Back to Journals » Open Access Emergency Medicine » Volume 18
Organizational Challenges and Emergency Response to a Massive Bee Attack on an Isolated Island in French Guiana
Authors Marlier J, Mutricy R, Kallel H, Deschamps C, Fremery A ![]()
Received 15 July 2025
Accepted for publication 27 January 2026
Published 18 March 2026 Volume 2026:18 553868
DOI https://doi.org/10.2147/OAEM.S553868
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Julien Marlier,1,* Rémi Mutricy,1,* Hatem Kallel,2 Camille Deschamps,1 Alexis Fremery1
1Emergency Department, Centre Hospitalier Universitaire de Guyane, Cayenne, Guyane Française, France; 2Intensive Care Unit, Centre Hospitalier Universitaire de Guyane, Cayenne, Guyane Française, France
*These authors contributed equally to this work
Correspondence: Alexis Fremery, Emergency Department, Centre Hospitalier Universitaire de Guyane, Avenue Alexis Blaise, Cayenne, Guyane Française, 97300, France, Email [email protected]
Introduction: In 2023, close to Cayenne, French Guiana, a significant attack by africanized honey bees struck a group of 35 tourists on an isolated island, with no available means of rescue.
Event Description: The incident resulted in 1 death, 2 critical emergencies, 6 moderate emergencies, and a total of 11 emergency room admissions, involving both adults and children.
Discussion: Analysis of challenges encountered that day, particularly in aerial and nautical operations, will help improve our emergency response and healthcare systems in our overseas territories.
Keywords: Africanized honey bees, exceptional health situation, massive attack, hymenoptera envenomation, emergency medicine
Introduction
French Guiana’s geographical isolation and limited healthcare resources shape the daily practice of emergency physicians, particularly when managing envenomations and environmental injuries.1 Hymenoptera stings represent a common cause of consultation in the region, with several dozen cases reported each year, although severe attacks remain rare.2,3 Africanized honeybees, introduced accidentally in Brazil in 1956,4 have progressively colonized the entire Amazonian basin. Their well-documented aggressiveness and tendency to inflict massive stings have led to numerous multi-victim events across South and Central America over the past decades.5 In this context, large-scale attacks pose specific challenges for prehospital and hospital systems, especially in isolated environments where communication, transport, and coordination capacities are limited. We report a mass-casualty bee envenomation event occurring on a remote islet in French Guiana and describe the organizational and medical difficulties encountered during the response.
Ethics
This retrospective case series was based on anonymized data routinely collected in the emergency department. In accordance with French law (Loi Jardé) and institutional policy, ethics committee approval was not required, as the study did not involve any intervention or identifiable personal data. The project was declared to the hospital’s Data Protection Officer and registered in the institutional data registry.
Event Description
On August 22, 2023, around 11:30 a.m., a wild swarm of approximately 80,000 bees (later estimated by an independent local beekeeping specialist) attacked 34 tourists on a small uninhabited island located 11 kilometers from the nearest port. At 11:36 a.m., the fire department’s call center received the first alert. At 12:51 p.m., the first Mobile Emergency and Resuscitation Service (SMUR) team arrived at Dégrad des Cannes harbor (Figure 1). Due to the unavailability of aerial resources, the SMUR team was split into two groups and reached the site by pleasure boats after a 45-minute journey. Although the attack had slowed, it was still ongoing. The initial overall assessment reported 33 moderate emergencies and 1 fatality (Figure 2). No medical care was provided on-site, apart from cardiopulmonary resuscitation.
