Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 14
Outcomes of laparoscopic cholecystectomy in patients with and without COPD
Authors Liao KM ![]() , Tseng CJ, Chen YC
, Tseng CJ, Chen YC ![]() , Wang JJ, Ho CH
, Wang JJ, Ho CH ![]()
Received 17 January 2019
Accepted for publication 30 April 2019
Published 27 May 2019 Volume 2019:14 Pages 1159—1165
DOI https://doi.org/10.2147/COPD.S201866
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Chunxue Bai
Kuang-Ming Liao,1 Chien-Jen Tseng,2 Yi-Chen Chen,3 Jhi-Joung Wang,3,4 Chung-Han Ho3,5
1Department of Internal Medicine, Chi Mei Medical Center, Chiali, Taiwan; 2Department of Surgery, Chi Mei Medical Center, Chiali, Taiwan; 3Department of Medical Research, Chi Mei Medical Center, Tainan, Taiwan; 4Allied AI Biomed Center, Southern Taiwan University of Science and Technology, Tainan, Taiwan; 5Department of Hospital and Health Care Administration, Chia Nan University of Pharmacy and Science, Tainan, Taiwan
Objective: The aim of this study was to investigate the outcomes of patients with COPD after laparoscopic cholecystectomy (LC).
Patients and methods: All COPD patients who underwent LC from 2000 to 2010 were identified from the Taiwanese National Health Insurance Research Database. The outcomes of hospital stay, intensive care unit (ICU) stay, and use of mechanical ventilation and life support measures in COPD and non-COPD populations were compared.
Results: A total of 3,954 COPD patients who underwent LC were enrolled in our study. There were significant differences in the hospitalization period, ICU stay, and use of mechanical ventilation and life support measures between the COPD and non-COPD populations. The mean hospital stay, ICU stay and number of mechanical ventilation days in the COPD and non-COPD groups were 7.81 vs 6.01 days, 5.5 vs 4.5 days and 6.40 vs 4.74 days, respectively. The use of life support measures, including vasopressors and hemodialysis, and the rates of hospital mortality, acute respiratory failure and pneumonia were also increased in COPD patients compared with those in non-COPD patients.
Conclusion: COPD increased the risk of mortality, lengths of hospital and ICU stays, ventilator days and poor outcomes after LC in this study.
Keywords: COPD, laparoscopic cholecystectomy, outcome
A Letter to the Editor has been published for this article.
A response to the letter has been published
Introduction
Laparoscopic cholecystectomy (LC) is a safe and effective treatment for patients with cholecystitis and is widely applied in clinical settings. LC has become the treatment of choice for many patients with symptomatic and asymptomatic gallstones.1
Patients who undergo LC can have a reduced operative time, less scarring, less pain and blood loss, improved convalescence, a shorter length of hospital stay and less medical expenditures than those who undergo open cholecystectomy.2,3
Factors predicting the technical difficulty have to be considered of primary importance since the conversion to laparotomy is a risk factor for postoperative respiratory insufficiency in high-risk groups. A previous meta-analysis showed that male sex, age >65 years, diabetes, acute cholecystitis, degree of gallbladder wall thickness, and history of upper abdominal surgery were all risk factors for converting LC to open cholecystectomy.4
Patients with COPD have airway obstructions that are not fully reversible by bronchodilators, decreased lung elasticity and reduced lung recoil pressure because of emphysema, which result in increased total lung capacity and pressure on the diaphragm.
Bayrak et al5 evaluated 60 COPD patients and showed that spinal anesthesia was better than general anesthesia in COPD patients who underwent LC because spinal anesthesia causes no impairment of lung function. Although studies have recognized the safety of LC in COPD patients, some studies have focused on LC vs open surgery and general anesthesia vs spinal anesthesia. The aim of our study was to compare the outcomes of COPD patients and the general population after LC in clinical practice using data from a large nationwide unselected population to assess the length of intensive care unit (ICU) and hospital stays, mortality, and resource use, including ventilator days, vasopressor use and hemodialysis. This study represents a comprehensive comparison of LC between COPD patients and the general population.
