Back to Journals » Clinical Interventions in Aging » Volume 20
Orthogeriatric Co-Management Improves Early Outcomes in Hip Fractures: A Post-Hoc Analysis of a Prospective Study
Authors Gao F ![]() , Wang Z, Chen Y, Bei M, Liu G, Yang M, Wu X
, Wang Z, Chen Y, Bei M, Liu G, Yang M, Wu X
Received 23 July 2025
Accepted for publication 19 November 2025
Published 27 November 2025 Volume 2025:20 Pages 2231—2240
DOI https://doi.org/10.2147/CIA.S555649
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Zhi-Ying Wu
Feng Gao,1,* Zongrui Wang,1,* Yimin Chen,1– 3,* Mingjian Bei,1– 3 Gang Liu,1– 3 Minghui Yang,1– 3 Xinbao Wu1– 3
1Department of Orthopaedics and Traumatology, Peking University Fourth School of Clinical Medicine, Beijing, People’s Republic of China; 2Department of Orthopaedics and Traumatology, Beijing Jishuitan Hospital, Capital Medical University, Beijing, People’s Republic of China; 3Department of Orthopaedics and Traumatology, National Center for Orthopaedics, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Minghui Yang; Department of Orthopaedics and Traumatology, Peking University Fourth School of Clinical Medicine, Beijing, People’s Republic of China, Email [email protected] Xinbao Wu, Department of Orthopaedics and Traumatology, Peking University Fourth School of Clinical Medicine, Beijing, People’s Republic of China, Email [email protected]
Purpose: To assess the effect of orthogeriatric co-management care on the geriatric hip fracture patients with high ASA score.
Patients and Methods: A post-hoc analysis of a prospective multicenter study was done. Patients with an ASA score of 3 or 4 were selected from the database for analysis. Patients were divided into the orthogeriatric co-management group (CM group) and traditional consultation mode group (TC group) depending on the management mode. With mortality as the primary outcome, multivariate regression analyses were performed to adjust for confounders. Mobility and quality of life were compared between groups.
Results: A total of 628 patients were included, 593 of whom completed follow-up (388 in CM group, 205 in TC group). The in-hospital mortality, 30-day mortality, 120-day mortality in CM group were significantly lower than those in TC group after adjustment (P < 0.05). The difference of 1-year mortality in the two groups was not statistically significant after adjustment (P > 0.05). The surgical intervention rate, the early surgery rate, preoperative waiting time, hospital length of stay (LOS), 30-day mobility, 30-day EuroQol-5 Dimensions (EQ-5D) index, 30-day EuroQol-Visual Analog Scale (EQ-VAS), 120-day EQ-5D index, the total incidence of clinical adverse events, as well as deep vein thrombosis (DVT) and cardiac complication between the two groups were statistically significantly different after adjustment (P < 0.05). The difference of 120-day mobility was not statistically significant after adjustment (P < 0.05). There was no significant difference in the in-hospital total cost, the incidence of other clinical adverse events, 120-day EQ-VAS, 1-year reoperation rate, 1-year mobility, 1-year EQ-5D index, 1-year EQ-VAS between the two groups (P > 0.05).
Conclusion: Compared with the traditional consultation mode, orthogeriatric co-management care significantly reduced early mortality and enhanced early mobility and quality of life in geriatric hip fracture patients with high ASA score.
Keywords: geriatric hip fractures, orthogeriatric, ASA, mortality, mobility, quality of life
Introduction
With the increasing aging of the population, the number of geriatric hip fracture patients is increasing globally.1,2 The treatment of geriatric hip fracture is primarily early surgical intervention, with non-operative treatment being recommended by clinicians only in cases where the patient is unable to tolerate anesthesia and surgery.3–10 It should be noted that non-operative treatment is associated with a higher mortality rate for geriatric hip fracture patients.11,12
Comorbidity indices seek to reduce a person’s diseases and their severity to a score that allows comparison with other people. Given the existence of different methods for assessing comorbidity, four indices have been used for assessing comorbidity in elderly patients: the Charlson Comorbidity Index (CCI)13–15 -the most used, the Cumulative Illness Rating Scale for Geriatrics (CIRS-G),16 the Index of Co-Existent Disease (ICED)17 and the American Society of Anesthesiologists Physical Status Classification System (ASA)18 -whose application is practically universal in surgical services around the world.
Geriatric hip fracture patients often present with multiple comorbidities and inherently have a higher ASA score. Furthermore, acute hip fractures deal a significant blow to the elderly, leaving them bedridden and enduring severe pain, which can precipitously worsen their overall physical condition, and on occasion, it may even elevate their ASA score.19,20
Previous studies have emphasized the significance of ASA score in predicting the prognosis of geriatric hip fracture patients. Elevated ASA score is linked to increased postoperative mortality, postoperative complications, extended hospital stays, and overall costs,21–29 particularly when the ASA score exceeds 3.22,30–37 For orthopedic surgeons, managing geriatric hip fracture patients with high ASA score has always been a challenge.24
Orthogeriatric co-management care refers to the collaborative care of orthopedic and geriatric physicians in the daily diagnosis and treatment of geriatric trauma patients. Previous research has reported that orthogeriatric co-management care could significantly improve the prognosis of geriatric hip fracture patients,38–43 but there is currently a lack of research focused on the subgroup with high ASA score. The purpose of this study is to assess the effect of orthogeriatric co-management care on the geriatric hip fracture patients with high ASA score.
Patients and Methods
Study Design
This study was a post-hoc analysis of a prospective, multicenter quasi-experimental study, designed to assess the efficacy of co-management care for geriatric hip fracture patients in China.41 The original study enrolled hip fracture patients aged ≥65 years and were admitted to 6 hospitals in Beijing from November 2018 to November 2019. Among the participating hospitals, one had established a dedicated orthogeriatric unit, implementing an orthogeriatric co-management approach for the perioperative care of geriatric hip fracture patients. This hospital was designated as the orthogeriatric co-management care (CM) group. The remaining 5 hospitals continued with the traditional consultation mode and were designated as the traditional consultation mode(TC) group. For the purpose of this study, we focused on the subgroup of patients with ASA score of 3 or 4 from both groups, and then conducted a retrospective comparison to evaluate the effect of these two distinct care modes on patient outcomes.
