Back to Journals » Patient Preference and Adherence » Volume 16
Patient Adherence to Therapy After Myocardial Infarction: A Scoping Review
Authors Zorina O ![]() , Fatkulina N
, Fatkulina N ![]() , Saduyeva F, Omarkulov B, Serikova S
, Saduyeva F, Omarkulov B, Serikova S
Received 24 January 2022
Accepted for publication 2 June 2022
Published 4 July 2022 Volume 2022:16 Pages 1613—1622
DOI https://doi.org/10.2147/PPA.S356653
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Olga Zorina,1 Natalja Fatkulina,2 Feruza Saduyeva,1 Bauyrzhan Omarkulov,3 Saltanat Serikova1
1Research School, Karaganda Medical University, Karaganda, Kazakhstan; 2Institute of Health Sciences, Vilnius University, Vilnius, Lithuania; 3Institute of Public Health and Professional Health, Karaganda Medical University, Karaganda, Kazakhstan
Correspondence: Olga Zorina; Natalja Fatkulina, Email [email protected]; [email protected]
Background: Patients with myocardial infarction have low adherence to secondary prevention. Patients with acute coronary syndromes usually decide not to take cardiac drugs for 7 days after discharge for various reasons and adherence rates are usually very low. The aim of this scoping review was to identify factors influencing treatment adherence after myocardial infarction and the role of interventions to improve treatment adherence.
Methods: Two electronic databases (PubMed and Web of Science) were systematically searched for relevant published reviews of interventions for adherence after myocardial infarction. Inclusion criteria were study design: randomized control trial, systematic reviews; published in English; sample age ≥ 18 years. The methodological framework proposed by Arksey & O’Malley was used to guide the review process of the study.
Results: Thirteen articles met the inclusion/exclusion criteria. Four of the thirteen studies assessed factors influencing patient adherence to therapy after myocardial infarction, the remaining studies examined various interventions increasing adherence to treatment after myocardial infarction.
Conclusion: There is a need to improve adherence of patients to treatment after myocardial infarction. Studies show that the use of modern technologies and communication with the patients by phone improve adherence to treatment.
Keywords: adherence, nursing, myocardial infarction
Introduction
Cardiovascular disease is a major burden of noncommunicable diseases.1 Reducing morbidity and mortality from cardiovascular diseases is recognized as a key global health priority for WHO.2
Non-adherence to treatment results in potentially preventable morbidity and mortality as well as unnecessary health care visits and therefore financial costs. Traditional methods of identifying patients with low adherence are based either on asking patients if they have difficulty taking medications on an individual basis or on analyzing pharmacy registration data to determine which patients have missed prescription-only medications.3 While significant resources are being devoted to the development of new therapies, non-adherence of existing drugs has become recognized but not well managed.4
More than half of all deaths in Kazakhstan were caused by cardiovascular diseases, stroke, myocardial infarction (MI) and other diseases of the circulatory system highlighting the need to combat non-communicable diseases. Patient adherence to prescribed antihypertensive drugs at the PHC level is too low, it is <30%.5 When analyzing adherence to treatment in Kazakhstan it was found that only 45.2% had been taking antihypertensive drugs daily.6
Ischemic heart disease is currently the leading cause of death in Europe. Of the 4,527,500 deaths reported in the European Union (EU) in 2016, 542,700 deaths were due to coronary diseases including heart attacks. Nearly 90% of these deaths were in people over 65 (475,600 deaths, 88% of the EU total). The highest mortality rate from coronary heart disease is reported to be in Lithuania, the lowest one is estimated to be in France. Lithuania where 5362 per million people died of heart attacks, had the highest rate of any EU member state in 2017. Adherence to statins in France is only 24%.6,7
About half of American adults say they have been prescribed at least one medication in the past 30 days and almost a quarter of them have been prescribed three or more medications a day. The use of several drugs per day creates difficulties for patients and thereby reduces patient adherence to treatment. It is estimated that in the United States the adherence of patients with chronic diseases is only 50%.8
Case management programs are one approach to personalized secondary prevention. These programs are designed to improve treatment adherence and provide guidance that encourages patients to make healthy lifestyle choices and optimal disease management. The importance of combination of counseling and regular assessment of risk factors and health status conducted in nurse-led clinics have been supported by some available researches.9 The aim of this scoping review is to identify factors influencing adherence of patients after myocardial infarction and management of therapy in terms of various interventions.
Methods
We described the methodological section of scoping review according to the recommendations of Arksey & O’Malley.10 The process of conducting a scoping review is carried out iteratively, interacting with each stage reflectively, repeating the stages if necessary for the breadth of coverage of the literature.
Search Strategy
At this stage we have formulated a research question that guides the literature search strategy (What has been known from the existing literature about adherence to therapy in patients with myocardial infarction?). PubMed and Web of Science databases were searched for studies published between 2010 and 2020 using the keywords (adherence, nursing, myocardial infarction, cardiac rehabilitation).
Building a search in PubMed
Gather separate concepts:
- Search 1: adherence AND myocardial infarction AND cardiac rehabilitation.
