Back to Journals » International Medical Case Reports Journal » Volume 19
Orbital Myiasis Secondary to Neglected Maxillary Sinus Squamous Cell Carcinoma in an 85-Year-Old Woman: A Case Report
Authors Trung NL ![]() , Ngan ND
, Ngan ND ![]() , Mai PT, Manh NT
, Mai PT, Manh NT
Received 18 December 2025
Accepted for publication 19 February 2026
Published 27 February 2026 Volume 2026:19 585599
DOI https://doi.org/10.2147/IMCRJ.S585599
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Giuseppe Giannaccare
Nguyen Le Trung,1 Nguyen Dinh Ngan,1 Pham Thi Mai,2 Ngo The Manh3
1Department of Ophthalmology, Military Medical University, Hanoi, Vietnam; 2Department of Oncology, Military Medical University, Hanoi, Vietnam; 3Department of Maxillofacial and Reconstructive Surgery, Military Medical University, Hanoi, Vietnam
Correspondence: Nguyen Le Trung, Email [email protected]
Background: Orbital myiasis is a rare and destructive infestation caused by fly larvae, often associated with chronic ulcerative lesions or malignancies in the head and neck region.
Case Presentation: We report the case of an 85-year-old female with stage IVB maxillary sinus squamous cell carcinoma who developed severe orbital myiasis. The patient presented with a large ulcerative facial lesion involving the lower eyelid and maxillary region, with multiple live larvae visible within necrotic tissue. Emergent removal of larvae, wound debridement, daily antiseptic irrigation, systemic antibiotics, and palliative care were performed.
Conclusion: Orbital myiasis in the setting of advanced head and neck malignancy is uncommon but can rapidly progress and significantly increase morbidity. Prompt recognition and early intervention are essential.
Plain Language Summary: Myiasis is an infection caused by fly larvae growing in human tissue.Elderly patients with large open wounds or untreated cancers are at high risk.In this case, an 85-year-old woman had advanced maxillary sinus cancer that created a large necrotic wound on her face.Flies laid eggs in the wound, which hatched into larvae that invaded the tissues around her eye.Doctors removed the larvae, cleaned the wound, used antibiotics, and provided palliative care.Early recognition and prompt treatment are crucial in preventing serious complications.
Keywords: orbital myiasis, maxillary sinus carcinoma, squamous cell carcinoma, ocular emergency, palliative care
Introduction
Squamous cell carcinoma of the maxillary sinus is a rare malignancy that tends to be detected late, especially in elderly or economically disadvantaged patients, leading to extensive tissue destruction and the formation of persistent open ulcers.1,2 When these tumors are not treated adequately, necrotic tissue and a contaminated environment create favorable conditions for serious infectious complications, including myiasis — a condition in which fly larvae invade and develop in living tissue.3,4
Myiasis of the facial-orbital region is an infrequent but severe complication, often seen in the elderly, malnourished, unhygienic, or those with malignant tumors who are not adequately cared for.3–5 The larvae can cause rapid tissue destruction, leading to severe edema, bleeding, widespread infection, and even spread to the sinuses, orbits, or intracranial space if not promptly treated.1,3,5
Myiasis can be classified into cutaneous, wound (traumatic), and cavitary forms, of which orbital–facial involvement represents a particularly destructive and vision-threatening manifestation. Although human myiasis is more frequently reported in tropical and subtropical regions, orbital myiasis remains rare and is typically associated with malignant wounds, chronic ulceration, advanced age, poor hygiene, and limited access to healthcare. In the present case, an elderly woman with advanced left maxillary sinus squamous cell carcinoma experienced progressive ulceration and necrosis over several months without oncologic treatment. Extensive tumor necrosis and chronic wound exposure created favorable conditions for larval infestation of the facial–orbital region, representing a rare but severe complication of malignant disease. This case highlights the urgent need for malignant wound care, increased public awareness of head and neck cancer, and the importance of early medical intervention in vulnerable populations.