The inclusion criteria: 1) Be 65 years or older; 2) Have a confirmed hip fracture (femoral neck, intertrochanteric, or subtrochanteric fracture) diagnosed by X-ray or CT scan; 3) Be admitted within 21 days from injury; 4) Have an ASA score of 3 or 4. The exclusion criteria: 1) Be diagnosed as neoplastic pathological fractures or peri-prosthesis fracture; 2) The ASA score was missing; 3) Have an ASA score of 1 or 2 or 5 or 6.
In this study, we excluded patients with ASA score of 1 and 2, as they were in relatively good overall health condition and did not align with the research objectives. And there were only 3 patients with an ASA score of 5 (moribund patient), which were also excluded to avoid confounder. There were no cases in this study with an ASA score of 6 (brain-dead patient). Therefore, patients with ASA score of 3 and 4 were screened in this study.
Intervention and Control
CM group: This group employed orthogeriatric co-management care. Upon admission, patients were directed to a dedicated orthogeriatric ward, co-managed by orthopedic and geriatric specialists. The mode emphasized early surgery (within 48 hours), comorbidity assessment, secondary fracture prevention, pressure sore avoidance, physical therapy, and expedited discharge. Geriatricians focused on comorbidity assessment and management, and secondary fracture prevention. Orthopedic surgeons handled surgical preparation and execution. Physical therapists and nutrition specialists, along with nurses, were also integral to perioperative care. The rehabilitation plan was collaboratively decided by the orthopedic surgeons and the physical therapists. Throughout the study, all patients at this hospital received co-management care in the orthogeriatric ward.
TC group: This group followed the traditional orthopedic care mode. Patients were admitted to orthopedic wards managed by orthopedic surgeons. The rehabilitation plan was primarily decided by orthopedic surgeon. Geriatricians, physical therapists and nutrition specialists can be consulted when necessary.
Data Collection and Outcome
In the original study, trained nurses were responsible for patients’ data collection at the baseline and follow-up. Recruited patients were followed up at three time points via telephone (30 days, 120 days, and 1 year post-admission). All data was established as a database. Patients with ASA score of 3 or 4 were selected from the database for analysis.
The primary outcome was mortality at in-hospital, 30-day, 120-day and 1-year. Secondary outcome variables encompassed surgical intervention rate, early surgery (within 48 hours) rate, preoperative waiting time, hospital length of stay (LOS), 1-year reoperation rate, in-hospital total cost, incidence of clinical adverse events (delirium, stroke, deep vein thrombosis (DVT), pneumonia, urinary tract infection, cardiac complications, and pressure ulcers), the mobility and quality of life at 30-day, 120-day and 1-year post-admission.
The EuroQol-5 Dimensions (EQ-5D) Questionnaire was employed to evaluate patients’ health-related quality of life (HRQoL). This tool systematically assesses HRQoL across five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is rated on a five-point scale, ranging from “no problems” to “unable to do/extreme problems”. The health status of these dimensions is quantified into an EQ-5D index value using a standardized scoring algorithm. Furthermore, the questionnaire included a 20-cm visual analog scale (VAS), enabling participants to self-assess their health status from 0 to 100 points (the worst to the best).
Statistical Analysis
Means with standard deviation (SD) or median with interquartile range (IQR) or proportion were used to describe patients’ data. Student’s t-test or Mann–Whitney U-test were adopted to test for continuous variables, while Chi-square test was adopted to test for categorical variables. Multiple logistic or linear regression was performed to adjust for confounders. Multivariate analysis included clinically meaningful variables (age, whether co-management care, ASA score) and statistically significant variables (living place, pre-fracture mobility, fracture type). Both the binary logistic regression and linear regression analyses were performed using the enter method. The multinomial logistic regression was fitted using a main effects model. Odds Ratios (OR), regression coefficient (b) and 95% confidence interval (95% CI) were calculated. Statistical analysis was performed using the IBM SPSS Statistical Package (version 25) (SPSS Inc., Chicago, IL, USA). All statistical significance was established at P < 0.05.
Results
A total of 628 geriatric hip fracture patients with an ASA score of 3 or 4 were recruited in this study, with 414 and 214 patients in the CM and TC groups, respectively. With 35 cases lost to follow-up, the mean follow-up rate was 94.43%, and there was no statistically significant difference between the two groups in follow-up rate (P = 0.283). The research flow chart is shown in Figure 1. The data of patients with complete follow-up were analyzed.
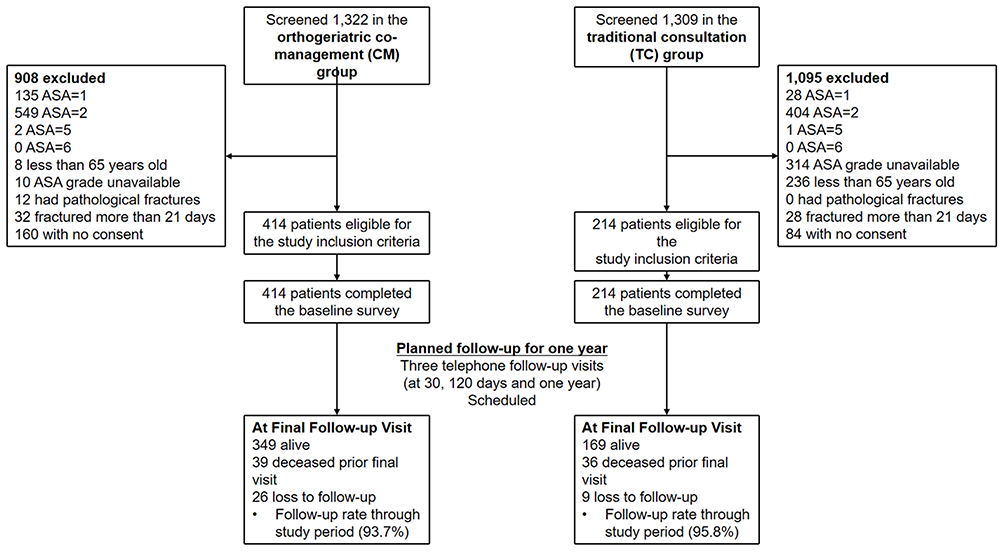 |
Figure 1 Research flow chart. |
The average age is 81.54 ± 7.30 years old. There was statistically significant difference in living place (P < 0.001), pre-fracture mobility (P < 0.001) and fracture type (P = 0.046). The baseline characteristics and the comparison between the two groups are presented in Table 1.
