Back to Journals » OncoTargets and Therapy » Volume 12
Pancreatic cancer in young adults: changes, challenges, and solutions
Authors Primavesi F ![]() , Stättner S
, Stättner S ![]() , Schlick K, Kiesslich T, Mayr C, Klieser E, Urbas R, Neureiter D
, Schlick K, Kiesslich T, Mayr C, Klieser E, Urbas R, Neureiter D
Received 15 January 2019
Accepted for publication 27 February 2019
Published 6 May 2019 Volume 2019:12 Pages 3387—3400
DOI https://doi.org/10.2147/OTT.S176700
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Arseniy Yuzhalin
Florian Primavesi,1 Stefan Stättner,1 Konstantin Schlick,2 Tobias Kiesslich,3,4 Christian Mayr,3,4 Eckhard Klieser,5,6 Romana Urbas,5,6 Daniel Neureiter5,6
1Department of Visceral, Transplant and Thoracic Surgery, Medical University of Innsbruck, Innsbruck, Austria; 2Department of Internal Medicine III – Division of Hematology, Medical Oncology, Hemostaseology, Rheumatology, Infectiology and Oncologic Center, Paracelsus Medical University, Salzburg, Austria; 3Department of Internal Medicine I, Paracelsus Medical University/Salzburger Landeskliniken (SALK), Salzburg, Austria; 4Institute of Physiology and Pathophysiology, Paracelsus Medical University, Salzburg, Austria; 5Institute of Pathology, Paracelsus Medical University/Salzburger Landeskliniken (SALK), Salzburg, Austria; 6Cancer Cluster Salzburg, Salzburg, Austria
Abstract: Despite improvements in multidisciplinary treatments, survival of pancreatic cancer (PC) patients remains dismal. Studies dealing with early onset pancreatic cancer (EOPC) patients are scarce. In this review, we discuss differences between EOPC and late-onset pancreatic cancer based on findings in original papers and reviews with a focus on morphology, genetics, clinical outcomes and therapy. In conclusion, families with a positive history of PC and patients with BRCA 1 or 2 mutations should be monitored. Patients with EOPC usually present with better overall fitness compared to the average PC population, however often with even more aggressive cancer behaviour. Therefore, potent state-of-the-art multi-modal systemic therapies should be applied whenever possible. Large-scale registries and randomized clinical trials dealing with EOPC in regard to distinct biology and outcome are warranted.
Keywords: early onset pancreatic cancer, risk factors, resectability, chemotherapy, surgery
Introduction
Pancreatic cancer (PC) is one of the deadliest malignant diseases, despite the availability of enhanced molecular tumor-associated technologies and novel therapeutic strategies in the past years.1 PC represents the fourth leading cause of cancer death with an estimated 7% five-year survival rate in the US,2 where epidemiological prediction models estimate it to become the second most frequent cause of cancer-related death by 2030.3 According to the national statistics of Austria, 1,757 new cases of PC were diagnosed in 2015, representing 4% of all malignancies ranking third as the leading causes of cancer-related deaths4 (Figure 1). Analysis of large clinical databases showed that the median age of patients with PC was about 70 years. Since younger patients are rarely affected, with <2% according to the actual Surveillance, Epidemiology, and End Results (SEER) registry (<45 years) and 3.4% in the Austrian registry (<50 years), clinical and pathological studies dealing with this specific patient cohorts are limited (Figure 1). In other recently published national analyses, the percentage of patients with PC and age <50 years at diagnosis was less than 10% as well.5,6 This patient group is commonly referred to as “early onset” or “very early onset pancreatic cancer” (EOPC) groups, depending on the applied age cutoff (<40, <45, or <50 years).5–8 Comparison of clinicopathologic data of younger and older patients showed no major statistically relevant differences in the literature (Table 1). Heterogeneous data regarding relevant clinical endpoints such as overall survival (OS), progression-free survival (PFS), or disease-free survival (DFS) are reported, whereby younger patients with PC consistently show better outcome values compared to older patients, which is reasonably explained by better physical constitution and reduced comorbidities in this patient group.9
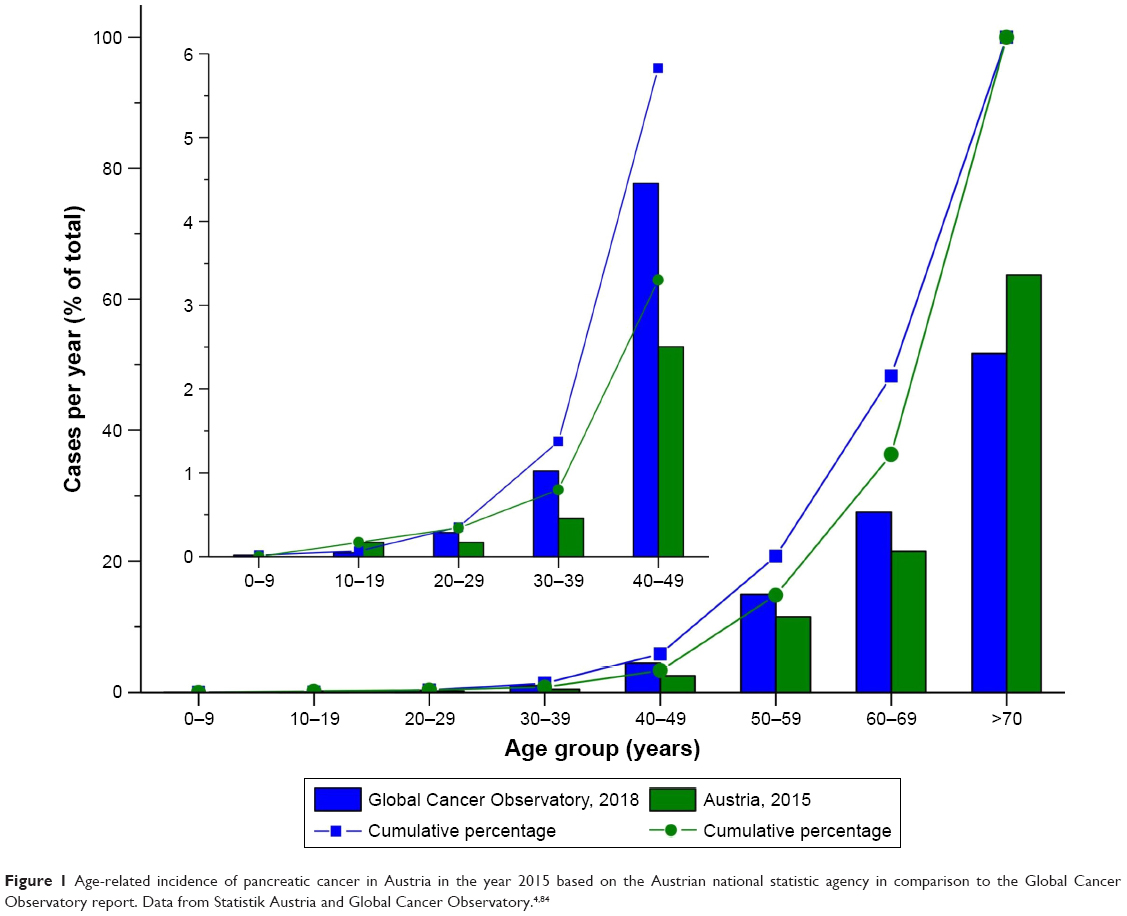 | Figure 1 Age-related incidence of pancreatic cancer in Austria in the year 2015 based on the Austrian national statistic agency in comparison to the Global Cancer Observatory report. Data from Statistik Austria and Global Cancer Observatory.4,84 |
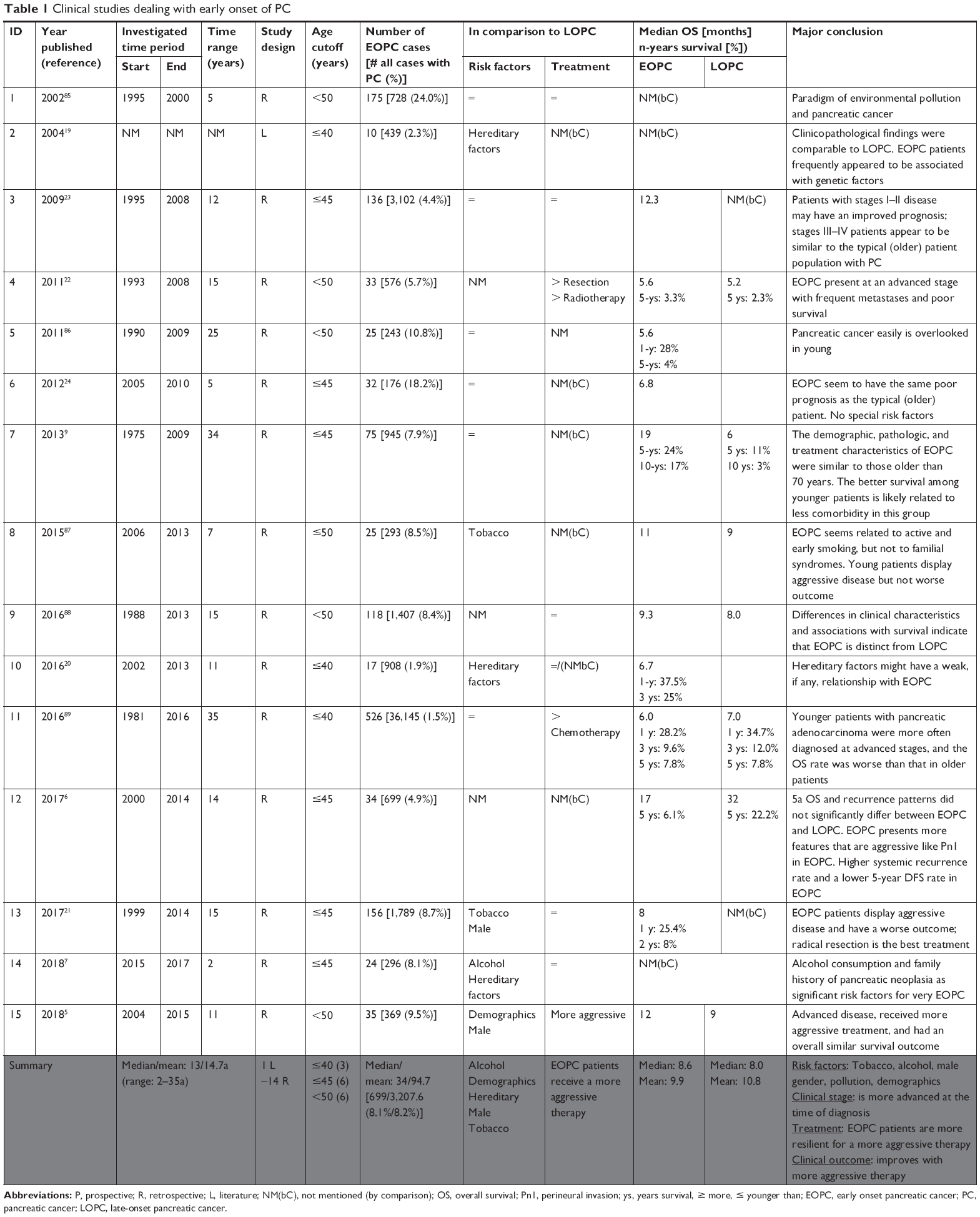 | Table 1 Clinical studies dealing with early onset of PC |
Surgical resection remains the only curative-intent therapeutic option in PC patients regardless of their age.9 State-of-the-art neoadjuvant chemotherapeutic approaches including combination schemas such as gemcitabine plus Abraxane, or FOLFIRINOX, are increasingly utilized in support for secondary surgery in primary unresectable cases of advanced PC even with major vascular invasion.10 Currently, numerous neoadjuvant chemotherapy and chemoradiotherapy trials are ongoing to elucidate new preoperative treatment strategies in order to bring more patients to resection.
The application of molecular techniques like next-generation sequencing technology with whole genome or exome sequencing has the potential to revolutionize the therapeutic armamentarium toward a patient-based molecular PC classification leading to a more personalized treatment with higher efficiency.11,12