- Search 2: nursing AND myocardial infarction AND cardiac rehabilitation.
- Search 3: NOT home-based cardiac rehabilitation.
We also selected filters to limit results, such as publication dates (last 10 years), English language, Humans, articles concerning particular age groups: ≥ 18, specific research study types: randomized control study, systematic review. We carried out the search strategy using a PRISMA (Figure 1).
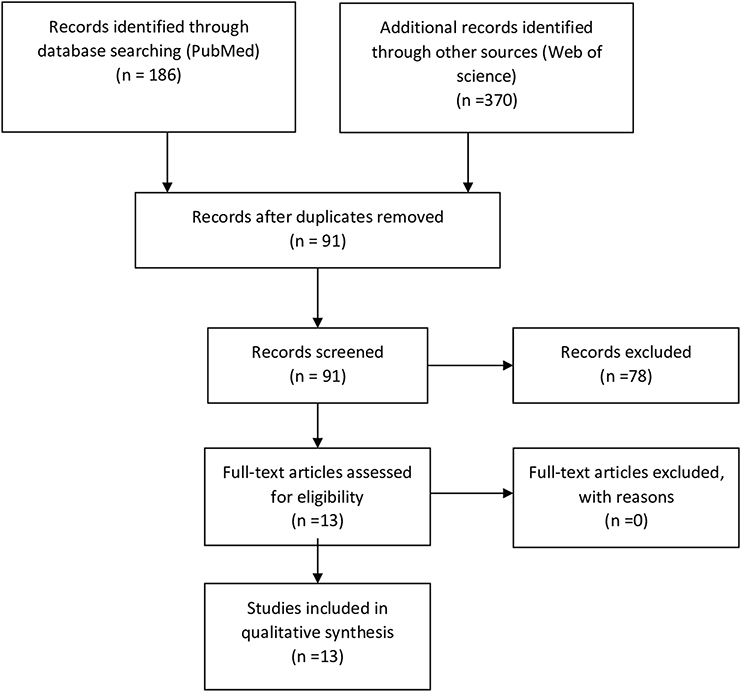 |
Figure 1 Study selection procedure. Notes: Adapted from: Page MJ, McKenzie JE, Bossuyt PM, Boutron I et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi: https://doi.org/10.1136/bmj.n71. Creative Commons Attribution (CC BY 4.0) license (https://creativecommons.org/licenses/by/4.0/legalcode). |
Study Selection
