Back to Journals » Clinical Optometry » Volume 17
Outcomes of Vision Therapy on Visual Skills and Oculomotor Functions in Children with Autism Spectrum Disorder: A Prospective Study
Authors Chhetri S ![]() , Belbase U
, Belbase U ![]() , Poudel M
, Poudel M ![]() , Dhakal D, Bhandari A
, Dhakal D, Bhandari A ![]() , Cantó-Cerdán M
, Cantó-Cerdán M ![]() , Subedi A
, Subedi A ![]() , Shrestha O
, Shrestha O ![]()
Received 4 July 2025
Accepted for publication 28 October 2025
Published 6 November 2025 Volume 2025:17 Pages 341—351
DOI https://doi.org/10.2147/OPTO.S551647
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Mr Simon Berry
Santosh Chhetri,1– 3 Umesh Belbase,2,3 Manish Poudel,4 Deepak Dhakal,5,6 Aastha Bhandari,7 Mario Cantó-Cerdán,8,9 Anup Subedi,10 Oshin Shrestha11
1Department of Binocular Vision, Shrawan Autism Child Care Center, Butwal, Nepal; 2Department of Optometry, Metro Eye Care Lumbini, Butwal, Nepal; 3Department of Ophthalmology, Butwal Hospital Pvt. Ltd, Butwal, Nepal; 4Department of Research and Biostatistics, Tilganga Institute of Ophthalmology, Kathmandu, Nepal; 5Department of Ophthalmology, Lumbini Province Hospital, Butwal, Nepal; 6Department of Ophthalmology, Metro Eye Care Lumbini, Butwal, Nepal; 7Department of Ophthalmology, Rapti Academy of Health Science, Ghorahi, Nepal; 8Department of Optometry, Vissum (Miranza), Alicante, Spain; 9Grupo de Investigación en Optometría (GIOptom), University of Alicante, Alicante, Spain; 10Department of Optometry, Himalaya Eye Institute, Pokhara, Nepal; 11Department of Behavioral Therapy, Shrawan Autism Child Care Center, Butwal, Nepal
Correspondence: Santosh Chhetri, Shrawan Autism Child Care Center, Butwal 32907, Lumbini, Nepal, Tel +977 9702026113, Email [email protected]
Purpose: Visual skills and Oculomotor function deficits are common in children with Autism Spectrum Disorder (ASD), potentially affecting their development and quality of life. This study aimed to evaluate the effectiveness of vision therapy in visual perceptual skills and oculomotor function in children with ASD.
Patients and Methods: This prospective interventional study was conducted using a convenience sampling method between February and May 2025. All children with a prior diagnosis of ASD who met the inclusion criteria were included in the study and underwent 45 sessions of vision therapy guided by the Developmental, Individual-Differences, Relationship-Based (DIR) model. Visual skills and oculomotor functions were assessed before and after vision therapy using the Wachs Analysis of Cognitive Structures (WACS) and the Northeastern State University College of Optometry (NSUCO) Oculomotor test, respectively. The paired t-test with Hedge’s g effect size was used to compare pre and post vision therapy outcomes for normally distributed data, while the Wilcoxon signed-rank test with effect size r was applied for non-normally distributed variables. Analysis of Covariance was used to examine the effect of ASD severity on post-therapy outcomes while controlling for age and gender.
Results: Among the 42 children with ASD enrolled in the study, 36 completed all 45 sessions of vision therapy. Significant post-therapy improvements with large effect size were observed in visual perceptual skills (WACS) and oculomotor functions (NSUCO). Children with mild to moderate ASD showed greater improvements than those with severe ASD. Analysis of covariance revealed a significant effect of ASD severity on post-therapy outcomes: WACS (F(1,32) = 36.80, p < 0.001, R2 = 0.55), saccades (F(1,32) = 36.75, p < 0.001, R2 = 0.54), and pursuits (F(1,32) = 35.54, p < 0.001, R2 = 0.54). Age and gender showed no statistically significant effects on the outcomes.
Conclusion: This prospective study provides preliminary evidence that DIR-guided vision therapy, particularly when combined with occupational and behavioral therapy, may enhance visual perceptual and oculomotor functions in children with ASD. However, randomized controlled studies with longer follow-up are needed to confirm these results.
