projective exercises, and passive observation of participant-provided video and photo captures detailing current practices. All study data were collected and recorded in such a manner that the identities of the participants could not be readily ascertained. In all cases, moderators had the opportunity to follow up asynchronously to confirm observations and probe for additional details. All study procedures were conducted in accordance with the Declaration of Helsinki and its subsequent revisions.
Participant Eligibility
Eligible participants were ≥18 years of age and currently self-administering SCIg in the home setting using a drug delivery device at the time of the study. Recruiting was performed throughout the United States using commercially available, nationwide panels of patients with chronic disease. Patients were enrolled based on convenience sampling with no quotas placed on specific SCIg indications, SCIg products or manufacturers, SCIg doses, or delivery devices. Convenience sampling was employed for recruiting practicality due to the rarity of the target population and the specialized nature of SCIg treatment. Patients were not eligible to participate if they did not have a reliable internet connection, computer, and smartphone, or if they or an immediate family member worked for a pharmaceutical company or market research firm. As one of the study goals was to inform user needs for LVSC delivery devices, patients who self-administered SCIg by “rapid push” (manual injection with a syringe alone) were also excluded.
Prior to enrollment, all participants completed a written informed consent form outlining the observational nature of the study, the requirements for participation, the intent to publish de-identified study data in a scientific journal, and the steps taken to protect their privacy throughout. Participants who expressed discomfort with taking photos and/or videos for the purposes of the study or having their de-identified study data shared for scientific purposes were excluded. All participants were compensated financially for their time, and both participants and the study sponsor were blinded to each other’s identities.
Data Collection and Analysis
Participants were asked to passively video record themselves recounting prior experiences, including previous in-clinic infusion experiences and at-home infusion initiation, and performing and narrating their current practices, including ordering, storing, preparing, administering, and disposing of medications and/or supplies. To minimize disruption and best capture real-world practices, participants were free to record each of these activities at their discretion according to their own individual workflows on and around their infusion days – no specific number or length of participant-provided videos was enforced. Patient-provided video recordings were not assessed for correctness but rather to provide insight into their experiences and allow researchers to verify participant authenticity. Participants were also asked to take photos, enter open text responses, and record supplemental videos to further illustrate their overall experiences with their disease, infusions, and delivery devices.
Video and open-ended submissions were collected, transcribed, and coded by the study moderators (JH and DK). Initial coding was executed as participants completed each activity to develop an opening codebook, followed by an iterative process of reviewing and refining coding sequences to develop mutually exclusive themes by two additional researchers (CF and MC), similar to what has been described elsewhere.86 As qualitative data accumulated for each participant, researchers continuously monitored for code saturation (the point at which no additional themes were identified) and meaning saturation (the point at which themes were fully understood and no further dimensions or nuances of issues could be discerned). Thematic saturation was determined to be reached after analysis of data from 9 participants, with an additional 2 participants included to confirm no new themes emerged. Saturation was assessed considering the study aim, sample specificity, use of established theory, quality of dialogue, and analysis strategy as suggested by Malterud et al.87 Finally, qualitative data were compiled and grouped into themes and subthemes that described the patient experience using a similar framework to that employed by Ridgeway et al.88 Given both the small sample size and ethnographic nature of this study, formal quantitative and subgroup analyses were not performed.
Results
Participant Characteristics
A total of 11 patients completed the remote study, all of whom were diagnosed with PIDD. The specific PIDD subtype was not captured, as it was not deemed important to the study goals. Most patients were white women between the ages of 36–65 years old with at least one year of experience using their current delivery device for SCIg infusion. Patient experience with their current delivery devices ranged from less than one year to more than five years, with the majority (72.7%) having at least three years of experience. All patients also had previous experience with intravenous immunoglobulin (IVIg) prior to transitioning to SCIg. Participants were currently infusing with one of five delivery devices: Freedom60® (KORU Medical Systems), SCIg60™ (EMED Technologies), Crono S-PID 50 (CANÈ SpA), CURLIN® 6000 (Moog Medical), or CADD-Solis VIP™ (ICU Medical), with the Freedom60 used most commonly. Most participants (63.6%) also had experience using other delivery devices prior to their current device. Patient-provided photographs of their delivery devices are available as Supplementary Material (see Data Sharing Statement). SCIg products varied between participants, with 5 infusing Hizentra® (CSL Behring), 3 infusing HyQvia® (Takeda), 2 infusing Cuvitru® (Takeda), and 1 infusing Xembify® (Grifols). All but one of these SCIg products was supplied to participants in a vial configuration. Administration-related parameters, including dosing frequency, infusion volume, infusion duration, and number of needle sites per infusion, differed across participants, although there was an expected relationship between these factors for each patient (Supplementary Table 1). An aggregate summary of baseline participant characteristics is presented in Table 3.
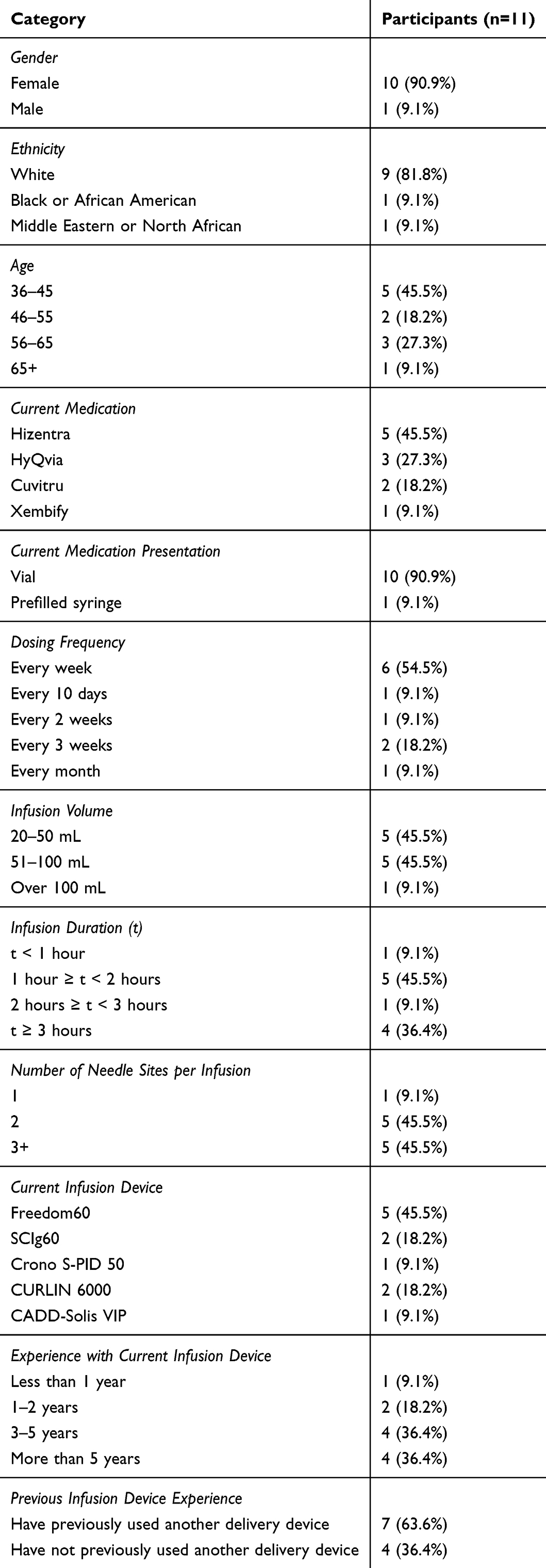 |
Table 3 Participant Characteristics |
Qualitative Themes
Patients unequivocally prefer SC infusions at home to in-clinic infusions
Study participants uniformly reported that receiving infusions in clinic, whether IV or SC, placed an immense time and emotional burden on them. Patients recalled that their IV infusions could require up to 12 hours of their day to be spent at the clinic (Table 4; Q1-Q3) and they needed to account for the time spent on transportation, which could range from less than an hour to multiple hours each way for those who live in rural areas (Table 4; Q2-Q4). Patients recalled that after an initial waiting period, they would need vitals taken and an IV site placed if they were receiving an IV infusion, and pharmacies may wait to begin medication preparation until these steps were complete, further delaying the process. The duration of infusion was reported to be up to 4 hours for an IV infusion (Table 4; Q3). Due to the effects of pre-medications and the infusion itself, some patients required another person to drive them home, complicating the routine (Table 4; Q4).
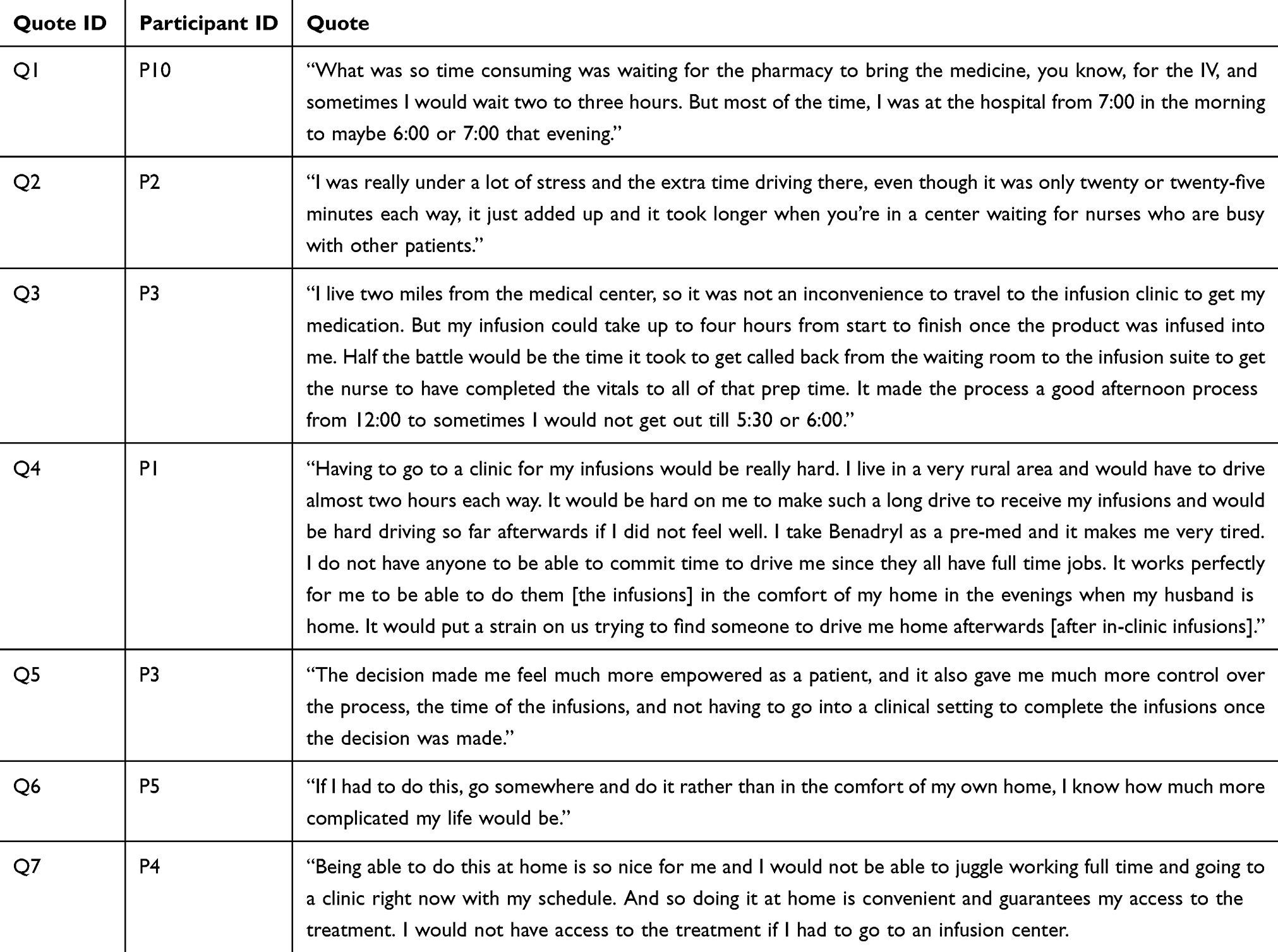 |
Table 4 Preference for SC at Home |
In contrast, SC administration in the home setting was reported to reduce burden and complexity for both patients and their caregivers (Table 4; Q4-Q7). Patients described a sense of empowerment due to their ability to control their own infusion schedule and infuse in the comfort of their own homes (Table 4; Q5). Some patients even reported they would not be able keep up with their lives and work schedules if self-administration was not an option and may otherwise have to forego treatment altogether (Table 4; Q7).
Patients are often responsible for ordering their infusion supplies and medications to be dispensed; this process is burdensome and dispensing errors are common
Patients revealed that they play an active role in the ordering process for both their medications and infusion supplies. In our sample, this involved contacting the specialty pharmacy and submitting written or verbal requests for medication refills and infusion supplies, which may take a considerable amount of time and lead to frustration (Table 5; Q1-Q5). Patients reported interacting with representatives who have little to no knowledge of these specialty products, adding to the frustration (Table 5; Q1-Q2). Some patients emphasized that follow-up calls and reminders are often needed to ensure their medication and supplies are shipped on time (Table 5; Q2-Q3). Several participants also noted that changing providers could exacerbate the dissatisfaction, frustration, and errors associated with the ordering and shipping processes, as it disrupts the procedures they have become accustomed to (Table 5; Q3-Q5).
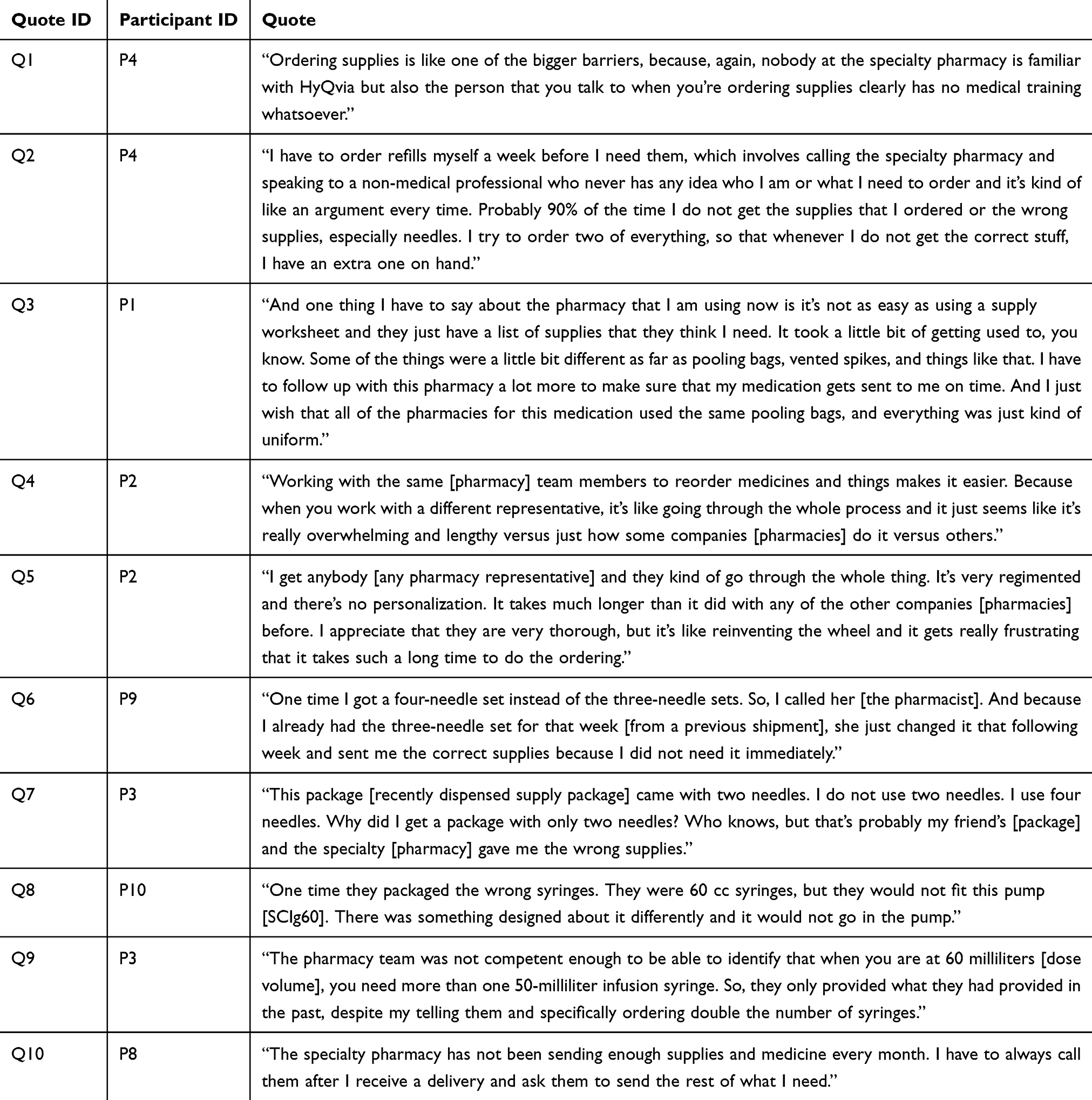 |
Table 5 Managing Medication/Supply Orders and Dispensing Errors |
Beyond the requirement to place refill and supply orders, patients were also burdened with verifying that the correct infusion supplies had been dispensed. Receiving the incorrect infusion supplies was a commonly reported occurrence (36.4% of patients) even in our small sample (Table 5; Q2, Q6-9), with one patient estimating that either incorrect supplies are sent or correct supplies are omitted “probably 90% of the time” (Table 5; Q2). When this occurs, patients noted that they often use surplus supplies stored from previous infusions if they are available (Table 5; Q2, Q6). In anticipation of this issue, some patients also reported that they intentionally request extra supplies to create a stockpile at home (Table 5; Q2). Other patients stated they need to routinely make additional shipment requests due to missing products (Table 5; Q10). Patient-provided photographs and/or video stills relevant to managing medication/supply orders and dispensing errors are available as Supplementary Material (see Data Sharing Statement).