In conducting this study based on patient adherence to treatment after myocardial infarction, in our initial search we included articles published in English that presented (1) patients after myocardial infarction, (2) factors affecting treatment in patients after myocardial infarction; and (3) interventions that improve treatment adherence. This search yielded 556 articles. Studies that did not report original results (eg, commentaries, reviews, study protocols, and letters to the editor) or were reported as poster abstracts or dissertations were also excluded. The remaining abstracts and full texts were then retrieved to confirm that they met our inclusion/exclusion criteria (Table 1). The reference lists of the retrieved full texts were also perused to identify any additional relevant articles. Finally, 13 articles met our inclusion/exclusion criteria for this scoping review (Figure 1). We excluded studies that focused on the rehabilitation of patients after MI at the hospital, we focused on the secondary prevention of MI at the primary health care level.
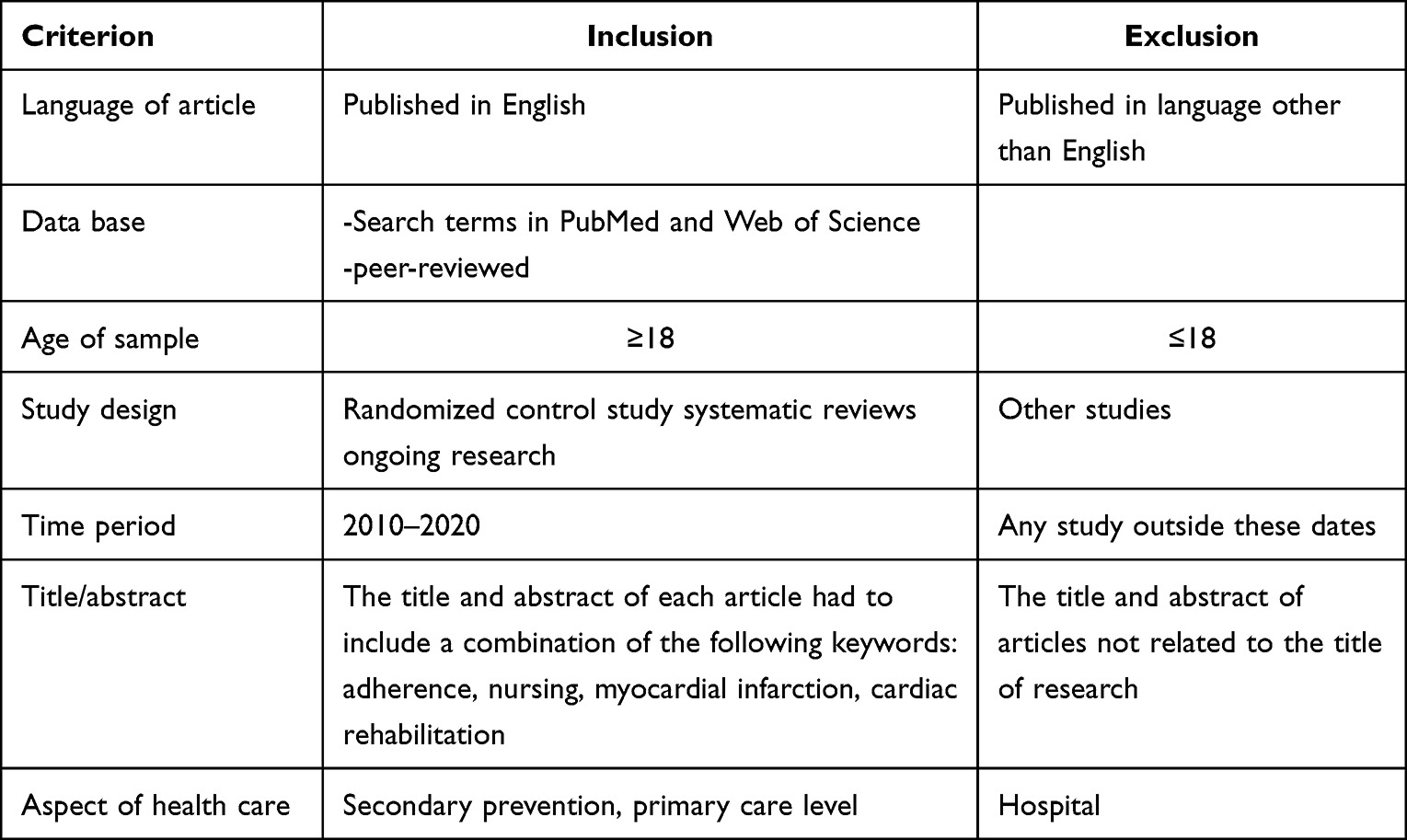 |
Table 1 Exclusion and Inclusion Criteria |
Data Abstraction and Analysis
From the final 13 articles, the following data were charted (Tables 2 and 3): (1) study design; (2) sample; (3) research instruments; (4) intervention; (5) data analysis, (6) statistical processing. These data were categorized and organized in Microsoft Excel with the use of narrative summaries to report the outcomes from the studies.
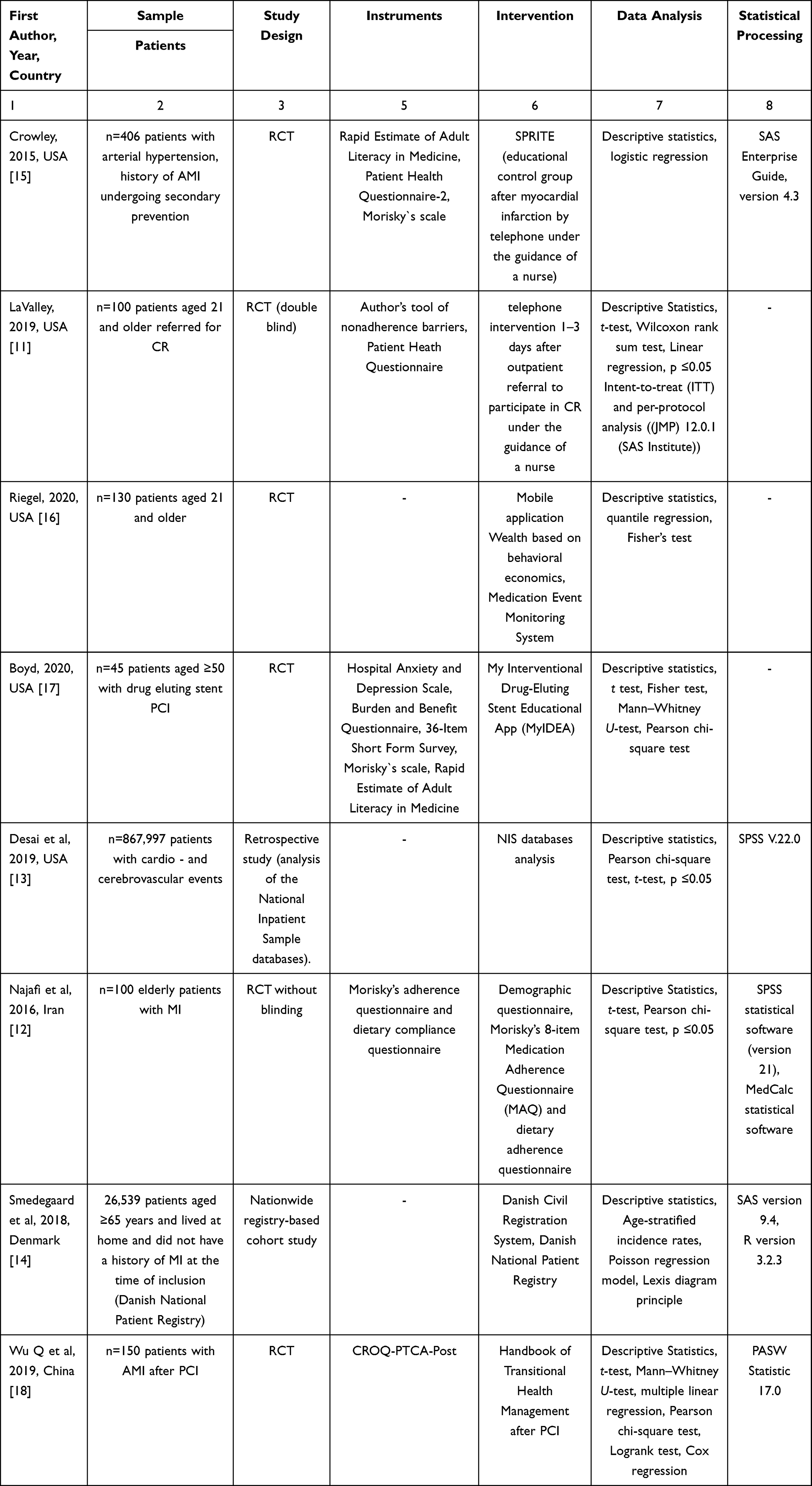 |
Table 2 Characteristics of Included Studies |
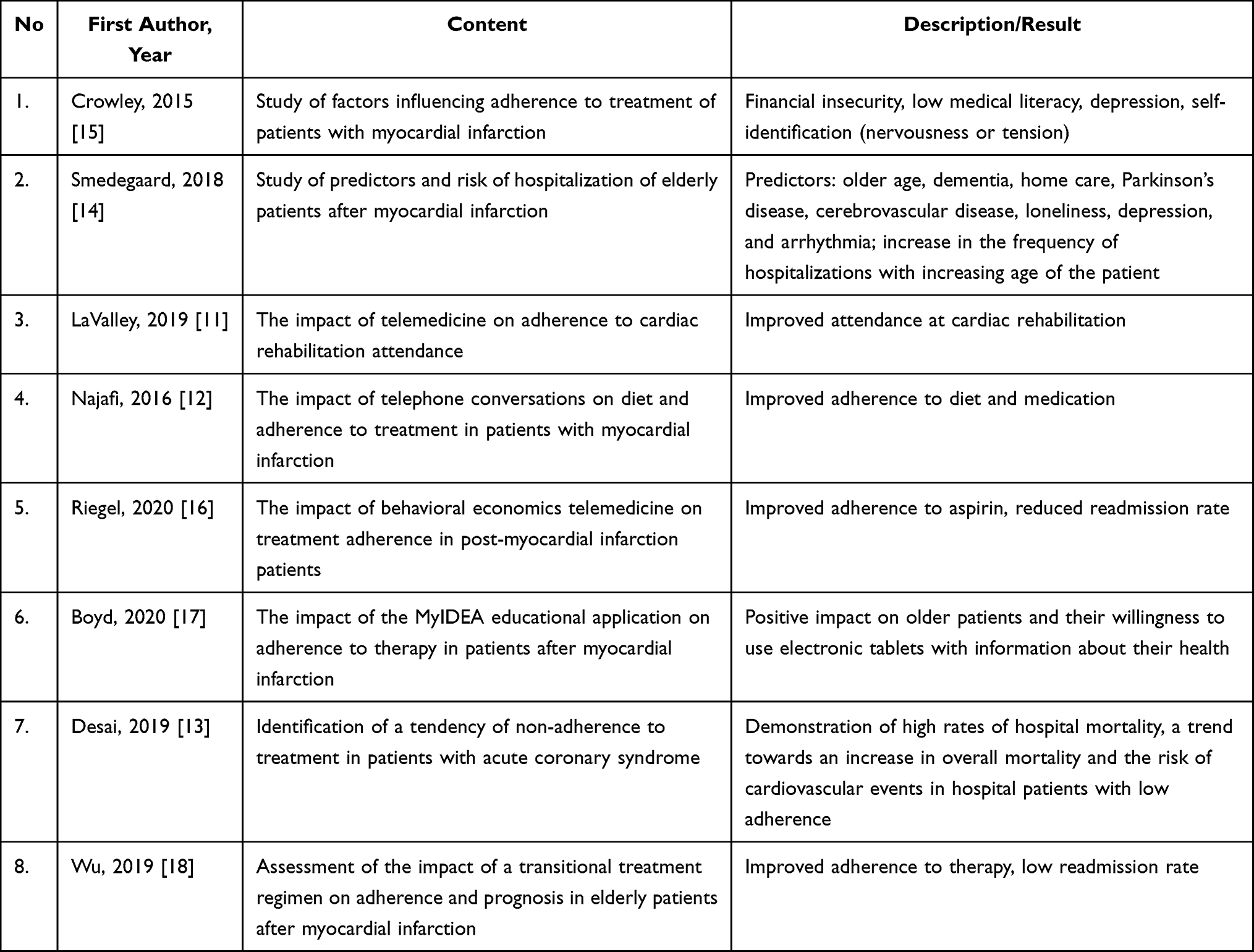 |
Table 3 Research Results |
Results
A detailed overview of the characteristics of and key outcomes from the 13 articles is provided in Tables 2 and 4 respectively. Five randomized control studies were conducted in USA11,13,15,16 and three in Iran,12 Denmark,14 China18 (Tables 2 and 3).
