Back to Journals » Journal of Asthma and Allergy » Volume 15
Parents’ Decision Making During Their Child’s Asthma Attack: Qualitative Systematic Review
Authors Goddard BMM, Hutton A, Guilhermino M, McDonald VM ![]()
Received 4 October 2021
Accepted for publication 3 July 2022
Published 6 August 2022 Volume 2022:15 Pages 1021—1033
DOI https://doi.org/10.2147/JAA.S341434
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Amrita Dosanjh
Bernadette MM Goddard,1,2 Alison Hutton,1 Michelle Guilhermino,1 Vanessa M McDonald1,3,4
1School of Nursing and Midwifery, College of Health, Medicine and Wellbeing, University of Newcastle, Callaghan, NSW, Australia; 2Paediatric Respiratory Department, John Hunter Children’s Hospital, New Lambton Heights, NSW, Australia; 3Centre of Excellence Treatable Traits, Level 2, West Wing, Hunter Medical Research Institute. Lot 1 Kookaburra Circuit, New Lambton Heights, NSW, 2305, Australia; 4Department of Respiratory and Sleep Medicine, John Hunter Hospital, New Lambton Heights, NSW, Australia
Correspondence: Vanessa M McDonald, Centre of Excellence Treatable Traits, Level 2, West Wing, Hunter Medical Research Institute, Lot 1 Kookaburra Circuit, New Lambton Heights, NSW, 2305, Australia, Tel +61 2 40420146, Fax +61 2 40420046, Email [email protected]
Objective: To conduct a systematic review and synthesis of qualitative evidence exploring the factors that influence a parent’s decision to seek medical assistance while their child is having an asthma attack.
Methods: Studies were included if they used qualitative methodologies and explored parent or carers’ experience of caring for a child (2 to 12 years) during an acute asthma attack at home or in the community. We searched MEDLINE (OVID interface, 1948 onwards), EMBASE (OVID interface, 1980 onwards) and CINAHL (EBSCO) electronic databases. Quality appraisal was assessed by the Critical Appraisal Skills Program CASP for qualitative research, and the qualitative studies in this review were analyzed by thematic synthesis.
Results: From 4798 identified studies, 17 met the inclusion criteria. Synthesis revealed two distinct processes used by parents to aid their decision to seek medical intervention for their child. The first, past experiences informing future decisions and secondly facilitators that drive parents’ to actively pursue medical help.
Conclusion: This review highlights the importance of providing asthma education that not only focuses on the provision of information on symptoms, triggers, medication, and device use but asthma education that targets parents’ unique experience. Using a family strength approach education can impact parents’ future behavior when deciding to seek medical assistance for their child when experiencing an asthma attack. There was not a specific funding source, which supported this review. This review was registered with PROSPERO Identification Number CRD4201912740.
Keywords: childhood wheeze, caregiver, choice behavior, medical help
Introduction
Asthma is the most common chronic disease in childhood with worldwide prevalence rates over 10%. It is a leading cause of hospital admissions and emergency department presentations in children.1–4 Despite availability of effective treatment, children with asthma continue to experience acute attacks, hospitalization and even death.5 The rate of asthma deaths is similar between Australia, United Kingdom, New Zealand and the United States of America.6 Arroyo et al (2018) observed an increase in pediatric asthma deaths from 2003 to 2015 and disturbingly most of these deaths were preventable.5 A National Review of Asthma Deaths (2014) in the UK found 65% of those who died had personal, environmental, and family-related factors that may have contributed to their death. Preventable factors included excessive use of short-acting relievers, exposure to tobacco smoke, non-adherence to medical advice and lack of medical review.7 The expert panel from the UK review of asthma deaths found inadequate recognition of the risk of death was an avoidable factor in 70% of children and 83% of young people in primary care.7
These data highlight the need to explore parents’ experiences of caring for their children when having an asthma attack, the decisions they make, and the actions they take to seek medical assistance. To date, there is an abundance of qualitative research investigating the parent’s overall experience of caring for a child with asthma, but there is a fundamental knowledge gap in understanding the barriers and facilitators that impact parents’ decisions to seek medical help during periods of high symptom severity. The objective of this systematic review of qualitative studies, was to identify the parents’ perceived factors that influence their decision to present to hospital when their child is having an asthma attack at home or in the community.
Method
Eligibility Criteria
The inclusion and exclusion criteria were defined in terms of study population, phenomenon of interest, context, study design and written in the English language (Table 1). The screening of the abstracts and full text articles were assessed against the inclusion and exclusion criteria.
