Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 17
Parametric Population Pharmacokinetics Model Repository of Rifampicin: Model-Informed Individualized Therapy
Authors Ju G ![]() , Liu X, Gu M, Chen L, Wang X, Li C, Yang N, Zhang G, Zhang C, Zhu X, He Q
, Liu X, Gu M, Chen L, Wang X, Li C, Yang N, Zhang G, Zhang C, Zhu X, He Q ![]() , Ouyang D
, Ouyang D ![]()
Received 29 November 2024
Accepted for publication 7 April 2025
Published 15 April 2025 Volume 2025:17 Pages 49—78
DOI https://doi.org/10.2147/CPAA.S502272
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Khaled Deeb
Gehang Ju,1– 3 Xin Liu,3,4 Meng Gu,4 Lulu Chen,3,5 Xintong Wang,3,5 Chao Li,3,6 Nan Yang,3,6 Gufen Zhang,3,6 Chenchen Zhang,7 Xiao Zhu,4 Qingfeng He,4,* Dongsheng Ouyang1– 3,5,*
1Department of Clinical Pharmacology, Xiangya Hospital, Central South University, Changsha, People’s Republic of China; 2Institute of Clinical Pharmacology, Central South University, Changsha, People’s Republic of China; 3Hunan Key Laboratory for Bioanalysis of Complex Matrix Samples, Changsha Duxact Biotech Co., Ltd., Changsha, People’s Republic of China; 4Department of Clinical Pharmacy, School of Pharmacy, Fudan University, Shanghai, People’s Republic of China; 5Changsha Duxact Biotech Co., Ltd., Changsha, People’s Republic of China; 6Phamark Data Technology Co., Ltd., Changsha, People’s Republic of China; 7School of Pharmaceutical Sciences, Sun Yat-sen University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Dongsheng Ouyang; Qingfeng He, Email [email protected]; [email protected]
Introduction: Rifampicin is a crucial first-line anti-tuberculosis drug that has been extensively studied through population pharmacokinetic (popPK) analyses. This study aims to construct a comprehensive rifampicin popPK model repository to support model-informed individualized therapy.
Methods: A systematic review was conducted using PubMed, Web of Science, and Embase databases up to September 2023 to retrieve popPK model articles on rifampicin. Extracted data included basic information, dosing regimens, sampling strategies, model parameters, and covariate details. Non-English studies, non-parametric models, and duplicates were excluded. The repository was built using R package mrgsolve, and a Shiny application was developed for simulation and individualized dosing predictions.
Results: A total of 29 studies were included in the rifampicin model repository: 23 on adults, 5 on pediatrics, 1 on both populations, and 1 on pregnant women. Most rifampicin popPK models were one-compartment linear elimination models, with transit compartment or lagged absorption models improving drug absorption fitting. An allometric growth model based on fat-free mass (FFM) might improved model fit. Postmenstrual age (PMA) significantly impacted elimination in pediatric patients. All models underwent internal validation, with three studies validated externally. Significant variations in exposure predictions were observed among models, indicating challenges in achieving therapeutic targets under standard treatment.
Discussion: The model repository provides a comprehensive resource for exploring various models and their application in different populations, supporting individualized rifampicin therapy. Further research is needed for special populations and to determine whether weight or FFM is more rational for dosing. External validation is essential for model development.
Keywords: rifampicin, model-informed precision dosing, population pharmacokinetics
Introduction
Despite significant therapeutic advances in the global fight against tuberculosis (TB), a notable proportion of patients still experience treatment failure due to issues related to drug safety and efficacy, with drug resistance remaining a persistent challenge.1 According to the World Health Organization’s standard treatment regimen, rifampin (RIF) is a crucial first-line anti-TB drug. It binds to the beta subunit of the mycobacterial DNA-dependent RNA polymerase enzyme, inhibiting transcription.
Pharmacokinetics (PK) plays an essential role in optimizing the therapeutic potential of drugs. For medications with a narrow therapeutic window or a high risk of developing resistance, such as rifampicin, strict control of drug exposure within the therapeutic window can reduce the occurrence of adverse events and delay the onset of resistance. The peak concentration (Cmax) of RIF can be detected 2 hours after oral administration, with approximately 20–30% of free unbound RIF remaining in plasma.2 RIF is approximately 70% bioavailable, and its absorption is modestly reduced by food intake.3 Prior research has implicated factors such as the hepatic organic anion transporter SLCO1B1, arylacetamide deacetylase (AADAC), auto-induction, non-cytochrome P450 pathways, gender, age, body weight, dietary status, alcohol consumption, concomitant diseases (eg, HIV, diabetes mellitus), and concomitant medications as potential sources of variability in rifampicin exposure, although their clinical significance remains uncertain.4–7 Due to the relatively narrow therapeutic range of rifampicin (8–24 mg/L) and the significant inter-individual variation in its PK properties, treatment outcomes may be affected, potentially contributing to the development of drug resistance.8
The recommended dosing for RIF is typically weight-based: 15 mg/kg (range 10–20) for children under 10 years old and 10 mg/kg for individuals 10 years and older. In clinical practice, RIF is usually administered orally at a standard dose of 600 mg.9 However, relying solely on body weight for dose adjustment or evaluating efficacy based solely on Cmax within 2 hours after administration may be insufficient. Population pharmacokinetic (popPK) modeling addresses these limitations by systematically quantifying interindividual variability in drug disposition through demographic, genetic, and physiological determinants of absorption, distribution, metabolism, and excretion (ADME).10 These models face inherent challenges stemming from heterogeneous data sources - geographic disparities, ethnic diversity, lifestyle patterns, and comorbidity profiles often lead to divergent covariate selections across studies. While demonstrating strong predictive performance within their original study populations, such models encounter generalizability constraints when extrapolated to external cohorts. Using popPK’s maximum a posteriori Bayesian simulation method, Area under the concentration curve (AUC) and Cmax exposure for patients can be predicted by combining drug concentration measurements with the matched model, allowing for the development of comprehensive dose adjustment strategies for individual patients. Notably, the clinical relevance of selected covariates (even when overlapping between models) requires rigorous validation, particularly given the potential discordance in covariate inclusion strategies across different modeling frameworks.
Previous reviews of RIF popPK models have been limited by search strategies and timeframes, which have led to the omission of certain models and a lack of comprehensive exposure comparisons between the models included.11 Additionally, no user-friendly clinical tools have been developed to facilitate individualized dosing in routine practice. To address these gaps, this study aims to systematically review and summarize existing RIF popPK models, identify key covariates influencing PK variability, compare PK profiles between models, and establish a comprehensive RIF popPK model repository for further analysis. Furthermore, we aim to develop a Shiny application for RIF model simulations to enable individualized dose adjustments and enhance clinical decision-making. Special attention will be given to the application of popPK models in vulnerable populations, such as children and pregnant women, where dosing optimization remains a critical challenge.
Methods
Search Strategy
A systematic search of PubMed, Web of Science, and Embase databases was conducted from their inception to September 23, 2023, for the initial retrieval. To ensure the inclusion of the most recent and relevant studies, a supplementary search was performed up to February 26, 2025. The search terms included MeSH terms (Medical Subject Headings) and Entry terms. Two authors conducted the literature screening work in parallel. The paper management software used was EndNote (Version 20; Thomson Scientific, Box Hill, Victoria, Australia).
Inclusion criteria were as follows:
Exclusion criteria were as follows:
The inclusion and exclusion criteria were established based on the standards for constructing the model repository, aiming to facilitate horizontal comparison of similar models and ensure the reproducibility of the models.