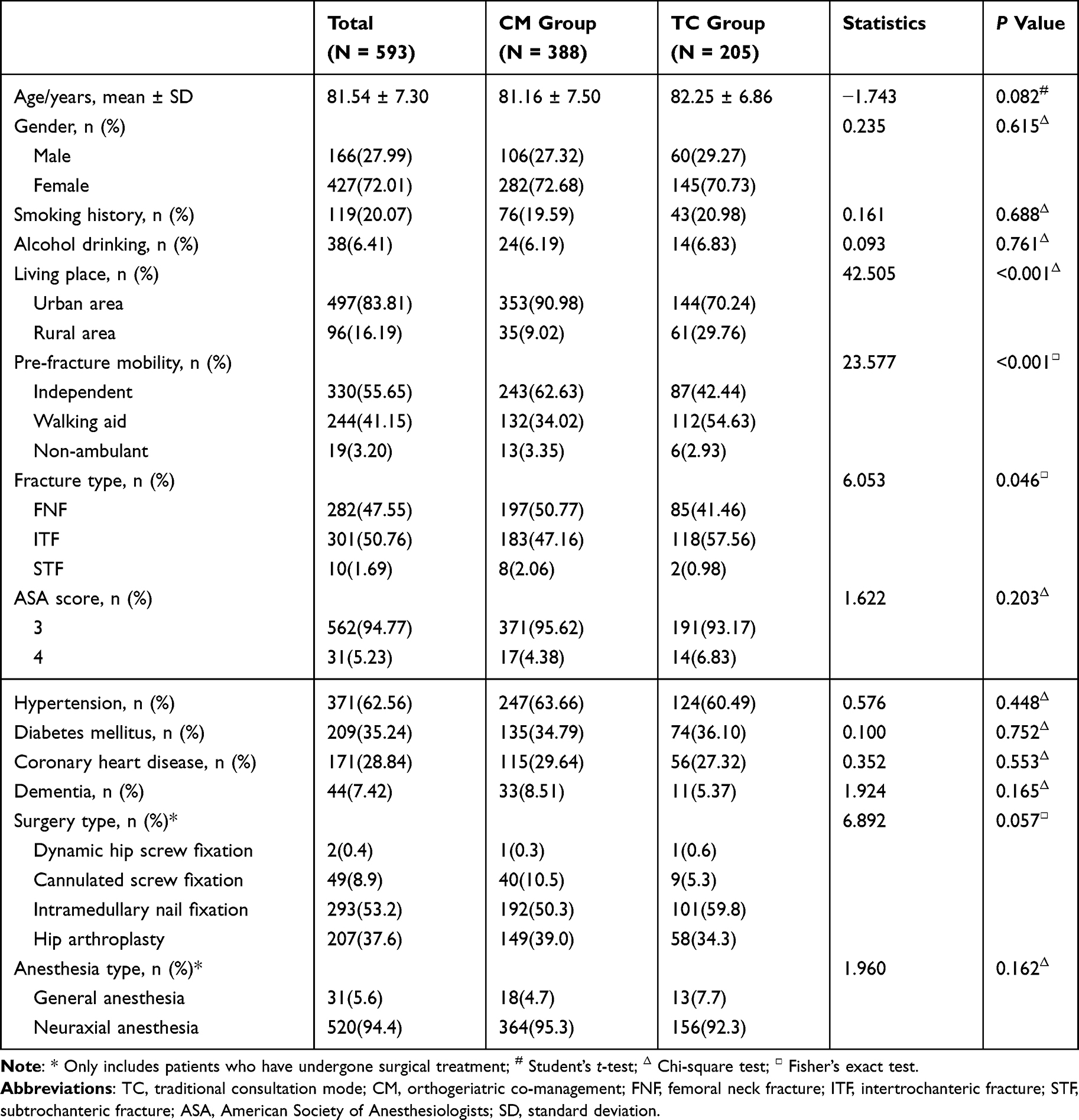 |
Table 1 Comparison of Baseline Characteristics |
The in-hospital mortality (0.26% vs 4.39%, P = 0.001), 30-day mortality (2.06% vs 7.80%, P = 0.001), 120-day mortality (5.41% vs 12.20%, P = 0.003) in CM group were significantly lower than those in TC group. After adjustment, there was still statistically significant difference between the two groups (P = 0.015, 0.008, 0.017). The 1-year mortality (10.05% vs 17.56%) in the two groups were also statistically significantly different (P = 0.009), but the difference was not statistically significant after adjustment (P = 0.065) (Table 2).