Risk factors for EOPC development are similar to late-onset pancreatic cancers (LOPC), including tobacco exposure, alcohol abuse, chronic pancreatitis, diabetes mellitus (type 1 and 2), diet, obesity (body mass index over 40 kg/m2), previous radiotherapy, as well as previous cholecystectomy, gastrectomy, and infections.13,14 Nevertheless, intrinsic and genetic-dependent risk factors of PC like familial history15 and hereditary genetic syndromes, such as hereditary pancreatitis,16 are more frequently observed in EOPC.14,17 Therefore, specific germline genetic analyses (like of the breast cancer type 1/2 susceptibility proteins, BRCA) in families with increased incidence of PC could help identify patients with high risk for developing PC and initiate surveillance programs.18
This review summarizes critical challenges and potential solutions in EOPC ranging from clinicopathologic aspects and molecular-genetic findings to optimal therapeutic options of this specific patient group.
Clinical studies
Between 2002 and 2018, 15 clinical studies on EOPC were published (Table 1): in summary, besides a systematic literature review, all the other studies are of retrospective nature with a mean study period of about 14 years (range: 2–34 years), comparing a median/mean of 34/95 EOPC cases with 699/3,207 LOPC cases. Accordingly, the population of EOPCs accounted for about 8.1% of all PC cases in these cohorts.
Six of these 15 studies found significant differences between clinical risk factors including gender (male), alcohol consumption, and tobacco use as well as hereditary and demographic factors.7,19–21 Overall, no differences were found with regard to the applied therapeutic procedures. Regarding clinical outcome parameters, only two studies described that EOPC patients benefit relevantly from a more aggressive therapy,5,9 whereby the statistical analysis revealed comparable median and mean OS times for EOPC and LOPC. However, it has been reported that EOPC patients initially present with advanced disease stage at diagnosis,22 potentially explaining why EOPC patients show a worse OS in some studies in comparison to LOPC patients.21–24
Pathological findings
More than half a century after the first PC report in 1818 by Todd et al, Bohn et al published an article about a 6-month-old female child with metastatic PC, cytologically describing the tumor as “typical carcinoma simplex”. Since then, both Todd’s and Bohn’s cases were frequently cited by many other authors as examples of pancreatic tumors in young patients.25,26
To analyze differences in clinicopathological aspects between EOPC and LOPC, in 2004, Lüttges et al compared a cohort of ten EOPC with 70 LOPC cases. Six of these EOPC cases showed a typical phenotype of pancreatic ductal adenocarcinoma (PDAC), two showed poor or no differentiation, one showed adenosquamous differentiation, and one showed mucinous morphology. In summary, the authors stated that they did not observe marked pathological differences,19 which was in line with a retrospective analysis by Ntala et al,5 who performed a retrospective analysis using database searches and data extraction of inhabitants of the greater London area over an 11-year period. They did not find any significant differences in terms of location (P=0.579), differentiation (P=0.315), stage (P=0.194), perineural invasion (P=0.34), or blood vessel invasion (P=0.051), comparing EOPC and LOPC patients. Another retrospective analysis by Kang et al in 20176 revealed that perineural invasion occurs more frequently in EOPC patients (97.1% vs 79.0%, P=0.0043). Furthermore, poor differentiation was more commonly found in LOPC patients (34% vs 51%), while moderately differentiated cancers were more frequently found in EOPC patients (46% vs 38%).
Regarding immunohistochemical protein patterns, Lüttges’ et al and Bergmann et al did not find any differences in p53 nuclear expression or DPC4, respectively.19,27 Moreover, both assessed the expression patterns of mismatch-repair gene products (Lüttges et al, MLH1 and MSH2; Bergmann et al, MLH1, MSH2, and MSH6) and could not detect microsatellite instability in EOPC cases. In addition, Bergmann et al did not find any changes in SMAD 4 or EGFR expression and Lüttges et al did not find any changes in MUC1 expression, which is continuously expressed in PDAC.19,27 The only difference was the stage of disease at which patients were diagnosed. Tingstedt et al conducted a study in 2011 comparing 33 EOPC cases with matched controls, in which the young cohort presented with a more advanced clinical stage.22 In only six patients, the disease was still locally confined, while 52% (n=17) showed initial distant metastases (P=0.001) and 27% (n=9) locoregional lymph node metastases (P=0.01). Nevertheless, in another paper published two years later, Jin He et al could not find any significant differences in the rate of lymph node positivity (P=0.27) and the lymph node ratio (P=0.78) between EOPC and LOPC patients.9
Molecular genetics
PC usually progresses from precursor lesions termed as pancreatic intraepithelial neoplasia (PanIN), classified as low-grade PanIN (PanIN-1) to high-grade PanIN (PanIN-3). This progression from precursor lesions is associated with an increased accumulation of specific gene mutations, resulting in activation of oncogenes and/or inactivation of tumor suppressors. Furthermore, the number of PanINs particularly with high-grade dysplasia is increased in patients with a family history of PC supporting the hypothesis that precursor lesions in these patients are often already established at a very young age.28 Genetic evolution of PC from the earliest genetic alteration in a precursor lesion to EOPC takes almost 12 years.
