Back to Journals » International Medical Case Reports Journal » Volume 19
Oral Necrotizing Ulcerations in Acute Leukemia Patients: Clinical Characteristics, Integrated Management, and Favorable Outcomes – A Case Series
Authors Priandhika FH ![]() , Hidayat W
, Hidayat W ![]() , Fitriasari N
, Fitriasari N
Received 17 October 2025
Accepted for publication 29 January 2026
Published 17 February 2026 Volume 2026:19 570294
DOI https://doi.org/10.2147/IMCRJ.S570294
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Xudong Zhu
Fajar Hani Priandhika,1 Wahyu Hidayat,2 Nuri Fitriasari3
1Oral Medicine Residency Program, Faculty of Dentistry, Universitas Padjadjaran, Bandung, Indonesia; 2Oral Medicine Department, Faculty of Dentistry, Universitas Padjadjaran, Bandung, Indonesia; 3Oral Health Polyclinic, Oral Medicine Division, Hasan Sadikin Central General Hospital, Bandung, Indonesia
Correspondence: Fajar Hani Priandhika, Oral Medicine Residency Program, Faculty of Dentistry, Universitas Padjadjaran, Jalan Sekeloa Selatan No. 1, Bandung, West Java, 40132, Indonesia, Tel +62 82375555553, Fax +62 22 7794121, Email [email protected]
Introduction: Leukemia often presents with diverse oral manifestations like ulceration, bleeding, and gingival enlargement due to immunosuppression and chemotherapy. The altered oral microbiome in leukemic patients increases infection risks, including bloodstream infections. Early diagnosis and targeted treatment of oral complications are vital to improve patient outcomes and quality of life.
Purpose: This case series aims to explore the clinical presentation, underlying systemic conditions, and treatment response of oral necrotizing ulcerations including necrotizing ulcerative gingivitis (NUG) and necrotizing stomatitis in patients with acute leukemia.
Patients and Methods: Three female patients aged 18 to 21 years were diagnosed with necrotizing ulcerative oral lesions associated with acute leukemia: two with Acute Lymphoblastic Leukemia (ALL) and one with Acute Myeloid Leukemia (AML). Detailed intraoral examinations were performed, alongside hematologic and biochemical laboratory analyses. Treatment protocols included gingival debridement with hydrogen peroxide 1,5%-3%, chlorine dioxide zinc antiseptic mouthwashes (chlorine dioxide zinc), topical hyaluronic acid, and Vaseline application. Suggestions of prescribing Metronidazole also been given to the referring departments. Patients were monitored through serial follow-ups for clinical progress.
Results: All three patients presented with crater-like ulcerations, greyish pseudomembranes, and gingival inflammation, with varying degrees of systemic hematologic compromise. The first patient (ALL) showed marked improvement by the third follow-up, with near-complete healing by the final visit. The second patient (AML) demonstrated reduction in gingival necrosis and inflammation, although gingival hyperplasia persisted. The third patient (ALL, pre-chemotherapy) initially presented with necrotizing stomatitis and NUG; significant clinical improvement and complete lesion resolution were observed over successive follow-ups. Systemic findings, including leukopenia, anemia, and elevated inflammatory markers, were consistent with hematologic malignancies and contributed to lesion severity. Our incapability to perform additional diagnostic test such as oral lesion biopsy or microbiology test was the limitations of this case report.
Conclusion: Oral Necrotizing Ulcerations, including NUG, NUP, and NUS, represent significant clinical manifestations of acute leukemia, reflecting the underlying immunosuppression, hematologic abnormalities, and oral microbial dysbiosis inherent to the disease. Early recognition of characteristic clinical features, followed by integrated local oral management and close coordination with systemic medical care, can lead to favorable healing outcomes despite profound hematologic compromise.
