Back to Journals » Open Access Journal of Contraception » Volume 16
Pathophysiological Consequences Associated with Hormonal Contraceptives Use in Sub-Saharan Africa: A Scoping Review
Authors Kampire MG, Hakizimana JC, Mucumbitsi J, Alagbonsi AI ![]()
Received 27 August 2025
Accepted for publication 8 November 2025
Published 14 November 2025 Volume 2025:16 Pages 171—187
DOI https://doi.org/10.2147/OAJC.S563680
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Marie Gorette Kampire,1,* Jean Claude Hakizimana,2,* Joseph Mucumbitsi,3,* Abdullateef Isiaka Alagbonsi2
1Department of Biochemistry, Adventist School of Medicine of East-Central Africa (ASOME), Kigali, Rwanda; 2Department of Physiology, School of Medicine and Pharmacy, College of Medicine and Health Sciences, University of Rwanda, Huye, Rwanda; 3Department of Microbiology, Adventist School of Medicine of East-Central Africa (ASOME), Kigali, Rwanda
*These authors contributed equally to this work
Correspondence: Abdullateef Isiaka Alagbonsi, Department of Physiology, School of Medicine and Pharmacy, College of Medicine and Health Sciences, University of Rwanda, Huye, Rwanda, Email [email protected]
Background: Although the safety profile of hormonal contraceptives (HCs) in African populations is still unclear, their use is growing in Sub-Saharan Africa (SSA) to lower unwanted pregnancies. Hematological, cardiometabolic, endocrine, immunological, and psychological consequences are among the reported negative outcomes. This scoping review summarizes the most recent data on the pathophysiological consequences associated with the use of HCs in SSA.
Methods: A comprehensive search via PubMed, African Journal Online, Wiley Online Library, and Google Scholar, following PRISMA-ScR guidelines, identified studies published between 2000 and 2025 on adverse outcomes of HCs in SSA. Eligible studies involved laboratory analysis, cross-sectional surveys, cohort studies, and randomized controlled trials and were conducted in English. Data were charted by country, design, contraceptive type, and adverse outcomes.
Results: Fifty-one eligible studies from SSA were analyzed, revealing diverse pathophysiological consequences. Hematological effects were reported in 7 studies, showing a higher hematological profile and reduced anemia risk among users of HCs. Cardiometabolic impacts were noted in 17 studies, with dyslipidemia (40– 60% prevalence), hypertension, and weight gain (1– 3 kg/m2 BMI increase) linked to depot medroxyprogesterone acetate (DMPA) and combined oral contraceptives (COCs). Endocrine effects were observed in 3 studies, while 12 studies showed vulnerability of HCs users to sexually transmitted and other forms of infections. Immune dysregulation and microbiota changes were reported in 5 studies. A study each reported varying consequences, including anthropometry, bone density, sexual dysfunction and depression, bleeding irregularities, electrocardiogram, spermatotoxicity, and biochemical changes.
Conclusion: Use of HCs in SSA is linked to a variety of diseases in the immunological, metabolic, endocrine, hematologic, and psychological domains. To inform safe contraceptive usage and reproductive health policy in SSA, these findings highlight the necessity of integrated contraceptive counseling, clinical monitoring for comorbidities, and additional region-specific research.
Keywords: contraceptives, pathophysiology, Sub-Sahara Africa
Corrigendum for this paper has been published.
Introduction
In sub-Saharan Africa (SSA), family planning is crucial for public health and socioeconomic development, as high fertility rates and rapid population growth lead to increased maternal and child mortality, strain on the healthcare system, and economic challenges. Modern contraceptives, such as combined oral contraceptives (COCs), progestin-only injectables like depot medroxyprogesterone acetate (DMPA) and norethisterone enanthate (NET-EN), subdermal implants, and intrauterine devices (IUDs), have been proven to reduce unintended pregnancies, unsafe abortions, and maternal mortality by allowing women to space or limit births.1 About 28.4% of women of reproductive age used modern contraceptives, including both short-acting and long-acting methods, with 18.7% using short-acting methods and 9.6% using long-acting methods, according to a 2025 multilevel multivariate analysis of Demographic and Health Survey (DHS) data from 23 SSA countries (2015–2023).2 Factors like parity, parental education, age, media exposure, and wealth index had a substantial impact on this prevalence.3 Even with these advancements, contraceptive use is not optimal, as barriers such as limited access, cultural stigma, and worries about side effects impede wider adoption.
Although hormonal contraceptives (HCs) provide significant advantages, their use is linked to various negative health effects, especially in the unique epidemiological context of SSA, which is marked by a high prevalence of Human Immunodeficiency virus (HIV), anemia, and emerging non-communicable diseases. There is a connection between hormonal contraceptives and metabolic disturbances such as dyslipidemia, high blood pressure, increased body mass index (BMI), and impaired glucose tolerance, all of which may raise cardiometabolic disorders.4–7 Hematological effects play a significant role as well, with certain studies indicating that hormonal contraceptives may offer protection against anemia,8–10 whereas copper IUDs can worsen iron deficiency in specific groups. There have also been reports of immunological effects, including changes in mucosal immune cell populations, cytokine production, and vaginal microbiota.11–13 For instance, DMPA use raised frequencies of Th17-like HIV target cells in the vaginal tract, according to a randomized experiment conducted in South Africa,14 which may alter vulnerability to HIV acquisition.
The significance of region-specific data is underscored by the interaction of these negative outcomes with contextual variables unique to SSA, including inadequate access to healthcare, comorbidities, and cultural perspectives. Levonorgestrel (LNG) implants, copper IUDs, and DMPA did not significantly increase the risk of HIV acquisition, according to large-scale studies like the Evidence for Contraceptive Options and HIV Outcomes (ECHO) trial.15 However, contradictory results from previous cohort studies16,17 underscore the need for method-specific and contextually relevant evaluations. Furthermore, little is known about the long-term hazards of continuous DMPA usage in SSA populations, especially for women and adolescents undergoing antiretroviral medication, apart from the reduction of bone mineral density.18
To develop safe and efficient family planning techniques, it is essential to synthesize the available data due to the variety of contraceptive methods and the conflicting facts regarding the health hazards they pose. This review maps the range of research on the metabolic, cardiovascular, hematological, and immunological effects of using contraceptives by combining results from randomized controlled trials, cohort studies, and cross-sectional assessments carried out in SSA communities. To promote the creation of context-specific guidelines that maximize the effectiveness of contraceptives and overall health outcomes in the area, the synthesis aims to identify important risk factors, clarify underlying mechanisms, and highlight information gaps.
Methodology
This scoping review systematically mapped and synthesized data on the pathophysiological effects of contraceptive use in SSA, focusing on contraceptive pathologies and their adverse effects. The review was retrospectively registered on the Open Science Framework (OSF) (registration number: 10.17605/OSF.IO/AMXSN). To guarantee methodological transparency, reproducibility, and thorough coverage of pertinent literature, the review complied with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR) standards.19
Search Strategy
From 2000 until August 12, 2025, a thorough and methodical search was conducted to identify pertinent studies. PubMed/MEDLINE, Wiley Online Library, and African Journals Online (AJOL) were among the electronic databases searched. Furthermore, regionally published research and grey literature that are not listed in major international databases were retrieved using Google Scholar. Medical Subject Headings (MeSH) and free-text keywords associated with SSA nations, physiological and pathophysiological impacts, and contraceptive techniques were incorporated in the search strategy. Combinations like “hormonal contraceptives”, “oral contraceptives”, “depot medroxyprogesterone acetate”, “levonorgestrel implant”, “injectable contraceptives”, or “copper IUD” AND (“lipid profile”, “dyslipidemia”, “blood pressure”, “glucose”, “anemia”, “cytokines”, or “bone mineral density”) AND (“Africa South of the Sahara” OR the names of specific SSA countries) were examples of search terms. Additional eligible papers were found by screening the reference lists of included research and pertinent reviews (Supplementary File S1).
Eligibility Criteria
Eligibility for inclusion in this scoping review encompassed studies conducted in Sub-Saharan Africa that investigated physiological changes associated with contraceptive use among reproductive-age (15–49 years) women and men, irrespective of comorbidities, HIV status, or parity. Studies were considered if they employed various designs, such as randomized controlled trials (RCTs), prospective and retrospective cohorts, cross-sectional analyses, and secondary data evaluations from DHS. The time frame for publication was restricted to studies from January 2000 up to July 2025 to ensure relevance to contemporary contraceptive methods and health contexts. Language restrictions were applied to include publications in English, reflecting the predominant languages in the region’s scientific literature.
