Back to Journals » International Journal of Nanomedicine » Volume 21
Osteoimmune Regulation in Dental Implant Osseointegration: From Foreign Body Response to Therapeutic Immunomodulation—A Narrative Review
Authors Jian XC, Dong YL, Zhang MM, Guo ZL ![]()
Received 16 October 2025
Accepted for publication 14 January 2026
Published 2 February 2026 Volume 2026:21 574786
DOI https://doi.org/10.2147/IJN.S574786
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Krishna Nune
Xiao-Chong Jian,1,* Yu-Lei Dong,1,2,* Miao-Miao Zhang,1,2 Zhu-Ling Guo1,2
1School of Dentistry, Hainan Medical University, Haikou, 570100, People’s Republic of China; 2Department of Health Management Center, The First Affiliated Hospital of Hainan Medical University, Haikou, 570102, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhu-Ling Guo, School of Dentistry, Hainan Medical University, Haikou, 570100, People’s Republic of China, Email [email protected]
Background: The long-term success of dental implants depends on osseointegration, traditionally viewed as a biomechanical process. Recent osteoimmunology research reveals it as an immune-mediated phenomenon, where successful integration results from a redirected foreign body reaction termed Foreign Body Equilibrium (FBE).
Objective: This review aims to redefine osseointegration through the lens of osteoimmunology, emphasizing macrophage polarization (M1-to-M2 switch) as the pivotal determinant of implant fate, and to evaluate strategies for immunomodulatory implant design.
Methods: A comprehensive literature search was conducted using databases including PubMed, Web of Science, and Scopus. We selected and synthesized pivotal studies focusing on the cellular and molecular mechanisms of osseointegration, specifically targeting macrophage-T cell crosstalk and the RANKL-OPG axis. The review critically analyzes modulatory factors (surface topography, wettability, patient-specific conditions) and evaluates emerging therapeutic strategies such as bioactive coatings and extracellular vesicle functionalization.
Conclusion: Osseointegration is an active osteoimmune process. Harnessing immunomodulation—particularly macrophage polarization—can transform implants from passive devices to therapeutic platforms, improving outcomes in diverse clinical scenarios.
Keywords: osseointegration, foreign-body reaction, immunomodulation, dental implants, macrophage activation, bone-immune system
Introduction
Dental implant therapy has emerged as the gold standard for replacing missing teeth, with success rates exceeding 95% in healthy individuals. The biological foundation of this success lies in osseointegration, a process first described by Brånemark as the direct structural and functional connection between living bone and the load-bearing implant surface.1 However, this classical definition, while clinically relevant, fails to capture the complex immunological processes that govern implant integration.2
Recent advances in osteoimmunology have fundamentally transformed our understanding of bone-implant interactions. Rather than viewing osseointegration as a purely mechanical phenomenon, contemporary research recognizes it as a dynamic, immune-mediated process.3 Any biomaterial implanted within the body inevitably triggers a foreign body reaction (FBR), a universal immune response to non-degradable materials. Traditionally, the FBR progresses through predictable stages: protein adsorption, acute inflammation, chronic inflammation, foreign body giant cell formation, and ultimately fibrous encapsulation—signifying implant failure.4 However, before these chronic stages, the initial wound healing phase is critical, where the immune system must efficiently clear debris and resolve acute inflammation to pave the way for tissue repair.
The paradigm shift introduced by osteoimmunology suggests that successful osseointegration represents a unique redirection of the FBR, where the immune system constructs a “biological capsule” of bone tissue rather than a fibrous barrier. This state, termed Foreign Body Equilibrium (FBE), represents a continuously maintained balance between immune surveillance and tissue integration.5 Understanding this osteoimmune dialogue is crucial for developing next-generation implant therapies that actively modulate host responses to achieve predictable, long-term success6 (Figure 1).
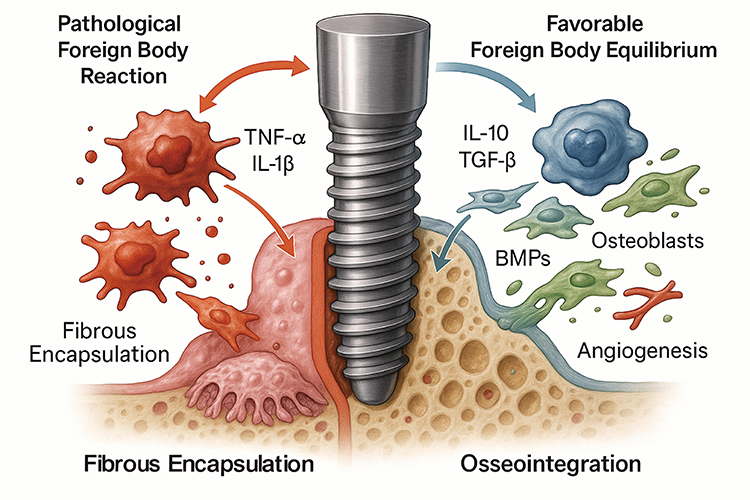 |
Figure 1 The Dichotomy of the Foreign Body Reaction at the Dental Implant Interface. The fate of a dental implant is determined by the host’s osteoimmune response. (Left Panel) A pathological foreign body reaction is characterized by the dominance of pro-inflammatory M1 macrophages, which release cytokines such as TNF-α and IL-1β. This sustained inflammation leads to fibrous encapsulation, preventing direct bone-to-implant contact and resulting in clinical failure. (Right Panel) Successful osseointegration is achieved through a state of “Foreign Body Equilibrium”. This favorable outcome is orchestrated by a timely shift to anti-inflammatory M2 macrophages, which secrete cytokines like IL-10 and TGF-β, and growth factors such as BMPs. These factors promote angiogenesis and stimulate osteoblasts to form new bone directly on the implant surface, leading to stable integration. |
While recent reviews, such as Kondo et al (2024), have elegantly outlined the innate immune regulations in osseointegration, there remains a need to systematically integrate these mechanisms with advanced therapeutic immunomodulation strategies. Distinct from previous works, this review specifically focuses on the “Foreign Body Equilibrium” concept and critically evaluates how emerging biomaterial technologies—from extracellular vesicles to cell-membrane camouflage—can actively engineer this immune balance for clinical success.
