Back to Journals » Clinical Ophthalmology » Volume 14
Outcomes of Epiretinal Membrane Removal Utilizing Triamcinolone Acetonide Visualization and Internal Limiting Membrane Forceps
Authors Asahi MG ![]() , Wallsh JO, Gallemore RP
, Wallsh JO, Gallemore RP
Received 31 August 2020
Accepted for publication 2 November 2020
Published 17 November 2020 Volume 2020:14 Pages 3913—3921
DOI https://doi.org/10.2147/OPTH.S279611
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Masumi G Asahi, Josh O Wallsh, Ron P Gallemore
Retina Macula Institute, Torrance, CA, USA
Correspondence: Ron P Gallemore
Retina Macula Institute, 4201 Torrance Boulevard, Suite 220, Torrance, CA, USA
Tel +1 310 944-9393
Fax +1 310 944-3393
Email [email protected]
Purpose: To evaluate epiretinal membrane (ERM) removal utilizing internal limiting membrane (ILM) forceps and visualization with triamcinolone acetonide (TA).
Methods: Retrospective interventional case series of eyes undergoing ERM removal with TA visualization with follow-up of up to five years. Best-corrected visual acuity (BCVA), central macular thickness (CMT), and incidence of complications were reviewed.
Results: A total of 132 eyes were included with 54 and 16 eyes completing 3- and 5-year follow-up, respectively. Mean BCVA and CMT improved significantly at all postoperative evaluations compared to baseline (p< 0.001). Pre-operative presence of PVD did not affect outcome measures. No intraoperative complications were reported. Immediate post-operative complications included one case of sterile endophthalmitis and one case of vitreous and perimacular hemorrhage. At one year, complications included progression of cataract in phakic eyes (65.4%), steroid-induced glaucoma (2.2%), retinal tear (0.8%), recurrent ERM (4.5%), and recurrent macular edema (11.3%). No further complications were reported at three- and five-year follow-up.
Conclusion: Combination ILM forceps and TA visualization offers an affordable and safe option for ERM removal with comparable or better outcomes than traditional methods of ERM surgery.
Keywords: chromovitrectomy, epiretinal membrane, triamcinolone acetonide
Introduction
An epiretinal membrane (ERM), also known as a macular pucker, is a fibrocellular tissue that proliferates on the surface of the internal limiting membrane (ILM). It can be idiopathic or secondary to retinal tear or detachment, trauma, intraocular surgery, ocular inflammatory diseases, or retinal vascular disorders such as diabetic retinopathy or retinal vein occlusion.1 Although many patients with ERMs can be asymptomatic, they can also cause blurred vision and metamorphopsia.1,2
ERM surgery is perhaps the most common vitreoretinal procedure performed. It involves removing the fibrocellular tissue from the retinal surface with or without the ILM.2 In recent years, there is a movement towards using dyes to stain the retinal surface to facilitate the procedure. Trypan blue (Tb), brilliant blue G (BBG), and now less commonly, indocyanine green (ICG) have been utilized for this purpose.3–5 There are concerns about toxicity with some of these agents.6–8
We report the largest case series to date utilizing intravitreal triamcinolone acetonide (TA) for visualization of ERM and membrane peeling with ILM forceps. The aim of this study is to report outcomes including best corrected visual acuity (BCVA), change in central macular thickness (CMT) on optical coherence tomography (OCT), and complications at one, three, and five years following surgery.
Methods
This retrospective interventional case series included all patients who underwent pars plana vitrectomy (PPV) for ERM with TA visualization and membrane peel with ILM forceps between January 2014 and January 2019 by a single physician (R.P.G.). Each patient received a complete ophthalmologic exam including BCVA and spectral domain-optical coherence tomography (Cirrus; Carl Zeiss Meditec AG, Jena, Germany) pre- and post-operatively. Patients were followed at one, three, six, twelve, thirty-six, and sixty months post-operatively. Fluorescein angiography (FA) was performed pre- and post-operatively in most cases.
This study was performed in accordance with the tenants of the Declaration of Helsinki and IRB exempt status was obtained by the Sterling IRB (IRB ID: 0877-RPGallemore). Written and informed consent was obtained from patients for publication of their cases and any accompanying images. Individual health information remained protected, and data confidentiality was maintained throughout the collection of data and writing of this article according to the Health Insurance Portability and Accountability Act (HIPPA) Privacy Rule and Security Rule.
Procedure
A standard 23-gauge three port vitrectomy technique was utilized to peel ERMs and the underlying ILM. After a quarter vitrectomy involving removal of the central vitreous and Weiss ring, and in some cases, creation of a posterior vitreous detachment (PVD), TA (TRIESENCE, Alcon Laboratories Inc., Fort Worth, TX) was applied to the retinal surface using a 25-gauge five eighths inch needle bevel down towards the retinal surface. Enough was used to cover the macula from arcade to arcade, then allowed to sit for moments, and aspirated off the retinal surface, leaving some granules behind. ILM forceps were then utilized to engage the retinal surface and pull back the ERM. TA was then added back, aspirated once again, and the underlying ILM was peeled away from arcade to arcade. Both the ERM and ILM were removed from the eye. Periphery was inspected with scleral depression to look for any new tears or detachments and treated with endolaser when required.