Keywords: ASD, visuomotor, spatial awareness, saccade, pursuit, DIR model
Introduction
Autism Spectrum Disorder (ASD) is a neurodevelopmental disorder characterized by persistent deficits in communication, social interaction, and restricted, repetitive patterns of behavior, interests, or activities.1,2 Although the exact cause of ASD remains unknown, several risk factors have been identified, including genetic disorders, environmental factors, low birth weight, older parental age, having a sibling with autism,3 and food intolerances.4
Around one in two children with ASD are found to have some form of ocular morbidity, including strabismus,5 amblyopia, or significant refractive error.6–8 Children with ASD often show poor eye contact and significant deficits in oculomotor function, visual-motor skills, visual analysis skills, spatial awareness, body awareness, and bilateral integration.9 These challenges can potentially impact their cognitive development, motor abilities, perception, behavior, social interactions, and communication skills.10,11
Although vision therapy is time-consuming,12 it has been shown to improve repetitive behaviors, social communication, and social interaction in children with ASD. In addition to these behavioral improvements, significant changes in oculomotor functions and visual skills have also been observed following vision therapy.10 In a case report by Michael Au and Rachel Coulter,13 vision therapy guided by the Developmental, Individual-Differences, Relationship-Based (DIR) model was shown to improve oculomotor functions and visual skills in children with ASD. They used the Northeastern State University College of Optometry (NSUCO) oculomotor test to assess oculomotor functions and the Wachs Analysis of Cognitive Structure (WACS) tool to evaluate visual skills. The DIR-based model plays a crucial role in understanding and addressing the unique developmental needs of children with ASD.14,15 By focusing on a child’s developmental stage, individual sensory processing differences, and the quality of relationships, the DIR model helps tailor interventions. Incorporating DIR principles into vision therapy ensures that activities not only target visual skills deficits but also align with the child’s emotional and sensory profile, thereby enhancing engagement, motivation, and overall therapy effectiveness.13
Recent systematic reviews and randomized controlled trials have highlighted persistent visual and oculomotor deficits in ASD, including abnormalities in eye movement control, visuomotor integration, and attentional orienting.16,17 Moreover, although some pilot studies and small-sample trials suggest that vision therapy or visual-motor interventions can improve functional outcomes,18 robust large-scale RCTs specifically focused on ASD remain limited. Importantly, no previous studies have combined structured vision therapy with DIR/Floortime principles, despite the potential synergistic benefits of targeting both neurophysiological and socio-emotional domains.19
From a neurophysiological perspective, vision therapy may enhance synaptic plasticity within cortico-subcortical networks that support eye movement control (frontal eye fields, superior colliculus, parietal cortex, and cerebellum). Improvements in oculomotor stability and visual attention are thought to support higher-order skills such as joint attention, visuospatial processing, and social engagement, which are commonly impaired in ASD.18
Despite these preliminary insights, gaps remain in the literature: (i) the scarcity of adequately powered controlled studies;16 (ii) limited integration of DIR-based approaches with structured vision therapy; and (iii) a lack of standardized outcome measures to assess both visual and functional domains. Addressing these gaps is critical to establish stronger evidence for clinical practice.In this context, the primary aim of this study was to evaluate the effect of vision therapy on visual skills and oculomotor functions in children with ASD, using the WACS and the NSUCO oculomotor test, with interventions guided by DIR principles. It also aimed to examine the influence of age, gender, and autism severity on the outcomes.
Materials and Methods
Participants
A total of 42 children with ASD who presented to the Binocular Vision Department of the Shrawan Autism Child Care Center, Butwal and Metro Eye Care Lumbini, Butwal from February to May 2025, participated in the study.
Inclusion and Exclusion Criteria
Children who already had a confirmed diagnosis of ASD, assessed using the Childhood Autism Rating Scale (CARS), and whose parents were willing to attend at least four weekly sessions (for a total of 45 sessions), were included in the study. Children were excluded if they had any known visual impairment, or systemic comorbidities such as cerebral palsy, hydrocephalus, or epilepsy. Written informed consent was obtained from the legally authorized representatives of all participants prior to enrollment, in accordance with ethical standards.
Study Design and Sample Size
This prospective interventional study was conducted using a convenience sampling method at the Department of Binocular Vision, Shrawan Autism Child Care Center, Butwal and Metro Eye Care Lumbini, Butwal.
There are no prior studies on the effects of perceptual vision therapy in children with ASD. A medium standardized effect size (Cohen’s d = 0.5) was assumed for calculating the sample size for a paired pre–post comparison. Using a significance level of 0.05 (Z = 1.96) and a power of 80%, the minimum required sample size was estimated to be 32.
Ocular Examination
The clinical examination was conducted by a team comprising one consultant ophthalmologist, two optometrists (a consultant pediatric optometrist and vision therapist, and a senior consultant optometrist), one ophthalmic assistant, and one clinical psychologist. The examination took place in the Binocular Vision Department of the Shrawan Autism Child Care Center. Both dry and cycloplegic retinoscopy were performed by the pediatric optometrist.
