Back to Journals » International Medical Case Reports Journal » Volume 13
Partial Central Retinal Artery Occlusion: An Underrecognized Entity
Authors Carranza-Casas M, Aceves-Velazquez JE, Cano-Hidalgo R ![]() , Graue-Wiechers F
, Graue-Wiechers F ![]()
Received 28 July 2020
Accepted for publication 25 September 2020
Published 26 November 2020 Volume 2020:13 Pages 637—642
DOI https://doi.org/10.2147/IMCRJ.S274409
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Mario Carranza-Casas, Jorge E Aceves-Velazquez, René Cano-Hidalgo, Federico Graue-Wiechers
Instituto de Oftalmología Conde de Valenciana IAP, Mexico City, Mexico
Correspondence: Mario Carranza-Casas Email [email protected]
Background: The objective of this publication is to report a case of an atypical partial central retinal artery occlusion (CRAO) with substantial visual recovery without treatment.
Case Presentation: An 83-year-old woman without significant medical history with sudden unilateral visual loss presented with no known significant ophthalmological or medical history besides systemic arterial hypertension. Examination showed multiple cotton-wool spots in a peripapillary distribution, as well as a heterogenous pattern of grey translucency in the macula resulting in an indistinct cherry-red spot. Fluorescein angiography showed normal choroidal filling and an important delay of dye transit through the retinal circulation. Carotid Doppler echography showed a small endothelial atherosclerotic plaque without hemodynamic repercussion. A detailed history and further examination revealed no other systemic diseases except for moderate hypercholesterolemia. The patient was referred for management of her hypertension but otherwise did not undergo specific therapy for CRAO because of the delayed presentation. Four weeks after the initial visual loss, the patient showed resolution of the retinal findings and a surprising improvement to 20/50 visual acuity.
Conclusion: This case highlights a rare subtype of central retinal artery occlusion. In this disease, partial occlusion reveals atypical signs including large cotton-wool spots as the predominant finding, making the initial diagnosis difficult. Visual recovery may be significant in partial CRAO, even without treatment.
Keywords: arterial occlusion, central retinal artery occlusion, partial central retinal artery occlusion, cotton-wool spots, occlusive disease, Purtscher-like retinopathy, Purtscher retinopathy, vascular disease, partial occlusion
Background
Central retinal artery occlusion (CRAO) is an obstructive vascular disease characterized by sudden, severe and painless vision loss associated with classic clinical findings, mainly posterior pole retinal whitening with a distinct central cherry-red spot conditioned by the intact choroidal vasculature beneath the fovea.1 Other findings include a pale optic disc, arterial narrowing and box-carring, or cotton-wool spots (CWS) in rare instances.2 CRAO results from various pathologic processes, most often embolization or atherosclerosis-related thrombosis, but can be caused by arterial spasm, carotid or ophthalmic artery obstruction or systemic disease like giant cell arteritis.1–3 The prognosis is poor, with a majority achieving final visual acuity of 20/400 or worse, and most cases with preserved vision being those with a patent cilioretinal artery.4 Different therapeutic approaches have been tried, with none being effective in evidence-based studies.4
A partial central retinal artery (CRA) occlusion is a lesser known entity, first referenced in 1971 by Wise, Dollery and Henkind as a rare form of CRAO in which the degree of arterial closure was incomplete enough to permit improvement in visual acuity, and the clinical picture was established by a mild retinal haze together with scattered, more opaque “cotton-wool-like patches,” and abnormally darker retinal veins indicating subpar venous blood oxygenation.5 In 1978 Oji and McLeod further detailed several cases, defining the remarkable fundus appearance of this disease as one showing sudden onset visual field loss, heterogenous macular swelling with a poorly defined cherry-red spot, large peripapillary CWS and retinal venous cyanosis presenting as darker than usual veins.6
To the author’s knowledge, there are few case reports of partial CRAO in the literature; thus, many clinicians are not familiarized with this uncommon presentation.
Here we describe one unusual case of an apparent partial CRAO being confused initially with Purtscher-Like Retinopathy (PLR) and improving markedly without any treatment.
