Back to Journals » International Journal of Women's Health » Volume 18
Outcomes and Risk Factors for Failed Trial of Labour After One Previous Caesarean Section in Selected Private Hospitals in Mogadishu, Somalia: An Unmatched Case-Control Study
Authors Adawe MMM, Ibrahim FH ![]() , Garba B, Mudei NM
, Garba B, Mudei NM ![]() , Mohamoud JH
, Mohamoud JH ![]() , Elmi AH
, Elmi AH ![]()
Received 4 February 2026
Accepted for publication 20 March 2026
Published 25 March 2026 Volume 2026:18 595847
DOI https://doi.org/10.2147/IJWH.S595847
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Mariam Mohamed Mohamud Adawe,1 Fahmo Hussein Ibrahim,1 Bashiru Garba,2 Nasteho Mohamud Mudei,1 Jamal Hassan Mohamoud,3 Abdullahi Hassan Elmi4
1Department of Obstetrics & Gynecology, Dr Sumait hospitals, SIMAD University, Mogadishu, Somalia; 2SIMAD Institute for Global Health, SIMAD University, Mogadishu, Somalia; 3Department of Public Health, Faculty of Medicine and Health Sciences, SIMAD University, Mogadishu, Somalia; 4Department of Nursing and Midwifery, Dr Sumait Hospital, Faculty of Medicine and Health Sciences, SIMAD University, Mogadishu, Somalia
Correspondence: Mariam Mohamed Mohamud Adawe, Email [email protected]
Background: Trial of labour after caesarean section (TOLAC) is an important strategy for reducing repeat caesarean deliveries among appropriately selected women. However, failed TOLAC, resulting in emergency repeat caesarean section, is associated with increased maternal and neonatal risks. Evidence on the outcomes and determinants of failed TOLAC remains limited in Somalia. This study assessed maternal and neonatal outcomes and identified factors associated with failed TOLAC among women with one previous caesarean section in selected private hospitals in Mogadishu, Somalia.
Methods: A hospital-based unmatched case-control study was conducted between October 2024 and May 2025 in selected private hospitals in Mogadishu, Somalia. A total of 228 women with one previous caesarean section who were eligible for TOLAC were included, comprising 114 cases with failed TOLAC resulting in emergency repeat caesarean section and 114 controls who achieved successful vaginal birth after caesarean (VBAC). Data were collected through structured interviews and medical record review. Multivariable logistic regression analysis was performed to identify independent predictors of failed TOLAC, and adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were reported.
Results: In the study sample, 114 women experienced failed TOLAC and 114 achieved successful VBAC. Maternal complications were more frequent among women with failed TOLAC, including blood transfusion in 14 (12.3%), wound dehiscence in 4 (3.5%), and uterine rupture in 1 (0.9%). After adjustment, failed TOLAC was independently associated with ruptured membranes at admission (AOR = 2.25; 95% CI: 1.13– 4.51), attending only two antenatal care visits (AOR = 2.99; 95% CI: 1.49– 6.02), an inter-pregnancy interval of less than two years (AOR = 2.84; 95% CI: 1.40– 5.79), referral from another health facility (AOR = 4.46; 95% CI: 2.17– 9.16), and a history of stillbirth (AOR = 2.37; 95% CI: 1.12– 5.01). Neonatal outcomes differed between the two groups and were reviewed carefully during revision to ensure consistency with the corrected tables.
Conclusion: Failed TOLAC among women with one previous caesarean section in Mogadishu was associated with both obstetric and health-system factors. Strengthening antenatal care, promoting optimal birth spacing, improving referral pathways, ensuring close intrapartum monitoring, and developing context-appropriate standardized TOLAC protocols may help improve maternal and neonatal outcomes.
Keywords: trial of labour after caesarean section, failed TOLAC, repeat caesarean section, maternal and neonatal outcomes, risk factors, Somalia
Introduction
Caesarean section (CS) is one of the most frequently performed obstetric procedures worldwide, and its use has increased substantially over recent decades. When medically indicated, CS can be lifesaving for both mother and newborn. However, population-level increases in CS above approximately 10% have not been consistently associated with further reductions in maternal or neonatal mortality, highlighting the importance of ensuring that the procedure is used appropriately rather than routinely.1 At the same time, repeated caesarean deliveries are associated with cumulative maternal risks, including adhesions, abnormal placentation, surgical complications, and increased complexity in subsequent pregnancies.2,3 These concerns have strengthened interest in strategies that can safely reduce unnecessary repeat caesarean births.