Hirschberg corneal light reflex was used to detect tropias, while the prism bar cover test was used to measure the angle of deviation in prism diopters. The external eye, anterior segment, and posterior segment (dilated) of all children were examined by ophthalmologists and optometrists using a pen torch, magnifying loupe, and direct ophthalmoscope. Pursuit and saccadic functions were assessed using the NSUCO Oculomotor test. Body awareness and bilateral integration, spatial awareness, visual analysis skills and visual-motor skills were evaluated using WACS. Both NSUCO oculomotor test and WACS tool were performed before and after 45 sessions of vision therapy. The refractive error was classified based on definitions of spherical equivalent refractive error (SER) by Breslin et al.20
Intervention
The various vision therapy activities listed in Table 1 were administered to each child over 45 sessions, with each session lasting 45–60 minutes and conducted by a vision therapist. In each session, participants performed a minimum of two activities of body awareness and bilateral integration, spatial awareness, visual analysis, visual-motor skills, and saccadic and pursuit training. The therapy activities began with simpler tasks, and the level of difficulty was gradually increased over time. The DIR-based framework was used to guide the intervention process, with input from the clinical psychologist. This approach allowed the team to tailor vision therapy activities to each child’s developmental level and sensory profile, thereby enhancing engagement, motivation, and therapeutic effectiveness.
 |
Table 1 Vision Therapy Activities Targeting Visual Perceptual Skills and Oculomotor Functions |
Tools
Wachs Analysis of Cognitive Structure (WACS)
The WACS test was recommended to fully elicit underlying deficits in visual processing. It is used to assess the body awareness and bilateral integration, spatial awareness, visual analysis skills and visual motor skills in children.13 The entire test comprises four subtests, totaling 22 items (after excluding 4 auditory items):
- Object Identification (3 items) – Assesses visual recognition and visual analysis skills.
- Object Design (6 items) – Assesses spatial awareness and visual-motor skills.
- Graphic Design (4 items) – Assesses visual analysis and visual-motor skills.
- General Movement (9 items) – Assesses body awareness, bilateral integration, spatial awareness, and visual-motor skills.
Each item is scored on a scale of 0 to 2, with 2 indicating the highest level of performance.
Northeastern State University College of Optometry (NSUCO)
The NSUCO Oculomotor test, developed by the Northern State University College of Optometry, is a standardized clinical tool used to assess saccadic and pursuit oculomotor functions in a structured and observable manner.21 The examiner observes the saccadic and pursuit eye movements and evaluates performance based on four categories: head movement, body movement, ability, and accuracy. Each category is scored on a scale from 1 to 5, with 5 indicating the highest level of performance.
Statistical Analysis
All statistical analyses were performed using SPSS version 20. The Shapiro–Wilk test was used to assess the normality of the data. A significance level of p < 0.05 was considered statistically significant. Paired-sample t-tests with Hedge’s g effect size were used for normally distributed pre- and post-therapy comparisons, while the Wilcoxon signed-rank test with effect size r was applied for non-normally distributed data. An Analysis of covariance (ANCOVA) was utilized to examine the effect of severity on each dependent variable while controlling for age and gender.
Ethical Consideration
Ethical clearance for the study was granted by the Institutional Review Committee of the Nepal Health Research Council. All procedures were conducted in adherence to the principles of the Declaration of Helsinki and applicable local ethical guidelines. Participation was entirely voluntary, and confidentiality was strictly maintained throughout the study. Written informed consent was obtained from the legally authorized representatives of all participants, in accordance with ethical standards. Assent was also obtained from minors when appropriate, and no financial compensation was provided. However, logistical support such as travel guidance and flexible scheduling was offered to participating families.
Results
Demographic and Clinical Profile
A total of 42 children with ASD participated in the study. Of these, 36 children (27 boys and 9 girls) with ASD completed all 45 sessions of vision therapy. These 36 children were between 6 and 12 years old, with a mean age of 8.02 ± 1.75 years, and included 22 with hypermetropia, 8 with emmetropia, and 6 with myopia. Based on the severity of ASD, 21 children had mild to moderate ASD, while 15 had severe ASD. Table 2 shows the demographic and clinical profiles of the participants who completed 45 sessions of vision therapy.