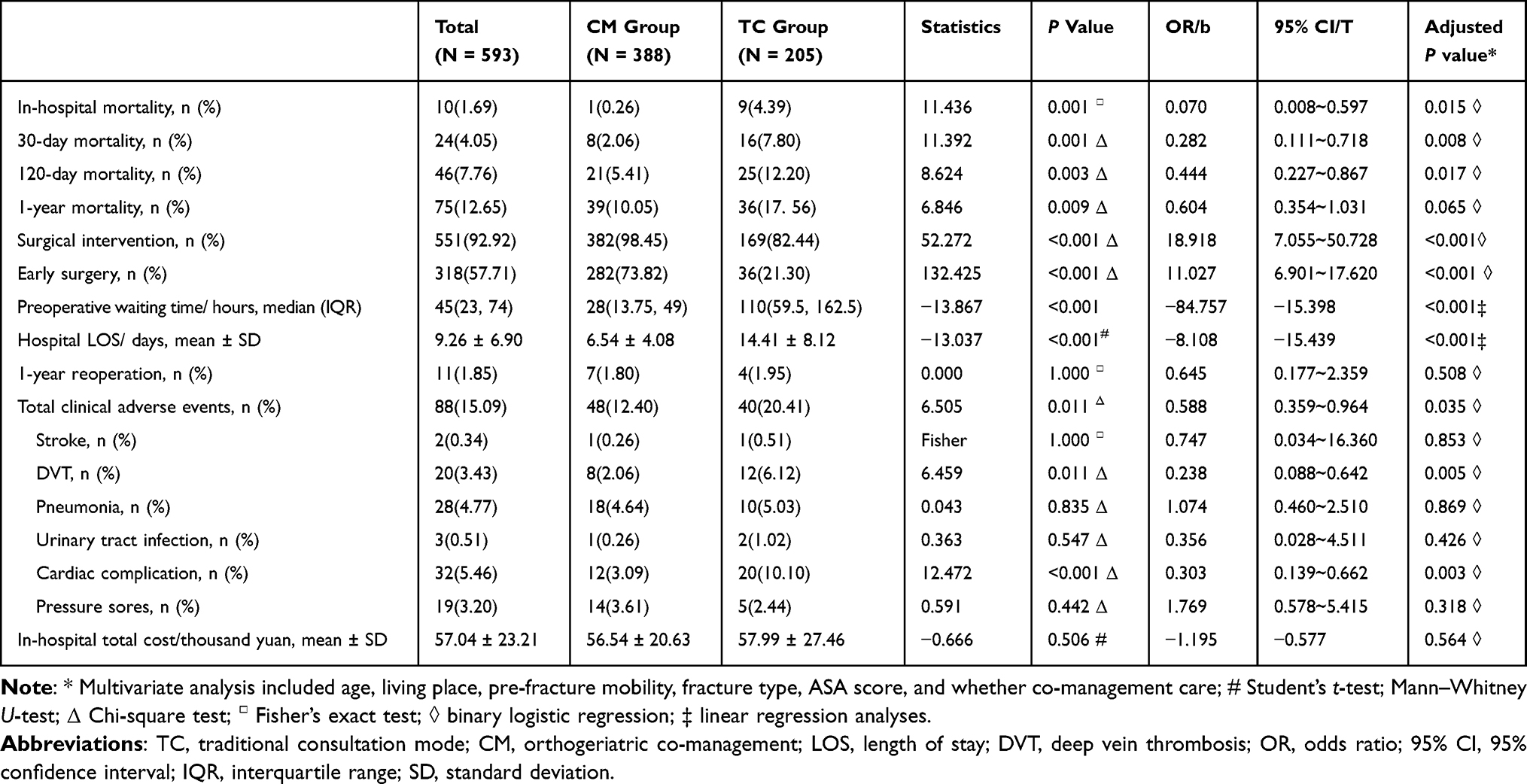 |
Table 2 Comparison of Major Outcome Variables |
The surgical intervention rate (98.45% vs 82.44%, P < 0.001), the early surgery rate (73.82% vs 21.30%, P < 0.001), preoperative waiting time (28 (13.75, 49) h vs 110 (59.5, 162.5) h, P < 0.001), hospital LOS (6.54 ± 4.08d vs 14.41 ± 8.12d, P < 0.001), 30-day mobility (independent: walking aid: non-ambulant 5.53%: 77.37%: 17.11% vs 2.65%: 49.74%: 47.62%, P < 0.001), 30-day EQ-5D index (0.57 ± 0.26 vs 0.38 ± 0.29, P < 0.001), 30-day EQ-VAS (70.14 ± 14.62 vs 62.20 ± 17.26), P < 0.001, 120-day EQ-5D index (0.74 ± 0.27 vs 0.64 ± 0.27, P < 0.001), the total incidence of clinical adverse events (12.40% vs 20.41%, P = 0.011), as well as DVT (2.06% vs 6.12%, P = 0.011) and cardiac complication (3.09% vs 10.10%, P < 0.001) between the two groups were statistically significantly different. And the difference was still statistically significant after adjustment (P < 0.05). The 120-day mobility (independent: walking aid: non-ambulant 20.71%: 69.48%: 9.81% vs 10.56%: 75.56%: 13.89%, P = 0.008) between the two groups was also statistically significantly different, but the difference was not statistically significant after adjustment (P = 0.138 and 0.538). There was no significant difference in the in-hospital total cost (P = 0.564), the incidence of other clinical adverse events (P > 0.05), 120-day EQ-VAS (P = 0.767), 1-year reoperation rate (P = 0.508), 1-year mobility (P = 0.178 and 0.292), 1-year EQ-5D index (P = 0.354), 1-year EQ-VAS (P = 0.063) between the two groups. Detailed data are shown in Table 2 and 3.
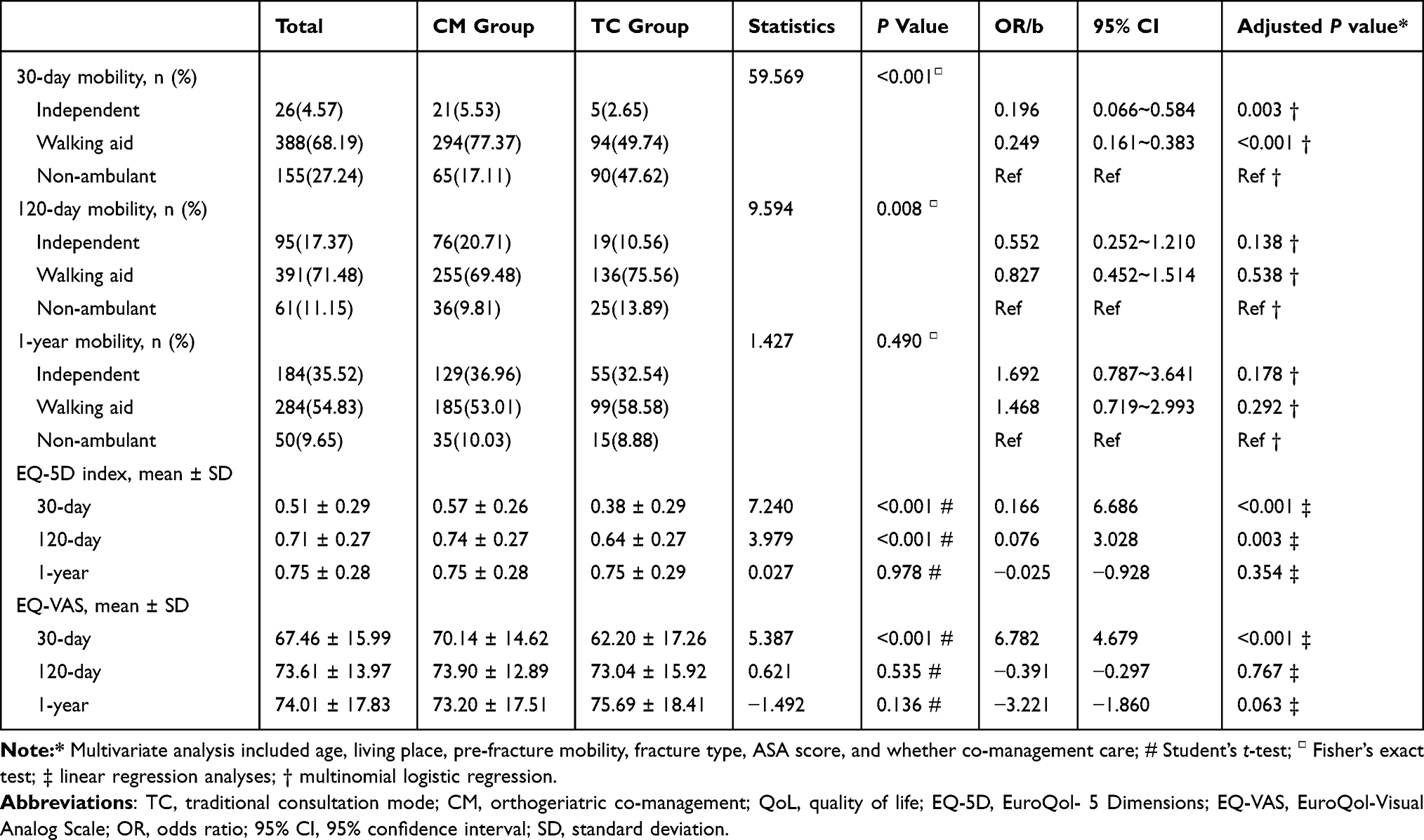 |
Table 3 Comparison of Mobility and QoL of Survived Patients at Follow-Up |
Discussion
Previous studies have explored the effect of orthogeriatric co-management on the general geriatric hip fracture population,41 and therefore, this study aims to delve deeper into the effect of orthogeriatric co-management on these patients with bad overall health condition. Given the constraints imposed by the available dataset, we were unable to secure a more objective metric, such as CCI,14,15 to assess the overall health status of the patients. Based on extensive international studies on ASA and geriatric hip fractures,26,29,44 which has showed that an ASA score ≥3 is a significant predictor of poor prognosis in geriatric hip fractures, we opted to employ the ASA score as a proxy, while acknowledging its inherent subjectivity in clinical practice.
In terms of the primary outcome, the results of this study suggest the orthogeriatric co-management care significantly reduces in-hospital, 30-day, and 120-day mortality rates among geriatric hip fracture patients with high ASA score, compared with the traditional consultation mode. This is consistent with the findings of other geriatric hip fracture patient groups in other studies.45,46 The reason is closely associated with geriatricians’ more meticulous and timely comorbidity management for elderly hip fracture patients with high ASA score. Geriatricians played an integral role in the management of elderly hip fracture patients, achieving a significant reduction in preoperative waiting time, and an increase in both the early surgery rate and the total surgical intervention