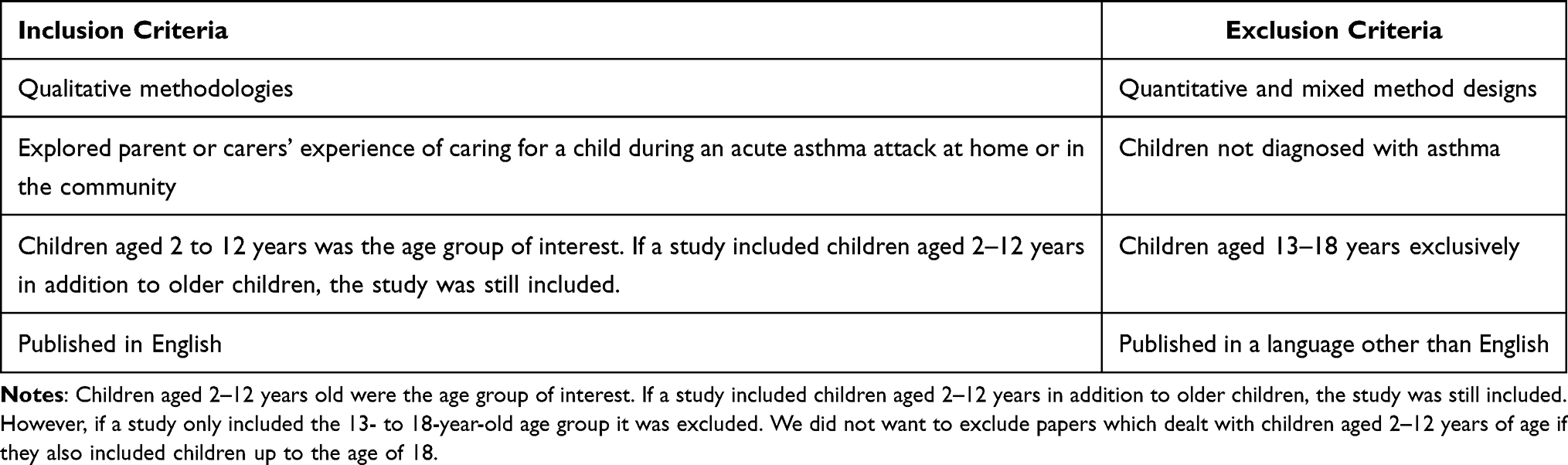 |
Table 1 Inclusion and Exclusion Criteria for Studies Included in the Systematic Review |
Information Sources
The search was initially conducted in April 2019 and updated in August 2021 and included studies published in the electronic databases MEDLINE (OVID interface, 1948 onwards), EMBASE (OVID interface, 1980 onwards) and CINAHL (EBSCO) electronic databases. The electronic database search was supplemented by searching grey literature.8–10 After screening the included studies, their reference lists were hand searched to identify other relevant articles for inclusion.
Search Strategy
See online Supplementary Table 1 for the search strategy.
Data Extraction and Synthesis
Covidence Systematic Review Software (Veritas Health Innovation, Melbourne, Australia) was used to screen each abstract and full text article against the inclusion and exclusion criteria to determine if a study was eligible. Two reviewers, BG and, jk MG, worked independently to decide which primary paper was to be included in the review. Discrepancies were resolved by a third reviewer (AH or VMcD). Data extraction from the included articles was an ongoing process, of reading and rereading the papers, extracting data, checking data and synthesizing the information.11 Extracted data included participant characteristics, country, culture and social context, study design, aims and key findings.
The qualitative studies in this review were analyzed by thematic synthesis. NVivo software (Version 12.6, 2018, QSR International, Melbourne Australia) was used to organize the data. Reviewer BG coded parent quotes and author’s analysis from the included studies and entered them into NVivo. From this iterative process, homogeneous codes were identified and grouped to form key concepts which remained true to the primary data. These key concepts were summarized as codes which were synthesized inductively until two main themes emerged.12 As part of the iterative process, the codes and themes were examined and checked with AH, VMcD and MG. Discussion between the authors ensued until agreement was met.13–15
Covidence systematic review (Veritas Health Innovation, Melbourne, Australia) was used to manage articles and facilitate the screening process.
Quality Assessment
Quality appraisal was assessed by the Critical Appraisal Skills Program CASP for qualitative research.16 The CASP tool examines the quality of a paper using several criteria. Section A examined the validity of the study, section B assessed ethical considerations and the rigor of data analysis and section C evaluated the overall value of the research. Studies were not excluded from the review based on quality but rather assessed to facilitate critical review.17 Each study was independently reviewed by two reviewers (BG and MG), when discrepancies occurred, they were discussed, and all were resolved between BG and MG.
See online Supplementary Table 2 for the overall CASP quality ratings.
Terminology
In this report, acute asthma episodes will be termed attacks except when primary studies described these as flares or exacerbations. Parents, caregivers, and guardians will be referred to as parents.
Results
Study Selection
The literature search yielded 4798 citations. There were 1319 duplicates removed and 3406 studies were irrelevant to our research question. Full text review was performed for 73 articles to assess eligibility for inclusion. After completion of the screening process 17 citations were included in this systematic review. The PRISMA diagram is presented in Figure 1.18 The study characteristics of country of origin, aims, design, cultural and social context, population, and findings can be found in Table 2 Study Characteristics.