Patients and methods
Data source
Taiwan’s National Health Insurance Research Database (NHIRD), which is a claims population database, was used in this study. The claims from NHIRD consist of disease diagnosis, prescriptions, ambulatory care and surgical records, outpatient visits, and inpatient care and surgical operation records. The disease records were identified according to the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) code. Encrypted personal identifiers are used in the NHIRD to protect patients’ privacy and to prevent the possibility of an ethical violation according to regulations of the Bureau of National Health Insurance in Taiwan. Because the identifiable personal information could not be found in the NHIRD, an exemption was approved by the Institutional Review Board of Chi Mei Medical Center.
Definition of study subjects
Patients having first-time surgery for LC from 1997 to 2013 were selected for this study. The order code of the medical expenditure application for LC was 75215B according to the rules of Taiwan’s national health insurance. COPD patients who received LC and were older than 40 years were identified as the case group. A diagnosis of COPD was based on the ICD-9-CM codes 490–492 and 496 from the hospital admission dataset. Patients with COPD diagnosis after LC and incomplete demographic data were excluded from this study. The controls were patients without COPD who received LC. For reducing the potential confounding bias, cases and controls were 1:8 matched by age and gender with enough statistical power.6 The selection process of the study subjects is presented in a flow diagram (Figure 1).
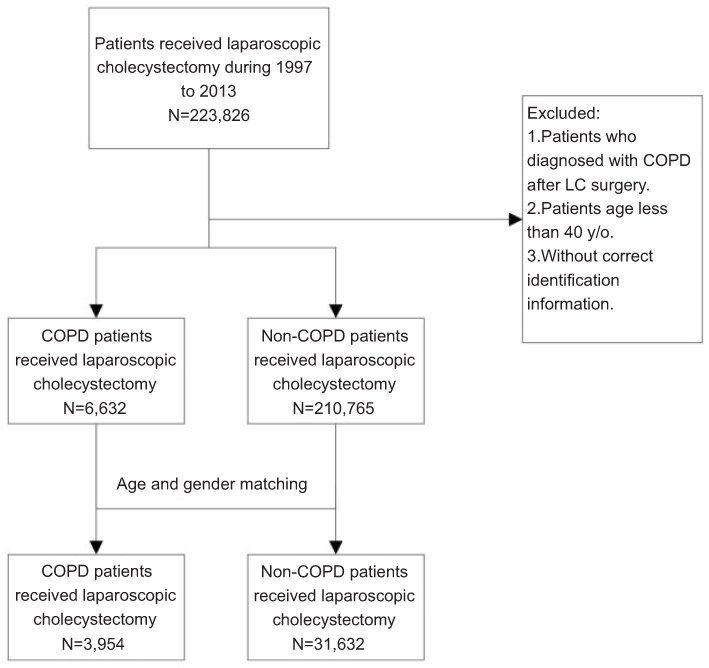 | Figure 1 The selection process of study subjects.Abbreviations: LC, laparoscopic cholecystectomy; y/o, year old. |
Measurements
Age, gender, income, hospital level, comorbidities, and anesthesia duration of receiving LC records were collected in this study. Comorbidities were defined following ICD-9-CM codes: diabetes (ICD-9-CM: 250), hypertension (ICD-9-CM: 401–405), dyslipidemia (ICD-9-CM: 272), congestive heart failure (ICD-9-CM: 428), atrial fibrillation (ICD-9-CM: 427.31), stroke (ICD-9-CM: 430–437), malignancy (ICD-9-CM: 140–208), chronic kidney disease (ICD-9-CM: 403–404, 580–587, 250.4, 274.1, 440.1, 442.1, 572.4, 753.1), peptic ulcer disease (ICD-9-CM: 531–534), and obesity (ICD-9-CM: 278). The anesthesia duration of receiving LC was also estimated according to the medical expenditure applications.