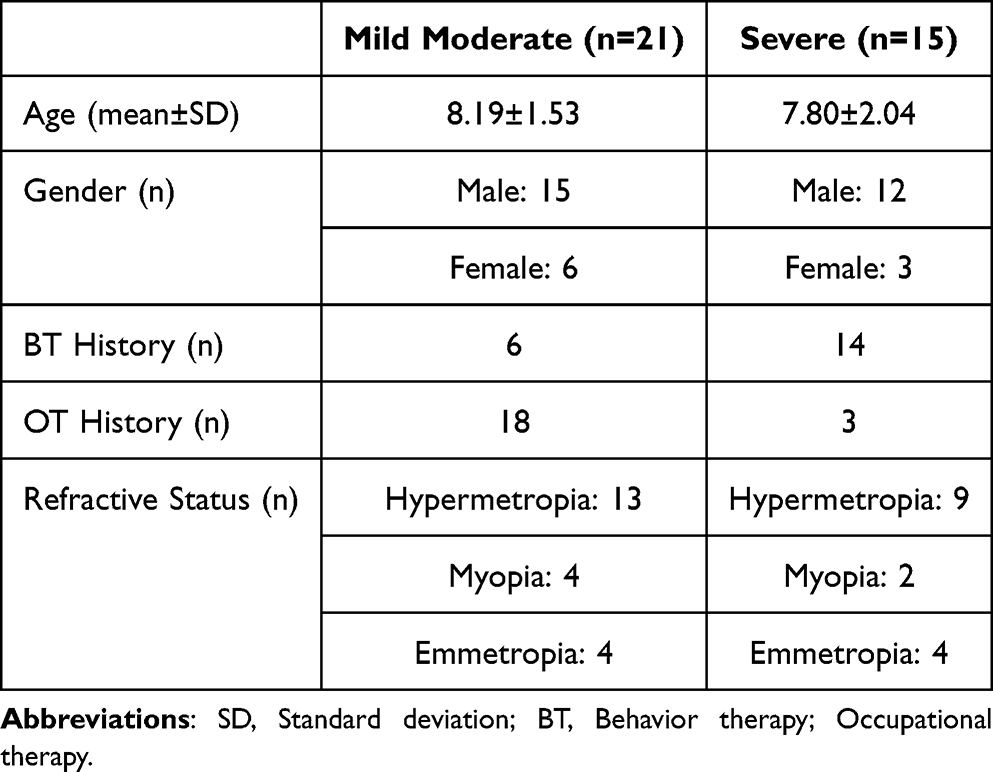 |
Table 2 Demographic Profile and Clinical Profile of the Participants Who Completed 45 Sessions of Vision Therapy |
Effect of Intervention on WACS
Statistical analysis of the before and after vision therapy of the WACS subtest revealed significant improvements in the identification of object, object design, graphic design, and general movement for both the mild-moderate group and the severe group (p < 0.05). The effect sizes (Hedge’s g) were greater than 1.80 in the mild to moderate group and greater than 0.65 in the severe group. Table 3 presents the WACS subtest scores before and after vision therapy, along with the effect sizes, for the mild to moderate and severe groups.
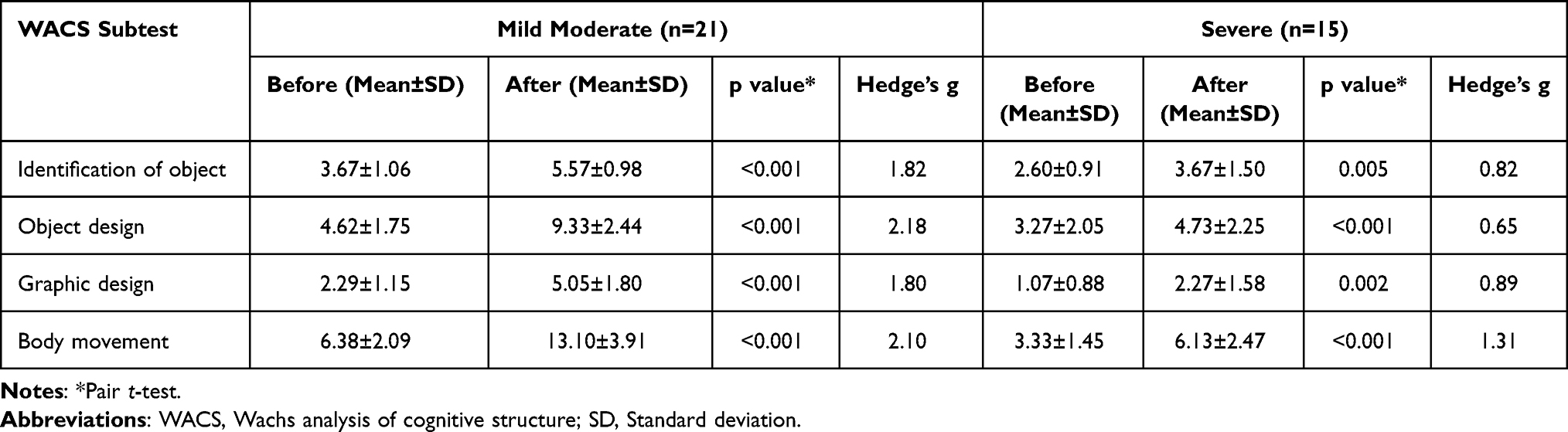 |
Table 3 WACS Subtest Score Before and After Vision Therapy for Mild Moderate and Severe Group |
An ANCOVA was conducted to examine the effect of severity on WACS after therapy while controlling for age and gender. There was a significant effect of severity on WACS after vision therapy, F(1, 32) = 36.80, p <0.001, and severity accounted for 55.0% of the variance in WACS after therapy (R2 = 0.55). However, age (F(1, 32) = 0.157, p =0.695) and gender (F(1, 32) = 0.103, p =0.751) did not have significant effects on post-WACS. The results are shown in Table 4 and Figure 1.