Study Assessments
Patients were examined pre-operatively, postoperatively day one and months one, three, six, and twelve in addition to years 3 and 5. During each visit, patients were examined with a complete ophthalmologic examination including assessment of BCVA and intraocular pressure (IOP). Additional testing including OCT imaging and, when indicated, fluorescein angiography (FA) were performed at follow-up visits. BCVA was assessed with the Snellen eye chart. Average CMT was calculated as the average of the foveal and four perifoveal ETDRS subfields within the 3mm circle displayed on OCT retinal thickness maps. Recurrent ME was defined as development of intraretinal cysts on OCT images or leakage seen on FA.
Statistical Analysis
All data were recorded on Microsoft Excel and statistical analysis was performed using Data Analysis Toolpak software. All snellen visual acuity values were converted to the logarithm of the minimum angle of resolution (logMAR). Patients who completed at least twelve months of follow up were included for analysis of baseline demographics, complications, and change in BCVA and CMT. Changes after surgery were determined as the difference between preoperative values and postoperative values at months one, three, six, and twelve, and years three and five. A paired Student’s t-test was used to compare preoperative to postoperative BCVA and CMT. A p-value of <0.05 was considered statistically significant.
Results
Of 142 identified eyes, 132 (92%) were included for analysis. Mean age was 67.7±11.4 years. Idiopathic ERMs were found in 62 (46.9%) eyes and secondary ERMs in 70 (53.1%) eyes (Table 1). 92% (n=132) completed 1 year follow up, 38% (n=54) completed 3-year follow up, and 11% (n=16) completed 5-year follow up.
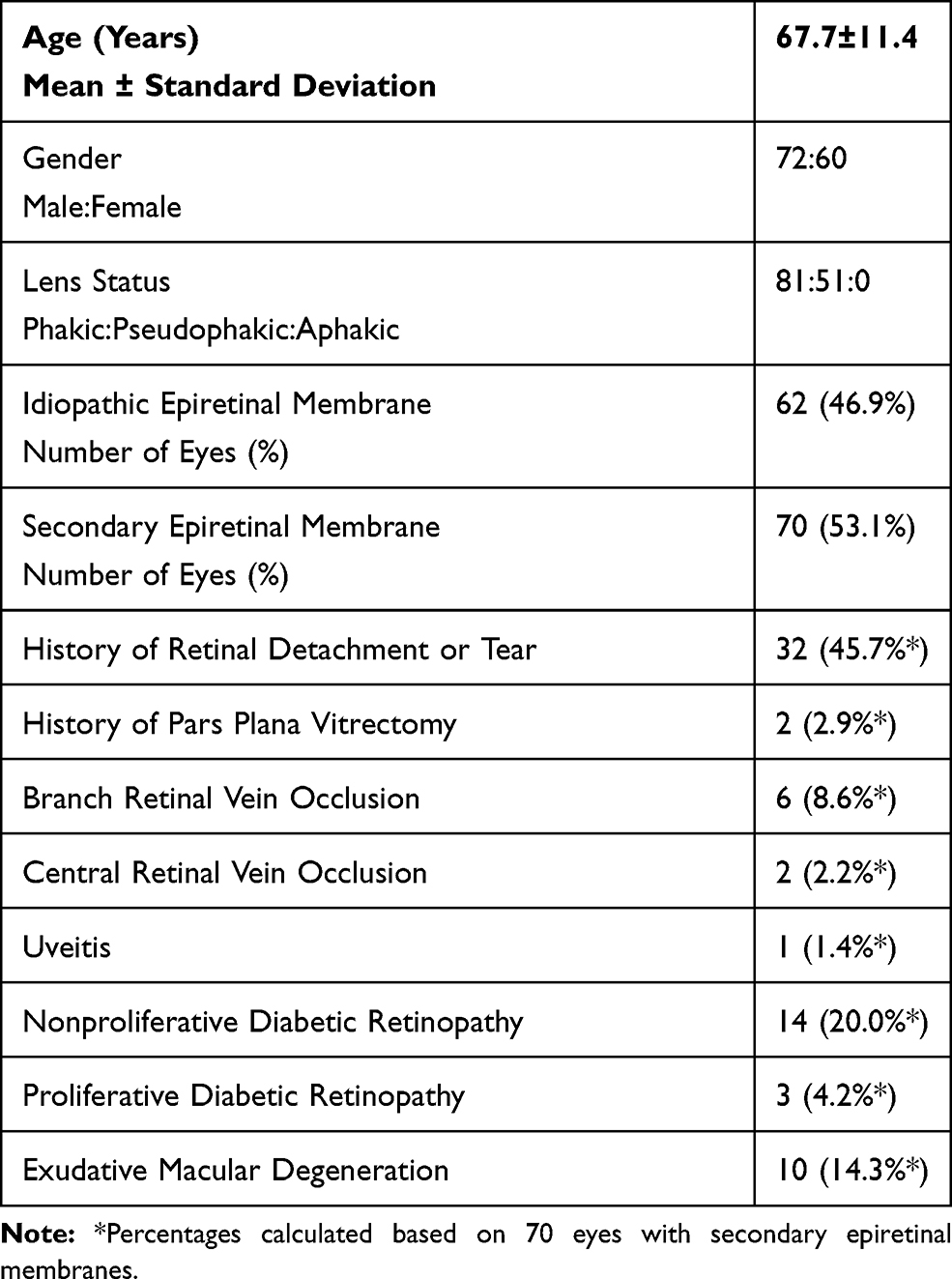 |
Table 1 Baseline Demographics |
BCVA and Average CMT
Mean pre-operative BCVA was 0.579± 0.417 logMAR (Snellen 20/75) and CMT 414.6±69.3 micrometers. At 1-year post-operative BCVA improved by a mean 0.275±0.033 logMAR (p<0.001) and CMT decreased by a mean of 70.5±7.8 micrometers (p<0.001). Similar statistically significant improvements were noted at months 1, 3, 6, 12, 36, and 60 (p<0.05, Figures 1 and 2).