Outcome measurements
The primary interesting outcomes were the resource utilization, such as length of ICU stay, the length of using mechanical ventilation, and life-support measures among the LC patients in this study. The life-support measurements included vasopressor use, hemodialysis and hospital mortality. Hospital mortality was based on the death records from the inpatient claims database. In addition, the complications of LC, such ARF (ICD-9-CM: 518.5, 518.81, 518.82, 518.84) and pneumonia (ICD-9-CM: 480–488), were also considered to measure the potential effects.
Statistical analysis
Statistical Analysis System (SAS) (version 9.4; SAS Institute, Inc., Cary, NC, USA) statistical software was applied for all analyses. The differences between patients with COPD and those without were estimated using Wilcoxon rank sum test for continuous variables and Pearson’s chi-square test for categorical variables. Logistic regression, which was adjusted all potential confounding factors, was used to estimate the associated risk of length of ICU stay, length of using MV, life-support measurements, and potential complications. The threshold for statistical significance was set P<0.05.
Results
A total of 3,954 COPD patients who underwent LC were enrolled in our study. Among the patients, 32.78% and 33.33% were aged 60–69 and 70–79 years, respectively. A total of 8.93% of the patients were older than 80 years. Most patients underwent LC in regional hospitals (41.81%), followed by medical centers and district hospitals. The most common comorbidity was hypertension (45.52%), and the second most common comorbidity was diabetes (29.69%). Most patients had an anesthesia duration (64%) that was between 0 and 2 hrs. Table 1 shows the characteristics of patients who underwent LC in the COPD and non-COPD populations.