The Foreign Body Equilibrium: Redefining Osseointegration
From Biomechanical Fixation to Immunological Integration
The traditional biocompatibility paradigm emphasizes material inertness and the absence of adverse reactions. However, contemporary osteoimmunology reveals that successful osseointegration requires active immune participation rather than immune avoidance.7 Upon implantation, the implant surface is immediately coated with host proteins through a process of competitive adsorption, forming a “provisional matrix” that serves as the primary interface for cellular recognition.8
This protein corona is not merely a passive film but constitutes the “first language” of host-implant communication. The composition, conformation, and density of adsorbed proteins directly influence subsequent cellular responses, particularly macrophage adhesion and activation.5 Surface hydrophobicity can induce protein unfolding, exposing cryptic epitopes that may be recognized as damage-associated molecular patterns (DAMPs), thereby initiating robust immune responses.9
The Inflammatory Cascade: A Double-Edged Sword
Surgical implant placement inevitably triggers acute sterile inflammation, characterized by the rapid recruitment of neutrophils followed by monocyte infiltration and macrophage differentiation. This initial inflammatory response serves essential functions in debris clearance and wound healing initiation. For biocompatible materials, this acute phase should be transient, resolving within approximately two weeks and transitioning to a pro-reparative environment.10
However, persistent inflammation represents a pathological deviation that leads to chronic tissue destruction. Factors such as bacterial contamination, excessive surgical trauma, or continuous particle release can sustain inflammatory responses, ultimately resulting in fibrous encapsulation and osseointegration failure.11 The immune system thus functions as a “biological switch”—controlled acute inflammation promotes bone regeneration, while uncontrolled chronic inflammation destroys it.
Cellular Orchestrators of the Osteoimmune Response
Macrophage Polarization: The Master Regulatory Switch
Macrophages represent the central coordinators of the FBR and osseointegration process, exhibiting remarkable phenotypic plasticity in response to environmental cues.12 The classical M1/M2 polarization paradigm, while simplified, provides a useful framework for understanding macrophage functions in implant integration.
M1 Macrophages: Essential Clearance but Potential Destruction
Classically activated M1 macrophages dominate the early post-implantation period, secreting high levels of pro-inflammatory cytokines including tumor necrosis factor-alpha (TNF-α), interleukin-1β (IL-1β), and interleukin-6 (IL-6).13,14 While essential for pathogen clearance and debris removal, sustained M1 activation promotes chronic inflammation and bone resorption through enhanced osteoclast activity via the RANKL-RANK signaling pathway.15
Titanium wear particles represent potent M1 inducers, activating the NLRP3 inflammasome and triggering the release of mature IL-1β, which creates a destructive positive feedback loop leading to aseptic loosening.16 This creates a clinical paradox regarding surface topography: while surface roughening (eg, via SLA) is intended to increase the surface area for osseointegration, it may inadvertently compromise the material’s wear resistance. Under mechanical loading, increased roughness can accelerate the liberation of titanium ions and particles. These debris are phagocytosed by macrophages, triggering NLRP3 inflammasome activation and sustaining a chronic inflammatory state that counteracts the initial benefits of the roughened surface.
M2 Macrophages: Architects of Tissue Regeneration
Alternatively activated M2 macrophages emerge as inflammation resolves, secreting anti-inflammatory cytokines such as interleukin-10 (IL-10) and transforming growth factor-β (TGF-β).17 These cells actively promote angiogenesis, extracellular matrix remodeling, and osteoblast differentiation through the release of growth factors including vascular endothelial growth factor (VEGF) and bone morphogenetic proteins.18
The transition from M1 to M2 phenotype represents the most critical checkpoint determining osseointegration success or failure. This phenotypic switch is regulated by multiple signals, including apoptotic neutrophil clearance, T lymphocyte-derived cytokines, and implant surface characteristics. Delayed or impaired M1-to-M2 transition results in persistent inflammation and ultimate implant failure (Figure 2).