Case Presentation
An 83-year-old woman was referred to our hospital approximately 96 hours after sudden onset of painless central visual loss in her right eye (OD), the patient denied any triggering events. She reported a 13-year history of mild systemic hypertension but no other relevant medical or ophthalmological history. At baseline, the best-corrected visual acuity (BCVA) was Count Fingers (CF) OD and 20/50 left eye (OS), the respective intraocular pressure values were 12 and 14 mmHg. A relative afferent pupillary defect (APD) was present in the right eye. Funduscopic examination of the right eye showed a normal-appearing optic nerve with multiple splinter hemorrhages on the rim, as well as multiple large CWS in a circumpapillary distribution that partially obscured retinal veins. An heterogenous pattern of grey translucency in the macula with notable periarterial sparing was evident. Neither segmental narrowing of the retinal arteries nor a defined cherry-red spot were visible, but a darker hue to the retinal veins was apparent (Figure 1). The left eye had a normal fundus appearance. A horizontal foveal spectral-domain optical coherence tomography (SD-OCT) scan revealed a generalized retinal thickening, with a significant increase in reflectivity signaling edema localized to the inner layers (Figure 2). Fluorescein angiography was performed, showing normal choroidal filling including a patent cilioretinal artery, and an important delay of the retinal circulation (Figure 3); slight leakage and staining of the optic disc and peripapillary arterioles were also noted in later phases with some dye masking corresponding with the location of the CWS (Figure 4). A hyperfluorescent/hypofluorescent-speckled pattern was noted in the periphery related to the retinal pigment epithelium degeneration both in early and late phases. Carotid and vertebral artery Doppler echography showed a mild endothelial atherosclerotic plaque in the right carotid bulb that involved 20% of the vessel lumen but without hemodynamic repercussion, with normal flow velocity and resistance indexes. Systemic examination showed no other diseases, and extensive bloodwork revealed moderate hypercholesterolemia as the only abnormality. Ophthalmic and central retinal artery Doppler echography studies were undertaken, finding a noteworthy reduction in CRA blood flow. Based on these findings, the case was diagnosed as a partial CRAO; the patient was referred for management of her hypertension but otherwise did not undergo specific therapy for CRAO because of the delayed presentation.
 |
Figure 1 Right eye fundus photograph shows large cotton-wool spots in a peripapillary distribution as well as a heterogeneous pattern of grey translucency with periarterial sparing in the macula. |
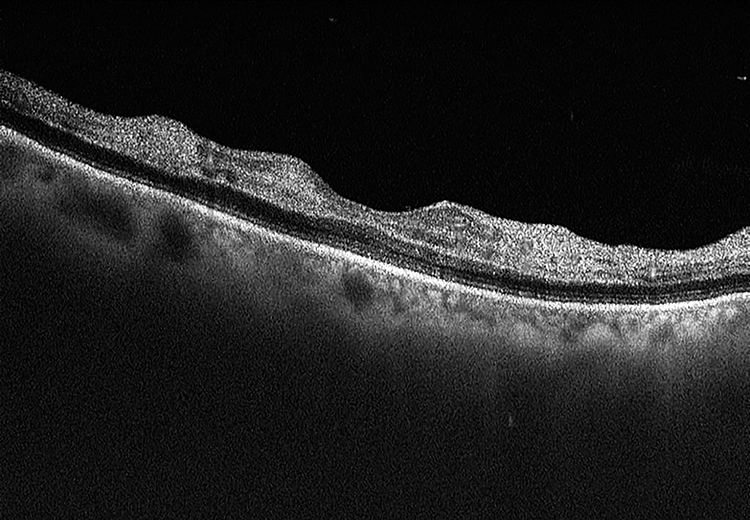 |
Figure 2 A horizontal spectral domain optical coherence tomography scan of the right eye was taken at foveal center, revealing an increase of the inner layer reflectivity and generalized inner retinal thickening. |
 |
Figure 3 Right eye widefield fluorescein angiography shows delayed choroidal filling, taken 43 seconds after administering the dye. |
 |
Figure 4 Right eye widefield fluorescein angiography shows peripheral pigmentary degeneration, discrete leakage and staining of the optic disc and peripapillary arterioles, taken 70 seconds after dye administration. |
The areas of retinal whitening and CWS progressively disappeared during the next 2 weeks. The patient’s visual capacity also gradually improving during this time, being 20/50 at last follow-up; approximately 4 weeks after initial presentation. The latest fundus findings showed normal retinal characteristics and resolution of the APD (Figure 5).