Exposures of interest included hormonal contraceptives, such as COCs, progestin-only formulations, injectable progestins, subdermal implants, and hormonal IUDs, as well as non-hormonal copper IUDs, when assessing related physiological outcomes. Included studies were required to report quantitative measurements of physiological alterations linked to contraceptive use, encompassing metabolic indicators, hematological parameters, immunological endpoints, and other physiological metrics. Outcomes focused on changes in body composition, cardiovascular function, glucose and lipid metabolism, bone health, menstrual patterns, and infection susceptibility, provided they were directly attributable to contraceptive exposure. This information was collected using a data extraction sheet (Table S1 in the Supplementary File S2).
Study Selection
Duplicate records were found and eliminated once all search results were uploaded into the Zotero reference management program. Two reviewers independently carried out a two-stage screening procedure on the remaining records. In order to eliminate research that was unrelated, titles and abstracts were first assessed against the predetermined eligibility criteria. The second step involved retrieving and evaluating full-text versions of possibly pertinent publications for inclusion. Consensus was used to settle any disputes amongst reviewers, and a third reviewer served as an arbiter when agreement could not be reached. To illustrate the number of records found, vetted, eliminated with justification, and added to the final synthesis, a PRISMA flow diagram was created.
Results
The scoping review screened 392 articles from PubMed, 146 articles from AJOL, and 498 articles from Wiley Online Library. From these 1036 search results, 235 were duplicates, and 299 lacked the necessary information for a study on pathologies attributable to contraceptive use in SSA. Out of the remaining 502 articles, 438 articles could not be retrieved. Thus, a total of 51 articles were used to synthesize information in this review, including 33 relevant articles from PubMed, Wiley Online Library, Africa Journal Online (AJOL), and 18 studies obtained from grey literature at Google Scholar. No methodological issues required the exclusion of any related contraceptive pathology study from SSA. The 51 most relevant papers (Supplementary File S2) that served as the review’s source materials were chosen using these rigorous selection processes, which are summed up in the modified PRISMA-ScR model that is displayed in Figure 1.
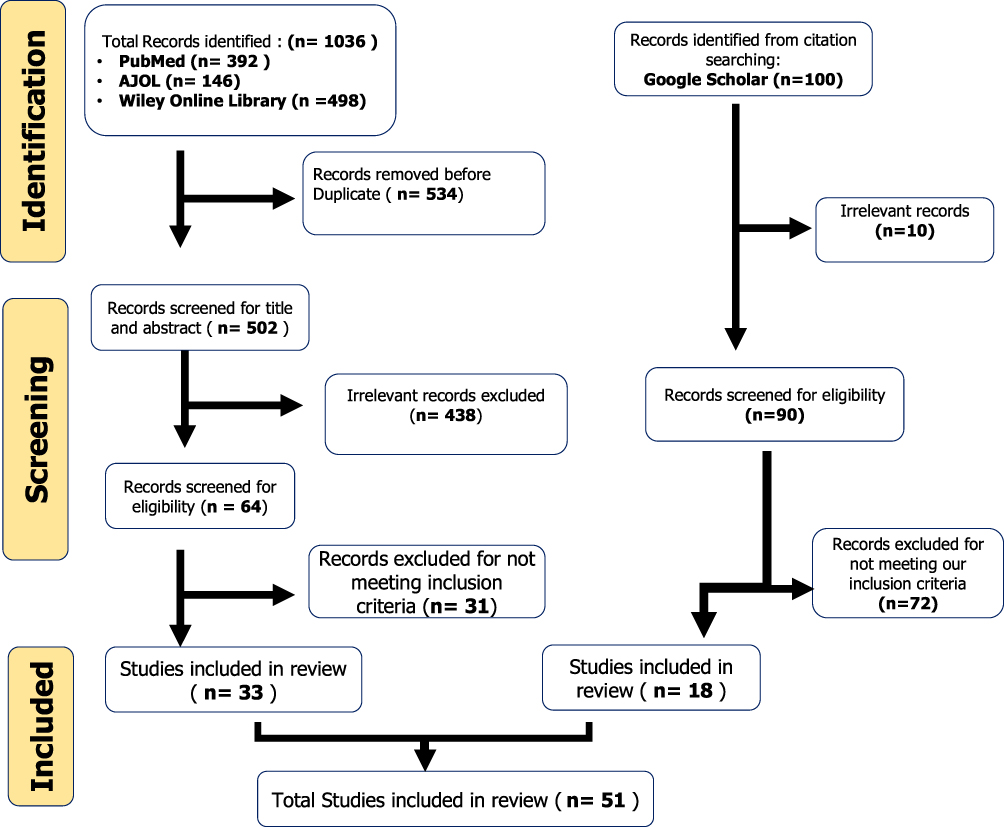 |
Figure 1 PRISMA flow chart of the article selection process. PRISMA-ScR flow chart illustrating the study selection process, including the number of records identified from databases, duplicates removed, records screened at title/abstract and full-text stages, exclusions with reasons, and the final number of studies included in the scoping review. Words or numbers are emboldened to indicate key indicators like databases used and the number of studies. |
Geographical Distribution of Studies Among the Sub-Saharan African Population
Fifty-one studies in all, from several Sub-Saharan African nations, satisfied the inclusion requirements. The most included studies were from South Africa (n=11), with Nigeria (n=8), Ethiopia (n=8), Rwanda (n=4), Uganda (n=4), Ghana (n=2), Zimbabwe (n=2), Tanzania (n=1), Cameroon (n=1), Malawi (n=1), and 9 were multi-country, including SSA data. The distribution is summarized in Figure 2.
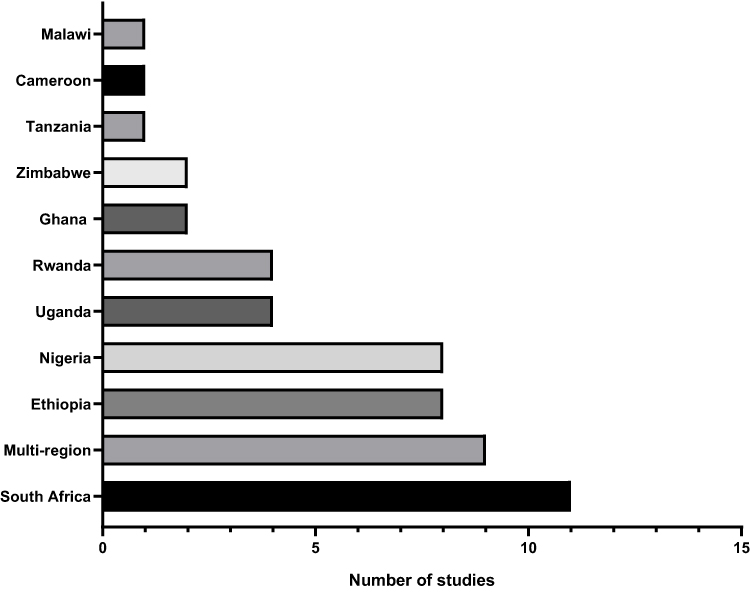 |
Figure 2 Distribution of studies among Sub-Saharan countries. Geographical distribution of included studies across Sub-Saharan African countries. |
Techniques Used to Determine Pathologies Linked to the Use of Contraceptives in SSA
Research on diseases linked to the use of contraceptives in Sub-Saharan Africa (SSA) used a wide range of methodological techniques, from RCTs to population-based cross-sectional analysis. Prominent RCTs that assessed HIV acquisition, immunological changes, STI risks, and overall contraceptive efficacy included the ASPIRE (A Study to Prevent Infection with a Ring for Extended Use), VOICE (Vaginal and Oral Interventions to Control the Epidemic), and ECHO trials, as well as several South African studies that examined DMPA and NET-EN. In South Africa, Rwanda, and Uganda, prospective and retrospective cohort studies were frequently used to investigate outcomes such as the progression of HIV illness, loss of bone density, and cardiometabolic hazards, including changes in the metabolism of glucose and lipids among contraceptive users. Laboratory and immunological analyses, especially in South Africa and Zimbabwe, provided mechanistic insights into host-pathogen interactions during exposure to HCs. These analyses included cytokine assays, vaginal microbiota profiling, and evaluations of immunological markers. Lastly, secondary analyses of sizable datasets, such as multi-country DHS and supplementary studies from clinical trials, offered more comprehensive epidemiological viewpoints on the safety and adverse effects of contraceptives throughout SSA.