 |
Figure 2 Cellular and Molecular Network Orchestrating Successful Osseointegration. This diagram illustrates the detailed mechanisms driving a favorable osteoimmune response. Upon implantation, host proteins adsorb to the titanium surface. The critical event is the M1-to-M2 macrophage polarization switch, which is promoted by regulatory T cells (Tregs). The resulting M2 macrophages are central coordinators, releasing IL-10 to resolve inflammation and VEGF to promote angiogenesis. They also stimulate mesenchymal stem cells (MSCs) to differentiate into bone-forming osteoblasts. Concurrently, the RANK-RANKL-OPG signaling axis is modulated to favor bone formation, with OPG inhibiting RANK on osteoclast precursors, thus preventing bone resorption. |
T Lymphocytes: Adaptive Immune Modulators
While the FBR has traditionally been considered a primarily innate immune phenomenon, mounting evidence reveals significant adaptive immune involvement.19 Dendritic cells can process implant-derived “antigens”—including metal ions, wear debris, or adsorbed bacterial products—and present them to T cells, initiating specific adaptive responses.3
Th Cell Subsets and Bone Homeostasis
The balance between different T helper (Th) cell subsets critically influences bone metabolism:
- Th1/Th2 Axis: Th1 cells secrete interferon-γ (IFN-γ), promoting M1 macrophage activation and pro-inflammatory responses. Conversely, Th2 cells produce IL-4 and IL-13, driving M2 polarization and tissue repair.20
- Th17/Treg Axis: Th17 cells represent a potent pro-inflammatory subset whose signature cytokine, IL-17, strongly promotes osteoclast formation and bone resorption. These cells serve as key drivers of pathological bone loss in periodontitis and peri-implantitis.21
Regulatory T Cells: Guardians of Immune Homeostasis
Regulatory T cells (Tregs) function as immune “peacekeepers,” suppressing excessive inflammatory responses to maintain tolerance.22 Tregs protect bone tissue through multiple mechanisms: direct inhibition of osteoclast formation, secretion of anti-inflammatory cytokines, and induction of macrophage M2 polarization. Importantly, Tregs can release extracellular vesicles expressing CD73, which converts ATP to adenosine, acting on macrophage A2A receptors to promote M2 polarization.23
In pathological states such as peri-implantitis, an imbalance in the Treg/Th17 ratio, characterized by relative Treg depletion, drives immune dysregulation and progressive bone destruction.24
Key Signaling Networks in Osteoimmunology
Two critical signaling pathways govern the osteoimmune dialogue:
The RANK-RANKL-OPG Axis
This pathway represents the master regulator of bone resorption. RANKL (Receptor Activator of Nuclear Factor κB Ligand), expressed by osteoblasts, osteocytes, and activated T cells, binds to RANK on osteoclast precursors, triggering their differentiation into mature bone-resorbing cells.25 Osteoprotegerin (OPG) acts as a decoy receptor, preventing RANKL-RANK interactions and inhibiting osteoclastogenesis. Pro-inflammatory cytokines disrupt this balance by upregulating RANKL expression, leading to pathological bone loss. Recent studies indicate that hydrophilic surfaces can downregulate RANKL expression in T cells, thereby shifting the balance towards osteogenesis.
NLRP3 Inflammasome Activation
The NLRP3 inflammasome functions as a danger sensor within macrophages, responding to biomaterial particles and other stress signals.26 Upon activation, it processes pro-IL-1β into its mature, highly potent form, creating inflammatory amplification loops that drive aseptic loosening and bone destruction. Consequently, modern immunomodulatory coatings, such as those incorporating miRNAs, specifically target the inhibition of NLRP3 assembly to prevent this inflammatory amplification.
Factors Modulating the Osteoimmune Response
Implant Surface Characteristics
The implant surface serves as the primary interface dictating subsequent immune responses through its physical topography and chemical composition.27 The immunomodulatory efficacy of these modifications is typically characterized using a combination of gene expression analysis (RT-qPCR for cytokine markers), protein secretion profiling (ELISA or Western blot for IL-10/TNF-α ratios), and detailed flow cytometry to assess macrophage M1/M2 surface marker shifts (eg, CD86 vs CD206).
Surface Topography and Immune Modulation
Micro- and nano-scale surface features profoundly influence cellular behavior. Moderately rough surfaces created by sandblasting and acid-etching (SLA) significantly increase surface area for cell attachment while promoting favorable protein adsorption profiles.28 Specific nanotopographies can reduce macrophage activation and guide M2 polarization, with approximately 30 nm diameter titanium nanotube arrays preferentially inducing M2 phenotypes compared to larger structures.29
Surface Chemistry and Wettability
Hydrophilic surfaces promote more favorable protein adsorption and accelerate early bone healing compared to hydrophobic counterparts.30 SLActive surfaces demonstrate reduced pro-inflammatory cytokine expression by adherent macrophages while enhancing anti-inflammatory factor production. The introduction of specific chemical functional groups (eg, -NH2, -COOH, -OH) can significantly modulate immune cell interactions, with negatively charged surfaces potentially promoting Treg formation.31
Tribocorrosion and Mechanical Modulators
Beyond topography and chemistry, the tribocorrosion behavior of the implant surface is a potent immunomodulator. The synergistic effect of mechanical wear and electrochemical corrosion releases metal ions that act as haptens, activating T cells and perpetuating inflammation. Surface treatments that enhance hardness and corrosion resistance, such as nitriding or diamond-like carbon (DLC) coatings, have been shown to mitigate this immune reactivity, preserving the integrity of the osseointegration interface.
