Back to Journals » International Journal of Women's Health » Volume 18
Ovarian Reserve Following Triple-Step Procedure on Bilateral Large Endometrioma: A Retrospective Study from Bali, Indonesia
Authors Adnyana IBPP, Anwar R ![]() , Adnyana IBP, Hartanto AI
, Adnyana IBP, Hartanto AI ![]() , Syahruddin SS
, Syahruddin SS
Received 4 March 2026
Accepted for publication 18 June 2026
Published 23 June 2026 Volume 2026:18 604447
DOI https://doi.org/10.2147/IJWH.S604447
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Ida Bagus Praja Putra Adnyana,1 Ruswana Anwar,1 Ida Bagus Putra Adnyana,2 Amadea Ivana Hartanto,3 Siti Shofiah Syahruddin4
1Reproductive Endocrinology and Infertility Division, Obstetrics and Gynecology Department, Dr. Hasan Sadikin General Hospital, Bandung, Indonesia; 2Reproductive Endocrinology and Infertility Division, Obstetrics and Gynecology Department, Bali Royal Hospital, Bali, Indonesia; 3Department of Obstetrics and Gynecology, Faculty of Medicine, Padjadjaran University, Dr. Hasan Sadikin General Hospital, Bandung, Indonesia; 4Faculty of Medicine, Padjadjaran University, Bandung, Indonesia
Correspondence: Amadea Ivana Hartanto, Department of Obstetrics and Gynecology, Faculty of Medicine, Padjadjaran University, Dr. Hasan Sadikin General Hospital, Jl. Pasteur No. 38, Bandung, West Java, 40161, Indonesia, Tel +62 821-2094-2011, Email [email protected]
Introduction: The triple-step method, which comprises transvaginal ultrasound-guided aspiration (TUGA) of cyst fluid, three cycles of a gonadotropin-releasing hormone (GnRH) agonist, and laparoscopic cystectomy, has been proposed for managing large endometriomas. The impact of this procedure on ovarian reserve can be measured using antral follicle count (AFC) and serum anti-Mullerian hormone (AMH) levels. We aimed to comprehensively evaluate the triple-step procedure for endometrioma and its effect on ovarian reserve in patients with large endometriomas at Bali Royal Hospital (BROS), Denpasar.
Methods: This study used a retrospective design and secondary data. The study population included all patients diagnosed with bilateral large endometriomas on transvaginal ultrasonography during a 3-year study period. A large endometrioma is an endometrial cyst measuring > 4 cm in diameter. AMH and AFC are measured before aspiration and three months after cystectomy. The collected data were processed using SPSS v.23.
Results: Most patients were aged < 35 years (n = 14; 73.7%). Based on infertility status, almost all patients had primary infertility (17 patients; 89.5%) with a duration of < 5 years (11 patients; 57.9%). Regarding preoperative AFC parameters, the minimum and maximum AFC values were 3.00 and 9.00, respectively, with a mean of 5.57 (1.952). After surgery, the minimum and maximum AFC values were 5.00 and 14.00, respectively, with a mean of 8.47 (2.412). The mean AMH levels before surgery were 2.95 ng/mL (2.027) and 2.83 ng/mL (1.611) after surgery, respectively. A significant difference was found in the AFC values between pre-surgery and post-surgery groups (p< 0.001). However, no significant difference in AMH values was found between the groups.
Conclusion: The triple-step procedure may conserve ovarian reserve in large bilateral endometriomas.