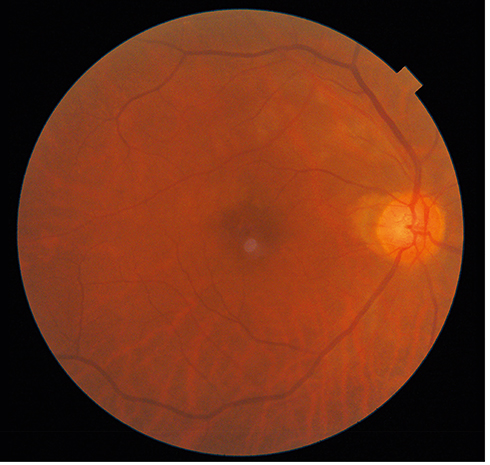 |
Figure 5 Right eye fundus photograph 4 weeks after initial presentation shows normal retinal characteristics. |
Discussion and Conclusions
Herein we present a case of a partial retinal arterial occlusion initially mistaken as PLR. Typical CRAO has a fundus appearance characterized by generalized retinal whitening in the posterior pole and a distinct cherry-red spot; with cotton-wool patches being reported only in 3% of cases.2 In this particular case, the retina did not show these classic manifestations, and large CWS were precisely the predominant finding, making the initial diagnosis complex.7 The significant decrease in visual acuity not normally found in PLR and afferent pupillary defect were warning signs of a more ominous underlying cause. The distinction between atypical CRAO and PLR has not been made in a definite manner and the latter has been theorized to be caused by endogenous emboli after leukocyte aggregation related to a systemic inflammatory response. However, this response has always been reported in association with traumatic injury or several other systemic diseases that might explain this endogenous embolization;8 after thorough investigation none of the previously reported causes of PLR were found in our patient. Additionally, fluorescein angiography showed a delayed arm-to-retina circulation time which has not been reported in eyes with PLR.8 Since no other causes for PLR were found, further testing of carotid and central retinal artery blood flow was undertaken, revealing CRA flow obstruction and supporting CRAO as the diagnosis. Furthermore, the imaging, clinical presentation, and visual improvement were atypical for CRAO but coincided with the description of cases reported by Kurimoto, Ikeda and Imasawa,7–9 and also descriptively detailed by Oji and McLeod as a partial occlusion.6,10 Typical course of a CRAO includes an embolic source of blockage and sudden visual loss with the “classic signs” already mentioned. Even though the artery can re-canalize over time and the edema can clear, most cases lead to permanent and severe loss of vision; this disease history is appropriately associated with a more severe degree of obstruction of the arterial flow.4 On the other hand, a partial CRAO is a well-defined clinical entity with incomplete obstruction that should be recognized independently. To distinguish this disease, we can look at the multiple large CWS that represent axoplasmic transport obstruction instead of the commonly referred nerve fiber layer infarcts from multiple retinal arteriolar occlusions. It is the combined influence of peripapillary, periarterial and, in some eyes, cilioretinal sparing from the effects of severe oligemia throughout the CRA territory that yields this clinical picture when blood flow obstruction is incomplete and not only transitory.6,10 The changes found after partial CRAO depend on the degree of panretinal hypoperfusion and the specific anatomical arrangement of the CRA branches within the affected eye, and thus the precise configuration, clinical variation and relative rarity of this critical degree of retinal hypoperfusion might explain why this subtype of occlusion tends not to be as commonly recognized.6,10
Other notable and characteristic findings include heterogenous translucency of macular retina resulting from ischemic anoxia not exceeding the survival time of the retinal tissue, or more prolonged, but sublethal, ischemic hypoxia.10 In these circumstances, osmotically obligated water enters affected cells and compromises retinal transparency. The non-lethal anoxia is caused by either incomplete closure of the CRA, or complete closure accompanied by important collateral flow channels, while temporary obstruction is not enough to warrant these distinct changes.10 The periarterial sparing accounting for the irregular pattern of macular whitening is caused by relatively high oxygen pressures in the retinal arterioles compared to macular retina.6 Darker coloration of retinal veins described in McLeod’s report is purportedly induced by a decrease in venous hemoglobin O2 saturation. Finally, hypo-fluorescence caused by the absence of dye in the location of cotton-wool spots8 is primarily due to masking related to the nerve fiber layer opacification. Acknowledging the differentiating retinal features is important because they can be appreciated with ophthalmoscopy alone, and the natural history of this condition includes the possibility of remarkable visual recovery. This favorable outcome may be equivalent or even better to that seen after CRAO with cilioretinal sparing, which was present in our patient. Nonetheless, when cilioretinal patency accounts for the improved prognosis the patients initially show the classic generalized retinal whitening with localized sparing of the retinal zone perfused by said artery.
The surprising improvement in visual acuity reported in these cases 2–4 weeks after initial presentation was more likely caused by spontaneous circulatory restitution in a retina suffering from non-lethal degrees of ischemia.10 Even though spontaneous recovery of poor vision in CRAO is known, it can be better approximated and explained by cases like this, where partial occlusion reveals a distinct clinical picture that allows the clinician to predict a relatively good prognosis for the patient.
CT o MR angiography was not realized in our patient, but she did undergo echocardiography and evaluation by a cardiologist. After further analysis and monitoring, no significant valvular disease or arrhythmia was diagnosed. It is agreed the minor carotid atherosclerotic plaque reported is unlikely to be the origin of the embolus but no other possibility was found after extensive follow-up. Without treatment the regression of the patients funduscopic signs indicates restoration of circulation and reperfusion of the central retinal artery territory with retina in ischemic penumbra surviving and re-establishing its functionality and in turn the patients visual capacity.
