Back to Journals » Psychology Research and Behavior Management » Volume 15
Over-Reporting of Somatic and Psychiatric PTSD Symptoms Among People Who Experienced Motor Vehicle Accidents and Did Not Seek Psychiatric Help in a Primary Care Setting
Authors Kertzman S, Vainder M, Spivak B, Goclaw Y, Markman U, Weizman A ![]() , Kupchik M
, Kupchik M
Received 30 September 2021
Accepted for publication 20 April 2022
Published 30 May 2022 Volume 2022:15 Pages 1347—1357
DOI https://doi.org/10.2147/PRBM.S340965
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Semion Kertzman,1,2 Michael Vainder,3 Baruch Spivak,1,2 Yosi Goclaw,1 Uri Markman,4 Abraham Weizman,2,5,6 Marina Kupchik1,2
1The Beer-Ya’akov/Ness Ziona Mental Health Center, Beer-Ya’akov, Israel; 2Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel; 3Environics Analytics, Toronto, Canada; 4The Abarbanel Mental Health Center, Bat Yam, Israel; 5Research Unit, Geha Mental Health Center, Petach Tikva, Israel; 6Felsenstein Medical Research Center, Petach Tikva, Israel
Correspondence: Semion Kertzman, Forensic Psychiatry Department, Beer-Yakov Mental Health Center, P.O. Box 1, Beer-Yakov, 70350, Israel, Tel +972-8-9776151, Fax +972-8-9776142, Email [email protected]
Background: Over-reporting of posttraumatic stress disorder (PTSD) symptoms has been observed in some cases, following a motor vehicle accident (MVA). It has been suggested, however, that these are cases of underdiagnoses in primary care settings. The current study focused on people with PTSD in primary care settings who experienced an MVA and do not seek psychiatric help.
Methods: In the over 3000 patient registry of a primary care clinic, 174 people who experienced an MVA (PE-MVA) were identified. The final sample included 45 PE-MVA, who were administered the Clinician-Administered Posttraumatic Stress Disorder Scale (CAPS-2), and completed the Injury Severity Scale (ISS) and the Minnesota Multiphasic Personality Inventory-2 (MMPI-2) content scales.
Results: PE-MVA with PTSD reported more psychopathology on both MMPI-2 and CAPS-2 than those without PTSD. Severity of injury, measured by the ISS, did not differ significantly between the two PE-MVA groups. The significant differences between the PE-MVA with PTSD and those without PTSD disappeared after adjusting for the covariates of bias scales [Infrequency (F) and Fake Bad (FBS)] in MMPI-2, but not in CAPS-2.
Conclusion: The results suggest that in primary care settings, PE-MVA with PTSD who do not seek psychiatric help, over-report psychiatric and somatic symptoms. In a personal injury setting the F scale of the MMPI-2 showed less sensitivity to exaggerated somatic symptoms than the FBS scale. Bias scales of PE-MVA with PTSD are major contributors to the elevation of the MMPI-2 scores but not the CAPS-2 score.
Keywords: posttraumatic stress disorder, PTSD, motor vehicle accidents, MVA, Minnesota multiphasic personality inventory-2, MMPI-2, clinician, administered posttraumatic stress disorder scale-2, CAPS-2, injury severity scale, ISS
Introduction
Motor vehicle accidents (MVA) are the leading cause of posttraumatic stress disorder (PTSD) in civilian populations.1 Diagnosing PTSD in people who experienced MVA (PE-MVA) is critical for the return to previous functioning levels.2 Diagnosis of the genuine PTSD after MVA can be difficult because the diagnosis relies heavily on subjective symptoms.3 The medical, financial and legal context can significantly influence the presentation of psychiatric symptoms after MVA.4 The relationship between traumatic event (eg, MVA) and the subsequent psychiatric symptoms made PTSD highly amenable to compensation claims.5 Furthermore, it is widely believed that most PE-MVA who seek psychiatric help are compensation-seeking persons motivated to exhibit more serious difficulties than they actually have.6 Young6 therefore suggests taking into consideration the option of malingering before diagnosing PTSD in situations where secondary gain may exist. In contrast, others noted that the possibility of compensation does not influence significantly presentation of PTSD symptoms in PE-MVA.7 Some PE-MVA may over-report PTSD symptoms due to a variety of reasons, such as (i) a “cry for help” related to severity of physical and psychiatric symptoms, (ii) hoping to obtain financial or social compensation and (iii) attempting to avoid criminal charges for having caused the MVA. In contrast, Green et al8 and Vermetten9 found that PE-MVA may play-down the difficulties they experience and under-report their symptoms in an act of denying their true distress. PTSD, therefore, is often under-diagnosed and subsequently goes untreated. Lange et al10 suggest that in a primary care setting, PE-MVA with PTSD may be under-diagnosed because they do not seek attention for their psychiatric symptoms. Little is known about the discrepancy between over-reporting of PTSD symptoms and under-diagnosing of PTSD patients in the primary care setting.