Trial of labour after caesarean section (TOLAC) is an important approach for women with a previous caesarean birth, particularly those with one prior low-transverse incision and no contraindication to vaginal delivery. When successful, TOLAC results in vaginal birth after caesarean (VBAC), which is associated with shorter recovery time, lower postoperative morbidity, and avoidance of the long-term risks associated with multiple caesarean deliveries.2,4–9 Major guidelines and large observational studies indicate that, in appropriately selected women, VBAC is achieved in approximately 60% to 80% of attempts.2,4,5,10 Nevertheless, failed TOLAC, which results in emergency repeat caesarean section, is associated with greater maternal and neonatal morbidity than successful VBAC and therefore requires careful patient selection, counselling, labour surveillance, and timely access to operative delivery.2,4,5,11–14
The likelihood of successful VBAC is influenced by both maternal and intrapartum factors. Previous vaginal birth, previous successful VBAC, spontaneous onset of labour, and favourable cervical findings are generally associated with higher success, whereas short inter-pregnancy interval, labour dystocia, induction in selected circumstances, suspected macrosomia, and other obstetric complications may reduce the probability of successful vaginal delivery.5,6,15,16 In addition, outcomes after TOLAC are shaped not only by individual clinical factors but also by the capacity of the health system. In low-resource and fragile settings, delayed referral, limited antenatal care utilization, gaps in continuous intrapartum monitoring, inconsistent availability of safe blood, and restricted access to comprehensive emergency obstetric and neonatal care may increase the risk of adverse outcomes when labour does not progress as expected.7–9,17–24
These issues are particularly relevant in Somalia. Nationally representative UNICEF data indicate that only about 2% of births in Somalia are delivered by caesarean section, suggesting major population-level limitations in access to surgical obstetric care.10,25 In contrast, hospital-based studies from Mogadishu and other Somali referral facilities have reported substantially higher CS proportions, including 21.6% in one tertiary hospital study and 37.0% in a recent multicenter hospital-based study, indicating marked differences between community-level access and facility-based obstetric practice.11,12,26 National strategy documents have also emphasized the need to strengthen antenatal care, referral systems, and access to basic and comprehensive emergency obstetric and neonatal care across the Somali health system.8,9,27 In this context, decisions regarding TOLAC are likely to be influenced by both obstetric risk and health-system readiness. Despite this, evidence on maternal and neonatal outcomes of TOLAC and on factors associated with failed TOLAC in Somalia remains very limited. In Mogadishu and similar urban Somali settings, decisions around TOLAC are shaped not only by individual obstetric factors but also by health-system capacity. National maternal and newborn health strategy documents emphasize the need for reliable antenatal care, functional referral pathways, skilled birth attendance, and access to Basic and Comprehensive Emergency Obstetric and Neonatal Care, including timely operative delivery when labour complications arise. Available Somali data also suggest persistent gaps in maternal care coverage, with low uptake of recommended antenatal visits at national level and uneven access to facility-based delivery and skilled attendance. In this context, the safety and success of TOLAC depend heavily on timely monitoring in labour, readiness for emergency theatre intervention, and efficient referral when complications develop.28,29 This study therefore aimed to assess maternal and neonatal outcomes and identify risk factors associated with failed TOLAC among women with one previous caesarean section in selected hospitals in Mogadishu, Somalia.
Methods
Study Site and Design
This was a hospital-based unmatched case-control study conducted in selected private hospitals in Mogadishu, Somalia. Eligible women with one previous caesarean section who were considered suitable for a trial of labour after caesarean section (TOLAC) were identified at admission and followed prospectively through delivery and discharge. Participants were then classified according to delivery outcome: women who underwent emergency repeat caesarean section after a trial of labour were defined as cases (failed TOLAC), whereas women who achieved vaginal birth after caesarean (VBAC) were defined as controls.
Study Population
The study population comprised all women with one previous caesarean section scar who were admitted for delivery at selected private hospitals in Mogadishu, regardless of whether they were admitted in labour or not.
Inclusion and Exclusion Criteria
All women with one previous caesarean section admitted for delivery at the selected hospitals during the study period were eligible for inclusion. Women admitted with confirmed intrauterine fetal death at the time of admission were excluded.
Sample Size Calculation and Sampling
The sample size was calculated using the formula for an unmatched case-control study: n = ((1 + 1/r) × (Zα/2 + Zβ)2 × p* × (1 − p*)) / (p1 − p2)2
where n is the required sample size for cases, r is the ratio of controls to cases, p1 is the proportion of exposure among cases, p2 is the proportion of exposure among controls, and p* is the average proportion exposed, calculated as (p1 + p2)/2. Based on a previous study, the expected proportions of exposure among cases and controls were 0.29 and 0.47, respectively, giving an average proportion exposed (p*) of 0.38. Using a 95% confidence level, 80% power, a 1:1 case-to-control ratio, and an absolute difference in exposure proportion of 0.18, the final sample size was 114 cases and 114 controls, for a total of 228 participants. Eligible participants were recruited consecutively during the study period and were classified as cases or controls according to the final delivery outcome.
Recruitment and Study Procedure
Women with one previous caesarean section and no contraindication to vaginal delivery in the current pregnancy were assessed and offered TOLAC by the routine managing team. Eligibility criteria included one previous lower-segment uterine scar, singleton pregnancy, cephalic presentation, estimated fetal weight of 4 kg or less, and absence of a current indication for immediate caesarean section. After enrolment, participants were followed from admission until delivery and discharge. Women whose TOLAC ended in emergency repeat caesarean delivery were classified as cases, while those who achieved vaginal birth after caesarean were classified as controls.
Operational Definition of Failed TOLAC
For this study, failed TOLAC was defined as a trial of labour in a woman with one previous caesarean section that ended in emergency repeat caesarean delivery after the onset of labour. Common indications included non-reassuring fetal status, failure to progress or labour arrest, suspected scar complications including uterine rupture, and other intrapartum obstetric indications requiring urgent operative delivery.
Data Collection Tools and Process
Data were collected using an interviewer-administered structured questionnaire and a review of participants’ medical records. The principal source of information was direct interviews with consenting participants, while additional clinical and obstetric data were obtained from hospital charts.
At first contact, eligible and consenting women were interviewed using a standardized questionnaire developed following extensive literature review. The questionnaire was then translated to Somali and then back translated to English to ensure consistency. Prior to deployment, the questionnaire was pretested on a sample of a similar population to validate it. The questionnaire comprised socio-demographic characteristics, past obstetric history, and medical conditions during the current pregnancy. Participants were then prospectively followed from admission until discharge. During follow-up, information on labour and delivery outcomes, current obstetric factors, health system–related factors, and maternal and fetal complications was recorded.
The research team maintained contact with each participant at least once daily throughout hospitalization. Data collection was conducted over an eight-month period, from October 2024 to May 2025.