Bioactive Ion Integration
The incorporation of bioactive ions into surface coatings represents an emerging immunomodulatory strategy. Strontium (Sr2⁺) exhibits “dual-action” capabilities, simultaneously promoting osteoblast proliferation while inhibiting osteoclast activity.32 Importantly, strontium induces macrophage M2 polarization and reduces pro-inflammatory cytokine expression.33 Similarly, zinc (Zn2⁺) modifications demonstrate both osteogenic and antibacterial properties while promoting anti-inflammatory responses.
Surgical Technique Considerations
Surgical trauma directly influences the magnitude and duration of inflammatory responses.34 Minimally invasive techniques, including flapless implant placement, generate less tissue damage and consequently milder inflammatory responses compared to conventional approaches. Clinical studies demonstrate reduced matrix metalloproteinase-8 (MMP-8) levels and decreased marginal bone loss in flapless procedures.35
However, the relationship between surgical trauma and healing is complex. Excessive minimization of immune activation may impair the recruitment of regenerative cells necessary for optimal bone formation.36 The optimal approach balances trauma reduction with sufficient immune stimulation to drive regenerative processes.37
Host-Specific Factors
Patient-specific characteristics significantly influence osseointegration outcomes through their effects on systemic and local immune environments.38
Age-Related Immunosenescence
Aging is associated with immunosenescence and chronic low-grade inflammation (“inflammaging”), which can compromise osseointegration.39 Age-related changes in mesenchymal stem cell (MSC) differentiation bias toward adipogenesis rather than osteogenesis, while immune dysfunction may impair proper inflammatory resolution.40
Systemic Disease Impact
Diabetes mellitus represents a significant risk factor due to its association with chronic systemic inflammation and M1 macrophage bias.41 Hyperglycemia promotes sustained pro-inflammatory environments that impair normal bone remodeling and may interfere with MSC osteogenic differentiation. Studies in diabetic models reveal NLRP3 inflammasome hyperactivation and M1/M2 imbalances around implants.42
Oral Microbiome Influence
The oral microbiome directly impacts peri-implant immune homeostasis. Microbial dysbiosis, characterized by pathogenic bacterial overgrowth, provides continuous immune stimulation leading to chronic inflammation. This persistent inflammatory state gradually erodes the bone-implant interface, ultimately resulting in peri-implantitis and implant failure.43
Therapeutic Immunomodulation Strategies
To actively promote a pro-reparative environment, various therapeutic interventions—ranging from pharmacological agents to advanced biomaterial coatings—have been developed (Table 1).
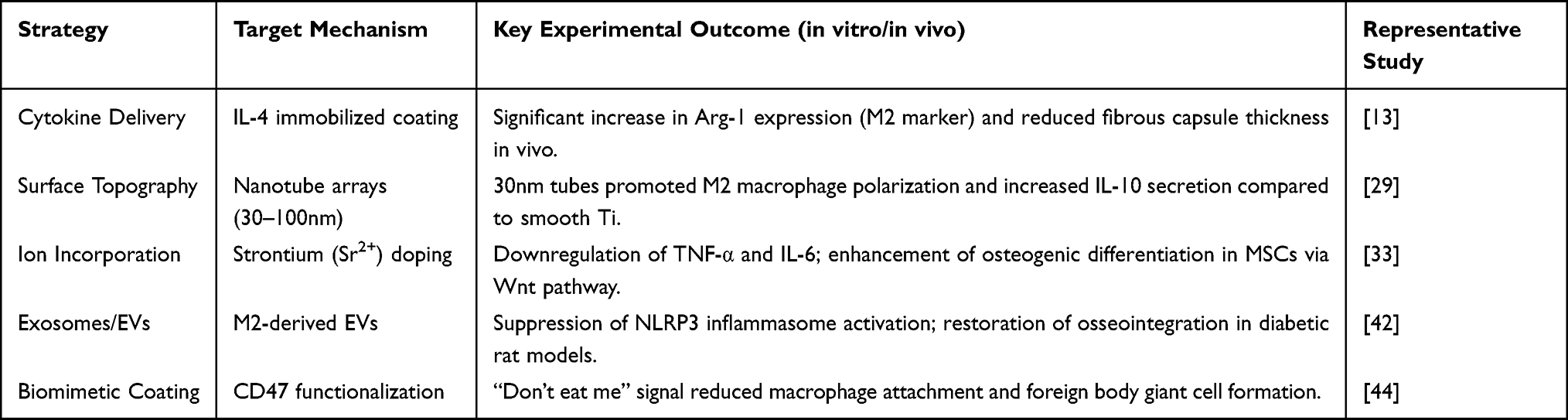 |
Table 1 Summary of Recent Studies on Immunomodulatory Approaches for Dental Implants |
Pharmacological Interventions
PDRN (Polydeoxyribonucleotide) Therapy
PDRN activates adenosine A2A receptors, inducing macrophage M2 polarization while increasing IL-10 and VEGF production.45 Clinical studies demonstrate PDRN’s ability to suppress RANKL-mediated osteoclast differentiation and promote tissue regeneration in inflammatory environments.46 As a small molecule therapeutic, PDRN shows high clinical translation potential.