The phenomenon of different response bias in reporting symptoms may cause clinicians to doubt PTSD in substantial portion of PE-MVA.11,12 In situation when potential disability-related financial compensation aspects of trauma are involved, the authenticity of psychopathological symptoms is unclear since it is inferred by subjective impression of the psychiatrist.13 It is not surprising, that prevalence of PTSD after MVA vary from 0% to 53%, depending on the diagnostic assessment method.14
The prevalence of PTSD is closely related to the assessment method, in which symptoms are evaluated.15 The use of a battery of reliable and valid instruments designed to provide an objective quantification of psychological “injury”, included trauma-specific measures (self-reports and observer’s rating scales) have been recommended as a practice standard in the diagnosis of PTSD.16 The Minnesota Multiphasic Personality Inventory-2 (MMPI-2)17 is the most widely used instrument in PTSD evaluation and helps to ascertain the severity of psychopathology, as well as to identify over- or under-reporting styles of symptom presentation.18
It is possible that over- or under-reporting of PTSD symptoms in MVA may stem from the fact that most studies on this subject were conducted either in outpatients who sought psychiatric treatment,19 or in forensic settings.20 It seems that in primary care, PE-MVA with PTSD tend to express somatic symptoms, rather than “mental” ones, probably because they are unaware of the association between physical symptoms and psychological trauma.21 Namely, these patients complain about experiencing things like accelerated pulse, headaches, various aches and pains, shortness of breath, etc., rather than expressing mental distress. Previously, PTSD has been associated with greater utilization of health-care resources.22
The influence of PTSD symptoms’ presentation on clinical diagnosis among MVA-victims in primary care setting is unclear. Moreover, it is unclear if PTSD diagnosis among patients who did not seek psychiatric help is related to the over-reporting of symptoms.
In the current study, we examined PE-MVA in a primary care clinic who did not seek psychiatric help despite the trauma they were exposed to. The diagnosis of PTSD was established with the Structured Clinical Interview for Axis I DSM-IV Disorders—Patient Version (SCID-I/P). The SCID-I/P was also used to assess the possible relationship between the PTSD and the MVA according to the temporal relationship between the two. The Clinician-Administered Posttraumatic Stress Disorder Scale (CAPS) was used to detect the severity of PTSD symptoms. Subsequently, the association between the patients’ subjective reports and the physician-rated scores of PTSD symptoms was assessed by the MMPI-2 and by the CAPS, respectively. We decided to focus on the relationship between the somatic versus mental patterns of PTSD symptoms as assessed by the MMPI-2 and the clinical interpretation in observer-rating CAPS in primary care setting.
Materials and Methods
Subjects
Participants consisted of adults who had been involved in MVAs between the years 1993–1999 (registration of PE-MVA began in 1993). Their data was retrieved from the medical registry of a general-health community outpatient clinic in the town of Ness-Ziona, Israel that serves a population of over 4000. The data consisted of the individuals’ medical records from the emergency room they visited following the MVA, medical practitioners in various specialties associated with the treatment of PE-MVA, and from information provided by the individuals themselves. This included police department confirmation of the road accident occurrence and records maintained by the hospital to provide insurance agencies with precise information regarding the MVA. Medical information concerning the potential participants was obtained from their medical records.
Individuals were included in the study if they were between the ages of 18 and 65 years and had been involved in an MVA that occurred at least 90 days prior to being interviewed in person. All PE-MVA (drivers, passengers, and pedestrians) with all injury types were included in the study sample. The procedures, clinical characteristics of the participants and comorbidities have been described in a previous publication based on the same data set.23 The current study constitutes a secondary analysis based on previously unanalyzed data from the same data set.
The data set comprised 174 medical records. The psychiatrist (M.K.) and the family physician systematically reviewed all the medical records. Pregnant patients (2 subjects), patients currently serving in the army (3 subjects), or patients who had a prior severe neurological or medical illnesses (12 subjects), schizophrenia (3 subjects), or intellectual disability (2 subjects) were excluded from the study. In addition, 20 patients were excluded from the study because they did not meet the age criteria. After excluding these patients, 132 participants were found to fit the inclusion criteria of the study.
The clinicians contacted all the potential participants by telephone. Thirty individuals were untraceable (due to an address or a phone number change). Out of the 102 people reached by telephone, 60 (61%) agreed to participate in the study. The subjects who agreed to participate were invited to the regional outpatient clinic. Participants who disagreed to attend the clinic for evaluation were visited at home by the psychiatrist. The purpose of the study was fully explained to all potential participants prior to the interview.
Fifteen participants (25%) were excluded because of a technical problem with their MMPI protocols (inability to complete MMPI protocols). The final sample included 45 participants. The group of PE-MVA with PTSD included 7 men (35%) and 13 women (65%). The controls – PE-MVA without PTSD – included 10 men (40%) and 15 (60%) women. In the PTSD group 15 (75%) of the participants were married, one person was single (5%) and 4 (20%) people were divorced. In the control group 18 participants were married (72%), two of them (8%) were single and 5 (20%) people were divorced (see Table 1).
 |
Table 1 Demographic and Clinical Data of People Who Experienced a Motor Vehicle Accident with and without PTSD |
The study was approved by the Ness-Ziona Mental Health Center Review Board and written informed consent was obtained from all participants.
Measurements
Structured Clinical Interview for Axis I DSM-IV Disorders—Patient Version (SCID-I/P)
As described previously,23 in the ambulatory setting, a trained research psychiatrist conducted face-to-face interviews for observer-rating scales in addition to clinical examination. Participants were asked to complete a questionnaire regarding their demographic characteristics (age, gender, education, marital status), employment since the MVA event, prior MVA history, history of psychiatric disorders before the current road accident, past and current physical diseases, and current pharmacological treatment. To assess the current MVA, subjects were questioned regarding the accident details, personal experiences of the traumatic event, self-report measures (MMPI-2), and the impact of the MVA on social, occupational, and other significant areas of functioning. The SCID-I/P24 was used to verify current and lifetime diagnoses (before and after the MVA) of the various DSM-IV Axis I disorders, including PTSD. All subjects with current PTSD met Criterion A for PTSD.