Case Presentation
An 85-year-old woman presented with a progressive ulcerative mass of the left mid-face and lower eyelid. The lesion began approximately eight months before admission as swelling, erythema, and pain, but remained untreated. She was first admitted to a tertiary ophthalmology center approximately two months after symptom onset, where biopsy and surgical exploration revealed marked obstruction of the left nasal cavity and tumor invasion of the left maxillary sinus. Histopathology demonstrated poorly differentiated, non-keratinizing squamous cell carcinoma, confirmed by immunohistochemistry (CK5/6+, p63+, Ki-67 high). The patient declined oncologic treatment and returned home, opting instead for non-medical remedies. Over the following months, the lesion enlarged, ulcerated further, and frequently bled. Approximately six months after initial presentation, she was readmitted with severe pain, foul odor, and numerous live larvae emerging from the necrotic wound, consistent with orbital–facial myiasis.
Examination
On examination, the patient appeared cachectic with poor general condition. There was extensive ulceration destroying the left lower eyelid, with necrotic soft tissue containing approximately 30–40 motile larvae measuring 5–10 mm in length. Marked periorbital edema and serosanguinous discharge were present, without external evidence of globe perforation. A clinical video documented active larval movement within the orbital cavity (Video S1).
Immediate management consisted of complete mechanical removal of larvae using sterile forceps, followed by copious irrigation with normal saline and diluted povidone-iodine solution. Necrotic tissue was gently debrided, and systemic antibiotics were administered to prevent secondary infection. Analgesia and palliative care were provided in coordination with oncology specialists. Daily wound dressing and close monitoring were continued to detect potential orbital or intracranial extension. The patient had previously received palliative radiotherapy, which partially reduced tumor bleeding but did not resolve ulceration.
Outcome
No further larval infestation was observed following complete mechanical removal and appropriate wound care. The wound gradually became cleaner with reduced odor; however, the overall prognosis remained poor due to advanced malignancy and extensive tissue destruction.
Diagnostic Assessment
Imaging
Contrast-free CT scan of the face obtained at readmission demonstrated a large destructive soft-tissue mass involving the left maxillary sinus and anterior orbit, with bony erosion and periorbital extension (Figure 1).
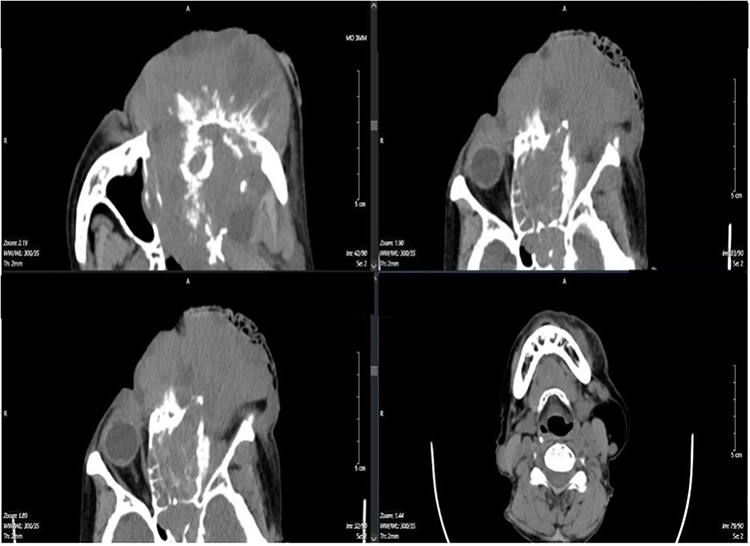 |
Figure 1 Contrast-free CT scan of the face showing a large destructive soft-tissue mass involving the left maxillary sinus with anterior orbital extension and bony erosion. |
Histopathology
Histopathological examination revealed poorly differentiated non-keratinizing squamous cell carcinoma with marked cellular atypia and extensive necrosis. Immunohistochemistry showed strong positivity for CK5/6 and p63, a high Ki-67 proliferation index, and negative staining for neuroendocrine markers (synaptophysin and TTF-1), consistent with an aggressive squamous cell carcinoma phenotype (Figure 2).