A well-known molecular driver of PC is the oncogene KRAS and its central role in PC development at various stages was shown in several studies: KRAS is mutated in about one-third of early disease stages and in 95% of advanced stages.29,30 Similarly, Nowak et al demonstrated that the gene encoding for c-MYC, another oncogene, is amplified in about 20%–30% of PC cases.31 Although the current literature suggests that genetic alterations of the c-MYC gene alone are not enough to drive PC tumorigenesis, Hessmann et al published that simultaneous alterations of both the c-MYC and KRAS genes heavily promote PC development.32
There are numerous other oncogenes involved in PC development and progression such as PAK4, MYB, and HER2, all regulating various cellular effects (for detailed review see Khan et al33). Silencing or loss of tumor suppressors also strongly contributes to the development of PC. Inactivation of the cell cycle inhibitor CDKN2a (p16) was described as an early event in PC development, resulting in uncontrolled cell divisions.34,35 Similarly, another cell cycle inhibitor, p53, is mutated in up to 75% of PC patients.36,37 In contrast to p16, mutations regarding the p53 gene are described as an event occurring at later stages of PC development.35 Mutations and deletions of SMAD4 are also common and associated with metastases and resistance toward chemotherapy.38 Like p16 and p53, the major tumor-suppressive role of SMAD4 is negative regulation of the cell cycle.
Mutations in the BRCA1 and BRCA2 genes are well-known predispositions for the development of breast and ovarian cancers.39 The products of these genes are involved in transcriptional control and DNA repair. However, recent reports connect BRCA1/2 mutations also with PC, as carriers of these mutations have an increased risk of PC development.40,41 Moreover, BRCA1/2 mutations in PC were observed more frequently in patients with familial PC, with a fivefold higher prevalence of these mutations compared to patients with unselected familial background.15 Also, the mean age of diagnosis was significantly lower in familial PC with BRCA1/2 mutations (BRCA1, 38 years; BRCA2, 39 years).17 These data suggest that, besides sporadic mutations, not only heritable factors contribute to PC but also family history regarding specific gene mutations represents a significant risk factor for PC development in young adults.
Besides these driver mutations and genetic alterations, several working groups conducted an interesting molecular classification approach.42–45 In these studies, the molecular characteristics of PDACs were comprehensively profiled with the aim to define different molecular PDAC subtypes (Table 2), based on their biological characteristics rather than by histology, resulting in significant prognostic implications. Although the sample material of these studies (eg, cell lines and primary resected tumors) and the screening methods (eg, gene expression microarray and whole genome sequencing) were not uniform, a set of molecular PDAC subtypes was clearly definable suggesting the existence of different biological backgrounds of PDAC. Interestingly, Waddell et al defined PDAC subtypes based on chromosomal rearrangements and reported that in the unstable-subtype (defined by a large number of rearrangement defects), BRCA1 and BRCA2 genes were frequently mutated.44 When comparing the underlying gene signatures of the postulated subtypes summarized in Table 2, a clear overlap becomes apparent (Table 2).46,47 For instance, when comparing the classical subtypes defined by Collisson et al, the classical subtypes defined by Moffitt et al, and the pancreatic progenitor subtypes by Bailey et al, a non-perfect overlap regarding the underlying gene signatures can be observed: for example, the gene CEACAM6 was described as an overexpressed subtype-defining gene in the studies by Collisson et al and Moffitt et al, and as an overexpressed gene in Bailey et al. A similar pattern was observed for numerous other genes. In other words, using varying approaches, the different working groups defined subtypes with biological similarity (to a certain extent), but used a different terminology to describe these subtypes. Based on such comparisons, others have described that the unstable-subtype identified by Waddell et al is similar to a certain degree to the quasi-mesenchymal, basal-like, and squamous subtype, respectively.47
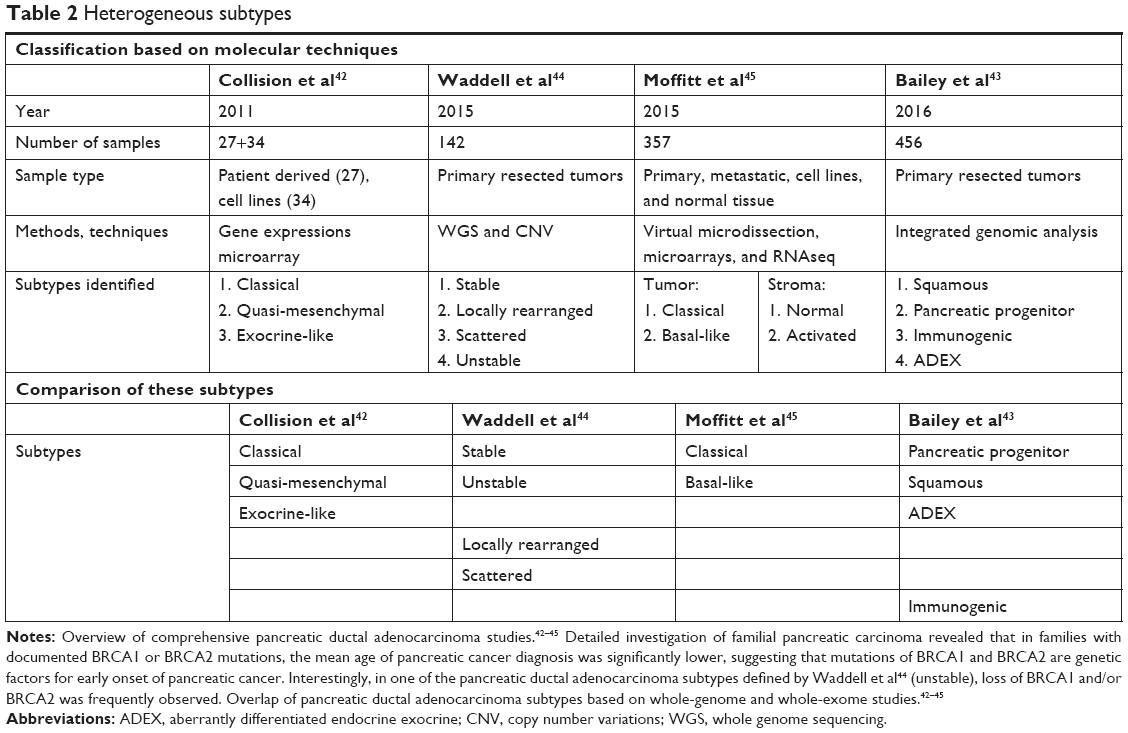 | Table 2 Heterogeneous subtypes |
Although these comparisons are still of descriptive nature and need further investigation, there is a possibility that the different terms or subtypes identified by the different working groups may describe (to a certain extent) similar biological subgroups of PC. The frequently observed BRCA1 and BRCA2 mutations in young PDAC patients might therefore be indicative of an underlying subtype with a specific genetic pattern. In view of the sophisticated methods used for this molecular classification, it will be of utmost importance for future studies to define consensus genetic patterns (eg, commonly mutated genes and upregulated or downregulated genes) among the different nomenclatures, which then may be translated into an immunohistochemical marker panel, new diagnostic approaches, as well as tailored therapeutic strategies for each subtype.