Cytokine-Based Modulation
Direct delivery of anti-inflammatory cytokines such as IL-4 and IL-10 represents a targeted immunomodulatory approach.47 IL-4-loaded coatings effectively drive macrophage M2 polarization while suppressing inflammatory responses, leading to enhanced bone formation in animal models.13
Advanced Biomaterial Strategies
Extracellular Vesicle Functionalization
(Figure 3) M2 macrophage-derived extracellular vesicles (M2-EVs) contain immunomodulatory microRNAs, including miR-23a-3p, which suppress NLRP3 inflammasome activation and reduce IL-1β levels. Polydopamine-mediated M2-EV coating significantly improves osseointegration quality in diabetic models by reversing M1 bias and restoring immune balance.42
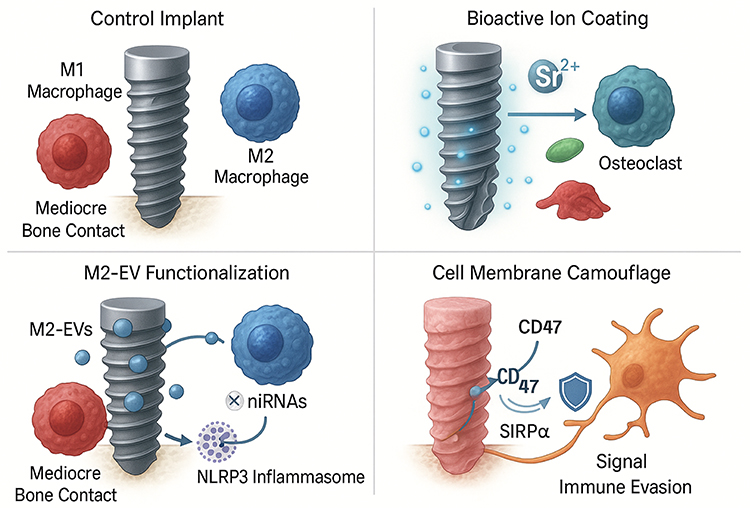 |
Figure 3 Advanced Immunomodulatory Strategies to Enhance Osseointegration. This figure compares a control implant with several advanced surface modification strategies designed to modulate the host immune response. (Top Left) A control implant elicits a mixed M1/M2 macrophage response, leading to mediocre bone contact. (Top Right) Bioactive ion coatings, such as those releasing Strontium (Sr2⁺), can promote M2 macrophage polarization while inhibiting osteoclast activity. (Bottom Left) M2-EV functionalization involves coating the implant with M2 macrophage-derived extracellular vesicles (M2-EVs). These EVs deliver microRNAs (miRNAs) that can suppress the NLRP3 inflammasome within M1 macrophages, re-educating them toward a pro-reparative phenotype. (Bottom Right) Cell membrane camouflage uses natural cell membranes displaying “don’t-eat-me” signals like CD47, which interacts with the SIRPα receptor on macrophages to evade immune recognition and reduce the foreign body reaction. |
Dual-Functional Ion-Peptide Coatings
Biomimetic mussel adhesion-mediated coatings enable simultaneous delivery of immunomodulatory Zn2⁺ ions and osteoinductive BMP-2 peptides.48 This dual-functional approach achieves synergistic effects: Zn2⁺ promotes M2 macrophage recruitment (∼92% increase) while BMP-2 directly stimulates osteoblast differentiation, resulting in superior bone-implant contact rates (82.1% vs 45.1% for uncoated controls).49
Biomimetic Cell Membrane Camouflage
Cell membrane coating technology represents a revolutionary “top-down” approach, where implant surfaces are cloaked with natural cell membranes (eg, red blood cell membranes) carrying “self-recognition” proteins such as CD47. This strategy effectively evades immune recognition, significantly reducing FBR intensity while maintaining biocompatibility.44
Smart Responsive Systems
The next frontier involves environment-responsive “smart” implants capable of dynamic immunomodulation.50 pH-sensitive hydrogel coatings can detect infection-induced acidification and respond by releasing antimicrobials and anti-inflammatory agents on demand.51 Such systems represent the evolution from passive implants to active therapeutic devices capable of real-time adaptation to changing biological conditions.
Clinical Translation Challenges and Future Perspectives
Translational Barriers
While preclinical data are encouraging, the translation to clinical practice faces distinct hurdles. First, regulatory complexity is a major barrier; implants with bioactive coatings or drug-eluting properties are often classified as combination products, requiring stringent safety data regarding release kinetics and systemic toxicity.52 Second, manufacturing reproducibility remains challenging. Scaling up nano-topographical modifications or delicate biological coatings (eg, cell membranes) without batch-to-batch variability is difficult and costly.53 Finally, the discrepancy between healthy animal models and compromised human patients (eg, smokers, diabetics) often leads to inconsistent clinical outcomes.54
Toward Personalized Immunomodulation
The “one-size-fits-all” approach is becoming obsolete. Future strategies must integrate immune profiling, where patients are stratified based on their cytokine baselines or genetic susceptibility to inflammation (eg, IL-1 polymorphisms).55 Emerging Artificial Intelligence (AI) and machine learning models could predict implant success by analyzing these complex immune signatures.56 Furthermore, 3D-printing technologies now allow for the fabrication of patient-specific implants with customized porous structures designed to modulate the local immune niche according to the individual’s bone density and inflammatory status.57
Advanced Preclinical Models
The development of patient-derived “organ-on-chip” and three-dimensional bioprinted tissue models will enable more predictive testing of implant responses before surgery.58 These platforms may bridge the translational gap between animal models and human clinical outcomes.