Keywords: necrotizing ulcerative gingivitis, acute leukemia, oral ulcerations
Introduction
Leukemia is a group of blood cancers that shows a diverse epidemiological pattern. Cases of Acute Lymphoblastic Leukemia (ALL) and Acute Myeloid Leukemia (AML) has seen an increased rate with incidence rate in adolescents and young adults reaching 3,1; 2,9; and 4,1 per 100.000 in the age group of 15–19, 20–29 and 30–39 years old, respectively.1 Over 90% percent cases of leukemia showed oral manifestations which includes petechiae, spontaneous bleeding, mucosal ulceration, gingival enlargement and necrosis of the oral mucosa. Herrera et al reported that the global prevalence of necrotizing ulcerative gingivitis (NUG) is generally low, estimated at less than 1% of the population in most countries. However, in specific high-risk groups, such as HIV-positive individuals, malnourished children, or populations under extreme stress and severe systemic diseases including leukemia, the prevalence of necrotizing periodontal diseases (NUG and NUP) can rise to 2%–6%.2 These findings underline the many different types of oral manifestations of leukemia and thus potentially serving as indicator of leukemia.3
Leukemia and necrotizing oral ulceration share a well-established relationship, primarily due to the immunosuppressive state induced by leukemia itself, which reduces the host’s ability to combat pathogens and maintain oral microbial homeostasis, thereby promoting dysbiosis.4 Another major factor contributing to the exacerbation of oral lesions in leukemic patients is chemotherapy, which further weakens the immune system and increases susceptibility to oral ulcerations and necrosis.3 Additionally, patients with leukemia often exhibit an altered oral microbiome characterized by a predominance of pathogenic bacteria such as Actinomyces and Fusobacterium species, which are associated with oral infections and ulcerations.5 The role of the oral microbiome is particularly significant in the development of infections among leukemic patients. Colonization by gram-negative bacilli and other pathogens not only leads to local oral infections but can also result in bloodstream infections, which are major contributors to mortality in this patient group.6
Oral manifestations play a critical role as potential initial indicators of leukemia, often preceding systemic signs and leading patients to seek dental care before a medical diagnosis is established. Leukemic infiltration of oral tissues and secondary effects of bone marrow failure can result in clinical features such as gingival enlargement, spontaneous gingival bleeding, petechiae, ecchymosis, mucosal pallor, and recurrent or persistent oral infections, including necrotizing lesions. These findings are frequently associated with thrombocytopenia, anemia, and immunosuppression, which are hallmark hematologic abnormalities in leukemia.7,8 Because the oral cavity is readily accessible for examination, dentists and oral health professionals are uniquely positioned to recognize these early, nonspecific manifestations. Prompt identification and appropriate referral based on suspicious oral signs can facilitate earlier diagnosis, timely initiation of therapy, and improved prognosis, underscoring the essential role of oral examination in the early detection of leukemia.
Patient and Methods
Case 1 (Necrotizing Ulcerative Gingivitis with ALL)
An 18-year-old female patient presented to the Department of Oral Medicine with complaints of persistent dull pain in the anterior gums, which had been ongoing for the past week. On subjective examination, the patient reported a pain score of 6/10 on the Visual Analogue Scale (VAS) and stated that this was the first time the patient had experienced such symptoms. Additionally, the patient reported a history of recurrent fever over the past two weeks. Her medical history revealed a diagnosis of ALL since June 2024, for which the patient had received packed red cells (PRC) and thrombocyte transfusions. The patient had not given chemotherapy regimen yet. The patient denied any associated swelling of the gums, recurrent oral ulcers, or any history of food or drug allergies. Prior to her referral to the Department of Oral Medicine, the patient had been diagnosed by the Department of Pediatrics with ALL, high-risk febrile neutropenia, and Stage 2 hypertension. The patient had been prescribed Ceftazidime, Paracetamol, Omeprazole, Captopril, Nifedipine, Furosemide, and Nystatin drops.
Extraoral Examination shows symmetrical face, Anemic conjunctiva, non icteric sclera, dry and exfoliated lips, Temporomandibular Joint (TMJ), Lymph Nodes, and mouth opening all within normal bounds. From the Intraoral Examination we found a Crater-like ulceration on the gingival margin of 12–22 with greyish necrotic tissue with irregular erythema on several sides, as can be seen in Figure 1. Pain is also experienced. From the Debris and Calculus Examination, we found an OHI-s (Oral Hygiene Index) scores of 2,4 which is moderate. There is no sign of mobilized teeth. Laboratory results show Low Hemoglobin (11,4 g/dL), Hematocrit (32,9%), Erythrocyte (3,17 million/uL), Leukocyte (0,96 x103/uL), MCHC (32,6%), and High Lymphocyte (96%), Erythrocyte Sedimentation Rate (34 mm/h), SGOT (106 U/L) and SGPT (405 U/L).
 |
Figure 1 Initial Presentation: Crater-like ulceration on the gingival margin of 12–22. |
Based on the clinical findings, the patient was then diagnosed as Necrotizing Ulcerative Gingivitis (NUG) and planned for gingival debridement using 1.5% hydrogen peroxide (H2O2) solution at the hospital. Additionally, the patient was instructed to use a chlorine dioxide zinc mouthwash three times daily after tooth brushing, to gargle for one minute, and to refrain from eating or drinking for 30 minutes afterward. Hyaluronic acid gel (0.025%) was prescribed for topical application on the maxillary gingival area twice daily. Vaseline was also recommended for application on the lips three times a day to maintain hydration. Administration of Metronidazole was also suggested to the Pediatric Department as a treatment of specific anaerobic bacterial infection. Further dental treatment, including scaling, was indicated once the patient’s general medical condition stabilized and was deemed suitable for the procedure.
Case 2 (Necrotizing Ulcerative Periodontitis with AML)
A 21-year-old female patient presented to the Oral Medicine Department with complaints of swollen and bleeding gums persisting for three weeks. During subjective examination, the patient reported a pain intensity of 5/10 on the VAS. This was the first occurrence of gingival pain for the patient. Additionally, the patient had been experiencing recurrent fever for the past three weeks. Four days prior to admission, the patient was hospitalized due to fatigue followed by a syncope episode. The patient had a prior diagnosis of AML since August 2024 and had undergone PRC transfusion but had not received thrombocyte transfusion. The patient had not given chemotherapy regimen yet. The patient denied any history of recurrent oral ulcers, food allergies, or drug allergies. Due to her condition, the patient was unable to eat normally and was receiving parenteral nutrition. Before referral to the Oral Medicine Department, the Internal Medicine Department had diagnosed the patient with AML, submental abscess, brain leukostasis, spurious hypocalcemia, and hypocalcemia secondary to vitamin D deficiency. The patient was under treatment with intravenous ceftriaxone, calcium carbonate, and paracetamol.