rate, which are significantly associated with the prognosis of the elderly hip fracture patients.5–10 This also suggests that for geriatric hip fracture patients with high ASA, early surgery after detailed preoperative assessment and management does not increase the risk of death, thereby confirming the significance of early surgical intervention for this patient cohort. Furthermore, the management of geriatrics is also effectively realized a marked reduction in perioperative overall adverse events incidence including DVT and cardiac complications, which may also be associated with reduced early mortality under orthogeriatric co-management care. The study by G Kastanis et al 24 noted that the treatment of geriatric hip fracture patients with high ASA score requires a multidisciplinary approach and special evaluation to reduce mortality and provide optimal function, and this study confirms this conclusion. This study showed no significant difference in 1-year mortality between the two groups, which is not consistent with some previous studies in other populations of elderly hip fracture patients.37,47,48 The reason for the difference may be that our study only included patients with higher ASA score, which have higher natural mortality and shorter natural life span, and these studies included a general population of geriatric hip fracture patients.37,47,48
This study demonstrated significant improvements in 30-day mobility among geriatric hip fracture patients under orthogeriatric co-management care, which is also better than the results of previous study,49 likely due to higher rates of early and overall surgery, more meticulous comorbidity management, better prevention of perioperative adverse events, and more timely rehabilitation guidance. While patients under this care mode also showed higher mobility at 120 days, the difference was not statistically significant after adjustment, and there was no significant difference in mobility between the two groups at 1 year, which is consistent with the expected natural recovery trajectory following geriatric hip fractures. Both the fracture and mobility typically recover by 1 year. In this study, 9.3% of elderly hip fracture patients were non-ambulant at the one-year mark, which is essentially consistent with the 13.3% reported in previous study.50 Due to the lack of data on pre-injury mobility, it is difficult to determine whether the patients’ mobility has returned to pre-injury levels, which depends on future research.
The orthogeriatric co-management care in this study led to significant improvements in the 30-day and 120-day quality of life for surviving patients. Research by Amarilla-Donoso FJ et al demonstrated that the geriatric hip fracture patients of traditional orthopedic ward could achieve an EQ-5D index of 0.16 ± 0.20, and an EQ-VAS of 48.3 ± 17.2 at 1 month after surgery,49 worse than the results in this study. This enhancement is likely attributed to the meticulous management of comorbidities and the effective prevention of perioperative adverse events in orthogeriatric co-management care. Similar to mobility, the quality of life at the 1-year mark showed a tendency towards consistency between the two groups, which may be also associated with the complete healing of the hip fracture.