Study Variables
The independent variables included: socio-demographic variables (age, marital status, and level of education); current obstetric variables (parity, gestational age at delivery, antenatal care attendance, onset of labour (spontaneous or induced), cervical dilatation at admission, membrane status at admission, duration of labour after admission, birth weight, and presence of comorbid medical conditions); past obstetric variables (indication for previous caesarean section, inter-delivery interval, and history of stillbirth); and health system–related variables (referral status and decision-to-delivery interval).
Outcome variables: Maternal outcomes included uterine rupture, hysterectomy, postpartum hemorrhage requiring blood transfusion, puerperal infection, duration of hospital stay, maternal death, and mode of delivery among women undergoing a trial of labour. Fetal and neonatal outcomes included five-minute Apgar score, stillbirth, admission to the neonatal unit, and neonatal death before discharge.
Data Analysis
Data were entered, cleaned, and analysed using SPSS version 22. Descriptive statistics were used to summarize the characteristics of cases and controls for continuous variables, while frequencies and percentages were used for categorical variables. Bivariable logistic regression analysis was first performed to examine the association between each independent variable and failed TOLAC. Variables with a p-value <0.20 in the bivariable analysis were entered into the multivariable logistic regression model. Multicollinearity among candidate variables was assessed using variance inflation factors (VIFs) and tolerance statistics before fitting the final model. Model fitness was evaluated using the Hosmer–Lemeshow goodness-of-fit test. Adjusted odds ratios (AORs) with 95% confidence intervals (CIs) were reported, and a p-value <0.05 was considered statistically significant.
Results
A total of 228 women with one previous caesarean section who were eligible for TOLAC were included in the study, comprising 114 cases with failed TOLAC resulting in emergency repeat caesarean section and 114 controls who achieved successful vaginal birth after caesarean (VBAC). The baseline socio-demographic, obstetric, and service-related characteristics of the participants are presented in Table 1. In the bivariable analysis, several factors were associated with failed TOLAC. Women with ruptured membranes at admission had higher odds of failed TOLAC than those with intact membranes (COR = 2.72; 95% CI: 2.52–4.89; p = 0.008). Having only two antenatal care visits was also associated with failed TOLAC compared with having more than three visits (COR = 3.49; 95% CI: 1.89–6.41; p < 0.001). In addition, an inter-pregnancy interval of less than two years was associated with increased odds of failed TOLAC (COR = 2.18; 95% CI: 1.23–3.86; p = 0.007). Post-term gestation was significant in the bivariable analysis (COR = 3.05; 95% CI: 1.06–8.77; p = 0.038), whereas maternal age, educational status, occupation, parity, and overall ANC attendance were not significantly associated with failed TOLAC (Table 1).
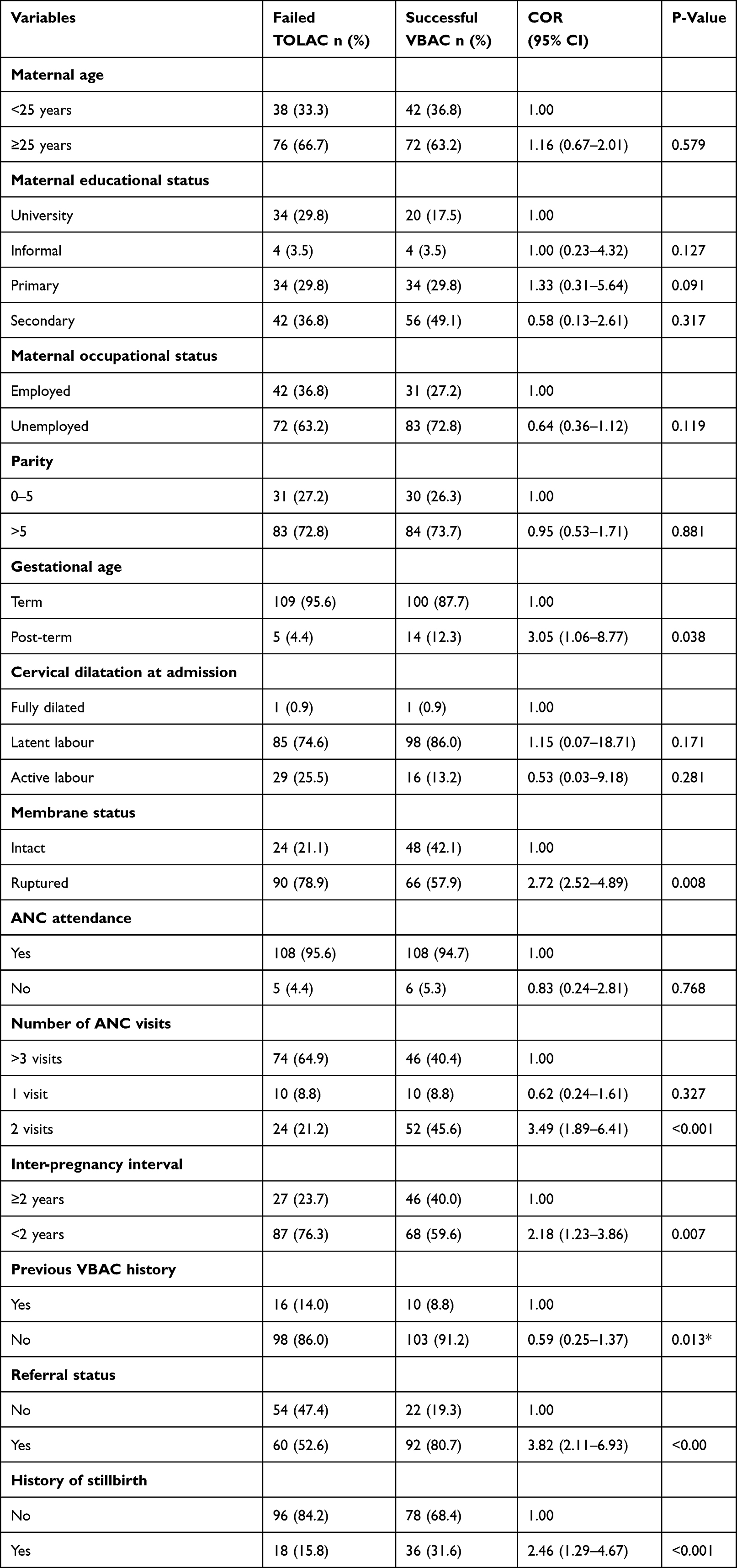 |
Table 1 Baseline Characteristics of Participants and Bivariate Analysis of Factors Associated with Repeat Caesarean Section |
Maternal complications were more frequent among women with failed TOLAC than among those with successful VBAC (Table 2). Blood transfusion was required in 14 (12.3%) women with failed TOLAC compared with 2 (1.8%) in the successful VBAC group. Wound dehiscence occurred in 4 (3.5%) cases and in none of the controls. Uterine rupture was rare and was observed in 1 (0.9%) woman with failed TOLAC, while no uterine rupture was recorded in the successful VBAC group.