Data Extraction
Two authors independently extracted the following information from eligible articles: (1) baseline data, including demographic data and laboratory test data (eg country, age, body weight, sex, etc).; (2) study characteristics: treatment regimens, sample counts, bioanalytical methods, the lower limit of quantification, etc.; (3) popPK characteristics: model parameters and formulation, structural models, covariates, methods used to identify and incorporate covariates, inter-individual variability, inter-occasion variability (IOV), and residual unexplained variability (RUV).
Literature Quality Assessment
The assessment of the quality of the included studies was performed by utilizing a 33-item checklist, consisting of 5 categories, according to a previously published popPK assessment method.12–14 This checklist was designed to assess the essential components necessary for the reporting of clinical pharmacokinetic (PK) studies. For each item, one point received if the involved study met the criteria, whereas incomplete data were assigned 0.5 points. If the item did not meet the criteria, it was assigned 0 points. To evaluate the quality of each population pharmacokinetic (popPK) study, compliance was calculated using the following equation i:

Comparison of the Retrieved Study
In our study, we summarized the covariates that affect both clearance (CL) and volume of distribution (Vd). However, since CL is considered the most critical pharmacokinetic parameter, we placed particular emphasis on examining how covariates affect rifampicin clearance. To facilitate comparison, continuous covariates were standardized to the same range, whereas binary covariates, such as HIV status, were coded as 0 for negative and 1 for positive. The minimum and maximum CL values were determined based on the range of covariates identified in each study. The median covariate values were normalized against to the reference value of CL, and the effect of covariates on CL was expressed as a percentage of the CL range divided by the CL reference value for each study. A forest plot was used to summarize and compare the identified covariates’ impact on CL. The covariate effects were calculated as follows: the maximum effect was determined using Equation ii, and the minimum effect was determined using Equation iii:


A change in CL within the 80% to 125% range was considered clinically insignificant according to bioequivalence standards.12,13,15
Monte Carlo Simulation
To assess the statistical and structural models of the popPK studies, Monte Carlo simulations of concentration-time profiles were performed, and visual predictive distributions (VPDs) were generated. It was assumed that the published models were sufficient to describe the data, and a predictive distribution of the simulated rifampicin concentration for each model would adequately represent the original data and its significant features. The MrgSolve package (version 1.1.1, https://mrgsolve.org) was utilized for solving and simulating ODE-based models. One thousand virtual patients were simulated for each identified study, and the concentration-time profiles were plotted using R software (version 4.2.2) according to the popPK model.
The VPDs incorporated the effects of body weight (BW)/Fat-free Mass (FFM), and postmenstrual age for neonates. Virtual patients were defined as infants (14/11kg, 2 years) or adults (60 kg/46 kg). The conversion between BW and FFM was referenced from the study by Kyle et al, and the age group stratification was used solely for horizontal comparison of exposure within the same population.16 Oral administration of 600 mg QD for adults or 150 mg QD for infants, based on existing treatment standards.8,9,17 The PK studies of RIF, as summarized in the earlier research by Abulfathi et al,18 indicate that the half-life of RIF post-administration ranges from 0.6 to 6.5 hours. In some individuals, there may be accumulation with repeated dosing. Considering the maximum half-life of 6.5 hours, it can be assumed that steady-state is achieved after 5 to 6 doses. Therefore, in this simulation, RIF is assumed to be administered consecutively for 7 doses, and the PK profile of the last dose is observed to assess its systemic exposure.
Model Simulation Software
Using the Shiny package (version 1.7.1. https://CRAN.R-project.org/package=shiny) and MrgSolve package, a rifampicin model repository was integrated into a simulation app. This app allows users to input patient age, BW/ FFM, sex, select the target model, and input the intended dosing regimen. Through Bayesian simulation techniques, we generated exposure predictions that reflect the typical values within a population, along with prediction intervals that account for IIV and IOV as reported in the literature.
Results
Study Identification