Therapeutic issues
Surgery
Surgical resection still represents the only potentially curative treatment for PC. After diagnostic evaluation of initial tumor stage and patient fitness, resectability is primarily determined through cross-sectional imaging techniques, ideally with contrast-enhanced computed tomography (CE-CT) or MRI (with lower accuracy in terms of vessel involvement).48 Local resectability is defined as either primary resectable PC, borderline resectable PC (BR-PC), or locally advanced PC (LA-PC), depending on the involvement of hepatic or mesenteric arterial and venous structures.49 Most commonly, patients with resectable PC should undergo surgical exploration with radical resection, while LA-PC patients should receive neoadjuvant therapy before exploration. In BR-PC, the debate regarding chemotherapy versus upfront resection is still ongoing (see section Chemotherapy). Patients with metastases are mostly considered for palliative treatment, although selected cases with limited spread might benefit from surgical resection after appropriate response to chemotherapy (Figure 2).50
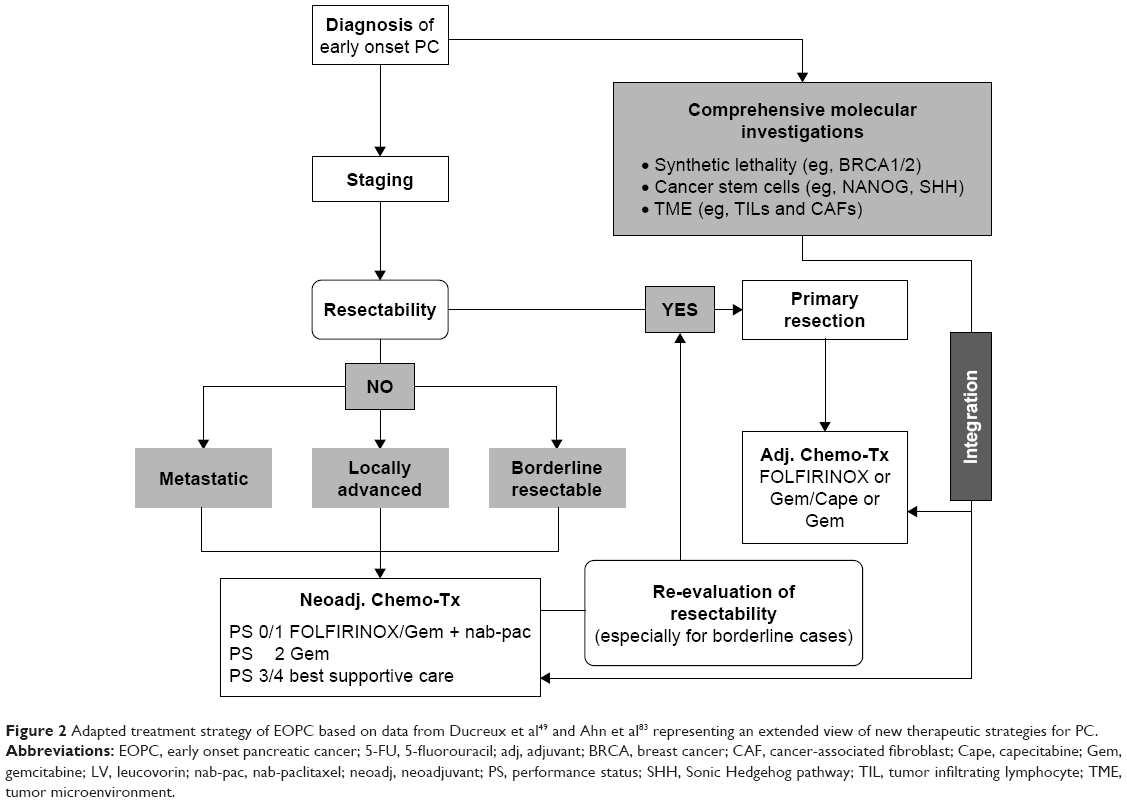 | Figure 2 Adapted treatment strategy of EOPC based on data from Ducreux et al49 and Ahn et al83 representing an extended view of new therapeutic strategies for PC. |
Diagnostic laparoscopy can help to rule out previously undetected local invasion or abdominal metastases, avoid futile explorative laparotomies, and define treatment paths, especially in patients at high risk for locally advanced tumors or systemic involvement.51–53
After surgical resection, the most common complications include pancreatic fistula, delayed gastric emptying, bleeding, and wound infections. Despite technical and perioperative improvements within the past years, overall mortality and morbidity after pancreatic resections even in experienced high-volume centers range at 2%–5% and 50%–60%, respectively. The only available study examining complications in young PC patients in detail compared 75 EOPC patients with a reference group of 870 PC patients at a median age of 75 years.9 With comparable other demographic, pathologic, and treatment characteristics, EOPC patients had significantly fewer postoperative complications (20% vs 31%). While pancreatic fistula (0% vs 8%) and delayed gastric emptying (5% vs 15%) were notably decreased, there was no significant difference in severe complications (Clavien-Dindo ≥3: 7% vs 13%) or 30-day mortality (0% vs 2%).
Since recent therapeutic improvements enable long-term survival rates of 20%–30% after surgery and adjuvant combination therapy,54 adverse effects of pancreatic resections leading to chronic conditions need to be addressed especially for young patients with a longer expected life span. For example, about 50% of patients undergoing distal pancreatectomy develop postoperative impaired glucose tolerance or new-onset diabetes.55 Furthermore, in a recent large, randomized, multicenter study, conducted in Germany, about 80% of the patients after pancreatoduodenectomy for pancreatic head cancer needed oral enzyme replacement after 12 months due to pancreatic exocrine insufficiency, 20% regularly experienced steatorrhea, and 30% developed new-onset diabetes that led to insulin dependency in two-thirds of the affected cases.56 Not only the type of pancreatic resection but also the type of pancreatic anastomosis after pancreatoduodenectomy may influence long-term complications and affect quality of life.57 However, so far only retrospective data are available and long-term results of prospective trials are warranted.56,58
Increased application of laparoscopic pancreatic resection could also further decrease postoperative complications and length of stay and possibly enhance quality of life in the future, but there are concerns regarding oncological safety.59 Since the data quality of available studies is still low,60,61 results of ongoing prospective trials are eagerly awaited.62,63
Concerning long-time follow-up, intensified radiological surveillance for early detection of recurrence, for example with enhanced imaging techniques such as PET-CT additionally to standard CE-CT, has shown increased sensitivity and specificity in a recent meta-analysis of seven retrospective studies.64 Although this might be of future importance especially in EOPC patients, prospective validation is pending and enhanced protocols to reduce significant radiation doses of PET-CT need to be considered.65
To further address the lack of evidence regarding surgical management of young patients with PC, their specific characteristics and therapeutic needs will also soon be assessed in a prospective registry analysis within the EURECCA (European Registry of Cancer Care or European Cancer Audit) network under auspices of the European Society of Surgical Oncology.66
Chemotherapy
Neoadjuvant therapy
To date, controversy still exists regarding the role of neoadjuvant systemic treatment versus upfront surgery followed by adjuvant therapy in primary resectable PC. Although, no randomized, prospective trial has been published so far, evidence from large-scale national registries such as the National Cancer Data Base from the US suggests that pathological outcomes might be improved after neoadjuvant treatment with higher rates of negative surgical margins (OR: 1.3) and negative lymph node state (OR: 2.9).67 Furthermore, preoperative chemotherapy compared to upfront resection did improve OS in a meta-analysis of studies providing intention-to-treat analysis of resectable or borderline-resectable patients.68 These studies are a principal proof that with neoadjuvant chemotherapy one can effectively treat micro-metastases in order to prolong OS not only in breast and gastric cancers but also in PC patients. The weighted median OS was 18.8 months for neoadjuvant therapy and 14.8 months for upfront surgery, and the difference was even larger in those patients that ultimately underwent resection (26.1 vs 15.0 months), also resulting in an increased R0 resection rate (87% vs 67%) and lower positive lymph node rates. This OS benefit was achieved, despite a lower percentage of patients finally undergoing resection in the neoadjuvant group (66% vs 81%). Hereby, neoadjuvant therapy serves as a test of tumor biology and patient fitness filtering out those patients that will not benefit from resection due to aggressive tumor progression or poor performance status. Until more solid evidence is available, the decision to apply neoadjuvant chemotherapy in resectable PC patients remains to be highly individual, based not only on anatomical but also on biological (CA 19–9>500 IU/mL or suspected lymph node metastases) and clinical patient conditions (performance status). This has recently been proposed in the 2017 definition of borderline resectability of the International Association of Pancreatology.69 Patients with EOPC were not explicitly addressed in the analysis of the aforementioned studies. Since they represent a cohort with often biologically aggressive tumors, neoadjuvant therapy might be a key element to increase survival in resectable EOPC patients in the future.