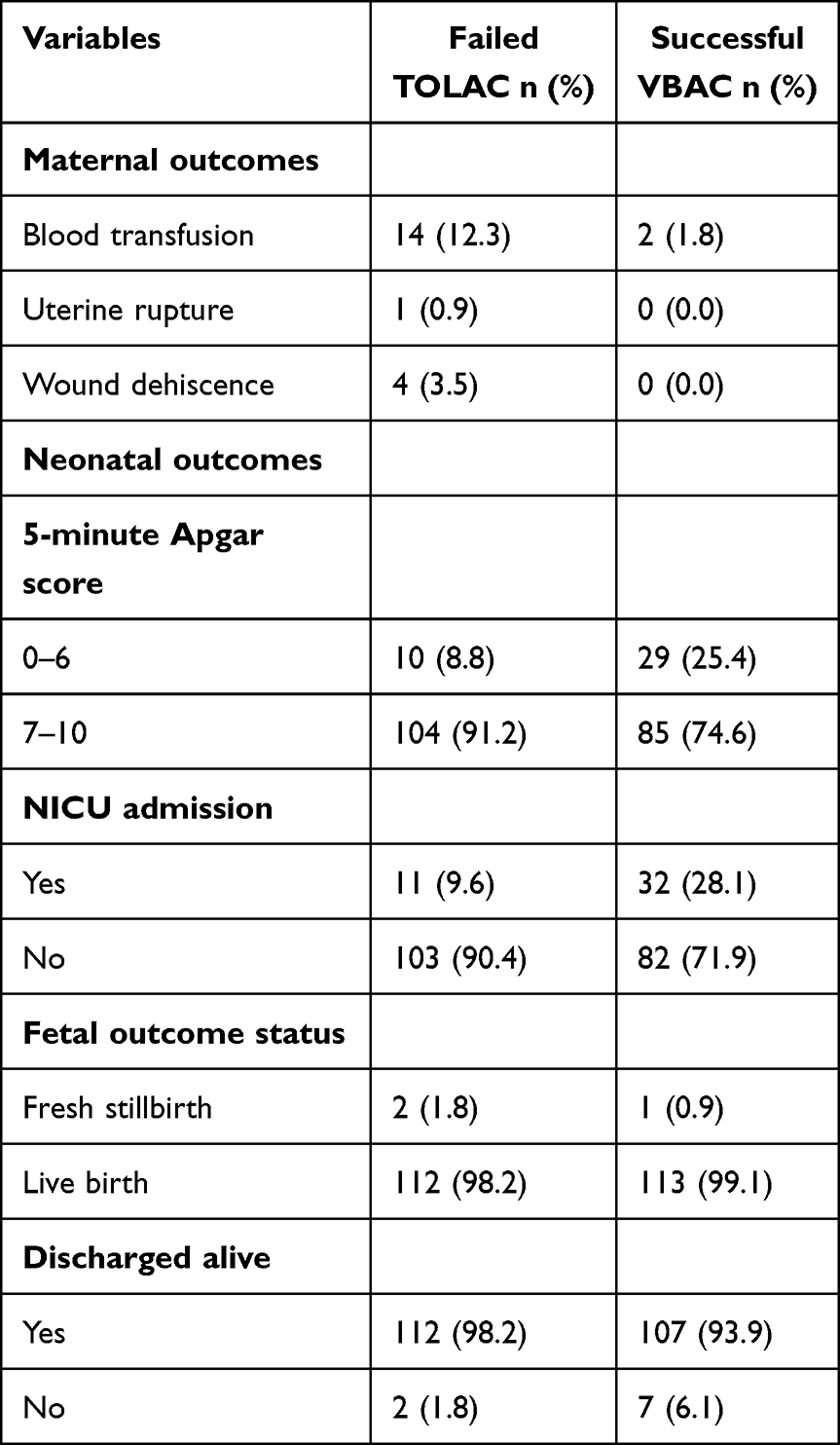 |
Table 2 Maternal and Neonatal Outcomes Among Women with Failed TOLAC and Successful VBAC |
Neonatal outcomes are also shown in Table 2. A 5-minute Apgar score of 0–6 was recorded in 10 (8.8%) neonates in the failed TOLAC group and 29 (25.4%) in the successful VBAC group, while NICU admission occurred in 11 (9.6%) and 32 (28.1%) neonates, respectively. Fresh stillbirth was uncommon in both groups, occurring in 2 (1.8%) cases and 1 (0.9%) controls. Most neonates were live born and discharged alive in both groups. Because the current neonatal outcome pattern in the tables differs from the direction described in the earlier manuscript narrative, these findings were reviewed carefully and are presented here conservatively in line with the tabulated data.