Patients are required to properly store large amounts of medication and supplies at home, prompting a variety of management strategies
As shown and described by those in our sample, medication and supply shipments can take up significant space in patients’ homes. Participants reported that shipments are large, as they often contain coolers, ice packs, and other disposable packaging materials (Table 6; Q1-Q3). A single infusion for patients in our sample often required multiple syringes, needles, transfer devices, tubing sets, and additional medications other than the SCIg product (eg, pre-medications, such as acetaminophen and diphenhydramine), and some patients expressed an overall sense of overwhelm associated with the volume and complexity of required supplies (Table 6; Q4). Patients reported that they may receive the materials required for multiple infusions all at once (eg, a month supply) and must store them until their infusion days. For some patients in our sample, a month supply comprised four infusions (one infusion/week) and therefore contained significant amounts of supplies per shipment (Table 6; Q1-Q3). Several participants also reported that their pharmacies routinely send extra supplies to account for potential use errors or product failures, or to rectify dispensing mistakes as discussed in the previous section. Some patients reported that these extra supplies are useful if they are needed but also mentioned that they can accumulate over time, especially if they are never used (Table 6; Q5-Q6).
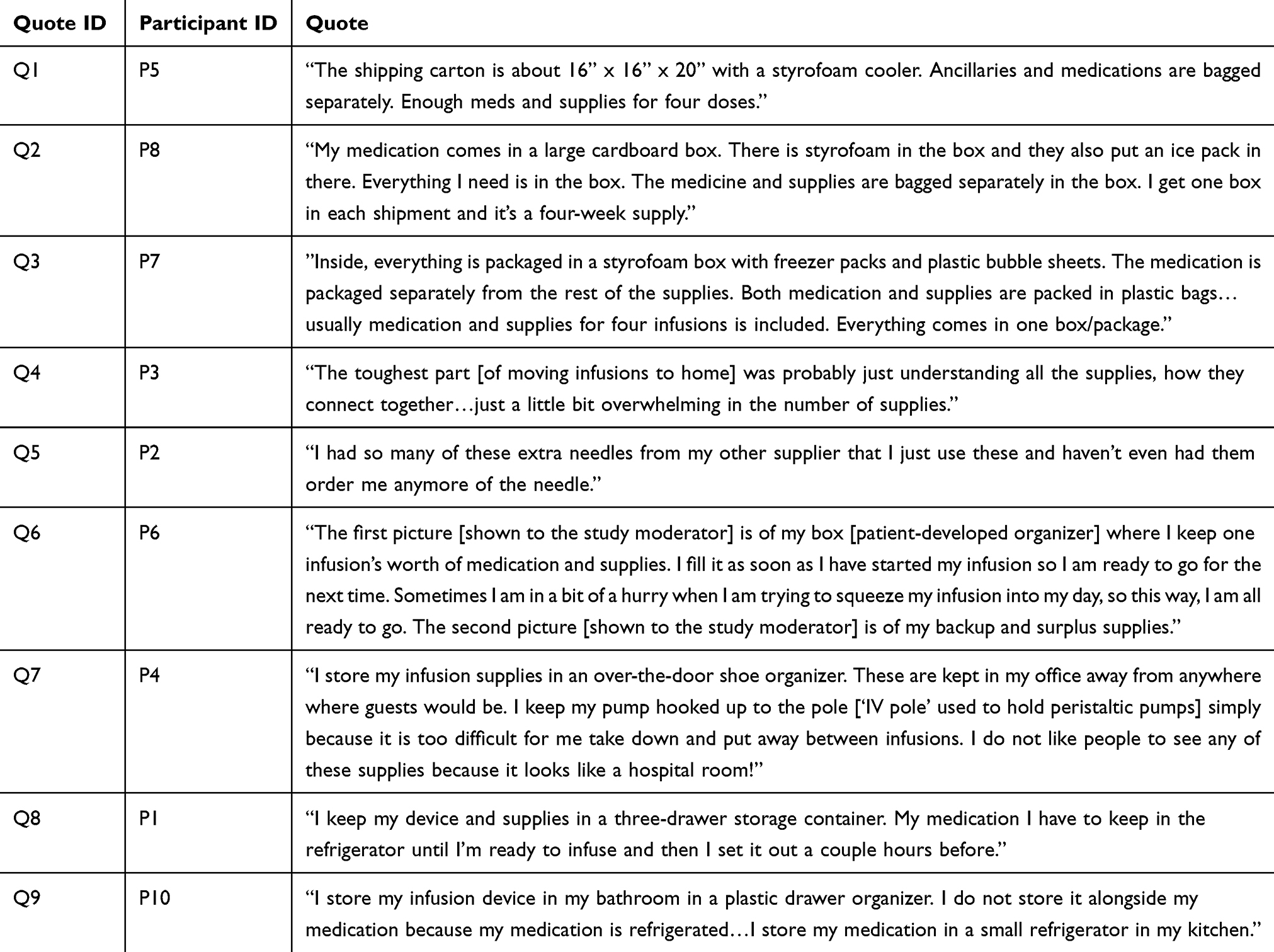 |
Table 6 Storing Medications and Supplies |
Patients in our sample often elected to develop their own creative, self-made systems to manage their medications and supplies, such as “kits” for each infusion, or repurposing storage bins, over-door shoe racks, or carts in an effort to keep materials together (Table 6; Q6-Q9). As components have different storage requirements (ie, medications need to be refrigerated whereas supplies do not), multiple locations may be necessary. Some patients utilized specific organizers or areas of their home in order to maintain privacy and prevent guests from seeing their supplies (Table 6; Q7). In addition to infusion supplies, patients often needed to store multiple medication vials safely and correctly, placing burden on limited refrigerator space and sometimes requiring designated storage locations (Table 6; Q8-Q9). Among patients in our sample, as many as 16 vials needed to be stored at one time. As most patients only had one refrigerator in their household, medications were typically stored alongside usual refrigerated items (eg, food) and accessible to family members or guests, compromising any desired discretion. This led some patients to purchase a separate refrigerator solely for medications as an alternative (Table 6; Q9). Patient-provided photographs and/or video stills relevant to storing medications and supplies are available as Supplementary Material (see Data Sharing Statement).
Although it is required for self-administration, patient training can be variable and insufficient
Participants in our sample described initiating self-administration at home as overwhelming and reported that adequate training helped ease their anxiety associated with the process (Table 7; Q1). However, we found that training experiences in our sample were highly inconsistent, with 5 of 11 participants (45.5%) reporting some degree of training inadequacy. While some patients reported positive training and support with multiple sessions and instructional material (Table 7; Q1-Q3), others reported training experiences that were suboptimal, with only a single training session in some cases (Table 7; Q4). Further, some patients expressed that the personnel responsible for training were sometimes ill-prepared to teach them how their delivery device operates, and instead, relied on online searches during the session (Table 7; Q5). Other patients reported they had no training at all on important aspects of their infusion process, such as emergency medication administration and device error troubleshooting (Table 7; Q6-Q8). If these situations occurred, patients expressed that they would often resort to publicly available resources such as Google, manufacturer websites or helplines, YouTube, or social media to teach themselves how to use their delivery devices (Table 7; Q8-Q10). Patient-provided photographs and/or video stills relevant to patient training are available as Supplementary Material (see Data Sharing Statement).
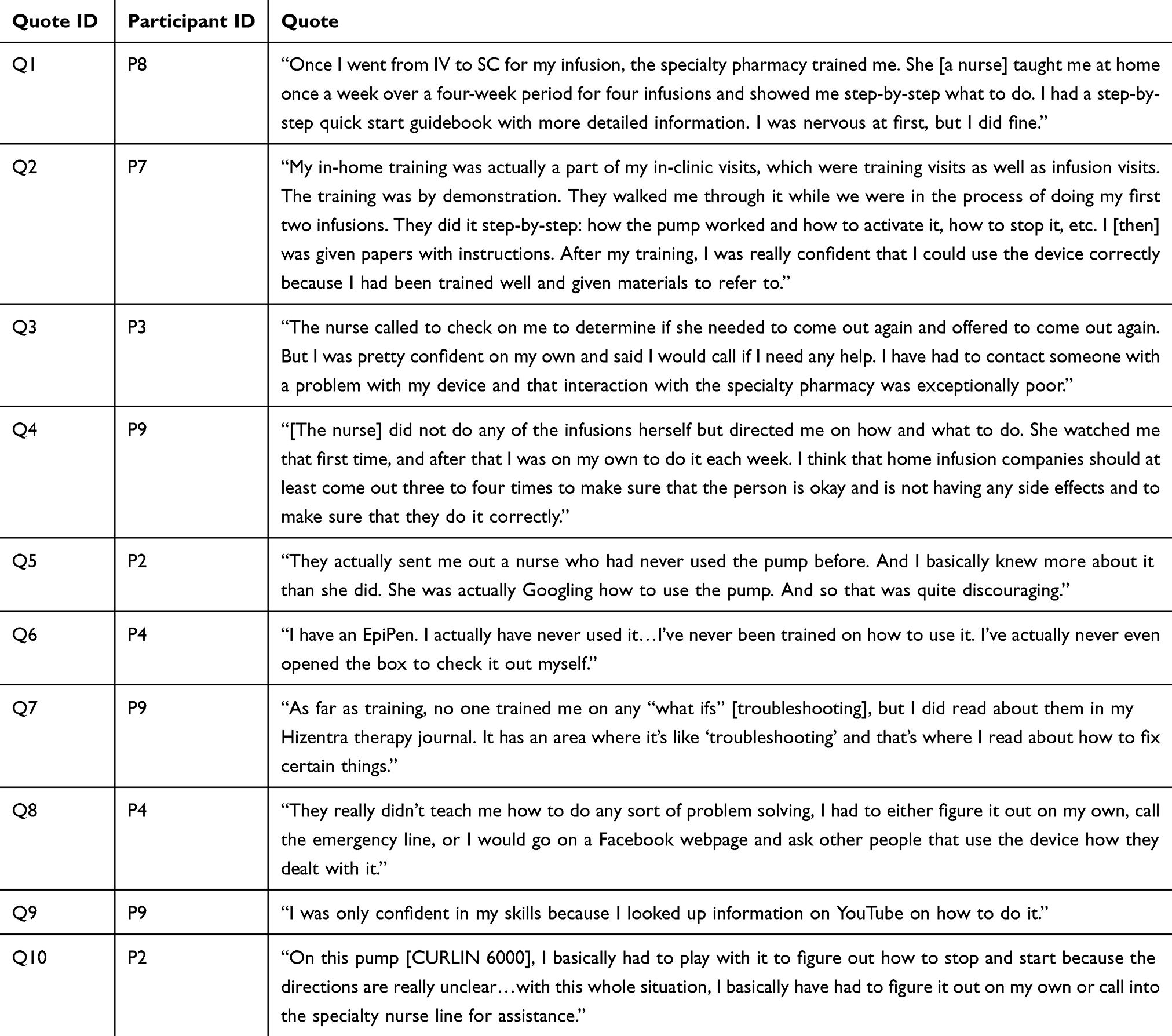 |
Table 7 Patient Training |
Medication preparation is complex, time-intensive, and physically demanding, increasing patient burden and error risk
The infusion preparations patients described and demonstrated in our study were complex, multi-step processes involving a variety of supplies, such as syringes, needles, vial spikes, tubing sets, and pooling bags. Tasks required for preparation included medication pooling from multiple vials into a single syringe, multiple syringes, or a bag depending on the required dose volume. Patients reported feeling overwhelmed with these tasks and nervous that they may make a mistake, which they considered a particular concern if they had any degree of cognitive impairment (Table 8; Q1-Q2). Some patients acknowledged that they frequently forget to perform recommended steps during preparation, such as wiping the tops of vials with alcohol swabs (Table 8; Q3). Despite this, all patients in our study still reported that they always prepare their infusions independently without assistance from in-home HCPs or caregivers.
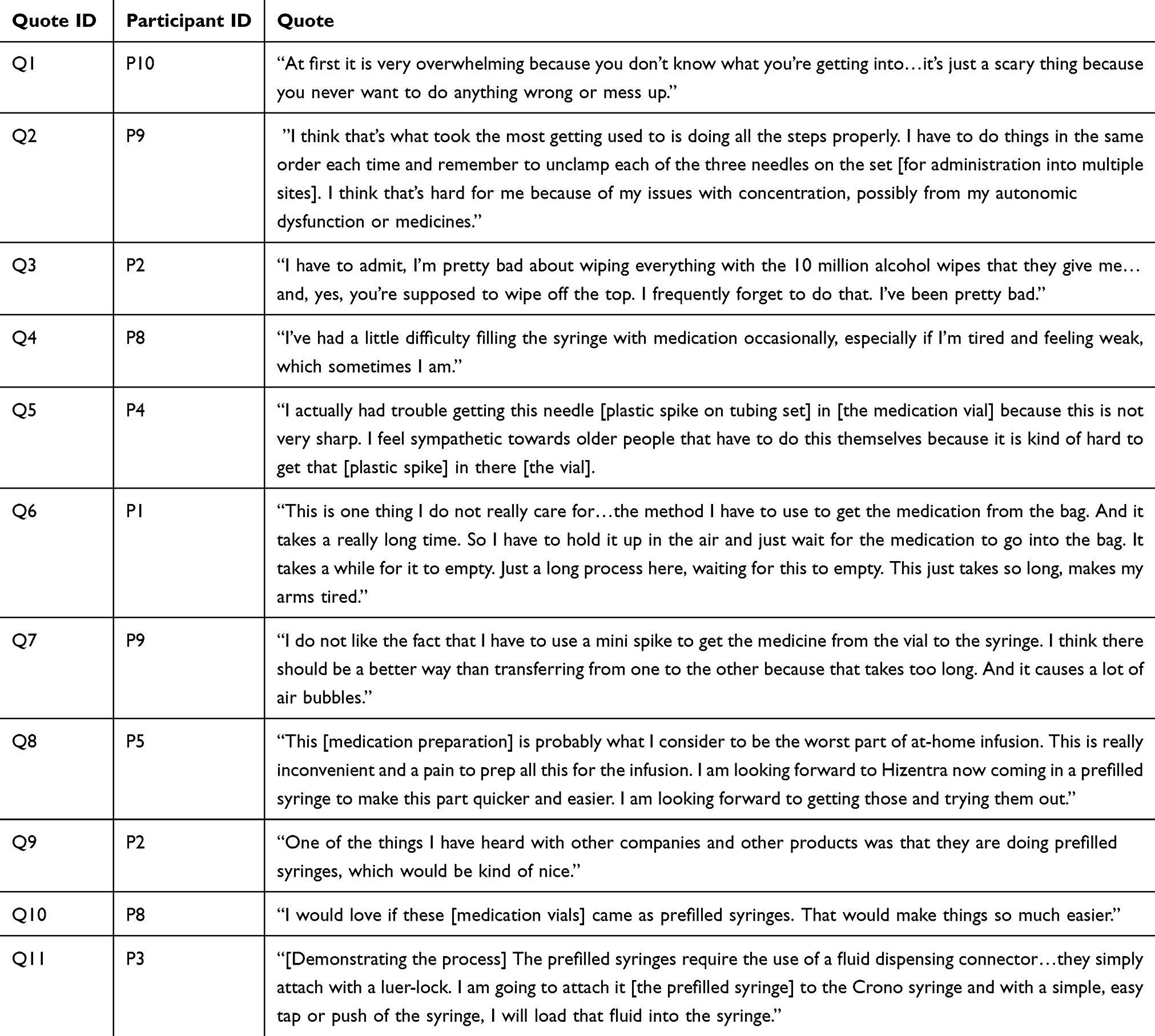 |
Table 8 Burdensome Preparation |
Syringe manipulations, including withdrawing and expelling volumes, were sometimes reported to be burdensome to perform and particularly difficult for those with motor impairments, such as hand weakness (Table 8; Q4). Some patients attributed preparation difficulty to how their drug products are presented (eg, in vials that need to be spiked), the supplies they must use (eg, tubing sets with plastic spikes), or the specific procedure required (eg, gravity transfer to bags) (Table 8; Q5-Q6). Even with the help of dedicated supplies like vial spikes, some patients reported that pooling multiple vials into a syringe is cumbersome, time-consuming, and potentially introduces unwanted air bubbles into the drug product (Table 8; Q7). Some patients stressed that these steps are the worst part of the home infusion process as a whole (Table 8; Q8) and suggested that new product presentations, such as PFSs, may improve the experience for them (Table 8; Q8-Q10). One participant who did use a PFS confirmed that the pooling process is indeed easier (Table 8; Q11). Patient-provided photographs and/or video stills relevant to burdensome preparation are available as Supplementary Material (see Data Sharing Statement).
