Back to Journals » Clinical Ophthalmology » Volume 20
Pars Plana Vitrectomy Using 0.025% Povidone-Iodine Irrigation for Acute Endophthalmitis: A Retrospective Case-Control Study
Authors Osorio-Landa HK ![]() , Velez-Montoya R
, Velez-Montoya R ![]() , Henaine-Berra A
, Henaine-Berra A ![]() , Fromow-Guerra J, Garcia-Aguirre G
, Fromow-Guerra J, Garcia-Aguirre G ![]()
Received 13 April 2026
Accepted for publication 16 June 2026
Published 14 July 2026 Volume 2026:20 616518
DOI https://doi.org/10.2147/OPTH.S616518
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yousef Fouad
Hillary Kimberly Osorio-Landa,1 Raul Velez-Montoya,1 Andrée Henaine-Berra,2 Jans Fromow-Guerra,1 Gerardo Garcia-Aguirre1
1Retina Department, Asociación para Evitar la Ceguera en México I.A.P., Mexico, 04030, Mexico; 2Médica Sur Hospital, Mexico, 14050, Mexico
Correspondence: Gerardo Garcia-Aguirre, Asociación para Evitar la Ceguera en México I.A.P, Vicente García Torres 46, Col. San Lucas Coyoacán, Mexico, 04030, Mexico, Tel +52 55 1084 1400, Fax +52 55 1084 1404, Email [email protected]
Purpose: To compare visual and anatomical outcomes of patients with acute endophthalmitis treated with pars plana vitrectomy (PPV) using either 0.025% povidone-iodine (PI) or standard balanced salt solution (BSS) irrigation and to evaluate the safety profile of intraocular PI.
Design: Retrospective case-control study.
Subjects: Ninety-two patients (48 in the PI group and 44 in the BSS group) aged ≥ 18 years with acute endophthalmitis of various etiologies treated between January 2017 and December 2024.
Methods: All patients underwent 23- or 25-gauge PPV and received intravitreal moxifloxacin and dexamethasone. The study group received 0.025% PI irrigation, whereas the control group received standard BSS irrigation. Main outcomes included best-corrected visual acuity (BCVA), infection resolution, reactivation, and postoperative findings potentially associated with ocular toxicity. Safety assessments were based on slit-lamp examination, retinal imaging, and optical coherence tomography.
Results: Clinical resolution at 1 week was achieved in 68.8% of eyes in the PI group and 65.9% in the control group (p = 0.83). No statistically significant differences were observed between groups regarding infection resolution, recurrence/reactivation, or BCVA outcomes. At 3 months, mean BCVA was logMAR 1.096 (approximately 20/250) in the PI group and logMAR 1.70 (count fingers) in the control group. Fewer postoperative findings potentially associated with ocular toxicity were observed in the PI group compared with controls (20.8% vs. 70.5%; p < 0.001).
Conclusion: In this retrospective case-control study, 0.025% PI irrigation during PPV was not associated with worse short-term anatomical or visual outcomes compared with standard BSS irrigation. Although postoperative adverse findings were less frequent in the PI group, this result should be interpreted cautiously given the non-randomized design and earlier timing of vitrectomy in the PI group. Prospective controlled studies are needed to confirm the safety and potential efficacy of this approach.
Keywords: endophthalmitis, povidone-iodine, pars plana vitrectomy, intravitreal antibiotics, ocular toxicity, antimicrobial resistance
Introduction
Endophthalmitis is a potentially blinding intraocular infection characterized by severe inflammation and tissue destruction. Visual outcomes largely depend on prompt diagnosis, timely intervention, and microbial virulence. Current management combines intravitreal antimicrobial therapy with pars plana vitrectomy (PPV) in severe cases to reduce microbial burden, remove inflammatory debris, and improve intraocular drug distribution.1–3
Increasing antimicrobial resistance has encouraged the exploration of adjunctive therapies. Povidone-iodine (PI) is a broad-spectrum antiseptic with rapid microbicidal activity, and diluted intraocular concentrations between 0.013% and 0.027% have shown bactericidal activity within a range considered safe for intraocular tissues.4–7 However, comparative clinical evidence evaluating PI-infused vitrectomy versus standard balanced salt solution (BSS) irrigation remains limited.4,5,8–12
Because acute endophthalmitis may arise from diverse clinical settings, evaluating PI across a real-world spectrum of etiologies may provide clinically relevant safety and outcome data.13 This study aimed to compare visual and anatomical outcomes in patients with acute endophthalmitis treated with PPV using either 0.025% PI or standard BSS irrigation.