Conclusions
Osseointegration is fundamentally an immune-modulated process governed by the Foreign Body Equilibrium. This review highlights that the long-term success of dental implants relies not on immune evasion, but on the precise manipulation of the host response—specifically, the timely polarization of macrophages from the M1 to the M2 phenotype. While surface modifications and bioactive coatings show immense potential in preclinical models, overcoming regulatory and manufacturing hurdles remains essential. Ultimately, the integration of personalized immune profiling with smart, responsive biomaterials represents the future of implant dentistry, transforming implants from passive devices into active therapeutic tools for tissue regeneration.
Acknowledgments
We are grateful for the funding provided by the National Natural Science Foundation of China (grant number 82201080), Hainan S&T Program (KJTP202561) and the Academic Enhancement Support Program of Hainan Medical University (grant number XSTS2025027), which made this study possible. In addition, we extend our gratitude to Chang’an Health Center (Jinjiang Town, Chengmai County) for their contribution to this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the National Natural Science Foundation of China (82201080), supported by the Hainan S&T Program (KJTP202561), and the Academic Enhancement Support Program of Hainan Medical University (XSTS2025027).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Brånemark PI, Hansson BO, Adell R, et al. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand J Plast Reconstr Surg Suppl. 1977;16:1–11.
2. Franz S, Rammelt S, Scharnweber D, Simon JC. Immune responses to implants – a review of the implications for the design of immunomodulatory biomaterials. Biomaterials. 2011;32(28):6692–6709. doi:10.1016/j.biomaterials.2011.05.078
3. Amengual-Peñafiel L, Córdova LA, Constanza Jara-Sepúlveda M, Brañes-Aroca M, Marchesani-Carrasco F, Cartes-Velásquez R. Osteoimmunology drives dental implant osseointegration: a new paradigm for implant dentistry. Jpn Dent Sci Rev. 2021;57:12–19. doi:10.1016/j.jdsr.2021.01.001
4. Sheikh Z, Brooks PJ, Barzilay O, Fine N, Glogauer M. Macrophages, foreign body giant cells and their response to implantable biomaterials. Materials. 2015;8(9):5671–5701. doi:10.3390/ma8095269
5. Mariani E, Lisignoli G, Borzì RM, Pulsatelli L. Biomaterials: foreign bodies or tuners for the immune response? Int J Mol Sci. 2019;20(3):636. doi:10.3390/ijms20030636
6. Rahaman J, Mukherjee D. Osteoimmunomodulatory biomaterials: engineering strategies, current progress, and future perspectives for bone regeneration. Appl Mater Today. 2025;44:102753. doi:10.1016/j.apmt.2025.102753
7. Yun JI, Yun SI, Kim JH, Kim DG, Lee DW. Mediation of osseointegration, osteoimmunology, and osteoimmunologic integration by tregs and macrophages: a narrative review. Int J Mol Sci. 2025;26(11):5421. doi:10.3390/ijms26115421
8. Wilson CJ, Clegg RE, Leavesley DI, Pearcy MJ. Mediation of biomaterial-cell interactions by adsorbed proteins: a review. Tissue Eng. 2005;11(1–2):1–18. doi:10.1089/ten.2005.11.1
9. Moyano DF, Goldsmith M, Solfiell DJ, et al. Nanoparticle hydrophobicity dictates immune response. J Am Chem Soc. 2012;134(9):3965–3967. doi:10.1021/ja2108905
10. Albrektsson T, Jemt T, Mölne J, Tengvall P, Wennerberg A. On inflammation-immunological balance theory-A critical apprehension of disease concepts around implants: mucositis and marginal bone loss may represent normal conditions and not necessarily a state of disease. Clin Implant Dent Relat Res. 2019;21(1):183–189. doi:10.1111/cid.12711
11. Mustapha AD, Salame Z, Chrcanovic BR. Smoking and dental implants: a systematic review and meta-analysis. Medicina. 2021;58(1):39. doi:10.3390/medicina58010039
12. Vishwakarma A, Bhise NS, Evangelista MB, et al. Engineering immunomodulatory biomaterials to tune the inflammatory response. Trends Biotechnol. 2016;34(6):470–482. doi:10.1016/j.tibtech.2016.03.009
13. Xue JD, Gao J, Tang AF, Feng C. Shaping the immune landscape: multidimensional environmental stimuli refine macrophage polarization and foster revolutionary approaches in tissue regeneration. Heliyon. 2024;10(17):e37192. doi:10.1016/j.heliyon.2024.e37192