Priming infusion sets with medication is manual, onerous, and inconsistently performed
Priming is the process of filling the tubing (and depending on the instructions, the needle – see Table 1) with medication before administration. For patients in our sample, this involved connecting the filled medication syringe(s) to the tubing set via luer-lock and pushing the solution through the tubing by manually depressing the syringe plunger. Depending on the specific product each patient used, the priming fluid was either SCIg itself (for Hizentra, Cuvitru, and Xembify) or hyaluronidase (for HyQvia). Priming was difficult for some patients, particularly those with motor impairments, who resorted to alternative, more gross motor techniques to depress the syringe plunger (Table 9; Q1-Q2). Beyond the mechanics of syringe depression, priming practices varied considerably between patients. Some opted to push the solution to the end of the tubing (ie, up to the needle) (Table 9; Q3-Q4) while others intentionally only primed the tubing partially, with a portion of patients stating that doing so helped to reduce pain upon needle insertion (Table 9; Q1, Q5-Q8). Other patients reported that they do not prime the tubing at all, expressing that it is not needed for SC infusions and therefore unnecessarily complicates the preparation process (Table 9; Q9). Patient-provided photographs and/or video stills relevant to priming tubing/needles are available as Supplementary Material (see Data Sharing Statement).
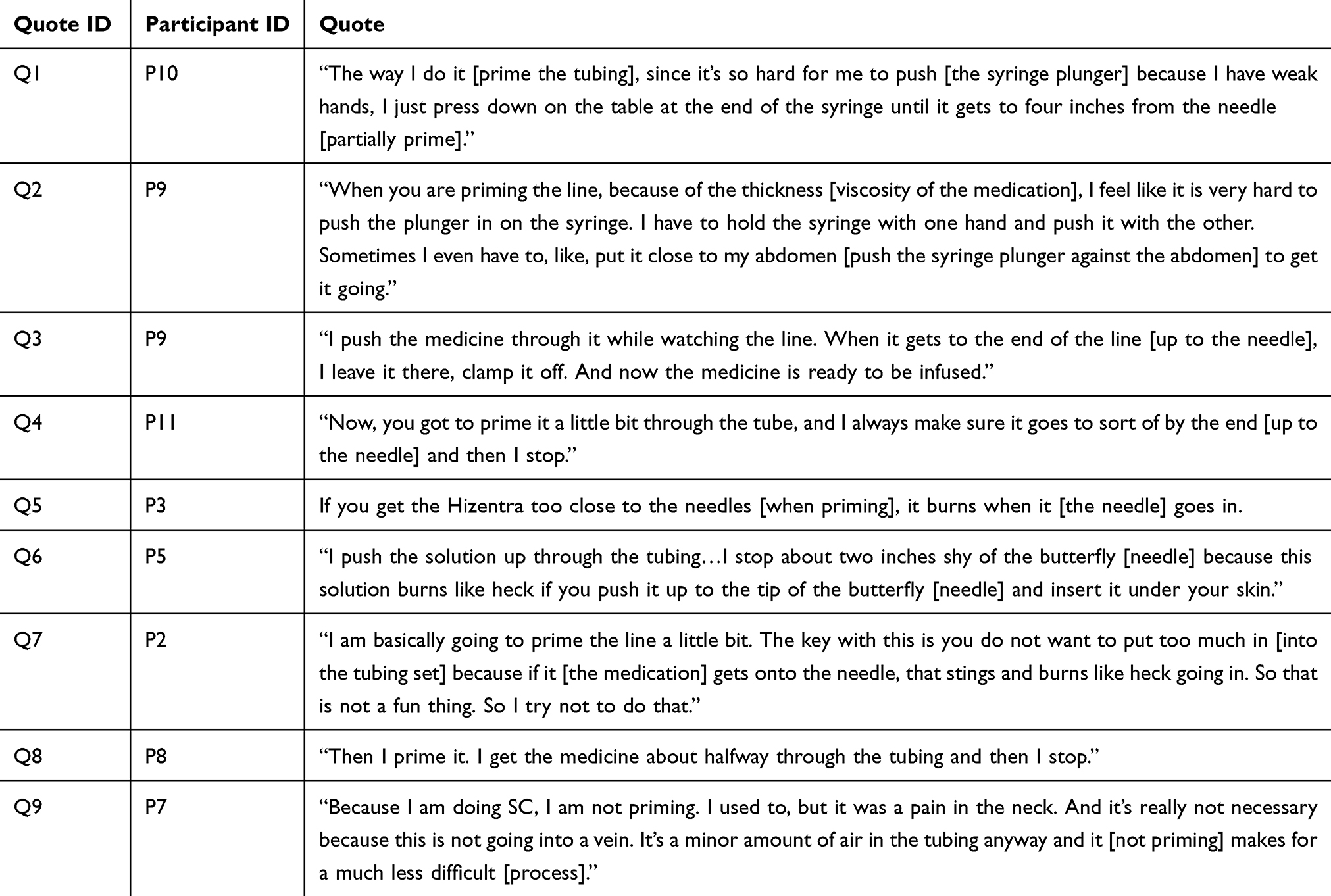 |
Table 9 Priming Tubing/Needles |
Needle insertion and adhesive removal are necessary but unpleasant steps for patients
Although they understood that needle insertion is required for drug delivery, patients reported significant emotional burden associated with needles, including nervousness and anxiety (Table 10; Q1-Q4). Most patients in our sample used more than one needle site per infusion, with some using as many as four, and several patients noted physical discomfort, pain, and sometimes burning upon each needle insertion (Table 9; Q5-Q7 and Table 10; Q3-Q4). Due to scar tissue development from repeated infusions, some patients needed to apply higher forces to insert their needles, leading to greater pain (Table 10; Q5). Patients in our sample employed several different strategies to minimize needle-induced pain. In addition to the partial priming technique discussed previously, some utilized lidocaine creams to reduce the pain and resulting anxiety associated with the needle insertion process (Table 10; Q4-Q5). Other strategies included ensuring proper hydration prior to the infusion (Table 10; Q6). One participant used an infusion set equipped with a soft cannula (ie, flexible plastic catheter) rather than a typical steel needle, citing reduced pain and increased comfort with this approach, particularly during movement (Table 10; Q7).
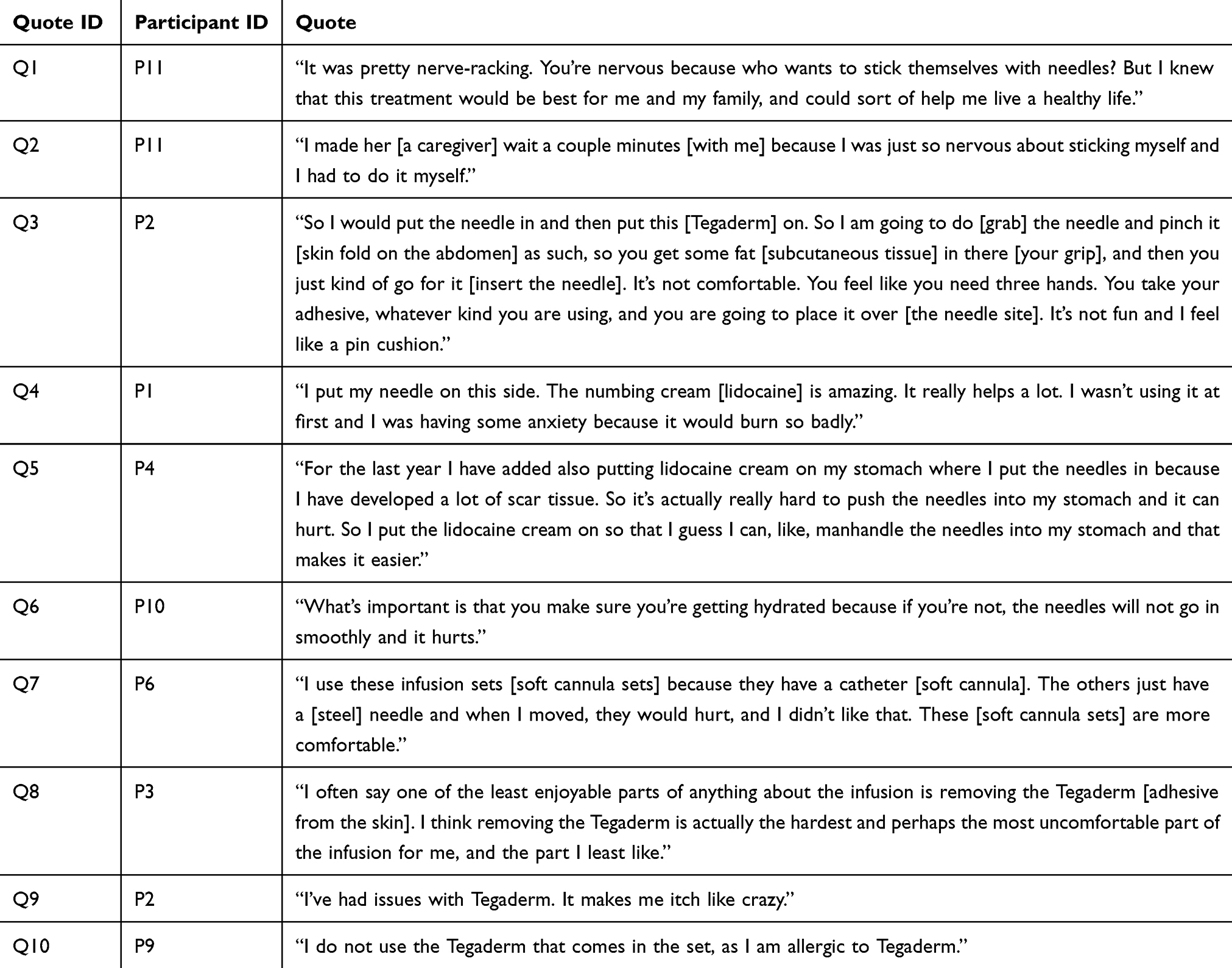 |
Table 10 Needle Insertion/Removal |
After needles were inserted, patients typically secured them in place using an adhesive dressing. Patients generally reported that the adhesive is often difficult to apply while holding the needle in their skin, with one expressing that “you feel like you need three hands” to complete this process (Table 10; Q3). Some patients felt that the removal and residual effects of the adhesive after infusion are some of the most uncomfortable and least enjoyable parts of the infusion process (Table 10; Q8). Adhesive removal was described as both painful and irritating, with multiple patients reporting itching or allergies to the most commonly used adhesive, Tegaderm® (3M) (Table 10; Q8-Q10). Patient-provided photographs and/or video stills relevant to needle insertion/removal are available as Supplementary Material (see Data Sharing Statement).
When required, delivery device programming is difficult, frustrating, and error-prone
Most patients (63.6%) in our sample used spring-based delivery devices (Freedom60 or SCIg60) that do not require programming. For the remaining participants (36.4%) who used programmable pumps (CURLIN 6000, Crono S-PID 50, or CADD-Solis VIP), all but one reported experiencing frustrations with the programming process. Some patients in our sample expressed that they were told or believed their specialty pharmacy or home infusion company would pre-program their pump for them prior to administration. However, several patients stressed that pre-programming was not performed, and they were therefore forced to manage programming themselves, which they considered challenging and not user-friendly (Table 11; Q1-Q2). One patient in particular expressed a specific desire for a pump that is ready-to-use upon startup, including the ability to automatically prime and then enter a “hold” state until the user chooses to begin the infusion (Table 11; Q2). Moreover, another patient reported that changes in dose/rate or power supply interruptions would require reprogramming of the device, which led to frustration, required technical knowledge to resolve, and resulted in failures (Table 11; Q3-Q4). Issues with programming even led this patient to refuse to recommend the device (Crono S-PID 50) to anyone who is not technically or mechanically competent, despite the device only having a limited number of buttons for programming (Table 11; Q4). Patients also reported that little support is available when programming difficulties arise, and instead, they must rely on previously supplied information or online sources that are insufficient to correctly guide them (Table 11; Q2-Q3). Patient-provided photographs and/or video stills relevant to device programming are available as Supplementary Material (see Data Sharing Statement).
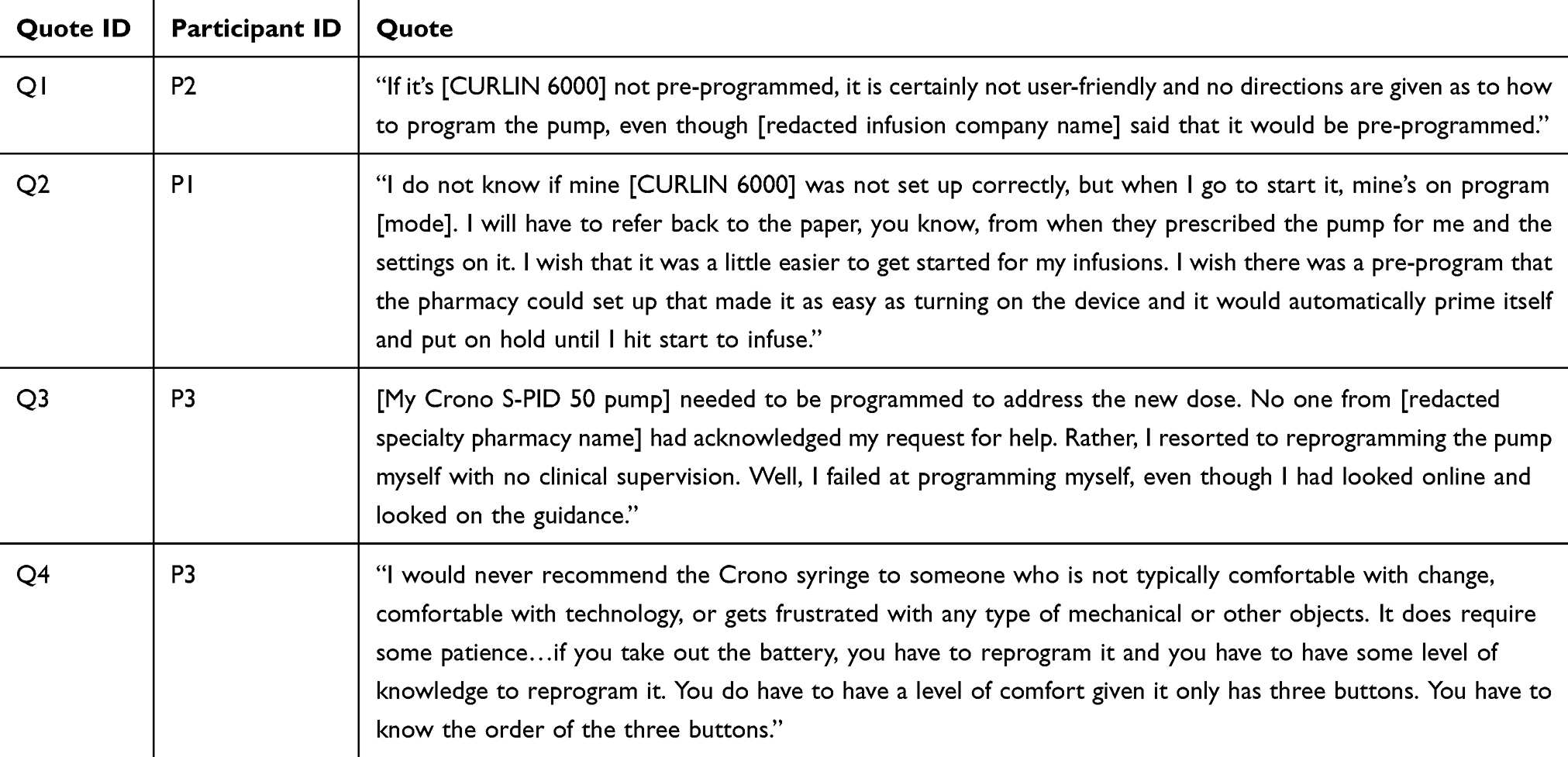 |
Table 11 Device Programming |
Reservoir and device volume constraints pose additional preparation and administration challenges
Most of the delivery devices used by patients in our sample (ie, Freedom60, SCIg60, and Crono S-PID 50) accommodate a maximum volume of 50–60 mL per administration, as they rely on conventional or modified polypropylene syringes as administration reservoirs. Notably, no participant utilized the compatible 60 mL Medline syringe for their Freedom60 device, effectively restricting its maximum volume capacity to 50 mL for the purposes of our study. As a result, patients with doses greater than 50 mL (54.5% of our sample) were forced to prepare, load, and administer multiple syringes to complete their prescribed doses (Table 12; Q1-Q3) or use a peristaltic pump after pooling their dose volumes into a larger reservoir (ie, a bag). For affected patients, syringe volume constraints increased the time, effort, and supplies needed for both infusion preparation and administration. To avoid this, some patients intentionally overfilled syringes past their maximum labeled volumes and visually estimated the additional volume in the absence of syringe graduations (Table 12; Q4-Q5). Patient-provided photographs and/or video stills relevant to volume constraints are available as Supplementary Material (see Data Sharing Statement).