In the multivariable logistic regression analysis, ruptured membranes at admission remained independently associated with failed TOLAC (AOR = 2.25; 95% CI: 1.13–4.51; p = 0.021). Women who had attended only two antenatal care visits had nearly three times higher odds of failed TOLAC than those with more than three visits (AOR = 2.99; 95% CI: 1.49–6.02; p = 0.002). Likewise, an inter-pregnancy interval of less than two years was independently associated with failed TOLAC (AOR = 2.84; 95% CI: 1.40–5.79; p = 0.004). Referral from another health facility (AOR = 4.46; 95% CI: 2.17–9.16; p < 0.001) and a history of stillbirth (AOR = 2.37; 95% CI: 1.12–5.01; p = 0.023) were also significant predictors in the final model, whereas previous VBAC history was not significantly associated with failed TOLAC after adjustment (AOR = 0.63; 95% CI: 0.23–1.70; p = 0.366) (Table 3).
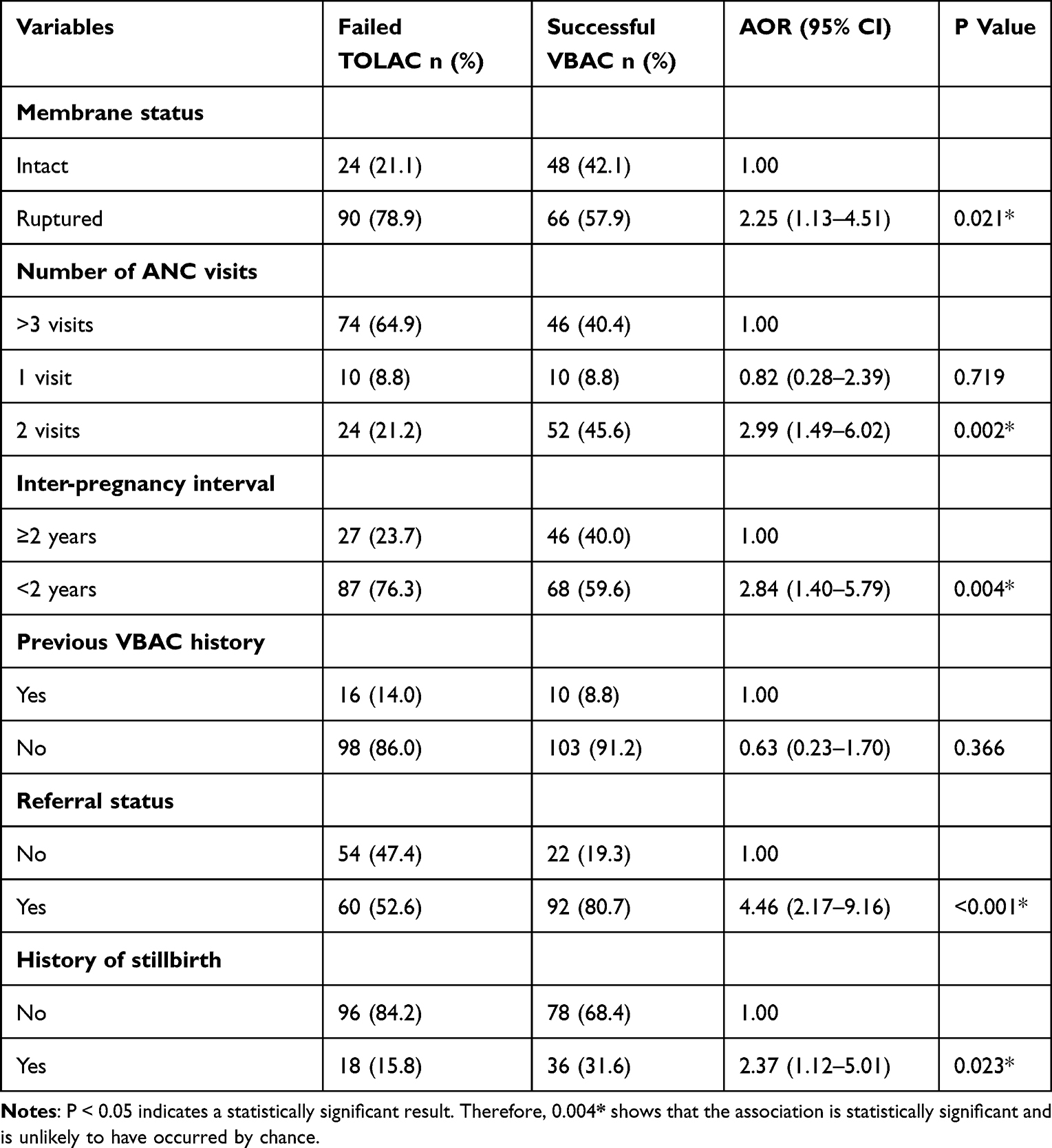 |
Table 3 Multivariable Logistic Regression Analysis of Factors Associated with Failed TOLAC |
The distribution of maternal outcomes demonstrated a higher frequency of complications among cases compared with controls. Blood transfusion and wound-related complications were observed predominantly among women who underwent repeat caesarean section, while uterine rupture was reported exclusively among cases (Figure 1).