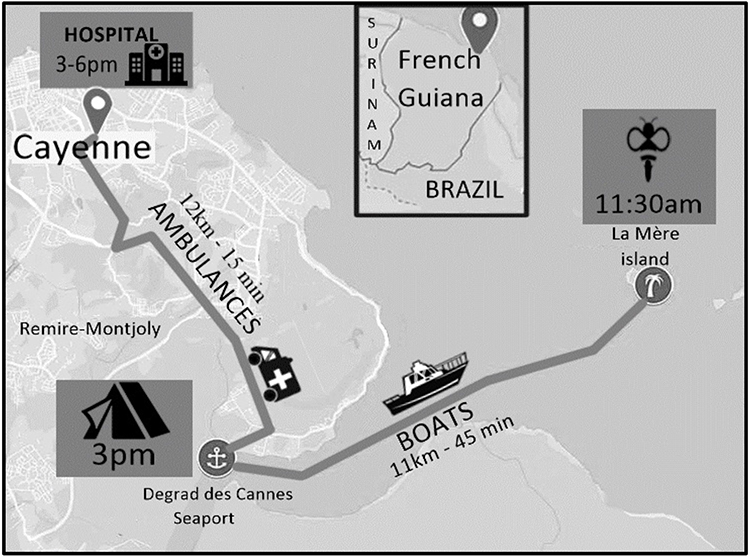 |
Figure 1 Medical evacuation mapping. |
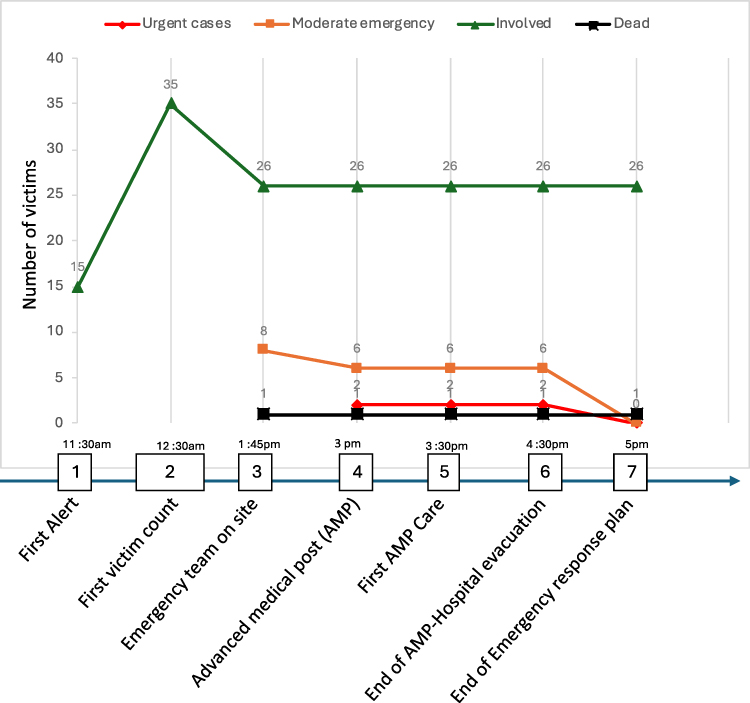 |
Figure 2 Evolution of the casualty toll. |
At the seaport, the Advanced Medical Post (AMP) became operational at 3:00 p.m. The Medical-Psychological Emergency Cell (MPEC) deployed two units: one at the AMP and another at the hospital. At the AMP, victims were reclassified into 2 urgent cases, 6 moderate emergencies, and 25 involved individuals. Some of the injured received intravenous fluids and low-dose adrenaline. A large-scale shuttle system transported around fifteen victims to the hospital, either to the emergency department or to the MPEC. In the emergency department, the injured were treated with corticosteroids and antihistamines for allergy relief, and bee stingers were removed. The deceased victim suffered over 1,500 stings, the 2 urgent cases around 500 stings each, and the moderate cases fewer than 50. Children presented with more severe symptoms, including malaise, apathy, pallor, and hemodynamic instability. Biologically, the envenomation resulted in renal failure and elevated troponin levels, followed by rhabdomyolysis and significant liver dysfunction. None of the patients required vasopressor support. Four individuals were hospitalized for more than 24 hours. The victims were managed at the Cayenne Hospital Center, the largest and only tertiary referral hospital in French Guiana. This non-seasonal 510-bed facility provides 24/7 emergency, intensive care, and specialized medical services, despite serving a vast and sparsely populated territory with limited critical care resources compared to mainland France.