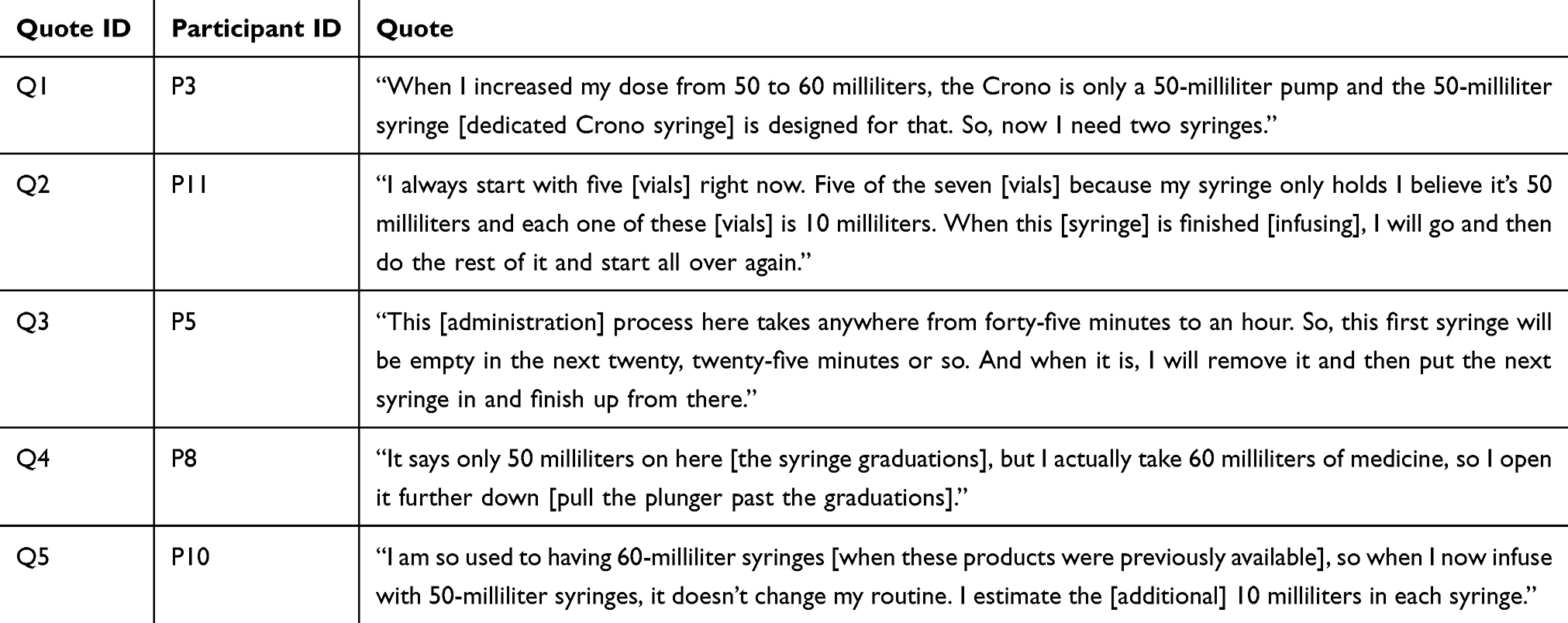 |
Table 12 Volume Constraints |
Delivery device loading is a manual, unintuitive, and technique-sensitive process
Patients described the process of loading or mounting administration reservoirs (ie, syringes or bags) into their delivery devices as highly manual and reliant on dexterity to avoid errors. For syringe-loaded devices (eg, Freedom60, SCIg60), this involved manipulating the syringe, tubing, and/or device components into their correct positions before administration. Patients reported incidents where the tubing or the syringe itself was not secured properly, leading to dislodgement, injury, or medication loss (Table 13; Q1-Q3). For some peristaltic pumps (eg, CURLIN 6000), the tubing set must be loaded precisely into the corresponding slots in the pump. Patients expressed difficulty with this process as well and imagined it would be particularly challenging for those with limited dexterity (Table 13; Q4). Patient-provided photographs and/or video stills relevant to device loading are available as Supplementary Material (see Data Sharing Statement).
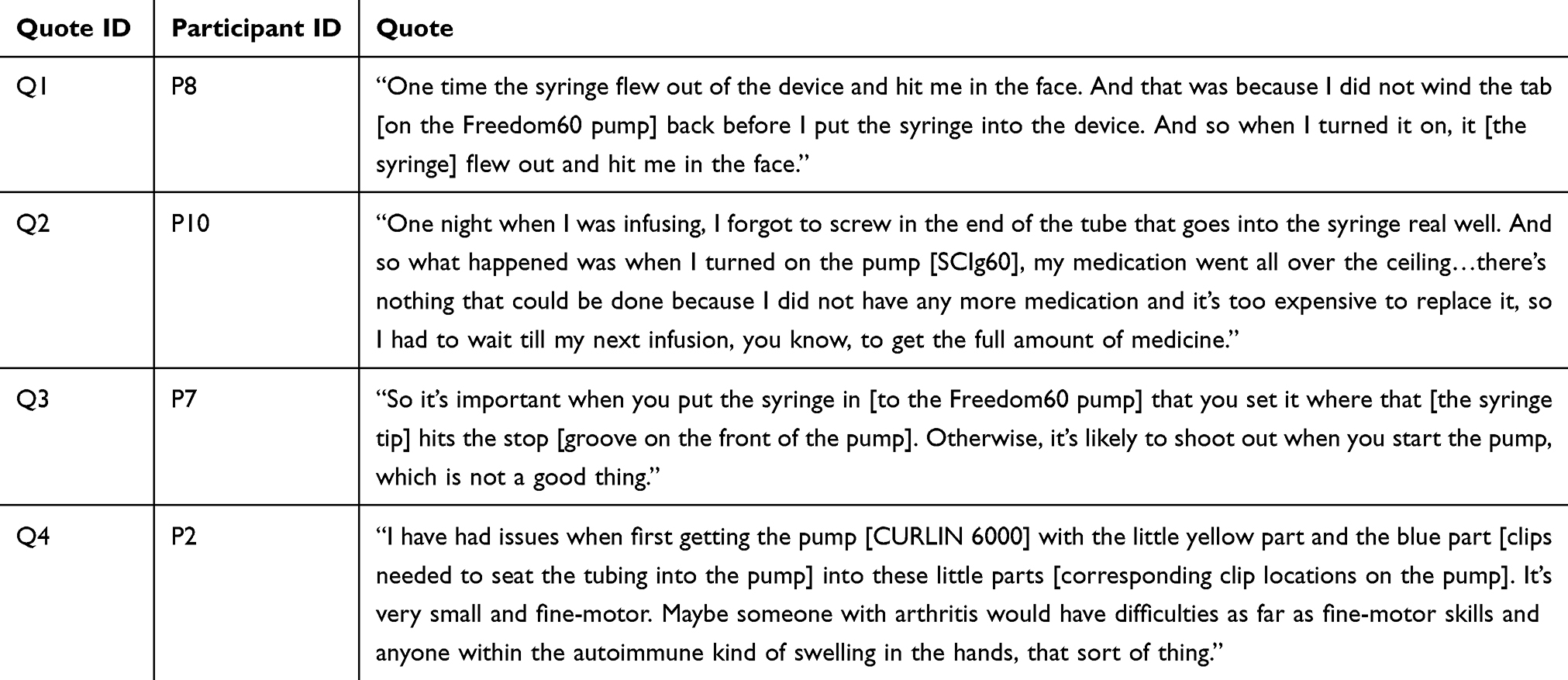 |
Table 13 Device Loading |
Discussion
A summary of observed qualitative themes and their implications for delivery device design is provided in Table 14. Implications are discussed in detail in the following sections in the order in which each theme was described above.
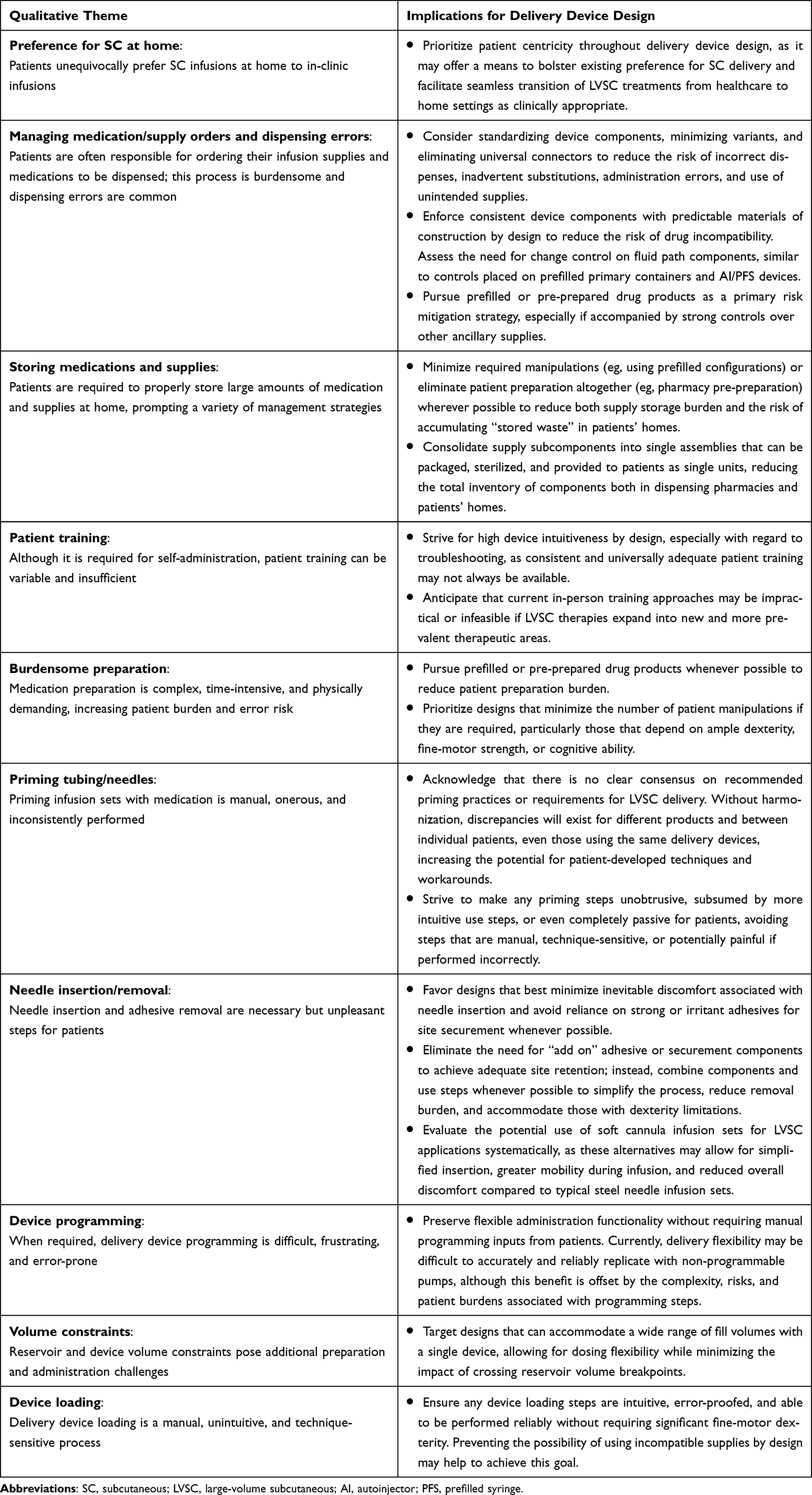 |
Table 14 Summary of Qualitative Themes and Implications for Delivery Device Design |
Preference for SC at Home
Patients in our study universally preferred their current SCIg treatments at home compared to their prior experiences receiving IVIg in clinic, consistent with prior research in PIDD and other therapeutic areas.12,70–72 Those in our sample attributed that preference to both practical benefits (eg, avoidance of travel) and emotional benefits (eg, control over treatment, setting, and timing), rationales that have also been reflected by a large, systematic review of patient preference for IV vs SC treatments.12 Similar preference for SC treatments has been observed in oncology therapeutic areas, both when IV and SC treatment options are administered in clinic9,89 and when home administration has been explored.33,36,37 Notably, however, most studies of at-home treatment with SC oncology biotherapeutics required administration from a trained HCP, and those that evaluated the feasibility of self-administration supplied patients with pre-prepared syringes and/or dedicated HCP education.90,91 As all SC oncology biotherapeutics are currently supplied in vials for administration with conventional syringes, it remains unclear how preference for self-administration would compare in the absence of patient-centered delivery devices.
Our study may serve as some indication that a portion of patients will struggle with purely manual administration (eg, by hand from a syringe), as several in our sample expressed difficulties even with the comparatively less manually demanding delivery devices they currently used for self-administration. While patients who self-administered SCIg by rapid push were excluded from our study by design, several authors have suggested that patients may have difficulty pushing syringe plungers with viscous Ig products.74,75,92 Similar difficulties with vial and syringe presentations have also been observed among HCPs, resulting in increased risk of preparation errors93 and musculoskeletal injuries.94 In both settings, PFS devices may offer preparation convenience and efficiency, but would likely suffer from the same manual administration disadvantages as disposable syringes filled from one or more vials. As more LVSC treatments are explored and become available for self-administration at home, the availability of patient-centric delivery devices may offer a means to bolster existing preference for SC delivery and facilitate seamless transition from healthcare to home settings as clinically appropriate.
Managing Medication/Supply Orders and Dispensing Errors
Operational issues with medication and supply ordering were consistently reported by several patients in our sample, sometimes leading to treatment complications. This was somewhat surprising, given how well established SCIg is in the treatment of PIDD and how few patients are treated with SCIg relative to more commonly used therapies that pharmacies routinely manage. One possible explanation is that operational issues are exacerbated by the patient-specific dosing and delivery device supply requirements of SCIg, which are typically not considerations for more conventional, small-volume SC products supplied in PFS or AI configurations.