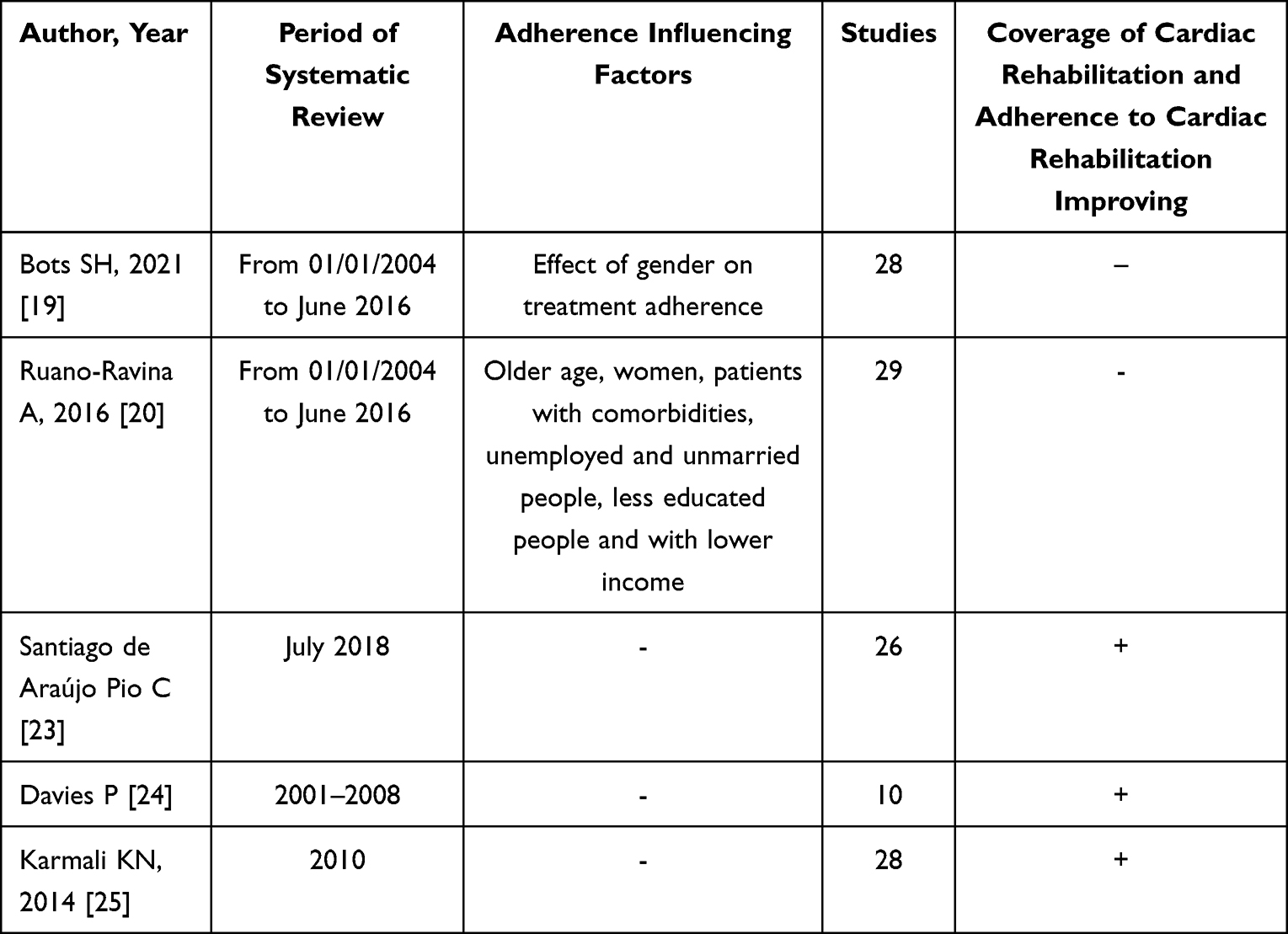 |
Table 4 Systematic Reviews |
Study Design
In the studies the authors quite often used a non-experimental design (Table 2). 6 studies were randomized controlled trials, 2 of which were double-blind11 and without blinding.12 One study was conducted using a retrospective design (analysis of national stationary sample databases)13 and the other study was a cohort design based on a nationwide registry.14
Sample
The analyzed studies enrolled patients (Table 2). The sample of patients included patients after MI, percutaneous coronary interventions, patient with arterial hypertension.
