Back to Journals » Therapeutics and Clinical Risk Management » Volume 12
Patent ductus arteriosus with persistent pulmonary artery hypertension after transcatheter closure
Authors Feng JQ, Kong XQ, Sheng YH, Yang R
Received 9 May 2016
Accepted for publication 19 August 2016
Published 3 November 2016 Volume 2016:12 Pages 1609—1613
DOI https://doi.org/10.2147/TCRM.S112400
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Jianqi Feng,1,2 Xiangqing Kong,1 Yanhui Sheng,1 Rong Yang1
1Department of Cardiology, the First Affiliated Hospital of Nanjing Medical University, Nanjing, Jiangsu, 2Department of Cardiology, the Second Affiliated Hospital of XuZhou Medical University, XuZhou, Jiangsu, People’s Republic of China
Objectives: To observe the change in pulmonary artery systolic pressure (PASP) of patients with persistent pulmonary arterial hypertension (PAH) after patent ductus arteriosus (PDA) occlusion.
Background: After occlusion of PDA in patients with PAH, some patients still tend to suffer from persistent PAH.
Methods: A chest X-ray, an electrocardiogram, and an echocardiogram were performed on nine patients at 24 hours, 1 and 6 months, and 1 year serially.
Results: There was a significant fall (P<0.05) in mean PASP after occlusion (to 59.3±12.7 mmHg). However, the aortic pressure and systemic arterial oxygen saturation changed slightly (P>0.05). During the follow up, there was a further fall in the PASP in five patients (No 1, 5, 6, 7, and 8). Four patients (No 2, 3, 4, and 8) showed the evidence of worsening PAH and were treated with sildenafil. Patient 2 died from acute right heart failure after a period of 11 months from the time of transcatheter closure, triggered by pulmonary infection.
Conclusion: Some patients with borderline hemodynamic data with PDA and PAH can deteriorate or keep sustained PAH after PDA closure. The treatment of permanent closure to these patients must be cautious.
Keywords: patent ductus arteriosus (PDA), transcatheter closure (TCC), pulmonary artery hypertension, follow-up
Introduction
Patent ductus arteriosus (PDA) is one of the most common congenital heart defects, accounting for 5%–10% of all congenital heart disease in infants.1 Transcatheter closure (TCC) PDA was first performed in 1971.2 With the progress of technique and material, TCC of PDA with various occluders has been well established and become the treatment of choice for the majority of patients with this condition.3–10 However, whether to attempt TCC of PDA in patients with severe pulmonary arterial hypertension (PAH) remains a challenging clinical problem, as there is not much information on the immediate and long-term effects of TCC of PDA in patients who have PAH, especially those with persistent PAH after occlusion.
Materials and methods
Patients
From July 2006 to January 2011, nine patients with clinical and echocardiographic findings of a PDA and severe pulmonary hypertension underwent TCC with the Amplatzer duct occluder (ADO, AGA Medical Corporation, Golden Valley, MN, USA). Pulmonary hypertension maintained after occlusion.
Their mean age was 24.2±8.2 years (range 16–42 years) and their median body weight was 53.6±7.8 kg (range 46–71 kg). The study was approved by the Ethics Committee of Nanjing Medical University. Written informed consents were obtained from all patients.
Interventional procedure
The technique of TCC of PDA using the ADO was similar to that described by Masura et al.11 After a complete hemodynamic evaluation and descending aortogram in the lateral or right anterior oblique view, trial occlusion with the ADO (the size of the occlusion device we chose was 4–6 mm larger than the narrowest size of the PDA) was performed for 30 minutes to record the change in hemodynamic and clinical data. If the pulmonary arterial pressure fell or did not increase, the aortic pressure did not decrease, and the signs and symptoms did not worsen, then the PDA occluder was released. A repeat descending aortogram excluded a moderate-to-large residual left-to-right shunt. Otherwise, the occluding device was retracted into the delivery sheath. Prophylactic antibiotics were routinely given after the procedure for 3 days. All the patients returned home after 2 days of observation in the cardiac ward.
Follow-up
A chest X-ray, an electrocardiogram, and an echocardiogram were performed on all the patients at 24 hours, 1 and 6 months, and 1 year serially.
Statistics
The results were analyzed using SPSS 13.0 (SPSS Inc., Chicago, IL, USA) and expressed as mean (standard deviation), with confidence intervals where applicable. Preocclusion and postocclusion data were compared using paired-samples t-tests. A probability value of P<0.05 was considered significant.