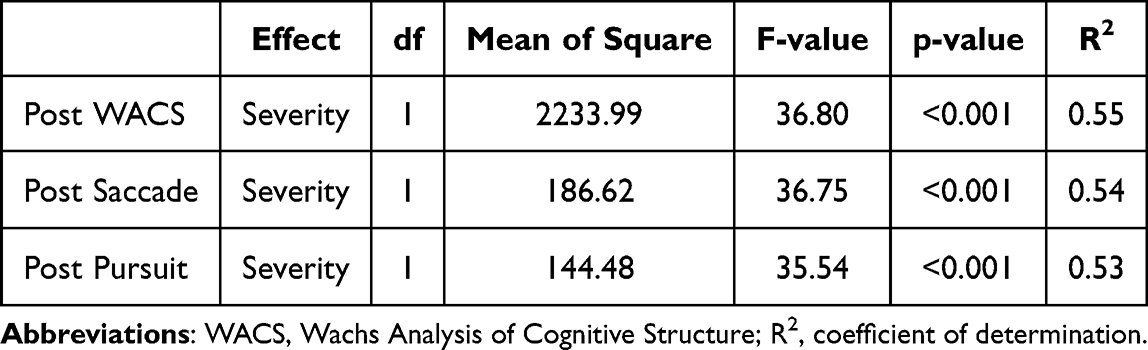 |
Table 4 ANCOVA Results for the Effect of Severity on Post-WACS, Post-Saccade, and Post-Pursuit Scores |
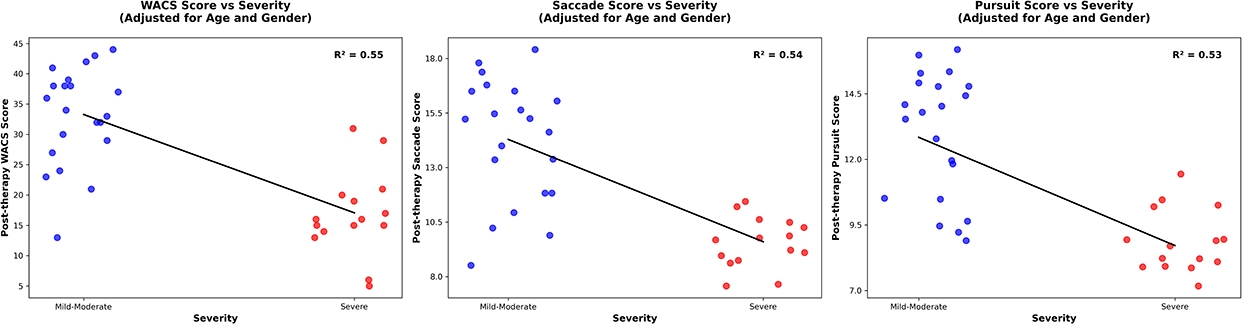 |
Figure 1 Left-Regression analyses between Severity of ASD vs Post therapy WACS score (Adjusted for age and gender; Middle-Severity of ASD vs Post therapy Saccade score (Adjusted for age and gender); Right- Severity of ASD vs Post therapy pursuit score (Adjusted for age and gender). |
Effect of Intervention on Saccade
Comparison of saccadic performance before and after vision therapy revealed significant improvements with large effect sizes in ability, accuracy, head movement, and body movement in both the mild-moderate and severe groups (p < 0.05), as shown in Table 5.
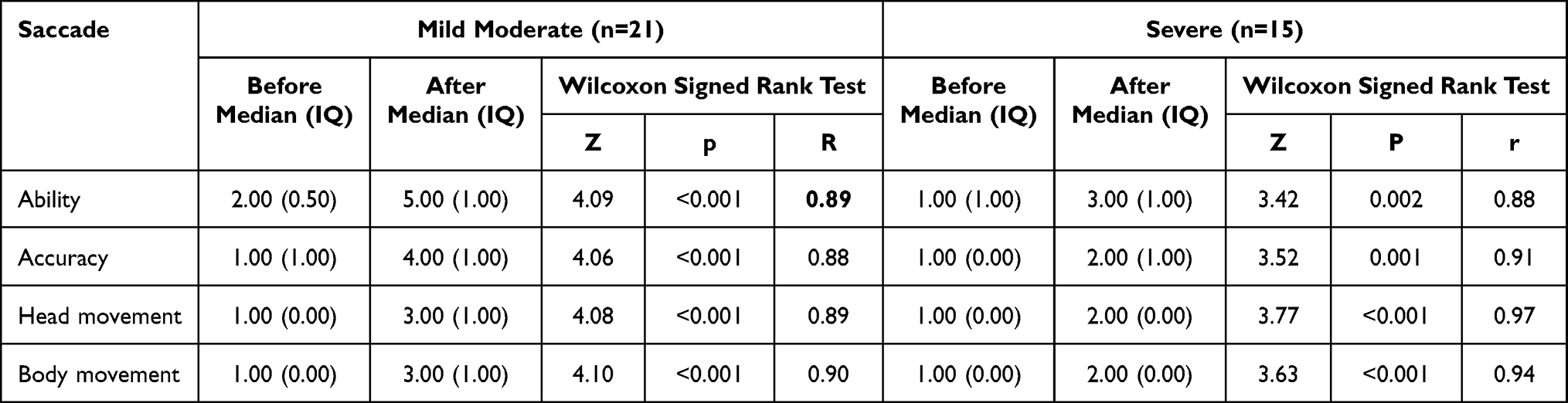 |
Table 5 Saccade Before and After Therapy for Mild Moderate and Severe Group |
An ANCOVA was conducted to examine the effect of severity on saccade after therapy while controlling for age and gender. There was a significant effect of severity on saccade after vision therapy, F(1, 32) = 36.75, p <0.001, which accounted for 53.8% of the variance in saccade (R2 = 0.53). However, age (F(1, 32) = 0.174, p = 0.679) and gender (F(1, 32) = 0.020, p = 0.889) did not have significant effects on saccade after vision therapy. The results are presented in Table 4 and Figure 1.