The Clinician-Administered Posttraumatic Stress Disorder Scale for DSM-IV, Part 2 (CAPS-2)
CAPS-2 is a structured interview used for assessing the severity of PTSD.25 It is considered to be the gold standard for the evaluation of the severity of PTSD and is claimed to be better than other psychometric assessments and self-report tests for this end.26 The CAPS-2 includes a 30-item structured interview to determine the frequency and intensity of PTSD symptoms in the preceding month, using a 5-point Likert scale (from 0 – indicates that the symptom does not occur or does not cause distress to 4 – indicates that the symptom occurs nearly every day or causes extreme distress and discomfort), as well as, questions assessing subjective distress and impairment in social and occupational functioning. It is usually takes about 1 hour to complete.26 The original CAPS scoring has a sensitivity of 48% and a specificity of 96% with a cutoff value of 71, based on a general population study excluding an intentional malingering group.27 The CAPS-2 has been shown to be sensitive for detection of PTSD in individuals following an MVA.7 Both SCID-I/P and CAPS were utilized in our study since the SCID-I/P provides a diagnostic evaluation and the CAPS quantifies the level of severity of symptomatology.
The Injury Severity Scale (ISS)
The severity of MVA-related physical injury was assessed by the ISS.28 The ISS was used separately for injuries of the head and neck, face, chest, abdomen and pelvis, and extremities. The different scores were summed up to a total score in a range between 1 and 75.
The Minnesota Multiphasic Personality Inventory (MMPI-2)
For the evaluation of psychological injury29 were used content scales of the MMPI-217 (567 items) in Hebrew and Russian.30 The style of symptom presentation was assessed by the original validity scales included: “no answers”, the Infrequency (F), the Defensiveness (K) and the Lie (L), and the complementary validity indicator the Infrequency Back Side (Fb). The Variable Response Inconsistency (VRIN) and the True Response Inconsistency (TRIN) validity scales were used to detect a random responding.17
Other validity scales that are not currently part of the MMPI-2 scoring were used: (i) the Infrequency Psychopathology (Fp) scale above the cutoff point (8 raw score) is a strong indicator of over-reporting of obvious “mental” symptoms,31 (ii) the Fake Bad32 (FBS) is a measure of an over-reporting of “somatic” and “cognitive” symptoms in personal injury using the erroneous somatic stereotypes,33 (iii) the Infrequent Somatic Responses (Fs) was developed to detect somatic over-reporting using rare somatic symptoms.34 The Response Bias Scale, part of the MMPI-2, is a validity scale empirically derived for the purpose of detecting feigned symptom reporting. In the current study, it was used to detect over/under reporting.
The MMPI-2 was administered individually. The results were analyzed by a senior psychiatrist who did not conduct the clinical interviews who were blind to the CAPS and ISS scores and the SCID data.
Ethical Aspects
Participation was voluntary. All participants gave informed consent indicating their willingness to participate in the study. The study was conducted in accordance with the Declaration of Helsinki and was approved by the local Research Ethics Committees Beer Yakov/Ness Ziona Mental Health Center.
Statistical Analysis
The data was analyzed using the Statistical Package for Social Sciences (SPSS) version 14. In the first step, univariate analysis was conducted to compare the demographic characteristics and MMPI-2 scores of the two MVA groups (with and without PTSD). A univariate analysis of demographics was conducted using Chi-square test for categorical variables (sex, marital status), t-test and Wilcoxon Signed Rank for numerical variables (age, education, past road accidents and number of comorbidities respectively). Fifteen MMPI-2 content scales, seven response bias scales (F, Fb, K, L, Fp, FBS, Fs); two validity scales (VRIN and TRIN), as well as the ISS and the CAPS scores were analyzed using a series of One-Way Analysis of Variance (ANOVA). The scores were used as dependent variables and MVA groups (with versus without PTSD) were used as the independent variable. Because of the large number of statistical tests conducted on the same dataset, the Benjamini-Hochberger correction was applied with FDR control at level of q = 0.1.35 According to Tabachnick and Fidell,36 a sample size of at least 20 in each group is sufficient for such analysis. The group of PE-MVA with PTSD was comprised of 20 patients, and the control group of MVA without PTSD was comprised of 25 participants. ANOVAs were chosen rather than a MANOVA due to the small sample sizes relative to the number of dependent variables.37 To assess the contribution of co-morbidity of PTSD, a comorbidity variable (number of additional disorders) was created. The non-parametric Mann–Whitney test was used to compare the distributions of the comorbidity variable in the two MVA groups.
In the second step, a comparison of groups was carried out using a series of analyses of covariance (ANCOVA). Only content MMPI-2 scales that were found to be significantly different between the two groups in the univariate analysis were chosen as dependent variables for ANCOVA. Any demographic factor and any of the six MMPI-2 response bias scales that were found to be significantly different between the two groups were considered as covariates in ANCOVA. Since the response bias scales were significantly correlated with one another, results of the inter-correlation analysis were used to reduce the multicollinearity effect in ANCOVA. Pearson’s correlation was used to assess the influence of bias scales on the overall rate of symptom presentation in the two groups. Two-tailed levels of significance were used in all tests.