Interventions
The studies were included that examined factors influencing adherence to treatment after myocardial infarction and educational interventions to improve adherence to therapy and prevent readmission. Two studies (Table 2) used telephone intervention to improve patient adherence after myocardial infarction.11,15 The studies show that behavioral economics-based motivational telephone interventions targeting patients at risk of early study dropout shortly after targeting cardiac rehabilitation improve both timeliness and potential patient return rates and represent an adjunct to outpatient adherence.11 The positive effect of telephone observation under the supervision of nurses was noted as a method of remote care for patients after myocardial infarction, which improves adherence to drug therapy and diet.12 Behavioral economics-based telemedicine intervention improved adherence to low-dose aspirin treatment in patients after hospitalization for acute coronary syndrome. Once-daily aspirin adherence remained high among study participants who received telemedicine interventions, readmission rates decreased.16
The most common reasons for discontinuing a medication are ignorance of how long patients will need to take the medication, thus requiring interventions to inform patients. The researches by Riegel and Boyd16,17 used apps to assess and improve patients’ knowledge and adherence to treatment. According to the above mentioned researches elderly patients were in 2020 ready to use electronic tablets to obtain information about their health status after myocardial infarction and secondary prevention of the disease. The power of using mobile medical technologies lies in their ability to involve the patient through individualized interventions.17
One study used by One study used Handbook of Transitional Health Management after percutaneous coronary heart disease evaluated the impact of transitional health management on adherence and prognosis in elderly patients after myocardial infarction. Evaluation of the effect of a transitional treatment regimen on adherence and prognosis in elderly patients with acute myocardial infarction (AMI) undergoing percutaneous coronary intervention showed an improvement in adherence to treatment.18
Two studies conducted retrospective researches using National Patient Registration System to investigate predictors and risk of hospitalization in elderly patients after MI with the aim of subsequently improving adherence to therapy.12–14
Outcomes and Measures
In this review the instruments (Table 2) can be classified by three criteria: 1) medication and diet adherence; 2) patients quality of life and measurement of anxiety and depression symptoms; 3) patients literacy about their health. More than one tool was used in 5 studies. The Morisky’s adherence questionnaire was used in three studies.15,17,18 Low adherence to therapy is often found in patients with chronic diseases, in particular with cardiovascular diseases. There is a significant or nearly significant bivariate association with non-compliance with factors such as financial insecurity, poor health literacy, depression, and patient self-identification (nervousness or tension)15 (Table 4).
Health literacy was assessed via the Rapid Estimate of Adult Literacy in Medicine (REALM) in 2 studies.15,17 The Patient Health Questionnaire was used in two studies and the aspect of identifying oneself as nervous and tense is a factor associated with non-compliance with the treatment regimen.15,18
The study applying the MyIDEA educational app used the following tools: Hospital Anxiety and Depression Scale, Burden and Benefit Questionnaire, 36-Item Short Form Survey and Morisky`s scale,17 Dietary compliance questionnaire12 and CROQ-PTCA-Post.18
The use of interventions aimed at studying the factors affect the increase in adherence to treatment. It is known that women are less adherent to lipid-lowering drugs than men.19 It is also noted that it is worth paying special attention to elderly patients with concomitant diseases; unemployed and unmarried people, less educated people, people with lower income people.
Discussion
Our scoping review identified only 13 studies that examined factors influencing treatment adherence in patients after myocardial infarction and the role of various interventions to increase adherence. Most of the studies used Morisky’s adherence questionnaire to measure patient adherence and were randomized controlled trials.
Non-adherence is a serious barrier to long-term treatment of patients after MI which can be associated with medical, social and economic consequences.2 Factors associated with non-compliance with the bivariate analysis regimen include younger age, smoking, financial insecurity, identification as a nervous or stressed person, a higher score in life chaos, more anxiety about myocardial infarction, and more anxiety about stroke.15
Factors influencing adherence to treatment are gender,19 older age, presence of comorbidities, unemployed and unmarried persons, persons with low education and income.20
Myocardial infarction is a life-threatening form of coronary heart disease. Long-term treatment of patients after myocardial infarction is based on the implementation of a therapeutic plan, including lifestyle changes and pharmacotherapy using various influences. The need to improve adherence of patients to treatment after myocardial infarction is required.2
Impact of transitional treatment on adherence and prognosis in elderly patients with acute myocardial infarction who underwent percutaneous coronary intervention demonstrated better adherence to treatment, adherence to follow-up examinations, a propensity for a healthy lifestyle and improved clinical parameters, as well as a lower incidence of adverse cardiovascular events and repeated hospitalizations. Transitional health management using the Handbook of Transitional Health Management is an effective intervention for patients with percutaneous coronary intervention after discharge.18
Nurse-led patient counseling based on a belief model21 positively affect the patient’s involvement in healthy behavior, improves patient adherence and self-control after myocardial infarction.12,15