Effect of Intervention on Pursuit
Statistical analysis of pursuit before and after vision therapy revealed significant improvements with large effect sizes in ability, accuracy, head movement, and body movement for both the mild to moderate and severe groups (p < 0.05), as shown in Table 6.
 |
Table 6 Pursuit Before and After Therapy for Mild Moderate and Severe Group |
An ANCOVA was conducted to examine the effect of severity on Pursuit after therapy while controlling for age and gender. There was a significant main effect of severity on Post-Pursuit, F(1, 32) = 35.54, p <0.001, which accounted for 54.0% of the variance in pursuit after therapy (R2 = 0.54). However, age F(1, 32) = 0.006, p =0.938) and gender (F(1, 32) = 0.267, p =0.609) did not have significant effects. The results are shown in Table 4 and Figure 1.
Discussion
We conducted a study to determine the effectiveness of vision therapy on spatial awareness, visual-motor skills, visual analysis, body awareness, and oculomotor function in children with Autism Spectrum Disorder (ASD). The use of the WACS and the NSUCO Oculomotor test before and after the vision therapy guided by a DIR-based model provided objective evidence of improvement in these skills. Currently, only a few case reports have explored the effectiveness of vision therapy on various visual skills and oculomotor functions. Therefore, this study is among the first to evaluate the impact of vision therapy on different visual skills and oculomotor functions.
Although our findings suggest positive effects, the absence of a control group limits causal interpretation. Improvements may partly reflect concurrent therapies, natural developmental progression, or nonspecific influences such as increased therapist attention, structured engagement, or placebo effects. These results should therefore be considered exploratory and hypothesis-generating rather than confirmatory.13
Visuo-spatial skills are frequently underdeveloped in children with autism, and they often compensate for these challenges through repetitive behaviors such as side glancing, toe walking, finger flicking near the eyes, or hand flapping.22,23 In this study, the General Movement subtest of the WACS particularly assessed visual-spatial skills, body awareness, and bilateral integration, all of which showed improvement following vision therapy. Similar to the findings of the present study, Rose and Torgerson24 also reported improvements in body awareness and bilateral integration following optometric vision therapy, which led to the disappearance of these behaviors. In the study by Arabi et al,25 the computer-based visual training group, which performed only exercises involving eye tracking and eye-hand coordination, showed no significant effect on the frequency of repetitive behaviors. However, as noted by Arabi et al,25 movement within the environment and spatial orientation appear to be key factors contributing to improvements in bodily responses and visual processing in children with autism. This suggests that incorporating physical movement and spatially engaging vision therapy activities, as used in the present study, may play a more significant role in enhancing visual-spatial body awareness than visual training exercises alone.
The Object Design, Graphic Design, and General Movement subtests of the WACS also assess visuomotor abilities. In this study, significant improvements in visuomotor functions were observed following vision therapy. Similar results were reported by Arabi et al, where visuomotor exercises usually show significant improvement in the gross motor skills of children with ASD, and the vision therapy activities used to improve visuomotor skills were closely aligned with those in our study. Gross motor coordination needs to be reinforced before establishing eye-hand coordination.26 In our study, most of the children were receiving occupational therapy prior to participation, which likely supported the development of their visuomotor skills. The development of oculomotor function is closely linked to overall body movement.13 An improvement in oculomotor function can help an individual stay grounded and support the learning of new skills.27 In each session of vision therapy, we included at least two activities targeting saccades and pursuits.