 | 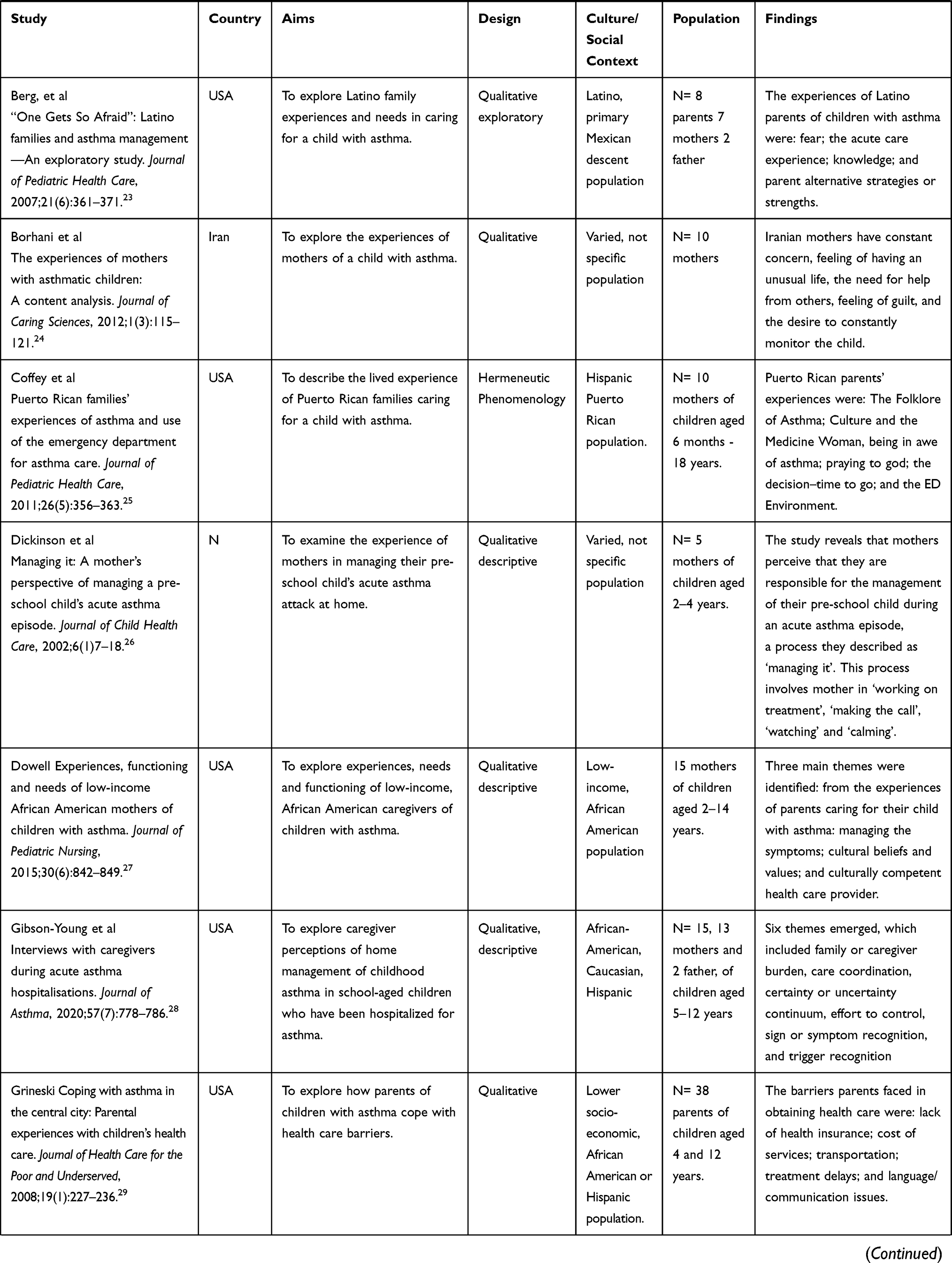 | 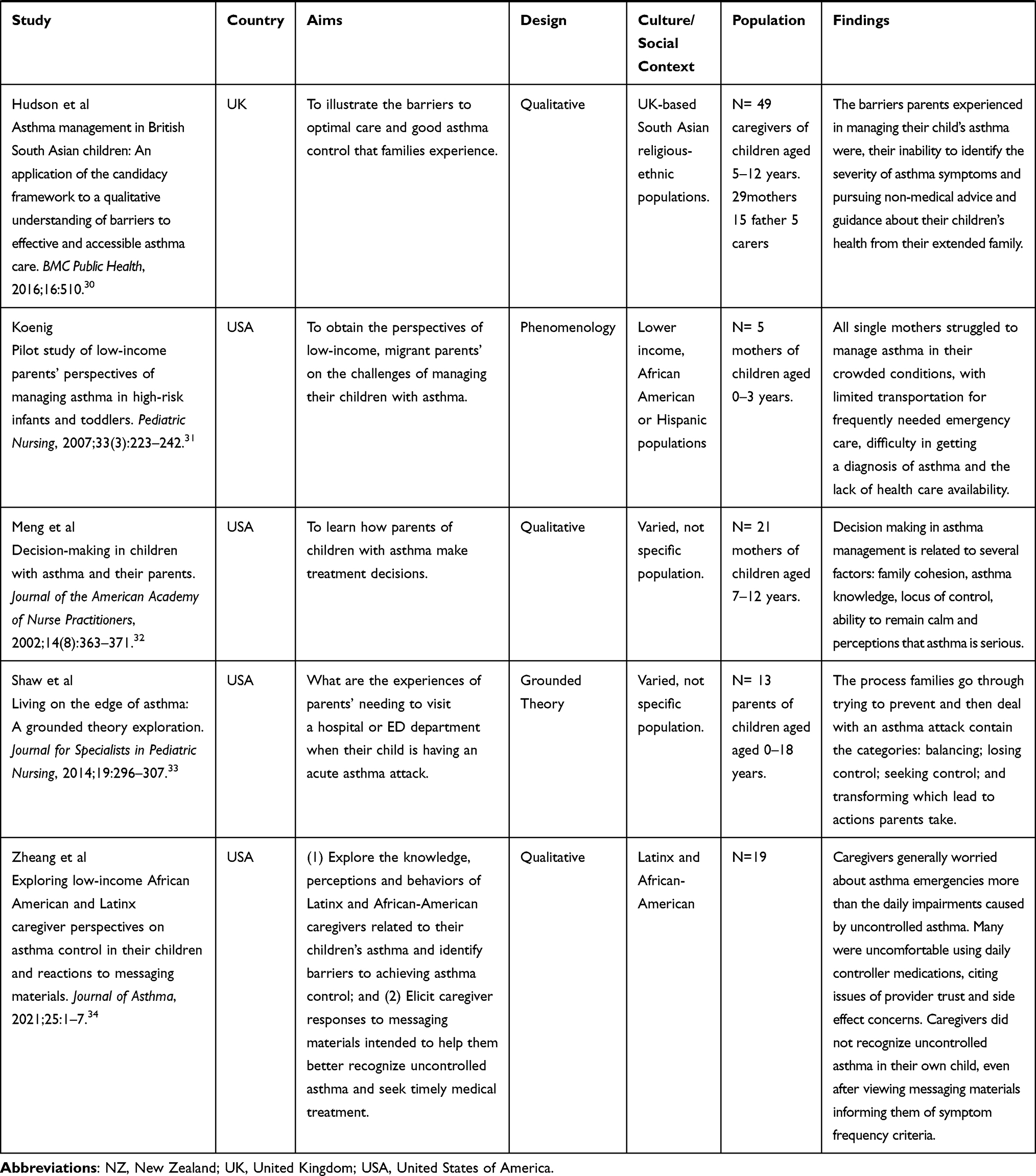 |
Table 2 Study Characteristics |
 |
Figure 1 PRISMA flow diagram of included studies. Notes: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM, et al.The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. Creative Commons.18 |
Characteristics of Included Studies
The 17 included studies were published (Table 2). These studies included 303 parents/caregivers/adults, of which 157 were mothers, 29 fathers, and five were secondary carers. Gender was not specified in 104 parents. Children of these parents/carers were aged 2–16 and all had been diagnosed with asthma. In the study by Alzayer et al, two populations were recruited, one being adults with asthma and the second, parents of children with asthma. For this review, we have only described the data relating to the parents of children with asthma. N = 19, n = 11 parent of child with asthma, n = 8 adult with asthma.