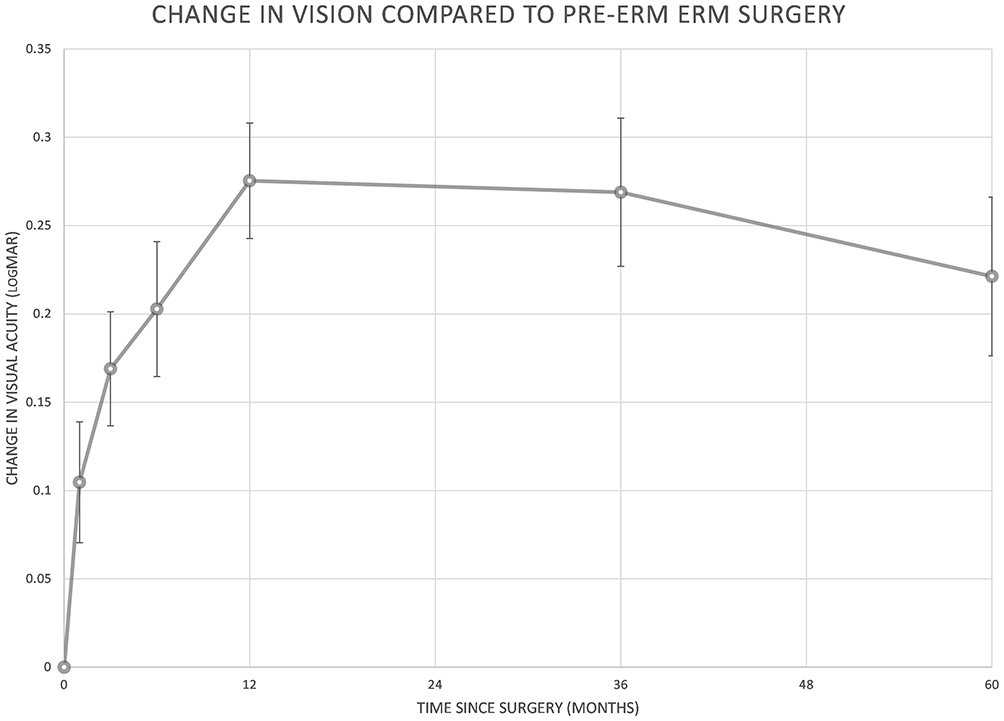 |
Figure 1 Mean change in best corrected visual acuity (BCVA) compared to preoperative BCVA at months one, three, six, twelve, thirty six, and sixty. Error bars represent the standard error of the mean value (SEM). Statistically significant improvements occurred at each month of follow-up (p<0.05). |
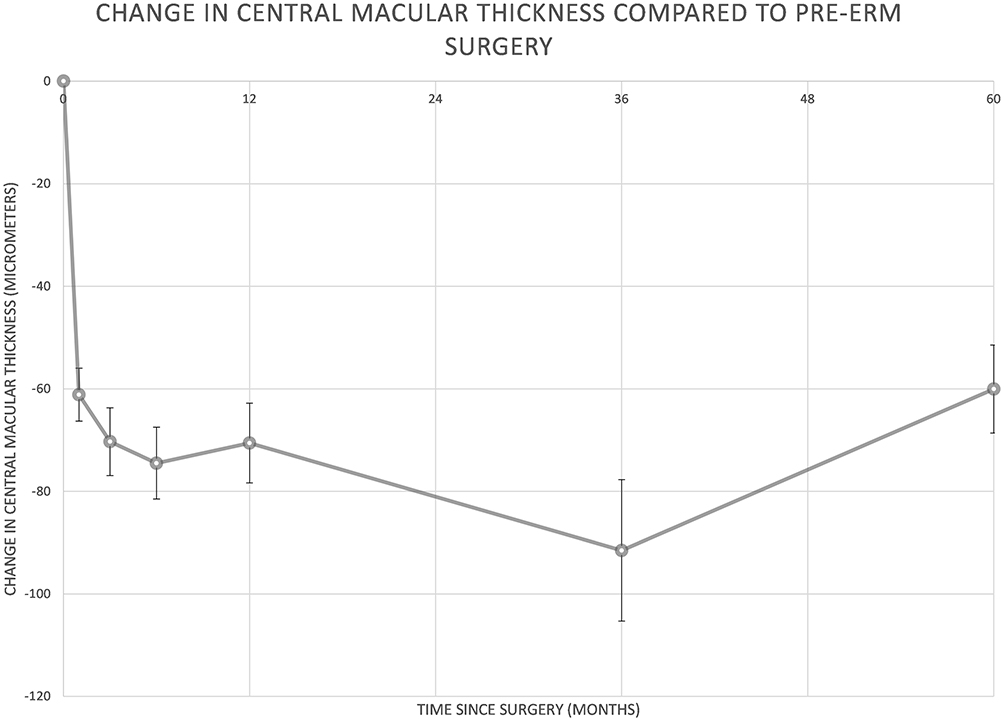 |
Figure 2 Mean change in central macular thickness (CMT) compared to preoperative CMT at months one, three, six, twelve, thirty six, and sixty. Error bars represent the standard error of the mean value (SEM). Statistically significant improvements occurred at each month of follow-up (p<0.05). |
Patients without PVD (n=51) had a mean preoperative BCVA of 0.653±0.409 logMAR with CMT of 470.7±96.2 micrometers and patients with PVD (n=81) had mean pre-operative BCVA of 0.470+/0.303logMAR with CMT of 454.9±75.9 micrometers. At one year, patients without PVD had BCVA 0.402±0.364 logMAR with CMT 367.8±50.0 microns and patients with PVD had BCVA 0.165±0.219 logMAR with CMT 387.3±53.8 microns. There was a statistically significant difference in pre-operative BCVA (P<0.001) and BCVA at one year (p≪0.001) between the two groups. There was not a significant difference in change in BCVA and CMT from preoperative to final postoperative visit between eyes with PVD compared to eyes without PVD (Figures 3 and 4).