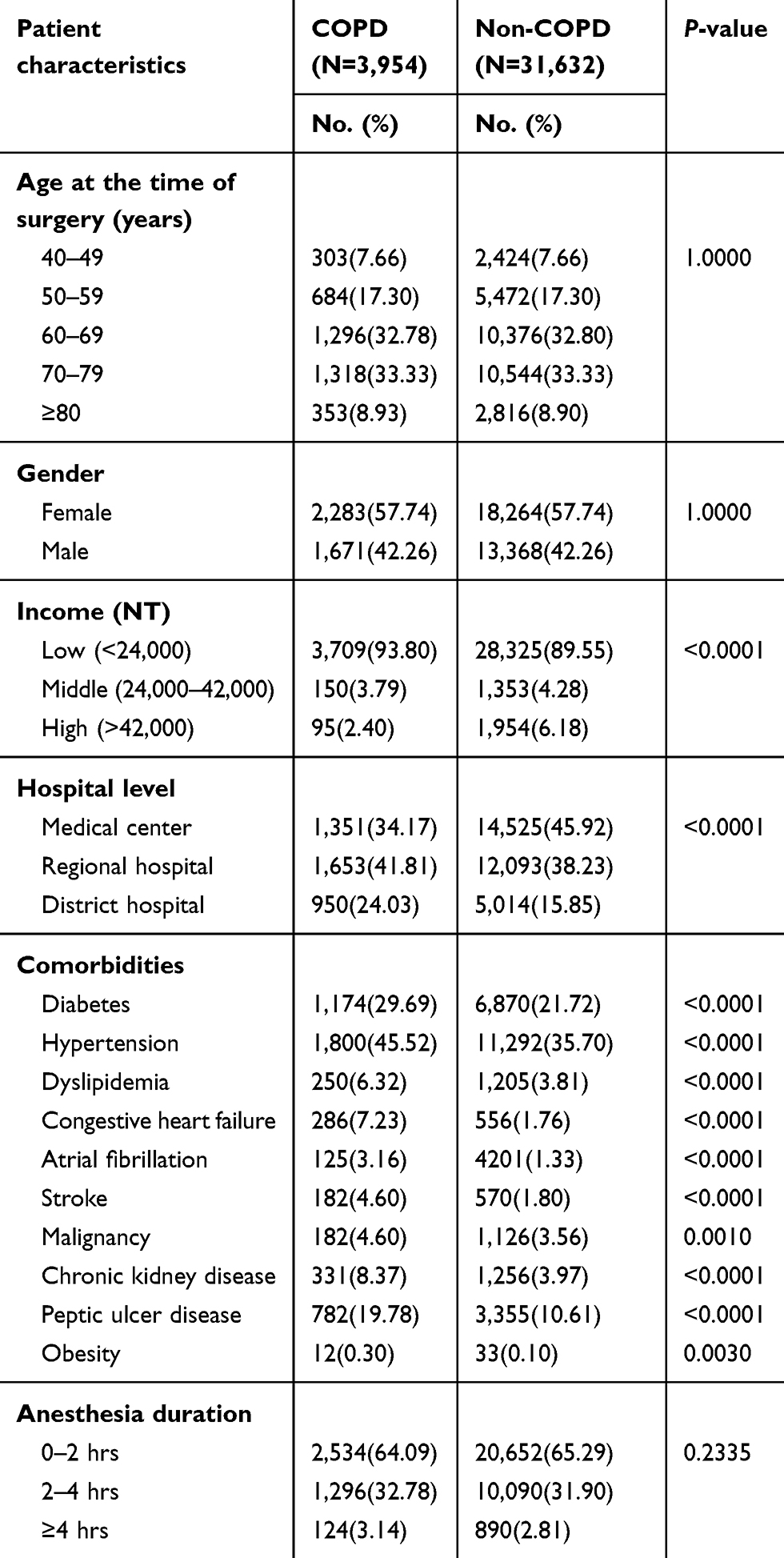 | Table 1 Comparison of laparoscopic cholecystectomy in patients with and without COPD |
Table 2 shows the resources used by the study population. There were significant differences in the hospitalization period, ICU stay, and use of mechanical ventilation and life support measures between the COPD and non-COPD populations. The mean hospital stay was 7.81 days in the COPD population and 6.01 days in the non-COPD population. The mean ICU stay was 5.5 days in the COPD population and 4.5 days in the non-COPD population. The duration of mechanical ventilation was also longer in the COPD population than in the non-COPD population at 6.40 and 4.74 days, respectively. The use of life support measures including vasopressor use and hemodialysis as well as hospital mortality were increased in the COPD population compared with those in the non-COPD population.
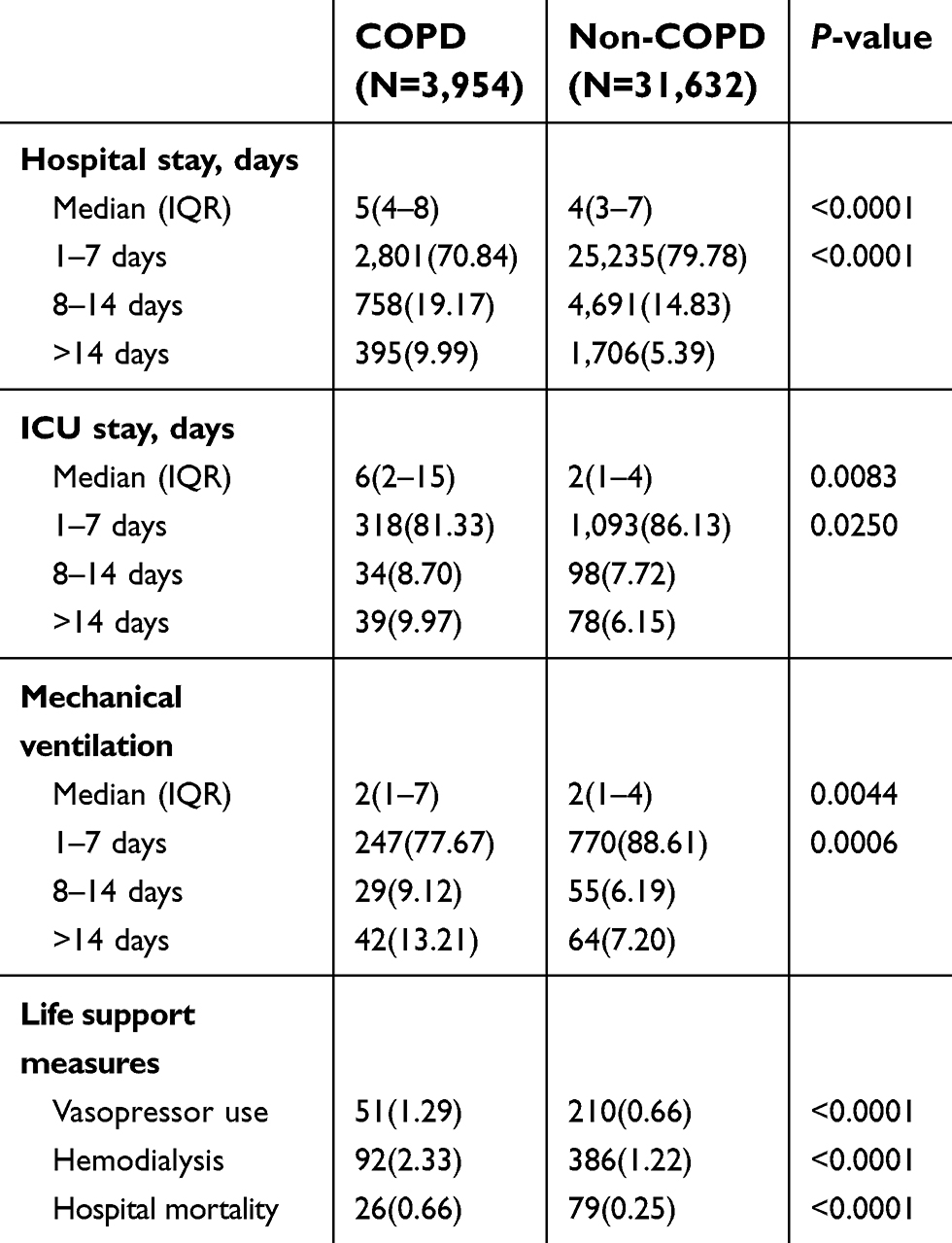 | Table 2 Resource use in the study population |
Table 3 shows the OR for adverse clinical outcomes among patients with and without COPD who underwent LC after adjusting for patient characteristics, including age, gender, income, hospital level, diabetes, hypertension, dyslipidemia, congestive heart failure, atrial fibrillation, stroke, malignancy, chronic kidney disease, peptic ulcer disease, obesity and anesthesia duration.