A total of 2278 studies were initially identified, comprising 628 articles from PubMed, 561 articles from Embase, 1089 articles from Web of Science. Subsequently, 30 articles were selected for the model repository. A supplementary search conducted up to February 26, 2024, identified one additional study, resulting in a final total of 31 articles included in the analysis. The flowchart illustrating the screening process for the initial search is provided in the supplementary material (Figure S1), and the detailed search strategy is summarized in Table S1.
The quality assessment results of retrieved studies are shown in Figure 1 and Table S2. The quality evaluation was generally good, with an average compliance of 88.31% (78.8–93.9%). There was no significant publication bias observed. However, most studies did not report: (1) missing data handling methods (22/31); (2) statistical methods and software (18/31); (3) covariate inclusion description was incomplete (15/31); (4) schematic of the final model (22/31); and (5) summary of the model-building process and the derived final model (30/31).
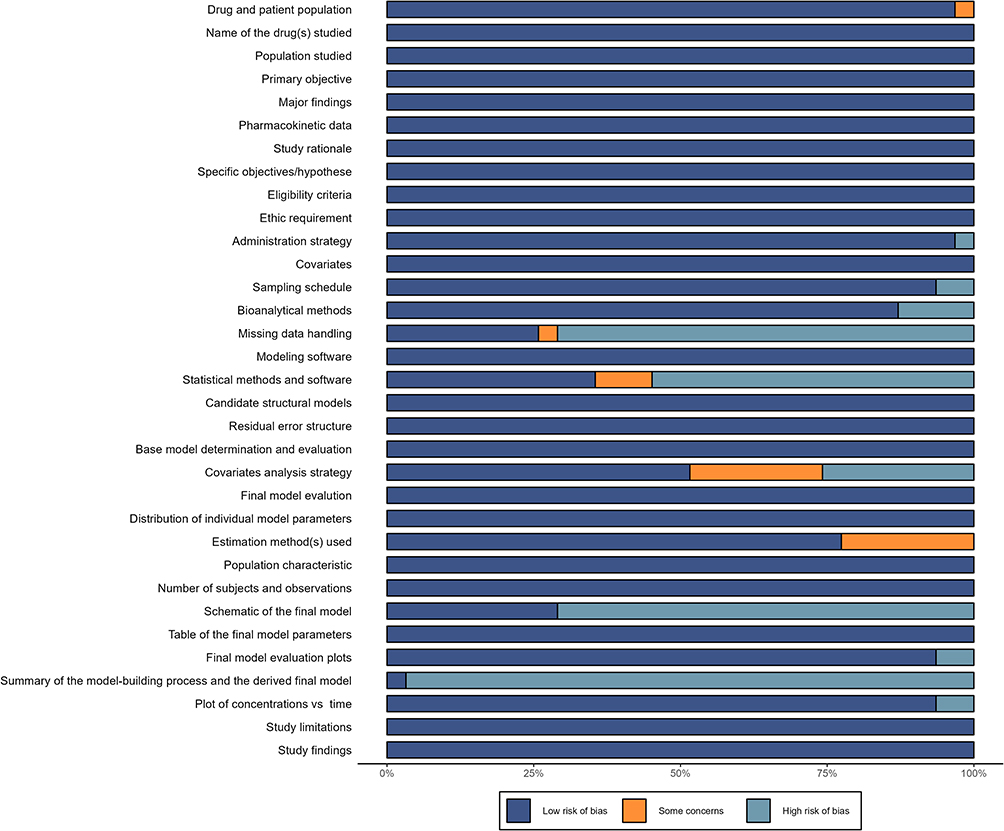 |
Figure 1 Risk-of-bias assessments of rifampicin popPK studies. |
Literature Characteristics
Basic Characteristics
The publication years of the included studies ranged from 2008 to 2024. The majority of subjects across the studies were diagnosed with tuberculosis, with 24 studies focused on adults,5,19–42 6 on pediatrics,43–48 1 on pregnant women,22 and 1 on both adults and pediatrics.36 In addition, 13 studies enrolled patients with HIV, and 4 studies included patients with diabetes. Plasma RIF concentrations were determined using either liquid chromatography with ultraviolet detection or mass spectrometry, with lower limits of quantification ranging from 0.008 to 0.5 mg/L. Detailed characteristics of the included studies are provided in Table 1. Savic did not report key demographic information for inclusion of pediatric patients and did not conduct follow-up simulation comparisons.48
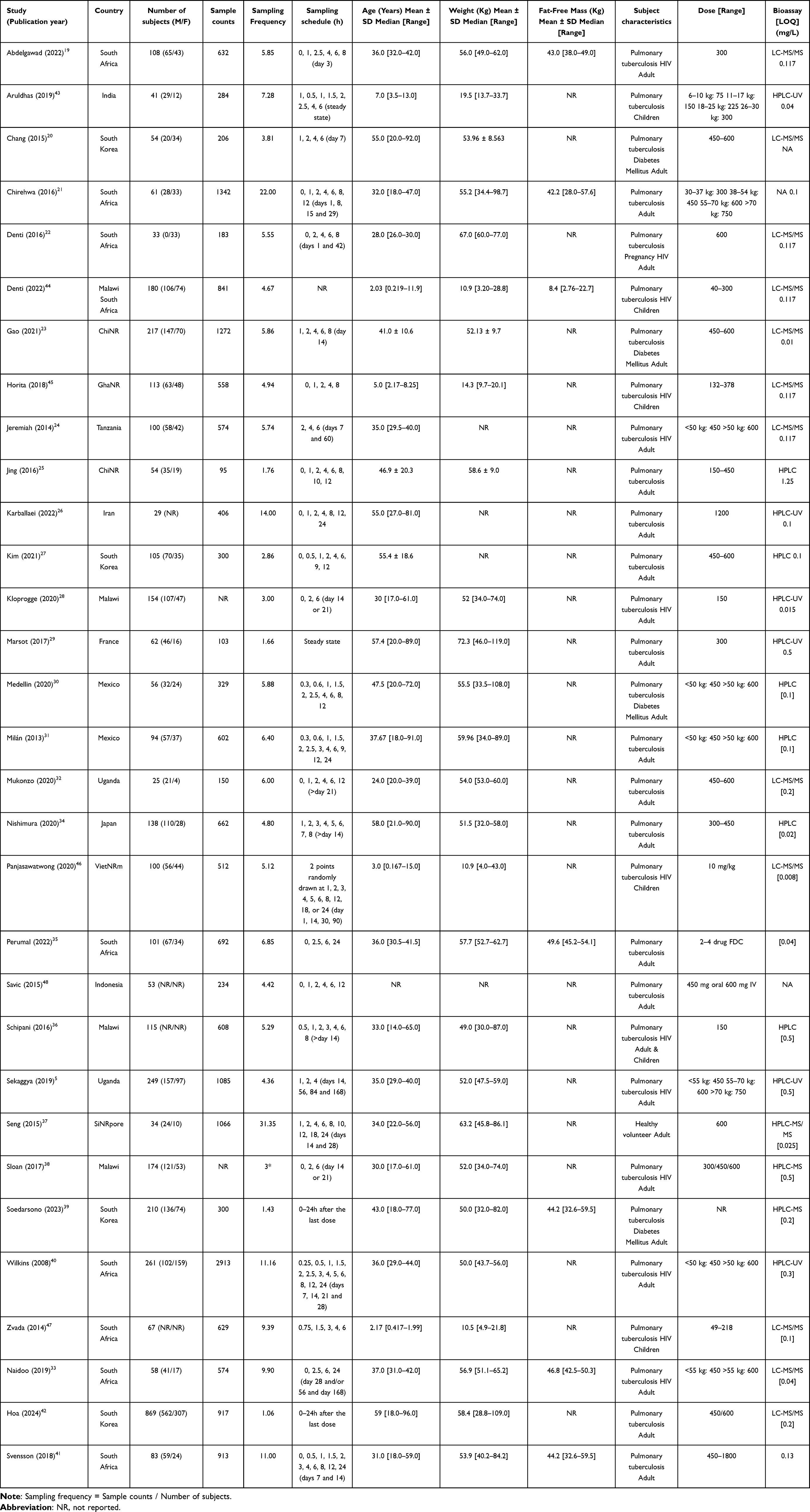 |
Table 1 Characteristics of Included RIF popPK Studies |
Population Pharmacokinetic Characteristics
Twenty-seven popPK models were conducted using NONMEM (Icon, Dublin, Ireland), 3 studies based on Monolix (Lixoft, Antony, France), and 1 study based on Phoenix NLME (Certara Inc, Princeton, USA). The first-order conditional estimation with the η-ε interaction (FOCE-I) was the most commonly used algorithm. Twenty-eight studies described the PK of RIF using a one-compartment model with first-order absorption and elimination, while only three studies used a two-compartment model. At high doses, the systemic exposure of RIF exhibits a dose-dependent increase.41 Most models included transit compartments or lag time (Tlag) during the absorption period. The allometric growth model was used in all pediatric popPK models, and PMA had a significant effect on CL. The model characteristics and PK parameters of all studies are presented in Table 2.
 |
Table 2 Population Pharmacokinetic Parameters of Retrieved Studies |
Inter-individual variability (IIV) was described by an exponential model in all studies. Residual unexplained variability (RUV) was described by proportional models in 8 studies, additive models in 6, and combined proportional and additive models in 16 studies. All proportional RUV values were less than 50%, whereas additive RUV ranged from 0.0032 to 2.256. Some studies reported the existence of inter-occasion variability (IOV) in Ka, bioavailability (F), Tlag, and model transit time (MTT).
All models were evaluated internally with visual predictive check (VPC), bootstrap, and goodness-of-fit (GOF) plots as the most commonly used methods. One study employed the normalized prediction distribution error (NPDE). Only four studies performed external evaluations using an independent dataset, demonstrating acceptable predictability. Enhancing the predictive performance of popPK models requires rigorous external validation to ensure their applicability across different populations and clinical settings.
Covariates of Inclusion
The majority of studies sought to identify covariates that explain the IIV of rifampicin pharmacokinetics, focusing on those with potential clinical significance. A stepwise approach involving forward inclusion and backward elimination was used in 23 of the 31 studies for covariate screening. Notably, 8 studies used forward inclusion and 11 studies used backward elimination, The specific inclusion or exclusion criteria were not reported in 7 studies. A summary of all tested and identified covariates for CL and Vd is presented in Table 3. The excluded and included covariates for CL and Vd in each study are illustrated in Figure 2. BW and FFM significantly affected rifampicin CL in the majority of included models. However, in studies that directly compared BW and FFM, FFM provided a better fit. In children, PMA affected CL, other demographic and laboratory indices (BRC, sex, pregnancy status, concomitant drugs, administration duration, and SLCO1B1*15) might influence CL or Vd. Of the 22 studies using allometric scaling models, 8 used FFM and 14 used BW as the covariate.