Oculomotor function may represent a useful biomarker for monitoring response to vision therapy in children with ASD. Objective measurements using eye-tracking technology can provide detailed data on saccades, pursuits, fixation stability, and visual attention, allowing clinicians and researchers to quantify changes over time. However, caution is warranted because there are currently no well-established normative values for either typically developing populations or children with neurodevelopmental conditions. As a result, comparisons must be interpreted relative to baseline performance or within-subject changes rather than against absolute normative benchmarks. Integrating oculomotor assessments into therapy protocols could enhance individualized treatment planning and provide early indicators of responsiveness, but further work is needed to standardize protocols and interpretive frameworks.28
Our results also indicated that, compared to the mild–moderate group, children with severe ASD showed less improvement in oculomotor function following the intervention. This pattern was also evident in other visual skills such as visuomotor integration, spatial awareness, and body awareness. Beyond baseline differences in oculomotor abilities, several additional factors may account for this reduced improvement. Children with higher severity levels often present greater difficulties with sensory integration, attentional regulation, and behavioral flexibility, which may hinder their consistent engagement with therapy tasks. Moreover, reduced neural plasticity in more severe cases may further constrain the capacity to consolidate and generalize newly acquired skills. These considerations highlight the need to tailor vision therapy approaches to the specific sensory and cognitive profiles of children with different ASD severity levels.29,30
ANCOVA results showed that ASD severity significantly influenced the extent of improvement across WACS and NSUCO scores, with children in the mild moderate category showing the greatest post-therapy improvement. This significant improvement in the mild moderate group may be attributed to the fact that most children in this category were already undergoing occupational therapy, which helps stabilize the body in space, counteract gravity, and maintain balance, as these factors are believed to support visual system development.13 In contrast, age and gender were not significant predictors, suggesting that vision therapy may be broadly effective across different age groups and genders.
The study’s strengths include providing preliminary evidence that vision therapy guided by DIR principles may enhance visual and oculomotor functions in children with ASD. It also accounts for ASD severity, offering valuable insights into which subgroups may benefit most from vision therapy interventions. Furthermore, the research was conducted at an autism center serving patients from diverse regions of Nepal and nearby areas of India, ensuring a varied and representative sample population. Conversely, this study has several limitations that should be acknowledged. First, the duration of vision therapy was relatively short, and potential rebound effects or regression after therapy cessation were not assessed. Second, many participants were concurrently receiving occupational or behavioral therapy, which may have influenced outcomes and made it difficult to isolate the effects of vision therapy alone. Third, the convenience sampling method may have caused selection bias and limits the generalizability of the findings. Fourth, the absence of functional outcome measures, such as school performance or daily autonomy, limits the assessment of real-world impact. Lastly, the absence of a control group limits causal inference. Future studies should use multicenter randomized designs with larger samples, control groups, and longer follow-up to evaluate the effects of vision therapy alone. Incorporating objective measures, such as eye tracking or neuroimaging, and assessing functional outcomes like school performance and daily autonomy, will provide a more comprehensive understanding of the impact of vision therapy.
Conclusion
This study demonstrated that short-duration vision therapy may support the development of visual-spatial, visual-analysis, visual-motor skills, and oculomotor functions in children with ASD, particularly when combined with occupational and behavioral therapy and guided by the DIR model. These findings are preliminary, and further research addressing the study’s limitations is needed to confirm and extend these results.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, SC, upon reasonable request.
Acknowledgments
We would like to express our sincere gratitude to the Sharawan Autism Child Care Center and Metro Eye Care Lumbini for their support. We are especially thankful to the children and their families who participated in our research. We also extend our appreciation to the teachers, therapists, and specialists who contributed to this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
All expenses related to this project were covered personally, and no financial assistance was received from any specific organization.
Disclosure
The authors report no conflicts of interest in this work.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