Pathophysiological Consequences of Hormonal Contraceptives in SSA
Several pathophysiological consequences of using HCs have been reported in SSA. However, most studies showed that cardiovascular and metabolic risks are the most common, followed by hematological changes and other risks related to sexually transmitted diseases, as shown in Table 1.
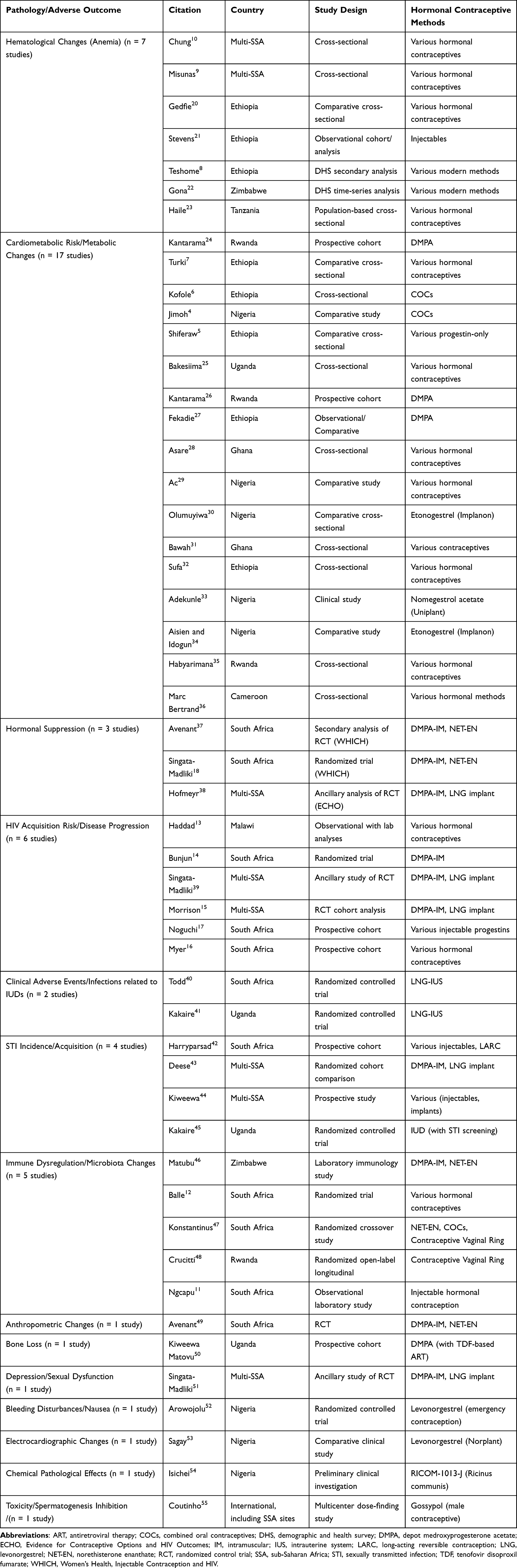 |
Table 1 Pathophysiological Outcomes Associated with Hormonal Contraceptives Across SSA |
Cardiometabolic Risk and Metabolic Changes
The effect of HCs on cardiometabolic health has been the subject of seventeen studies carried out throughout SSA, with consistent evidence of changes in weight, cholesterol levels, and metabolic risk indicators. According to Kantarama and others, DMPA was associated with increases in BMI and fasting glucose among long-term users in Rwanda.24 Another cross-sectional study from Rwanda also found that women using HCs had abnormal lipid profiles, including elevated levels of total cholesterol and LDL.35 A significant correlation between the usage of HCs and metabolic syndrome characteristics, such as central obesity, hypertension, and dyslipidemia, was also reported in Cameroon, underscoring the systemic metabolic burden.36
Ethiopian data add credence to these patterns. Showed that people who used progestin-only contraceptives had worse lipid profiles and higher blood pressure than people who did not use them.5 Similarly, a cross-sectional study showed a greater incidence of dyslipidemia among users, and verified that using OCs together was linked to increased atherogenic risk ratios.6,7 It also identified high rates of dyslipidemia among HCs users in Harar, Eastern Ethiopia,32 and a previous study showed significant increases in triglycerides and LDL with continued DMPA use.27
Similar cardiometabolic risks were shown in Nigeria by some comparative investigations. Users of COCs were more likely than non-users to develop atherogenic dyslipidemia.4 The increased cholesterol fractions in users of HCs were also found,29 but negative lipid alterations in users of etonogestrel implants.30 A previous clinical trial showed increases in cholesterol and triglycerides with nomegestrol acetate subdermal implants.33 However, Implanon users had adverse changes in serum lipoproteins.34
Ghanaian data also support metabolic impacts, highlighting comparable trends, demonstrating higher LDL and triglycerides across various contraceptive forms, and it was found a substantial increase in cardiovascular risk indices and total cholesterol was found among HC users.28,31 A regional pattern of lipid abnormalities linked to hormonal treatments was further supported by a report on dyslipidemias in women taking HCs in Uganda.3
Put together, these results show that the use of HCs in SSA is regularly linked to changes in lipid metabolism, elevated cardiovascular risk indicators, and occasionally more general metabolic syndrome characteristics.
Hematological Changes (Anemia)
The use of HCs and anemia status among women of reproductive age are consistently linked, according to data from national and multi-country studies conducted in SSA, as reported by seven included studies. Current HC users were considerably less likely to be anemic than non-users, indicating a protective link, according to a recent large-scale analysis employing 46 DHS throughout SSA.10 Likewise, it was found that the use of HCs was associated with a lower prevalence of moderate-to-severe anemia, especially among women who used injectable formulations, in a multi-country investigation spanning low- and middle-income nations, including SSA.9
Studies conducted at the national level supported similar conclusions. In a comparative cross-sectional study conducted in Ethiopia, researchers discovered that women who used HCs had considerably higher hemoglobin levels and lower rates of anemia than those who did not.20 While secondary DHS data showed that the use of modern contraceptives was independently associated with lower odds of anemia in Ethiopian women.8 On the other hand, consistent results were observed in an observational analysis that contraceptive users exhibited improved hematological profiles.21
Similarly, a time-series framework was used to evaluate DHS data from Zimbabwe and verified a decrease in the prevalence of anemia among women using HCs, indicating a long-term population-level benefit.22 A population-based study conducted in Tanzania also found that women who had previously used HCs had lower incidences of anemia and better iron status than those who had not.23
When combined, these results from national studies in Ethiopia, Zimbabwe, and Tanzania, as well as multi-country datasets, show that using HCs, especially injectable ones, is linked to better hematological status and a lower risk of anemia in SSA women who are of reproductive age.
Endocrine and Hormonal Suppression
Three studies found that the HCs have quantifiable effects on endocrine function, specifically ovarian suppression, according to data from SSA. Based on a secondary study of the Women’s Health, Injectable Contraception and HIV (WHICH) randomized trial conducted in South Africa, women who used injectable progestins showed higher suppression of progesterone and estradiol than those who were assigned to non-hormonal treatments.37 Similarly, from the WHICH study, DMPA users showed significant decreases in endogenous gonadotropins and ovarian activity, indicating robust hypothalamic-pituitary-ovarian axis suppression.18 Similar suppression patterns were observed throughout SSA sites, according to complementary data from the ECHO trial,38 which reported consistent drops in ovarian hormone levels among women randomly assigned to injectable or implantable progestin treatments.
Immune Dysregulation and Microbiota Changes
Five investigations in SSA have looked at how hormonal contraceptives affect the vaginal microbiota and immune system. Through laboratory-based immunological assays, it was shown that DMPA use in Zimbabwe was linked to changes in cytokine expression, indicating a shift toward a pro-inflammatory immune milieu that may affect host susceptibility to infections.46 In a randomized experiment conducted in South Africa, demonstrated that the start of DMPA was associated with notable alterations in immunological markers of the genital tract, including decreased levels of protective innate immune mediators.12 Additionally, utilizing a randomized crossover approach, it has been proven that several HCs elicited unique patterns of mucosal cytokine responses and immunological activation, suggesting method-specific immunomodulatory effects.47
Variations in the vaginal microbiome have also been reported, in addition to immunological markers. In a randomized, open-label longitudinal trial conducted in Rwanda, researchers discovered that the use of contraceptive vaginal rings led to a relative increase in Lactobacillus species in a population where bacterial vaginosis was highly prevalent.48 This finding suggests that there may be a beneficial microbial shift at play. In contrast, an observational laboratory study conducted in South Africa found that the use of injectable HCs was linked to lower levels of innate immune factors and soluble chemotactic cytokines in the lower female genital tract, which may compromise mucosal immunity.11
Together, our results show that HC techniques might affect vaginal microbial ecology and mucosal immune responses. Injectable formulations tend to inhibit protective immune mediators, while vaginal rings may promote advantageous microbiota profiles.