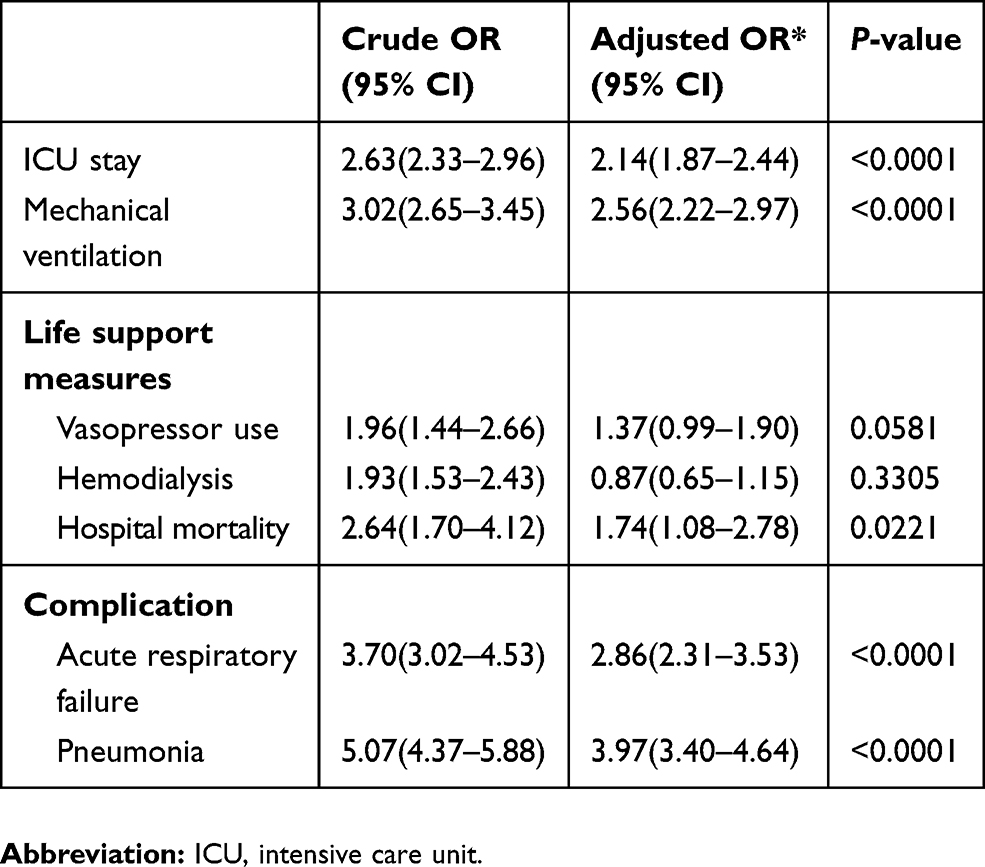 | Table 3 OR for adverse clinical outcomes for laparoscopic cholecystectomy patients with and without COPD |
COPD is a strong predictor of the length of ICU stay, duration of mechanical ventilation, acute respiratory failure and pneumonia after LC with adjusted hazard ratios and 95% CIs of 2.14 (1.87–2.44), 2.56 (2.22–2.97), 2.86 (2.31–3.53) and 3.97 (3.40–4.64), respectively.
Discussion
Our study showed that patients with COPD had a longer hospital and ICU stays, a longer duration of mechanical ventilation, increased use of life support medical resources, and increased rates of acute respiratory failure, pneumonia and mortality.
LC has become the most common and preferred method for surgery compared with open cholecystectomy. LC is associated with a smaller wound, faster operative time, less incisional pain, and faster recovery than open cholecystectomy. Although there are many advantages to laparoscopic surgery compared to open surgery, laparoscopy may not be suitable for all patients.
LC and COPD
Gramatica et al7 presented 28 COPD patients who successfully underwent LC under epidural anesthesia. Lowndes et al8 used the American College of Surgeons National Surgical Quality Improvement Program database and showed that COPD was not a significant predictor of an operative duration of >60 mins.
There are some special considerations for access in patients with umbilical hernias or prior abdominal surgery9 and obese10 or pregnant patients.11 Patients with COPD may need additional pulmonary function tests and arterial blood gas analyses. Stéphane et al12 created a preoperative score to evaluate the operative difficulty in patients undergoing LC and found that male sex, a previous cholecystitis attack, and laboratory data (fibrinogen levels, neutrophil counts, and alkaline phosphatase levels) can predict operative difficulties. However, they did not mention the impact of patient comorbidities. Lowndes et al8 identified some patient factors were related to the operative duration. In their studies, COPD, cardiovascular disease, and diabetes were not associated with the operative duration. However, their study focused on procedural difficulty and did not mention complications after surgery or utilization of medical resources. During the LC procedure, insufflation of the abdomen with carbon dioxide to displace the abdominal wall from the internal organs can reduce lung and chest wall compliance. In addition, carbon dioxide can transfer from the abdominal cavity to the circulation via peritoneal absorption and excretion from the airways. These effects may not influence the general population but may deteriorate lung function in patients with COPD and increase complications or the length of hospital stay.
Hospitalization and complications
To our knowledge, limited data are available comparing the complications and medical resource utilization between COPD and non-COPD populations. Hsieh13 enrolled 21 COPD patients, including 20 patients with mild COPD and 1 patient with moderate COPD, to compare with patients without COPD undergoing LC and showed that the operative duration and duration of hospitalization were similar in both groups. There were also no pulmonary complications reported in COPD patients.