Keywords: AFC, AMH, large endometrioma, triple-step procedures
Introduction
Endometrioma is a type of endometriosis specified by the presence of ectopic endometrial stroma and glands within the ovary. The size of endometriomas can range from 1 to 20 cm. Cysts larger than 4 cm are considered a large endometrioma. This disease is dependent on estrogen and is referred to as “chocolate cyst” because they contained dark reddish-brown blood.1
About 17–44% of women diagnosed with endometriosis manifested as endometriomas. Endometriosis itself is estimated to affect around 10% women of reproductive age worldwide.2 One study found endometriotic lesions in 260 of 1191 women presenting with subfertility, corresponding to a prevalence of 21.8%. Epidemiological investigations have further estimated the annual incidence of endometriosis among reproductive-aged women to be approximately 0.14%.3,4
Large endometriomas are generally managed with traditional single-stage laparoscopic cystectomy.5,6 Nonetheless, increasing evidence suggests that cystectomy may adversely affect ovarian reserve because of the unavoidable elimination of healthy ovarian tissue.6 A prospective research conducted by Anh et al reported a significant depletion in anti-Mullerian hormone (AMH) levels after laparoscopic cystectomy for endometrioma, with a 54.8% decrease observed at 6 months postoperatively.7 Similarly, Rius et al reported an approximately 35% reduction in antral follicle count (AFC) at 6 months compared to preoperative levels.8 To mitigate the risk of diminished ovarian reserve, Tsolakidis et al proposed the triple-step approach.9
For the past 3 years, Bali Royal Hospital has consistently used a modified triple-step approach for the management of large endometriomas. This protocol consists of ultrasound-guided cyst aspiration, administration of three cycles of gonadotropin-releasing hormone (GnRH) agonist using leuprolide acetate 3.75 mg, and subsequent laparoscopic cystectomy. Following completion of medical therapy, patients undergo cyst reassessment two weeks after the final GnRH agonist injection. Surgical cystectomy is then performed when the cyst diameter has decreased to less than 3 cm, with the intention of minimizing damage to healthy ovarian tissue.10
Ultrasound-guided aspiration is a minimally invasive procedure that allows drainage of endometriotic cyst contents. GnRH agonist suppresses pituitary gonadotropin secretion (follicle-stimulating hormone and luteinizing hormone), resulting in reduced ovarian estrogen production and the induction of a temporary hypoestrogenic state. This hormonal suppression contributes to cyst shrinkage and facilitates less invasive surgical excision.11 The final step, laparoscopic cystectomy, aims to remove residual endometriotic cyst while preserving healthy ovarian tissue, thereby relieving symptoms, reducing recurrence risk, and improving reproductive outcomes.12
Ovarian reserve reflects both the quantity and quality of patients’ oocyte function and is a determinant of reproductive potential. Endometriomas may compromise ovarian reserve through several mechanisms: compression of the ovarian cortex, disruption of local blood supply, and creation of an inflammatory microenvironment that promotes follicular damage. Evaluation of ovarian reserve is commonly performed using serum AMH levels and AFC. Interpretation of AMH levels and AFC should take the patient’s age into account.13,14 Evaluation of AFC is typically performed before treatment and during postoperative follow-up, as recovery of ovarian function is generally expected within 3–6 months after surgery.15
With these considerations, this study aimed to describe the implementation of the triple-step approach for large endometriomas and to evaluate its effect on ovarian reserve among patients treated at the Bali Royal Hospital, Denpasar.
Materials and Methods
Study Design
This study used a retrospective approach, with secondary data collection, namely medical records of patients treated at Bali Royal Hospital, Denpasar, who then underwent follow-up to assess the ovarian reserve after the triple-step procedure for endometrioma.
Population and Sample
The study population included all patients diagnosed with bilateral large endometriomas on transvaginal ultrasonography during the study period. The total sampling technique was used in this study. Total sampling was defined as the inclusion of all consecutive eligible patients meeting study criteria during the study period. The inclusion criteria were complete medical record data. The exclusion criteria were prior to medical or surgical treatment for endometrioma, previous ovarian surgery, incomplete GnRH treatment, incomplete records, and inability to aspirate cyst contents (eg, thick, viscous fluid), cysts >3 cm remaining after GnRH agonist therapy (cystectomy not performed). Thus, 19 patients were included in this study.
Data and Variable
The variables in this study were age, infertility status (type and duration), the mean diameter of the largest cyst, calculated from two-dimensional ultrasonography, type of GnRH agonist used, disease recurrence, and in vitro fertilization (IVF) procedure status. Recurrence of large endometriomas refers to the reappearance or worsening of symptoms and lesions associated with large endometriomas after a period of relief or improvement following treatment.34 Ovarian reserve parameters were measured using AFC and AMH before and three months after cystectomy.