After neoadjuvant treatment, all patients with PC showing stable disease or visible tumor response after restaging should undergo surgical exploration after restaging. Only cases with obvious progress should continue with palliative therapy, since imaging response in this setting is rarely predicting intraoperative resectability or actual pathological regression.
Regarding patients with BR-PC, one randomized Phase II/III trial has been published to date comparing neoadjuvant chemoradiation with upfront resection followed by adjuvant therapy.70 This Korean study with 50 patients was terminated prematurely after showing a clear median and 2-year survival benefit (40.7% and 21 months vs 26.1% and 12 months) for the neoadjuvant therapy group.
Regarding patients with LA-PC, a number of studies have shown that preoperative treatment (eg, with FOLFIRINOX or chemoradiation) results in markedly improved OS compared to upfront resection, the latter in many cases being inferior to palliative treatment alone.48,71 Following neoadjuvant treatment, resection rates of around 50%–60% can be achieved, resulting in a median postoperative survival of 16 months (plus 5–6 months treatment time). Neoadjuvant treatment approaches have resulted in high rates of secondary resection, thus allowing conversion surgery in an otherwise palliative treatment situation. Only cases with obvious progress should continue with palliative therapy, since imaging response in this setting is rarely predicting intraoperative resectability or actual pathologic regression.
As high-level evidence with regard to neoadjuvant treatment in primary resectable PC is lacking, specific sub-analysis of young patients has not been conducted in BR-PC or LA-PC so far. Therefore, current recommendations for the general PC population should be applied also in EOPC patients until further evidence are generated.
Adjuvant therapy
Regarding postoperative systemic treatment (see Table 3 for summarizing the three major positive clinical trials in advanced PC72–74), major advances have been published within the past 2 years. First, in 2017, the ESPAC-4 trial has reported a median OS of 28.0 months after adjuvant combination therapy with gemcitabine and capecitabine (GemCap), providing the new gold standard since 2017.54 However, very recently, a joint group from France and Canada presented a late-breaking abstract at the annual ASCO 2018 meeting followed by publication in the New England Journal of Medicine of their results from the Phase III multicenter, randomized clinical trial PRODIGE 24/CCTG PA.6.75 This study compared adjuvant chemotherapy with modified (m)-FOLFIRINOX to gemcitabine. After a median follow-up of 30.5 months, the median DFS was 21.6 months in the m-FOLFIRINOX arm versus 12.8 months in the gemcitabine arm. Astonishingly, the median OS was 54.4 months versus 35.0 months, respectively, providing high-level evidence that treatment with m-FOLFIRINOX resulted in the longest OS yet reported following resection of PC. Toxicity, however, was much higher with m-FOLFIRINOX: 75.8% grade 3/4 adverse events versus 51.5% in the gemcitabine arm. This regimen should therefore only be considered for patients who are fit enough to tolerate it, which might be ideal especially for younger patients.
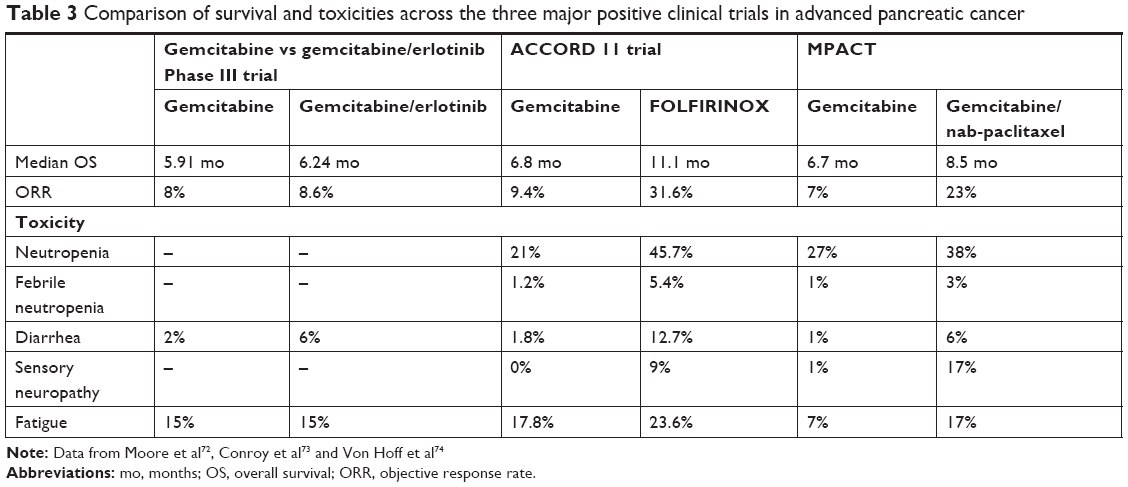 | Table 3 Comparison of survival and toxicities across the three major positive clinical trials in advanced pancreatic cancer |
Patients of age >75 years and with reduced Eastern Cooperative Oncology Group (ECOG) performance status should receive gemcitabine with or without capecitabine according to the ESPAC-4 trial.54 Although patients with EOPC were not specifically addressed in sub-analysis of both studies, patients <65 years experienced the same benefit from FOLFIRINOX (HR 0.61) or GemCap (HR 0.82) as older patients when compared to gemcitabine alone. Furthermore, patient age was not associated with survival in univariable analysis. Accordingly, until further evidence specifically on EOPC patients is available from prospective trials, FOLFIRINOX should represent the gold standard in adjuvant therapy also for all young patients after resection.
Palliative therapy
According to the latest ESMO guidelines, options for systemic treatment in palliative PC mainly depend on the performance status (ECOG) of patients.49 In cases with good ECOG status (0 or 1), combination chemotherapy with FOLFIRINOX or gemcitabine and nab-paclitaxel is recommended, while patients with ECOG 2 should receive gemcitabine with or without nab-paclitaxel. All others (ECOG 3/4, significant comorbidities, and short life expectancy) should receive symptomatic treatment only. The same principles apply for EOPC patients.
Radiotherapy
Indications for radiotherapy in PC among others include neoadjuvant therapy (chemoradiation), further as an adjunct treatment for positive resection margins after pancreatic surgery or in the setting of local recurrence after resection and palliation treatment. In a nationwide review of >14,000 patients with unresectable PC in the US, palliative chemotherapy (CTX; 38.1% of patients) alone was compared to CTX with external-beam radiotherapy (EBRT; 44.8%), intensity-modulated radiotherapy (IMRT; 2.3%), and stereotactic body radiotherapy (SBRT; 14.8%).76 After matching patients for demographics and tumor characteristics, SBRT treatment showed significantly longer median survival (13.9 months) than IMRT (12.2 months), EBRT (11.6 months), and chemotherapy alone (10.2 months). In this cohort, 44.9% of the patients were younger than 65 years, but no analysis on the impact of age on outcome was performed. In subsequent studies, SBRT was also very effective in terms of pain control, with more than 80% of patients with locally advanced or metastatic PC reporting partial or complete pain relief.77,78 However, acute and late toxicity rates (≥ grade 3) of 3%–18% and 6%–8% need to be taken into consideration, including duodenal, gastric or small bowel ulcers, perforation, hemorrhage, and obstruction.
In the setting of BR-PC or LA-PC, SBRT may also be effective additionally after neoadjuvant combination of CTX, for example, with FOLFIRINOX prior to resection (median survival 34 months) or after surgery, with no delay of initiation of adjuvant chemotherapy because of the short treatment course of SBRT (median survival after resection: 27 months).76 In case of R1 resection, a recent study reported a median survival of 22 months in patients receiving conventional adjuvant chemoradiation.79
About 30% of the patients develop isolated local recurrence after resection for PC.80 A systematic review published in 2017 compared re-resection with chemoradiotherapy (CRTX) and SBRT, however, with limited number of patients (n=100/153/60).80 Mortality was low with 0–1% for all treatment modalities. Re-resection studies showed the best outcome in terms of median survival after treatment of up to 32 months (range 16–32) versus 19 months (CRTX; range 16–19) and 16 months (SBRT; range 9–16). However, the cohorts were not matched and, therefore, probably differed in terms of patient’s fitness, comorbidities, and local tumor extent. Also, some newer studies showed a median survival of SBRT up to 36 months (range: 18–36) after treatment, but they were not readily available for this review.81,82 Furthermore, re-resection is potentially associated with a restricted quality of life due to necessity of mostly total pancreatectomy resulting in insulin-dependent diabetes in all patients.