Sexually Transmitted Infections (STIs) Acquisition Risk and Disease Progression
The impact of HCs use on HIV susceptibility or progression in SSA was investigated by ten studies in several extensive trials and cohort studies. DMPA-IM usage was linked to higher indicators of HIV target cell activation in Malawi; it was also integrated with clinical follow-up with laboratory immunological investigations.13 However, total acquisition risk did not change significantly between users and non-users. A randomized experiment conducted in South Africa showed that progestin-only injection users did not significantly increase their risk of contracting HIV in comparison to copper IUD users.14 These results were validated by additional data from the ancillary investigations of the ECHO trial, in the full ECHO cohort analysis across multiple SSA countries, which found no significant difference in HIV incidence among the three methods studied,15 while reporting no elevated acquisition risk across DMPA, levonorgestrel implant, and copper IUD arms.51 Previous prospective cohort data indicated potential risk elevations observed comparable relationships in a Cape Town cohort,16 while higher HIV-1 acquisition was observed among South African women using injectable progestins.17
On the other hand, Research on the acquisition of non-HIV STIs has yielded inconsistent findings for various forms of contraception. According to a prospective cohort study conducted in South Africa, women who used DMPA had greater incidence rates of Neisseria gonorrhoeae and Chlamydia trachomatis infections than non-users.42 These trends were further supported by data from ECHO-related studies: In several SSA nations, researchers discovered that users of HCs were more likely to acquire specific STIs than users of copper IUDs.43 It has also been reported that a higher rate of STIs among high-risk women starting different HCs in a larger prospective cohort that included several SSA locations.44 On the other hand, a randomized trial conducted in Uganda revealed that, in contrast to conventional care, intrauterine contraception implantation did not significantly raise STI risk, indicating method-specific variations.41
Weight, Body Mass Index, and Anthropometric Alterations
The only available data on anthropometric results came from secondary analysis of randomized trials reported from the WHICH randomized trial in South Africa, which showed a measurable correlation between injectable contraceptive use and weight gain.49 They found that women who were randomly assigned to DMPA-IM had significantly higher increases in BMI and weight over follow-up compared to those who used copper IUDs.
Bone Loss and Bone Mineral Density
Long-term use of injectable progestins may have a detrimental effect on bone health, according to one study from East Africa. A prospective cohort study conducted in Uganda showed that, in comparison to non-users, women who used DMPA showed a gradual decrease in bone mineral density in the hip and lumbar spine, with the effects being more noticeable in younger women and those who had been using the drug for a longer period.50
Sexual Dysfunction and Depression
A large randomized trial was analyzed in an additional way to assess the effects on sexual and psychological health. Although there were only slight absolute differences between the groups, women who were randomly assigned to receive an LNG implant or DMPA reported higher rates of sexual dysfunction and depressive symptoms than those who used copper IUDs.39
Nausea and Bleeding Disturbances
A randomized controlled study in Nigeria to assess levonorgestrel regimens for emergency contraception.52 They found that menstrual irregularities, such as nausea and intermenstrual bleeding, were common side effects, but they were usually temporary and self-limiting.
Changes in Electrocardiograms
Small clinical trials have indicated cardiac conduction effects. Although no significant clinical cardiac problems were reported, Sagay found that Norplant implant users in Nigeria had electrocardiographic changes, including T-wave variations, as compared to controls.53
Effects of Chemical Pathology
According to preliminary biochemical data from Nigeria, using contraceptives may cause systemic metabolic changes. Although the study was constrained by a small sample size, it examined RICOM-1013-J, a plant-derived contraceptive candidate, and revealed chemical pathological abnormalities in female volunteers, including changes in liver enzymes and hematological markers.54
Inhibition of Spermatogenesis and Toxicity
Coutinho and others evaluated gossypol as a male contraceptive at the multicenter level in foreign locations, including SSA.55 They found that gossypol blood levels increased in tandem with a dose-dependent reduction of spermatogenesis. Fatigue, hypokalemia, and, in certain situations, irreversible reproductive reduction were among the side effects.
IUD-Related Clinical Adverse Events and Infections
Two studies investigate the differential risks of infections and adverse effects on intrauterine contraception in SSA. A study done by Todd and others examined the safety profile of the levonorgestrel-releasing intrauterine system (LNG-IUS) in South Africa by comparing it to copper IUDs among women with HIV.40 They found no discernible rise in pelvic infections. The acceptability and tolerability of hormonal IUDs in this population were further supported by Kakaire, who conducted a randomized controlled trial among women with HIV in Uganda and found no increased risk of clinical infections after LNG-IUS insertion in comparison to standard copper IUD users.41
Discussion
Key Findings and Comparisons with Existing Literature
This scoping review synthesizes evidence from Sub-Saharan Africa (SSA) on the physiological and pathological effects of HCs, encompassing hematological alterations, cardiometabolic impacts, endocrine suppression, HIV/STI risks, and diverse adverse clinical outcomes. Across the 51 included studies, HCs demonstrated consistent associations with endocrine suppression, hematological benefits in anemia reduction alongside context-specific risks, and metabolic disturbances such as dyslipidemia, elevated cardiovascular indices, and weight gain. Evidence on infectious outcomes remained heterogeneous, with prospective cohorts suggesting potential HIV and STI vulnerabilities, though large randomized trials, such as the ECHO trial, reported no significant elevation in HIV acquisition risk with progestin-only injectables compared to non-hormonal methods.15 Additional adverse effects identified included bone mineral density loss, mood disturbances, sexual dysfunction, bleeding irregularities, and, less commonly, biochemical and electrocardiographic changes. Of particular note, LNG-IUS demonstrated robust safety profiles among HIV-positive women in African cohorts, underscoring their potential as a viable contraceptive option in this population.40,41
The modification of endometrial physiology by progestin and estrogen explains the continuous decrease in anemia risk among hormonal contraception users in SSA.10,23 By suppressing estrogen receptor expression and preventing angiogenesis in the endometrium, progestins like DMPA cause the endometrium’s estrogen and progesterone receptors to be downregulated with long-term exposure.56 This leads to decreased glandular atrophy and cellular proliferation, resulting in thinner endometrial tissue and less monthly bleeding.57 Additionally, by suppressing matrix metalloproteinases (MMPs) and upregulating vascular endothelial growth factor (VEGF) inhibitors, estrogen components in combined oral contraceptives stabilize endometrial vessels and reduce breakthrough bleeding. Reduced menstrual blood loss helps preserve iron stores throughout the body, maintaining hepatic ferritin levels and supporting effective erythropoiesis.58 Trials showing improved hemoglobin and ferritin levels with LNG-IUS compared to copper IUDs support this, aligning with the SSA data.59
Steroid hormones regulate peripheral glucose absorption and hepatic lipid metabolism, leading to the metabolic changes observed in African cohorts.25,26,28 Hepatic androgen and progesterone receptors are activated by progestins with androgenic activity, which increases the secretion of very-low-density lipoprotein (VLDL) and suppresses lipoprotein lipase (LPL) activity, resulting in lower HDL and higher triglycerides.60 In contrast, estrogens increase HDL by stimulating hepatic apolipoprotein A1 synthesis, but they also promote triglyceride production through hepatic lipogenesis.61 Weight gain associated with DMPA use, especially in teenagers, has been confirmed by longitudinal studies in the US and Europe.62 Notably, more favorable lipid profiles are linked to newer hormonal delivery methods like LNG-IUS and the vaginal ring (NuvaRing®), suggesting that technology choice can help reduce metabolic risk.63
Progestins in adipose tissue decrease insulin sensitivity by reducing GLUT4 translocation in skeletal muscle and boost hunger through hypothalamic neuropeptide Y (NPY) signaling. These effects promote the accumulation of visceral fat, which appears as weight gain. This is especially evident with DMPA use.62 By increasing endothelial nitric oxide (NO) production, estrogen provides some vasculoprotective benefits; however, the overall impact depends on the estrogen-progestin combination. Newer methods, such as the vaginal ring and LNG-IUS, have more favorable lipid profiles because they involve lower systemic steroid exposure.64
Additionally, our study found evidence that genital immune regulation is linked to hormonal contraceptives.12,46 Progestins like DMPA suppress pro-inflammatory cytokines like IL-1β and TNF-α and reduce the secretion of protective innate immune factors like secretory leukocyte protease inhibitor (SLPI) by acting on glucocorticoid receptors expressed in cervical and vaginal epithelial cells.11 This increases vulnerability to HIV and other STIs by causing a mucosal condition that is hypo-inflammatory but immunocompromised. Contrariwise, Lactobacillus species, which generate lactic acid and keep the vaginal pH low, boost colonization with contraceptive vaginal rings, creating a protective microbial environment.48 Therefore, whether the net mucosal effect is protective or permissive to infection depends on the type of contraception.