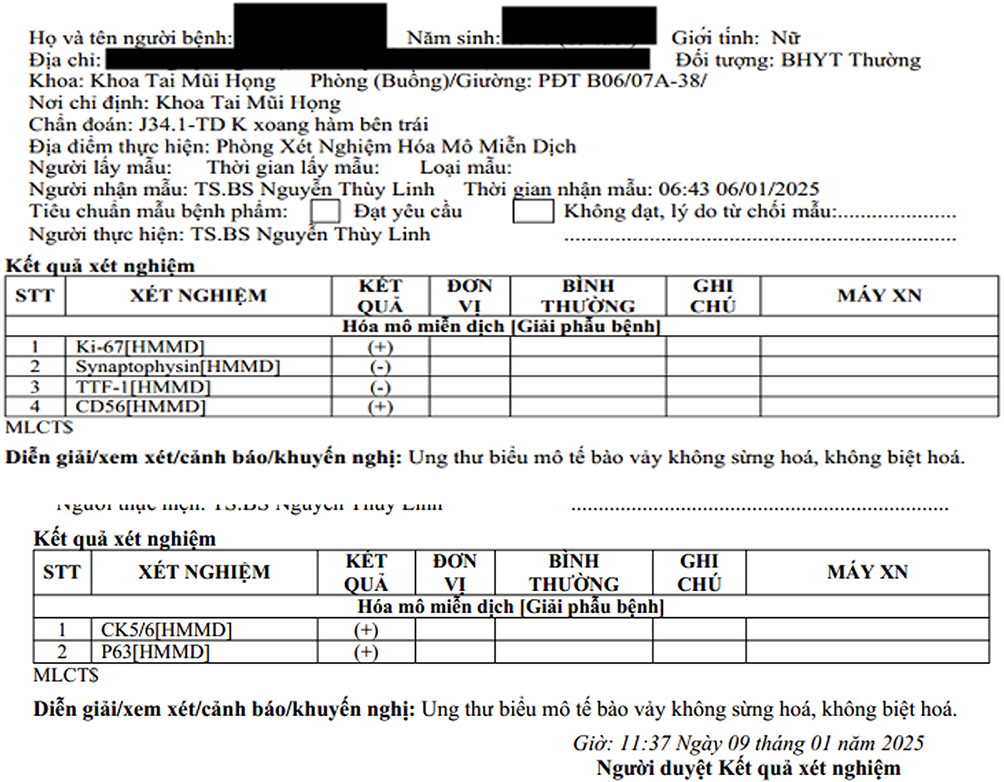 |
Figure 2 Histopathological findings of the maxillary sinus lesion showing poorly differentiated non-keratinizing squamous cell carcinoma with marked cellular atypia and extensive necrosis. Immunohistochemistry demonstrates strong positivity for CK5/6 and p63 with a high Ki-67 proliferation index, and negative staining for synaptophysin and TTF-1. |
Clinical Images
Clinical photographs and the supplementary video demonstrated extensive ulceration of the left mid-face and lower eyelid with loss of soft-tissue architecture, a deep necrotic cavity extending into the orbit, and multiple live larvae actively migrating within the wound. (Figure 3 and Video S1) These findings support the diagnosis of advanced orbital–facial myiasis secondary to malignant wound breakdown.
 |
Figure 3 Clinical photographs demonstrating extensive ulceration of the left mid-face and lower eyelid with loss of soft-tissue architecture, a deep necrotic cavity extending into the orbit, and multiple live larvae within the wound, consistent with advanced orbital–facial myiasis secondary to malignant wound breakdown. |
Timeline
Several months before admission: Onset of swelling and pain in the left periorbital region; no treatment pursued.