Results
The demographic and clinical data of the PE-MVA with and without PTSD are presented in Table 1. No significant differences were found in age, sex, years of education and number of comorbidities (Table 1). Therefore, these characteristics were not used as covariates in the analyses.
Mean scores and standard deviations of the CAPS-2 and ISS are presented in Table 2. ANOVA analysis of the results of these two scales demonstrated significant differences between the two groups in severity of PTSD symptoms as measured by CAPS-2. The ISS scores, which measure severity of physical injuries, did not demonstrate a significant difference between the two groups. Thus, severity of the physical injury was not used as covariate in the analyses. The mean score of the two validity scales (VRIN and TRIN) indicated that both MVA groups responded consistently to the MMPI-2 items. There was no significant difference in L scale (“social desirability”) scores between the two groups (Table 3).
 |
Table 2 Clinician-Administered Posttraumatic Stress Disorder Scale-2 Scores of People Who Experienced a Motor Vehicle Accident with and without PTSD |
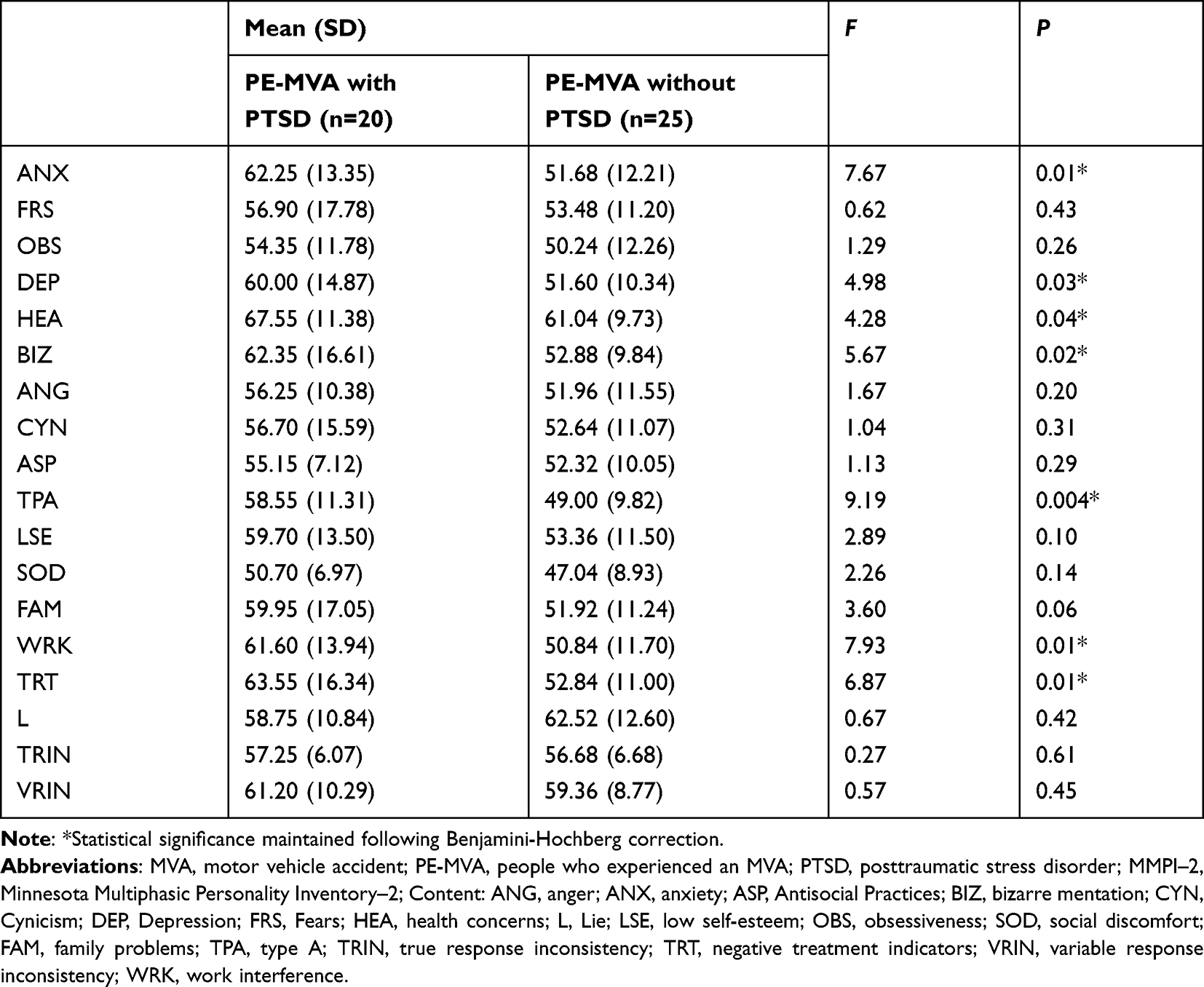 |
Table 3 Minnesota Multiphasic Personality Inventory–2 Content and Validity Scale Scores of People Who Experienced a Motor Vehicle Accident with and without PTSD |
The mean T scores and standard deviations of the MMPI-2 content scales of the two groups are presented in Table 3. The ANOVA demonstrated a significant difference between the groups. MVAs with PTSD felt more anxious, nervous, worried, and apprehensive (elevation of the ANX scale); depressed (DEP scale), and reported poor physical health (HEA scale, which reflects the tendency to develop somatic complaints in response to stress and to seek medical attention, a description consistent with somatization) than MVAs without PTSD. MVAs with PTSD reported more bizarre mentation (BIZ scale). PE-MVA with PTSD presented themselves as hard-working persons, as reflected by significantly higher TPA and WRK scale scores compared to PE-MVA who did not develop PTSD. They also have a higher negative attitude toward mental health treatment (TRT scale) than MVAs without PTSD. All significant differences between the two groups were determined following the Benjamini-Hochberger correction for multiple comparisons.