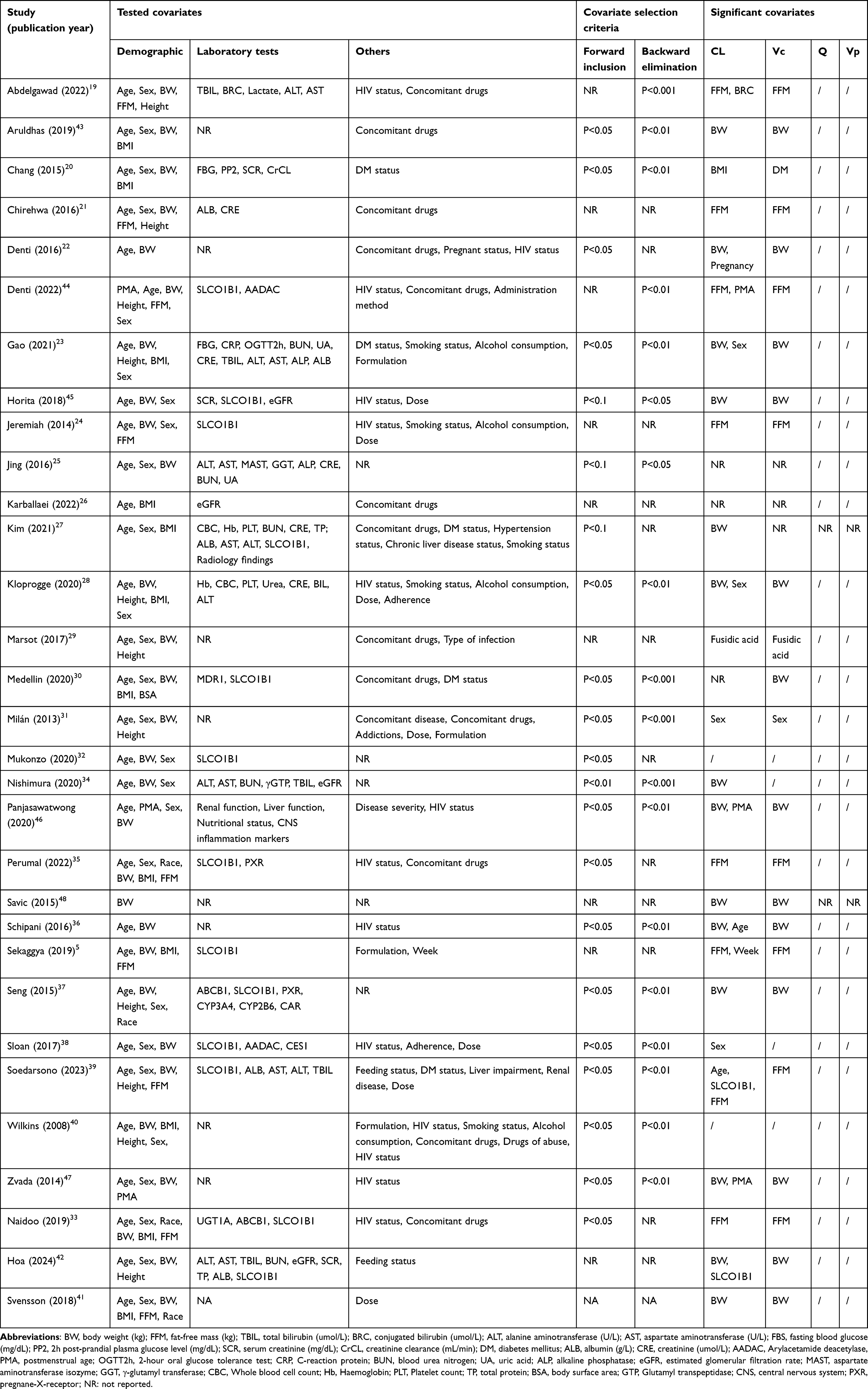 |
Table 3 List of Tested and Significant Covariates in the Model |
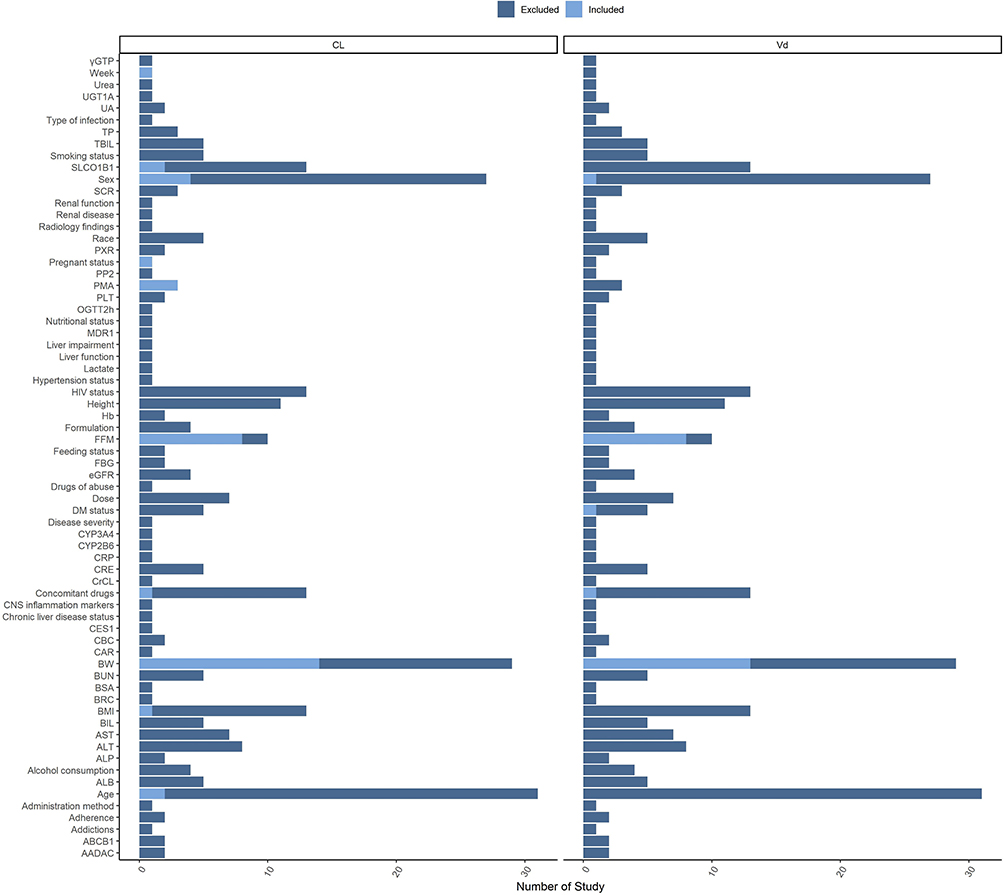 |
Figure 2 Excluded and Included covariates for clearance and volume of rifampicin. Abbreviations: BW, body weight (kg); FFM, fat-free mass (kg); TBIL, total bilirubin (umol/L); BRC, conjugated bilirubin (umol/L); ALT, alanine aminotransferase (U/L); AST, aspartate aminotransferase (U/L); FBS, fasting blood glucose (mg/dL); PP2, 2h post-prandial plasma glucose level (mg/dL); SCR, serum creatinine (mg/dL); CrCL, creatinine clearance (mL/min); DM, diabetes mellitus; ALB, albumin (g/L); CRE, creatinine (umol/L); AADAC, Arylacetamide deacetylase, PMA, postmenstrual age; OGTT2h, 2-hour oral glucose tolerance test; CRP, C-reaction protein; BUN, blood urea nitrogen; UA, uric acid; ALP, alkaline phosphatase; eGFR, estimated glomerular filtration rate; MAST, aspartate aminotransferase isozyme; GGT, γ-glutamyl transferase; CBC, Whole blood cell count; Hb, Haemoglobin; PLT, Platelet count; TP, total protein; BSA, body surface area; GTP, Glutamyl transpeptidase; CNS, central nervous system; PXR,pregnane-X-receptor. |
The forest plot of covariate effects on CL (Figure 3) showed that pregnancy, BMI, BRC, and SLCO1B1 genotype might not have clinically significant impacts on rifampicin clearance. The combination of fusidic acid significantly affected RIF clearance. In studies that evaluated both FFM and BW as covariates, FFM provided a better fit for the allometric scaling models, particularly for rifampicin clearance. These studies consistently preferred FFM over BW, suggesting that FFM may better capture the variability in drug clearance. Other studies that considered only BW did not provide comparative analysis, and thus did not assess the potential advantages of FFM.
 |
Figure 3 Forest plot of covariates effect on the clearance of rifampicin. Note: The horizontal bars represent the covariate effect on clearance in each study. The shadow area ranges from 0.8–1.25. |
Exposure Comparison
The simulated concentration-time profiles of included popPK models are presented in Figure 4A–B. Based on the simulated PK profiles, the concentrations in most typical patients did not reach the therapeutic concentration range. Gender factors may introduce differences in rifampicin exposure, with simulation results from three studies indicating lower exposure in males than in females. However, variations in rifampicin exposure related to genetic polymorphisms in the SLCO1B1 gene were not considered clinically significant. There are substantial exposure differences among various models when subjected to the same dosing regimen, and understanding the origins of these exposure discrepancies between models is crucial. Due to issues such as the complexity of the model reported by Svensson and the inability to unify parameter units,41 simulation reproduction could not be achieved, and the model exposure comparison was not included.