There was a limited number of patients (21 COPD patients) included in the previous study. We enrolled 3,954 COPD patients from a nationwide database and comprehensively included COPD patients with 4 different stages of COPD (mild, moderate, severe and very severe). Our data showed that COPD patients had a longer duration of hospitalization and higher risk of pneumonia and acute respiratory failure than patients without COPD. Because of the underlying destruction of lung structure in COPD, patients with COPD were more susceptible to pneumonia and acute respiratory failure than those without COPD, and these results were also observed in our previous studies.14–16
Some studies have shown that complications were rare after LC in patients with COPD. Gramatica et al7 presented 28 COPD patients who underwent LC with epidural anesthesia. Pursnani et al17 performed LC in 6 patients with obstructive airway disease. However, they enrolled few cases in these studies, and the patients may have been specifically selected. The risks of performing LC in patients with COPD also need more meticulous attention.
PaCO2 after LC in COPD
Hsieh13 surveyed patients undergoing LC and found that the end-tidal carbon dioxide value was significantly higher in COPD patients than in those without COPD with similar ventilator settings. However, a previous study13 showed that COPD patients had similar outcomes to non-COPD patients. Previous studies have shown that the benefits of laparoscopy included an improved operative field and faster mobilization after surgery.18 During LC with carbon dioxide insufflation into the peritoneal cavity, patients with COPD exhibited an increased partial pressure of carbon dioxide (PaCO2) that reached the highest level after extubation and did not return to baseline levels.19 These physiological levels may not play an important role in the general population of patients without chronic lung disease. For patients with COPD, an increased PaCO2 that results in acidosis is a poor prognosis factor. Acidosis deteriorates hemodynamics and metabolism and increases mortality in COPD patients.20
Although our limitations included the lack of data from arterial blood gas analyses and pulmonary lung function testing, we thought that PaCO2 may increase in patients with COPD after LC and impacts on outcomes and complications. Meticulous attention should be paid in terms of preoperative evaluation, medical therapy optimization, indications for surgery and appropriate patient selection.
Limitations
There are some limitations associated with the retrospective analysis of the database performed in our study. First, the most important limitation is the lack of COPD staging among patients and, therefore, subgroup analyses. Second, we were unable to review data, including arterial blood gas analysis, pulmonary function testing, gallbladder wall thickness, body mass index and the actual onset of disease, in our database. Our results represent a comprehensive evaluation of COPD patients with varying severities of COPD. Third, the operative time in this study was estimated according to the medical expenditures from the beginning of analgesia to the recovery from analgesia and may not reflect the original data. Fourth, the reason why LC or open surgery was selected is unknown. Patients may have had contraindications for LC or economic reasons to elect a specific procedure. Therefore, selection bias may exist; however, we anticipate that this bias is similar in both COPD and non-COPD patients. Fifth, this analysis relied on the accuracy of both the procedural and diagnostic records. The diagnosis of COPD has been validated in a previous study.21 Despite these limitations, our results compared the outcomes in COPD patients who underwent LC with those of patients without COPD.
Conclusion
LC is associated with a longer duration of hospitalization and a poorer prognosis in COPD patients than in non-COPD patients. Given the increased prevalence of COPD and longevity, safer surgical approaches may be of considerable benefit to this population. As age and comorbidities increase, physicians need an appropriate diagnosis and treatment of COPD prior to LC, considering the higher postoperative complication rate in this subgroup of patients.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lamberts MP. Indications of cholecystectomy in gallstone disease. Curr Opin Gastroenterol. 2018;34(2):97–102. doi:10.1097/MOG.0000000000000419
2. Legorreta AP, Silber JH, Costantino GN, et al. Increased cholecystectomy rate after the introduction of laparoscopic cholecystectomy. Jama. 1993;270:1429–1432. doi:10.1001/jama.1993.03510120051029
3. Zacks SL, Sandler RS, Rutledge R, Brown RS
4. Yang TF, Guo L, Wang Q. Evaluation of preoperative risk factor for converting laparoscopic to open cholecystectomy: a meta-analysis. Hepatogastroenterology. 2014;61(132):958–965.