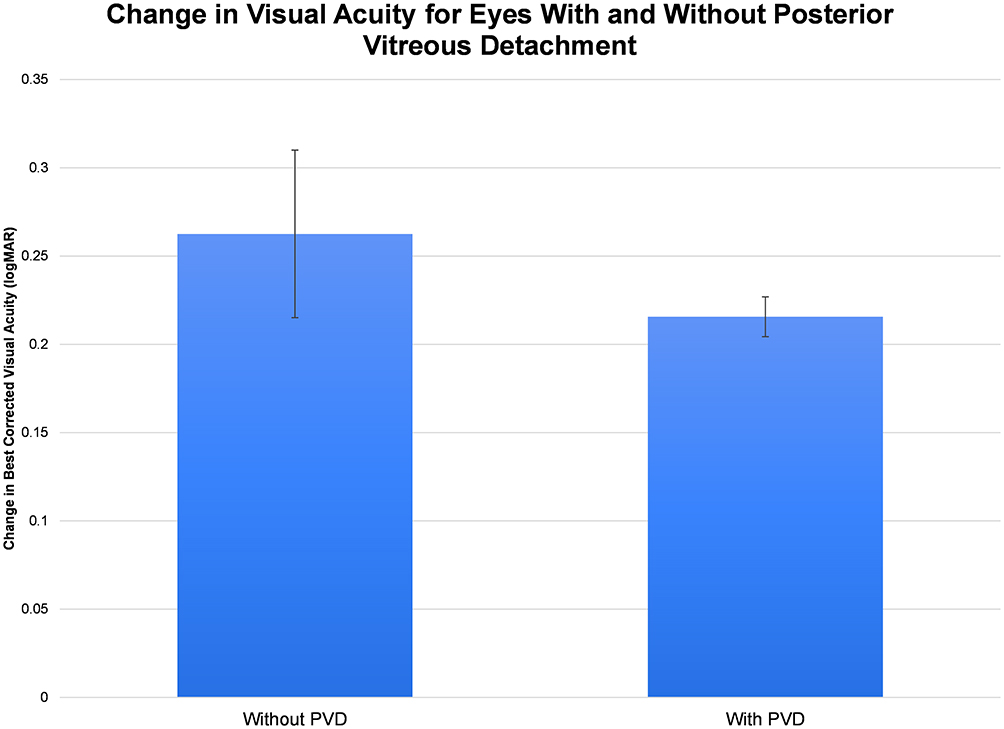 |
Figure 3 Change in best-corrected visual acuity from preoperative to final postoperative visit in eyes with and without preoperative posterior vitreous detachments (PVDs). Differences were not statistically (p=0.44). |
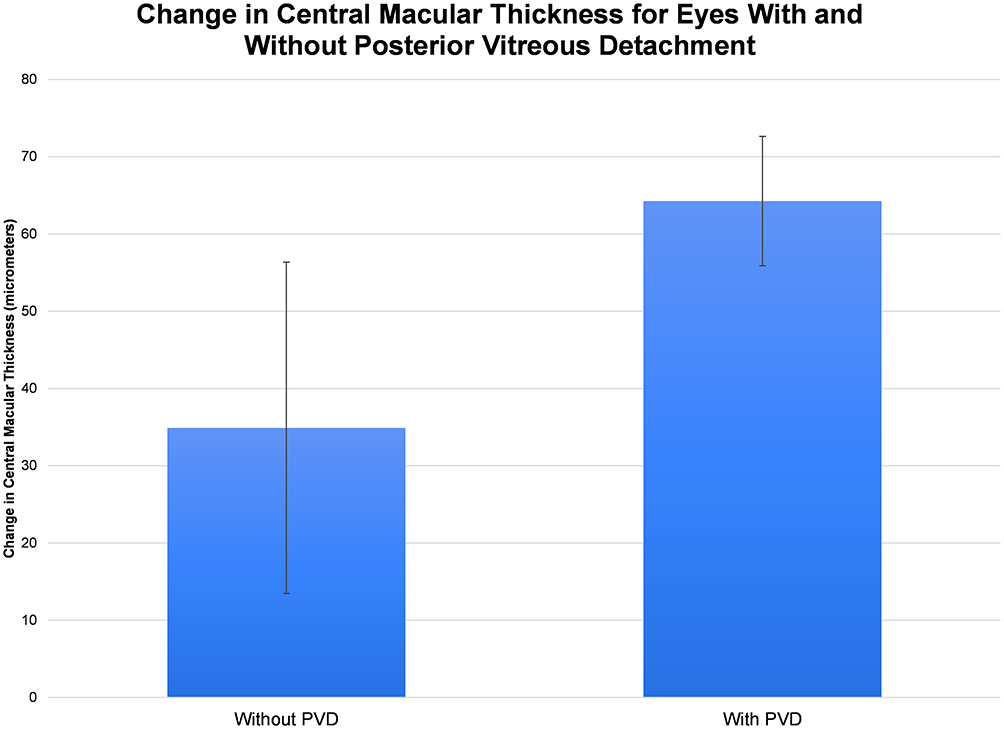 |
Figure 4 Change in central macular thickness from preoperative to final postoperative visit in eyes with and without preoperative posterior vitreous detachments (PVDs). Differences were not statistically significant (p=0.20). |
Complications
No intraoperative complications were reported. Immediate post-operative complications included 1 case of sterile endophthalmitis presumptively treated with intravitreal antibiotics but vitreous tap was without microorganism growth. Another case developed vitreous and premacular hemorrhage immediately postoperatively in a patient who had forgotten to discontinue aspirin and plavix prior to surgery.
Cataract progression was seen in 53 phakic eyes (65.4%) with 32 (60.0%) undergoing surgery. The majority of these occurred within the first year following surgery. 4.5% (n=6) developed recurrent ERM and 11.3% (n=15) developed recurrent ME post-operatively. Three (2.2%) eyes developed steroid-induced glaucoma which was successfully managed medically in all cases (Table 2).
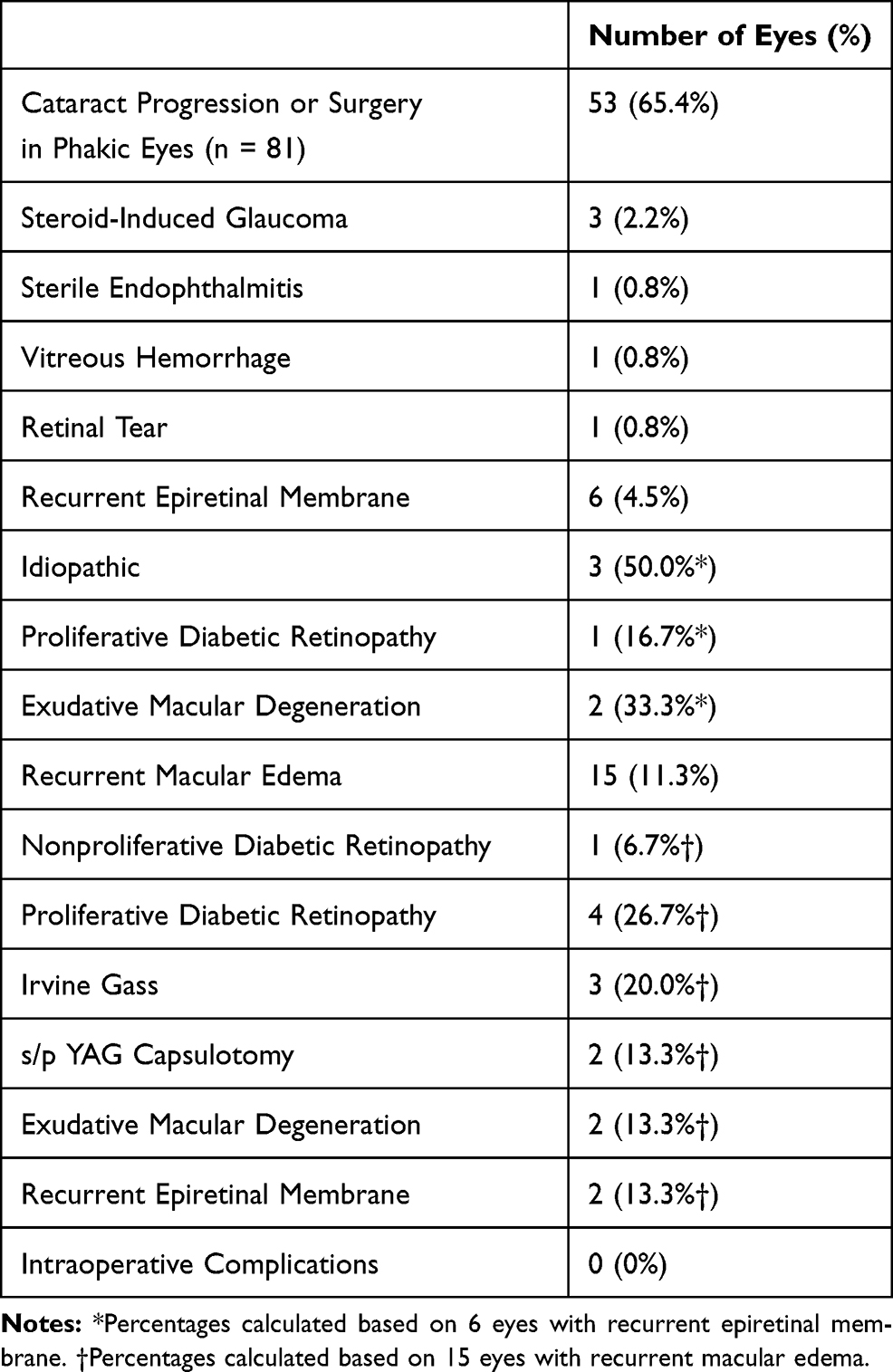 |
Table 2 Complications |
Discussion
We demonstrated that TA can facilitate visualization of the ERM and ILM with outcomes equal to or better than ERM surgery with traditional methods of staining.2,9–14
There was a statistically significant improvement in both BCVA and CMT at all postoperative time points. Although preoperative values are highly varied among prior studies, they all demonstrated similar improvements with one year postoperative vision ranging between 0.180 and 0.690 logMAR (Snellen 20/30 to 20/100) and CMT 268–375µm.9,10,13–15 BCVA at five years was 0.109±0.029 logMAR (Snellen 20/25), which is better than another study reporting outcomes of ERM surgery with ICG visualization (0.449±0.487logMAR; Snellen 20/60).2 Dawson et al demonstrated that surgical intervention on patients with better preoperative BCVA yields a better final BCVA and patients with poorer preoperative BCVA showed a greater change in BCVA following ERM surgery.10 This may account for the greater postoperative BCVA in the 5-year follow-up group as their mean preoperative BCVA was 0.33 logMAR (Snellen 20/40). It is important to note that given the patients' associated macular edema with these patients’ underlying condition, all were maintained on topical anti-inflammatory drops with few on topical steroids, and often in combination with antiglaucoma drops, pre- and post-operatively, which may confound these results in our study cohort.