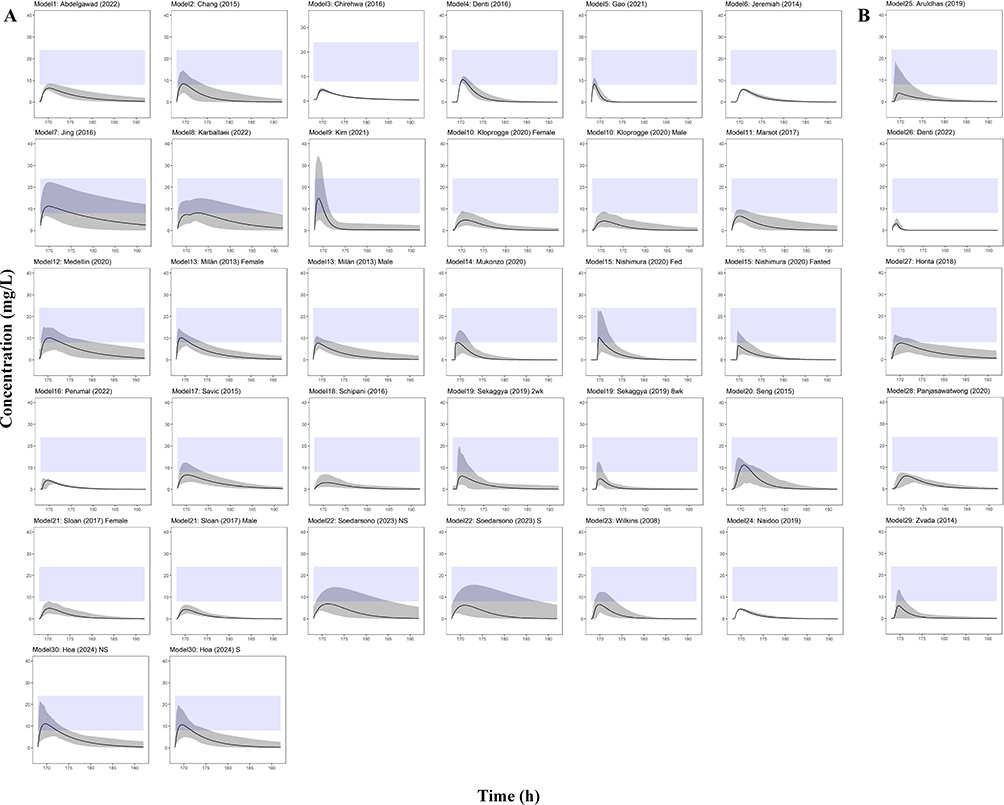 |
Figure 4 Concentration-time profiles at steady state in retrieved studies. Note: (A) Adult model; (B) Pediatric model. The light purple shadow means the population prediction range (90% CI); the light blue shadow means the efficacy range (8–24 mg/L). |
Model Application
The code for the RIF popPK repository and the Shiny app is available at Github (https://github.com/727397883/Rifampicin-PopPK-Repository). The graphical presentation interface of the shiny app is provided in the supplementary material (Figure S2).
Discussion
This study systematically reviewed existing population pharmacokinetic models of rifampicin and constructed a comprehensive rifampicin model repository using mrgsolve. Additionally, we developed a Shiny application based on this model repository to facilitate individualized dosing strategies. The article compiles extensive information from the studies, including study design, population characteristics, dosing regimens, sampling strategies, and bioanalytical methods, modeling techniques, as well as covariate models. It objectively compares the quality of reporting, inclusion of covariates among the models, while assessing the clinical significance of all included covariates. Bayesian simulation techniques are employed to compare exposure differences across studies in typical populations and evaluate the attainment of therapeutic targets under standard treatment regimens.
Model Performance
Among the 30 included popPK models, 27 adopted a one-compartment first-order elimination model, and improved fitting performance by incorporating transit compartments or lag time absorption models. Rifampicin exhibits rapid metabolism and minimal accumulation in vivo. Although 28 studies utilized internal validation methods such as GOF, VPC, Bootstrap, or NPDE, only 4 studies incorporated external validation using independent datasets,23,30,31,42 which raises concerns about their generalizability. For studies involving small sample sizes or sparse sampling points, the informational content of the modeling data may be insufficient to fully elucidate the PK characteristics of RIF in the human body. As such, external validation is crucial for models based on smaller sample sizes and limited sampling points. All 30 studies reported high-quality models with low bias risks, providing guidance for individualized predictions in clinical practice.
Covariate Effects
Previous research examined numerous demographics, laboratory, comorbidity, concomitant medication, and genomic factors affecting rifampicin PK. Body weight (BW) and fat-free mass (FFM) are considered critical covariates in 21 studies employing allometric growth models, with eight studies comparing BW and FFM separately. Eight studies indicate that FFM provides a better fit and enhanced model performance compared to BW.5,19,21,24,33,35,39,44 While WHO guidelines recommend body weight-based dosing for rifampicin, considerable variation exists within broad body weight categories.17 Using FFM results in less fluctuation in rifampicin clearance rates across different intervals, however, caution should be exercised at extremely low FFM levels. While BW was the predominant covariate in most models, studies that included a direct comparison with FFM suggest that FFM may provide a better fit, particularly in patients with muscle wasting, where relying solely on BW could lead to dosage errors. This indicates that while BW remains widely accepted standard, FFM might be more appropriate in certain cases.5,49 Gender, BMI, and dosing cycles might influence rifampicin clearance, but according to the covariate analyses, their impact may not be clinically significant, thus justifying against dose adjustments based on these factors. Only one study reported the effect of dosing cycle on clearance, indicating the need for further exploration regarding whether rifampicin exposure varies significantly with the dosing regimen.5
Laboratory assessments have considered liver function, renal function, nutritional status, and central nervous system inflammation markers, yet only one study incorporated direct bilirubin, finding no clinically significant effect on clearance. Thirteen studies investigated the impact of SLCO1B1 gene phenotypes on PK parameters, yet only two of them ultimately included this parameter. Furthermore, the examination of covariate effects revealed that the influence of SLCO1B1 gene phenotypes lacks clinical significance. This further supports the notion that SLCO1B1 genetic testing may not be necessary for rifampicin.
Regarding comorbidities, DM and HIV status were frequently analyzed. DM is a known risk factor for TB development, with reports suggesting a threefold increased risk in DM patients.50 Despite five studies incorporating DM status, only one found an effect on volume of distribution.20 In African populations, none of the 13 rifampicin studies found HIV status to affect PK parameters. Among concomitant medications, fusidic acid was reported by one study to influence rifampicin clearance and volume of distribution, with covariate analysis revealing substantial changes in CL.29 However, the mechanism underlying fusidic acid’s impact on rifampicin’s ADME process remains unclear.