14. Nagashima H, Morio Y, Yamane K, Nanjo Y, Teshima R. Tumor necrosis factor-alpha, interleukin-1beta, and interleukin-6 in the cerebrospinal fluid of patients with cervical myelopathy and lumbar radiculopathy. Eur Spine J. 2009;18(12):1946–1950. doi:10.1007/s00586-009-1069-7
15. Ono T, Okamoto K, Nakashima T, et al. IL-17-producing γδ T cells enhance bone regeneration. Nat Commun. 2016;7:10928. doi:10.1038/ncomms10928
16. Nich C, Takakubo Y, Pajarinen J, et al. Macrophages-Key cells in the response to wear debris from joint replacements. J Biomed Mater Res Part A. 2013;101(10):3033–3045. doi:10.1002/jbm.a.34599
17. Rőszer T. Understanding the Mysterious M2 macrophage through activation markers and effector mechanisms. Mediators Inflammation. 2015;2015:816460. doi:10.1155/2015/816460
18. Brown BN, Ratner BD, Goodman SB, Amar S, Badylak SF. Macrophage polarization: an opportunity for improved outcomes in biomaterials and regenerative medicine. Biomaterials. 2012;33(15):3792–3802. doi:10.1016/j.biomaterials.2012.02.034
19. Banchereau J, Steinman RM. Dendritic cells and the control of immunity. Nature. 1998;392(6673):245–252. doi:10.1038/32588
20. Gaffen SL, Jain R, Garg AV, Cua DJ. The IL-23-IL-17 immune axis: from mechanisms to therapeutic testing. Nat Rev Immunol. 2014;14(9):585–600. doi:10.1038/nri3707
21. Huang N, Dong H, Luo Y, Shao B. Th17 cells in periodontitis and its regulation by A20. Front Immunol. 2021;12:742925. doi:10.3389/fimmu.2021.742925
22. Oparaugo NC, Ouyang K, Nguyen NPN, Nelson AM, Agak GW. Human regulatory T cells: understanding the role of tregs in select autoimmune skin diseases and post-transplant nonmelanoma skin cancers. Int J Mol Sci. 2023;24(2):1527. doi:10.3390/ijms24021527
23. Vignali DA, Collison LW, Workman CJ. How regulatory T cells work. Nat Rev Immunol. 2008;8(7):523–532. doi:10.1038/nri2343
24. Dutzan N, Kajikawa T, Abusleme L, et al. A dysbiotic microbiome triggers T(H)17 cells to mediate oral mucosal immunopathology in mice and humans. Sci trans med. 2018;10(463):eaat0797. doi:10.1126/scitranslmed.aat0797
25. Lacey DL, Timms E, Tan HL, et al. Osteoprotegerin ligand is a cytokine that regulates osteoclast differentiation and activation. Cell. 1998;93(2):165–176. doi:10.1016/s0092-8674(00)81569-x
26. Guo H, Callaway JB, Ting JP. Inflammasomes: mechanism of action, role in disease, and therapeutics. Nat med. 2015;21(7):677–687. doi:10.1038/nm.3893
27. Wennerberg A, Albrektsson T. Effects of titanium surface topography on bone integration: a systematic review. Clin Oral Implants Res. 2009;20 Suppl 4:172–184. doi:10.1111/j.1600-0501.2009.01775.x
28. Le Guéhennec L, Soueidan A, Layrolle P, Amouriq Y. Surface treatments of titanium dental implants for rapid osseointegration. Dent Mater. 2007;23(7):844–854. doi:10.1016/j.dental.2006.06.025
29. Oh S, Brammer KS, Li YS, et al. Stem cell fate dictated solely by altered nanotube dimension. Proc Natl Acad Sci U S A. 2009;106(7):2130–2135. doi:10.1073/pnas.0813200106
30. Rupp F, Scheideler L, Olshanska N, de Wild M, Wieland M, Geis-Gerstorfer J. Enhancing surface free energy and hydrophilicity through chemical modification of microstructured titanium implant surfaces. J Biomed Mater Res A. 2006;76(2):323–334. doi:10.1002/jbm.a.30518
31. Hotchkiss KM, Reddy GB, Hyzy SL, Schwartz Z, Boyan BD, Olivares-Navarrete R. Titanium surface characteristics, including topography and wettability, alter macrophage activation. Acta Biomater. 2016;31:425–434. doi:10.1016/j.actbio.2015.12.003
32. Caverzasio J. Strontium ranelate promotes osteoblastic cell replication through at least two different mechanisms. Bone. 2008;42(6):1131–1136. doi:10.1016/j.bone.2008.02.010
33. Zhang W, Zhao F, Huang D, Fu X, Li X, Chen X. Strontium-substituted submicrometer bioactive glasses modulate macrophage responses for improved bone regeneration. ACS Appl Mater Interfaces. 2016;8(45):30747–30758. doi:10.1021/acsami.6b10378
34. Lin GH, Chan HL, Bashutski JD, Oh TJ, Wang HL. The effect of flapless surgery on implant survival and marginal bone level: a systematic review and meta-analysis. J Periodontol. 2014;85(5):e91–103. doi:10.1902/jop.2013.130481
35. Jeong SM, Choi BH, Li J, et al. Flapless implant surgery: an experimental study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007;104(1):24–28. doi:10.1016/j.tripleo.2006.11.034
36. Zhao Z, Zhao Q, Gu B, et al. Minimally invasive implantation and decreased inflammation reduce osteoinduction of biomaterial. Theranostics. 2020;10(8):3533–3545. doi:10.7150/thno.39507