Despite having similar preoperative CMT values, eyes with PVD were found to have a significantly better preoperative BCVA compared to eyes without PVD (p<0.001). BCVA one year post-operatively in the PVD group was also significantly better than eyes without PVD (p≪0.001), likely due to the better pre-operative BCVA in the eyes with PVD compared to the eyes without PVD. Both groups showed similar trends in improvement in BCVA and CMT postoperatively at one year and final visit, suggesting that creation of a PVD intra-operatively does not affect visual or anatomic outcomes as measured by BCVA and CMT.
Interestingly, no intraoperative retinal tears were noted in our study, which has been reported to be as high as 6% in one study and 8.9% in eyes being operated on with dyes.10,13 These findings are consistent with a multicentered controlled clinical trial that demonstrated eyes undergoing PPV with TA showed a reduced incidence of intraoperative complications including retinal detachment and retinal breaks compared to eyes undergoing traditional PPV without dyes.16 However, it is important to note that the results in our study were obtained from one surgeon and similar surgical techniques in other hands may demonstrate different intraoperative results.
There is also concern for cataract formation, glaucoma, and endophthalmitis with the use of steroids. In our study, cataract progression was the most common finding (65.4% in phakic eyes) with rates comparable to other studies ranging from 28%-89%.10,12–14 There was one case of sterile endophthalmitis in our study. One study found only one case of acute endophthalmitis due to S. epidermidis in 1886 cases of TA-assisted PPV, suggesting that TA is not a high-risk factor for acute endophthalmitis.17 We reported three cases of steroid-induced glaucoma, which was controlled with antiglaucoma drops. Another study found antiglaucoma eye drops were required more frequently after TA-assisted PPV than after conventional PPV without dyes, but IOP was well controlled in both groups.18 ERM in our study was within the range of previous reports of 5–12%, although one study reported recurrence as high as 58% at 5-year follow-up.19,20
Chromovitrectomy
The use of dyes to improve the poor intra-operative visibility of the ERM and ILM is increasingly seen in practice. In addition to improving visualization, dyes can help with shortening the duration of surgery and can minimize retinal trauma during ERM removal. Each dye offers different advantages and risks.