Special Populations
Pregnant women and children are key patient groups requiring tailored drug therapy. Studies have shown that physiological and pathophysiological changes during pregnancy can impact drug ADME processes,51,52 while infants and preterm/very-low birthweight children often have immature organ systems, necessitating personalized dosing.53 Our model repository includes one study on pregnant women, identifying pregnancy as a significant covariate for rifampicin clearance, although the covariate analysis suggests its impact may not be statistically significant relative to other populations.22 For pediatric populations, PMA and FFM/BW are more influential on rifampicin exposure.44,46,47 Further research is needed to substantiate the impact of pregnancy on rifampicin exposure.
Rifampicin Simulations
The rifampicin simulation curves revealed inter-model variability in drug PK. Under WHO-recommended and standard clinical doses, most studies did not achieve the therapeutic range.9,17 Asians appear more likely to reach this interval relative to other populations,20,23,25,27,37,39,46 however, considering that TB treatment success rates exceed 90%, the validity of the effective range (8–24 mg/L)8 based on Cmax may be questioned along with the consistency of the efficacy window across countries. The long-term follow-up results of 142 tuberculosis patients by Pasipanodya et al indicate that an AUC of rifampin less than 13 mg*h/L is associated with adverse outcomes, demonstrating that a low AUC can predict the clinical prognosis of tuberculosis patients.54 Three studies built gender-specific covariate models, with simulations showing women generally more easily achieving the therapeutic range.23,28,38 Two study involving SLCO1B1 gene typing demonstrated similar simulation outcomes.39,42 Food intake was observed to increase rifampicin exposure in one study,34 while another study noted that rifampicin exposure decreased between the second and eighth dosing cycles due to auto-induction effects, which led to accelerated elimination and approximately 20% reduction in drug exposure after prolonged administration, consistent with prior reports.5 The PopPK model analysis results from Svensson et al’s ultra-high dose group indicate that the dose level of rifampin significantly influences the drug’s bioavailability and clearance rate.41 Therefore, particular attention should be paid to its PK/PD response when administering high doses.
Utilization of the Model Repository
Our study establishes a rifampicin popPK model repository and a Shiny application, facilitating individualized dosing strategies using mrgsolve for RIF. We have previously developed a parameter-based popPK model repository for isoniazid.14 By leveraging both rifampicin and isoniazid repositories, users can make precise exposure predictions for individual patients based on their specific characteristics and dosing regimens. These drugs are recommended by WHO for combined therapy,1 and their models joint application allows for more accurate in vivo exposure analysis.
The Shiny application provides a user-friendly interface that enables clinicians and researchers to simulate RIF dosing regimens based on various patient-specific parameters such as age, sex, BW or FFM. By leveraging Bayesian simulation techniques, the application allows for precise exposure predictions, facilitating the optimization of therapeutic regimens tailored to individual patient needs. The primary advantages of our model application include: (i) Ease of Use: The Shiny application offers an intuitive interface, making it accessible to users with varying levels of technical expertise. (ii) Comprehensive Data Integration: The application integrates demographic, genetic, and physiological data to provide a holistic view of the patient’s pharmacokinetic profile. (iii) Real-Time Simulations: Users can perform real-time simulations to explore potential drug exposure scenarios, potentially informing future research and model refinement. (iv) Model Repository: Our extensive repository of popPK models enables users to select models most relevant to specific patient characteristics and clinical scenarios. (v) Research Support: By allowing users to explore exposure predictions, the application can support research and educational efforts, contributing to better understanding of rifampicin pharmacokinetics in specific populations. Moreover, this model repository enables seamless integration with other model-informed optimal experimental design, such as sampling strategy optimization, dosing regimen selection, and missed or delayed dose scenarios.55
In managing drugs with a narrow therapeutic window and a high risk of resistance, maintaining drug exposure within the effective therapeutic range is essential to minimize adverse effects and reduce the likelihood of early resistance development. While rifampicin has traditionally been associated with a specific target concentration, recent findings suggest a broader therapeutic range, particularly at higher doses, highlighting the need for flexible, patient-tailored dosing strategies. Given the increasing concern over multi-drug-resistant tuberculosis and the growing emphasis on precision medicine, this comprehensive overview underscores the critical role of popPK models in enhancing our understanding of rifampicin’s pharmacokinetics and improving patient care through evidence-based, individualized treatment approaches.
Limitations
This study employed simulated populations to eliminate confounding factors and assess model performance under controlled conditions (eg, typical population and fixed dosing regimen). While this approach provides consistency, it does not account for real-world variability, limiting the direct applicability of our findings to clinical practice.
The Shiny application developed in this study is designed as an investigative and educational tool for exploring population pharmacokinetic models and is not intended for direct application in clinical practice. For clinical use, it is recommended to validate or optimize the models with patient data, ensuring the best model is matched before its application in clinical settings.
Our focus on standard clinical dosing models intentionally excluded the Svensson et al41 study, which investigates high-dose rifampicin with complex pharmacokinetics, including saturation and autoinduction. These differences precluded its inclusion in our analysis.
In the current PopPK model report, correlations between certain covariates, such as body weight and sex, may exist and require further exploratory analysis during model inclusion. Additionally, we did not perform a non-compartmental analysis to quantify exposure differences between the models. These limitations provide opportunities for improvement in future work. Future research will focus on validating the models included in the Shiny application, conducting external validation, and exploring ways to enhance its clinical applicability.
Conclusion
This study underscores the importance of model-informed precision dosing in optimizing rifampin therapy. By systematically reviewing 31 popPK models, we identified key covariates affecting rifampin pharmacokinetics, including FFM, BW, and PMA in pediatrics, while SLCO1B1 polymorphisms and other covariates showed limited clinical relevance.
Significant inter-model variability was observed in exposure predictions, reflecting differences in model structures and covariate selection. Most models employed a one-compartment approach, while two-compartment models suggested a more complex distribution profile. The lack of external validation in most studies highlights the need for further validation efforts.
To facilitate individualized dosing, we developed a rifampin model repository and Shiny application, enabling real-time exposure simulations. Future research should focus on refining model structures, validating findings across diverse populations, and assessing long-term metabolic changes during therapy to enhance personalized treatment strategies.
Study Highlights
What is the Current Knowledge on the Topic?
Rifampicin is a key first-line drug for tuberculosis treatment, extensively studied through population pharmacokinetic (popPK) models to understand its pharmacokinetics and optimize therapy. Variability in rifampicin exposure due to factors like body weight, genetic polymorphisms, and comorbidities can affect treatment outcomes and contribute to drug resistance. Previous reviews of rifampicin popPK models have limitations, and there is a need for a comprehensive repository to support individualized therapy.
What Question Did This Study Address?
This study aimed to construct a comprehensive rifampicin popPK model repository to support model-informed individualized therapy. It sought to identify significant covariates influencing rifampicin pharmacokinetics, compare pharmacokinetic profiles of different models, and develop a Shiny application for simulation and individualized dosing predictions.
What Does This Study Add to Our Knowledge?
This study provides a comprehensive repository of rifampicin popPK models, incorporating data from 29 studies on various populations, including adults, pediatrics, and pregnant women. It identifies key covariates affecting rifampicin clearance, such as body weight and fat-free mass, and highlights the importance of individualized dosing strategies. The developed Shiny application allows for real-time simulations and personalized dosing adjustments based on patient-specific parameters.
How Might This Change Drug Discovery, Development, and/or Therapeutics?