Some concerns raised in our sample are fairly unique to the types of devices patients used, such as the propensity for device supplies to be sporadically replaced with different products over the course of therapy.95 In healthcare settings, changes to inexpensive commodity supplies are expected, whether due to shortages, stockouts, cost reduction efforts, or other factors. In such cases, universal components, such as luer-lock connectors, are highly desirable, as they allow HCPs to readily interchange supplies while preserving functional intent. However, as demonstrated in our study, while this practice allows for flexibility for suppliers and specialty pharmacies, it also increases the risk of dispensing errors, creates uncertainty for patients, and could result in delayed, incorrect, or missed doses. In contrast to HCPs who are accustomed to supply changes, patients may be confused and frustrated by them, even if they have no functional impact on drug delivery, as they have comparatively less experience and confidence to manage these discrepancies. Worse, changes to particular supplies (eg, luer-lock flow restrictors used with certain delivery devices)96–98 may be unrecognizable to patients but could indeed substantially impact drug delivery parameters. This risk should be contemplated in the context of future LVSC therapies, as some may require variable doses akin to SCIg and demand similar if not more careful coordination between the patient and pharmacy to ensure dispensing is performed correctly. Dose timing may be especially critical for biotherapeutics used to treat cancer, as treatments are typically delivered in regimented cycles that are often contingent on patient monitoring parameters or the administration of other medications.99–102
Further still, many venous access devices (VADs) also rely on universal luer-lock interfaces and, while likely rare among patients receiving SCIg, are commonly used to administer anti-cancer agents,103 including those that are frequently given alongside SC oncology biotherapeutics.99–102 As a result, wrong-route errors (eg, inadvertent administration of SC agents intravenously) facilitated by luer-lock interfaces could present new and potentially serious risks104 if existing supplies are used for at-home, self-administration of SC oncology agents. This may be particularly true for products available in both (but distinct) IV and SC formulations105 or in scenarios where patients are receiving both IV and SC medications as part of their treatment regimens.99–102 Future drug delivery devices should therefore consider standardizing device components, minimizing variants, and eliminating universal connectors to reduce the risk of incorrect dispenses, inadvertent substitutions, administration errors, and use of unintended supplies.
Finally, beyond its potential impact on drug delivery parameters, use of variable and uncontrolled supplies may also pose unforeseen drug compatibility issues. As an example, closed-system transfer devices (CSTDs), adaptors designed to prevent leakage or aerosolization of potentially hazardous drug products, can compromise physiochemical stability and dose accuracy when used to prepare or administer biotherapeutics.106–109 In some cases, these concerns have led industry working groups to actively recommend against the use of these adaptors to ensure the integrity and correct dosing of their drug products.110 While no patient in our study used a CSTD during preparation (SCIg is not a hazardous drug), comparable concerns may exist with similar supplies, especially given variability in their materials of construction, selection by pharmacies, and use by patients. This further underpins the need to enforce consistent device components with predictable materials of construction by design and potentially establish change control on fluid path components (ie, similar to prefilled primary containers and AI/PFS devices) to reduce the risk of drug incompatibility. Pursuing prefilled or pre-prepared drug products could serve as a primary risk mitigation strategy, especially if accompanied by strong controls over other ancillary supplies.
Storing Medications and Supplies
The need for ancillary supplies (eg, syringes, needles, spikes, tubing sets, bags) that are decoupled from the drug product and in some cases, the delivery device, created a host of challenges in our study. Beyond the risks associated with incorrect or incompatible supplies discussed in the previous section, receiving and storing supplies placed a significant, ongoing burden on patients in our sample. A prior evaluation of patient experience with SCIg reported similar findings, concluding that managing and storing supplies was a major contributor to burden of treatment.79
Patients in our study reported considerable bulk to manage, owing to their pharmacies’ propensity to repackage separately supplied components together for convenience, provide enough medication and supplies for every dosing interval, and accommodate different storage conditions in the same shipment. Moreover, to prospectively address inevitable errors or supply failures, pharmacies often sent (and patients often requested) frequent “backup” supplies. While this is seemingly practical, it resulted in substantial supply accumulation in patients’ homes. This degree of “stored waste” observed in our study was well in excess of quantities needed for each dosing interval or episodic component replacement. Such waste may have implications that extend beyond individual patient burden and may affect the long-term environmental sustainability of this use model, especially as the topic gains increasing attention in the industry.111 Unlike most disposables, these supplies are manufactured, sterilized, purchased, shipped, and stored, but are not always used by patients. Thus, it may be possible that the per-infusion sustainability impact not only includes the actual supplies consumed, but also a portion of the extra supplies dispensed that are never or seldom consumed. Quantifying the impact of stored waste was not conceived in this study but deserves dedicated focus in future research.
Regardless, minimizing required manipulations (eg, using prefilled configurations) or eliminating patient preparation altogether (eg, pharmacy pre-preparation) wherever possible would presumably help to reduce both supply storage burden and the risk of accumulating stored waste in patients’ homes. Consolidating supply subcomponents into single assemblies that can be packaged, sterilized, and provided to patients as single units may also help to reduce the total inventory of components both in dispensing pharmacies and patients’ homes.
Patient Training
Patient experience with onboarding, education, and training was highly variable in our sample, with some participants describing very positive interactions and others noting significant shortcomings. Negative experiences included insufficient training sessions, lack of trainer preparedness or competence, and absence of instruction on navigating rare occurrences or troubleshooting altogether, forcing patients to seek out their own sources to resolve issues. Patient education and training are considered requirements per clinical guidelines for SCIg therapy,48 provisioned for in the Medicare durable medical equipment (DME) and home infusion therapy services benefits,112,113 and specified in clinical programs in both the US and Europe.92,114,115 Ensuring accessible and high-quality training has also been associated with higher treatment satisfaction.78
While most quantitative surveys of patients self-administering SCIg suggest that patient training is adequately conducted, variability has still been observed in areas consistent with our findings, with some portion of patients reporting training difficulty, dissatisfaction, barriers, nonconfidence and/or lack of trainer competence.66,78,116 The need for better troubleshooting and error state resolution has also been reinforced by a qualitative study of treatment burden in patients receiving facilitated SCIg, where some patients expressed that they were left to figure out how to resolve pump alarms on their own.79 Moreover, similar variability in training practices has been observed in other therapeutics areas with simpler, small-volume SC delivery devices, including lack of education on nuanced error states and patient propensity to seek out their own resources, even if they are not accurate.117,118 These studies also draw attention to the variable and oftentimes limited training HCPs themselves receive on how drug delivery devices should be properly used. Nursing guidelines for SCIg administration express comparable sentiments, specifically noting that standard curricula for nursing education programs do not provide the level of detailed infusion therapy training necessary for administering and managing Ig therapies.119 Taken together, these sources suggest that existing gaps may be attributable to limited healthcare resources (eg, HCP time, HCP training on devices, dedicated staff), which may become further constrained or even unscalable if LVSC therapies expand into new and more prevalent therapeutic areas. To address this prospectively, future devices should strive for high device intuitiveness by design, especially with regard to troubleshooting, as consistent and universally adequate patient training may not always be available.
Burdensome Preparation
Patients in our sample expressed that preparing their medications for infusion at home presented a variety of challenges. Some issues were due to product presentation and required supplies (eg, pooling multiple vials using vial spikes, transferring contents into bags) and others were simply related to the process of performing manipulations at all (eg, remembering steps, filling syringes). Difficulties were particularly evident among those with cognitive or motor impairments. Syringe manipulation was specifically mentioned as a pain point in our study and has been similarly noted in prior literature on patient challenges with manual SCIg injections.74,75,92 Consistent with our findings overall, preparation complexity, anxiety associated with performing steps correctly, and need for adequate coordination, dexterity, and hand strength, have also been described elsewhere as contributors to burden of treatment for patients self-administering SCIg.79,95,120 In contrast, shorter preparation durations have been associated with higher treatment satisfaction scores,78 although the average preparation time among SCIg users is still estimated to be approximately 36 minutes.121
Some, but not all, of the preparation burden described in our study could be alleviated by the use of prefilled product configurations (eg, PFSs), and several patients in our sample specifically noted a desire to have their products supplied prefilled. The potential benefits of PFS configurations are already well-described122 and a recent survey of SCIg vial vs PFS users confirmed that PFSs were associated with significantly shorter infusion preparation times compared to vials.66 Notably, however, PFS users in this survey had lower global treatment satisfaction scores compared to vial users, which the authors attributed to the lack of availability of larger-volume, pump-compatible PFSs (20 mL and 50 mL) at the time of study and the associated patient requirement to perform multiple tip-to-tip transfers to conventional polypropylene syringes. Whether this concern is completely attenuated by the current availability of larger-volume PFS configurations remains unknown, although it is expected that many patients will still require multiple-syringe administrations, given that a reported 53% of adult SCIg patients receive more than 10 grams (ie, more than 50 mL of 20% solution) of Ig per infusion.121
Still, one element that remains a challenge for prefilled products is the ability to accommodate variable-dosed (ie, not fixed-dose) medications. For SCIg, this is accounted for by making several vial or syringe presentations available, as doses are typically rounded to the nearest vial or syringe size and ultimately managed by patients at the point of use.123,124 However, for prefilled biologic-device combination products that are designed to deliver fixed doses, this situation often necessitates separate device variants for each dose, as evidenced by several products currently supplied in AIs/PFSs.17 More complex still would be medications that require truly precise, weight-based or otherwise patient-specific doses that cannot be rounded as SCIg is. For example, while many oncology biotherapeutics can be administered in fixed doses23,125 this approach may not be appropriate for all molecules126 and dose-escalation studies (ie, evaluation of several, gradually increasing doses) are still commonplace during clinical development to determine exposure–response relationships.25 Such cases where dose variability is required may warrant exploration of other use models, such as pharmacy filling (ie, rather than manufacturer filling) for home use, which has been established for select products that require highly patient-specific dosing.127
Lastly, while not specifically evaluated here, patient-developed routines and rituals have been identified as coping strategies to ease the burden of self-administration in both SCIg users74,81 and elsewhere in small-volume self-injection.128 Purposeful future exploration of these practices among patients receiving LVSC therapies could potentially reveal new strategies to improve patient experience. Overall, our study and others suggest that future devices should pursue prefilled or pre-prepared drug products whenever possible to reduce patient preparation burden. If infeasible, manufacturers should prioritize designs that minimize the number of required patient manipulations, particularly those that depend on ample dexterity, fine-motor strength, or cognitive ability.
Priming Tubing/Needles
The tubing/needle priming process was also a significant pain point described in our study, with several patients citing technique-sensitivity and issues such as difficulty pushing syringe plungers and pain associated with priming medication to the end of the needle. In some cases, these concerns caused patients to deliberately prime the tubing only partially or abandon priming altogether to simplify the preparation and administration processes. These priming struggles are consistent with large-scale evaluations of patient-reported outcomes in those receiving SCIg, where a portion of patients noted priming as their greatest training concern.66,116 Nursing guidelines also emphasize that priming can be highly technique-sensitive and a key consideration for certain SCIg administration approaches.95 As mentioned previously, challenges associated with depressing syringe plungers, particularly with viscous medications, are commonly cited in the literature,74,75,119 and some authors even suggest that difficulty with manually pushing syringes could preclude patients from using certain needle types or delivery methods.92
Regarding priming volumes, a “dry priming” technique (intentionally stopping fluid approximately 1 to 1½ inches before the needle) is explicitly recommended in some SCIg nursing guidelines to avoid pain and site reactions.67,92,119 This practice is consistent with many of the patient demonstrations and accounts in our study and also reflected in some (but notably not all) SCIg product Instructions for Use (Table 1). However, patient-reported techniques such as leaving a greater volume of residual air in the tubing or entirely omitting priming deviate from both guideline and product-specific priming recommendations. These deviations are potential areas for future exploration, as it is unclear from our small sample if such priming variations are more widely practiced and whether they have any implications on medication efficacy or tolerability. Interestingly, one SCIg nursing guideline recommends that after the infusion, some patients can inject a small amount (5 cc) of air into the tubing to flush the line and create an air lock at the end of the needle,92 suggesting that small volumes of air injected SC are unlikely to pose major concerns. A similar “air sandwich” technique (pulling air into the needle, followed by drug, followed by air into the bottom of the syringe barrel) has also been recommended for the administration of SC oncology agents to prevent leakage after injection.27
Altogether, lack of consensus and inconsistencies in practice indicate that priming remains a clear area of improvement for current devices and warrants consideration for future devices that may require it. Notably, in the context of pump programming (described in a subsequent section), one study participant expressed a desire for a device that would “automatically prime itself” to make this step completely free from user interaction. This type of use model appears ideal, and if possible, device manufacturers should strive to make any priming steps unobtrusive, subsumed by more intuitive use steps, or even completely passive for patients, avoiding steps that are manual, technique-sensitive, or potentially painful if performed incorrectly.
Needle Insertion/Removal
Unsurprisingly, activities surrounding the use of needles were among the most frequently cited pain points in our sample. Needle phobia and associated anxieties with self-injection have been exhaustively characterized50 and similarly noted as significant concerns among patients self-administering SCIg.66,116 Needle-related patient concerns in our sample can be broadly categorized into two groups: those associated with needle insertion itself (eg, pain, burning, overall discomfort) and those associated with the adhesives used to ensure site integrity and proper medication delivery.
In terms of needle insertion, patients clearly expressed that this process is uncomfortable, nerve-racking, and cumbersome, and although they would like to avoid it, accepted that it is a requirement for their treatments. Desire to minimize needle insertions as much as possible is strongly supported by several large discrete choice studies, where the notion of fewer needle sticks was a major driver of treatment preference for patients receiving Ig,70–72 particularly among those with longer disease histories.72 Several patients in our sample mentioned that using numbing creams containing local anesthetics, a technique that has also been described in nursing guidelines for SCIg administration,92,119 can make the needle insertion process significantly more tolerable. Others noted that using an infusion set with a soft cannula rather than a typical steel needle created a more comfortable experience. Soft cannula products are widely used for insulin delivery129 and have also been successfully employed to deliver LVSC infusions in clinical trials,130 but are not commonly discussed in the context of SCIg.58
In addition to the increased perception of comfort observed in our study, soft cannula infusion sets may also address some of the ergonomic challenges (eg, the need for “three hands”) raised by patients in our sample, as these products typically have integral adhesives and assisted or guided insertion mechanisms.131 Further, novel soft cannula designs that can be left indwelling for extended durations and mitigate adverse events during wear are becoming increasingly available.132 Still, as most SCIg delivery devices currently have corresponding steel needle infusion sets, it is unclear how widely used soft cannula sets are in this patient population or how broadly compatible they are with existing devices. Future studies may therefore be warranted to more systematically evaluate the use of soft cannula sets for LVSC applications.
Interestingly, while patients in our sample certainly expressed discomfort during needle insertion as discussed, a roughly equal number complained about site securement, with some even insisting that using or removing adhesives is the most uncomfortable part of the infusion process. Issues with adhesive securement and skin irritation/sensitivity have also been reported elsewhere, including cases of needle displacement due to adhesive failure58 and recommendations to avoid product use in patients with potential adhesive allergies.133 Other literature has suggested that adhesives may pose additional complications for specific delivery devices during LVSC infusion, such as false pump occlusion alarms if the adhesive is pulled too taut95 or wearable device dislodgement if the adhesive fails to withstand administration-related tissue swelling.130 Notably, the latter scenario may require use of stronger adhesives, which patients in our sample were adamantly opposed to. Moreover, use of creams, lotions, or ointments, which was prevalent in our sample, may exacerbate such adhesive securement issues. Indeed, the Instructions for Use for one currently approved non-biotherapeutic OBI product specifically warns users not to apply lotions, oils, or ointments at the injection site,134 presumably to avoid interactions with the device adhesive. Ultimately, our study suggests that device manufacturers should favor designs that best minimize inevitable discomfort associated with needle insertion and avoid reliance on strong or irritant adhesives for site securement whenever possible.
Device Programming
Device programming practices were variable among patients who used programmable delivery devices in our sample. In most cases, patients expressed that their pumps were intended to be programmed by their pharmacies or home infusion providers but there were several instances where this was either missed or circumstances arose that required them to take on programming responsibility themselves (eg, a change in dose or interruption of power). Affected patients reported that in such events, their designated support channels (eg, pharmacy, home infusion provider, supplied educational materials, or online sources) were either unavailable or unable to provide adequate assistance, and they struggled and sometimes failed outright as a result. These patients insisted that performing programming is not a reasonable expectation and should be easier, condemning programming steps as not user-friendly and requiring technical competence to complete. Fewer programming steps also did not seem to change this sentiment, as some patients still felt burdened by devices with limited programming options (eg, Crono S-PID 50) compared to others (eg, CURLIN 6000, CADD-Solis VIP). Instead, patients explicitly stated that an ideal system would perform any programming and setup steps completely passively, including priming, as discussed above.
Surprisingly, practices and issues related to device programming among patients self-administering SCIg are sparsely discussed in the literature. One large-scale survey conducted by the Immune Deficiency Foundation reported that patients’ physicians are typically the ones responsible for determining the rate of SCIg infusion, but responsibility for pump programming itself was not mentioned.121 Another study noted that reprogramming conventional peristaltic pumps is mandatory for facilitated SCIg administration to avoid pump occlusion alarms, although it similarly did not specify who is responsible for this step.135 Along with easy programmability, the study authors recommended that other attributes of an ideal home infusion pump should include minimized size and noise, long battery life, and flexibility for dose/rate titrations.