37. Su N, Villicana C, Yang F. Immunomodulatory strategies for bone regeneration: a review from the perspective of disease types. Biomaterials. 2022;286:121604. doi:10.1016/j.biomaterials.2022.121604
38. Monje A, Aranda L, Diaz KT, et al. Impact of maintenance therapy for the prevention of peri-implant diseases: a systematic review and meta-analysis. J Dent Res. 2016;95(4):372–379. doi:10.1177/0022034515622432
39. Franceschi C, Garagnani P, Parini P, Giuliani C, Santoro A. Inflammaging: a new immune-metabolic viewpoint for age-related diseases. Nat Rev Endocrinol. 2018;14(10):576–590. doi:10.1038/s41574-018-0059-4
40. Ma Y, Wang S, Wang H, et al. Mesenchymal stem cells and dental implant osseointegration during aging: from mechanisms to therapy. Stem Cell Res Ther. 2023;14(1):382. doi:10.1186/s13287-023-03611-1
41. Rohm TV, Meier DT, Olefsky JM, Donath MY. Inflammation in obesity, diabetes, and related disorders. Immunity. 2022;55(1):31–55. doi:10.1016/j.immuni.2021.12.013
42. Cheng Y, Dong X, Shi J, et al. Immunomodulation with M2 macrophage-derived extracellular vesicles for enhanced titanium implant osseointegration under diabetic conditions. Mater Today Bio. 2025;30:101385. doi:10.1016/j.mtbio.2024.101385
43. Assery NM, Jurado CA, Assery MK, Afrashtehfar KI. Peri-implantitis and systemic inflammation: a critical update. Saudi Dent J. 2023;35(5):443–450. doi:10.1016/j.sdentj.2023.04.005
44. Gao W, Hu CM, Fang RH, Luk BT, Su J, Zhang L. Surface functionalization of gold nanoparticles with red blood cell membranes. Adv Mater. 2013;25(26):3549–3553. doi:10.1002/adma.201300638
45. Galeano M, Bitto A, Altavilla D, et al. Polydeoxyribonucleotide stimulates angiogenesis and wound healing in the genetically diabetic mouse. Wound Repair Regener. 2008;16(2):208–217. doi:10.1111/j.1524-475X.2008.00361.x
46. Gan K, Lian H, Yang T, et al. Periplogenin attenuates LPS-mediated inflammatory osteolysis through the suppression of osteoclastogenesis via reducing the NF-κB and MAPK signaling pathways. Cell Death Discov. 2024;10(1):86. doi:10.1038/s41420-024-01856-0
47. Martinez FO, Gordon S. The M1 and M2 paradigm of macrophage activation: time for reassessment. F1000prime Rep. 2014;6:13. doi:10.12703/p6-13
48. Lee H, Dellatore SM, Miller WM, Messersmith PB. Mussel-inspired surface chemistry for multifunctional coatings. Science. 2007;318(5849):426–430. doi:10.1126/science.1147241
49. Wang T, Bai J, Lu M, et al. Engineering immunomodulatory and osteoinductive implant surfaces via mussel adhesion-mediated ion coordination and molecular clicking. Nat Commun. 2022;13(1):160. doi:10.1038/s41467-021-27816-1
50. Stuart MA, Huck WT, Genzer J, et al. Emerging applications of stimuli-responsive polymer materials. Nat Mater. 2010;9(2):101–113. doi:10.1038/nmat2614
51. Zhuo S, Zhang F, Yu J, Zhang X, Yang G, Liu X. pH-sensitive biomaterials for drug delivery. Molecules. 2020;25(23):5649. doi:10.3390/molecules25235649
52. Tian J, Song X, Wang Y, et al. Regulatory perspectives of combination products. Bioact Mater. 2022;10:492–503. doi:10.1016/j.bioactmat.2021.09.002
53. Damiati L, Eales MG, Nobbs AH, et al. Impact of surface topography and coating on osteogenesis and bacterial attachment on titanium implants. J Tissue Eng. 2018;9:2041731418790694. doi:10.1177/2041731418790694
54. Salthouse D, Novakovic K, Hilkens CMU, Ferreira AM. Interplay between biomaterials and the immune system: challenges and opportunities in regenerative medicine. Acta Biomater. 2023;155:1–18. doi:10.1016/j.actbio.2022.11.003
55. Chapelle N, Fantou A, Marron T, Kenigsberg E, Merad M, Martin JC. Single-cell profiling to transform immunotherapy usage and target discovery in immune-mediated inflammatory diseases. Front Immunol. 2022;13:1006944. doi:10.3389/fimmu.2022.1006944
56. Revilla-León M, Gómez-Polo M, Vyas S, et al. Artificial intelligence applications in implant dentistry: a systematic review. J Prosthetic Dent. 2023;129(2):293–300. doi:10.1016/j.prosdent.2021.05.008
57. Li Z, Wang Q, Liu G. A Review of 3D Printed Bone Implants. Micromachines. 2022;13(4):528. doi:10.3390/mi13040528
58. Luo Y, Li X, Zhao Y, Zhong W, Xing M, Lyu G. Development of organs-on-chips and their impact on precision medicine and advanced system simulation. Pharmaceutics. 2023;15(8):2094. doi:10.3390/pharmaceutics15082094
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.