ICG was utilized early in chromovitrectomy visualization due to intensity of staining and ease of ILM removal, but its use can be complicated by retinal toxicity including retinal pigment epithelial damage, optic nerve atrophy, visual field defects and decreased multifocal electroretinographic responses.3,7,8 Due to its packaging as a lyophilized powder, ICG will not dissolve in intraocular irrigation solution alone and requires dilution which can be tedious to both prepare and remove from the eye.4 Tb emerged as the alternative to ICG, but has also been associated with retinal toxicity and requires an air-fluid exchange before application.4,5 BBG was later introduced as the most promising alternative to ICG and Tb.4 These granules can easily be dissolved in intraocular irrigating solution alone and ILM staining patterns are similar to that of ICG solution with little possibility of light toxicity.5 Although rare, BBG has also been associated with macular toxicity in a few cases.6 Comparative studies have found BBG to be superior to TB and similar to ICG in terms of staining and ease of ILM removal.4,5
Interestingly, TA was the first FDA-approved agent for chromovitrectomy and despite its limited use in recent years, there is still a role for TA visualization in ERM surgery. TA has been used in PPV and found to have outcomes similar to conventional PPV and has been well documented for visualization.18,21,22 Unlike the dyes, TA can be utilized in visualization of the vitreous, ERM, and ILM. In vitreous visualization, the crystals become trapped in the vitreous gel with the suspension allowing for good contrast between the whitened vitreous and the post-hyaloid space. This allows ease of removal of vitreous and hyaloid membrane, which if left behind may provide scaffolding for fibrovascular proliferation and lead to a recurrent ERM or may provide a foundation of traction that can precipitate a macular hole or vitreomacular traction.23,24
Advantages of TA visualization compared to other agents include ease of use given its readiness for immediate use without need for dilution or preparation, no reported retinal toxicity in doses of 2 to 4mg, and no requirement for an air-fluid exchange.25 TA coats the surface of ERMs and ILMs and integrates into their superficial collagen fibrils compared to the dyes, which stain the membranes.24,26,27 This allows any remaining TA particles to be removed from the eye with aspiration or irrigation. TA is also less likely to make the view hazy if there is disbursement of the agent.