Outside of SCIg, large observational studies and systematic reviews have demonstrated that pump programming errors still occur even among trained HCPs using smart infusion pumps (ie, those equipped with pre-programmed drug libraries),6,136–138 and would presumably be at least as common among patients using devices without such safety features. While it did not quantify programming error rates, one exploration of user-friendliness of home care technologies, including IV infusion pumps, did find that older patients in particular were not comfortable with the electronic components of the studied programmable pump and struggled with the physical and cognitive demands of using it.139 Impaired ability to read digital screens was specifically noted, and none of the home technologies in this study were ultimately considered truly user-friendly by patients. Lack of intuitiveness of programming displays and display malfunctions have also been considered by regulators, who recommend specific evaluation of how these failures could compromise safe operation of infusion pumps.140,141
Of course, alternatives to programmable pumps, such as the Freedom60 and SCIg60 devices, also exist and were frequently used by patients in our study. These systems employ different forms of rate-controlled tubing sets that provide fluidic resistance against constant-pressure drive mechanisms (ie, springs), therefore regulating flow. This is accomplished with either an adjustable dial on the tubing set or through selection of one of several (up to 20) tubing set flow restrictor variants, each of which is intended to achieve a target flowrate. In either case, the actual flowrate is a function of the selected fluidic restriction (ie, target flowrate) and other fluidic influences, such as temperature, barometric pressure, solution viscosity, and infusion equipment or conditions (eg, pump, syringe, tubing components, number of needles, vertical distance between pump and injection site, physical activity, etc).96,98 As a result, flowrate variability is expected, as it is specifically noted in approved product Instructions for Use61,96 and has been reported in practice.142,143 The limitations of constant-pressure drive mechanisms, including flowrate variability and overall lack of flowrate regulation, compared to more sophisticated systems has also been described in the context of other delivery devices, such as wearable infusors.77 While flowrate variability may have little pharmacokinetic impact for some but not necessarily all biotherapeutics,25,130,144,145 unexpected variation in infusion duration may still be disconcerting for patients142,143 and potentially affect how they schedule or behave during administrations. The exact impact that these and other factors have on actual or desired activities during infusion was outside the scope of this study, however, and warrants future exploration.
Finally, the need for multiple flow restrictor component variants may also contribute to the supply burden, environmental sustainability impact, and risks of incorrect supply usage discussed in the sections above. All things considered, our observations suggest that programmable pumps preserve valuable delivery flexibility that may be difficult to accurately and reliably replicate with non-programmable pumps. However, this benefit is offset by the complexity, risks, and patient burdens associated with programming steps. Future devices should therefore strive to achieve flexible administration functionality without requiring manual inputs from patients.
Volume Constraints
As described above and referenced in Table 2, available devices for SCIg administration are often broadly categorized into two groups – syringe driver pumps and peristaltic pumps – with pump choice dependent on a variety of factors, including Ig product, administration volume, insurance coverage, and patient preference.92,95,135 Technical distinctions (eg, drive mechanism, control method, programmability) between these pump types aside, the total volume capacity of the pump reservoir has an important impact on required preparation and administration steps. For example, most commonly used syringe drivers have maximum volume capacities of 50–60 mL,59,92 as a compatible syringe must be loaded into the pump in a specific orientation. To the extent they are available, larger syringes or other rigid containers simply cannot fit into these systems for proper administration and require other purpose-built syringe pumps with bespoke containers filled at point of use (eg, Crono S-PID 100). In contrast, many peristaltic pumps can accommodate reservoirs that are on the order of hundreds of mLs, limited only by which flexible container is selected from numerous available options (eg, 25 mL, 50 mL, 100 mL, 250 mL, 500 mL, 1000 mL, etc).
More than half of patients in our sample infused SCIg dose volumes greater than 50 mL, and therefore required multiple (ie, sequential) syringe reservoirs per administration if they did not use a peristaltic pump. To avoid additional preparation and administration steps, several of these patients resorted to overfilling their syringe reservoirs beyond their maximum measurable volumes, risking inaccurate dosing and potential leakage due to plunger dislodgement. While the goal of this study was not to quantify such risks, many patients are likely to face this use case, as more than half of patients receiving SCIg reportedly require dose volumes that will exceed a 50 mL syringe capacity even with highly concentrated products.121 Some patients in our sample opted for or were recommended to use peristaltic pumps as alternatives to sequential syringe administrations, pooling their larger dose volumes into single flexible bag reservoirs instead. However, potential tradeoffs between the consequences of volume constraints and risks associated with more complex devices cannot be adequately weighed using our small sample alone, and future, large-scale studies are needed to properly evaluate these factors as they relate to device preference.
Further, the variable-dose nature of SCIg may exacerbate inherent issues posed by reservoir volume constraints. Unlike most biologic-device combination products that are consistently dosed as fixed volumes for the duration of therapy, even a marginal increase in SCIg dose could cause a patient to cross the volume “threshold” imposed by syringe reservoir capacity. This occurred several times in our sample, where any dose volume change beyond 50 mL required the addition of another syringe per infusion. Notably, adding an additional syringe is the correct method to ensure accurate dosing, though some patients opted for the “overfilling method” described above specifically to avoid having to use additional syringes.
Limited reservoir capacities and/or variable dose volumes have presented issues for other delivery devices as well. In a study comparing an investigational wearable infusor vs the Crono S-PID 50 infusion pump for SCIg administration, the combination of variable doses and device volume capacities limited to 10 or 20 mL required the use of 2–5 (median 3) wearable infusors per weekly infusion.77 Despite patients preferring the wearable infusor to the Crono S-PID 50 pump in this study, the authors concluded that the need for multiple, single-use devices per dosing interval could pose substantial economic or sustainability challenges. In this case, device disposal necessarily implied discarding both the medication reservoir and power system (ie, mechanical components) for each wearable infusor, which was multiplied by the number of devices required at each volume breakpoint. The same would be true for other single-use, self-contained devices, such as those with motors, batteries, or other electronic components. These concerns may still be prohibitive even with fewer/smaller wearable devices, as one manufacturer recently discontinued plans to commercialize an electromechanical OBI product that required only two devices per dosing interval.47 In light of all of these factors, device manufacturers should ideally target designs that can accommodate a wide range of fill volumes with a single device, allowing for dosing flexibility while minimizing the impact of crossing reservoir volume breakpoints.
Device Loading
Finally, similar to other steps in the preparation and administration process, patients in our sample reported that loading reservoirs or other components into their devices was technique-sensitive and could result in failures if not performed correctly. This was true for both syringe driver and peristaltic pumps, although the Freedom60 pump was the most frequently implicated device. In particular, several patients cited instances where the syringe or the medication itself would be inadvertently ejected from the pump if the components were not properly fastened. This issue has also been reported in product complaints for this device.146,147 While some of these failure modes may be attributed to unclear user feedback or the force/dexterity required to perform syringe loading correctly as observed in our study, others may be related to the use of incompatible supplies with the Freedom60 device, which has already been discussed in detail in prior sections. Specifically, the flow restrictors (Precision™ Flow Rate Tubing) used to regulate infusion rate each contain an integral luer disc that mates with a groove on the pump nose to retain the restrictor (and thus the syringe) in place.96 If a different product is used or the tubing set is connected directly to the syringe without this component, its functions to control the flowrate, prevent unintended rapid delivery, and secure the syringe to the pump nose are compromised.
For peristaltic pumps, patient complaints in our study mostly centered on the fine-motor steps required to load tubing elements into the pumps. Although patients specifically attributed this issue to the CURLIN 6000 pump, similar issues with seating tubing or medication reservoirs have been observed for other peristaltic pumps, including CADD pumps. For example, difficulties or errors associated with latching CADD cassettes to their respective pumps, resulting in alarms signaling improper cassette attachment, have been reported in product complaints.148,149 Overall, patient complaints in our study and elsewhere suggest that any device loading steps should ideally be intuitive, error-proofed, and able to be performed reliably without requiring significant fine-motor dexterity. Preventing the possibility of using incompatible supplies by design may also help to achieve this goal.
Limitations
Our study has several limitations. First, the small sample size and qualitative, observational design of this study warrant larger, prospective studies to confirm our observations and explore how they may vary across different patient subgroups. Similarly, our sample was primarily composed of white women, reflective of convenience sampling of patients available on nationwide recruiting panels rather than the population epidemiology of SCIg users, which may limit the overall generalizability of our findings to broader patient demographics. While necessary to access sufficient study participants, convenience sampling may have also been a source of self-selection bias independent of demographics, with potentially more engaged or motivated patients being overrepresented. Our sample also largely consisted of those who have been self-administering SCIg for many years. While this allowed patients to draw from a wealth of experience, including how their process has evolved over time, it also required them to report on events that may have occurred long ago (eg, initial training), increasing the risk of recall bias.
SCIg was chosen as the primary focus of our study to inform other potential LVSC use cases and delivery devices, as it is the most established LVSC biotherapeutic available on the market. However, while SCIg represents many of the potential axes of variability in LVSC therapy characteristics in line with our study intent, there are some elements of the SCIg use process that may not always be generalizable to all LVSC therapies. Examples may include patient-specific dosing, instances of very large dose volumes (eg, hundreds of mLs), patient preparation requirements (eg, manipulating drug vials), and use of general-purpose PIP devices rather than purpose-built delivery devices. To encompass other potential LVSC use cases, such as those with relatively smaller volumes (eg, 2.25–5 mL) and/or different device types, our sample would have ideally also included patients using other products, such as the Empaveli (pegcetacoplan), Repatha (evolocumab), Skyrizi® (risankizumab-rzaa) (AbbVie), and Furoscix® (furosemide) (scPharmaceuticals) OBIs. Unfortunately, however, most of these products were either not yet approved or no patient users could be identified for recruiting at the time of study enrollment. Future studies should also consider these use cases to understand their similarities and differences, and broaden applicability to more LVSC treatments as they continue to become available.
Conclusion
Although LVSC administration at home is largely preferred to the alternatives, the current SCIg use process presents a variety of challenges for patients. In our study, the most salient pain points were those related to: managing medication/supply orders and dispensing errors; storing medications/supplies and associated waste; troubleshooting device issues due to insufficient training; performing burdensome medication preparation steps; priming tubing sets manually; inserting and securing steel needles; programming delivery devices; adapting to device volume constraints; and properly loading reservoirs or tubing into delivery devices. These challenges represent concrete barriers to optimal LVSC self-administration that emerged consistently across our sample, and reveal how seemingly small design decisions have the potential to substantially impact patient experiences with LVSC therapies. While not all of these factors will apply to every LVSC scenario, these insights, along with their corresponding implications for device design, provide a framework to inform user needs for LVSC self-administration, anticipate obstacles during development of new LVSC therapies, and improve existing delivery devices. As LVSC delivery continues to expand to more prevalent disease states and complex therapies, addressing the unmet needs observed in this study may become critical for successful at-home adoption and effective use.
Data Sharing Statement
The Supplementary Material for this study consists of one Supplementary Table (available with this publication) and a comprehensive collection of anonymized, participant-provided photographs and video stills referenced throughout the manuscript. Due to file size limitations, these high-resolution images have been deposited in an external scientific repository and can be accessed upon request. These images provide visual documentation of real-world practices with self-administered SCIg that support and contextualize the findings presented in this manuscript. Researchers interested in obtaining additional information about these materials may contact the corresponding author at [email protected].
Ethics Statement
All study procedures were conducted in accordance with the Declaration of Helsinki and its subsequent revisions. Written informed consent was obtained from all participants prior to enrollment for publication of anonymized images and video stills of their infusion equipment, supplies, and processes. This was a non-interventional, observational study as described in the United States 45 CFR 46.104(d)(2) and all required criteria were met for exempt research under this policy.
Acknowledgments
The authors would like to sincerely thank the study participants for sharing their infusion practices and personal experiences with the research team. All product names and brands are the property of their respective owners, and any mention of specific companies, products, or services used in this manuscript are for identification purposes only. Use of these names does not imply endorsement. James Hawthorne’s current affiliation is Sobi North America, Waltham, MA, USA; Dimos Katsaros’ current affiliation is Kiniksa Pharmaceuticals, Lexington, MA, USA.
Funding
Matchstick received consulting fees and research support from SHL Medical through an unrestricted grant. The sponsor had no influence on the study design, analysis, or reporting of results, nor did they exercise editorial oversight over this manuscript.
Disclosure
Dr Chris Franzese reports grants from SHL Medical during the conduct of this study; in addition, Dr Franzese has a patent US20230372610A1 pending to Assignee: SHL Medical, a patent US20230226272A1 pending to Assignee: SHL Medical, a patent US20230390483A1 pending to Assignee: SHL Medical, a patent WO2024217896A1 pending to Assignee: SHL Medical, and a patent WO2024042040A1 pending to Assignee: SHL Medical. Dr James Hawthorne reports grants from SHL Medical during the conduct of this study; in addition, Dr Hawthorne has a patent WO2024042040A1 pending to Assignee: SHL Medical. Dr Dimos Katsaros reports grants from SHL Medical during the conduct of this study. Mr Marty Coyne reports grants from SHL Medical during the conduct of this study; in addition, Mr Coyne has a patent US20230372610A1 pending to Assignee: SHL Medical, a patent US20230226272A1 pending to Assignee: SHL Medical, a patent US20230390483A1 pending to Assignee: SHL Medical, a patent WO2024217896A1 pending to Assignee: SHL Medical, and a patent WO2024042040A1 pending to Assignee: SHL Medical. The authors report no other conflicts of interest in this work.
References
1. Xu Z, Leu JH, Xu Y, et al. Development of therapeutic proteins for a new subcutaneous route of administration after the establishment of intravenous dosages: a systematic review. Clin Pharmacol Ther. 2023;113(5):1011–1029. doi:10.1002/cpt.2823
2. Aumann I, Kreis K, Damm K, Golpon H, Welte T, Graf von der Schulenburg JM. Treatment-related experiences and preferences of patients with lung cancer: a qualitative analysis. Health Expect. 2016;19(6):1226–1236. doi:10.1111/hex.12417
3. Cheng AC, Levy MA. Measures of treatment workload for patients with breast cancer. JCO Clin Cancer Inform. 2019;3:1–10. doi:10.1200/CCI.18.00122
4. Vescia S, Baumgärtner AK, Jacobs VR, et al. Management of venous port systems in oncology: a review of current evidence. Ann Oncol. 2008;19(1):9–15. doi:10.1093/annonc/mdm272
5. Schmier J, Ogden K, Nickman N, et al. Costs of providing infusion therapy for rheumatoid arthritis in a hospital-based infusion center setting. Clin Ther. 2017;39(8):1600–1617. doi:10.1016/j.clinthera.2017.06.007
6. Lyons I, Furniss D, Blandford A, et al. Errors and discrepancies in the administration of intravenous infusions: a mixed methods multihospital observational study. BMJ Qual Saf. 2018;27(11):892. doi:10.1136/bmjqs-2017-007476
7. Sugalski JM, Kubal T, Mulkerin DL, et al. National comprehensive cancer network infusion efficiency workgroup study: optimizing patient flow in infusion centers. J Oncol Pract. 2019;15(5):e458–e466. doi:10.1200/JOP.18.00563
8. Jusufi H, Boivin N. Navigating access and optimizing medication infusions in an academic medical center: a quality improvement study. Pharmacy. 2023;11(4):111. doi:10.3390/pharmacy11040111
9. Anderson KC, Landgren O, Arend RC, Chou J, Jacobs IA. Humanistic and economic impact of subcutaneous versus intravenous administration of oncology biologics. Future Oncol. 2019;15(28):3267–3281. doi:10.2217/fon-2019-0368
10. McCloskey C, Ortega MT, Nair S, Garcia MJ, Manevy F. A systematic review of time and resource use costs of subcutaneous versus intravenous administration of oncology biologics in a hospital setting. Pharmacoecon Open. 2023;7(1):3–36. doi:10.1007/s41669-022-00361-3
11. Epstein RS. Payer perspectives on intravenous versus subcutaneous administration of drugs. Clinicoecon Outcomes Res. 2021;13:801–807. doi:10.2147/CEOR.S317687
12. Overton PM, Shalet N, Somers F, Allen JA. Patient preferences for subcutaneous versus intravenous administration of treatment for chronic immune system disorders: a systematic review. Patient Prefer Adherence. 2021;15:811–834. doi:10.2147/PPA.S303279
13. Mateos MV, Nahi H, Legiec W, et al. Subcutaneous versus intravenous daratumumab in patients with relapsed or refractory multiple myeloma (COLUMBA): a multicentre, open-label, non-inferiority, randomised, Phase 3 trial. Lancet Haematol. 2020;7(5):e370–e380. doi:10.1016/S2352-3026(20)30070-3
14. Tan AR, Im SA, Mattar A, et al. Fixed-dose combination of pertuzumab and trastuzumab for subcutaneous injection plus chemotherapy in HER2-positive early breast cancer (FeDeriCa): a randomised, open-label, multicentre, non-inferiority, phase 3 study. Lancet Oncol. 2021;22(1):85–97. doi:10.1016/S1470-2045(20)30536-2
15. van den Bemt BJF, Gettings L, Domańska B, Bruggraber R, Mountian I, Kristensen LE. A portfolio of biologic self-injection devices in rheumatology: how patient involvement in device design can improve treatment experience. Drug Deliv. 2019;26(1):384–392. doi:10.1080/10717544.2019.1587043
16. Bittner B. Customer-centric product presentations for monoclonal antibodies. AAPS Open. 2023;9(1):3. doi:10.1186/s41120-022-00069-y
17. Guo J, Weng J, Zhu Q, et al. A review of recent FDA-approved biologic-device combination products. J Pharm Sci. 2024;113(4):866–879. doi:10.1016/j.xphs.2023.12.022
18. Jolles S, Sleasman JW. Subcutaneous immunoglobulin replacement therapy with Hizentra, the first 20% SCIG preparation: a practical approach. Adv Ther. 2011;28(7):521–533. doi:10.1007/s12325-011-0036-y
19. Repro-Medical System, Inc. Freedomedge syringe infusion system. 510(k) premarket notification K214045. U.S. Food and Drug Administration. Available from: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpmn/pmn.cfm?ID=K214045.