To the best of our knowledge, so far, no publication specifically evaluated the applicability, survival outcomes, and quality-of-life data of radiotherapy in any of the above settings for young patients with PC. In the light of recent encouraging results, especially of SBRT, prospective studies should also focus on EOPC patients.
Discussion, summary, and outlook
Roughly estimated, about 50 EOPC cases are registered in Austria each year. Worldwide, the incidence figures are similar (Figure 1). Compared to other malignant diseases, this patient group thus represents a minority group. Regardless of whether patients develop PC at a young age or at an advanced age, the 5-year survival rate is conceivably poor. Nevertheless, the question arises whether there are differences between EOPC and LOPC. In morphological and immunohistochemical terms, several studies and case reports did not reveal any differences between these two patient groups.19,27 From a molecular genetic point of view, however, there are certain peculiarities. Typical oncogenes such as KRAS and c-Myc and the tumor suppressor genes TP53, CDKN2a, and SMAD4 also play a driving role in EOPC.29–31,34–38 However, special attention should be paid to patients with mutations in the BRCA1/2 genes. These mutations occur primarily in cases with familial pancreatic carcinoma and, in addition, these patients show a particularly early disease onset.15,40,41 Consequently, members of a family with numerous PCs in history or even BRCA1/2 germline mutations need specific surveillance. In addition, potential molecular subtypes (Table 2) may not only explain a link with BRCA1/2 mutations in EOPC but also prove the existence of different biological backgrounds and supply new starting points for diagnostic approaches and therapies.42–45 However, these subtypes need to be specified more in detail first.
At present, surgical resection is still the only potentially curative therapeutic approach,50 and similar to LOPC, early detection is crucial to ensure resectability in EOPC. In order to avoid futile pancreatectomy or R2 pancreatic resections, preoperative evaluation of resectability by experienced surgeons and radiologists is important to distinguish between upfront resectable, BR-PC, and LA-PC in order to utilize the optimal therapeutic options. Not surprisingly, EOPC patients experience significantly fewer postoperative complications after surgical intervention than LOPC patients due to lower comorbidities of affected patients. As previously mentioned, there is no study to date that explicitly examines the behavior of EOPC in relation to (neo)adjuvant or palliative chemotherapy or radiotherapy. Nevertheless, a number of studies conducted in the general PC population – although not distinguishing between different patient age groups – show advantages of neoadjuvant chemotherapy over upfront surgery.67,68,70 Even in a palliative setting, patients do clearly benefit from systemic chemotherapy.49 Notably, EOPC patients are more susceptible to multimodal therapy approaches due to better performance status. In conclusion, EOPC seems to be associated with familial accumulation and mutations in BRCA-1 and -2 genes. Therefore, patients with these risk factors should be closely monitored. Furthermore, several trials are currently ongoing involving PARP inhibitors, specifically targeting BRCA-mutated cancers.83 The development of molecular subtypes may give new insights for future diagnostic and therapeutic approaches, but consensual definitions are still pending. Since EOPC patients usually present with fewer comorbidities, they are more susceptible to a multi-modal therapy. Concerning future treatment targets, comprehensive molecular investigations will particularly focus on cancer stem cells as well as tumor microenvironment including the stroma and immune system, for example, by analyzing tumor-infiltrating lymphocytes and cancer-associated fibroblast (Figure 2).83 The ultimate goal of all these investigations is to overcome chemotherapy resistance and advance treatment successes in this highly aggressive malignant disease.
Disclosure
The authors report no conflicts of interest in this work.
References
Tesfaye AA, Kamgar M, Azmi A, Philip PA. The evolution into personalized therapies in pancreatic ductal adenocarcinoma: challenges and opportunities. Expert Rev Anticancer Ther. 2018;18(2):131–148. doi:10.1080/14737140.2018.1417844 | ||
Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7–30. doi:10.3322/caac.21442 | ||
Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74(11):2913–2921. doi:10.1158/0008-5472.CAN-14-0155 | ||
Statistik Austria, Jahrbuch der Gesundheitsstatistik 2016. Available from: https://www.statistik.at/web_de/services/publikationen/4/index.html?includePage=detailedView§ionName=Gesundheit&pubId=495. Accessed January 14, 2019. | ||
Ntala C, Debernardi S, Feakins RM, Crnogorac-Jurcevic T. Demographic, clinical, and pathological features of early onset pancreatic cancer patients. BMC Gastroenterol. 2018;18(1):139. doi:10.1186/s12876-018-0863-2 | ||
Kang JS, Jang JY, Kwon W, Han Y, Kim SW. Clinicopathologic and survival differences in younger patients with pancreatic ductal adenocarcinoma-A propensity score-matched comparative analysis. Pancreatology. 2017;17(5):827–832. doi:10.1016/j.pan.2017.08.013 | ||
Bunduc S, Iacob R, Costache R, Stoica B, Radu C, Gheorghe C. Very early onset pancreatic adenocarcinoma – clinical presentation, risk factors and therapeutic options. Chirurgia (Bucur). 2018;113(3):405–411. doi:10.21614/chirurgia.113.3.405 | ||
McWilliams RR, Maisonneuve P, Bamlet WR, et al. Risk factors for early-onset and very-early-onset pancreatic adenocarcinoma: a Pancreatic Cancer Case-Control Consortium (PanC4) analysis. Pancreas. 2016;45(2):311–316. doi:10.1097/MPA.0000000000000392 | ||
He J, Edil BH, Cameron JL, et al. Young patients undergoing resection of pancreatic cancer fare better than their older counterparts. J Gastrointest Surg. 2013;17(2):339–344. doi:10.1007/s11605-012-2066-4 | ||
Chin V, Nagrial A, Sjoquist K, et al. Chemotherapy and radiotherapy for advanced pancreatic cancer. Cochrane Database Syst Rev. 2018;3:CD011044. | ||
Roberts NJ, Norris AL, Petersen GM, et al. Whole genome sequencing defines the genetic heterogeneity of familial pancreatic cancer. Cancer Discov. 2016;6(2):166–175. doi:10.1158/2159-8290.CD-15-0402 | ||
Sjoquist KM, Chin VT, Chantrill LA, et al. Personalising pancreas cancer treatment: when tissue is the issue. World J Gastroenterol. 2014;20(24):7849–7863. doi:10.3748/wjg.v20.i24.7849 | ||
Becker AE, Hernandez YG, Frucht H, Lucas AL. Pancreatic ductal adenocarcinoma: risk factors, screening, and early detection. World J Gastroenterol. 2014;20(32):11182–11198. doi:10.3748/wjg.v20.i32.11182 | ||
Raimondi S, Maisonneuve P, Lohr JM, Lowenfels AB. Early onset pancreatic cancer: evidence of a major role for smoking and genetic factors. Cancer Epidemiol Biomarkers Prev. 2007;16(9):1894–1897. doi:10.1158/1055-9965.EPI-07-0341 | ||
Chen F, Roberts NJ, Klein AP. Inherited pancreatic cancer. Chin Clin Oncol. 2017;6(6):58. doi:10.21037/cco | ||
Raphael KL, Willingham FF. Hereditary pancreatitis: current perspectives. Clin Exp Gastroenterol. 2016;9:197–207. doi:10.2147/CEG.S84358 | ||