Approximately two months later: First hospital admission. Biopsy confirms poorly differentiated SCC of the maxillary sinus.
Over the following months: The patient declined oncologic treatment; the tumor enlarged, ulcerated, and bled continuously.
At readmission: Severe ulceration, foul odor, and live larvae were observed; orbital myiasis was diagnosed.
Same day: Larval extraction, irrigation, debridement, antibiotics, hemostasis.
Subsequent days: Transfer for palliative oncologic management; wound care continued.
Over the subsequent two weeks, the patient received palliative radiotherapy with daily wound dressing using povidone-iodine.
Discussion
Myiasis is a rare but clinically meaningful condition characterized by the invasion of living or necrotic tissue by fly larvae. Ocular myiasis accounts for a small proportion of all human myiasis cases but can be rapidly destructive due to the highly vascular and anatomically complex nature of the maxillofacial tissues. Several previous studies have shown that elderly, debilitated, immunocompromised, or those with inadequately managed facial malignancies are at increased risk of developing this disease.2,3,6
In our patient’s case, advanced age, left maxillary sinus squamous cell carcinoma, persistent necrotic ulceration, and interruption of cancer treatment created ideal conditions for fly attraction and larval development. This pathogenesis is entirely consistent with the description of previous authors.3,4,7 Malignant tumors of the maxillofacial region are prone to necrosis, foul-smelling discharge, and exposed soft tissue, making them a particularly favorable environment for flies to lay eggs.3,4,6 The larvae initially feed on necrotic tissue but can quickly invade healthy tissue, causing widespread necrosis, severe inflammation, and secondary infection if not treated promptly.
Recent reports show that myiasis in malignant lesions of the maxillofacial region is increasing, especially in patients like this case, elderly patients who have interrupted cancer treatment. Corrêa et al described a similar case in a patient with maxillary sinus cancer, in which necrotic tissue and persistent discharge acted as a strong attractant for flies.4 Meanwhile, Cuestas et al noted that myiasis most frequently appeared in ulcerative-necrotic SCC lesions, which is entirely consistent with the clinical picture of the patient in our study.3
Raina et al noted that orbital myiasis is often seen in the background of untreated facial malignancies, especially when the ulcerative and necrotic lesions have prolonged discharge. This environment creates favorable conditions for flies to lay eggs and larvae to invade, while increasing the risk of tissue destruction and spread if not treated promptly.5 Although Varshney et al did not directly describe myiasis, the authors emphasized that progressive sinus-base tumors, ulcerative necrosis in the context of late presentation or interrupted treatment, can cause many serious complications.1 This is also the clinical context commonly seen in cases of “malignant wound myiasis” reported in the literature. These observations reinforce the clinical value of our case, where myiasis served as both a complication and a warning signal.
Recent studies have also highlighted the importance of imaging, especially a CT scan, in assessing the extent of bone invasion and the risk of intracranial spread.1,4 This is entirely consistent with our management strategy: the patient underwent an orbital-sinus CT scan upon admission, which showed no bone destruction or intracranial invasion, thus avoiding unnecessary radical surgical intervention.
The management of myiasis in malignant lesions of the maxillofacial region follows three main principles: complete removal of larvae, daily cleaning and disinfection of the lesion, and systemic antibiotics in the event of secondary infection. These steps were described in detail by Corrêa et al in the treatment of oronasal myiasis in older adults, and also confirmed by Cuestas et al in a systematic review of myiasis in malignant lesions.3,4 Our patient was managed according to the above principles: repeated myiasis removal, wound irrigation with povidone-iodine 5% and systemic antibiotics.