Results
The clinical and hemodynamic data before and after occlusion of nine patients are shown in Tables 1 and 2. The PDA size was 8.9 (3.0) mm (range 5–15 mm). The mean ADO diameter was 14.8 (3.0) mm (11–20 mm). The ratio of pulmonary blood flow to systemic flow (Qp/Qs) was 2.2 (0.7) (range 1.7–3.94). The mean pulmonary vascular resistance (PVR) at baseline was 6.4 (2.8) Woods units (range 2.7–12.6 Woods). The mean pulmonary artery systolic pressure (PASP) and aortic systolic pressure at baseline were 106.7 (21.5) mmHg (range 78–140 mmHg) and 137.1 (8.1) mmHg (range 127–147 mmHg), respectively. There was a significant fall (P<0.05) in mean PASP after occlusion (to 59.3±12.7 mmHg). However, the change in aortic pressure and systemic arterial oxygen saturation (SaO2) was insignificant (P>0.05).
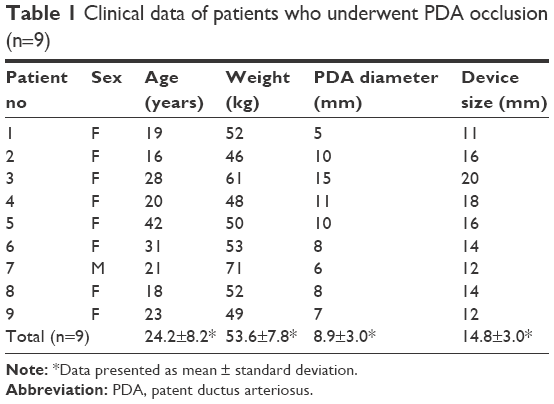 | Table 1 Clinical data of patients who underwent PDA occlusion (n=9) |
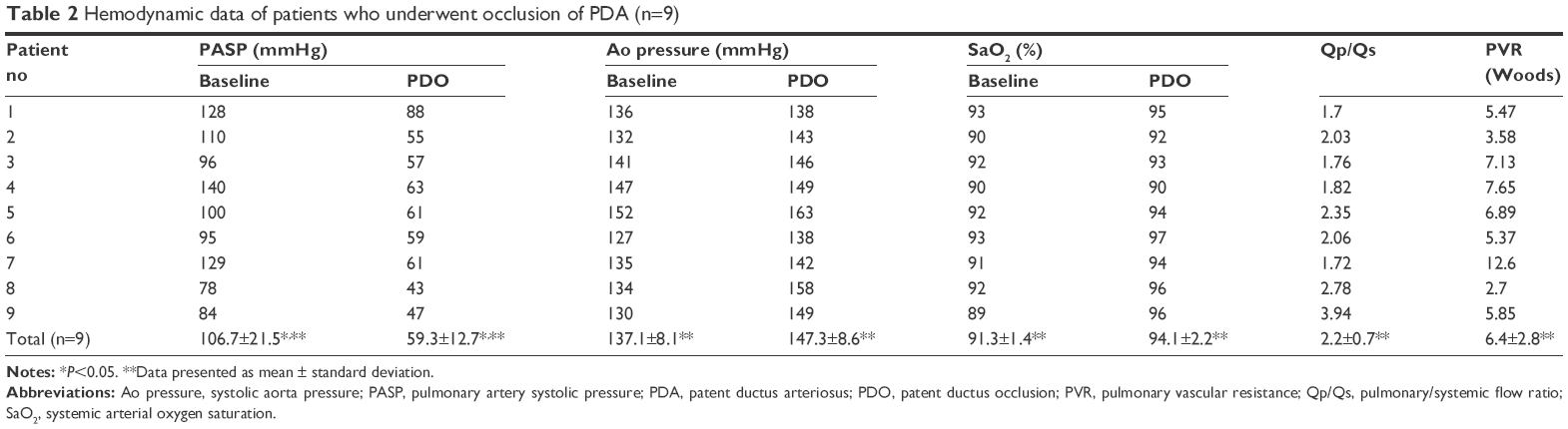 | Table 2 Hemodynamic data of patients who underwent occlusion of PDA (n=9) |
The mean follow-up time was 3.6 years (range 0.9–7 years). During the follow up, PASP was obtained from echo/Doppler study. There was a further fall of PASP in five patients (No 1, 5, 6, 7, and 8). Four patients (No 2, 3, 4, and 8) showed evidence of worsening of PAH and were treated with sildenafil. Patient 2 died from acute right heart failure after a period of 11 months from the time of TCC, which was triggered by a pulmonary infection (Table 3, Figures 1 and 2).