In this study, the 1-year reoperation rate of 1.85% was notably lower than the rates reported in previous research, which ranged from 7% to 13%.51–55 This reduction may be attributed to the lower need in the elderly with multiple comorbidities, coupled with their increased vulnerability to surgical risks, thus making them more inclined to evade a second surgery. The LOS in this study was shorter under orthogeriatric co-management care, which was in line with previous studies.39,42 This suggests that the orthogeriatric co-management care, which advocates for early discharge, can effectively enhance the utilization of medical resources. It is important to note that the orthogeriatric co-management care does not impose an additional financial burden on the patients in this study, which is consistent with the results of previous studies.56
This study represents a pioneering effort as the first multicenter, prospective, and controlled study to meticulously assess the efficacy of orthogeriatric co-management care specifically for elderly hip fracture patients who have an ASA score of 3 or 4. The findings are poised to furnish guidance for the management of these geriatric hip fracture, while also providing pivotal evidence for the advancement of orthogeriatric co-management care in China. Despite the methodological rigor employed in this study, including the use of multivariate analysis to mitigate confounding biases, several limitations warrant acknowledgment: (1) The ASA score, being somewhat subjective, may introduce biases in patient assessment; (2) The study design is prospective but not randomized; (3) The composition of the study groups, with the CM group encompassing a single hospital and TC group comprising five hospitals of different calibers, introduces potential center-effect biases; (4) Fewer patients were included in the post hoc analysis, which may reduce statistical power, especially for outcomes with low incidence; (5) The outcome assessment was conducted by telephone, which may not be reliable and may introduce bias; (6) There may be some factors in the overall management of patients that cannot be quantified, such as surgical and anesthesia techniques, surgeon’s surgical details, surgical instruments, anesthesia drugs, development and implementation of the rehabilitation protocols, etc., which may lead to bias. It is imperative that the conclusions drawn from this study need to be corroborated through additional large-scale, multicenter, controlled trials with more objective metric to assess the overall health status and more detailed follow-up. It should be emphasized the quest for the optimal management paradigm is still ongoing, necessitating further exploration and improvement.
Conclusion
Compared with the traditional consultation mode, orthogeriatric co-management care significantly reduced early mortality and enhanced early mobility and quality of life in geriatric hip fracture patients with high ASA score.
Abbreviations
TC, traditional consultation mode; CM, orthogeriatric co-management; FNF, femoral neck fracture; ITF, intertrochanteric fracture; STF, subtrochanteric fracture; ASA, American Society of Anesthesiologists; LOS, length of stay; DVT, deep vein thrombosis; QoL, quality of life; EQ-5D, EuroQol-5 Dimensions; EQ-VAS, EuroQol-Visual Analog Scale; OR, odds ratio; 95% CI, 95% confidence interval; SD, standard deviation; IQR, interquartile range.
Data Sharing Statement
The datasets used in this study are not publicly available because of patient confidentiality but are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
Approval was obtained from the Institutional Review Board at Peking University Health Science Centre (IRBo0001052-17021) and Biomedical Ethics Committee at 6 center Hospital: Beijing Jishuitan Hospital, Capital Medical University (201807-11); Beijing Hospital (2018BJYYEC-130-01); Beijing Anzhen Hospital, Capital Medical University (Relied on the approval from the lead center, thus no separate number was issued); Beijing Changping District Hospital (2018-GK-001-A); Beijing Fangshan District Liangxiang Hospital (201690); Beijing Changping District Hospital (Relied on the approval from the lead center, thus no separate number was issued). All procedures used adhere to the tenets of the Declaration of Helsinki. Informed consent was obtained from all individual participants included in the study.
Acknowledgments
We sincerely thank all participants and researchers of this study for their invaluable contributions. We extend our sincere gratitude to the following colleagues for their contributions to data collection: Jing Zhang, Jiusheng He, Liangyuan Wen, Xianhai Wang, Zongxin Shi, Sanbao Hu, Fengpo Sun, Zishun Gong, Mingyao Sun, Maoyi Tian.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Capital’s Funds for Health Improvement and Research (2022-1-2071, 2018-1-2071), Beijing Scholar Training Program 2021, the National Natural Science Foundation of China (No. 82372386), and Beijing JST Research Funding (YGQ-202214).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sing CW, Lin TC, Bartholomew S, et al. Global epidemiology of hip fractures: secular trends in incidence rate, post-fracture treatment, and all-cause mortality. J Bone Miner Res. 2023;38(8):1064–1075. doi:10.1002/jbmr.4821
2. Hawley S, Dela S, Burton A, Paruk F, Cassim B, Gregson CL. Incidence and number of fragility fractures of the Hip in South Africa: estimated projections from 2020 to 2050. Osteoporos Int. 2022;33(12):2575–2583. doi:10.1007/s00198-022-06525-5
3. Quinn RH, Mooar PA, Murray JN, Pezold R, Sevarino KS. Treatment of hip fractures in the elderly. J Am Acad Orthop Surg. 2017;25(5):e102–e104. doi:10.5435/JAAOS-D-16-00431
4. Bhandari M, Swiontkowski M. Management of acute hip fracture. N Engl J Med. 2017;377(21):2053–2062. doi:10.1056/NEJMcp1611090
5. Loggers SAI, Van Lieshout EMM, Joosse P, Verhofstad MHJ, Willems HC. Prognosis of nonoperative treatment in elderly patients with a Hip fracture: a systematic review and meta-analysis. Injury. 2020;51(11):2407–2413. doi:10.1016/j.injury.2020.08.027