20. Badkar AV, Gandhi RB, Davis SP, LaBarre MJ. Subcutaneous delivery of high-dose/volume biologics: current status and prospect for future advancements. Drug Des Devel Ther. 2021;15:159–170. doi:10.2147/DDDT.S287323
21. Jiskoot W, Hawe A, Menzen T, Volkin DB, Crommelin DJA. Ongoing challenges to develop high concentration monoclonal antibody-based formulations for subcutaneous administration: quo vadis?. J Pharm Sci. 2022;111(4):861–867. doi:10.1016/j.xphs.2021.11.008
22. Bittner B, Schmidt J, eds.. Formulation and Device Lifecycle Management of Biotherapeutics: A Guidance for Researchers and Drug Developers.
23. Bittner B, Schmidt J. Advancing subcutaneous dosing regimens for biotherapeutics: clinical strategies for expedited market access. BioDrugs. 2024;38(1):23–46. doi:10.1007/s40259-023-00626-1
24. Pang Y, D’Cunha R, Mohammad AS, et al. Clinical bridging from prefilled syringe to on-body injector for risankizumab in crohn’s disease. Clin Ther. 2024;46(1):30–39. doi:10.1016/j.clinthera.2023.10.008
25. Davis JD, Bravo Padros M, Conrado DJ, et al. Subcutaneous administration of monoclonal antibodies: pharmacology, delivery, immunogenicity, and learnings from applications to clinical development. Clin Pharmacol Ther. 2024;115(3):422–439. doi:10.1002/cpt.3150
26. Jackisch C, Müller V, Dall P, et al. Subcutaneous trastuzumab for HER2-positive breast cancer – evidence and practical experience in 7 German centers. Geburtshilfe Frauenheilkd. 2015;75(6):566–573. doi:10.1055/s-0035-1546172
27. Boudreau A. Practical considerations for the integration of subcutaneous targeted therapies into the oncology clinic. Can Oncol Nurs J. 2019;29(4):267–270. doi:10.5737/23688076394267270
28. Dent S, Ammendolea C, Christofides A, et al. A multidisciplinary perspective on the subcutaneous administration of trastuzumab in HER2-positive breast cancer. Curr Oncol. 2019;26(1):e70–e80. doi:10.3747/co.26.4220
29. DuMond B, Patel V, Gross A, Fung A, Weber S. Fixed-dose combination of pertuzumab and trastuzumab for subcutaneous injection in patients with HER2-positive breast cancer: a multidisciplinary approach. J Oncol Pharm Pract. 2021;27(5):1214–1221. doi:10.1177/1078155221999712
30. Eisenberg S. Subcutaneous administration: evolution, challenges, and the role of hyaluronidase. Clin J Oncol Nurs. 2021;25(6):663–671. doi:10.1188/21.CJON.663-671
31. Wolfromm A, Mittaine B, Gandrille N, Dallemagne J, Delarue R. Home administration of subcutaneous rituximab is safe and associated with significant cost saving: a single-center experience. Blood. 2017;130(Suppl 1):4676. doi:10.1182/blood.V130.Suppl_1.4676.4676
32. Iuliano F, Iuliano E, Rossi M. Assisted administration of subcutaneous rituximab to the patient’s home: significant reduction of indirect costs incurred by care recipients and unpaid caregivers together with a total adherence to the treatment schedule and same safety. Blood. 2018;132(Supplement 1):5869. doi:10.1182/blood-2018-99-118756
33. Denys H, Martinez-Mena CL, Martens MT, et al. Safety and tolerability of subcutaneous trastuzumab at home administration, results of the phase IIIb open-label BELIS study in HER2-positive early breast cancer. Breast Cancer Res Treat. 2020;181(1):97–105. doi:10.1007/s10549-020-05604-7
34. ten Tije AJ, van Steenis S, Briers J, Elsten EM. Safety and tolerability of subcutaneous trastuzumab (H SC) self-administered at home via single-use injection device (SID) in patients with HER2-positive early breast cancer (EBC): primary and final analysis of the open-label, phase IIIB HOMERUS study. Ann Oncol. 2020;31:S330. doi:10.1016/j.annonc.2020.08.2334
35. Wardley A, Canon JL, Elsten L, et al. Flexible care in breast cancer. ESMO Open. 2021;6(1):100007. doi:10.1016/j.esmoop.2020.100007
36. Dang CT, Tolaney SM, Riaz F, et al. Preliminary analysis of an expanded access study of the fixed-dose combination of pertuzumab (P) and trastuzumab (H) for subcutaneous injection (PH FDC SC) for at-home administration (admin) in patients (pts) with HER2-positive (HER2+) breast cancer (BC) during the COVID-19 pandemic. J Clin Oncol. 2022;40(16_suppl):1515. doi:10.1200/JCO.2022.40.16_suppl.151
37. Radecka B, Hudała-Klecha J, Sawka D, et al. Home-based treatment with subcutaneous trastuzumab: safe and acceptable not only during a pandemic – final analysis of the RWD project ‘FlexCare’. Oncol Clin Pract. 2023. doi:10.5603/ocp.2023.0025
38. Binder AF, Martinez-Outschoorn UE, Wilde L, et al. Open label single arm study to assess the implementation of home based daratumumab administration in patients being treated for multiple myeloma. J Clin Oncol. 2023;41(16_suppl):TPS1609–TPS1609. doi:10.1200/JCO.2023.41.16_suppl.TPS1609
39. A study to evaluate patient preference for home administration of fixed-dose combination of pertuzumab and trastuzumab for subcutaneous administration in participants with early or locally advanced/inflammatory HER2-positive breast cancer (ProHer) [clinical trial]. ClinicalTrials.gov. Identifier NCT05415215. Available from: https://clinicaltrials.gov/study/NCT05415215?intr=trastuzumab%20AND%20home&rank=4.
40. Comparison of in-home versus in-clinic administration of subcutaneous nivolumab through cancer CARE (connected access and remote expertise) beyond walls (CCBW) program [clinical trial]. ClinicalTrials.gov. Identifier NCT06265285. Available from: https://clinicaltrials.gov/study/NCT06265285?intr=home%20AND%20cancer%20AND%20subcutaneous&rank=1.
41. Cook G, Ashcroft J, Fernandez M, et al. Benefits of switching from intravenous to subcutaneous daratumumab: perspectives from UK healthcare providers. Front Oncol. 2023;13:1063144. doi:10.3389/fonc.2023.1063144
42. Amgen Inc. Repatha (evolocumab) prescribing information.
43. AbbVie Inc. Skyrizi (risankizumab) prescribing information.
44. Alexion Pharmaceuticals, Inc. Ultomiris (ravulizumab) prescribing information.
45. Apellis Pharmaceuticals. Empaveli (pegcetacoplan) prescribing information.
46. Amgen Inc. Important notice for patients: discontinuation of repatha (evolocumab) pushtronex® system (single-dose on-body infusor with prefilled cartridge). Available from: https://www.repatha.com/pushtronexsystemupdate#xd_co_f=MmIyNjg2YmYtZjY5Yy00MjMwLTgzYmItN2NhNzE3M2QxMTE3.
47. AstraZeneca PLC. AstraZeneca 9M and Q3 2023 results. Available from: https://www.astrazeneca.com/content/dam/az/PDF/2023/q3/9M_and_Q3_2023_results_announcement.pdf.
48. Perez EE, Orange JS, Bonilla F, et al. Update on the use of immunoglobulin in human disease: a review of evidence. J Allergy Clin Immunol. 2017;139(3S):S1–S46. doi:10.1016/j.jaci.2016.09.023
49. Epland K, Suez D, Paris K. A clinician’s guide for administration of high-concentration and facilitated subcutaneous immunoglobulin replacement therapy in patients with primary immunodeficiency diseases. Allergy Asthma Clin Immunol. 2022;18(1):87. doi:10.1186/s13223-022-00726-7
50. Mathias N, Huille S, Picci M, et al. Towards more tolerable subcutaneous administration: review of contributing factors for improving combination product design. Adv Drug Deliv Rev. 2024;209:115301. doi:10.1016/j.addr.2024.115301
51. Octapharma USA Inc. Cutaquig (human immune globulin subcutaneous) prescribing information.
52. Takeda Pharmaceuticals USA, Inc. Cuvitru (immune globulin subcutaneous) prescribing information.
53. Takeda Pharmaceuticals USA, Inc. Gammagard Liquid (immune globulin intravenous and subcutaneous) prescribing information.
54. Behring AG CSL. Hizentra (immune globulin subcutaneous) prescribing information.
55. Grifols Therapeutics LLC. Xembify (immune globulin subcutaneous) prescribing information.
56. Takeda Pharmaceuticals USA, Inc. HyQvia (immune globulin intravenous and recombinant human hyaluronidase) prescribing information.
57. Jolles S, Orange JS, Gardulf A, et al. Current treatment options with immunoglobulin G for the individualization of care in patients with primary immunodeficiency disease. Clin Exp Immunol. 2015;179(2):146–160. doi:10.1111/cei.12485
58. Duff C, Ochoa D, Riley P, Murphy E, Zampelli A. Importance of ancillary supplies for subcutaneous immunoglobulin infusion: management of the local infusion site. J Infus Nurs. 2013;36(6):384–390. doi:10.1097/NAN.0000000000000009
59. Mitschang T. Selecting SCIG pumps and needle sets. IG Living. 2015:44–46. Available from: https://www.igliving.com/magazine/articles/IGL_2015-04_AR_Product-Guide-Selecting-SCIG-Pumps-and-Needle-Sets.pdf.
60. Takeda Pharmaceuticals USA, Inc. Administration systems for HyQvia®. Available from: https://www.hyqviahcp.com/content/dam/takeda/imported/hyqvia/pdfs/ancillaries-guide.pdf.
61. KORU Medical Systems. FREEDOM60 Syringe Infusion System International Instructions for Use. Available from: https://d1io3yog0oux5.cloudfront.net/_3cbce79c603eec42c673e2bc7a921db7/korumedical/files/pages/IFUs/337125_F60Intl_IFU_English_Rev_A_%281%29.pdf.
62. KORU Medical Systems. FreedomEdge Syringe Infusion System International Instructions for Use. Available from: https://d1io3yog0oux5.cloudfront.net/_3cbce79c603eec42c673e2bc7a921db7/korumedical/files/pages/IFUs/347202_EdgeIntl_IFU_English_RevA_%281%29.pdf.
63. EMED Technologies Corporation. SCIg60 Infusion System User Manual, USA users. Available from: https://www.emedtc.com/_files/ugd/61b77c_30f5a016593048d38feb16f481ef4d34.pdf.
64. Moog Medical Devices Group. 6000 CMS and 6000 CMS IOD Ambulatory Infusion System User Manual. Available from: https://www.moogmedical.com/wp-content/uploads/2019/06/CURLIN-6000-User-Manual-1.pdf.
65. Smiths Medical, Inc. (now ICU Medical, Inc.). CADD-Solis VIP Ambulatory Infusion Pump Technical Manual. Avaialble from: http://www.hhvna.com/files/IV/CADD_Solis_VIP_Technical_Manual.pdf.
66. Mallick R, Solomon G, Bassett P, et al. Subcutaneous immunoglobulin replacement therapy in patients with immunodeficiencies: impact of drug packaging and administration method on patient-reported outcomes. BMC Immunol. 2024;25(1):18. doi:10.1186/s12865-024-00608-0
67. Immune Deficiency Foundation. IDF Guide for Nurses: Immunoglobulin Therapy for Primary Immunodeficiency Diseases 4th ed. Immune Deficiency Foundation; 2016. Available from: https://primaryimmune.org/resources/print-material/idf-guide-for-nurses-immunoglobulin-therapy-for-primary-immunodeficiency-diseases.