It is often injected following PPV to treat ME and inflammation in various retinal diseases and uveitis, which may offer an additional benefit in the treatment of postoperative CME following ERM removal. TA has also been shown to reduce post-operative inflammation and inhibit the postoperative breakdown of the blood-ocular barrier when utilized in conjunction with PPV.28,29 Microscopic granules left behind following aspiration of TA could contribute to improved outcomes in these patients.
The use of TA use does not come without disadvantages. TA is a steroid, which is known to be associated with cataract progression and intraocular pressure elevation. The coating ability of TA may limit the ability to discriminate residual ILM from ILM defects following ERM removal. A case series demonstrated incomplete removal of perifoveal ILM in 29% of cases undergoing ILM removal with TA and subsequent ICG to assess the status of the remaining ILM.30 The residual ILM can serve as a scaffold for recurrent ERM formation.31 There has been a move away from the use of TA in recent years with the argument that vital dyes more accurately stain the ERM and differentiate the ILM. This has not been our experience. The consistency of the ILM visualized with TA is clearly distinct from the ERM and an experienced surgeon with understanding of the retinal anatomy should have no difficulty differentiating.
Limitations
This retrospective study has several limitations. In addition to its retrospective nature, the study did not utilize a control arm and cannot state with certainty the advantages or disadvantages of TA visualization over other agents. Future studies that compare outcomes of ERM surgery with different visualization agents may be able to further elucidate the differences in outcomes intra-operatively and post-operatively.
Conclusion
Combination ILM forceps and TA visualization offers an affordable option for ERM removal with comparable or better outcomes than traditional methods of ERM surgery. We demonstrated that there is a reduced incidence of intraoperative complications with TA in PPV for ERM, which is consistent with prior studies.18,32 Complications at one year post-operatively were consistent with prior reports and we saw no further complications at three and five years post-operatively with statistically significant improvement in BCVA and CMT at all time points post-operatively.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sheard RM, Sethi C, Gregor Z. Acute macular pucker. Ophthalmology. 2003;110(6):1178–1184. doi:10.1016/S0161-6420(03)00266-5
2. Sultan H, Wykoff CC, Shah AR. Five-year outcomes of surgically treated symptomatic epiretinal membranes with and without internal limiting membrane peeling. Ophthalmic Surg Lasers Imaging Retina. 2018;49(5):
3. Schumann RG, Gandorfer A, Priglinger S, et al. Vital dyes for macular surgery: a comparative electron microscopy study of the internal limiting membrane. Retina. 2009;29(5):669–676. doi:10.1097/IAE.0b013e318196b1c8
4. Shukla D, Kalliath J, Neelakantan N, et al. A comparison of brilliant blue G, trypan blue, and indocyanine green dyes to assist internal limiting membrane peeling during macular hole surgery. Retina. 2011;31(10):2021–2025. doi:10.1097/IAE.0b013e318213618c
5. Kagimoto HT, Hisatomi T, Enaida H, Ishibashi T. Brilliant Blue G for ILM staining and peeling. Retina Surg Global Perspectives. 2011;45–48.