Mucosal immunology provides a scientific explanation for the variation found in African studies on HIV risk and hormonal contraception use. Progestins like DMPA work by partially agonizing glucocorticoid receptors present in cervical and vaginal epithelial cells in addition to progesterone receptors.65 This signaling pathway decreases the production of antimicrobial peptides like defensins and secretory leukocyte protease inhibitor (SLPI) by the epithelium and inhibits the transcription of pro-inflammatory cytokines like IL-1β, TNF-α, and IL-6.11 Due to a decrease in tight-junction proteins such as occludin and claudin, the epithelial barrier integrity is compromised at the cellular level, making it easier for viruses to infiltrate.66
Additionally, DMPA promotes the recruitment of HIV target cells by increasing dendritic cell activation and cervical CD4+ T cell CCR5 expression, which expands the virus’s cellular entry locations.67 The vaginal milieu is shifted toward higher pH and increased mucosal inflammation due to altered vaginal microbiota, particularly decreased colonization of Lactobacillus crispatus and increased anaerobic bacteria like Gardnerella vaginalis. This further predisposes the vagina to HIV and STI acquisition.12,48
In contrast, delivery systems like vaginal rings and LNG-IUS reduce systemic progestin exposure, maintaining local contraceptive efficacy while preserving mucosal immune defense.68,69 This mechanistic difference explains why SSA findings with systemic injectables differ from those with locally acting methods.
According to recognized endocrine physiology, Ugandan women who used DMPA experienced a reduction in bone mineral density.44 Reduced luteinizing hormone (LH) and follicle-stimulating hormone (FSH) secretion from the pituitary results from DMPA’s suppression of pulsatile gonadotropin-releasing hormone (GnRH) release from the hypothalamus.64 Ovarian suppression and a significant drop in circulating estradiol, a crucial modulator of skeletal homeostasis, are the outcomes of this.
At the cellular level, osteoprotegerin (OPG), the natural decoy receptor that prevents osteoclastogenesis, is decreased when estrogen deprivation increases osteoclast development through activation of the RANK-RANKL-NFATc1 signaling cascade.70 This imbalance accelerates bone resorption. Estrogen often increases osteoblast survival and type I collagen synthesis simultaneously; when it is suppressed, bone formation rates are reduced.71
This suppression is particularly detrimental to young women and teenagers who are still gaining their peak bone mass. According to DEXA-based longitudinal studies conducted outside of SSA, DMPA causes a 2–3% annual loss of bone.72 Crucially, following cessation, there is a partial recovery as bone remodeling rebalances and estrogen levels return to baseline.73 When giving DMPA to younger women or those with a baseline risk of osteoporosis, the WHO advises carefully weighing the risks and benefits. These mechanisms support this approach.
Broader neuroendocrine pathways are in line with SSA findings of higher sexual dysfunction and depressive symptoms among DMPA and implant users.51 Progestins easily penetrate the blood-brain barrier and alter neurosteroid pathways, especially when they are converted into metabolites like allopregnanolone, which function as GABA-A receptor positive allosteric modulators.74 Chronic exposure may desensitize GABA-A receptors, resulting in dysregulated inhibitory tone and depressed phenotypes, even though this usually has anxiolytic effects.75
Additionally, via lowering tryptophan hydroxylase expression and serotonin transporter regulation in the dorsal raphe nuclei, progestin-induced hypoestrogenism decreases serotonergic activity.76 As a result, there is less synaptic serotonin available, which is a known route in mood disorders. Because synthetic progestins have partial glucocorticoid action, which amplifies cortisol signaling and increases susceptibility to stress-related depression, the hypothalamic-pituitary-adrenal (HPA) axis may also be dysregulated.77
The mechanisms underlying sexual dysfunction are similarly obvious. Nitric oxide synthase activity in the genital vasculature is decreased by ovarian estradiol and testosterone suppression, which affects lubrication and arousal as well as clitoral and vaginal blood flow.78 Sexual desire is further reduced by lower central dopamine signaling, which is often boosted by estrogen.79 According to SSA and Western cohort data, women on DMPA or implants frequently experience decreased libido and impaired sexual pleasure, which can be explained by these physiological changes.80 Progestin-induced endometrial alterations are the cause of bleeding disorders observed in SSA.52 Endometrial gland atrophy and stromal decidualization brought on by prolonged progestin exposure upset the angiogenic equilibrium. Progestins decrease vascular stabilizers, including vascular endothelial growth factor (VEGF) and angiopoietin-1, while increasing matrix metalloproteinases (MMP-2, MMP-9) that break down the extracellular matrix surrounding endometrial arteries.81 The outcome is fragile, superficial arteries prone to breakthrough bleeding, a leading cause of contraceptive cessation globally.82
Progestin-mediated modification of cardiac ion channel expression may explain the electrocardiographic (ECG) changes observed among Norplant users in Nigeria.53 Some women experience longer QT intervals as a result of progesterone and its analogs’ alteration of HERG potassium channel function.83 Progestins also decrease circulating estrogen, which typically increases vasodilation through nitric oxide. This might cause autonomic balance to shift toward sympathetic dominance, which can lead to arrhythmic tendencies.84
Progestins’ actions on the control of hepatic enzymes are probably the cause of the biochemical changes documented in early Nigerian research.54 Through androgenic or glucocorticoid cross-talk at hepatic nuclear receptors, synthetic progestins raise hepatic lipase activity and may change the production of albumin and globulins.85 Reports of changed liver enzymes and protein profiles in chronic users can be explained by these systemic metabolic changes.
Lastly, the local immunological tolerance of the uterus is reflected in the low incidence of IUD-related infections in SSA, provided appropriate screening and asepsis are maintained.40,41 By thickening cervical mucus, the LNG-IUS lowers the chance of ascending infection, while copper ions generated from Cu-IUDs have bacteriostatic effects.86 Collectively, these processes account for the widely held conclusion that, when used sterilely, contemporary IUDs pose very little danger of long-term infection.
Recommendations for Assessing Pathologies Related to Contraceptives Among SSA
The results highlight the need for more methodologically sound, context-specific research in SSA to elucidate the relationships between the usage of HCs and a variety of diseases. First, to remove the dependence on cross-sectional surveys, longitudinal cohort designs with defined laboratory endpoints (such as hemoglobin, bone mineral density, lipid subfractions, insulin resistance indicators, and inflammatory cytokines) are required. Second, emphasis should be placed on integrating biomarker-driven monitoring, such as enhanced flow cytometry for immunological phenotyping, continuous glucose monitoring (CGM) for metabolic risk, and dual-energy X-ray absorptiometry (DXA) for bone health. Third, more representative insights may be obtained through multi-country partnerships that use the DHS with biomarker modules integrated. Adolescents and rural people, who are still underrepresented but extremely susceptible to negative consequences, should also be included in studies.
Clinical Implications
Clinicians in SSA have to weigh the potential skeletal, cardiometabolic, and hematological side effects of treatments such as DMPA against their high contraceptive efficacy and accessibility. Family planning programs should include routine screening for anemia, lipid abnormalities, and weight changes, especially for women who already have prior vulnerabilities like HIV infection or malnutrition. Long-term DMPA users may benefit from bone health monitoring, which includes nutritional counseling and vitamin D/calcium supplements. Importantly, if the use of HCs overlaps with an increased risk of HIV acquisition, HIV risk reduction methods, such as dual protection with condoms and pre-exposure prophylaxis (PrEP), should be heavily emphasized. Individualized contraceptive counseling should be taken into account in clinical recommendations, along with patient comorbidities, reproductive goals, and follow-up care accessibility.