6. Shah A, Matharu GS, Inman D, Fagan E, Johansen A, Judge A. Variation in timely surgery for hip fracture by day and time of presentation: a nationwide prospective cohort study from the national hip fracture database for England, Wales and Northern Ireland. BMJ Qual Saf. 2021;30(7):559–566. doi:10.1136/bmjqs-2020-011196
7. Shiga T, Wajima Z, Ohe Y. Is operative delay associated with increased mortality of Hip fracture patients? Systematic review, meta-analysis, and meta-regression. Canad J Anaesthes J Canad D’anesthesie. 2008;55(3):146–154. doi:10.1007/BF03016088
8. Simunovic N, Devereaux PJ, Sprague S, et al. Effect of early surgery after Hip fracture on mortality and complications: systematic review and meta-analysis. Cmaj. 2010;182(15):1609–1616. doi:10.1503/cmaj.092220
9. Moja L, Piatti A, Pecoraro V, et al. Timing matters in Hip fracture surgery: patients operated within 48 hours have better outcomes. A meta-analysis and meta-regression of over 190,000 patients. PLoS One. 2012;7(10):e46175. doi:10.1371/journal.pone.0046175
10. Bottle A, Aylin P. Mortality associated with delay in operation after Hip fracture: observational study. BMJ. 2006;332(7547):947–951. doi:10.1136/bmj.38790.468519.55
11. van de Ree CLP, De Jongh MAC, Peeters MAC, et al. Hip fractures in elderly people: surgery or no surgery? a systematic review and meta-analysis. Geriatr Orthop Surg Rehabil. 2017;8(3):173–180. doi:10.1177/2151458517713821
12. Lewis SR, Macey R, Stokes J, Cook JA, Eardley WG, Griffin XL. Surgical interventions for treating intracapsular Hip fractures in older adults: a network meta-analysis. Cochrane Database Syst Rev. 2022;2(2):Cd013404. doi:10.1002/14651858.CD013404.pub2
13. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
14. Stewart NA, Chantrey J, Blankley SJ, Boulton C, Moran CG. Predictors of 5 year survival following Hip fracture. Injury. 2011;42(11):1253–1256. doi:10.1016/j.injury.2010.12.008
15. Hernández-Pascual C, Santos-Sánchez J, Hernández-Rodríguez J, et al. Partial weight bearing and long-term survival outcomes in extracapsular Hip fractures treated with trochanteric Gamma3 nails. BMC Musculoskelet Disord. 2025;26(1):129. doi:10.1186/s12891-024-08043-3
16. Miller MD, Paradis CF, Houck PR, et al. Rating chronic medical illness burden in geropsychiatric practice and research: application of the cumulative illness rating scale. Psychiatry Res. 1992;41(3):237–248. doi:10.1016/0165-1781(92)90005-N
17. Cleary PD, Greenfield S, Mulley AG, et al. Variations in length of stay and outcomes for six medical and surgical conditions in Massachusetts and California. JAMA. 1991;266(1):73–79. doi:10.1001/jama.1991.03470010077034
18. Horvath B, Kloesel B, Todd MM, Cole DJ, Prielipp RC. The evolution, current value, and future of the American Society of Anesthesiologists Physical Status Classification System. Anesthesiology. 2021;135(5):904–919. doi:10.1097/ALN.0000000000003947
19. Rodriguez-Fernandez P, Adarraga-Cansino D, Carpintero P. Effects of delayed Hip fracture surgery on mortality and morbidity in elderly patients. Clin Orthop Relat Res. 2011;469(11):3218–3221. doi:10.1007/s11999-010-1756-z
20. Zhang P, Li X, Yuan Y, et al. Risk factor analysis for in-hospital death of geriatric Hip fracture patients. Saudi med j. 2022;43(2):197–201. doi:10.15537/smj.2022.43.2.20210717
21. Haugan K, Klaksvik J, Foss OA. 30-day mortality in patients after Hip fracture surgery: a comparison of the Charlson Comorbidity Index score and ASA score used in two prediction models. Injury. 2021;52(8):2379–2383. doi:10.1016/j.injury.2021.02.004
22. Lizaur-Utrilla A, Serna-Berna R, Lopez-Prats FA, Gil-Guillen V. Early rehospitalization after Hip fracture in elderly patients: risk factors and prognosis. Arch Orthop Trauma Surg. 2015;135(12):1663–1667. doi:10.1007/s00402-015-2328-1
23. Varady NH, Gillinov SM, Yeung CM, Rudisill SS, Chen AF. The charlson and elixhauser scores outperform the American Society of Anesthesiologists score in assessing 1-year mortality risk after hip fracture surgery. Clin Orthop Relat Res. 2021;479(9):1970–1979. doi:10.1097/CORR.0000000000001772
24. Kastanis G, Topalidou A, Alpantaki K, Rosiadis M, Balalis K. Is the ASA score in geriatric hip fractures a predictive factor for complications and readmission? Scientifica. 2016;2016:7096245. doi:10.1155/2016/7096245
25. Michel JP, Klopfenstein C, Hoffmeyer P, Stern R, Grab B. Hip fracture surgery: is the pre-operative American Society of Anesthesiologists (ASA) score a predictor of functional outcome? Aging Clin Exp Res. 2002;14(5):389–394. doi:10.1007/BF03324467
26. Al-Husinat L, Azzam S, Sharie SA, et al. Impact of the American Society of Anesthesiologists (ASA) classification on Hip fracture surgery outcomes: insights from a retrospective analysis. BMC Anesthesiol. 2024;24(1):271. doi:10.1186/s12871-024-02660-0
27. Liu Y, Peng M, Lin L, Liu X, Qin Y, Hou X. Relationship between American Society of Anesthesiologists (ASA) grade and 1-year mortality in nonagenarians undergoing Hip fracture surgery. Osteoporos Int. 2015;26(3):1029–1033. doi:10.1007/s00198-014-2931-y
28. Meyer AC, Eklund H, Hedström M, Modig K. The ASA score predicts infections, cardiovascular complications, and hospital readmissions after Hip fracture - A nationwide cohort study. Osteoporos Int. 2021;32(11):2185–2192. doi:10.1007/s00198-021-05956-w
29. Smith T, Pelpola K, Ball M, Ong A, Myint PK. Pre-operative indicators for mortality following Hip fracture surgery: a systematic review and meta-analysis. Age Ageing. 2014;43(4):464–471. doi:10.1093/ageing/afu065
30. Nkanang B, Parker M, Parker E, Griffiths R. Perioperative mortality for patients with a Hip fracture. Injury. 2017;48(10):2180–2183. doi:10.1016/j.injury.2017.07.007
31. Endo Y, Aharonoff GB, Zuckerman JD, Egol KA, Koval KJ. Gender differences in patients with Hip fracture: a greater risk of morbidity and mortality in men. J Orthop Trauma. 2005;19(1):29–35. doi:10.1097/00005131-200501000-00006
32. Hamlet WP, Lieberman JR, Freedman EL, Dorey FJ, Fletcher A, Johnson EE. Influence of health status and the timing of surgery on mortality in Hip fracture patients. Am J Orthop. 1997;26(9):621–627.