Results of Synthesis
Data synthesis revealed two overarching themes relating to parental decision making for seeking medical assistance when their child is having an asthma attack. These two themes, (1) “past experiences that inform future decisions” and (2) “facilitators that drive parents to actively pursue medical help”, work in synergy with each other due to their interrelationship.
The first theme “past experiences that inform future decisions” provides a background that underpins a parent’s decision to seek medical help. In this theme, there were three subthemes (i) the challenge parents faced in perceiving their child’s asthma symptoms (ii) parents’ ability to manage their child’s asthma and (iii) health-care professionals’ (HCP) relationship with parents (Figure 2). The second overarching theme was “facilitators that drive parents” to actively pursue medical help’. Within this theme there were also three subthemes, (i) socioeconomic characteristics that impact parents’ decision to seek help, (ii) identifying and acting on severity and (iii) cultural characteristics that impact parents’ decisions to seek help (Figure 3).
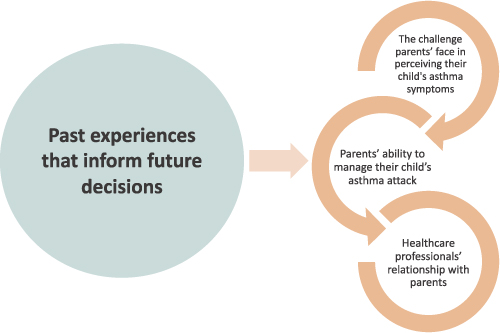 |
Figure 2 Themes and subthemes of past experiences that inform future decisions. |
 |
Figure 3 Themes and subthemes: facilitators that drive parents’ to actively pursue medical help. |
Theme One: Past Experiences That Inform Future Decisions
All the included studies described parents’ experiences of caring for their child during an asthma attack and it was evident that parents’ past asthma experience informed the management of their child’s current asthma episode.19–35 The three key subthemes and their interrelationship with each other are presented in Figure 2.
Theme One, Subtheme One: The Challenges Parents Face in Perceiving Their Child’s Asthma Symptoms
This subtheme represents the parents’ difficulty in assessing the severity of their child’s symptoms during an asthma attack. This issue and the rationale for it was identified in ten studies.21–23,25,28–30,33,34 Parents identified that managing symptoms before their child was formally diagnosed, was a particular challenge. Reasons offered were that they had to respond to symptoms without understanding the trajectory of an asthma attack or treatment options such as bronchodilators.22,23,29–31 Hudson et al investigated the health outcomes of South Asian children compared to white children in the UK and reported that 13 of the 30 families stated that they were not aware that their child had been diagnosed with asthma, despite being prescribed asthma treatment and being enrolled in an asthma study. Furthermore, the experience of families caring for their child with undiagnosed asthma was found to impact their future actions when deciding to present to a health-care facility.30 The lack of diagnosis identified in five studies came from lower socioeconomic or culturally diverse populations.21,23,29–31 The culturally diverse populations investigated in three of the studies were 1) American Latino, 2) African American and 3) Latino and African American populations.23,29,31 The remaining two studies examined an Australian cohort, and a South Asian community residing in the UK.21,30 These vulnerable populations had an increased challenge in obtaining a diagnosis due to the parents’ inability to effectively navigate the health-care system and the fragmentation of care they received.