Kim DH, Crawford B, Ziegler J, Beattie MS. Prevalence and characteristics of pancreatic cancer in families with BRCA1 and BRCA2 mutations. Fam Cancer. 2009;8(2):153–158. doi:10.1007/s10689-008-9220-x | ||
Salo-Mullen EE, O’Reilly EM, Kelsen DP, et al. Identification of germline genetic mutations in patients with pancreatic cancer. Cancer. 2015;121(24):4382–4388. doi:10.1002/cncr.29664 | ||
Luttges J, Stigge C, Pacena M, Kloppel G. Rare ductal adenocarcinoma of the pancreas in patients younger than age 40 years. Cancer. 2004;100(1):173–182. doi:10.1002/cncr.11860 | ||
Ohmoto A, Yachida S, Kubo E, et al. Clinicopathologic features and germline sequence variants in young patients (</=40 years old) with pancreatic ductal adenocarcinoma. Pancreas. 2016;45(7):1056–1061. doi:10.1097/MPA.0000000000000574 | ||
Jiang QL, Zhang SS, Chen YT, Zhang JW, Wang CF. Risk factors for early-onset pancreatic cancer patients, and survival analysis. Int J Clin Exp Med. 2017;10(6):9416–9423. | ||
Tingstedt B, Weitkamper C, Andersson R. Early onset pancreatic cancer: a controlled trial. Ann Gastroenterol. 2011;24(3):206–212. | ||
Duffy A, Capanu M, Allen P, et al. Pancreatic adenocarcinoma in a young patient population 12-year experience at Memorial Sloan Kettering Cancer Center. J Surg Oncol. 2009;100(1):8–12. doi:10.1002/jso.21292 | ||
Raissouni S, Rais G, Mrabti H, et al. Pancreatic adenocarcinoma in young adults in a moroccan population. J Gastrointest Cancer. 2012;43(4):607–611. doi:10.1007/s12029-012-9407-0 | ||
Vejcho S. Carcinoma of the pancreas in childhood: a case report of long term survival. J Med Assoc Thai. 1993;76(3):177–183. | ||
Corner BD. Primary carcinoma of the pancreas in an infant aged seven months. Arch Dis Child. 1943;18(94):106–108. | ||
Bergmann F, Aulmann S, Wente MN, et al. Molecular characterisation of pancreatic ductal adenocarcinoma in patients under 40. J Clin Pathol. 2006;59(6):580–584. doi:10.1136/jcp.2005.027292 | ||
Shi C, Klein AP, Goggins M, et al. Increased prevalence of precursor lesions in familial pancreatic cancer patients. Clin Cancer Res. 2009;15(24):7737–7743. doi:10.1158/1078-0432.CCR-09-0004 | ||
Pylayeva-Gupta Y, Grabocka E, Bar-Sagi D. RAS oncogenes: weaving a tumorigenic web. Nat Rev Cancer. 2011;11(11):761–774. doi:10.1038/nrc3106 | ||
Eser S, Schnieke A, Schneider G, Saur D. Oncogenic KRAS signalling in pancreatic cancer. Br J Cancer. 2014;111(5):817–822. doi:10.1038/bjc.2014.215 | ||
Nowak NJ, Gaile D, Conroy JM, et al. Genome-wide aberrations in pancreatic adenocarcinoma. Cancer Genet Cytogenet. 2005;161(1):36–50. doi:10.1016/j.cancergencyto.2005.01.009 | ||
Hessmann E, Schneider G, Ellenrieder V, Siveke JT. MYC in pancreatic cancer: novel mechanistic insights and their translation into therapeutic strategies. Oncogene. 2016;35(13):1609–1618. doi:10.1038/onc.2015.216 | ||
Khan MA, Azim S, Zubair H, et al. Molecular drivers of pancreatic cancer pathogenesis: looking inward to move forward. Int J Mol Sci. 2017;18(4):779. doi:10.3390/ijms18040779 | ||
Kanda M, Matthaei H, Wu J, et al. Presence of somatic mutations in most early-stage pancreatic intraepithelial neoplasia. Gastroenterology. 2012;142(4):730–733e9. doi:10.1053/j.gastro.2011.12.042 | ||
Distler M, Aust D, Weitz J, Pilarsky C, Grutzmann R. Precursor lesions for sporadic pancreatic cancer: PanIN, IPMN, and MCN. Biomed Res Int. 2014;2014:474905. doi:10.1155/2014/474905 | ||
Redston MS, Caldas C, Seymour AB, et al. p53 mutations in pancreatic carcinoma and evidence of common involvement of homocopolymer tracts in DNA microdeletions. Cancer Res. 1994;54(11):3025–3033. | ||
Morton JP, Timpson P, Karim SA, et al. Mutant p53 drives metastasis and overcomes growth arrest/senescence in pancreatic cancer. Proc Natl Acad Sci U S A. 2010;107(1):246–251. doi:10.1073/pnas.0908428107 | ||
Chen YW, Hsiao PJ, Weng CC, et al. SMAD4 loss triggers the phenotypic changes of pancreatic ductal adenocarcinoma cells. BMC Cancer. 2014;14:181. doi:10.1186/1471-2407-14-181 | ||
King MC, Marks JH, Mandell JB. New York Breast Cancer Study G. Breast and ovarian cancer risks due to inherited mutations in BRCA1 and BRCA2. Science. 2003;302(5645):643–646. doi:10.1126/science.1088759 | ||
Thompson D, Easton DF. Breast Cancer Linkage C. Cancer incidence in BRCA1 mutation carriers. J Natl Cancer Inst. 2002;94(18):1358–1365. | ||
Breast Cancer Linkage C. Cancer risks in BRCA2 mutation carriers. J Natl Cancer Inst. 1999;91(15):1310–1316. | ||
Collisson EA, Sadanandam A, Olson P, et al. Subtypes of pancreatic ductal adenocarcinoma and their differing responses to therapy. Nat Med. 2011;17(4):500–503. doi:10.1038/nm.2344 | ||
Bailey P, Chang DK, Nones K, et al. Genomic analyses identify molecular subtypes of pancreatic cancer. Nature. 2016;531(7592):47–52. doi:10.1038/nature16965 | ||
Waddell N, Pajic M, Patch AM, et al. Whole genomes redefine the mutational landscape of pancreatic cancer. Nature. 2015;518(7540):495–501. doi:10.1038/nature14169 | ||
Moffitt RA, Marayati R, Flate EL, et al. Virtual microdissection identifies distinct tumor- and stroma-specific subtypes of pancreatic ductal adenocarcinoma. Nat Genet. 2015;47(10):1168–1178. doi:10.1038/ng.3398 | ||
Du Y, Zhao B, Liu Z, et al. Molecular subtyping of pancreatic cancer: translating genomics and transcriptomics into the clinic. J Cancer. 2017;8(4):513–522. doi:10.7150/jca.17622 | ||
Pishvaian MJ, Brody JR. Therapeutic implications of molecular subtyping for pancreatic cancer. Oncology (Williston Park). 2017;31(3):159–166, 168. | ||
Hackert T. Surgery for pancreatic cancer after neoadjuvant treatment. Ann Gastroenterol Surg. 2018;2(6):413–418. doi:10.1002/ags3.12203 | ||
Ducreux M, Cuhna AS, Caramella C, et al. Cancer of the pancreas: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2015;26(Suppl 5):v56–v68. doi:10.1093/annonc/mdv295 | ||
Hackert T, Niesen W, Hinz U, et al. Radical surgery of oligometastatic pancreatic cancer. Eur J Surg Oncol. 2017;43(2):358–363. doi:10.1016/j.ejso.2016.10.023 | ||
Peng JS, Mino J, Monteiro R, et al. Diagnostic laparoscopy prior to neoadjuvant therapy in pancreatic cancer is high yield: an analysis of outcomes and costs. J Gastrointest Surg. 2017;21(9):1420–1427. doi:10.1007/s11605-017-3470-6 | ||
Allen VB, Gurusamy KS, Takwoingi Y, Kalia A, Davidson BR. Diagnostic accuracy of laparoscopy following computed tomography (CT) scanning for assessing the resectability with curative intent in pancreatic and periampullary cancer. Cochrane Database Syst Rev. 2016;7:CD009323. | ||
Paracha M, Van Orden K, Patts G, Tseng J, McAneny D, Sachs T. Opportunity lost? Diagnostic laparoscopy in patients with pancreatic cancer in the national surgical quality improvement program database. World J Surg. 2018;43(3):937–943. | ||
Neoptolemos JP, Palmer DH, Ghaneh P, et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): a multicentre, open-label, randomised, phase 3 trial. Lancet. 2017;389(10073):1011–1024. doi:10.1016/S0140-6736(16)32409-6 | ||
Kang JS, Jang JY, Kang MJ, et al. Endocrine function impairment after distal pancreatectomy: incidence and related factors. World J Surg. 2016;40(2):440–446. doi:10.1007/s00268-015-3228-9 | ||