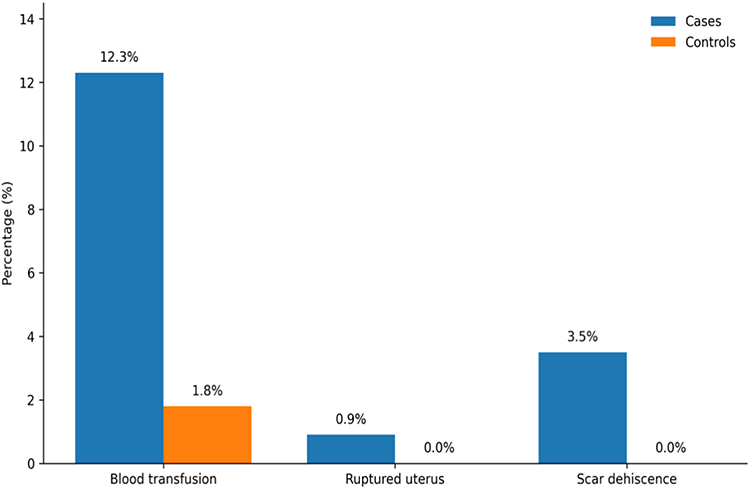 |
Figure 1 Distribution of maternal outcomes between cases and controls. |
Discussion
This study assessed the outcomes and determinants of failed trial of labour after one previous caesarean section (TOLAC) among women in selected hospitals in Mogadishu, Somalia. To our knowledge, it adds to the limited published evidence on TOLAC outcomes in Somalia and highlights the importance of both obstetric and health-system factors in shaping delivery outcomes in this setting. Overall, the findings suggest that failed TOLAC was associated with several clinically relevant predictors, including ruptured membranes at admission, limited antenatal care attendance, short inter-pregnancy interval, referral from another facility, and a history of stillbirth. These findings are broadly in line with previous studies from African and international settings that have shown TOLAC outcomes to depend not only on maternal and obstetric characteristics, but also on the quality and timeliness of intrapartum care and referral systems.1,2,6–9,20–27
Maternal complications were more frequent among women with failed TOLAC than among those who achieved successful vaginal birth after caesarean (VBAC). In particular, blood transfusion, wound dehiscence, and uterine rupture occurred predominantly in the failed TOLAC group. Although uterine rupture was rare in this study, its occurrence only among women requiring emergency repeat caesarean section is clinically important because it remains one of the most serious complications associated with TOLAC. This pattern is consistent with previous reports showing that unsuccessful TOLAC is associated with higher maternal morbidity than successful VBAC, especially when labour complications are recognized late or when emergency operative care is delayed.18–26
The neonatal findings in the present study require more cautious interpretation. After rechecking the tabulated results, the distribution of 5-minute Apgar scores and NICU admissions did not follow the pattern most commonly reported in the literature, where successful VBAC is generally associated with more favorable neonatal outcomes than failed TOLAC or emergency repeat caesarean section. Rather than forcing these findings to fit prior studies, we have revised the manuscript to present them conservatively and in direct accordance with the verified tables. Possible explanations include data-recording or classification issues in the originally prepared tables, differences in case mix between the two groups, timing of referral, or closer neonatal observation and admission practices among certain delivery categories. These findings should therefore be interpreted with caution and confirmed in future studies with more standardized neonatal outcome assessment.1,6,13,16–27
Among the independent predictors identified, ruptured membranes at admission remained significantly associated with failed TOLAC. This may reflect more advanced labour complexity, prolonged labour, or a higher likelihood of intrapartum concern by the time of hospital assessment. Similar findings have been reported in previous studies, where membrane rupture and intrapartum complications were associated with reduced VBAC success and increased emergency operative delivery. In settings where continuous fetal monitoring and rapid operative response may be constrained, the clinical implications of ruptured membranes may be even greater.7,8,16–27
A short inter-pregnancy interval was also independently associated with failed TOLAC. This finding is consistent with prior evidence suggesting that intervals of less than 18 to 24 months may increase the risk of uterine scar complications, failed labour, and adverse maternal outcomes in women with a previous caesarean section. Short birth spacing may also reflect broader reproductive health and counselling gaps, particularly in low-resource settings where postpartum family planning access is limited.9–11,20–25
Limited antenatal care attendance emerged as another important predictor. Women who had attended only two antenatal care visits were more likely to experience failed TOLAC than those with more than three visits. Adequate antenatal care provides an opportunity to review the indication for the previous caesarean section, assess current pregnancy risk, counsel women on the suitability of TOLAC, and prepare an individualized delivery plan. Reduced ANC utilization may therefore contribute to delayed risk identification and suboptimal labour preparation. This interpretation is consistent with studies showing that stronger prenatal follow-up improves delivery planning and may support safer TOLAC decision-making.4,7,20–23
Referral from another health facility showed a strong association with failed TOLAC in the adjusted analysis. Although this variable should be interpreted alongside the corrected final dataset and table coding, the overall pattern supports the importance of referral pathways in shaping labour outcomes. Women referred from other facilities may arrive later in labour, with more complications, or after unsuccessful initial management, all of which can reduce the likelihood of successful VBAC. In fragile or resource-limited health systems, referral delays and interruptions in continuity of care can substantially affect both maternal and neonatal outcomes.3,8,20–24
A history of stillbirth was also associated with failed TOLAC. This may reflect more cautious intrapartum decision-making by clinicians and families in women with a prior adverse pregnancy outcome, leading to a lower threshold for emergency repeat caesarean section when labour progress becomes uncertain. Although the relationship between prior stillbirth and TOLAC outcome has not been as widely reported as other predictors, it is plausible that previous obstetric loss influences both risk perception and clinical management during labour.7,12,18,21,25
In contrast, maternal age, educational status, occupational status, and parity were not significantly associated with failed TOLAC in this study. This differs from some studies in high-income settings that have reported lower VBAC success among older women and those with less favourable baseline obstetric profiles. The difference may reflect variations in study population, patient selection, referral patterns, labour management, and health-system context. It may also indicate that, in this setting, intrapartum and service-related factors play a more prominent role than some background socio-demographic characteristics.10–25,27
Taken together, the findings of this study highlight that failed TOLAC in Mogadishu is shaped by both clinical and health-system factors. Maternal complications were clearly more frequent among women with failed TOLAC, reinforcing the importance of careful selection, adequate antenatal preparation, timely referral, and close intrapartum monitoring. The neonatal findings were less straightforward and did not fully mirror the direction commonly reported in prior literature, so they have been interpreted conservatively in this revised manuscript. Overall, these results support the need for strengthened antenatal counselling, improved birth spacing, better referral coordination, and context-appropriate intrapartum management protocols when TOLAC is offered in Somali hospitals.4,5,7,18,20–23,25–27
Strengths and Limitations
This study benefits from a multicenter design, which allowed data collection from multiple private hospitals, enhancing the representativeness of hospital-based deliveries in Mogadishu. The prospective and systematic follow-up of participants from admission through discharge ensured accurate capture of maternal and neonatal outcomes, minimizing recall bias. Additionally, the inclusion of both maternal and fetal variables, as well as health system factors such as referral status and mode of decision-making, provides a comprehensive assessment of determinants affecting TOLAC success and repeat caesarean delivery.