Materials and Methods
The study was conducted in accordance with the tenets of the Declaration of Helsinki and approved by the Institutional Review Board of Asociación para Evitar la Ceguera en México I.A.P. (RE-24-06).
Due to the retrospective nature of the study, the use of previously collected anonymized clinical data, and the absence of any intervention outside routine clinical practice, the requirement for specific informed consent for this study was waived by the Institutional Review Board.
All patients admitted to our institution routinely sign a general informed consent authorizing the use of anonymized medical information for academic and research purposes. Patient confidentiality was strictly maintained throughout the study in compliance with institutional policies, the Mexican Federal Law for the Protection of Personal Data in Possession of Individuals (NOM-024-SSA3-2010), and the Health Insurance Portability and Accountability Act (HIPAA) regulations.
Generative artificial intelligence (AI) was not employed in the development of the manuscript’s conceptual content. However, AI-assisted tools were used to support spelling correction, grammar refinement, and readability improvements.
Retrospective, case-control study. We reviewed all electronic medical records of patients aged 18 years or older with a clinical diagnosis of acute endophthalmitis, including post-surgical, post-intravitreal injection, post-traumatic, bleb-associated, and cases secondary to corneal suture removal. All patients underwent pars plana vitrectomy between January 2017 and December 2024.
Patients were grouped according to whether a 0.025% povidone iodine irrigation solution or a standard balanced saline solution (BSS) was used during surgery. Following vitrectomy, all patients received at least three doses of intravitreal antibiotics administered every 48 hours (moxifloxacin 500 mcg/0.1 mL and dexamethasone 100 mcg/0.1 mL). In cases demonstrating inadequate clinical improvement or microbiological evidence suggesting resistance, treatment was modified to intravitreal vancomycin 1.0mg/0.1 mL and ceftazidime 2.25 mg/0.1 mL with dexamethasone 100 mcg/0.1 mL. Treatment began immediately after surgery and continued every 48 hours during follow-up until resolution of endophthalmitis. We excluded records of patients with endophthalmitis associated with infectious keratitis, suspected chronic or endogenous endophthalmitis, incomplete or missing data, or loss to follow-up within three months after surgery; therefore, no imputation methods were required.
The PI-infused solution was prepared following Nakashizuka et al method In summary, 1.25mL of a 10% PI solution (Germisin, Altamirano Laboratories, Mexico City, Mexico) was added to a bottle of 500 mL of BSS (Alcon Laboratories, Fort Worth, TX) 15 minutes before trocar placement.4 A standard valved 23 or 25 gauge, three-port pars plana vitrectomy (Constellation system, Alcon Surgical, Fort Worth, TX) was performed by experienced vitreoretinal surgeons using a standardized technique and the same institutional treatment protocol. An undiluted dry vitreous sample was obtained in all cases for microbiologic analysis and culture. Vitrectomy was performed as completely as possible, including shaving of the vitreous base and elevation of the posterior hyaloid whenever feasible or safe.
From all records, we obtained the time to endophthalmitis inactivation (days), defined as the absence of hypopyon, corneal edema, and pain, without worsening of vitreous haze following vitrectomy. When applicable, we also recorded the time to endophthalmitis reactivation or recurrence (days), defined as the presence of any of the following within three months after vitrectomy: unchanged or decreased visual acuity (VA) by ≥5 ETDRS letters, unchanged or increased pain on the Visual Analog Scale (VAS) by ≥1 scale, increase or recurrence of hypopyon (mm), or an increase in vitreous haze by ≥1 grade.1,14 Best corrected visual acuity (BCVA) was recorded at three time points for all patients: pre-endophthalmitis (after the inciting surgery or event and before infection onset), basal (at the time of endophthalmitis diagnosis and prior to pars plana vitrectomy), and post-endophthalmitis (three months after vitrectomy). BCVA was reported in logMAR, being count fingers (CF) equivalent to 1.7 logMAR, hand movement (HM) to 2.0 logMAR, light perception (LP) to 2.3 logMAR, and no light perception (NLP) to 3.0 logMAR.