A triple step is defined as three treatment procedures, including ultrasound-guided cyst fluid aspiration (TUGA) using a 17-gauge needle, followed by three cycles of GnRH agonist treatment and cystectomy. TUGA was performed on the fifth day until both cysts collapsed. Therapy was continued with leuprolide acetate 3.75 mg as the GnRH agonist for 3 cycles. Two weeks after the last GnRH agonist therapy, endometriosis cysts were re-evaluated. A cystectomy was performed if the cyst size was <30 mm, performed by a single experienced reproductive endocrinology surgeon using a stripping technique. Hemostasis was achieved using low-power bipolar coagulation, avoiding suturing of the ovarian hilum. AFC and AMH examinations were performed before aspiration and three months after cystectomy.
Statistical Analysis
Statistical Package for the Social Sciences (SPSS) and Microsoft Excel were used to process the collected data, and then verified. The Shapiro–Wilk test was used to assess the normality of the continuous variables. Normally distributed data (AFC, AMH) were presented as mean ± standard deviation (SD). To compare pre- and post-procedure mean AFC and AMH values, a paired t-test was utilized. p-value was considered statistically significant if it was less than 0.05.
Results
Baseline Characteristics
The mean age of the study samples was 31.316 ± 5.302 years old. Most patients were aged <35 years (n = 14; 73.7%). The mean length of infertility in the study sample was 4.895 ± 3.619 years. Almost all patients had primary infertility (17 patients; 89.5%) with a duration of <5 years (11 patients; 57.9%). The mean cyst diameter was 4.895 ± 1.333 cm. Most