However, several limitations should be considered. First, the study relied on hospital-based populations, which may not fully reflect outcomes in rural areas or among women delivering at home, limiting generalizability. In addition, the use of consecutive sampling among eligible women may have introduced selection bias, as the enrolled participants may not have fully represented all women attempting TOLAC during the study period. Second, selection bias may also have occurred, as women deemed higher risk may have been preferentially assigned to repeat caesarean delivery rather than TOLAC. Third, some variables, such as socio-economic status and exact gestational age, depended on patient self-reporting and medical record accuracy, introducing potential measurement bias. Finally, resource constraints limited continuous intrapartum monitoring, which may have influenced the observed complication rates.
Future research should aim to evaluate interventions designed to enhance TOLAC success, such as standardized labour protocols, improved antenatal counselling, risk stratification tools, and strengthened referral systems. Additionally, exploring community-based approaches to expand access to skilled birth attendants and timely emergency obstetric care would help address systemic barriers to safe vaginal birth after caesarean, particularly in resource-limited settings. In addition, the use of consecutive sampling among eligible women may have introduced selection bias, as the enrolled participants may not have fully represented all women attempting TOLAC during the study period.
Conclusion
In this study, failed trial of labour after caesarean section among women with one previous caesarean birth in Mogadishu was associated with several important obstetric and health-system factors, including ruptured membranes at admission, limited antenatal care attendance, short inter-pregnancy interval, referral from another health facility, and a history of stillbirth. Women with failed TOLAC also experienced more maternal complications than those who achieved successful vaginal birth after caesarean. These findings highlight the importance of careful patient assessment, timely referral, adequate antenatal preparation, and close intrapartum monitoring when offering TOLAC in resource-limited settings. Strengthening counselling on birth spacing, improving referral pathways, and ensuring readiness for emergency obstetric care may help improve outcomes. In addition, developing context-appropriate standardized TOLAC assessment and intrapartum management protocols in Somalia could support safer clinical decision-making and enhance maternal and neonatal care.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
Ethical approval for this study was obtained from the Center for Research and Development of SIMAD University (approval number: EC000172). All participants provided written informed consent after receiving an explanation of the study objectives, the voluntary nature of participation, their right to withdraw at any time, and assurances of confidentiality. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Acknowledgments
The author extends sincere appreciation to healthcare workers, including obstetricians, midwives, nurses, and allied maternal health professionals across Somalia for their dedication and frontline service delivery, which informed the perspectives discussed in this article. The author also acknowledges the Center for Research and Development (CRD), SIMAD University, for its guidance, academic support, and encouragement in research capacity building. Special thanks are extended to Dr. Sumait Hospital for fostering a supportive environment that promotes clinical inquiry and research engagement.
Funding
This work received institutional support from SIMAD University, Mogadishu, Somalia.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Adanu R, McCarthy M. Vaginal birth after cesarean delivery in the West African setting. Int J Gynaecol Obstet. 2007;98(3):227–12. doi:10.1016/j.ijgo.2007.03.056
2. Aisien A, Oronsaye A. Vaginal birth after one previous caesarean section in a tertiary institution in Nigeria. J Obstet Gynaecol. 2004;24(8):886–890. doi:10.1080/01443610400018742
3. Anderson GA, Ilcisin L, Kayima P, et al. Out-of-pocket payment for surgery in Uganda: the rate of impoverishing and catastrophic expenditure at a government hospital. PLoS One. 2017;12(10):e0187293. doi:10.1371/journal.pone.0187293
4. Begum KS, Khan NU, Akter F. Factors affecting the pregnancy outcome in patients with previous one caesarean section. Med Today. 2014;26(1):1–3. doi:10.3329/medtoday.v26i1.21300