The rifampicin popPK model repository and Shiny application enhance clinical decision-making by providing accurate exposure predictions and supporting tailored therapeutic regimens. This approach can improve treatment outcomes, reduce the risk of drug resistance, and pave the way for better patient care through evidence-based, individualized therapy. It also highlights the need for further research on special populations and the impact of covariates on rifampicin pharmacokinetics.
Acknowledgments
Thanks to Changsha Duxact Clinical Laboratory Co., Ltd and Phamark Data Technology Co, Ltd, Changsha, Hunan, China for the statistical support.
Funding
The research was funded by the National Natural Science Foundation of China (grant number 81803837), the Natural Science Foundation of Hunan Province (grant number 2022JJ80100, 2019JJ50839), the Hunan Province Foundation of High-level Health Talent (grant number 225), Shanghai Pujiang Programme (No. 23PJD016), the National Natural Science Foundation of China (Grant No. 82204502) and the Science and Technology Key Program of Hunan Provincial Health Committee (grant number 20201904).
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization GS. Global tuberculosis report. 2022. 2022.
2. Boman G, Ringberger VA. Binding of rifampicin by human plasma proteins. Eur J Clin Pharmacol. 1974;7(5):369–373. doi:10.1007/BF00558209
3. Friedman LN, Dedicoat M, Davies PDO, editors. Clinical Tuberculosis (6th Ed.). CRC Press; 2020.
4. McIlleron H, Wash P, Burger A, et al. Determinants of rifampin, isoniazid, pyrazinamide, and ethambutol pharmacokinetics in a cohort of tuberculosis patients. Antimicrob Agents Chemother. 2006;50(4):1170–1177. doi:10.1128/AAC.50.4.1170-1177.2006
5. Sekaggya-Wiltshire C, Chirehwa M, Musaazi J, et al. Low antituberculosis drug concentrations in HIV-tuberculosis-coinfected adults with low body weight: is it time to update dosing guidelines? Antimicrob Agents Chemother. 2019;63(6). doi:10.1128/AAC.02174-18.
6. Nijland HM, Ruslami R, Stalenhoef JE, et al. Exposure to rifampicin is strongly reduced in patients with tuberculosis and type 2 diabetes. Clin Infect Dis. 2006;43(7):848–854. doi:10.1086/507543
7. Babalik A, Ulus IH, Bakirci N, et al. Plasma concentrations of isoniazid and rifampin are decreased in adult pulmonary tuberculosis patients with diabetes mellitus. Antimicrob Agents Chemother. 2013;57(11):5740–5742. doi:10.1128/AAC.01345-13
8. Peloquin CA, Davies GR. The Treatment of Tuberculosis. Clin. Pharmacol. Ther. 2021;110(6):1455–1466. doi:10.1002/cpt.2261
9. van Ingen J, Aarnoutse RE, Donald PR, et al. Why do we use 600 mg of rifampicin in tuberculosis treatment? Clin Infect Dis. 2011;52(9):e194–9. doi:10.1093/cid/cir184
10. Darwich AS, Polasek TM, Aronson JK, et al. Model-Informed Precision Dosing: background, Requirements, Validation, Implementation, and Forward Trajectory of Individualizing Drug Therapy. Annu Rev Pharmacol Toxicol. 2021;61(1):225–245. doi:10.1146/annurev-pharmtox-033020-113257
11. Muda MR, Harun SN, Syed Sulaiman SA, et al. Population pharmacokinetics analyses of rifampicin in adult and children populations: a systematic review. Br J Clin Pharmacol. 2022;88(7):3132–3152. doi:10.1111/bcp.15298
12. Liu X, et al. Escitalopram Personalized Dosing: A Population Pharmacokinetics Repository Method. Vol. 17. Drug Des Devel Ther; 2023:2955–2967
13. Yang W, Mak W, Gwee A, et al. Establishment and evaluation of a parametric population pharmacokinetic model repository for ganciclovir and valganciclovir. Pharmaceutics. 2023;15(7):1801. doi:10.3390/pharmaceutics15071801
14. Ju G, Liu X, Yang W, et al. Model-informed precision dosing of isoniazid: parametric population pharmacokinetics model repository. Drug Des Devel Ther. 2024;18:801–818. doi:10.2147/DDDT.S434919
15. Qin Y, Zhang -L-L, Ye Y-R, et al. Parametric population pharmacokinetics of linezolid: a systematic review. Br J Clin Pharmacol. 2022;88(9):4043–4066. doi:10.1111/bcp.15368
16. Kyle UG, Schutz Y, Dupertuis YM, et al. Body composition interpretation. Contributions of the fat-free mass index and the body fat mass index. Nutrition. 2003;19(7–8):597–604. doi:10.1016/S0899-9007(03)00061-3
17. World Health Organization GS. WHO consolidated guidelines on tuberculosis: tuberculosis preventive treatment: module 1: prevention. 2020.
18. Abulfathi AA, Decloedt EH, Svensson EM, et al. Clinical pharmacokinetics and pharmacodynamics of rifampicin in human tuberculosis. Clin Pharmacokinet. 2019;58(9):1103–1129. doi:10.1007/s40262-019-00764-2
19. Abdelgawad N, Chirehwa M, Schutz C, et al. Pharmacokinetics of antitubercular drugs in patients hospitalized with HIV-associated tuberculosis: a population modeling analysis. Wellcome Open Res. 2022;7:72. doi:10.12688/wellcomeopenres.17660.2
20. Chang MJ, Chae J-W, Yun H-Y, et al. Effects of type 2 diabetes mellitus on the population pharmacokinetics of rifampin in tuberculosis patients. Tuberculosis. 2015;95(1):54–59. doi:10.1016/j.tube.2014.10.013
21. Chirehwa MT, Rustomjee R, Mthiyane T, et al. Model-based evaluation of higher doses of rifampin using a semimechanistic model incorporating autoinduction and saturation of hepatic extraction. Antimicrob. Agents Chemother. 2016;60(1):487–494. doi:10.1128/AAC.01830-15
22. Denti P, Martinson N, Cohn S, et al. Population pharmacokinetics of rifampin in pregnant women with tuberculosis and HIV coinfection in Soweto, South Africa. Antimicrob. Agents Chemother. 2016;60(3):1234–1241. doi:10.1128/AAC.02051-15
23. Gao Y, Davies Forsman L, Ren W, et al. Drug exposure of first-line anti-tuberculosis drugs in China: a prospective pharmacological cohort study. Br. J. Clin. Pharmacol. 2021;87(3):1347–1358. doi:10.1111/bcp.14522
24. Jeremiah K, Denti P, Chigutsa E, et al. Nutritional supplementation increases rifampin exposure among tuberculosis patients coinfected with HIV. Antimicrob. Agents Chemother. 2014;58(6):3468–3474. doi:10.1128/AAC.02307-13
25. Jing Y, Zhu LQ, Yang JW, et al. Population pharmacokinetics of rifampicin in Chinese patients with pulmonary tuberculosis. J Clin Pharmacol. 2016;56(5):622–627. doi:10.1002/jcph.643
26. Karballaei-Mirzahosseini H, Kaveh-Ahangaran R, Shahrami B, et al. Pharmacokinetic study of high-dose oral rifampicin in critically Ill patients with multidrug-resistant Acinetobacter baumannii infection. Daru. 2022;30(2):311–322. doi:10.1007/s40199-022-00449-5
27. Kim ES, Kwon BS, Park JS, et al. Relationship among genetic polymorphism of SLCO1B1, rifampicin exposure and clinical outcomes in patients with active pulmonary tuberculosis. Br. J. Clin. Pharmacol. 2021;87(9):3492–3500. doi:10.1111/bcp.14758
28. Kloprogge F, Mwandumba HC, Banda G, et al. Longitudinal pharmacokinetic-pharmacodynamic biomarkers correlate with treatment outcome in drug-sensitive pulmonary tuberculosis: a population pharmacokinetic-pharmacodynamic analysis. Open Forum Infect Diseases. 2020;7(7). doi:10.1093/ofid/ofaa218.