33. Pereira SR, Puts MT, Portela MC, Sayeg MA. The impact of prefracture and Hip fracture characteristics on mortality in older persons in Brazil. Clin Orthop Relat Res. 2010;468(7):1869–1883. doi:10.1007/s11999-009-1147-5
34. Vaseenon T, Luevitoonvechkij S, Wongtriratanachai P, Rojanasthien S. Long-term mortality after osteoporotic Hip fracture in Chiang Mai, Thailand. J Clin Densitom. 2010;13(1):63–67. doi:10.1016/j.jocd.2009.10.003
35. Min L, Linyi Y, Chen L, Jiang S, Chen C. Preoperative moderate to severe anemia is associated with increased postoperative major adverse cardiac and cerebral events and pulmonary complications: a propensity score-matched analysis in Hip fracture surgery patients over 80 years old. Perioperative Med. 2023;12(1):56. doi:10.1186/s13741-023-00349-5
36. Geleit R, Bence M, Samouel P, Craik J. Biomarkers as predictors of inpatient mortality in fractured neck of femur patients. Arch Gerontol Geriatr. 2023;111:105004. doi:10.1016/j.archger.2023.105004
37. Folbert EC, Hegeman JH, Vermeer M, et al. Improved 1-year mortality in elderly patients with a Hip fracture following integrated orthogeriatric treatment. Osteoporos Int. 2017;28(1):269–277. doi:10.1007/s00198-016-3711-7
38. Folbert EC, Hegeman JH, Gierveld R, et al. Complications during hospitalization and risk factors in elderly patients with Hip fracture following integrated orthogeriatric treatment. Arch Orthop Trauma Surg. 2017;137(4):507–515. doi:10.1007/s00402-017-2646-6
39. Van Heghe A, Mordant G, Dupont J, Dejaeger M, Laurent MR, Gielen E. Effects of orthogeriatric care models on outcomes of hip fracture patients: a systematic review and meta-analysis. Calcif Tissue Int. 2022;110(2):162–184. doi:10.1007/s00223-021-00913-5
40. Grigoryan KV, Javedan H, Rudolph JL. Orthogeriatric care models and outcomes in Hip fracture patients: a systematic review and meta-analysis. J Orthop Trauma. 2014;28(3):e49–55. doi:10.1097/BOT.0b013e3182a5a045
41. Zhang J, Yang M, Zhang X, et al. The effectiveness of a co-management care model on older Hip fracture patients in China - A multicentre non-randomised controlled study. Lancet Reg Health West Pac. 2022;19:100348. doi:10.1016/j.lanwpc.2021.100348
42. Gao F, Liu G, Ge Y, et al. Orthogeriatric co-managements lower early mortality in long-lived elderly Hip fracture: a post-hoc analysis of a prospective study. BMC Geriatr. 2023;23(1):571. doi:10.1186/s12877-023-04289-z
43. Bugaevsky Y, Levy Y, Hershkovitz A, et al. Characteristics and outcomes of hip fracture patients hospitalized in an orthogeriatric unit versus an orthopedic department: a retrospective cohort study. Geriatr Orthop Surg Rehabil. 2021;12:2151459320986299. doi:10.1177/2151459320986299
44. Kivrak S, Haller G. Scores for preoperative risk evaluation of postoperative mortality. Best Pract Res Clin Anaesth. 2021;35(1):115–134. doi:10.1016/j.bpa.2020.12.005
45. Ekmann A, Jensen TG, Kristensen MT, et al. Readmission and mortality before and after introduction of orthogeriatric home visits: a retrospective cohort study in Hip fracture patients. Injury. 2024;55(12):111937. doi:10.1016/j.injury.2024.111937
46. Yee DKH, Lau TW, Fang C, Ching K, Cheung J, Leung F. Orthogeriatric multidisciplinary co-management across acute and rehabilitation care improves length of stay, functional outcomes and complications in geriatric hip fracture patients. Geriatr Orthop Surg Rehabil. 2022;13:21514593221085813. doi:10.1177/21514593221085813
47. Chen CH, Huang PJ, Huang HT, et al. Impact of orthogeriatric care, comorbidity, and complication on 1-year mortality in surgical Hip fracture patients: an observational study. Medicine. 2019;98(47):e17912. doi:10.1097/MD.0000000000017912
48. van Leendert JAA, Linkens A, Poeze M, et al. Mortality in Hip fracture patients after implementation of a nurse practitioner-led orthogeriatric care program: results of a 1-year follow-up. Age Ageing. 2021;50(5):1744–1750. doi:10.1093/ageing/afab031
49. Amarilla-Donoso FJ, López-Espuela F, Roncero-Martín R, et al. Quality of life in elderly people after a Hip fracture: a prospective study. Health Qual Life Outcomes. 2020;18(1):71. doi:10.1186/s12955-020-01314-2
50. Iosifidis M, Iliopoulos E, Panagiotou A, Apostolidis K, Traios S, Giantsis G. Walking ability before and after a Hip fracture in elderly predict greater long-term survivorship. J Orthop Sci. 2016;21(1):48–52. doi:10.1016/j.jos.2015.09.009
51. French DD, Bass E, Bradham DD, Campbell RR, Rubenstein LZ. Rehospitalization after Hip fracture: predictors and prognosis from a national veterans study. J Am Geriatr Soc. 2008;56(4):705–710. doi:10.1111/j.1532-5415.2007.01479.x
52. Lin JC, Liang WM. Mortality, readmission, and reoperation after Hip fracture in nonagenarians. BMC Musculoskelet Disord. 2017;18(1):144. doi:10.1186/s12891-017-1493-5
53. Radcliff TA, Henderson WG, Stoner TJ, Khuri SF, Dohm M, Hutt E. Patient risk factors, operative care, and outcomes among older community-dwelling male veterans with Hip fracture. J Bone Joint Surg Am. 2008;90(1):34–42. doi:10.2106/JBJS.G.00065
54. Giusti A, Barone A, Razzano M, Pizzonia M, Oliveri M, Pioli G. Predictors of hospital readmission in a cohort of 236 elderly discharged after surgical repair of Hip fracture: one-year follow-up. Aging Clin Exp Res. 2008;20(3):253–259. doi:10.1007/BF03324779
55. Buecking B, Eschbach D, Koutras C, et al. Re-admission to Level 2 unit after Hip-fracture surgery - Risk factors, reasons and outcome. Injury. 2013;44(12):1919–1925. doi:10.1016/j.injury.2013.05.012
56. Prestmo A, Hagen G, Sletvold O, et al. Comprehensive geriatric care for patients with Hip fractures: a prospective, randomised, controlled trial. Lancet. 2015;385(9978):1623–1633. doi:10.1016/S0140-6736(14)62409-0
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.