The means of the raw scores, standard deviations of the MMPI-2 scales measuring style of symptom presentation are presented in Table 4. The results of the ANOVA indicate that PE-MVA with PTSD had significantly higher scores on the F scale and significantly lower scores on the K scale (“exaggerated presentation”) than PE-MVA without PTSD. PE-MVA with and without PTSD did not differ on the Fp and Fb scales, but differed significantly on the F and FBS scales. All significant differences between the two groups were determined following the Benjamini-Hochberger correction for multiple comparisons.
 |
Table 4 Minnesota Multiphasic Personality Inventory–2 Response Bias Scale Scores of People Who Experienced a Motor Vehicle Accident with and without PTSD |
We conducted a series of ANCOVAs with MMPI-2 content scales as dependent variables and MMPI-2 response bias scales as covariates. Univariate analyses demonstrated that only four of six bias scales (F, K, Fs and FBS) were significantly different between the two groups. Possible multicollinearity effects in ANCOVA correlations between these four bias scales were analyzed. Table 5 demonstrates strong correlations between the MMPI-2 bias scales. To avoid the multicollinearity effect of these 4 scales in ANCOVA only two (F and FBS) were chosen as covariates.
 |
Table 5 Inter-Correlations Between Minnesota Multiphasic Personality Inventory–2 Response Bias Scales |
Pearson’s correlation was used to assess the influence of symptom presentation on the overall rate of subjective psychopathology in the two groups (see Table 6). Correlations between F and FBS and the content scales were significantly higher in PE-MVA with PTSD than those without PTSD. The association of F was found to be stronger with BIZ and that of FBS was found to be stronger with HEA. Moreover, differences in correlations between research and control group were significantly higher for the FBS scale than for the F scale (Table 6).
 |
Table 6 Correlations of Response Bias Scale Scores with the Minnesota Multiphasic Personality Inventory–2 Content Scale Scores of People Who Experienced a Motor Vehicle Accident with and without PTSD |
ANCOVA was performed separately on each of the six content scales with scales F and FBS as covariates. After adjustment for the F and FBS scores, no significant differences were found between the groups regarding the MMPI-2 content scales. The content scales used in this analysis were Anxious (ANX) [F(1,43)=1.62, P=0.21], Depression (DEP) [F(1,43)=0.15, P=0.70], Bizarre mentation (BIZ) [F(1,43)=1.65, P=0.21], Physical Health (HEA) [F(1,43)=0.02, P=0.90], Type A (TPA) [F(1,43)=3.39, P=0.07], Work Interference (WRK) [F(1,43)=1.28, P=0.27], Negative Treatment Indicators (TRT) [F(1,43)=0.59, P = 0.45].
Significant differences were found between the groups in total CAPS-2 scores, even after adjustment for covariates F and FBS [F(1,43)=11.5, P = 0.002].
Discussion
The current study attempted to characterize the way of PTSD symptoms are presented by PE-MVA, who turned to a primary care setting, and do not seek psychiatric help. PE-MVA with PTSD scored high on the CAPS, compared to MVA without PTSD; however, the scores were lower than those reported previously.38 The ISS score did not discriminate between two groups. These results are consistent with previous findings,39 which suggested that objective measures of injury severity correlate poorly with PE-MVA’s psychological sequelae. Hodgson and Webster40 found that accident severity had no direct effect on post-MVA emotional distress. It was found that the PE-MVA with PTSD reported significantly more psychopathology (anxiety, depression, bizarre mentation) and especially significantly more worries concerning their physical health than the PE-MVA without PTSD, as measured by the MMPI-2 content scales and that despite the former not seeking psychiatric help. Moreover, the scores of the MMPI-2 were lower than expected.
It was previously found that the significant elevation of Infrequency (F) score of MMPI–2 often leads to mistrust of the elevation of clinical scales, to doubt to patients’ reports of PTSD symptoms and the validity of the PTSD diagnosis in general.41 However, the extreme elevations on the F scale may be related not only to over-reporting or malingering of symptoms but also to subjectively feeling distress and a “cry for help” response style. An elevated F scale is associated with an elevated MMPI-2 psychopathological profile but does not separate exaggerated symptom presentation from genuine stress-related responses.42 Although most MMPI-2 scales were in the normal range, findings show significant differences between MMPI-2 scales in PE-MVA with PTSD and in PE-MVA without PTSD in the following items: DEP (Depression), HEA (Health Concerns), BIZ (Bizarre Mentation), TPA (Type A), WRK (Work Interference) and TRT (Negative Treatment Indicators). In addition, PE-MVA with PTSD, who turned to a primary care setting express elevation of the HEA (Health Concerns) scale score over the 65 cutoff. We found that the MMPI-2 did not differ between PE-MVA with and without PTSD after adjusting for F and FBS as covariates.