5. Bayrak M, Altıntas Y. Comparing laparoscopic cholecystectomy in patients with chronic obstructive pulmonary disease under spinal anesthesia and general anesthesia. BMC Surg. 2018;18(1):65. doi:10.1186/s12893-018-0396-1
6. Hennessy S, Bilker WB, Berlin JA, Strom BL. Factors influencing the optimal control-to-case ratio in matched case-control studies. Am J Epidemiol. 1999;149(2):195–197.
7. Gramatica L
8. Lowndes B, Thiels CA, Habermann EB, Bingener J, Hallbeck S, Yu D. Impact of patient factors on operative duration during laparoscopic cholecystectomy: evaluation from the National Surgical Quality Improvement Program database. Am J Surg. 2016;212(2):289–296. doi:10.1016/j.amjsurg.2016.01.024
9. AUJansen FW, Kapiteyn K, Trimbos-Kemper T, Hermans J, Trimbos JBS. Complications of laparoscopy: a prospective multicentre observational study. J Obstet Gynaecol. 1997;104(5):595. doi:10.1111/j.1471-0528.1997.tb11539.x
10. AULamvu G, Zolnoun D, Boggess J, Steege JFS. Obesity: physiologic changes and challenges during laparoscopy. J Obstet Gynecol. 2004;191(2):669. doi:10.1016/j.ajog.2004.05.077
11. AUHärkki-Sirén P, Kurki TSO. A nationwide analysis of laparoscopic complications. Obstet Gynecol. 1997;89(1):108. doi:10.1016/S0029-7844(96)00390-0
12. Bourgouin S, Mancini J, Monchal T, Calvary R, Bordes J, Balandraud P. How to predict difficult laparoscopic cholecystectomy? Proposal for a simple preoperative scoring system. Am J Surg. 2016;212(5):873–881. doi:10.1016/j.amjsurg.2016.04.003
13. Hsieh CH. Laparoscopic cholecystectomy for patients with chronic obstructive pulmonary disease. J Laparoendosc Adv Surg Tech A. 2003;13(1):5–9. doi:10.1089/109264203321235395
14. Liao KM, Lu HY. Complications after total knee replacement in patients with chronic obstructive pulmonary disease: anationwide case-control study. Medicine (Baltimore). 2016;95(37):e4835. doi:10.1097/MD.0000000000004864
15. Liao KM, Lu HY. A national analysis of complications following total hip replacement in patients with chronic obstructive pulmonary disease. Medicine (Baltimore). 2016;95(12):e3182. doi:10.1097/MD.0000000000004864
16. Ho CH, Chen YC, Chu CC, Wang JJ, Liao KM. Postoperative complications after coronary artery bypass grafting in patients with chronic obstructive pulmonary disease. Medicine (Baltimore). 2016;95(8):e2926. doi:10.1097/MD.0000000000004864
17. Pursnani KG, Bazza Y, Calleja M, Mughal MM. Laparoscopic cholecystectomy under epidural anesthesia in patients with chronic respiratory disease. Surg Endosc. 1998;12(8):1082–1084.
18. Lai JH, Law WL. Laparoscopic surgery for colorectal cancer. Br Med Bull. 2012;104:61–89. doi:10.1093/bmb/lds026
19. Ozyuvaci E, Demircioglu O, Toprak N, Topacoglu H, Sitilci T, Akyol O. Comparison of transcutaneous, arterial and end-tidal measurements of carbon dioxide during laparoscopic cholecystectomy in patients with chronic obstructive pulmonary disease. J Int Med Res. 2012;40(5):1982–1987. doi:10.1177/030006051204000540
20. Bruno CM, Valenti M. Acid-base disorders in patients with chronic obstructive pulmonary disease: a pathophysiological review. J Biomed Biotechnol. 2012;2012:915150. doi:10.1155/2012/915150
21. Ho TW, Ruan SY, Huang CT, Tsai YJ, Lai F, Yu CJ. Validity of ICD9-CM codes to diagnose chronic obstructive pulmonary disease from National Health Insurance claim data in Taiwan. Int J Chron Obstruct Pulmon Dis. 2018;13:3055–3063. doi:10.2147/COPD.S174265
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.