Discussion
The final assessment reported 1 death, 2 urgent cases, 6 moderate emergencies, and 25 involved individuals. Debriefings were organized by the police headquarters, the emergency call center, the fire department, and beekeeping specialists to address the various issues encountered during the response.
First, telecommunications revealed significant vulnerabilities. In late August, malfunctions in the Guianese electrical network caused disruptions in telephony services. Consequently, several emergency calls failed due to operator faults. Moreover, due to poor network coverage on Îlet La Mère, most calls were unusable. One proposed solution was to deploy a secondary emergency telecommunications network.
Another challenge was the lack of organization prior to the rescuers’ arrival. Tourist agencies were inadequately trained in supervision, and no signage was available on the island to instruct visitors on how to respond. Additionally, the heliport was not cleared. Post-event debriefings identified the need to remind tourism professionals of the protocols for contacting marine rescue services in an emergency and to reorganize helicopter landing zones for future operations.
In French Guiana, maritime interventions are rare, and responders lack the appropriate resources. Coincidentally, neither the SAMU’s private helicopter, the Civil Security’s, nor the Air Force’s was available at the time (due to ongoing missions or maintenance). Ultimately, the law enforcement helicopter was mobilized, although it was not suited for medical support. Maritime mutual aid proved essential in facilitating the rapid evacuation of victims. Following the incident, authorities recommended the development of a protocol for maritime emergency responses and the establishment of a dedicated marine rescue unit in the area.
In the emergency department, several challenges also emerged. The first concerned the patient flow management software, which was unable to provide reliable tracking of patient numbers and locations. Furthermore, the medical teams lacked sufficient knowledge of the hospital’s emergency response plan, leading to some confusion. Efforts are underway to adapt the new software for future mass-casualty events.
The medical treatments administered also warrant discussion. Massive bee envenomation involves several venom components, chiefly melittin, the main cytolytic peptide, and also apamin, a minor neurotoxic constituent. This clinical presentation is an emerging nosological entity (ICD-10 classification: T63.4 - Toxic effect of venom of other arthropods). To date, the pathophysiological mechanisms remain poorly understood,6 and no standardized treatment protocol exists. Schmidt’s classification,7 based on the sting-to-body-weight ratio, estimates the direct cytotoxicity of the injected venom but fails to account for individual anaphylactoid reactions. Finally, the role of adrenaline in cases of massive hymenoptera envenomation requires further evaluation.
Data Sharing Statement
The collected data are available upon reasonable request from the corresponding author.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Epelboin L, Abboud P, Abdelmoumen K, et al. Panorama des pathologies infectieuses et non infectieuses de Guyane en 2022. Méd Trop Santé Int. 2023;3(1). doi:10.48327/mtsi.v3i1.2023.308
2. Castro PHC, Paiva ALB, Peixoto GVM, Oliveira-Mendes BBR, Calaça P, Matavel A. Epidemiology of arthropods envenomation in Brazil: a public health issue. An Acad Bras Cienc. 2023;95(suppl 1):e20220850. doi:10.1590/0001-3765202320220850
3. Maurer J, Mutricy R, Negrello F, et al. Epidemiology and management of wildlife contacts in an emergency department of French Guiana. PLoS Negl Trop Dis. 2025;19(12):e0013771. doi:10.1371/journal.pntd.0013771
4. Kerr WE. The history of the introduction of African bees in Brazil. South African Bee J. 1967;39:33–4
5. Geoffroy S, Lambert Y, Fremery A, Marty C, André N. Case report: « killer bee » swarm attacks in french guiana: the importance of prompt care. Am J Trop Med Hyg. 2021;105(1):
6. Geoffroy S, Fremery A, Lambert Y, Marty C, Elenga N. Case report: acute kidney failure due to massive envenomation of a two-year-old child caused by killer bee stings. Am J Trop Med Hyg. 2021;105(1):
7. Schmidt JO. Clinical consequences of toxic envenomations by Hymenoptera. Toxicon off J Int Soc Toxinol. 2018;150:
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.