Patients who have had a myocardial infarction need to undergo cardiac rehabilitation to improve their health and prevent complications and recurrences of myocardial infarction. Evidence shows that attending the maximum number of sessions of cardiac rehabilitation reduces the risk and improves survival in older people after myocardial infarction,22 therefore an intervention to improve adherence is needed to optimize risk reduction and secondary prevention. Telephone intervention shows improved patient adherence to medications and cardiac rehabilitation attendance.11 Interventions using telemedicine such as individual consultations of patients by phone, the use of audio and video communications increase adherence of patients to cardiac rehabilitation.23,24
This scoping review describes interventions that address patient-identified barriers to attending cardiac rehabilitation after myocardial infarction, interventions that help increase the likelihood of rehabilitation success. These programs are: regular nurse or therapist-led visits, early post-discharge visits, letters of motivation, gender-responsive programs, and transition phase programs for older patients.25
Compliance with the dietary and drug regimen plays an important role in successful treatment and reduces the negative complications and severity of the course of diseases of the cardiovascular system. Approximately 24% of patients with ACS do not take their heart medications within 7 days of discharge, adherence rates are typically around 60–75% adherence to secondary prevention is low26 Modern technologies can help solve the problem of treatment adherence.27 Riegel and others have used telemedicine intervention to improve adherence to low-dose aspirin treatment in patients after hospitalization for acute coronary syndrome. Once-daily aspirin adherence remained high among study participants who received telemedicine interventions, and readmission rates were reduced.16
The power of using mobile medical technologies lies in their ability to involve the patient through individual interventions and increase adherence to therapy.28,29 The MyIDEA educational app is a tablet-based educational program developed in collaboration with patients, cardiologists, pharmacists, nurses, computer scientists and biomedical illustrators. This application used the stories of patients with cardiovascular disease to help an elderly patient plan and overcome common barriers to adherence, which had a positive impact on treatment adherence.17
Conclusion
In this scoping review we present results from 13 adherence studies of patients after myocardial infarction. Existing evidence demonstrates the importance of improving adherence to treatment among patients after myocardial infarction through the use of telemedicine in the form of telephone interventions and modern applications.
Implications for Practice
This study uncovers interventions that can increase adherence to treatment and participation in cardiac rehabilitation, such as telephone counseling, the use of various applications, taking into account the barriers to adherence. Strategies to overcome barriers to adherence can be helpful in improving adherence. Barriers to adherence to and participation in cardiac rehabilitation are many and varied, and reasons for non-participation may vary from person to person.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Aringazina A, Kuandikov T, Arkhipov V. Burden of the Cardiovascular Diseases in Central Asia. Cent Asian J Glob Health. 2018;7(1):321. doi:10.5195/cajgh.2018.321
2. Diem G, Brownson RC, Grabauskas V, Shatchkute A, Stachenko S. Prevention and control of noncommunicable diseases through evidence-based public health: implementing the NCD 2020 action plan. Glob Health Promot. 2016;23(3):5–13. doi:10.1177/1757975914567513
3. Zullig LL, Jazowski SA, Wang TY, et al. Novel application of approaches to predicting medication adherence using medical claims data. Health Serv Res. 2019;54(6):1255–1262. PMID: 31429471; PMCID: PMC6863234. doi:10.1111/1475-6773.13200
4. Smith SC Jr, Zheng ZJ. The impending cardiovascular pandemic in China. Circ Cardiovasc Qual Outcomes. 2010;3:226–227. doi:10.1161/CIRCOUTCOMES.110.957183
5. Wolrd Health Organization. Prevention and control of noncommunicable diseases in Kazakhstan. The case for investment; 2019. Available from: https://www.euro.who.int/en/countries/kazakhstan/publications/prevention-and-control-of-noncommunicable-diseases-in-kazakhstan.-the-case-for-investment-2019.
6. Eurostat. Deaths due to coronary heart diseases in the EU. Available from: https://ec.europa.eu/eurostat/web/products-eurostat-news/-/edn-20200928-1.
7. Radisauskas R, Kirvaitiene J, Bernotiene G, Virviciutė D, Ustinaviciene R, Tamosiunas A. Long-term survival after acute myocardial infarction in Lithuania during transitional period (1996–2015): data from population-based kaunas ischemic heart disease register. Medicina. 2019;55(7):357. PMID: 31324034; PMCID: PMC6681332. doi:10.3390/medicina55070357
8. Naderi SH, Bestwick JP, Wald DS. Adherence to drugs that prevent cardiovascular disease: meta-analysis on 376,162 patients. Am J Med. 2012;125:882–887. doi:10.1016/j.amjmed.2011.12.013
9. Kirsch F, Becker C, Kurz C, Schwettmann L, Schramm A. Effects of adherence to pharmacological secondary prevention after acute myocardial infarction on health care costs - an analysis of real-world data. BMC Health Serv Res. 2020;20(1):1145. PMID: 33342431; PMCID: PMC7751107. doi:10.1186/s12913-020-05946-4
10. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8:19–32. doi:10.1080/1364557032000119616
11. LaValley G, Storer A, Szalai H, Farah M, Pack QR. A motivational telephone intervention to reduce early dropouts in cardiac rehabilitation: a Feasibility Pilot Study. J Cardiopulm Rehabil Prev. 2019;39(5):318–324. doi:10.1097/HCR.0000000000000425
12. Najafi SS, Shaabani M, Momennassab M, Aghasadeghi K. The nurse-led telephone follow-up on medication and dietary adherence among patients after myocardial infarction: a randomized controlled clinical trial. Int J Community Based Nurs Midwifery. 2016;4(3):199–208.