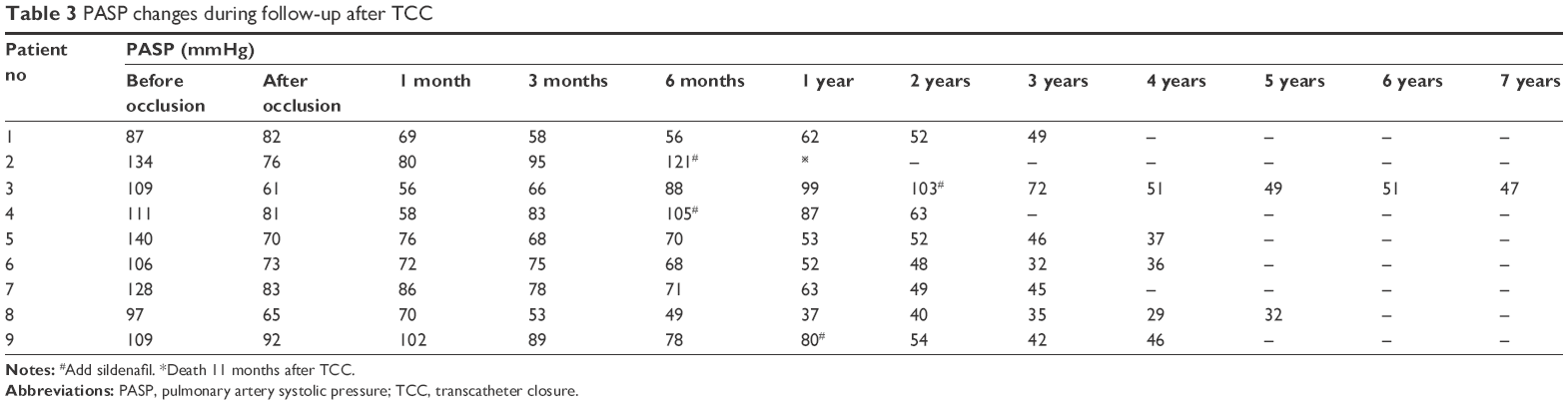 | Table 3 PASP changes during follow-up after TCC |
 | Figure 1 PASP changes within 1 year after TCC. |
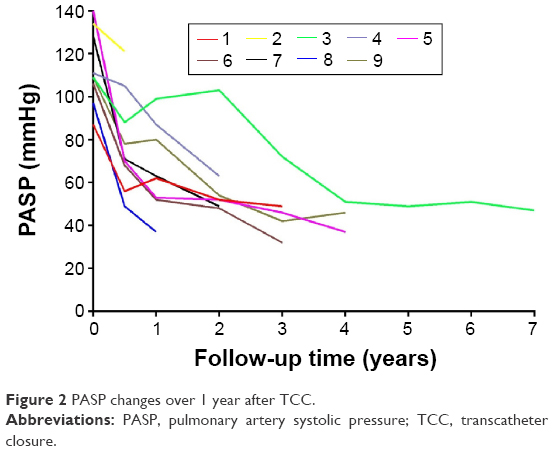 | Figure 2 PASP changes over 1 year after TCC. |
Discussion
TCC is now widely accepted as the first-choice treatment of PDA. The increasing experience allows PDA patients with PAH to be evaluated for transcatheter device occlusion. The findings of the present study indicated that TCC of PDA in patients with PAH is feasible, effective, and safe, even in severely symptomatic patients.12–17 However, a small percentage of patients with borderline hemodynamic data with PDA and PAH can deteriorate after PDA closure due to non-regression of pulmonary hypertension, progressive pulmonary vascular disease, and right heart failure. Their natural history is similar to idiopathic PAH. In our study, the PASP of nine patients decreased by >20% immediately after occlusion. During the follow-up of these patients, PASP of five patients decreased further and worsened in the remaining four patients. The PASP of all nine patients did return back to normal. For patients 1 and 7, the PDA diameter was only 5 or 6 mm. According to the clinical classification of pulmonary hypertension,18 this is generally classified as PAH associated with small defects. But we were unable to differentiate whether it was PDA with idiopathic PAH.