patients had cysts >4 cm in diameter (15 patients; 78.9%). The most widely used GnRH agonist therapy was tapros (leuprorelin acetate) in 16 patients (84.2%); only three patients (15.7%) experienced recurrence after the procedure. Only 5 patients (26.4%) underwent IVF. All characteristic data are presented in Table 1.
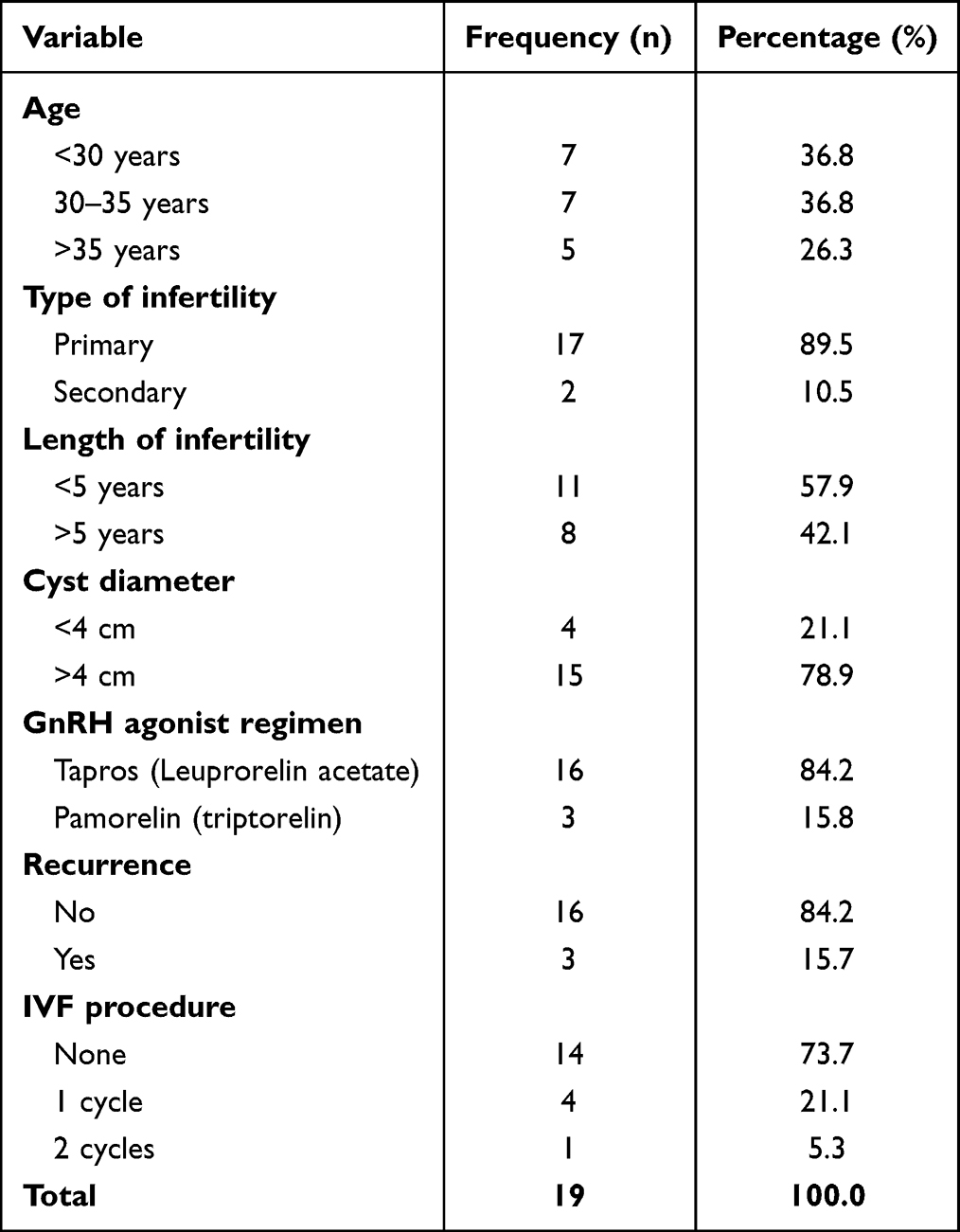 |
Table 1 Baseline Characteristics |
Characteristics of Ovarian Reserve
The mean of pre-laparoscopic cystectomy AFC in the study samples was 3.00 ± 1.00 for the right ovary, 2.57 ± 1.121 for the left ovary, and 5.57 ± 1.952 in both ovaries. In contrast, the mean post-laparoscopic cystectomy AFC in the study samples was 4.52 ± 1.88 for the right ovary, 3.94 ± 1.508 for the left ovary, and 8.47 ± 2.412 for both ovaries. The minimum and maximum AFC values are 3.00 and 14.00, respectively. The mean AMH levels before surgery were 2.95 ng/mL ± 2.027 and 2.83 ng/mL ± 1.611 after surgery, respectively. Ovarian reserve parameters are shown in Table 2.
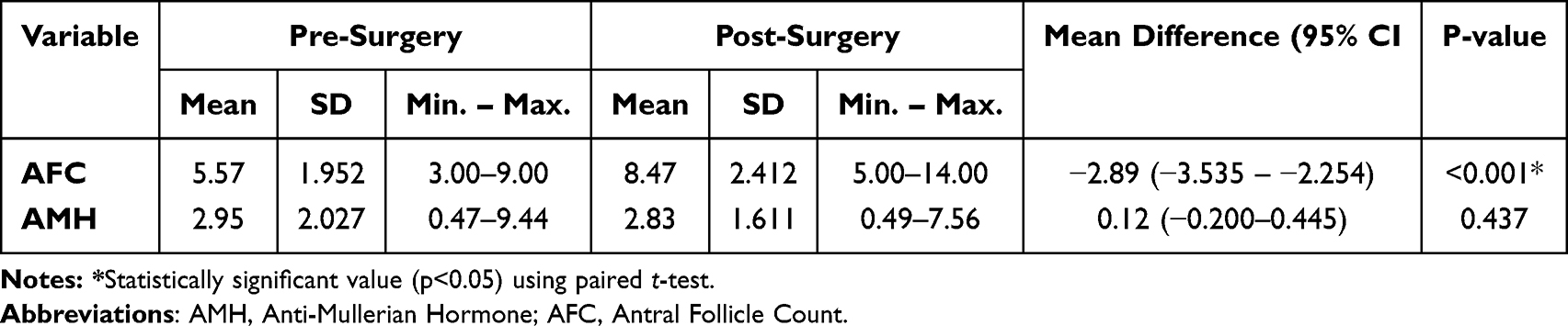 |
Table 2 Characteristics and Differences of Ovarian Reserve Parameters Before and After Surgery |
Differences in Ovarian Reserve Parameters Before and After Surgery
Bivariate analysis was performed to determine the differences in ovarian reserve parameters before and after procedures. The difference in mean AFC was −2.89 (−3.535 – −2.254). We found a significant difference in AFC values between the groups (p<0.001). The difference in mean AMH value was 0.12 ng/mL (−0.200–0.445). However, no significant difference in AMH levels was found between the two groups. Table 2 presents the results of these analyses.