2. World Health Organization. Autism spectrum disorders – fact sheet. 2019.
3. Kavitha U, Kayalvizhi E, Revathy K, Brindha TR, Muthulakshmi R, Chandrasekar M. A systematic review on valproate induced rat model of autism: pathophysiology, treatment, developmental and neurobehavioral assessment of rat offsprings. Biomed. 2021;41(1):9–15. doi:10.51248/.v41i1.526
4. Baspinar B, Yardimci H. Gluten-free casein-free diet for autism spectrum disorders: can it be effective in solving behavioural and gastrointestinal problems? Eurasian J Med. 2020;52(3):292–297. doi:10.5152/eurasianjmed.2020.19230
5. Black K, McCarus C, Collins MLZ, Jensen A. Ocular manifestations of autism in ophthalmology. Strabismus. 2013;21(2):98–102. doi:10.3109/09273972.2013.786733
6. Ezegwui IR, Lawrence L, Aghaji AE, et al. Refractive errors in children with autism in a developing country. Niger J Clin Pract. 2014;17(4):467–470. doi:10.4103/1119-3077.134042
7. Ikeda J, Davitt BV, Ultmann M, Maxim R, Cruz OA. Brief report: incidence of ophthalmologic disorders in children with autism. J Autism Dev Disord. 2013;43(6):1447–1451. doi:10.1007/s10803-012-1475-2
8. Kabatas EU, Ozer PA, Ertugrul GT, Kurtul BE, Bodur S, Alan BE. Initial ophthalmic findings in Turkish children with autism spectrum disorder. J Autism Dev Disord. 2015;45(8):2578–2581. doi:10.1007/s10803-015-2428-3
9. Leekam SR, Nieto C, Libby SJ, Wing L, Gould J. Describing the sensory abnormalities of children and adults with autism. J Autism Dev Disord. 2007;37(5):894–910. doi:10.1007/s10803-006-0218-7
10. Arunachalam V, Suresh K, Venkatesh L, Thiyagarajan S. Vision therapy for children with autism spectrum disorder – a review and case report. Biomed. 2022;42(4):836–840. doi:10.51248/.v42i4.1833
11. Grinter EJ, Maybery MT, Badcock DR. Vision in developmental disorders: is there a dorsal stream deficit? Brain Res Bull. 2010;82(3–4):147–160. doi:10.1016/j.brainresbull.2010.02.016
12. Chhetri S, Thapa Magar S, Adhikari S, Belbase U. Clinical scenario of pseudomyopia before and after vision therapy: two case reports. Nepal J Ophthalmol. 2024;16(31):74–79. doi:10.3126/nepjoph.v16i1.59178
13. Au M, Coulter R. Vision therapy for the autistic patient: a literature review and case report. Optom Vis Perform. 2014;2(5):244–250.
14. Coulter RA. Understanding the visual symptoms of individuals with autism spectrum disorder (ASD). Optom Vis Dev. 2009;40(3):164–175.
15. Wieder S, Greenspan S. Can children with autism master the core deficits and become empathetic, creative, and reflective? In:
16. Forbes EJ, Tiego J, Langmead J, et al. Oculomotor function in children and adolescents with autism, ADHD or co-occurring autism and ADHD. J Autism Dev Disord. 2025; 0123456789. doi:10.1007/s10803-024-06718-3
17. Longo R, Allegrini F, Gusson E, et al. Visual-motor involvement in autism spectrum disorder: could the stereopsis deficit affect motor coordination? Front Psychiatry. 2023;14(November). doi:10.3389/fpsyt.2023.1130185
18. Chan AS, Leung PY, Pang TWY, Sze SL. Eye-tracking training improves visuospatial working memory of children with attention-deficit/hyperactivity disorder and autism spectrum disorder. Autism Res. 2024;17(11):2244–2260. doi:10.1002/aur.3238
19. Chung K, Chung E. Randomized controlled pilot study of an app-based intervention for improving social skills, face perception, and eye gaze among youth with autism spectrum disorder. Front Psychiatry. 2023;14(April):1–12. doi:10.3389/fpsyt.2023.1126290
20. Breslin KMM, O’Donoghue L, Saunders KJ. A prospective study of spherical refractive error and ocular components among Northern Irish schoolchildren (the NICER study). Investig Ophthalmol Vis Sci. 2013;54(7):4843–4850. doi:10.1167/iovs.13-11813
21. Scheiman M, Wick B. Clinical Management of Binocular Vision: Heterophoric, Accommodative, and Eye Movement Disorders.
22. Jiang YV, Swallow KM. Body and head tilt reveals multiple frames of reference for spatial attention. J Vis. 2013;13(13):1–11. doi:10.1167/13.13.9
23. Peachey GT. Perspectives on optometric visual training. Clin Exp Optom. 1989;72(1):8–14. doi:10.1111/j.1444-0938.1989.tb03762.x
24. Rose M, Torgerson NG. A behavioral approach to vision and autism. J Optometric Vision Development. 1994;25:269–275.
25. Arabi M, Kakhki AS, Sohrabi M, Kouhbanani SS, Nooghabi MJ. Is visuomotor training an effective intervention for children with autism spectrum disorders? Neuropsychiatr Dis Treat. 2019;15:3089–3102. doi:10.2147/NDT.S214991
26. Taub MB, Mahaphon TK, Rodena J. A developmental approach to congenital ocular motor apraxia: case report and literature review. Optom Vis Dev. 2005;36(2):99–107.
27. Dudley L,M, Vasche T. Vision therapy for A patient with developmental delay literature review & case report. J Behav Optometry. 2010;21:39–45.
28. Cantó-Cerdán M, Hernández-Rodríguez CJ, Martínez-Abad A. Evidence on the parameters of oculomotor skills and normative values: a systematic review. J Optom. 2025;18(3):100570. doi:10.1016/j.optom.2025.100570
29. Gonçalves AM, Monteiro P. Autism Spectrum Disorder and auditory sensory alterations: a systematic review on the integrity of cognitive and neuronal functions related to auditory processing. J Neural Transm. 2023;130:325–408. doi:10.1007/s00702-023-02595-9
30. Chen Z, Wang X, Zhang S, Han F. Neuroplasticity of children in autism spectrum disorder. Front Psychiatry. 2024;15(April):1–12.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.