6. Jindal A, Pathengay A, Mithal K, et al. Macular toxicity following brilliant blue G-assisted macular hole surgery – a report of three cases. Nepal J Ophthalmol. 2014;6(11):98–101. doi:10.3126/nepjoph.v6i1.10779
7. Rodrigues EB, Meyer CH, Mennal S, Farah ME. Mechanisms of intravitreal toxicity of indocyanine green dye: implications for chromovitrectomy. Retina. 2007;27(7):958–970. doi:10.1097/01.iae.0000253051.01194.ab
8. Ferencz M, Somfai GM, Farkas A, et al. Functional assessment of the possible toxicity of indocyanine green dye in macular hole surgery. Am J Ophthalmol. 2006;142(5):765–770. doi:10.1016/j.ajo.2006.05.054
9. Guber J, Pereni I, Scholl HPN, et al. Outcomes after epiretinal membrane surgery with or without internal limiting membrane peeling. Ophthalmol Ther. 2019;8(2):
10. Dawson SR, Shunmugam M, Williamson TH. Visual acuity outcomes following surgery for idiopathic epiretinal membrane: an analysis of data from 2001 to 2011. Eye. 2014;28(2):219–224. doi:10.1038/eye.2013.253
11. Michels RG. Vitreous surgery for macular pucker. Am J Ophthalmol. 1981;92(5):
12. Pielen A, Guerra NI, Böhringer D, et al. Intra- and postoperative risks and complications of small-gauge (23-G) versus conventional (20-G) vitrectomy for macular surgery. Eur J Ophthalmol. 2014;24(5):
13. Wong JG, Sachdev N, Beaumont PE, Chang AA. Visual outcomes following vitrectomy and peeling of epiretinal membrane. Clin Exp Ophthalmol. 2005;33(4):
14. Reilly G, Melamud A, Lipscomb P, Toussaint B. Surgical outcomes in patients with macular pucker and good preoperative visual acuity after vitrectomy with membrane peeling. Retina. 2015;35(9):
15. Gotzaridis SV, Mela VA. Long term outcomes after pars plana vitrectomy for the treatment of epiretinal membranes. Adv Ophthalmol Vis Syst. 2016;5(3):256–260. doi:10.15406/aovs.2016.05.00156
16. Yamakiri K, Sakamoto T, Noda Y, et al. Reduced incidence of intraoperative complications in a multicenter controlled clinical trial of triamcinolone in vitrectomy. Ophthalmology. 2007;114(2):289–296. doi:10.1016/j.ophtha.2006.07.044
17. Sakamoto T, Enaida H, Kubota T, et al. Incidence of acute endophthalmitis after triamcinolone-assisted pars plana vitrectomy. Am J Ophthalmol. 2004;138(1):
18. Yamakiri K, Sakamoto T, Noda Y, et al. One-year results of a multicenter controlled clinical trial of triamcinolone in pars plana vitrectomy. Graefes Arch Clin Exp Ophthalmol. 2008;246(7):959–966. doi:10.1007/s00417-008-0829-0
19. Sandali O, El Sanharawi M, Basli E, et al. Epiretinal membrane recurrence: incidence, characteristics, evolution, and preventive and risk factors. Retina. 2013;33(10):2032–2038. doi:10.1097/IAE.0b013e31828d2fd6
20. Fleissig E, Zur D, Moisseiev E, et al. Five-year follow-up after epiretinal membrane surgery: a single-center experience. Retina. 2018;38(7):1415–1419. doi:10.1097/IAE.0000000000001711
21. Horio N, Horiguchi M, Yamamoto N. Triamcinolone-assisted internal limiting membrane peeling during idiopathic macular hole surgery. Arch Ophthalmol. 2005;123:96–99. doi:10.1001/archopht.123.1.96
22. Kumagai K, Furukawa M, Ogino N, et al. Long-term outcomes of macular hole surgery with triamcinolone acetonide-assisted internal limiting membrane peeling. Retina. 2007;27:1249–1254. doi:10.1097/IAE.0b013e3180ed45cc
23. Doi N, Uemura A, Nakao K, Sakamoto T. Vitreomacular adhesion and the defect in posterior vitreous cortex visualized by triamcinolone-assisted vitrectomy. Retina. 2005;25((6):):742–745. doi:10.1097/00006982-200509000-00009
24. Gandorfer A, Haritoglou C, Scheler R, et al. Residual cellular proliferation on the internal limiting membrane in macular pucker surgery. Retina. 2012;32:477–485. doi:10.1097/IAE.0b013e3182246e2a
25. Peyman GA, Cheema R, Conoway MD, Fang T. Triamcinolone acetonide as an aid to visualization of the vitreous and the posterior hyaloid during pars plana vitrectomy. Retina. 2000;20(5):554–555. doi:10.1097/00006982-200005000-00024
26. Messmer EM, Heidenkummer HP, Kampik A. Ultrastructure of epiretinal membranes associated with macular holes. Graefes Arch Clin Exp Ophthalmol. 1998;236:248–254. doi:10.1007/s004170050072
27. Smiddy WE, Michels RG, de Bustros S, et al. Histopathology of tissue removed during vitrectomy for impending idiopathic macular holes. Am J Ophthalmol. 1989;108(4):360–364. doi:10.1016/S0002-9394(14)73301-X
28. Takamura Y, Shimura M, Katome T, et al. Effect of intravitreal triamcinolone acetonide injection at the end of vitrectomy for vitreous haemorrhage related to proliferative diabetic retinopathy. Br J Ophthalmol. 2018;102(10):1351–1357. doi:10.1136/bjophthalmol-2017-311377
29. Sakamoto T, Miyazaki M, Hisatomi T, et al. Triamcinolone-assisted pars plana vitrectomy improves the surgical procedures and decreases the postoperative blood-ocular barrier breakdown. Graefe’s Arch Clin Exp Ophthalmol. 2002;240(6):423–429. doi:10.1007/s00417-002-0454-2
30. Tabandeh H, Boyer H, Liao D. Triamcinolone Acetonide (TA) assisted removal of Internal Limiting Membrane (ILM). Invest Ophthalmol Vis Sci. 2013;54(15):3341.
31. Shimada H, Nakashizuka H, Hattori T, et al. Double staining with brilliant blue G and double peeling for epiretinal membranes. Ophthalmology. 2009;116(7):1370–1376. doi:10.1016/j.ophtha.2009.01.024
32. Couch SM, Bakri SJ. Use of triamcinolone during vitrectomy surgery to visualize membranes and vitreous. Clin Ophthalmol. 2008;2(4):891–896. doi:10.2147/opth.s3434
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.