Discussion
Various surgical modalities are offered to manage bilateral endometriomas, including single-stage laparoscopy cystectomy, plasma-energy ablation, laser ablation, electrocoagulation, and combined techniques.16 The European Society of Human Reproduction and Embryology (ESHRE) guidelines recommend ovarian cystectomy as the preferred surgical intervention for endometriomas, especially for cysts exceeding 3 cm in diameter, as it is related to reduced recurrence of cyst and endometriosis-associated pain, but it may adversely affect the ovarian reserve.5 AMH and AFC may be deemed as the best markers of ovarian reserve and are generally utilized to evaluate the damage of surgery in endometriomas.16
Our study found a significant increase in AFC parameters after the triple-steps procedure in patients with endometriomas (P<0.001), and no significant difference in AMH levels before and after surgery, suggesting a favorable effect on ovarian reserve. These findings are aligned with the first prospective RCT comparing the ovarian reserve of patients with endometriomas who underwent laparoscopic cystectomy vs triple-step procedures conducted by Tsolakidis et al9 They found a significant increase in AFC of the operated ovary (P=0.002) in triple-step procedure group (from 1.27–4.36) compared to traditional laparoscopic cystectomy (from 2–2.38). Furthermore, the mean AMH serum level was significantly reduced (P=0.26) in the cystectomy group (from 3.9–2.9 ng/mL) compared to triple-step procedure group (from 4.5–3.9 ng/mL). Another prospective RCT conducted by Salem et al also supports our findings.17 Moreover, mean serum AMH levels decreased significantly in patients with large endometriomas who received combined excisional and ablative surgery (from 3.8 to 2.9 ng/mL), whereas a non-significant reduction was observed in the triple-step procedure group (from 4.1 to 3.7 ng/mL). Kitajima et al also reported a promising benefit for ovarian reserve, as measured by AMH levels, with triple-step laparoscopy surgery compared to one-step surgery, although dienogest (synthetic progestin) was used instead of GnRH agnoist.18
Assessment of serum AMH levels prior to cystectomy provides important information regarding ovarian reserve.8 AMH is secreted by the granulosa cells of small ovarian follicles and can be measured through a blood test at any stage of the menstrual cycle, as its concentrations remain relatively stable throughout the cycle. Following cystectomy, serial evaluation of serum AMH levels may help monitor changes in ovarian reserve and function over time. Although our findings demonstrated an immediate postoperative decline in AMH levels, preservation of sufficient ovarian reserve may allow reconstruction of the follicular cohort, potentially leading to recovery of AMH levels during subsequent follow-up.18
AFC is typically measured using transvaginal ultrasound during the early follicular phase of the menstrual cycle (usually between days 2 and 5) and reflects the number of growing follicles present in the ovaries. AFC may be a helpful marker for ovarian reserve evaluation after cystectomy, as it reflects the remaining ovarian follicular pool and can provide information about the potential for future fertility or hormonal function.10 The significant increase in mean AFC after triple-step procedures in our study could be explained by the minimally invasive technique that avoids the removal of normal ovarian tissue.9 This underlying reason could also be explained by the result of a prospective RCT conducted by Rius et al, as they reported a significantly higher AFC in the later-treated group (from 667 to 9.33) versus the excisional technique (from 6.75 to 4.38), a procedure that may inadvertently remove healthy ovarian tissue, at the 6-month follow-up.8