29. Marsot A, Ménard A, Dupouey J, et al. Population pharmacokinetics of rifampicin in adult patients with osteoarticular infections: interaction with fusidic acid. Br. J. Clin. Pharmacol. 2017;83(5):1039–1047. doi:10.1111/bcp.13178
30. Medellin-Garibay SE, et al., A population approach of rifampicin pharmacogenetics and pharmacokinetics in Mexican patients with tuberculosis. Tuberculosis, 2020. 124.
31. Milán Segovia RC, Domínguez Ramírez AM, Jung Cook H, et al. Population pharmacokinetics of rifampicin in Mexican patients with tuberculosis. J Clin Pharm Therapeutics. 2013;38(1):56–61. doi:10.1111/jcpt.12016
32. Mukonzo JK, Kengo A, Kutesa B, et al. Role of pharmacogenetics in rifampicin pharmacokinetics and the potential effect on TB-rifampicin sensitivity among Ugandan patients. Transactions of the Royal Society of Tropical Medicine and Hygiene. 2020;114(2):107–114. doi:10.1093/trstmh/trz108
33. Naidoo A, Chirehwa M, Ramsuran V, et al. Effects of genetic variability on rifampicin and isoniazid pharmacokinetics in South African patients with recurrent tuberculosis. Pharmacogenomics. 2019;20(4):225–240. doi:10.2217/pgs-2018-0166
34. Nishimura T, Kohno H, Nagai H, et al. The population pharmacokinetics of rifampicin in Japanese pulmonary tuberculosis patients. Drug Res. 2020;70(5):199–205. doi:10.1055/a-1122-8129
35. Perumal R, Arodola-Oladoyinbo O, Naidoo A, et al. Altered drug exposures of first-line TB drugs in a moxifloxacin-containing treatment regimen. Int J Tuberc Lung Dis. 2022;26(8):766–774. doi:10.5588/ijtld.21.0702
36. Schipani A, Pertinez H, Mlota R, et al. A simultaneous population pharmacokinetic analysis of rifampicin in Malawian adults and children. Br. J. Clin. Pharmacol. 2016;81(4):679–687. doi:10.1111/bcp.12848
37. Seng K-Y, Hee K-H, Soon G-H, et al. Population pharmacokinetics of rifampicin and 25-deacetyl-rifampicin in healthy Asian adults. J Antimicrob Chemother. 2015;70(12):3298–3306. doi:10.1093/jac/dkv268
38. Sloan DJ, McCallum AD, Schipani A, et al. Genetic determinants of the pharmacokinetic variability of rifampin in Malawian adults with pulmonary tuberculosis. Antimicrob. Agents Chemother. 2017;61(7). doi:10.1128/AAC.00210-17.
39. Soedarsono S, et al. Development of Population Pharmacokinetics Model and Bayesian Estimation of Rifampicin Exposure in Indonesian Patients With Tuberculosis. Tuberculosis; 2023:139.
40. Wilkins JJ, Savic RM, Karlsson MO, et al. Population pharmacokinetics of rifampin in pulmonary tuberculosis patients, including a semimechanistic model to describe variable absorption. Antimicrob. Agents Chemother. 2008;52(6):2138–2148. doi:10.1128/AAC.00461-07
41. Svensson RJ, Aarnoutse RE, Diacon AH, et al. A population pharmacokinetic model incorporating saturable pharmacokinetics and autoinduction for high rifampicin doses. Clin Pharmacol Ther. 2018;103(4):674–683. doi:10.1002/cpt.778
42. Hoa PQ, Kim HK, Jang TW, et al. Population pharmacokinetic model of rifampicin for personalized tuberculosis pharmacotherapy: effects of SLCO1B1 polymorphisms on drug exposure. Int J Antimicrob Agents. 2024;63(2):107034. doi:10.1016/j.ijantimicag.2023.107034
43. Aruldhas BW, Hoglund RM, Ranjalkar J, et al. Optimization of dosing regimens of isoniazid and rifampicin in children with tuberculosis in India. Br. J. Clin. Pharmacol. 2019;85(3):644–654. doi:10.1111/bcp.13846
44. Denti P, Wasmann RE, van Rie A, et al. Optimizing dosing and fixed-dose combinations of rifampicin, isoniazid, and pyrazinamide in pediatric patients with tuberculosis: a prospective population pharmacokinetic study. Clinl Infect Dis. 2022;75(1):141–151. doi:10.1093/cid/ciab908
45. Horita Y, Alsultan A, Kwara A, et al. Evaluation of the adequacy of WHO revised dosages of the first-line antituberculosis drugs in children with tuberculosis using population pharmacokinetic modeling and simulations. Antimicrob. Agents Chemother. 2018;62(9). doi:10.1128/AAC.00008-18.
46. Panjasawatwong N, Wattanakul T, Hoglund RM, et al. Population pharmacokinetic properties of antituberculosis drugs in Vietnamese children with tuberculous meningitis. Antimicrob Agents Chemother. 2020;65(1). doi:10.1128/AAC.00487-20.
47. Zvada SP, Denti P, Donald PR, et al. Population pharmacokinetics of rifampicin, pyrazinamide and isoniazid in children with tuberculosis: in silico evaluation of currently recommended doses. J Antimicrob Chemother. 2014;69(5):1339–1349. doi:10.1093/jac/dkt524
48. Savic RM, Ruslami R, Hibma JE, et al. Pediatric tuberculous meningitis: model-based approach to determining optimal doses of the anti-tuberculosis drugs rifampin and levofloxacin for children. Clin. Pharmacol. Ther. 2015;98(6):622–629. doi:10.1002/cpt.202
49. Smythe W, Khandelwal A, Merle C, et al. A semimechanistic pharmacokinetic-enzyme turnover model for rifampin autoinduction in adult tuberculosis patients. Antimicrob. Agents Chemother. 2012;56(4):2091–2098. doi:10.1128/AAC.05792-11
50. Jeon CY, Murray MB. Diabetes mellitus increases the risk of active tuberculosis: a systematic review of 13 observational studies. PLoS Med. 2008;5(7):e152. doi:10.1371/journal.pmed.0050152
51. Hobson S, Gandhi S, Sobel M. Intrahepatic cholestasis of pregnancy. Cmaj. 2022;194(48):E1650. doi:10.1503/cmaj.220334
52. Pavek P, Ceckova M, Staud F. Variation of drug kinetics in pregnancy. Curr Drug Metab. 2009;10(5):520–529. doi:10.2174/138920009788897993
53. Holford N, Heo YA, Anderson B. A pharmacokinetic standard for babies and adults. J Pharm Sci. 2013;102(9):2941–2952. doi:10.1002/jps.23574
54. Pasipanodya JG, McIlleron H, Burger A, et al. Serum drug concentrations predictive of pulmonary tuberculosis outcomes. J Infect Dis. 2013;208(9):1464–1473. doi:10.1093/infdis/jit352
55. Nyberg J, Ueckert S, Strömberg EA, et al. PopED: an extended, parallelized, nonlinear mixed effects models optimal design tool. Comput Methods Programs Biomed. 2012;108(2):789–805. doi:10.1016/j.cmpb.2012.05.005
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Population Pharmacokinetics of Tiapride in Children and Adolescents with Tic Disorders: Leveraging Plasma and Saliva Concentration to Guide Individualized Dosing
Huang W, Shen J, Luo X, Wu Y, Zheng Y, Zhou J, Xu B, Yin X, Wu X
Drug Design, Development and Therapy 2026, 20:587387
Published Date: 21 April 2026