At one week of follow-up, slit-lamp findings involving the cornea, anterior chamber, lens, and retina were analyzed to assess postoperative findings potentially associated with ocular toxicity.
Iritis was identified by the presence of anterior chamber cells and/or flare, according to the Standardization of Uveitis Nomenclature (SUN) classification. When appropriate, cataract progression was determined by comparing preoperative and postoperative lens opacities using the Lens Opacification Classification System (LOCS) III. Macular edema and retinal necrosis were assessed using spectral domain optical coherence tomography (Spectralis, Heidelberg Engineering, Heidelberg, Germany) and wide-field fundus photography.5,6
As this was a retrospective study including all eligible consecutive cases during the study period, no a priori sample size calculation was performed, and masking of surgeons and outcome assessors was not feasible. Statistical analyses were performed using IBM SPSS Statistics software (version 25) and JAMOVI software (2.7). General demographic data and variable descriptions were summarized using measures of central tendency and dispersion. The normality of all the variables was assessed using the D’Agostino–Pearson omnibus test. Continuous variables were analyzed using Student’s t-test or the Mann–Whitney U-test, as appropriate. Categorical variables were analyzed using the chi-square test or Fisher’s exact test, when applicable. A significance level (alpha) of 0.05 was used to determine statistical significance.
Results
We reviewed a total of 92 records that met the inclusion and exclusion criteria: 48 in the study group (0.025% PI-infuse PPV) and 44 in the control group (BSS-PPV). General demographic data and group characteristics are summarized in Table 1. The mean age in both groups was approximately 61 years. Sex and laterality of the affected eye were evenly distributed between groups.
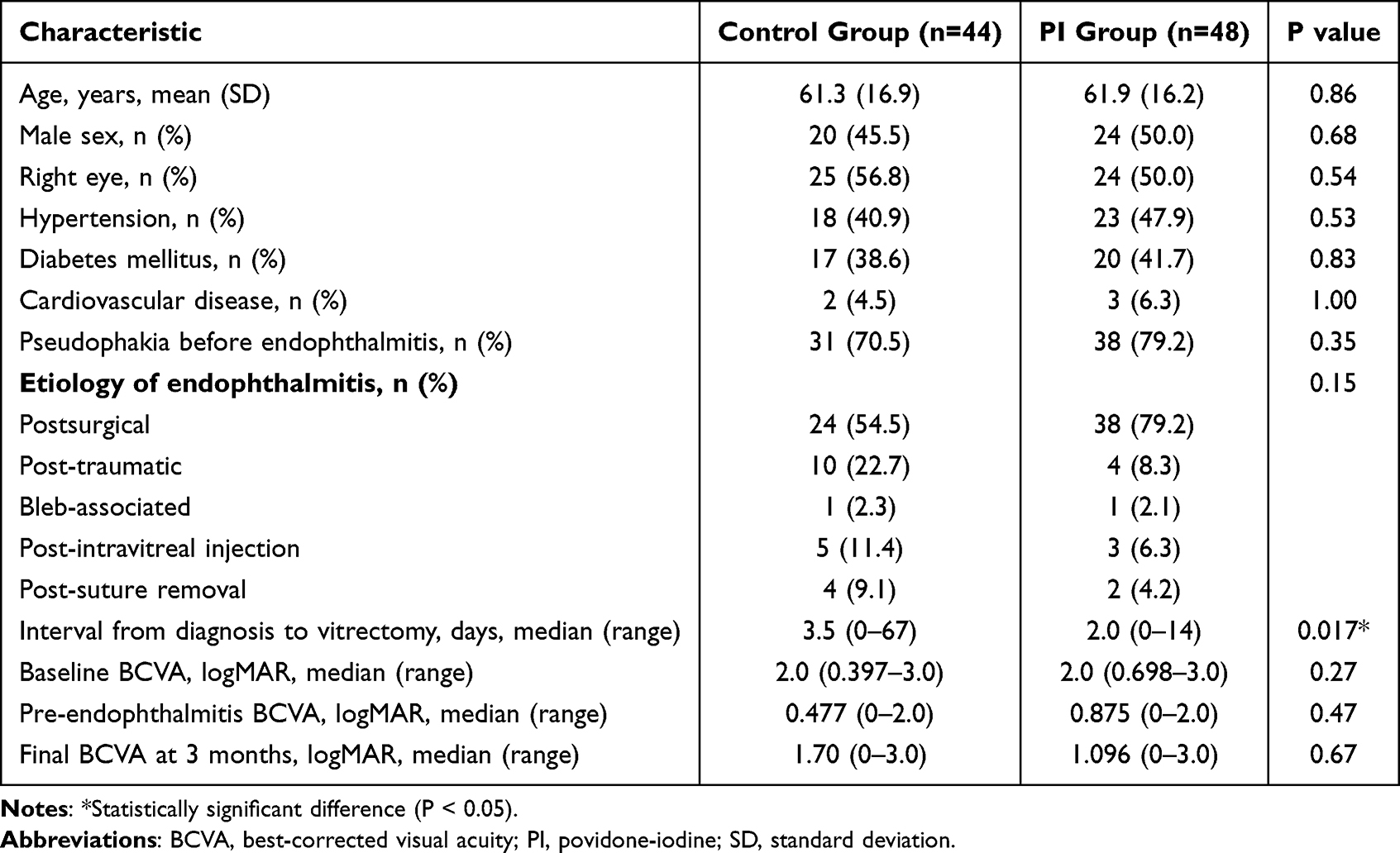 |
Table 1 Baseline Characteristics of Patients with Acute Endophthalmitis |