Our study used leuprorelin acetate as the GnRH agonist for the second step procedure. A comparative study of preferences for GnRH agonist agents has not yet been conducted. GnRH agonists are generally used for the treatment of large endometriomas. These agents stimulate the secretion of gonadotropins, namely follicle-stimulating hormones (FSH) and luteinizing hormones (LH), from the pituitary gland, resulting in a transient increase in estrogen production.19 However, prolonged administration leads to desensitization of the pituitary gland, causing downregulation and suppression of gonadotropin release.11,20 GnRH agonists are particularly useful when first-line therapies, such as nonsteroidal anti-inflammatory drugs (NSAIDs) or hormonal contraceptives, fail to adequately control symptoms, or when surgical management is not preferred or feasible. Their mechanism of action involves binding to and activating GnRH receptors in the pituitary gland.11 GnRH agonists have been demonstrated to effectively reduce pelvic pain, dysmenorrhea, and other symptoms associated with large endometrioma in many patients. GnRH agonists can induce menopause and amenorrhea, providing temporary relief from endometrioma-associated symptoms. However, symptoms may recur following discontinuation of GnRH agonist therapy, particularly in the absence of additional treatments such as hormonal contraceptives or surgical intervention. Although GnRH agonists can provide symptomatic relief in women with large endometrioma-associated infertility, they are not fertility-enhancing agents. Fertility may be temporarily impaired during GnRH agonist therapy due to the hypoestrogenic state induced by these medications. However, fertility typically returns after treatment.21 Leuprorelin acetate, marketed under various brand names such as Lupron, Eligard, and Lucrin, is a synthetic analog of GnRH and is widely used as a GnRH agonist in the management of large endometriomas.12,19
This study has several limitations. First, due to patient limitations, we had only a small sample size. Second, our study was conducted retrospectively and non-randomized. Third, our findings are restricted to short-term biomarker changes. Therefore, our results should be interpreted with caution. Overall, triple-step procedures have become a promising option for patients at risk of diminished ovarian reserve, particularly those with bilateral large endometriomas, as their minimally invasive procedure may help optimize fertility outcomes.20,22 Close collaboration between gynecologists, reproductive endocrinologists, and infertility specialists is essential for individualizing treatment plans and addressing both the underlying large endometrioma and associated infertility factors.23
Conclusion
Based on the research results, it can be concluded that the triple-step procedure was associated with a significant increase in AFC and no significant change in AMH, suggesting potential conservation of ovarian reserve, in bilateral large endometriomas. These preliminary results warrant further investigation with larger sample sizes, longer follow-up periods, and assessment of reproductive outcomes to confirm their long-term efficacy and safety.
Data Sharing Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethical Issues
This research has been reviewed and approved by the Ethics Committee of Bali Royal Hospital (BROS) with reference number 288/BROS/DIR.RS/VI/2024. All procedures are conducted in accordance with the Declaration of Helsinki. Owing to the study’s retrospective and the use of de-identified data, the ethics committee waived the requirement for individual informed consent.
Author Contributions
All authors made a significant contribution in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these aspects; took part in drafting, revising or critically reviewing the manuscript; approved the final version to be published gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and accept responsibility for all aspects of the work.
Funding
This publication charge is funded by Unpad through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/ B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025).
Disclosure
The authors declare that they have no conflicts of interest related to this work.
References
1. Krina TZ, Christian MB, Stacey AM. Endometriosis, review article. N Engl J Med. 2020;382:56. doi:10.1056/NEJMra1810764
2. Becker CM, Bokor A, Heikinheimo O, et al. ESHRE PAGES The members of the Endometriosis Guideline Core Group. Hum Reprod. 2022;1–7.
3. Morassutto C, Monasta L, Ricci G, Barbone F, Ronfani L. Incidence and estimated prevalence of endometriosis and adenomyosis in northeast italy: a data linkage study. PLoS One. 2016;11:e0154227. doi:10.1371/journal.pone.0154227
4. Kristjansdottir A, Rafnsson V, Geirsson RT. Comprehensive evaluation of the incidence and prevalence of surgically diagnosedpelvic endometriosis in a complete population. Acta Obstet Gynecol Scand. 2023;102:1329–1337. PMID: 36965019. doi:10.1111/aogs.14556