The current results demonstrate that the FBS is more sensitive to atypical somatic posttraumatic symptoms than F, F(p), and Fs scales in PE-MVA in a primary care setting. In contrast, significant differences between PE-MVA with and without PTSD in CAPS-2 scores existed even after adjusting for bias MMPI F and FBS scales as covariates.
As expected, no difference was found on the MMPI-2 between MVA with and without PTSD after adjusting for F as covariate. In this line, Arbisi and Ben-Porath31 introduced the Fp scale that was developed to differentiate feigned from a genuine psychopathology. Individuals who suffer from generalized stress reactions were found to have high F scores but not elevated Fp scores. In contrast, subjects who feigned “mental” psychopathology exhibited elevation in both F and Fp scales. In the current study, PE-MVA with PTSD differed significantly from PE-MVA without PTSD on the F scale but not on the Fp scale. These results are consistent with previous studies that demonstrated that genuine PTSD is often associated with over-reporting of symptoms and there is no malicious attempt to deceive.43 The current study found significant differences between groups on bias scales (F, K, FBS, Fs), but not on the validity scales, that directly assess the consistency of responses (VRIN and TRIN). The present findings provide additional evidence to support the hypothesis that most PE-MVA with PTSD, who do not seek psychiatric help, with elevated MMPI–2 F scale scores are not consciously over-reporting their distress. Such consistency of responses (VRIN and TRIN) argues against malingering. Lilienfeld et al44 suggested that in the assessment context, over-reporting can be placed on a continuum of dimensionality, from unconscious-based somatic complaints to outright conscious malingering. Recently, researchers found the relationship between PTSD symptom severity and over-reporting of symptoms.45
PE-MVA with PTSD differed significantly from those without PTSD on the Fs and FBS scales. Thus, MVA with PTSD, who did not seek psychiatric help, over-reported PTSD symptoms using erroneous somatic stereotypes (as measured by the elevation of the FBS MMPI-2 score) and rare somatic symptoms (as measured by the elevation of the Fs MMPI-2 score). In the MVA group with PTSD there was no participant with FBS scores beyond the cutoff point of 24 for “somatic malingering”.46
This study has several limitations. Some PE-MVA with PTSD were diagnosed with several Axis I diagnoses prior to the MVA. Inclusion of people with both psychiatric and physical comorbidities in the current study limits the generalizability of the findings. However, the rate of comorbidity did not differ between the PE-MVA with or without PTSD and was not therefore included in the analysis as a covariate. Nevertheless, the impact of comorbidity on self-assessment, especially chronic pain46 warrants additional research. Moreover, although all the participants in the study experienced MVA before coming to the primary care setting, PTSD diagnosis and symptoms could not be specified as MVA-related. It is most likely that the PTSD diagnosis, as assessed by the SCID-I/P and the symptoms severity as assessed by CAPS-2, were mostly related to the MVA.
An additional and important limitation is the small sample size which reduces the statistical power and generalization of the findings.
Another limitation is the fact that 67% of PE-MVA did not complete the MMPI-2. It seems that without some motivation or compensation, most MVA participants in primary care, who do not seek psychiatric help, refuse completion of the MMPI-2 assessment. Still, the rate was better than expected according to previous reports on the low rate of completion of personality questionnaires.47 To the authors’ knowledge, no similar comparable data have been described in the medical literature.
Conclusions
The present study uses MMPI-2, ISS, and CAPS instruments to determine whether the relationship between subjective mental state and clinician’s evaluation of PTSD symptoms after MVA is related to an over-reporting strategy among PE-MVA who did not seek psychiatric help. The results of our study suggest that PE-MVA with PTSD who sought help in a primary health-care setting but did not seek psychiatric help tend to exaggerate PTSD symptoms presenting unsuitable, rare and stereotypical somatic symptoms. The F scale of MMPI-2 showed less sensitivity to exaggerated somatic symptoms than the FBS scale in a primary care setting. The present findings demonstrate the direct effect of F and FBS scales on the significant elevation of the MMPI-2 profile but not on the scoring of the CAPS-2 among the PE-MVA with PTSD. Further studies replicating the current results across various medical settings and with different samples of PE-MVA are warranted.
Abbreviations
CAPS-2, Clinician-Administered Posttraumatic Stress Disorder Scale-2; ISS, Injury Severity Scale; MMPI-2, Minnesota Multiphasic Personality Inventory-2; MVA, motor vehicle accident; PTSD, posttraumatic stress disorder; SCID-I/P, Structured Clinical Interview for Axis I DSM-IV Disorders—Patient Version; PE-MVA, persons who experienced a motor vehicle accident.
Acknowledgment
The authors thank Helena Lidogoster, Marina Vainder, and Moshe Almagor for their contribution to this work. They also thank all the clinicians who referred patients to the current study or who were involved in the management of the patients.