13. Desai R, Thakkar S, Fong HK, et al. Rising trends in medication non-compliance and associated worsening cardiovascular and cerebrovascular outcomes among hospitalized adults across the United States. Cureus. 2019;11(8):e5389. doi:10.7759/cureus.5389
14. Smedegaard L, Kragholm K, Numé AK, Charlot MG, Gislason GH, Hansen PR. Nursing home admission after myocardial infarction in the elderly: a nationwide cohort study. PLoS One. 2018;13(8):e0202177. doi:10.1371/journal.pone.0202177
15. Crowley MJ, Zullig LL, Shah BR, et al. Medication non-adherence after myocardial infarction: an exploration of modifying factors. J Gen Intern Med. 2015;30(1):83–90. doi:10.1007/s11606-014-3072-x
16. Riegel B, Stephens-Shields A, Jaskowiak-Barr A, Daus M, Kimmel SE. A behavioral economics-based telehealth intervention to improve aspirin adherence following hospitalization for acute coronary syndrome. Pharmacoepidemiol Drug Saf. 2020;29(5):513–517. doi:10.1002/pds.4988
17. Boyd AD, Ndukwe CI, Dileep A, et al. Elderly medication adherence intervention using the my interventional drug-eluting stent educational app: multisite randomized feasibility trial. JMIR Mhealth Uhealth. 2020;8(6):e15900. PMID: 32579120; PMCID: PMC7381043. doi:10.2196/15900
18. Wu Q, Zhang D, Zhao Q, et al. Effects of transitional health management on adherence and prognosis in elderly patients with acute myocardial infarction in percutaneous coronary intervention: a cluster randomized controlled trial. PLoS One. 2019;14(5):e0217535. doi:10.1371/journal.pone.0217535
19. Bots SH, Inia JA, Peters SA. Medication adherence after acute coronary syndrome in women compared with men: a systematic review and meta-analysis. Front Glob Womens Health. 2021;2. doi:10.3389/fgwh.2021.637398
20. Ruano-Ravina A, Pena-Gil C, Abu-Assi E, et al. Participation and adherence to cardiac rehabilitation programs. A systematic review. Int J Cardiol. 2016;223:436–443. PMID: 27557484. doi:10.1016/j.ijcard.2016.08.120
21. Becker MH, Maiman LA. Sociobehavioral determinants of compliance with health and medical care recommendations. Med Care. 1975;13(1):10–24. PMID: 1089182. doi:10.1097/00005650-197501000-00002
22. Goff DC Jr, Lloyd-Jones DM, Bennett G, et al. American Heart Association/American College of Cardiology guideline on the assessment of cardiovascular risk. Circulation. 2013;25(Suppl 2):S49–S73.
23. Santiago de Araújo Pio C, Chaves GS, Davies P, Taylor RS, Grace SL. Interventions to promote patient utilisation of cardiac rehabilitation. Cochrane Database Syst Rev. 2019;2(2):CD007131. doi:10.1002/14651858.CD007131.pub4
24. Davies P, Taylor F, Beswick A, et al. Promoting patient uptake and adherence in cardiac rehabilitation. Cochrane Database Syst Rev. 2010;7:CD007131. PMID: 20614453; PMCID: PMC4164451. doi:10.1002/14651858.CD007131.pub2
25. Karmali KN, Davies P, Taylor F, Beswick A, Martin N, Ebrahim S. Promoting patient uptake and adherence in cardiac rehabilitation. Cochrane Database Syst Rev. 2014:CD007131. PMID: 24963623. doi:10.1002/14651858.CD007131.pub3
26. Zhang Y, Kaplan CM, Baik SH, Chang CC, Lave JR. Medication adherence and readmission after myocardial infarction in the Medicare population. Am J Manag Care. 2014;20(11):e498–505.
27. Paterson M, Kinnear M, Bond C, McKinstry B. A systematic review of electronic multi-compartment medication devices with reminder systems for improving adherence to self-administered medications. Int J Pharm Pract. 2017;25(3):185–194. PMID: 26833669. doi:10.1111/ijpp.12242
28. Hsu G, Crawford S, Paolella G, et al. Design of customized mobile application for patient adherence to oral anticancer medications utilizing user-centered design. J Biocommun. 2017;41(1). doi:10.5210/jbc.v41i1.7499
29. Militello LG, Saleem JJ, Borders MR, et al. Designing colorectal cancer screening decision support: a cognitive engineering enterprise. J Cogn Eng Decis Mak. 2016;10(1):74–90. doi:10.1177/1555343416630875
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.