Every time there is a different doctor! Every time different medicine! They cannot reach to a [diagnosis] conclusion or there is no solid result or a procedure to follow ….30
Some parents had difficulty recognizing severe symptoms and the level of respiratory distress experienced by their child during asthma attacks.22–25,30,32,33 A participant from the study reported by Meng and McConnell stated they had “difficulty distinguishing a pseudo attack from a true attack”.32 Another parent stated that they did not perceive their child’s blue lips to be a symptom of concern.35 The lack of recognition of the child’s asthma symptoms and severity had a significant influence on parents’ decision to seek help, one parent described:
“When I decided she needed to go (to hospital), she was very listless, and it was hard to rouse her out of more of a stupor”.33
Theme One, Subtheme Two: Parents’ Ability to Manage Their Child’s Asthma Attack
Parents’ asthma management experience and ability was addressed in all 17 studies and several barriers to asthma management were identified.19–34 A notable aspect of this subtheme were the limited skills and resources that parents held. Access to a vital asthma treatment such as a reliever inhaler was discussed in four studies.19,22,29 Parents commented that they would forget to take the reliever inhaler with them when going out, they found it embarrassing to use it in public or considered it unnecessary to keep it at daycare and school. A parent offered that reason for not leaving the puffer at childcare “ … she’s just a spry little girl and um, she’s also very tough”.35 One study found a misconception of the parent confusing the preventive with the reliever puffer.28 Some parents commented that they had difficulty in obtaining new inhalers if they were lost or empty because they did not have a prescription or the money to purchase the puffer.22,29
We get paid at the end of the week and sometimes we need to wait to get [the prescription] refilled. But then he’s struggling and it’s a no-win situation because if he misses a dose, he’s irritated and can have trouble breathing.29
Moreover, Archibald et al identified that “the majority of parents reported that at some point since diagnosis, they had not known how and when to properly use the inhaler”.35
Another gap that affected the management of an asthma attack was related to asthma action plans. Parents identified not having a plan or knowing where it was located or how to follow it.19,22,25–27,31,33
A notable aspect of this subtheme was parents’ lack of knowledge, which challenged their ability to care for their child.19–23,32,33 A participant commented
What makes it hard is the lack of information. If one would be well informed, one could deal with it better … [What’s hard is] the not knowing what to do, to see your child sick and not being able to do nothing. [SIC]23
This lack of parental knowledge had a pervasive impact on all aspects of the child’s asthma care.35 It ranged from not knowing what to do through to the developmentally inappropriate expectation that their child was able to care for their own asthma without parental input. In fact, Meng and McConnell reported that parents perceived the notion of “self-management” to mean that the child should manage their own asthma.32
Theme One, Subtheme Three: Health Care Professionals (HCP) Relationship with Parents
The studies included in this review described both positive and negative relationships between the health-care professionals (HCP) and parents. This relationship could affect the parents’ future actions when caring for their child during an acute asthma attack.20–27,29–31,33 Additionally, parents’ future actions were found to be affected by their previous hospital experience which could delay or expedite their decision to seek help. Barton et al identified that some parents who were dissatisfied with their previous hospital experience delayed presenting to the health-care facility.21 In contrast, other parents stated “Once you’re there [at the ED], you’re relieved because you know it’s not your responsibility anymore. They’ve got to fix him, you don’t have to anymore”.21 Another parent exclaimed, “We get quiet time when we’re staying (in the hospital), we get quiet time and we put all of the responsibilities on you all.”.33
The amount and quality of education parents received was described in eight articles.19,20,22,23,26,30,33 Challenges described by some parents included a lack of advice, and inconsistent, contradictory, or incorrect asthma education by HCP.
They say, here’s a pump, here’s a chamber, she needs to take, you know four times day of whatever it is, um, but no one actually stops to show you how to use it.35
A particular challenge for the un-informed was the difficulty knowing what you need to know “I can’t even articulate what I think I should know right now … or what I would like some help with”.35
Language and communication were found to be a challenge for parents especially if English was a second language, or if they experienced poverty or had poor health literacy.23,27,29
There are some doctors that don’t know Spanish and I cannot speak with this person and say, ‘My child has this, has that, this happens, take care of him quickly, and things like that’.23
Conversely, participants from ten studies identified that they had a positive relationship with their HCP with whom they trusted and valued.20,21,24–27,29,30,33
I just feel so much more prepared since having this doctor (asthma specialist), um like everything’s just under control and the doctor’s really following him ….33
Theme Two: Facilitators That Drive Parents’ to Actively Pursue Medical Help
The facilitators that drive parents to actively pursue medical help and the three subthemes that emerged from the included studies are presented in Figure 3. The decision to seek medical help was termed by parents as “making the call”, “time to go” or “point of no return”. This was a decision parents did not take lightly and was thought to be a complex, difficult, and stressful component of parents’ care for their child during an asthma attack.21,25,26,33
Theme Two, Subtheme One: Socioeconomic Characteristics That Impact Parents’ Decision to Seek Help
Socio-economic status was found to influence parents’ asthma management in the context of poverty and access to health care.22,23,29–32 Delaying a treatment decision was prominent in low income, single parent families or when a parent’s job restricted their ability to care for their child.32 Access to health care was another influencing factor for parents when choosing to seek medical assistance. The cost of attending emergency department (ED), lack of transport, money for medications and lack of health insurance were identified as barriers for parents when accessing the health-care system.22,23,29–32 Some parents used ED as a resource to obtain inhaled medications or scripts due to lack of funds or prescriptions: “Sometimes I will literally have to bring him to the emergency room just to get another script [prescription]”.22
Theme Two, Subtheme Two: Identifying and Acting on Asthma Severity
Asthma acuity or severity as it was reported was the main indicator used when deciding to seek medical help, so when a parent has difficulty identifying the severity of the asthma attack, the decision to act in a timely manner is compromised, which is a significant threat to a child’s wellbeing.21–23,25,30,33 A participant was noted to say that their child was “close to having a cardiac arrest” or they were “urgently instructed to seek emergency medical care”.35
Theme Two, Subtheme Three: Cultural Characteristics That Impact Parents’ Decision to Seek Help
Cultural influence was an issue discussed in seven studies which specifically recruited parents from culturally diverse backgrounds.21–24,27,29,30 They described how coping with a sick child is difficult, but for a migrant family the burden is greater due to several barriers associated with culturally competent care and ED presentations.27 Berg et al found that Latino parents felt more distressed after arriving in ED because they felt helpless, and that the system had failed them. A mother was dismayed at the lack of information she was given.