Study Limitations
This scoping review encounters several limitations affecting its scope and applicability. Variability in study designs, demographics, and outcome measures hinders direct comparability across the 51 included studies, despite broad database coverage, with many relying on cross-sectional or secondary DHS analyses that limit causal inference due to recall and selection bias. Geographically, the evidence is skewed toward South Africa, Ethiopia, and Nigeria, with Central Africa underrepresented, potentially limiting regional generalizability. Additionally, small sample sizes and short follow-up periods in several studies obscure long-term pathophysiological effects. As a scoping review focused on mapping evidence rather than appraising quality,87,88 no meta-analysis or formal risk-of-bias assessment was conducted, and findings should be interpreted as evidence synthesis rather than definitive effect size estimates.
Conclusion
A wide range of diseases, including hematological disorders, cardiometabolic abnormalities, changes in bone mineral density, and vulnerability to HIV and other infections, are associated with the use of HCs in SSA, according to this scoping review. Contraceptives remain essential for both public health and reproductive autonomy, but it is important to consider their systemic effects. SSA evidence suggests that region-specific conditions such as anemia, HIV prevalence, and nutritional deficiencies may influence the likelihood of adverse outcomes. Future efforts should focus on enhancing research infrastructure for mechanistic and longitudinal studies, integrating contraceptive services with comprehensive health monitoring, and providing tailored, evidence-based guidance to improve women’s health outcomes. By contextualizing international research within local settings, SSA can move closer to offering safe, equitable, and sustainable contraceptive care.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no financial support was received for the research.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Mankelkl G, Kinfe B. Pooled prevalence of modern contraceptive utilization and its associated factors among reproductive age women in East Africa: derived from demographic and health surveys. J Health Popul Nutr. 2025;44(1):261. doi:10.1186/s41043-025-01019-6
2. Demissie KA, Jejaw M, Teshale G, Tiruneh MG, Tafere TZ, Hagos A. Multinomial multilevel analysis of factors affecting the use of modern contraceptives in sub-Saharan Africa: evidence from 2015 to 2023 demographic health survey. Sci Rep. 2025;15(1):16751. doi:10.1038/s41598-025-01622-x
3. Bakesiima R, Beyeza-Kashesya J, Tumwine JK, et al. Effect of peer counselling on acceptance of modern contraceptives among female refugee adolescents in northern Uganda: a randomised controlled trial. PLoS One. 2021;16(9):e0256479. doi:10.1371/journal.pone.0256479
4. Jimoh O, Abdul I, Balogun O, et al. Atherogenic and cardiovascular risks of women on combined oral contraceptives: a comparative study. Niger J Clin Pract. 2021;24(12):1759–1765. doi:10.4103/njcp.njcp_431_20
5. Shiferaw M, Kassahun W, Zawdie B. Anthropometric indices, blood pressure, and lipid profile status among women using progestin-only contraceptives: comparative cross-sectional study. BMC Womens Health. 2021;21(1):34. doi:10.1186/s12905-021-01178-8
6. Kofole Z, Haile D, Solomon Y. Fasting blood glucose, blood pressure and body mass index among combined oral contraceptive users in Chencha town Southern Ethiopia, 2019. Front Glob Womens Health. 2023;4:992750. doi:10.3389/fgwh.2023.992750
7. Turki A, Ayalew A, Mossie A, Mitiku S. Effects of hormonal contraceptives on lipid profile among women attending family planning unit in Goba Town Public Health Facilities, Bale, Southeast Ethiopia: a comparative cross-sectional study. Reprod Health. 2023;20(1):185. doi:10.1186/s12978-023-01727-4
8. Teshome AA, Berra WG, Hiruy AF. Modern contraceptive methods predict hemoglobin levels among women of childbearing age from DHS 2016. OAJC. 2022;13:1–8. doi:10.2147/OAJC.S329045
9. Misunas C, Hindin MJ, Phillips-Howard PA, Sommer M. The association between hormonal contraceptive use and anemia among adolescent girls and young women: an analysis of data from 51 low- and middle-income countries. J Adolesc Health. 2024;74(3):563–572. doi:10.1016/j.jadohealth.2023.09.013
10. Chung SR, Spain MX, Hoppes E, Mackenzie A. Estimating the effect of hormonal contraceptive use on anemia: a cross-sectional comparative analysis of 46 demographic and health surveys. PLoS One. 2025;20(7):e0327083. doi:10.1371/journal.pone.0327083
11. Ngcapu S, Masson L, Sibeko S, et al. Lower concentrations of chemotactic cytokines and soluble innate factors in the lower female genital tract associated with the use of injectable hormonal contraceptive. J Reprod Immunol. 2015;110:14–21. doi:10.1016/j.jri.2015.03.007
12. Balle C, Konstantinus IN, Jaumdally SZ, et al. Hormonal contraception alters vaginal microbiota and cytokines in South African adolescents in a randomized trial. Nat Commun. 2020;11(1):5578. doi:10.1038/s41467-020-19382-9
13. Haddad LB, Tang JH, Davis NL, et al. Influence of hormonal contraceptive use and HIV on cervicovaginal cytokines and microbiota in Malawi. mSphere. 2023;8(1):e00585–22. doi:10.1128/msphere.00585-22
14. Bunjun R, Ramla TF, Jaumdally SZ, et al. Initiating intramuscular depot medroxyprogesterone acetate increases frequencies of Th17-like human immunodeficiency virus target cells in the genital tract of women in South Africa: a randomized trial. Clinl Infect Dis. 2022;75(11):2000–2011. doi:10.1093/cid/ciac284
15. Morrison CS, Hofmeyr GJ, Thomas KK, et al. Effects of depot medroxyprogesterone acetate, copper intrauterine devices, and levonorgestrel implants on early HIV disease progression. AIDS Res Hum Retroviruses. 2020;36(8):632–640. doi:10.1089/aid.2020.0015
16. Myer L, Denny L, Wright TC, Kuhn L. Prospective study of hormonal contraception and women’s risk of HIV infection in South Africa. Int J Epidemiol. 2007;36(1):166–174. doi:10.1093/ije/dyl251
17. Noguchi LM, Richardson BA, Baeten JM, et al. Risk of HIV-1 acquisition among women who use different types of injectable progestin contraception in South Africa: a prospective cohort study. Lancet HIV. 2015;2(7):e279–e287. doi:10.1016/S2352-3018(15)00058-2
18. Singata-Madliki M, Smit J, Beksinska M, et al. Effects of injectable contraception with depot medroxyprogesterone acetate or norethisterone enanthate on estradiol levels and menstrual, psychological and behavioral measures relevant to HIV risk: the WHICH randomized trial. PLoS One. 2024;19(3):e0295764. doi:10.1371/journal.pone.0295764
19. Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
20. Gedfie S, Getawa S, Kassahun W, Gashaye KT, Melku M. Hematological parameters of reproductive-age women using hormonal contraceptives at University of Gondar Comprehensive Specialized Referral Hospital, Northwest Ethiopia: a comparative cross-sectional study. PLoS One. 2022;17(11):e0277254. doi:10.1371/journal.pone.0277254
21. Stevens R, Malbos B, Gurmu E, Riou J, Alvergne A. Anemic women are more at risk of injectable contraceptive discontinuation due to side effects in Ethiopia. Stud Fam Plann. 2022;53(1):193–208. doi:10.1111/sifp.12186
22. Gona PN, Gona CM, Chikwasha V, Haruzivishe C, Mapoma CC, Rao SR. Intersection of HIV and Anemia in women of reproductive age: a 10-year analysis of three Zimbabwe demographic health surveys, 2005–2015. BMC Public Health. 2021;21(1):41. doi:10.1186/s12889-020-10033-8
23. Haile ZT, Kingori C, Teweldeberhan AK, Chavan B. The relationship between history of hormonal contraceptive use and iron status among women in Tanzania: a population-based study. Sex Reproduct Healthcare. 2017;13:97–102. doi:10.1016/j.srhc.2017.07.003
24. Kantarama E, Uwizeye D, Uwineza A. Cardiometabolic risk marker changes in centrally obese women using Depot Medroxyprogesterone Acetate (DMPA) in Kigali, Rwanda. Rwanda J Med Health Sci. 2025;8(1):17–29. doi:10.4314/rjmhs.v8i1.2
25. Bakesiima R, Byakika-Kibwika P, Tumwine JK, et al. Dyslipidaemias in women using hormonal contraceptives: a cross-sectional study in Mulago Hospital Family Planning Clinic, Kampala, Uganda. BMJ Open. 2018;8(10):e022338. doi:10.1136/bmjopen-2018-022338
26. Kantarama E, Uwizeye D, Uwineza A, Muvunnyi CM. Effect of depot medroxyprogesterone acetate on cardiometabolic risk factors among women of reproductive age in Rwanda: a prospective cohort study. IJMS. 2023;76:28–35. doi:10.25259/IJMS_205_2022
27. Fekadie M, Seifu D, Kumpi S, Kokeb A. Effect of Depo-medroxyprogesterone acetate (DMPA) on Lipid Metabolism. Int J Res Biotechnol Biochem. 2016;6(1):6–11.