68. Boyle JM, Buckley RH. Population prevalence of diagnosed primary immunodeficiency diseases in the United States. J Clin Immunol. 2007;27(5):497–502. doi:10.1007/s10875-007-9103-1
69. Tangye SG, Al-Herz W, Bousfiha A, et al. Human inborn errors of immunity: 2019 update on the classification from the international union of immunological societies expert committee. J Clin Immunol. 2020;40(1):24–64. doi:10.1007/s10875-019-00737-x
70. Mohamed AF, Kilambi V, Luo MP, Iyer RG, Li-McLeod JM. Patient and parent preferences for immunoglobulin treatments: a conjoint analysis. J Med Econ. 2012;15(6):1183–1191. doi:10.3111/13696998.2012.716804
71. Español T, Prevot J, Drabwell J, Sondhi S, Olding L. Improving current immunoglobulin therapy for patients with primary immunodeficiency: quality of life and views on treatment. Patient Prefer Adherence. 2014;8:621–629. doi:10.2147/PPA.S60771
72. Gonzalez JM, Ballow M, Fairchild A, Runken MC. Primary immune deficiency: patients’ preferences for replacement immunoglobulin therapy. Front Immunol. 2022;13:827305. doi:10.3389/fimmu.2022.827305
73. Shapiro RS. Subcutaneous immunoglobulin therapy given by subcutaneous rapid push vs infusion pump: a retrospective analysis. Ann Allergy Asthma Immunol. 2013;111(1):51–55. doi:10.1016/j.anai.2013.04.015
74. Cozon GJN, Clerson P, Dokhan A, Fardini Y, Sala TP, Crave JC. In-depth interviews of patients with primary immunodeficiency who have experienced pump and rapid push subcutaneous infusions of immunoglobulins reveal new insights on their preference and expectations. Patient Prefer Adherence. 2018;12:423–429. doi:10.2147/PPA.S156983
75. Bienvenu B, Cozon G, Mataix Y, et al. Rapid push vs pump-infused subcutaneous immunoglobulin treatment: a randomized crossover study of quality of life in primary immunodeficiency patients. J Clin Immunol. 2018;38(4):503–512. doi:10.1007/s10875-018-0507-x
76. Warnatz K, Jolles S, Agostini C, et al. Subcutaneous gammanorm® by pump or rapid push infusion: impact of the device on quality of life in adult patients with primary immunodeficiencies. Clin Immunol. 2022;236:108938. doi:10.1016/j.clim.2022.108938
77. Wasserman RL, Cunningham-Rundles C, Anderson J, et al. Systemic IgG exposure and safety in patients with primary immunodeficiency: a randomized crossover study comparing a novel investigational wearable infusor versus the Crono pump. Immunotherapy. 2022;14(16):1315–1328. doi:10.2217/imt-2022-0097
78. Mallick R, Henderson T, Lahue BJ, Kafal A, Bassett P, Scalchunes C. Subcutaneous immunoglobulin in primary immunodeficiency – impact of training and infusion characteristics on patient-reported outcomes. BMC Immunol. 2020;21(1):47. doi:10.1186/s12865-020-00371-y
79. Petersson C, Fust R, Hagstedt C, Wågström P, Nilsdotter-Augustinsson Å. “Experiences of the burden of treatment” – patient reports of facilitated subcutaneous immunoglobulin treatment in adults with immunodeficiency. J Clin Nurs. 2018;27(23–24):4270–4278. doi:10.1111/jocn.14580
80. Anderson JT, Cowan J, Condino-Neto A, Levy D, Prusty S. Health-related quality of life in primary immunodeficiencies: impact of delayed diagnosis and treatment burden. Clin Immunol. 2022;236:108931. doi:10.1016/j.clim.2022.108931
81. Chérin P, Pindi Sala T, Clerson P, et al. Recovering autonomy is a key advantage of home-based immunoglobulin therapy in patients with myositis: a qualitative research study. Medicine. 2020;99(7):e19012. doi:10.1097/MD.0000000000019012
82. Meelad RA, Hamid IJA, Hashim IF, et al. Impact of primary immunodeficiency diseases on the life experiences of patients in Malaysia from the caregivers’ perspective: a qualitative study. Front Pediatr. 2022;10:846393. doi:10.3389/fped.2022.846393
83. Köse S, Sabetsarvestani R, Geçkil E, Kaleci E, Dönmez H. The experiences of children with primary immunodeficiency who receive immunoglobulin subcutaneously instead of intravenously. J Pediatr Health Care. 2024;38(1):13–20. doi:10.1016/j.pedhc.2023.08.002
84. Stevenson J, Poker R, Schoss J, et al. Pharmaceutical and biotech industry perspectives on optimizing patient experience and treatment adherence through subcutaneous drug delivery design. Adv Drug Deliv Rev. 2024;209:115322. doi:10.1016/j.addr.2024.115322
85. Green P, Schneider A, Lange J. Navigating large-volume subcutaneous injections of biopharmaceuticals: a systematic review of clinical pipelines and approved products. mAbs. 2024;16(1):2402713. doi:10.1080/19420862.2024.2402713
86. Baggott C, Chan A, Hurford S, et al. Patient preferences for asthma management: a qualitative study. BMJ Open. 2020;10(8):e037491. doi:10.1136/bmjopen-2020-037491
87. Malterud K, Siersma VD, Guassora AD. Sample size in qualitative interview studies: guided by information power. Qual Health Res. 2016;26(13):1753–1760. doi:10.1177/1049732315617444
88. Ridgeway JL, Egginton JS, Tiedje K, et al. Factors that lessen the burden of treatment in complex patients with chronic conditions: a qualitative study. Patient Prefer Adherence. 2014;8:339–351. doi:10.2147/PPA.S58014
89. Aguiar-Ibáñez R, Fotheringham I, Mittal L, Sillah A, Pathak S. Differences between intravenous and subcutaneous modes of administration in oncology from the patient, healthcare provider, and healthcare system perspectives: a systematic review. Adv Ther. 2024;41(12):4396–4417. doi:10.1007/s12325-024-02985-9
90. Deppenweiler M, Debled M, Robquin J-L, Lortal-Canguilhem B. Subcutaneous auto-administration of trastuzumab following therapeutic education: a case report. J Oncol Pharm Pract. 2019;25(6):1523–1525. doi:10.1177/1078155218792364
91. Dodhia V, Ng HW, Alves C, et al. A service evaluation of joint working across sectors to promote self-administration of subcutaneous systemic anti-cancer therapy in breast cancer patients. Int J Pharm Pract. 2022;30(Suppl_2):ii17–ii18. doi:10.1093/ijpp/riac089.019
92. Younger ME, Blouin W, Duff C, Epland KB, Murphy E, Sedlak D. Subcutaneous immunoglobulin replacement therapy: ensuring success. J Infus Nurs. 2015;38(1):70–79. doi:10.1097/NAN.0000000000000087
93. Hertig JB, Degnan DD, Scott CR, Lenz JR, Li X, Anderson CM. A comparison of error rates between intravenous push methods: a prospective, multisite, observational study. J Patient Saf. 2018;14(1):60–65. doi:10.1097/PTS.0000000000000419
94. Ammor W, Chapron P, Goubil A, Fronteau C, Peyrilles E, Cormier N. 5PSQ-151 optimisation of the subcutaneous administration of daratumumab. Eur J Hosp Pharm. 2022;
95. Miars LK, Tran M, Duff K. Practical considerations for self-administration of subcutaneous immunoglobulin G utilizing recombinant human hyaluronidase, an advanced method of subcutaneous administration: a nurse’s perspective. J Infus Nurs. 2016;39(6):359–368. doi:10.1097/NAN.0000000000000182
96. KORU Medical Systems. Freedom60 infusion system instructions for use (US). Available from: https://d1io3yog0oux5.cloudfront.net/_6c7f6d5ccc26de450e7f1f00dcc32632/korumedical/files/pages/IFUs/F60_Domestic_IFU_337126_Rev_D_%282%29.pdf.
97. KORU Medical Systems. FreedomEdge syringe infusion system instructions for use (US). Available from: https://d1io3yog0oux5.cloudfront.net/_c8c67187e5feb382936ec2d0dcfa02a6/korumedical/files/pages/IFUs/FreedomEdge_Domestic_IFU_347201_Rev_A_%281%29.pdf.
98. EMED Technologies Corporation. VersaRate plus instructions for use. Available from: https://www.emedtc.com/_files/ugd/61b77c_145c69c0f7f84b39bb9a263d6ec01208.pdf.
99. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: multiple myeloma version 1 2025. National Comprehensive Cancer Network. 2024.
100. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: breast cancer. version 6.2024. National Comprehensive Cancer Network. 2024.
101. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: b-cell lymphomas. version 1.2025. National Comprehensive Cancer Network. 2024.
102. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: non-small cell lung cancer. version 1.2025. National Comprehensive Cancer Network. 2024.
103. Backler C, Kirmse JM, eds.. Access Device Guidelines: Recommendations for Nursing Practice and Education.
104. Bloch-Teitelbaum A, Lüde S, Rauber-Lüthy C, et al. Medication wrong route administration: a poisons center-based study. Expert Opin Drug Saf. 2013;12(2):145–152. doi:10.1517/14740338.2013.770468
105. Liptrott S, Cambon N, Berthillon N, Mendoza M, Smith R. Minimization of administration route errors with subcutaneous rituximab. J Oncol Pharm Pract. 2016;22(1):186–187. doi:10.1177/1078155214556010
106. Sreedhara SA, Zamiri C, Goswami S, et al. Challenges of using closed system transfer devices with biological drug products: an industry perspective. J Pharm Sci. 2020;109(1):22–29. doi:10.1016/j.xphs.2019.10.042
107. Besheer A, Burton L, Rj G, et al. An industry perspective on compatibility assessment of closed system drug-transfer devices for biologics. J Pharm Sci. 2021;110(2):610–614. doi:10.1016/j.xphs.2020.10.047
108. Gopalrathnam G, Christian TR, Jagannathan B, et al. An industry perspective on the challenges of using closed system transfer devices with biologics and communication guidance to healthcare professionals. J Pharm Sci. 2021;110(6):2329–2335. doi:10.1016/j.xphs.2021.02.008
109. Wozniewski M, Besheer A, Sediq AS, Huwyler J, Mahler HC, Levet V. Characterization of silicone from closed system transfer devices and its migration into pharmaceutical drug products. J Pharm Sci. 2024;113(2):419–426. doi:10.1016/j.xphs.2023.11.012
110. Fast J, Christian T, Crul M, et al. Use of closed system transfer devices (CSTDs) with protein-based therapeutic drugs – a non-solution for a non-problem?. J Pharm Sci. 2024;113(2):298–305. doi:10.1016/j.xphs.2023.11.014
111. Di Russo M, Zjalic D, Lombardi GS, et al. Impact of the 50 biggest pharma companies: a review of environmental report aspiring to NetZero. Eur J Public Health. 2023;33(Suppl 2):
112. Centers for Medicare & Medicaid Services. Durable medical equipment, prosthetic devices, prosthetics, orthotics, & supplies (DMEPOS). Available from: https://www.cms.gov/medicare/payment/fee-schedules/dmepos.
113. Centers for Medicare & Medicaid Services. Home infusion therapy/home IVIG services. Available from: https://www.cms.gov/medicare/payment/fee-for-service-providers/home-infusion-therapy.
114. Murphy E, Vanname C, McNeill R, Bullock M, Barrett L, Kafal A. Infusion parameters and demographics of patients with chronic inflammatory demyelinating polyneuropathy during subcutaneous immunoglobulin self-administration training. J Infus Nurs. 2021;44(5):289–297. doi:10.1097/NAN.0000000000000441
115. Chapel H, Gardulf A. Subcutaneous immunoglobulin replacement therapy. Curr Opin Allergy Clin Immunol. 2013;13(6):623–629. doi:10.1097/ACI.0000000000000013
116. Mallick R, Solomon G, Bassett P, Zhang X, Patel P, Lepeshkina O. Immunoglobulin replacement therapy in patients with immunodeficiencies: impact of infusion method on patient-reported outcomes. Allergy Asthma Clin Immunol. 2022;18(1):110. doi:10.1186/s13223-022-00746-3
117. Rinaldi A, Katsaros D, Hawthorne J, et al. The current paradigm for biologic initiation: a mixed-methods exploration of practices, unmet needs, and innovation opportunities in self-injection training. Expert Opin Drug Deliv. 2021;18(8):1–18. doi:10.1080/17425247.2021.1912009
118. Hawthorne J, Katsaros D, Rinaldi A, et al. The current paradigm for biologic initiation: a confirmatory quantitative analysis of self-injection training practices. Expert Opin Drug Deliv. 2022;19(6):733–742. doi:10.1080/17425247.2022.2078300
119. Younger ME, Aro L, Blouin W, et al. Nursing guidelines for administration of immunoglobulin replacement therapy. J Infus Nurs. 2013;36(1):58–68. doi:10.1097/NAN.0b013e3182798af8
120. Anderson-Smits C, Park M, Bell J, Mitchell S, Hartley L, Hawe E. Subcutaneous immunoglobulin use in immunoglobulin-naive patients with primary immunodeficiency: a systematic review. Immunotherapy. 2022;14(5):373–387. doi:10.2217/imt-2021-0265
121. Immune Deficiency Foundation. Treatment experiences and preferences among patients with primary immunodeficiency: national survey of patients (2018). Available from: https://primaryimmune.org/resources/print-material/national-survey-of-patients-2018.
122. Kafal AR, Vinh DC, Langelier MJ. Prefilled syringes for immunoglobulin G (IgG) replacement therapy: clinical experience from other disease settings. Expert Opin Drug Deliv. 2018;15(12):1199–1209. doi:10.1080/17425247.2018.1546692
123. Niebur HB, Duff CM, Shear GF, et al. Efficacy and tolerability of 16% subcutaneous immunoglobulin compared with 20% subcutaneous immunoglobulin in primary antibody deficiency. Clin Exp Immunol. 2015;181(3):441–450. doi:10.1111/cei.12623
124. Gardulf A. Clinical experiences in primary and secondary immunodeficiencies and immune-mediated conditions using Gammanorm(®). Immunotherapy. 2016;8(5):633–647. doi:10.2217/imt-2015-0013
125. Paci A, Desnoyer A, Delahousse J, et al. Pharmacokinetic/pharmacodynamic relationship of therapeutic monoclonal antibodies used in oncology: part 1, monoclonal antibodies, antibody-drug conjugates and bispecific T-cell engagers. Eur J Cancer. 2020;128:107–118. doi:10.1016/j.ejca.2020.01.005
126. Desnoyer A, Broutin S, Delahousse J, et al. Pharmacokinetic/pharmacodynamic relationship of therapeutic monoclonal antibodies used in oncology: part 2, immune checkpoint inhibitor antibodies. Eur J Cancer. 2020;128:119–128. doi:10.1016/j.ejca.2020.01.003
127. United Therapeutics. Remunity User Guide. Available from: https://www.remodulin.com/assets/files/Remunity-User-Guide.pdf.
128. Coyne M, Rinaldi A, Brigham K, et al. Impact of routines and rituals on burden of treatment, patient training, cognitive load, and anxiety in self-injected biologic therapy. Patient Prefer Adherence. 2022;16:2593–2607. doi:10.2147/PPA.S375037
129. Heinemann L. Insulin infusion sets: a critical reappraisal. Diabetes Technol Ther. 2016;18(5):327–333. doi:10.1089/dia.2016.0013
130. Dolton MJ, Chesterman A, Moein A, et al. Safety, tolerability, and pharmacokinetics of high-volume subcutaneous crenezumab, with and without recombinant human hyaluronidase in healthy volunteers. Clin Pharmacol Ther. 2021;110(5):1337–1348. doi:10.1002/cpt.2385
131. Evert AB, Bode BW, Buckingham BA, et al. Improving patient experience with insulin infusion sets: practical guidelines and future directions. Diabetes Educ. 2016;42(4):470–484. doi:10.1177/0145721716642526
132. Zhang G, Romo-Anselmo E, Kwa T, et al. Advances in insulin infusion set in the new era of automated insulin delivery: a systematic review. J Diabetes Sci Technol. 2023;17(2):302–313. doi:10.1177/19322968221145731
133. Apellis Pharmaceuticals. Empaveli Injector Instructions for Use. Available from: https://pi.apellis.com/files/IFU_Empaveli_Injector.pdf.
134. scPharmaceuticals, Inc. Furoscix Instructions for Use. Avaialble from: https://www.furoscix.com/wp-content/uploads/instructions-for-use.pdf.
135. Ponsford M, Carne E, Kingdon C, et al. Facilitated subcutaneous immunoglobulin (fSCIg) therapy – practical considerations. Clin Exp Immunol. 2015;182(3):302–313. doi:10.1111/cei.12694
136. Ohashi K, Dalleur O, Dykes PC, Bates DW. Benefits and risks of using smart pumps to reduce medication error rates: a systematic review. Drug Saf. 2014;37(12):1011–1020. doi:10.1007/s40264-014-0232-1
137. Schnock KO, Dykes PC, Albert J, et al. The frequency of intravenous medication administration errors related to smart infusion pumps: a multihospital observational study. BMJ Qual Saf. 2017;26(2):131–140. doi:10.1136/bmjqs-2015-004465
138. Blandford A, Dykes PC, Franklin BD, et al. Intravenous infusion administration: a comparative study of practices and errors between the United States and England and their implications for patient safety. Drug Saf. 2019;42(10):1157–1165. doi:10.1007/s40264-019-00841-2
139. Lehoux P. Patients’ perspectives on high-tech home care: a qualitative inquiry into the user-friendliness of four technologies. BMC Health Serv Res. 2004;4(1):28. doi:10.1186/1472-6963-4-28
140. U.S. Food and Drug Administration. White paper: infusion pump improvement initiative. 2010. Available from: https://www.fda.gov/medical-devices/infusion-pumps/white-paper-infusion-pump-improvement-initiative.
141. U.S. Food and Drug Administration. Infusion pumps total product life cycle: guidance for industry and FDA staff. December 2014. Available from: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/infusion-pumps-total-product-life-cycle.
142. U.S. Food and Drug Administration. Manufacturer and User Facility Device Experience (MAUDE) database; report number MW5120433. Available from: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfMAUDE/Detail.CFM?MDRFOI__ID=17436790&pc=FRN.
143. U.S. Food and Drug Administration. Manufacturer and User Facility Device Experience (MAUDE) database; report number MW5112862. Available from: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfMAUDE/Detail.CFM?MDRFOI__ID=15674289&pc=FRN.
144. Jain M, Doughty D, Clawson C, et al. Tralokinumab pharmacokinetics and tolerability when administered by different subcutaneous injection methods and rates. Int J Clin Pharmacol Ther. 2017;55(7):606–620. doi:10.5414/CP203023
145. Bruin G, Hockey HP, La Stella P, et al. Comparison of pharmacokinetics, safety and tolerability of secukinumab administered subcutaneously using different delivery systems in healthy volunteers and in psoriasis patients. Br J Clin Pharmacol. 2020;86(2):338–351. doi:10.1111/bcp.14155
146. U.S. Food and Drug Administration. Manufacturer and User Facility Device Experience (MAUDE) database; report number MW5070008. Available from: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfMAUDE/Detail.CFM?MDRFOI__ID=6587469&pc=FRN.
147. U.S. Food and Drug Administration. Manufacturer and User Facility Device Experience (MAUDE) database; report number MW5097586. Available from: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfMAUDE/Detail.CFM?MDRFOI__ID=10770289&pc=FRN.
148. U.S. Food and Drug Administration. Manufacturer and User Facility Device Experience (MAUDE) database; report number 3012307300-2019-01566. Available from: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfMAUDE/Detail.CFM?MDRFOI__ID=8506112&pc=FRN.
149. U.S. Food and Drug Administration. Manufacturer and User Facility Device Experience (MAUDE) Database; report number 3012307300-2018-08238. Available from: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfMAUDE/Detail.CFM?MDRFOI__ID=8066546&pc=FRN.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.