Keck T, Wellner UF, Bahra M, et al. Pancreatogastrostomy versus pancreatojejunostomy for RECOnstruction after PANCreatoduodenectomy (RECOPANC, DRKS 00000767): perioperative and long-term results of a multicenter randomized controlled trial. Ann Surg. 2016;263(3):440–449. | ||
Schmidt U, Simunec D, Piso P, Klempnauer J, Schlitt HJ. Quality of life and functional long-term outcome after partial pancreatoduodenectomy: pancreatogastrostomy versus pancreatojejunostomy. Ann Surg Oncol. 2005;12(6):467–472. doi:10.1245/ASO.2005.04.005 | ||
Wellner UF, Brett S, Bruckner T, et al. Pancreatogastrostomy versus pancreatojejunostomy for RECOnstruction after partial PANCreatoduodenectomy (RECOPANC): study protocol of a randomized controlled trial UTN U1111-1117-9588. Trials. 2012;13:45. doi:10.1186/1745-6215-13-45 | ||
van Hilst J, de Rooij T, Klompmaker S, et al. Minimally invasive versus open distal pancreatectomy for ductal adenocarcinoma (DIPLOMA): a Pan-European propensity score matched study. Ann Surg. 2019;269(1):10–17. doi:10.1097/SLA.0000000000002561 | ||
Riviere D, Gurusamy KS, Kooby DA, et al. Laparoscopic versus open distal pancreatectomy for pancreatic cancer. Cochrane Database Syst Rev. 2016;4:CD011391. | ||
Klompmaker S, van Hilst J, Wellner UF, et al. Outcomes after minimally-invasive versus open pancreatoduodenectomy: a Pan-European propensity score matched study. Ann Surg. 2018. Epub 2018, June 1. | ||
de Rooij T, van Hilst J, Bosscha K, et al. Minimally invasive versus open pancreatoduodenectomy (LEOPARD-2): study protocol for a randomized controlled trial. Trials. 2018;19(1):1. doi:10.1186/s13063-017-2423-4 | ||
de Rooij T, van Hilst J, Busch OR, et al. Laparoscopic distal pancreatectomy for pancreatic ductal adenocarcinoma: time for a randomized controlled trial? results of an all-inclusive national observational study. Ann Surg. 2017;266(6):e84. doi:10.1097/SLA.0000000000001710 | ||
Daamen LA, Groot VP, Goense L, et al. The diagnostic performance of CT versus FDG PET-CT for the detection of recurrent pancreatic cancer: a systematic review and meta-analysis. Eur J Radiol. 2018;106:128–136. doi:10.1016/j.ejrad.2018.07.010 | ||
Saade C, Ammous A, Abi-Ghanem AS, Giesel F, Asmar K. Body weight-based protocols during whole body FDG PET/CT significantly reduces radiation dose without compromising image quality: findingsin a large cohort study. Acad Radiol. 2018. Epub 2018 August 22. | ||
EUropean REgistry of Cancer CAre or EURopEan CanCer Audit. Available from: https://www.essoweb.org/eurecca-activityreport/. Accessed January 14, 2019. | ||
Hashmi A, Kozick Z, Fluck M, et al. Neoadjuvant versus adjuvant chemotherapy for resectable pancreatic adenocarcinoma: a national cancer database analysis. Am Surg. 2018;84(9):1439–1445. | ||
Versteijne E, Vogel JA, Besselink MG, et al. Meta-analysis comparing upfront surgery with neoadjuvant treatment in patients with resectable or borderline resectable pancreatic cancer. Br J Surg. 2018;105(8):946–958. doi:10.1002/bjs.10870 | ||
Isaji S, Mizuno S, Windsor JA, et al. International consensus on definition and criteria of borderline resectable pancreatic ductal adenocarcinoma 2017. Pancreatology. 2018;18(1):2–11. doi:10.1016/j.pan.2017.11.011 | ||
Jang JY, Han Y, Lee H, et al. Oncological benefits of neoadjuvant chemoradiation with gemcitabine versus upfront surgery in patients with borderline resectable pancreatic cancer: a prospective, randomized, open-label, multicenter phase 2/3 trial. Ann Surg. 2018;268(2):215–222. doi:10.1097/SLA.0000000000002705 | ||
Hackert T, Sachsenmaier M, Hinz U, et al. Locally advanced pancreatic cancer: neoadjuvant therapy with folfirinox results in resectability in 60% of the patients. Ann Surg. 2016;264(3):457–463. doi:10.1097/SLA.0000000000001850 | ||
Moore MJ, Goldstein D, Hamm J, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J Clin Oncol. 2007;25(15):1960–1966. doi:10.1200/JCO.2006.07.9525 | ||
Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011;364(19):1817–1825. doi:10.1056/NEJMoa1011923 | ||
Von Hoff DD, Ervin T, Arena FP, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med. 2013;369(18):1691–1703. doi:10.1056/NEJMoa1304369 | ||
Conroy T, Hammel P, Hebbar M, et al. FOLFIRINOX or gemcitabine as adjuvant therapy for pancreatic cancer. N Engl J Med. 2018;379(25):2395–2406. doi:10.1056/NEJMoa1809775 | ||
de Geus SWL, Eskander MF, Kasumova GG, et al. Stereotactic body radiotherapy for unresected pancreatic cancer: A nationwide review. Cancer. 2017;123(21):4158–4167. doi:10.1002/cncr.30856 | ||
Rwigema JC, Parikh SD, Heron DE, et al. Stereotactic body radiotherapy in the treatment of advanced adenocarcinoma of the pancreas. Am J Clin Oncol. 2011;34(1):63–69. doi:10.1097/COC.0b013e3181d270b4 | ||
Buwenge M, Macchia G, Arcelli A, et al. Stereotactic radiotherapy of pancreatic cancer: a systematic review on pain relief. J Pain Res. 2018;11:2169–2178. doi:10.2147/JPR.S167994 | ||
Park S, Kim SC, Hong SM, et al. Postoperative radiotherapy for pancreatic cancer with microscopically-positive resection margin. Anticancer Res. 2017;37(2):755–764. doi:10.21873/anticanres.11374 | ||
Groot VP, van Santvoort HC, Rombouts SJ, et al. Systematic review on the treatment of isolated local recurrence of pancreatic cancer after surgery; re-resection, chemoradiotherapy and SBRT. HPB (Oxford). 2017;19(2):83–92. doi:10.1016/j.hpb.2016.11.001 | ||
Ryan JF, Groot VP, Rosati LM, et al. Stereotactic body radiation therapy for isolated local recurrence after surgical resection of pancreatic ductal adenocarcinoma appears to be safe and effective. Ann Surg Oncol. 2018;25(1):280–289. doi:10.1245/s10434-017-6134-6 | ||
Comito T, Cozzi L, Zerbi A, et al. Clinical results of stereotactic body radiotherapy (SBRT) in the treatment of isolated local recurrence of pancreatic cancer after R0 surgery: a retrospective study. Eur J Surg Oncol. 2017;43(4):735–742. doi:10.1016/j.ejso.2016.12.012 | ||
Ahn DH, Ramanathan RK, Bekaii-Saab T. Emerging therapies and future directions in targeting the tumor stroma and immune system in the treatment of pancreatic adenocarcinoma. Cancers (Basel). 2018;10(6):193. doi:10.3390/cancers10110400 | ||
Global Cancer Observatory. Available from: https://gco.iarc.fr/today/online-analysis-table. Accessed January 14, 2019. | ||
Soliman AS, El-Ghawalby N, Ezzat F, et al. Unusually high rate of young-onset pancreatic cancer in the East Nile Delta region of Egypt. Int J Gastrointest Cancer. 2002;32(2–3):143–151. doi:10.1385/IJGC:32:2-3:143 | ||
Lin JC, Chan DC, Chen PJ, et al. Clinical characteristics of early onset pancreatic adenocarcinoma: a medical center experience and review of the literature. Pancreas. 2011;40(4):638–639. doi:10.1097/MPA.0b013e318214fe56 | ||
Piciucchi M, Capurso G, Valente R, et al. Early onset pancreatic cancer: risk factors, presentation and outcome. Pancreatology. 2015;15(2):151–155. doi:10.1016/j.pan.2015.01.013 | ||
Beeghly-Fadiel A, Luu HN, Du L, et al. Early onset pancreatic malignancies: clinical characteristics and survival associations. Int J Cancer. 2016;139(10):2169–2177. doi:10.1002/ijc.30273 | ||
Eguchi H, Yamaue H, Unno M, et al. Clinicopathological characteristics of young patients with pancreatic cancer: an analysis of data from Pancreatic Cancer Registry of Japan Pancreas Society. Pancreas. 2016;45(10):1411–1417. doi:10.1097/MPA.0000000000000636 |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.