Pre-endophthalmitis pseudophakia was present in approximately 70% of patients in both groups. The most frequent cause of endophthalmitis was post-surgical, primarily following phacoemulsification, followed by combined procedures (phacoemulsification with pars plana vitrectomy). The mean interval between clinical diagnosis of endophthalmitis and PPV was significantly shorter in the study group (2 days) compared to the control group (3.5 days; p = 0.01).
Microbiological analysis from vitreous samples revealed predominantly gram-positive organisms in both groups, most commonly Staphylococcus epidermidis and Staphylococcus aureus. No major qualitative differences in microorganism distribution or apparent virulence patterns were identified between groups. Antibiotic susceptibility profiles generally demonstrated sensitivity to fluoroquinolones, followed by vancomycin and ceftazidime sensitivity in culture-positive cases.
There was no statistically significant difference in BCVA between groups at any evaluated time point. Mean BCVA at 3 months was logMAR 1.096 in the PI group and logMAR 1.70 in the control group (p = 0.67).
At the 1-week follow-up, resolution of endophthalmitis was achieved in 68.8% of patients in the study group and 65.9% in the control group (p = 0.83). Table 2 summarizes the clinical outcomes and postoperative ocular findings observed in both groups.
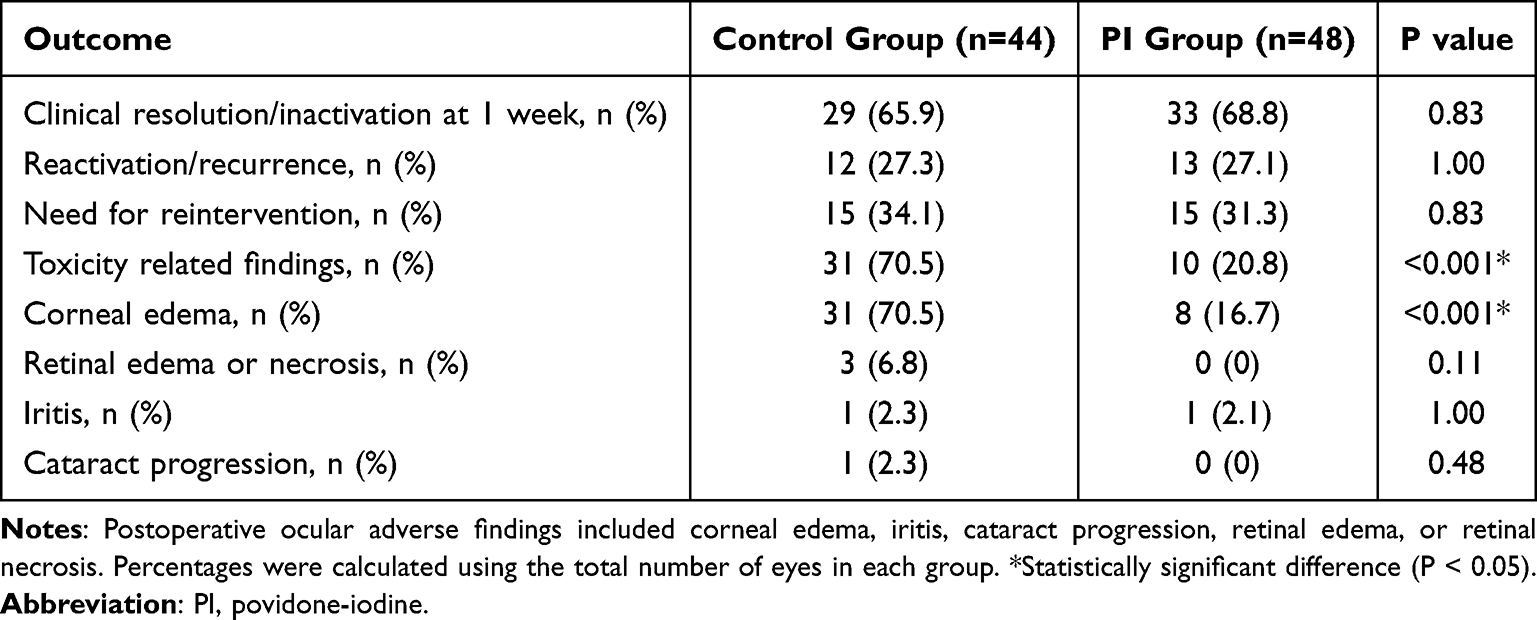 |
Table 2 Clinical Outcomes and Postoperative Ocular Findings |
Fewer postoperative findings potentially associated with ocular toxicity were observed in the PI group compared with controls (20.8% vs. 70.5%; p <0.001). Corneal edema was the most common postoperative ocular finding in both groups and occurred significantly less frequently in the PI group (16.7% vs. 70.5%; p <0.001) (Table 2).