Author Contributions
All authors made a significant contribution to the work reported, whether it be the conception, study design, execution, acquisition of data, analysis and interpretation, or all these areas. All authors took part in drafting, revising or critically reviewing the article, gave final approval of the version to be published, have agreed to the journal to which the article was submitted and accept accountability for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Heron-Delaney M, Kenardy J, Charlton E, Matsuoka Y. A systematic review of predictors of posttraumatic stress disorder (PTSD) for adult road traffic crash survivors. Injury. 2013;44(11):1413–1422. doi:10.1016/j.injury.2013.07.011
2. Popiel A, Zawadzki B, Pragłowska E, Teichman Y. Prolonged exposure, paroxetine and the combination in the treatment of PTSD following a motor vehicle accident. A randomized clinical trial the “TRAKT” study. J Behav Ther Exp Psychiatry. 2015;48:17–26. doi:10.1016/j.jbtep.2015.01.002
3. Hall RC, Hall RC. Detection of malingered PTSD: an overview of clinical, psychometric, and physiological assessment: where do we stand?. J Forensic Sci. 2007;52(3):717–725. doi:10.1111/j.1556-4029.2007.00434.x
4. Sellbom M, Lee TT, Ben-Porath YS, Arbisi PA, Gervais RO. Differentiating PTSD symptomatology with the MMPI-2-RF (Restructured Form) in a forensic disability sample. Psychiatry Res. 2012;197(1–2):172–179. doi:10.1016/j.psychres.2012.02.003
5. Beck JG, Coffey SF. Assessment and treatment of PTSD after a motor vehicle collision: empirical findings and clinical observations. Prof Psychol Res Pr. 2007;38(6):629–639. doi:10.1037/0735-7028.38.6.629
6. Young G. PTSD in court I: introducing PTSD for court. Int J Law Psychiatry. 2016;49(Pt B):238–258. doi:10.1016/j.ijlp.2016.10.012
7. Blanchard EB, Hickling EJ. After the Crash: Assessment and Treatment of Motor Vehicle Accident Survivors.
8. Green MM, McFarlane AC, Hunter CE, Griggs WM. Undiagnosed posttraumatic stress disorder following motor vehicle accidents. Med J Aust. 1993;159(8):529–534. doi:10.5694/j.1326-5377.1993.tb138006.x
9. Vermetten E, Baker DG, Jetly R, McFarlane AC. Concerns over divergent approaches in the diagnostics of posttraumatic stress disorder. Psychiatr Ann. 2016;46(9):498–509. doi:10.3928/00485713-20160728-02
10. Lange JT, Lange CL, Cabaltica RB. Primary care treatment of post-traumatic stress disorder. Am Fam Physician. 2000;62(5):1035–1040.
11. Kazantzis N, Kennedy-Moffat J, Flett RA, Petrik AM, Long NR, Castell B. Predictors of chronic trauma-related symptoms in a community sample of New Zealand motor vehicle accident survivors. Cult Med Psychiatry. 2012;36(3):442–464. doi:10.1007/s11013-012-9265-z
12. Nicholson К, Martelli MF. The problem of pain. J Head Trauma Rehabil. 2004;19(1):2–9. doi:10.1097/00001199-200401000-00002
13. Lane R. Expanding boundaries in psychiatry: uncertainty in the context of diagnosis‐seeking and negotiation. Sociol Health Illn. 2020;42(S1):69–83. doi:10.1111/1467-9566.13044
14. Greene T, Neria Y, Gross R. Prevalence, detection and correlates of PTSD in the primary care setting: a systematic review. J Clin Psychol Med Settings. 2016;23(2):160–180. doi:10.1007/s10880-016-9449-8
15. Kleinman SB, Martell D. Failings of trauma-specific and related psychological test in detecting posttraumatic stress disorder in forensic settings. Psychiatry Behav Sci. 2015;60(1):76–83.
16. Butcher JN, Miller KB. Personality assessment in personal injury litigation. In: Hess AK, Weiner IB, editors. The Handbook of Forensic Psychology.
17. Butcher JN, Graham JR, Ben-Porath YS, Tellegen A, Dahlstrom WG, Kaemmer B. MMPI-2: Manual for Administration, Scoring, and Interpretation.
18. Arbisi PA, Ben-Porath YS, McNulty JL. The ability of the MMPI-2 to detect feigned PTSD within the context of compensation seeking. Psychol Serv. 2006;3(4):249–261. doi:10.1037/1541-1559.3.4.249
19. Koirala R, Søegaard EGI, Ojha SP, Hauff E, Thapa SB. Trauma related psychiatric disorders and their correlates in a clinical sample: a cross-sectional study in trauma affected patients visiting a psychiatric clinic in Nepal. PLoS One. 2020;15(6):e0234203. doi:10.1371/journal.pone.0234203
20. Arce R, Fariña F, Buela G. Assessing and detecting the ability to faking psychological injury as a consequence of a motor vehicle accident on the MMPI-2 using mock victims. Rev Latinoam Psicol. 2008;40(3):485–496.
21. Nakell L. Adult post-traumatic stress disorder: screening and treating in primary care. Prim Care. 2007;34(3):593–610. doi:10.1016/j.pop.2007.05.010
22. Thompson EJ, Anderson VA, Hearps SJ, et al. Posttraumatic stress symptom severity and health service utilization in trauma-exposed parents. Health Psychol. 2017;36(8):779–786. doi:10.1037/hea0000476
23. Kupchik M, Strous RD, Erez R, Gonen N, Weizman A, Spivak B. Demographic and clinical characteristics of motor vehicle accident victims in the community general health outpatient clinic: a comparison of PTSD and non-PTSD subjects. Depress Anxiety. 2007;24(4):244–250. doi:10.1002/da.20189
24. First MB, Spitzer RL, Gibbon M, Williams JBW. Structured Clinical Interview for Axis I DSM-IV Disorders, Patient Version (SCID-I/P), Version 2. New York: New York State Psychiatric Institute, Biometrics Research; 1996.