” … for someone to come and say I am going to explain the procedure, nothing is going to happen to your child. All they would say is “Calm down, everything will be fine”.23
In the study by Berg et al, a mother stated
This woman told me I had to have brought her earlier … I was upset. I had nerves. I had taken my child very sick to that place and I had another child with me too … I don’t think it was right for the woman to treat me like that … I have seen the receptionists, the nurses talking, laughing at us and they have us waiting until they feel good and ready to call us.23
Mothers with English as a second language or who only spoke their native tongue found communication barriers ubiquitous.29 Some parents felt they were not respected by ED staff and some EDs did not provide culturally competent care.22,24,27,29,30 However, this was not always the case. An African American mother described her primary care doctor,
He actually understands our cultural needs very well, he knows that people are different and react [SIC] in different ways you can’t treat everybody the same. So, he takes his time and listens to us very well.27
Discussion
This review identified factors that influenced parents’ decisions to present to hospital when their child is having an asthma attack. Overarching themes identified in our synthesis included, (i) parents’ previous experience that informs their future decision to seek medical assistance, and (ii) the facilitators that drive parents’ to actively pursue medical help. The synthesis of these data provides important insights into parental decision making during acute asthma attacks, and this understanding can inform potential strategies to help parent decision making to identify their child’s deterioration and to respond and manage asthma attack effectively.
Factors that emerged from the first theme, “parents” previous experience that informed their future decision’ were threefold, first the challenge parents faced in perceiving their child’s asthma symptoms, secondly parents’ asthma management knowledge and last, the parent health-care professional relationship. Past experiences not only influence decisions but also impacts the outcome of these decisions.36 This highlights the importance of understanding the parents’ perspectives, providing written action plans to guide parent decision making and effective self-management strategies for implementing such plans. Yoos et al found that symptom assessment is the basis for implementing asthma management at home as well as measuring its effectiveness. Therefore, it is important for parents to have the capacity to assess their child’s symptom intensity.37 A number of studies in this review support the notion that parents overestimate their child’s asthma control while underestimating the severity of worsening symptoms.37–41 Harrington et al found parents’ health literacy regarding asthma control impacted their child’s health outcomes and was associated with increased frequency of ED presentations and hospital admissions.42
An important finding within this review, is that parents’ asthma management is related to their knowledge, availability of resources and whether their child had an asthma diagnosis. Similarly, Sukartini et al found that education based on the beliefs and behaviors of parents’ increased their perception of the seriousness of their child’s symptoms.43 McDonald and Gibson’s review on adult asthma education concluded that for asthma education to change behavior and improve outcomes it needs to focus on self-management skills, which includes written asthma action plans, self-monitoring and regular medical review.44 Smith et al reported that parents needed knowledge in order to learn from their experiences of caring for their child when unwell.45
The relationship with HCPs has been found to both cloud and focus a parent’s opinion and actions on their help-seeking behavior. The relationship with HCP can impede or facilitate action in managing one’s asthma. The findings in our review are supported by Miles et al who conducted a systematic review of studies evaluating the barriers and facilitators of effective self-management in asthma. They concluded that HCPs need sound communication, provision of mutual trust and respect, creation of a partnership and personalized consistent advice.46 This finding is also consistent with the results found in adults with severe asthma.47 These data highlight the importance of effective parent-HCP professional relationships for both stable and acute asthma.
The facilitators that drive parents to actively pursue medical help was the second theme that emerged from the data synthesis. The factors from this theme were also threefold, (i) socioeconomic characteristics that impact parents’ decision to seek help, (ii) identifying and acting on severity and (iii) cultural characteristics that impact parents’ decision to seek help. For parents to take appropriate asthma action they need to be knowledgeable. Auger et al found that parents with greater asthma knowledge had an increased readmission rate to hospital compared to parents who demonstrated less knowledge.48 Auger et al postulated several reasons for this, one of which stated parents with increased asthma knowledge may decide to seek help more quickly.48 This notion was supported by Carroll et al who found that parents who were poor perceivers of asthma severity delayed taking action.38
Another important finding from this review is that socioeconomic and cultural factors can facilitate or hinder parents’ pursuit of medical aid.21–23,27,29–32 It is well known that social determinants of health (SDH) have a profound effect on an individual’s access to health services. Social determinants of health are the factors that impact an individual’s wellness, propensity for illness and injury and can strengthen or undermine a person’s or community’s health status.49 Our review found that cultural and socioeconomic factors such as unaffordability of health services, lack of transport, money for medications and lack of health insurance influenced parents’ decisions and actions which were governed by their SDH.22,23,29–32 This finding was supported by Bird et al who reported children from low-income families had been known to use ED as a free or inexpensive service.50 Lower socioeconomic status (SES) and race were also found to have lower accuracy rates for detecting children’s asthma symptom severity.37 Mudd et al postulated that lower income families significantly correlated with an increased sense of urgency to present to ED, which may result from limited resources to continue to manage the child at home.51 The studies in our review support the conclusion that cultural and socioeconomic factors did have an adverse consequence on a parent’s management of their child’s asthma.21–23,27,29–32 Therefore, it is a priority for asthma education and management services to ensure these vulnerable families receive education and supports that are targeted to their social, economic, and cultural needs.