28. Asare G, Santa S, Ngala R, Asiedu B, Afriyie D, Amoah A. Effect of hormonal contraceptives on lipid profile and the risk indices for cardiovascular disease in a Ghanaian community. IJWH. 2014;2014:597. doi:10.2147/ijwh.s59852
29. Ac M, Mo F, Mbakwem A. Lipid profile of Nigerian women using hormonal contraceptives. J Clin Sci. 2003;3(2):16–20.
30. Olumuyiwa R, Adeyemi A, Adeniran F, Michael O, Olatubosun A. The effects of etonorgestrel implant (ImplanonR) on the lipid profile of Nigerian women. Trop J Obstet Gynaecol. 2018;35(2):165. doi:10.4103/tjog.tjog_43_17
31. Bawah AT, Boateng MA, Kuffour FAO, Seini MM, Amoah P, Alidu H. Lipid profile and cardiovascular risk indices of women on various types of contraceptives in the Ho Municipality of Ghana. Int J Reprod Contracept Obstet Gynecol. 2018;7(11):4342. doi:10.18203/2320-1770.ijrcog20184475
32. Sufa B, Abebe G, Cheneke W. Dyslipidemia and associated factors among women using hormonal contraceptives in Harar town, Eastern Ethiopia. BMC Res Notes. 2019;12(1):120. doi:10.1186/s13104-019-4148-9
33. Adekunle AO, Fakokunde AF, Arowojolu AO, Ladipo OA. The effects of nomegestrol acetate subdermal implant (Uniplant®) on serum cholesterol, triglycerides, and lipoproteins in Nigerian users. Contraception. 2000;61(2):139–144. doi:10.1016/s0010-7824(00)00088-3
34. Aisien A, Idogun S. Effect of Implanon (etonogestrel) implant on serum lipids and lipoproteins. Trop J Obstet Gynaecol. 2016;33(3):257. doi:10.4103/0189-5117.199812
35. Habyarimana T, Yadufashije C, Mukantwali V, et al. Association between hormonal contraceptive use and derangement of lipid profile among women attending Muhoza Health Center, Rwanda. Sahel Med J. 2022;25(2):47–51. doi:10.4103/smj.smj_70_20
36. Marc Bertrand DS, Donald Séverin DB, Floraise Lynda T, François ZN. Metabolic syndrome and related factors in Cameroonian women under contraceptive use. PLoS One. 2024;19(11):e0309054. doi:10.1371/journal.pone.0309054
37. Avenant C, Singata-Madliki M, Bick AJ, et al. The injectable contraceptives depot medroxyprogesterone acetate and norethisterone enanthate substantially and differentially decrease testosterone and sex hormone binding globulin levels: a secondary study from the WHICH randomized clinical trial. PLoS One. 2024;19(8):e0307736. doi:10.1371/journal.pone.0307736
38. Hofmeyr GJ, Singata-Madliki M, Batting J, Balakrishna Y, Morroni C. Effects of depot medroxyprogesterone acetate, the copper IUD and the levonorgestrel implant on testosterone, sex hormone binding globulin and free testosterone levels: ancillary study of the ECHO randomized clinical trial. BMC Womens Health. 2024;24(1):167. doi:10.1186/s12905-024-02990-8
39. Singata-Madliki M, Lawrie TA, Balakrishna Y, d’Hellencourt FCL, Hofmeyr GJ. Behavioral effects of different contraceptive methods and HIV acquisition: an ancillary study of the ECHO randomized trial. Reprod Health. 2021;18(1):192. doi:10.1186/s12978-021-01232-6
40. Todd CS, Jones HE, Langwenya N, et al. Safety and continued use of the levonorgestrel intrauterine system as compared with the copper intrauterine device among women living with HIV in South Africa: a randomized controlled trial. PLoS Med. 2020;17(5):e1003110. doi:10.1371/journal.pmed.1003110
41. Kakaire O, Byamugisha JK, Tumwesigye NM, Gemzell-Danielsson K. Clinical versus laboratory screening for sexually transmitted infections prior to insertion of intrauterine contraception among women living with HIV/AIDS: a randomized controlled trial. Hum Reprod. 2015;30(7):1573–1579. doi:10.1093/humrep/dev109
42. Harryparsad R, Meyer B, Taku O, et al. Prevalence and incidence of sexually transmitted infections among South African women initiating injectable and long-acting contraceptives. PLoS One. 2023;18(11):e0294285. doi:10.1371/journal.pone.0294285
43. Deese J, Philip N, Lind M, et al. Sexually transmitted infections among women randomised to depot medroxyprogesterone acetate, a copper intrauterine device or a levonorgestrel implant. Sex Transm Infect. 2021;97(4):249–255. doi:10.1136/sextrans-2020-054590
44. Kiweewa FM, Brown E, Mishra A, et al. Acquisition of sexually transmitted infections among women using a variety of contraceptive options: a prospective study among high‐risk African women. J Intern AIDS Soc. 2019;22(2):e25257. doi:10.1002/jia2.25257
45. Kakaire O, Byamugisha JK, Tumwesigye NM, Gemzell-Danielsson K. Intrauterine contraception among women living with human immunodeficiency virus: a randomized controlled trial. Obstet Gynecol. 2015;126(5):928–934. doi:10.1097/AOG.0000000000001087
46. Matubu AT, Hillier SL, Meyn LA, et al. Effect of injectable progestin‐only contraceptives, depot medroxyprogesterone acetate and norethisterone enanthate, on cytokine production during T‐cell activation. Am J Reprod Immunol. 2021;86(1):e13405. doi:10.1111/aji.13405
47. Konstantinus IN, Balle C, Jaumdally SZ, et al. Impact of hormonal contraceptives on cervical T-helper 17 phenotype and function in adolescents: results from a randomized, crossover study comparing long-acting injectable Norethisterone Oenanthate (NET-EN), combined oral contraceptive pills, and combined contraceptive vaginal rings. Clinl Infect Dis. 2020;71(7):e76–e87. doi:10.1093/cid/ciz1063
48. Crucitti T, Hardy L, Van De Wijgert J, et al. Contraceptive rings promote vaginal lactobacilli in a high bacterial vaginosis prevalence population: a randomised, open-label longitudinal study in Rwandan women. PLoS One. 2018;13(7):e0201003. doi:10.1371/journal.pone.0201003
49. Avenant C, Bick AJ, Skosana SB, et al. Misreporting contraceptive use and the association of peak study progestin levels with weight and BMI among women randomized to the progestin-only injectable contraceptives DMPA-IM and NET-EN. PLoS One. 2023;18(12):e0295959. doi:10.1371/journal.pone.0295959
50. Kiweewa Matovu F, Kiwanuka N, Nabwana M, et al. Intramuscular depot medroxyprogesterone acetate accentuates bone loss associated with tenofovir disoproxil fumarate-containing antiretroviral therapy initiation in young women living with HIV (the BONE: CARE study): a prospective cohort study in Uganda. Lancet Glob Health. 2022;10(5):e694–e704. doi:10.1016/S2214-109X(22)00080-8
51. Singata‐Madliki M, Carayon‐Lefebvre d’Hellencourt F, Lawrie TA, Balakrishna Y, Hofmeyr GJ. Effects of three contraceptive methods on depression and sexual function: an ancillary study of the ECHO randomized trial. Int J Gynecol Obstet. 2021;154(2):256–262. doi:10.1002/ijgo.13594
52. Arowojolu AO, Okewole IA, Adekunle AO. Comparative evaluation of the effectiveness and safety of two regimens of levonorgestrel for emergency contraception in Nigerians. Contraception. 2002;66(4):269–273. doi:10.1016/S0010-7824(02)00337-2
53. Sagay AS, Okeahialam BN, Imade GE. Electrocardiographic changes among Nigerian Norplant users. West Afr J Med. 2002;21(2):146–148.