5. Becker CM, Bokor A, Heikinheimo O, et al. ESHRE guideline: endometriosis. Hum Reprod Open. 2022;2022. doi:10.1093/hropen/hoac009
6. Alammari R, Lightfoot M, Hur HC. Impact of cystectomy on ovarian reserve: review of the literature. J Minim Invasive Gynecol. 2017;24:247–257. PMID: 28089684. doi:10.1016/j.jmig.2016.12.010
7. Anh ND, Ha NTT, Tri NM, et al. Long-term follow-up of anti-mullerian hormone levels after laparoscopic endometrioma cystectomy. Int J Med Sci. 2022;19:651–658. PMID: 35582413. doi:10.7150/ijms.69830
8. Rius M, Gracia M, Ros C, et al. Impact of endometrioma surgery on ovarian reserve: a prospective, randomized, pilot study comparing stripping with CO2 laser vaporization in patients with bilateral endometriomas. J Int Med Res. 2020:48. PMID: 32527167. doi:10.1177/0300060520927627
9. Tsolakidis D, Pados G, Vavilis D, et al. The impact on ovarian reserve after laparoscopic ovarian cystectomy versus three-stage management in patients with endometriomas: a prospective randomized study. Fertil Steril. 2010;94:71–77. PMID: 19393996. doi:10.1016/j.fertnstert.2009.01.138
10. Zanetta G, Lissoni A, Valle CD, Trio D, Pittelli M, Rangoni G. Ultrasound-guided aspiration of endometriomas: possible applications and limitations. Fertil Steril. 1995;64:709–713. PMID: 7672139. doi:10.1016/S0015-0282(16)57843-1
11. Veth VB, van de Kar M, Duffy JMN, van Wely M, Mijatovic V, Maas JWM. Gonadotrophin-releasing hormone analogues for endometriosis. Cochrane Database Syst Rev. 2021;2021. doi:10.1002/14651858.CD014788
12. Yu L, Sun Y, Fang Q. Efficacy of laparoscopic surgery combined with leuprorelin in the treatment of endometriosis associated with infertility and analysis of influencing factors for recurrence. Front Surg. 2022;9:1–7. doi:10.3389/fsurg.2022.873698
13. Romanski PA, Brady PC, Farland LV, Thomas AM, Hornstein MD. The effect of endometriosis on the antimüllerian hormone level in the infertile population. J Assist Reprod Genet. 2019;36:1179–1184. PMID: 31020439. doi:10.1007/s10815-019-01450-9
14. Pacchiarotti A, Frati P, Milazzo GN, Catalano A, Gentile V, Moscarini M. Evaluation of serum anti-Mullerian hormone levels to assess the ovarian reserve in women with severe endometriosis. Eur J Obstetrics Gynecol Reprod Biol. 2014;172:62–64. PMID: 24210790. doi:10.1016/j.ejogrb.2013.10.003
15. Tian Z, Zhang Y, Zhang C, Wang Y, Zhu HL. Antral follicle count is reduced in the presence of endometriosis: a systematic review and meta-analysis. Reprod Biomed Online. 2021;42:237–247. PMID: 33168492. doi:10.1016/j.rbmo.2020.09.014
16. Muzii L, Galati G, Mattei G, et al. Expectant, medical, and surgical management of ovarian endometriomas. J Clin Med. 2023;12(5):1858. doi:10.3390/jcm12051858
17. Salem HAM, Moustafa MZE, Abd Elnaby EA. Large ovarian endometrioma: three-step procedure or combined excisional and ablative surgery. Fertil Steril. 2013;100(3):S74–S75. doi:10.1016/j.fertnstert.2013.07.1913
18. Kitajima M, Matsumoto K, Murakami N, et al. Ovarian reserve after three-step laparoscopic surgery for endometriomas utilizing dienogest: a pilot study. Reprod Med Biol. 2020;19:425–431. doi:10.1002/rmb2.12349
19. Hu X, Zhang Q, Zheng Y, et al. A single-dose, randomized, open-labeled, parallel-group study comparing the pharmacokinetics, pharmacodynamics and safety of leuprolide acetate microspheres 3.75 mg and Enantone® 3.75 mg in healthy male subjects. Front Pharmacol. 2022;13:1–10. doi:10.3389/fphar.2022.946505
20. Ramachandran A, Dhulkhed S, Bhakta R, et al. Influence of endomeriotic cyst diameter and the severity of endometriosis on theovarian parenchyma excised during laparoscopic cystectomy. J Clin Diagn Res. 2013;7:2241–2243. PMID: 24298486. doi:10.7860/JCDR/2013/5730.3481
21. Rzewuska AM, Żybowska M, Sajkiewicz I, et al. Gonadotropin-releasing hormone antagonists—a new hope in endometriosis treatment? J Clin Med. 2023;12:1008. doi:10.3390/jcm12031008
22. Roman H. Endometriosis surgery and preservation of fertility, what surgeons should know. J Visceral Surg. 2018;155:S31–6. PMID: 29709485. doi:10.1016/j.jviscsurg.2018.03.002
23. Horne AW, Missmer SA. Pathophysiology, diagnosis, and management of endometriosis. BMJ. 2022;379:e070750. PMID: 36375827. doi:10.1136/bmj-2022-070750
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.