Treatment of advanced maxillary sinus cancer in elderly patients is always a significant challenge. While surgery remains the standard method for early cases, studies have shown that elderly patients, frail patients, or patients with extensive lesions are no longer suitable for radical intervention.1 In such cases, palliative radiotherapy is considered a reasonable option to relieve pain, reduce odor, limit bleeding, and shrink the tumor. This regimen not only improves quality of life but also helps reduce the risk of myiasis recurrence by reducing necrotic tissue and surface exudates. Our treatment options are also based on current recommendations for advanced maxillary sinus cancer, where surgery is no longer indicated.1
If left untreated, myiasis in the facial tumor can cause dangerous complications such as orbital destruction, extension to the cavernous sinus, sepsis, or intracranial invasion. Thanks to early detection and coordinated treatment between specialists, the patient in our study avoided these complications.1,5
In conclusion, this case emphasizes that myiasis in patients with facial malignancies is not only a complication of tissue necrosis but also an essential sign of treatment interruption and inadequate wound care. Early diagnosis, aggressive management, and treatment of the underlying cancer play a crucial role in limiting tissue destruction and reducing the risk of recurrence.
A limitation of this report is that larval species identification was not performed in a parasitology laboratory, which may have provided additional diagnostic and epidemiological value. In addition, long-term follow-up was limited due to the advanced stage of malignancy and the palliative intent of care.
Conclusion
Orbital myiasis is a rare but serious complication of advanced head and neck malignancies. Early recognition and prompt removal of larvae are essential to prevent deeper tissue destruction. This case highlights the importance of appropriate wound care, patient education, and multidisciplinary management in elderly cancer patients.
Ethics and Consent
Institutional approval was not required for the publication of this single case report, and written informed consent for publication was obtained from the patient. Written informed consent was obtained from the patient for the use of her personal information for scientific research and for the publication of clinical details, images, and video associated with this case report. The patient agreed to allow her personal and medical information to be used for academic and scientific purposes. Written informed consent for publication was obtained in accordance with the principles of the Declaration of Helsinki and the guidelines of the Committee on Publication Ethics (COPE). All identifying information has been removed to protect patient confidentiality.
Funding
This study received no funding.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Varshney S, Bist S, Gupta N, Singh R, Bhagat S. Anterior craniofacial resection—for paranasal sinus tumors involving anterior skull base. Indian J Otolaryngol Head Neck Surg. 2010;62(2):103–6. doi:10.1007/s12070-010-0045-1
2. Dulguerov P, Jacobsen MS, Allal AS, Lehmann W, Calcaterra T. Nasal and paranasal sinus carcinoma: are we making progress? A series of 220 patients and a systematic review. Cancer. 2001;92(12):3012–3029. doi:10.1002/1097-0142(20011215)92:12<3012::AID-CNCR10131>3.0.CO;2-E
3. Cuestas D, Pedraza J, Herrera H, et al. Cutaneous myiasis in skin cancer and malignant wounds: a systematic review. Int J Dermatol. 2021;60(12):1529–1546. doi:10.1111/ijd.15672
4. Corrêa APS, Beneti IM, Ribeiro ED, Pereira CCS, Souza FÁ, Garcia-Júnior IR. Myiasis in elderly involving oral and nasal cavities—diagnosis and treatment. J Craniofac Surg. 2015;26(3):989–990. doi:10.1097/SCS.0000000000001579
5. Raina UK, Gupta M, Kumar V, Ghosh B, Sood R, Bodh S. Orbital myiasis in a case of invasive basal cell carcinoma. Oman J Ophthalmol. 2009;2(1):41–42. doi:10.4103/0974-620X.48422
6. Francesconi F, Lupi O. Myiasis. Clin Microbiol Rev. 2012;25(1):79–105. doi:10.1128/CMR.00010-11
7. Gupta S, Naik S, Halkud R, Nanjundappa A. Advanced case of invasive basal cell carcinoma with extensive ocular myiasis. Int J Head Neck Surg. 2014;4(1):36–40. doi:10.5005/jp-journals-10001-1133
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.