5. Betran A, Torloni M, Zhang J, Gülmezoglu A. WHO statement on caesarean section rates. BJOG. 2015;122(5):667–670.
6. Betran AP, Torloni MR, Zhang J, et al. What is the optimal rate of caesarean section at population level? A systematic review of ecologic studies. Reprod Health. 2015;12(1):57. doi:10.1186/s12978-015-0043-6
7. Birara M, Gebrehiwot Y. Factors associated with success of vaginal birth after one caesarean section (VBAC) at three teaching hospitals in Addis Ababa, Ethiopia: a case-control study. BMC Pregnancy Childbirth. 2013;13(1):31. doi:10.1186/1471-2393-13-31
8. Boatin AA, Agaba E, Nyongozi B, Wylie BJ. Stage of labor at admission among Ugandan women with a prior cesarean, and its impact on management and delivery outcomes. Int J Gynaecol Obstet. 2017;139(1):14–20. doi:10.1002/ijgo.12252
9. Bujold E, Gauthier RJ. Risk of uterine rupture associated with an interdelivery interval between 18 and 24 months. Obstet Gynecol. 2010;115(5):1003–1006. doi:10.1097/AOG.0b013e3181d992fb
10. Bujold E, Hammoud AO, Hendler I, et al. Trial of labor in patients with a previous cesarean section: does maternal age influence the outcome? Am J Obstet Gynecol. 2004;190(4):1113–1118. doi:10.1016/j.ajog.2003.09.055
11. Bujold E, Mehta SH, Bujold C, Gauthier RJ. Interdelivery interval and uterine rupture. Am J Obstet Gynecol. 2002;187(5):1199–1202. doi:10.1067/mob.2002.127138
12. Butt T, Akhtar S. Vaginal birth after previous one caesarean section: term pregnancy outcome. J Postgrad Med Inst. 2011;19(4):478–482.
13. Carroll CS, Magann EF, Chauhan SP, Klauser CK, Morrison JC. Vaginal birth after cesarean section versus elective repeat cesarean delivery: weight-based outcomes. Am J Obstet Gynecol. 2003;188(6):1516–1522. doi:10.1067/mob.2003.472
14. Cragin EB. Conservatism in obstetrics. N Y Med J. 1916;104:1–2.
15. Durnwald CP, Ehrenberg HM, Mercer BM. The impact of maternal obesity and weight gain on vaginal birth after cesarean section success. Am J Obstet Gynecol. 2004;191(3):954–957. doi:10.1016/j.ajog.2004.05.051
16. Eden KB, McDonagh M, Denman MA, et al. New insights on vaginal birth after cesarean: can it be predicted? Obstet Gynecol. 2010;116(4):967–981. doi:10.1097/AOG.0b013e3181f2de49
17. Flamm BL. Once a cesarean, always a controversy. Obstet Gynecol. 1997;90(2):312–315. doi:10.1016/S0029-7844(97)00263-9
18. Grobman WA, Lai Y, Landon MB, et al. Development of a nomogram for prediction of vaginal birth after cesarean delivery. Obstet Gynecol. 2007;109(4):806–812. doi:10.1097/01.AOG.0000259312.36053.02
19. Guise JM, McDonagh MS, Osterweil P, Nygren P, Chan BKS, Helfand M. Systematic review of the incidence and consequences of uterine rupture in women with previous caesarean section. BMJ. 2004;329(7456):19–25. doi:10.1136/bmj.329.7456.19
20. Tefera M, Assefa N, Teji Roba K, Gedefa L. Predictors of success of trial of labor after cesarean section: a nested case-control study at public hospitals in Eastern Ethiopia. Womens Health. 2021;17:17455065211061960.
21. Landon MB, Hauth JC, Leveno KJ, et al. Maternal and perinatal outcomes associated with a trial of labor after prior cesarean delivery. N Engl J Med. 2004;351(25):2581–2589. doi:10.1056/NEJMoa040405
22. Madaan M, Agrawal S, Nigam A, Aggarwal R, Trivedi S. Trial of labour after previous caesarean section: the predictive factors affecting outcome. J Obstet Gynaecol. 2011;31(3):224–228. doi:10.3109/01443615.2010.544426
23. Kalisa R, Rulisa S, van Roosmalen J, van den Akker T. Maternal and perinatal outcome after previous caesarean section in rural Rwanda. BMC Pregnancy Childbirth. 2017;17(1):272. doi:10.1186/s12884-017-1467-5
24. Ngonzi J, Tornes YF, Mukasa PK, et al. Puerperal sepsis, the leading cause of maternal deaths at a tertiary university teaching hospital in Uganda. BMC Pregnancy Childbirth. 2016;16(1):207. doi:10.1186/s12884-016-0986-9
25. Landon MB, Leindecker S, Spong CY, et al. The MFMU Cesarean Registry: factors affecting the success of trial of labor after previous cesarean delivery. Am J Obstet Gynecol. 2005;193(3 Pt 2):1016–1023. doi:10.1016/j.ajog.2005.05.066
26. Silver RM, Landon MB, Rouse DJ, et al. Maternal morbidity associated with multiple repeat cesarean deliveries. Obstet Gynecol. 2006;107(6):1226–1232. doi:10.1097/01.AOG.0000219750.79480.84
27. American College of Obstetricians and Gynecologists. ACOG practice bulletin no. 115: vaginal birth after previous cesarean delivery. Obstet Gynecol. 2010;116(2 Pt 1):450–463. doi:10.1097/AOG.0b013e3181eeb251
28. Federal Government of Somalia, Ministry of Health and Human Services. Reproductive, Maternal, Neonatal, Child and Adolescent Health Strategy 2019–2023. Mogadishu, Somalia: Ministry of Health and Human Services; 2019. Available from: https://moh.gov.so/en/wp-content/uploads/2020/07/Reproductive-Maternal-Neonatal-Child-And-Adolescent-Health-Strategy-2019-2023-1.pdf.
29. World Health Organization Regional Office for the Eastern Mediterranean. Time to Act—Making Motherhood and Childhood Safer in Somalia. Cairo, Egypt: WHO Regional Office for the Eastern Mediterranean; 2023. Available from: https://www.emro.who.int/images/stories/somalia/RMNCAH-Policy-Brief-August-2023.pdf.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Urolithiasis Burden in Somalia: Associated Factors and Regional Distribution Among Patients Undergoing CT Scan in Selected Centers in Mogadishu
Dirie NI, Ahmed MM, Olad OM, Shire IH, Mohamud AK, Garba B, Mohamoud JH, Asowe HA, Orey FAH, Hassan J, Adam MH
Research and Reports in Urology 2025, 17:105-118
Published Date: 3 April 2025