Whether to attempt TCC of PDA in patients with severe PAH remains a challenging clinical problem. In this condition, the most important determinant of management and prognosis is whether the severe PAH is reversible. Clinical examination is used to evaluate the reversibility of severe PAH. However, taking a decision to intervene is difficult if the clinical examinations are equivocal and there are some limitations for calculating PVR in PDA. A multicenter study by Balzar et al concluded that the use of vasodilators, including inhaled nitric oxide, has limited utility in deciding operability.19 Contrary to the popular belief, a recent study showed that preoperative hemodynamic information does not correlate with postoperative outcome for various reasons.20
Trial occlusion of PDA with device has been in use to decide on the contribution of left to right shunt and PVR to PAH.15,19,21–23 The criteria that we followed were as follows: 1) a fall in the pulmonary artery pressure or no elevation; 2) no decrease in the aortic pressure and SaO2; and 3) no worsening of signs and symptoms. If all the criteria were satisfied, we considered the PAH to be reversible. Otherwise, it was considered to be irreversible PAH and occlusion was abandoned. This is a reliable test to exclude patients with borderline hemodynamic data from undergoing device closure.15,21,24
Sildenafil has been shown to improve exercise capacity, oxygen saturations, cardiopulmonary hemodynamics, and World Health Organization function class in patients with PAH, including PAH in patients with congenital heart disease having PAH.25–29 Longer-term studies have suggested sustained benefits. A larger randomized trial of 278 patients, including 7% with Eisenmenger syndrome, showed significant benefit after 19 months.25 In our study, after being treated with sildenafil, there was a decrease in the PASP of patients with PDA after closure.
Study limitations
There are two main limitations in our study. First, the major limitation of the study was the small sample size which limited its power. Second, during the follow-up, pulmonary arterial pressure was only evaluated by ultrasound. No patients underwent catheterization again.
Conclusion
TCC for PDA with severe PAH is currently the preferred method. However, some patients with borderline hemodynamic data with PDA and PAH can deteriorate or keep sustained PAH after PDA closure, although PAP would decrease by >20% immediately after trial occlusion. In such patients, the treatment of permanent closure must be performed with caution.
Disclosure
The authors report no conflicts of interest in this work.
References
Schneider DJ, Moore JW. Patent ductus arteriosus. Circulation. 2006;114(17):1873–1882. | ||
Portsmann W, Wierny L, Warnke H, Gerstberger G, Romaniuk PA. Catheter closure of patent ductus arteriosus, 62 cases treated without thoracotomy. Radiol Clin North Am. 1971;9(2):203–218. | ||
Baumgartner H, Bonhoeffer P, De Groot NM, et al. Guidelines for the management of grown-up congenital heart disease (new version 2010): the task force on the management of grown-up congenital heart disease of the European society of cardiology (ESC), endorsed by the association for European paediatric cardiology (AEPC). Eur Heart J. 2010;31(23):2915–2957. | ||
Rao PS, Kim SH, Choi JY, et al. Follow-up of transvenous occlusion of patent ductus arteriosus with the buttoned device. J Am Coll Cardiol. 1999;33(3):820–826. | ||
Hijazi ZM, Geggel RL. Transcatheter closure of large patent ductus arteriosus (≥4 mm) with multiple Gianturco coils: immediate and mid-term results. Heart. 1996;76(6):536–540. | ||
Uzun O, Hancock S, Parsons JM, Dickinson DF, Gibbs JL. Transcatheter occlusion of the atrial duct with Cook detachable coil: early experience. Heart. 1996;76(6):269–273. | ||
Hijazi ZM, Geggel RL. Results of anterograde transcatheter closure of patent ductus arteriosus using single or multiple Gianturco coils. J Am Coll Cardiol. 1994;74(9):925–929. | ||
Verin VE, Saveliev SV, Kolody SM, Prokubovski VI. Results of transcatheter closure of the patent ductus arteriosus with the Botalloocluder. J Am Coll Cardiol. 1993;22(5):1509–1514. | ||