An exploratory subgroup analysis was performed including only patients with post-phacoemulsification endophthalmitis, representing the most homogeneous cataract-surgery subgroup in the cohort. Seventeen eyes in the PI group and twenty eyes in the control group met these criteria. Clinical resolution was achieved in 70.6% of eyes in the PI group and 50.0% of eyes in the control group (p=0.32). Rates of reactivation (29.4% vs 25.0%, p=1.00) and reintervention (17.6% vs 30.0%, p=0.46) were also comparable between groups. However, corneal edema was significantly less frequent in the PI group (11.8% vs 60.0%, p=0.006). Overall, the subgroup analysis demonstrated a pattern of results consistent with that observed in the full cohort.
Discussion
Acute endophthalmitis remains a vision-threatening ophthalmologic emergency despite advances in antimicrobial therapy and vitreoretinal surgery. In this retrospective case-control study, the use of 0.025% PI as an intraoperative irrigation solution during PPV appeared to be safe when combined with intravitreal antibiotics, achieving infection control and visual outcomes comparable to those obtained with standard BSS.1–3
The most notable finding of the present study was the significantly lower frequency of toxicity-related findings in the PI group despite the theoretical concern regarding intraocular antiseptic toxicity. Corneal edema was the most common finding in both groups; however, it occurred substantially less frequently among patients receiving PI infusion. This observation was unexpected and suggests that appropriately diluted PI may not increase ocular toxicity when used intraoperatively. Several factors may explain this result. First, patients in the study group underwent vitrectomy significantly earlier than those in the control group (2 vs. 3.5 days), potentially reducing the duration of intraocular inflammation and tissue exposure to infectious damage. Second, the continuous irrigation and meticulous dilution protocol may have maintained PI concentrations within the previously reported safe therapeutic range.4,5 Finally, the possibility of selection bias inherent to the retrospective design cannot be excluded.