54. Isichei CO, Das SC, Ogunkeye OO, et al. Preliminary clinical investigation of the contraceptive efficacy and chemical pathological effects of RICOM-1013-J of Ricinus communis var minor on women volunteers. Phytother Res. 2000;14(1):40–42. doi:10.1002/(SICI)1099-1573(200002)14:1<40::AID-PTR323>3.0.CO;2-1
55. Coutinho EM, Athayde C, Atta G, et al. Gossypol blood levels and inhibition of spermatogenesis in men taking gossypol as a contraceptive. Contraception. 2000;61(1):61–67. doi:10.1016/S0010-7824(99)00117-1
56. Thurman AR, Soper DE. Endometrial histology of Depomedroxyprogesterone acetate users: a pilot study. Infect Dis Obstet Gynecol. 2006;2006:69402. doi:10.1155/IDOG/2006/69402
57. Casper RF. Regulation of estrogen/progestogen receptors in the endometrium. Int J Fertil Menopausal Stud. 1996;41(1):16–21.
58. Petry N, Olofin I, Hurrell R, et al. The proportion of anemia associated with iron deficiency in low, medium, and high human development index countries: a systematic analysis of national surveys. Nutrients. 2016;8(11):693. doi:10.3390/nu8110693
59. Hurskainen R, Teperi J, Rissanen P, et al. Clinical outcomes and costs with the levonorgestrel-releasing intrauterine system or hysterectomy for treatment of Menorrhagia: randomized trial 5-year follow-up. JAMA. 2004;291(12):1456. doi:10.1001/jama.291.12.1456
60. Berenson AB, Rahman M. Changes in weight, total fat, percent body fat, and central-to-peripheral fat ratio associated with injectable and oral contraceptive use. Am J Clin Exp Obstet Gynecol. 2009;200(3):
61. Lopez LM, Ramesh S, Chen M, et al. Progestin-only contraceptives: effects on weight. Cochrane Database Syst Rev. 2016;2016(8). doi:10.1002/14651858.cd008815.pub4
62. Bonny AE, Ziegler J, Harvey R, Debanne SM, Secic M, Cromer BA. Weight gain in obese and nonobese adolescent girls initiating depot medroxyprogesterone, oral contraceptive pills, or no hormonal contraceptive method. Arch Pediatr Adolesc Med. 2006;160(1):40. doi:10.1001/archpedi.160.1.40
63. Diedrich JT, Klein DA, Peipert JF. Long-acting reversible contraception in adolescents: a systematic review and meta-analysis. Am J Clin Exp Obstet Gynecol. 2017;216(4):
64. Edwards M, Can AS. Progestins. In: StatPearls. StatPearls Publishing; 2025.
65. Matubu A, Hillier SL, Meyn LA, et al. Depot medroxyprogesterone acetate and norethisterone enanthate differentially impact T-cell responses and expression of immunosuppressive markers. Am J Reprod Immunol. 2020;83(3):e13210. doi:10.1111/aji.13210
66. Gosmann C, Anahtar MN, Handley SA, et al. Lactobacillus-deficient cervicovaginal bacterial communities are associated with increased HIV acquisition in young South African Women. Immunity. 2017;46(1):29–37. doi:10.1016/j.immuni.2016.12.013
67. Ray RM, Maritz MF, Avenant C, et al. The contraceptive medroxyprogesterone acetate, unlike norethisterone, directly increases R5 HIV-1 infection in human cervical explant tissue at physiologically relevant concentrations. Sci Rep. 2019;9(1):4334. doi:10.1038/s41598-019-40756-7
68. Baeten JM, Palanee-Phillips T, Brown ER, et al. Use of a vaginal ring containing dapivirine for HIV-1 prevention in women. N Engl J Med. 2016;375(22):2121–2132. doi:10.1056/NEJMoa1506110
69. Polis CB, Curtis KM, Hannaford PC, et al. An updated systematic review of epidemiological evidence on hormonal contraceptive methods and HIV acquisition in women. AIDS. 2016;30(17):2665–2683. doi:10.1097/QAD.0000000000001228
70. Cenci S, Toraldo G, Weitzmann MN, et al. Estrogen deficiency induces bone loss by increasing T cell proliferation and lifespan through IFN-γ-induced class II transactivator. Proc Natl Acad Sci USA. 2003;100(18):10405–10410. doi:10.1073/pnas.1533207100
71. Riggs BL, Khosla S, Melton LJ. Sex steroids and the construction and conservation of the adult skeleton. Endocr Rev. 2002;23(3):279–302. doi:10.1210/edrv.23.3.0465
72. Cromer BA, Scholes D, Berenson A, Cundy T, Clark MK, Kaunitz AM. Depot medroxyprogesterone acetate and bone mineral density in adolescents—The Black Box Warning: a position paper of the society for adolescent medicine. J Adolesc Health. 2006;39(2):296–301. doi:10.1016/j.jadohealth.2006.03.011
73. Scholes D, LaCroix AZ, Ichikawa LE, Barlow WE, Ott SM. Injectable hormone contraception and bone density: results from a prospective study. Epidemiology. 2002;13(5):581–587. doi:10.1097/00001648-200209000-00015
74. Schiller CE, Johnson SL, Abate AC, Schmidt PJ, Rubinow DR. Reproductive steroid regulation of mood and behavior. In: Prakash YS, editor. Comprehensive Physiology.
75. Bäckström T, Bixo M, Johansson M, et al. Allopregnanolone and mood disorders. Prog Neurobiol. 2014;113:88–94. doi:10.1016/j.pneurobio.2013.07.005
76. Bethea CL, Lu NZ, Gundlah C, Streicher JM. Diverse actions of ovarian steroids in the serotonin neural system. Front Neuroendocrinol. 2002;23(1):41–100. doi:10.1006/frne.2001.0225
77. Anderl C, Li G, Chen FS. Oral contraceptive use in adolescence predicts lasting vulnerability to depression in adulthood. Child Psychol Psychiatry. 2020;61(2):148–156. doi:10.1111/jcpp.13115
78. Traish AM, Kim N, Min K, Munarriz R, Goldstein I. Role of androgens in female genital sexual arousal: receptor expression, structure, and function. Fertil Sterility. 2002;77:11–18. doi:10.1016/S0015-0282(02)02978-3
79. Pfaus JG. Pathways of Sexual Desire. J Sex Med. 2009;6(6):1506–1533. doi:10.1111/j.1743-6109.2009.01309.x
80. Skovlund CW, Mørch LS, Kessing LV, Lidegaard Ø. Association of hormonal contraception with depression. JAMA Psychiatry. 2016;73(11):1154. doi:10.1001/jamapsychiatry.2016.2387
81. Maybin JA, Critchley HOD. Menstrual physiology: implications for endometrial pathology and beyond. Hum Reprod Update. 2015;21(6):748–761. doi:10.1093/humupd/dmv038
82. Hubacher D, Lara-Ricalde R, Taylor DJ, Guerra-Infante F, Guzmán-Rodríguez R. Use of copper intrauterine devices and the risk of tubal infertility among nulligravid women. N Engl J Med. 2001;345(8):561–567. doi:10.1056/NEJMoa010438
83. Wu ZY, Yu DJ, Soong TW, Dawe GS, Bian JS. Progesterone impairs Human Ether-a-go-go-related Gene (HERG) trafficking by disruption of intracellular cholesterol homeostasis. J Biol Chem. 2011;286(25):22186–22194. doi:10.1074/jbc.M110.198853
84. Barrett-Connor E, Wehren LE, Siris ES, et al. Recency and duration of postmenopausal hormone therapy: effects on bone mineral density and fracture risk in the National Osteoporosis Risk Assessment (NORA) study. Menopause. 2003;10(5):412–419. doi:10.1097/01.GME.0000086467.82759.DA
85. Sitruk-Ware R. New progestagens for contraceptive use. Hum Reprod Update. 2006;12(2):169–178. doi:10.1093/humupd/dmi046
86. Grimes DA, Lopez LM, Schulz KF, Van Vliet HA, Stanwood NL. Immediate post-partum insertion of intrauterine devices. In: The Cochrane Collaboration, editor. Cochrane Database of Systematic Reviews. John Wiley & Sons, Ltd; 2010:
87. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
88. Aromataris E, Lockwood C, Porritt K, Pilla B, Jordan Z, editors.. JBI Manual for Evidence Synthesis. JBI; 2024. doi:10.46658/JBIMES-24-01
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.