Hosking MCK, Benson LN, Musewe N, Dyck JD, Freedom RM. Transcatheter occlusion of the persistently patent ductus arteriosus: forty-month follow-up and prevalence of residual shunting. Circulation. 1991;84(6):2313–2317. | ||
Rashkind WJ, Mullins CE, Helenbrand WE, Tait MA. Non-surgical closure of patent ductus arteriosus: clinical application of the Rashkind PDA occluder system. Circulation. 1987;75(3):583–592. | ||
Masura J, Kevin P, Thanopoulos B, et al. Catheter closure of moderate to large-sized patent ductus arteriosus using the new Amplatzer duct occluder: immediate and short-term results. J Am Coll Cardiol. 1998;31(4):878–882. | ||
Zhang CJ, Huang YG, Huang XS, et al. Transcatheter closure of large patent ductus arteriosus with severe pulmonary arterial hypertension in adults: immediate and two-year follow-up results. Chinese. Med J. 2012;125(21):3844–3850. | ||
Tharakan J, Venkateshwaran S. Large patent ductus arteriosus: to close or not to close. Ann Pediatr Cardiol. 2012;5(2):141–144. | ||
Bhalgat PS, Pinto R, Dalvi BV. Transcatheter closure of large patent ductus arteriosus with severe pulmonary arterial hypertension: short and intermediate term results. Ann Pediatr Cardiol. 2012;5(2):135–140. | ||
Yan C, Zhao S, Jiang S, et al. Transcatheter closure of patent ductus arteriosus with severe pulmonary arterial hypertension in adults. Heart. 2007;93(4):514–518. | ||
Ji Q, Feng J, Mei Y, et al. Transcatheter closure of adult patent ductus arteriosus with severe pulmonary hypertension. Hypertens Res. 2008;31(11):1997–2002. | ||
Yu ML, Huang XM, Wang JF, Qin YW, Zhao XX, Zheng X. Safety and efficacy of transcatheter closure of large patent ductus arteriosus in adults with a self-expandable occluder. Heart Vessels. 2009;24(6):440–445. | ||
Simonneau G, Robbins IM, Beghetti M, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. 2009;54(1 Suppl):S43–S54. | ||
Balzer DT, Kort HW, Day RW, et al. Inhaled Nitric Oxide as a Preoperative Test (INOP Test I): the INOP Test Study Group. Circulation. 2002;106(12 Suppl 1):176–181. | ||
Kannan BR, Sivasankaran S, Tharakan JA, et al. Long term outcome of patients operated for large ventricular septal defects with increased pulmonary vascular resistance. Indian Heart J. 2003;55(2):161–166. | ||
Yang SW, Zhou YJ, Hu DY, et al. Feasibility and safety of transcatheter intervention for complex patent ductus arteriosus. Angiology. 2010;61(4):372–376. | ||
Thanopoulos BD, Tsaousis GS, Djukic M, AL Hakim F, Eleftherakis NG, Simeunovic SD. Transcatheter closure of high pulmonary pressure persistent ductus arteriosus with Amplatzer muscular ventricular septal defect occluder. Heart. 2002;87(3):260–263. | ||
Roy A, Juneja R, Saxena A. Use of Amplatzer duct occluder to close severely hypertensive ducts: utility of transient balloon occlusion. Indian Heart J. 2005;57(4):332–336. | ||
Viswanathan S, Kumar RK. Assessment of operability of congenital cardiac shunts with increased pulmonary vascular resistance. Catheter Cardiovasc Interv. 2008;71(5):665–670. | ||
Galiè N, Ghofrani HA, Torbicki A, et al. Sildenafil Use in pulmonary arterial hypertension (SUPER) study group. sildenafil citrate therapy for pulmonary arterial hypertension. N Engl J Med. 2005;353(20):2148–2157. | ||
Chau EM, Fan KY, Chow WH. Effects of chronic sildenafil in patients with Eisenmenger syndrome versus idiopathic pulmonary arterial hypertension. Int J Cardiol. 2007;120(3):301–305. | ||
Singh TP, Rohit M, Grover A, Malhotra S, Vijayvergiya R. A randomized, placebocontrolled, double-blind, crossover study to evaluate the efficacy of oral sildenafil therapy in severe pulmonary artery hypertension. Am Heart J. 2006;151(4):851, e1–e5. | ||
Garg N, Sharma MK, Sinha N. Role of oral sildenafil in severe pulmonary arterial hypertension: clinical efficacy and dose response relationship. Int J Cardiol. 2007;120(3):306–313. | ||
Tay EL, Papaphylactou M, Diller GP, et al. Quality of life and functional capacity can be improved in patients with Eisenmenger syndrome with oral sildenafil therapy. Int J Cardiol. 2011;149(3):372–376. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.