Accordingly, this patient gradually recovered vision from CF to 20/50 in approximately 4 weeks without treatment, this being a highly unusual outcome for a typical CRAO and supportive of the incomplete or partial occlusion diagnosis regardless of the echographic results.
There is a remarkable heterogeneity in the approach to acute treatment of patients with CRAO, with intravenous fibrinolysis, anterior chamber paracentesis, ocular massage and hyperbaric oxygen therapy being the preferred initial treatment options in a recent US survey.11
Therapeutic recanalization of the CRA using fibrinolysis is intended to restore inner retinal perfusion within the survival time of the tissue; retinal tissue is to be rescued from the immediate danger of oncotic necrosis. The specific retinal survival time is not perfectly defined, however, as it depends not only on the inherent capability of the tissue to reverse the negative processes induced but also on the degree of oligemia.10 If the survival time of retinal tissues has already been exceeded, expediting reversal by fibrinolytic treatment is unlikely to confer a better visual prognosis over that deriving from spontaneous reinstatement of circulation.10 Research so far has not shown these interventions to be useful.4
In conclusion, ophthalmologists and retina specialists must be aware of this distinct presentation of CRAO and its clinical manifestations to better diagnose and counsel patients regarding their need for treatment and prognosis. More clinical trials should be undertaken to define a possible therapeutic rationale in these cases since treatment regimens administered so far to central artery occlusions have not proven to be effective but could have a different outcome when limited to partial occlusions.
Abbreviations
CRAO, Central retinal artery occlusion; CWS, Cotton-wool spots; CRA, Central retinal artery; PLR, Purtscher-like retinopathy; OD, Right eye; BCVA, Best-corrected visual acuity; CF, Counting fingers vision; APD, Afferent pupillary defect; OS, Left eye; SD-OCT, Spectral-Domain optical coherence tomography.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
Ethical approval appropriate to the country in which the research was performed was obtained by the corresponding ethics committee (Comité de Ética del instituto de Oftalmología Conde de Valenciana) and approved and labeled as Investigation without risk. The information obtained in the clinical records of the institution or directly from the patient will be kept under maximum confidentiality, therefore, no data will be published that could compromise the privacy of the patients.
Consent for Publication
Written informed consent for publication was obtained from the patient, our institutional consent form is available from the corresponding author on reasonable request.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
Not applicable: No funding was necessary for this case report.
Disclosure
The authors declare that they have no proprietary interests, no competing interests, and no conflicts of interest for this work.
References
1. Mangat HS. Retinal artery occlusion. Surv Ophthalmol. 1995;40(2):145–156. doi:10.1016/S0039-6257(95)80004-2
2. Hayreh SS, Zimmerman MB. Fundus changes in central retinal artery occlusion. Retina. 2007;27(3):276–289.
3. Mehta N, Marco RD, Goldhardt R, Modi Y. Central retinal artery occlusion: acute management and treatment. Curr Ophthalmol Rep. 2017;5(2):149–159. doi:10.1007/s40135-017-0135-2
4. Dattilo M, Biousse V, Newman NJ. Update on the management of central retinal artery occlusion. Neurol Clin. 2017;35(1):83–100. doi:10.1016/j.ncl.2016.08.013
5. Wise GN, Dollery CT, Henkind P. The Retinal Circulation. New York, Evanston, San Francisco, London: Harper and Row; 1971.
6. Oji EO, McLeod D. Partial central retinal artery occlusion. Trans Ophthalmol Soc U K. 1978;98(1):156–159.
7. Imasawa M, Morimoto T, Iijima H. Recovery of visual field loss due to central retinal artery occlusion. Jpn J Ophthalmol. 2004;48(3):294–299.
8. Kurimoto T, Okamoto N, Oku H. et al. Central retinal artery occlusion resembling Purtscher-like retinopathy. Clin Ophthalmol.2011; 1083. doi:10.2147/OPTH.S22786
9. Ikeda Y, Sano I, Fujihara E, Tanito M. Periarteriolar-sparing retinal edema in acute central retinal artery occlusion. Case Rep Ophthalmol. 2015;6(3):390–393. doi:10.1159/000442175
10. McLeod D. Letter to the editor: partial central retinal artery occlusion offers a unique insight into the ischemic penumbra. Clin Ophthalmol. 2012;6:9–22.
11. Youn TS, Lavin P, Patrylo M, et al. Current treatment of central retinal artery occlusion: a national survey. J Neurol. 2017;265(2):330–335. doi:10.1007/s00415-017-8702-x
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.