The practice implications from this review suggest that parental asthma education requires a family strength approach which targets the parent’s previous experience and the impact this has on the child’s asthma management. Asthma education needs to be aimed at the individual’s health literacy level and be developed in partnership with the family to address their needs and health-care barriers. Approaches that involve an assessment of the parent’s “activation” level may help to personalize asthma self-management education more effectively.52,53
A strength of this review is the consolidation of the evidence that supports the notion that one’s past experiences impact on their future decisions. The findings from our review were corroborated across the studies providing evidence and support that the general themes of experience and actions were interlinked and impacted the health outcomes of children with asthma.
The limitations were that the demographics of the included studies varied, with the majority originating in the United States of America.20,22,23,25,27–29,31–34 However, only two of these studies investigated a non-specific, general cohort and the remaining nine studies investigated socioeconomic and cultural factors affecting families and children with asthma. Besides, the findings from this review are difficult to transfer to other populations as the large proportion included specific cohorts from one distinct health-care system. This identifies a need for further research in other populations.
Conclusion
Our review highlights the importance of past experiences informing future decisions and the facilitators that drive parents’ to actively pursue medical help. The parents’ experiences were a foundation built from parental skills, knowledge, and beliefs which collectively informed future actions of parents when pursuing medical assistance for their child when having an acute asthma attack. Parents utilize their experiences to take actions as part of their decision-making process. This process creates the capacity for them to decide how they will manage periods of high symptom severity and when to seek help when their child’s asthma deteriorates. Understanding these processes highlights the importance of addressing parents’ experiences and how this effects their decision to seek help. These data can inform personalized self-management approaches to crisis management of children with asthma and the carers.
Registration and Protocol
In 2019, a systematic review protocol was registered with PROSPERO (CRD42019127405). The review methodology was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement, see figure 1.18
Disclosure
Professor Vanessa M McDonald reports grants, personal fees from GSK, grants, personal fees from Astra Zeneca, outside the submitted work. The authors report no conflicts of interest in this work.
References
1. Chung HS, Hathaway DK, Lew DB. Risk factors associated with hospital readmission in pediatric asthma. J Pediatr Nurs. 2015;30(2):364–384.
2. Australian Institute of Health and Welfare. Asthma Hospitalisations in Australia 2010-2011. Australian Institute of Health and Welfare; 2013.
3. Mallol J, García-Marcos L, Solé D, Brand P, Group. ES. International prevalence of recurrent wheezing during the first year of life: variability, treatment patterns and use of health resources. Thorax. 2010;65(11):1004–1009.
4. Uijen JH, Schellevis FG, Bindels PJ, Willemsen SP. van der Wouden JC. Low hospital admission rates for respiratory diseases in children. BMC Fam Pract. 2010;9(11):76.
5. Arroyo A, Chee CP, Camargo CA, Wang NE. Where do children die from asthma? National Data from 2003–2015. J Allergy Clin Immunol Pract. 2018;6(3):1034–1036.
6. Australian Centre for Asthma Monitoring. Asthma in Australia 2011. Canberra Australia: Australian Centre for Asthma Monitoring; 2011.
7. Royal College of Physicians. Why Asthma Still Kills: The National Review of Asthma Deaths (NRAD) Confidential Enquiry Report. London: Royal College of Physicians; 2014.
8. Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. USA: Global Initiative for Asthma; 2018.
9. National Asthma Council Australia Asthma Australia. National Asthma Strategy 2018. Canberra: Health Do; 2018.
10. NSW Ombudsman. NSW Child Death Review Team Annual Report 2013. NSW Ombudsman; 2014.
11. Noyes J, Lewin S, et al. Chapter 5: extracting qualitative evidence. In: Noyes J, Booth A, Hannes K, editors. Supplementary Guidance for Inclusion of Qualitative Research in Cochrane Systematic Reviews of Intervention. Cochrane Collaboration Qualitative Methods Group; 2011.
12. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101.
13. Richards L. Handling Qualitative Data: A Practical Guide. SAGE Publications; 2006.
14. Coughlan M, Cronin P. Doing a Literature Review in Nursing, Health and Social Care.
15. Thomas J, Harden A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol. 2008;8:45.
16. Critical Appraisal Skills Programme. CASP (Qualitative) Checklist. 2022; Available from: www.casp-uk.net:.
17. Long HA, French DP, Brooks JM. Optimising the value of the critical appraisal skills programme (CASP) tool for quality appraisal in qualitative evidence synthesis. Res Methods Med Health Sci. 2020;1(1):31–42.
18. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
19. Alzayer R, Almansour HA, Basheti I, Chaar B, Saini B. Asthma patients in Saudi Arabia – preferences, health beliefs and experiences that shape asthma management. Ethn Health. 2020;27(4):877–893.
20. Arcoleo K, Zayas LE, Hawthorne A, Begay R. Illness representations and cultural practices play a role in patient-centered care in childhood asthma: experiences of Mexican mothers. J Asthma. 2015;52(7):699–706.
21. Barton C, Sulaiman N, Clarke D, Abramson M. Experiences of Australian parents caring for children with asthma: it gets easier. Chronic Illn. 2005;1(4):303–314.
22. Bellin MH, Land C, Newsome A, et al. Caregiver perception of asthma management of children in the context of poverty. J Asthma. 2017;54(2):162–172.
23. Berg J, Anderson NLR, Tichacek MJ, Tomizh AC, Rachelefsky G. “One Gets So Afraid”: latino Families and Asthma Management-An Exploratory Study. J Pediatr Health Care. 2007;21(6):361–371.