Although no statistically significant differences were identified regarding clinical resolution of endophthalmitis, final BCVA, or recurrence rates, the results suggest that PI infusion did not compromise infection control or visual outcomes when compared with standard BSS irrigation. The earlier timing of surgery in the study group may have contributed to these findings, as prompt vitrectomy has been associated with improved visual outcomes and reduced inflammatory damage in severe endophthalmitis.1–3
Our findings are consistent with previous experimental and clinical studies supporting the intraocular use of diluted PI. Prior investigations have demonstrated bactericidal activity, favorable visual outcomes, and absence of significant retinal or ocular toxicity when concentrations ranging from 0.013% to 0.027% were employed during vitrectomy.4,5,9 Experimental studies have further shown no significant electroretinographic or histopathologic abnormalities at these concentrations.7 More recent clinical experience has also suggested that intraocular PI may be safe when appropriately diluted and combined with standard antimicrobial therapy.15 Collectively, the available evidence and our results support the feasibility of PI as an adjunctive intraoperative antiseptic in the management of endophthalmitis.
The potential role of PI is particularly relevant in the current era of increasing antimicrobial resistance. Unlike conventional antibiotics, PI possesses broad-spectrum activity against bacteria, fungi, viruses, and protozoa, while no clinically relevant microbial resistance has been reported.4,5,8,10,11 Additionally, it is inexpensive, widely available, and does not require microbiological identification prior to use. These characteristics make PI an attractive adjunctive therapeutic option, particularly in resource-limited settings or when microbiological results are delayed.
To address the potential confounding effect of heterogeneous endophthalmitis etiologies, an exploratory subgroup analysis restricted to post-phacoemulsification endophthalmitis was performed. Although no significant differences were observed in clinical resolution, reactivation, or reintervention rates, the lower frequency of corneal edema remained significant in the PI group. While this finding should be interpreted cautiously given the limited sample size and retrospective design, it suggests that the observed difference in postoperative ocular findings was not solely attributable to etiologic heterogeneity.
Several limitations should be considered when interpreting our findings. The retrospective design, relatively small sample size, and lack of randomization may have introduced confounding factors and selection bias. The significantly shorter interval between diagnosis and surgery in the study group may have influenced both visual and toxicity-related outcomes. Furthermore, corneal edema and anterior segment inflammation may result not only from intraocular interventions but also from the underlying infectious and inflammatory process itself, limiting their specificity as markers of procedure-related toxicity.
Standardized specular microscopy measurements were not consistently available, restricting objective assessment of endothelial toxicity. In addition, the limited number of culture-positive cases precluded a robust comparative analysis of microbial spectrum, virulence and antimicrobial susceptibility patterns between groups. Moreover, the relatively short follow-up period was adequate for evaluating infection resolution and short-term visual outcomes but may not fully capture late recurrence or delayed ocular toxicity.
The observed reduction in postoperative findings potentially associated with ocular toxicity should be interpreted cautiously, as no multivariable adjustment or propensity-score analysis was performed, residual confounding cannot be excluded and the observed associations should not be interpreted as evidence of causality. Finally, the high baseline prevalence of pseudophakia reduced the usefulness of cataract progression as an indicator of ocular toxicity.
Conclusion
Within the limitations of this retrospective, non-randomized case-control study, 0.025% povidone-iodine irrigation during PPV was not associated with worse short-term anatomical or visual outcomes compared with standard BSS irrigation. Although postoperative ocular adverse findings were less frequent in the PI group, this observation should be interpreted cautiously because of potential confounding, particularly the shorter interval between diagnosis and vitrectomy in the PI group. Prospective controlled studies with standardized toxicity assessment and microbiologic stratification are needed to determine whether PI irrigation provides additional therapeutic benefit.
Funding
No funds were allocated to the realization of this research.