25. Blake DD, Weathers FW, Nagy LM, Kaloupek DG, Charney DS, Keane TM. Clinician-Administered Post Traumatic Stress Disorder Scale for DSM-IV (CAPS-2). Boston: National Center for Posttraumatic Stress Disorder, Behavioral Science Division; 1990.
26. Weathers F, Keane T, Davidson J. Clinician-administered PTSD scale: a review of the first ten years of research. Depress Anxiety. 2001;13(3):132–156. doi:10.1002/da.1029
27. Weathers FW, Ruscio AM, Keane TM. Psychometric properties of nine scoring rules for the clinician-administered posttraumatic stress disorder scale. Psychol Assess. 1999;11(2):124–133. doi:10.1037/1040-3590.11.2.124
28. Baker SP, O’Neill B, Haddon W, Long WB. The injury severity score: a method for describing patients with multiple injuries and evaluating emergency care. J Trauma. 1974;14(3):187–196. doi:10.1097/00005373-197403000-00001
29. Duckworth MP, Iezzi T. Motor vehicle collisions and their consequences—part II: predictors of impairment and disability. Psychol Inj Law. 2018;11(3):288–306. doi:10.1007/s12207-018-9334-x
30. Almagor M, Bodesko D, Montag I, Navo B. Hebrew and Russian Version of MMPI-2. University of Haifa; 1991.
31. Arbisi PA, Ben-Porath YS. An MMPI-2 infrequent response scale for use with psychopathological populations: the infrequency-psychopathology scale, F(p). Psychol Assess. 1995;7(4):424–431. doi:10.1037/1040-3590.7.4.424
32. Lees-Haley PR, English LT, Glenn WJ. A fake bad scale on the MMPI-2 for personal injury claimants. Psychol Rep. 1991;68(1):203–210. doi:10.2466/pr0.1991.68.1.203
33. Greiffenstein MF, Fox DD, Lees-Haley PR. The MMPI-2 fake bad scale in detection of noncredible brain injury claims. In: Boone K, editor. Assessment of Feigned Cognitive Impairment: A Neuropsychological Perspective. New York: The Guilford Press; 2007:210–238.
34. Wygant DB, Ben-Porath YS, Arbisi PA. Development and initial validation of a scale to detect infrequent somatic complaints.
35. Benjamini Y, Yekutieli D. Quantitative trait loci analysis using the false discovery rate. Genetics. 2005;171(2):783–790. doi:10.1534/genetics.104.036699
36. Tabachnick BG, Fidell LS. Using Multivariate Statistics.
37. Lucenko BA, Gold SN, Elhai JD, Russo SA, Swingle JM. Relations between coercive strategies and MMPI-2 scale elevations among women survivors of childhood sexual abuse. J Trauma Stress. 2000;13(1):169–177. doi:10.1023/A:1007785201112
38. Blanchard EB, Hickling EJ, Barton KA, et al. One-year prospective follow-up of motor vehicle accident victims. Behav Res Ther. 1996;34(10):775–786. doi:10.1016/0005-7967(96)00038-1
39. Fujita G, Nishida Y. Association of objective measures of trauma exposure from motor vehicle accidents and posttraumatic stress symptoms. J Trauma Stress. 2008;21(4):425–429. doi:10.1002/jts.20353
40. Hodgson RC, Webster RA. Mediating role of peritraumatic dissociation and depression on post-MVA distress: path analysis. Depress Anxiety. 2011;28(3):218–226. doi:10.1002/da.20774
41. Tsushima WT, Geling O, Fabrigas J. Comparison of MMPI-2 validity scale scores of personal injury litigants and disability claimants. Clin Neuropsychol. 2011;25(8):1403–1414. doi:10.1080/13854046.2011.613854
42. Butcher JN. Historical highlights on use of the MMPI/MMPI-2 in PTSD evaluations; 2013. Available from: http://www.umn.edu/mmpi.
43. Merckelbach H, Dandachi-FitzGerald B, van Helvoor D, Jelicic M, Otgaar H. When patients overreport symptoms: more than just malingering. Curr Dir Psychol Sci. 2019;28(3):321–326. doi:10.1177/0963721419837681
44. Lilienfeld SO, Thames AD, Watts AL. Symptom validity testing: unresolved questions, future directions. J Exp Psychopathol. 2013;4(1):78–87. doi:10.5127/jep.028312
45. Brady RE, Bujarski SJ, Feldner MT, Pyne JM. Examining the effects of alexithymia on the relation between posttraumatic stress disorder and over-reporting. Psychol Trauma. 2017;9(1):80–87. doi:10.1037/tra0000155
46. Beck JG, Clapp JD. A different kind of comorbidity: understanding posttraumatic stress disorder and chronic pain. Psychol Trauma. 2011;3(2):101–108. doi:10.1037/a0021263
47. Kongsved SM, Basnov M, Holm-Christensen K, Hjollund NH. Response rate and completeness of questionnaires: a randomized study of Internet versus paper-and-pencil versions. J Med Internet Res. 2007;9(3):e25. doi:10.2196/jmir.9.3.e25
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.