24. Borhani F, Asadi N, Mohsenpour M. The experiences of mothers with asthmatic children: a content analysis. J Caring Sci. 2012;1(3):115–121.
25. Coffey J, Cloutier M, Meadows-Oliver M, Terrazos C. Puerto Rican families’ experiences of asthma and use of the emergency department for asthma care. J Pediatric Healthcare. 2012;26(5):356–363.
26. Dickinson AR, Dignam D. Managing it: a mother’s perspective of managing a pre-school child’s acute asthma episode. J Child Health Care. 2002;6(1):7–18.
27. Dowell JA. Experiences, functioning and needs of low-income african american mothers of children with asthma. J Pediatr Nurs. 2015;30(6):842–849.
28. Gibson-Young LM, Aroian KJ, Weglicki LS, Lang JE, Norris CL. Interviews with caregivers during acute asthma hospitalisations. J Asthma. 2020;57(7):778–786.
29. Grineski S. Coping with asthma in the central city: parental experiences with children’s health care. J Health Care Poor Underserved. 2008;19(1):227–236.
30. Hudson N, Culley L, Johnson M, et al. Asthma management in British South Asian children: an application of the candidacy framework to a qualitative understanding of barriers to effective and accessible asthma care. BMC Public Health. 2016;16:510.
31. Koenig K. Pilot study of low-income parents’ perspectives of managing asthma in high-risk infants and toddlers. Pediatr Nurs. 2007;33(3):223–228, 242.
32. Meng A, McConnell S. Decision-making in children with asthma and their parents. J Am Acad Nurse Pract. 2002;14(8):363–371.
33. Shaw MR, Oneal G. Living on the edge of asthma: a grounded theory exploration. J Specialists Pediatric Nursing. 2014;19(4):296–307.
34. Zheang M, Rodriguez E, Alvarado C, Correa R, Kahlor L, Matsui EC. Exploring low-income African American and Latinx caregiver perspectives on asthma control in their children and reactions to messaging materials. J Asthma. 2021;1:548.
35. Archibald M, Caine V, Hartling L, Scott S. What is left unsaid: an interpretive description of the information needs of parents of children with asthma. Res Nurs Health. 2015;38(1):19–28.
36. Dietrich C. Decision Making: factors that influence decision making, heuristics used, and decision outcomes. Inquiries J Social Sci Arts Humanities. 2010;2:2.
37. Yoos HL, Kitzman H, McMullen A, Sidora K. Symptom perception in childhood asthma: how accurate are children and their parents? J Asthma. 2003;40(1):27–39.
38. Carroll WD, Wildhaber J, Brand PL. Parent misperception of control in childhood/adolescent asthma: the Room to Breathe survey. Eur Respir J. 2012;39(1):90–96.
39. Silva CM, Barros L. Asthma knowledge, subjective assessment of severity and symptom perception in parents of children with asthma. J Asthma. 2013;50(9):1002–1009.
40. Garbutt J, Highstein G, Nelson KA, Rivera-Spoljaric K, Strunk R. Detection and home management of worsening asthma symptoms. Ann Allergy Asthma Immunol. 2009;103(6):469–473.
41. Searle A, Jago R, Henderson J, Turner KM. Children’s, parents’ and health professionals’ views on the management of childhood asthma: a qualitative study. NPJ Primary Care Respir Med. 2017;27(1):53.
42. Harrington KF, Zhang B, Magruder T, Bailey WC, Gerald LB. The impact of parent’s health literacy on pediatric asthma outcomes. Pediatric Allergy Immunol Pulmonol. 2015;28(1):20–26.
43. Sukartini T, Alfa S, Utami S, Nursalam N. Development of asthma management based on health belief model in parents. Int J Psychosocial Rehabilitation. 2020;24:7.
44. McDonald VM, Gibson PG. Asthma self-management education. Chron Respir Dis. 2006;3(1):29–37.
45. Smith J, Cheater F, Bekker H. Parents’ experiences of living with a child with a long-term condition: a rapid structured review of the literature. Health Expect. 2013;18:452–474.
46. Miles C, Arden-Close E, Thomas M, et al. Barriers and facilitators of effective self-management in asthma: systematic review and thematic synthesis of patient and healthcare professional views. Primary Care Respir Med. 2017;2:27.
47. Foster JM, McDonald VM, Guo M, Reddel HK. “I have lost in every facet of my life”: the hidden burden of severe asthma. Eur Respir J. 2017;4:50.
48. Auger KA, Kahn RS, Davis MM, Simmons JM. Pediatric asthma readmission: asthma knowledge is not enough? J Pediatr. 2015;166(1):101–108.e101.
49. Australian Institute of Health and Welfare. Australia’s Health 2016. Canberra, Australia: Australian Institute of Health and Welfare; 2016.
50. Bird SR, Noronha M, Kurowski W, Orkin C, Sinnott H. Integrated care facilitation model reduces use of hospital resources by patients with pediatric asthma. J Healthc Qual. 2012;34(3):25–33.
51. Mudd SS, Ogborn CJ, Bollinger ME, et al. Parental decision making associated with pediatric emergency department use for asthma. Ann Allergy Asthma Immunol. 2016;117(5):490–494.
52. Kearns R, Harris-Roxas B, McDonald J, Jung Song H, Dennis S, Harris M. Implementing the Patient Activation Measure (PAM) in clinical settings for patients with chronic conditions: a scoping review. Integrated Healthcare J. 2020;2:87.
53. Hibbard JH. Patient activation and the use of information to support informed health decisions. Patient Educ Couns. 2017;100:5–7.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.