Disclosure
Dr Raul Velez-Montoya reports grants from SUN Pharma, Bayer AG, and Alcon Lab, outside the submitted work. Dr Gerardo Garcia-Aguirre reports consulting fees from Astellas, Nidek, Alcon; Honoraria from Abbvie, Roche Genentech, Nidek, Bayer, and Alcon, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Velez-Montoya R, Monroy-Esquivel L, Ortiz-Guevara R, Quiroz-Mercado H, Fromow-Guerra J. Mexican Endophthalmitis Study Group. Alternative intravitreal antibiotics: a systematic review for consideration in recalcitrant or resistant endophthalmitis. Retina. 2023;43(9):1433–6. doi:10.1097/IAE.0000000000003773
2. Soliman MK, Gini G, Kuhn F, et al. International practice patterns for the management of acute postsurgical and postintravitreal injection endophthalmitis. Ophthalmol Retina. 2019;3(6):461–467. doi:10.1016/j.oret.2019.03.009
3. Forster RK. The endophthalmitis vitrectomy study. Arch Ophthalmol. 1995;113(12):1555–1557. doi:10.1001/archopht.1995.01100120085015
4. Nakashizuka H, Shimada H, Hattori T, et al. Vitrectomy using 0.025% povidone-iodine in balanced salt solution plus for postoperative endophthalmitis. Retina. 2015;35(6):1087–1094. doi:10.1097/IAE.0000000000000634
5. Nakashizuka H, Shimada H, Hattori T, et al. Intravitreal injection of 1.25% povidone iodine followed by vitrectomy using 0.025% povidone iodine irrigation. Transl Vis Sci Technol. 2019;8(1):21. doi:10.1167/tvst.8.1.21
6. Whitacre MM, Crockett RS. Tolerance of intravitreal povidone-iodine in rabbit eyes. Curr Eye Res. 1990;9:725–732. doi:10.3109/02713689008999567
7. Trost LW, Kivilcim M, Peyman GA, et al. The effect of intravitreally injected povidone-iodine on staphylococcus epidermidis in rabbit eyes. J Ocul Pharmacol Ther. 2007;23(1):70–77. doi:10.1089/jop.2006.0076
8. Liu C, Xu K, Hu Y, et al. Vitrectomy using 0.025% povidone-iodine irrigation for post-traumatic endophthalmitis. Front Surg. 2023;9:988776. doi:10.3389/fsurg.2022.988776
9. Mi X, Malbin B, Lin X. Intraocular povidone iodine during pars plana vitrectomy for severe and atypical endophthalmitis. Ophthalmic Surg Lasers Imaging Retina. 2021;52(9):485–490. doi:10.3928/23258160-20210820-01
10. Kitagawa Y, Shimada H, Nakashizuka H, et al. Intraocular lens implantation and vitrectomy using 0.025% povidone-iodine for bleb-related endophthalmitis. Int J Ophthalmol. 2020;13(9):1499–1502. doi:10.18240/ijo.2020.09.24
11. Huang D, Tran L, Li JY, et al. Povidone iodine-infused pars plana vitrectomy for severe Arthrographis kalrae fungal endophthalmitis. Am J Ophthalmol Case Rep. 2024;36:102207. doi:10.1016/j.ajoc.2024.102207
12. Choi MY, Ryu G, Moon D, et al. Four cases of 0.625% povidone-iodine intravitreal injection. J Ocul Retina. 2024;9(2):204. doi:10.21561/jor.2024.9.2.204
13. You H, Kim J. Endogenous endophthalmitis from urinary tract infection caused by Group B Streptococcus: a case report. Medicina. 2024;60(5):700. doi:10.3390/medicina60050700
14. Velez-Montoya R, Rivera-Cortes MA, Ledesma-Gil G, et al. Combined therapeutic penetrating keratoplasty and pars plana vitrectomy for infectious keratitis endophthalmitis. Cornea. 2023;42(7):805–814. doi:10.1097/ICO.0000000000003114
15. Machida Y, Nakashizuka H, Onoe H, et al. Intravitreal povidone-iodine injection and low-dose antibiotic irrigation for infectious endophthalmitis. Pharmaceutics. 2025;17(8):995. doi:10.3390/pharmaceutics17080995
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Post-Cataract Surgery Endophthalmitis Prophylaxis Survey in Thai Ophthalmologists
Kasetsuwan P, Chansangpetch S, Pruksacholavit J, Surawatsatien N, Pongsaschareonnont PF, Reinprayoon U
Clinical Ophthalmology 2025, 19:4585-4596
Published Date: 12 December 2025