Extraoral Examination shows symmetrical face, Anemic conjunctiva, non icteric sclera, dry and exfoliated lips, springy consistency of the right and left submandibular nodes, measured 5 × 3 × 2 cm in size, two fingers limited mouth opening, and TMJ within normal bounds. Intraoral Examination revealed Gingival hyperplasia across almost the entire palatal region of the maxilla, as well as the labial and lingual regions of the mandible, extending to several areas in the posterior region. The gingiva exhibited a positive tendency for bleeding but was not associated with pain. An ulcerated, crater-like lesion covered by a greyish pseudomembrane was identified in the 31–43 region, accompanied by the presence of a white plaque and erythema along the sulcus border, as can be seen in Figure 2. Pain was reported to be present in the area of the ulcerative lesion, along with second degree mobilized teeth of 42 and 43. From the Debris and Calculus Examination, we found an OHI-s scores of 2,8 which is moderate. Laboratory results shows Low Hemoglobin (8,9 g/dL), Hematocrit (27,3%), Erythrocyte (3,07 million/uL), Thrombocyte (59 thousand/uL), MCHC (32,6%), High Quantitative CRP (13.31 mg/dL), and Very High Leukocyte (157,67 x103/uL). From the Panoramic Radiographic examination, we found horizontal bone loss in the region of 41 and 42, along with loss of periodontal attachment and thickening of lamina dura.
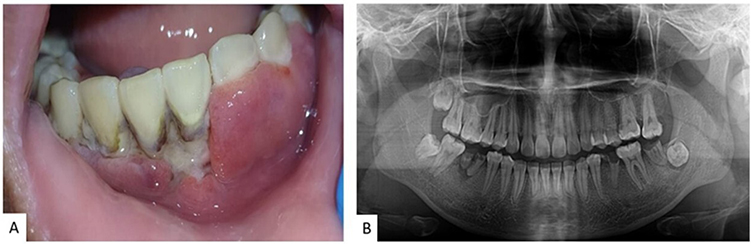 |
Figure 2 Initial Presentation: An ulcerated, crater-like lesion covered by a greyish pseudomembrane in 31–43 region, with a second degree mobility of teeth 42 and 43 (A); Horizontal Bone Loss at area of the tooth 31–43, along with loss of periodontal attachment and thickening of lamina dura, observed from Panoramic Examination (B) indicating massive penetration of pathogen bacteria, resulting in Periodontitis. |
Based on the clinical findings, the patient was then diagnosed as NUP and planned for gingival debridement using 3% H2O2 and localized scaling restricted to the affected areas while hospitalized. Additionally, the patient was instructed to use chlorine dioxide zinc mouthwash three times daily after tooth brushing, with each session followed by gargling for one minute and refraining from eating or drinking for 30 minutes afterward. Hyaluronic acid 0.025% was prescribed for topical application on the mandibular gingival area twice daily, and Vaseline was advised to be applied on the lips three times a day to maintain hydration. Administration of Metronidazole was also suggested to the Internal Medicine Department as a treatment of specific anaerobic bacterial infection A full-mouth scaling procedure will be indicated once the patient’s general systemic condition is considered stable and ideal. The patient is scheduled for a control period in order to observe the progress of the treatment.
Case 3 (Necrotizing Ulcerative Stomatitis + NUG with ALL)
A 19-year-old female patient presented to the Oral Medicine Department with complaints of persistent pain in the palate and maxillary gingiva for the past two weeks. Upon subjective examination, the patient reported a pain intensity of 7/10 on the VAS and noted recurrent episodes of fever over the last week. The patient had previously been diagnosed with ALL in September 2024 but had not yet commenced chemotherapy. The patient had undergone PRC and thrombocyte transfusions. The patient denied experiencing gingival bleeding, gingival swelling, or recurrent oral ulcers. There was no reported food allergy; however, the patient did report a known allergy to omeprazole. Two weeks prior, the patient was prescribed oral suspension Nystatin (4 × 1 mL) as part of her treatment. Before being referred to the Oral Medicine Department, the patient had been diagnosed by the Pediatric Department with B-cell Acute Lymphoblastic Leukemia (L2) and a history of Fixed Drug Eruption (FDE). At the time of presentation, the patient was on multiple medications, including paracetamol, folic acid, vitamin D (1000 IU), sucralfate, methylprednisolone, ranitidine, ciprofloxacin, granulocyte colony-stimulating factor (G-CSF), and nystatin drops.
Extraoral Examination shows symmetrical face, Anemic conjunctiva, non icteric sclera, dry and exfoliated lips, Temporomandibular Joint (TMJ), Lymph Nodes, and mouth opening all within normal bounds. Intraoral examination revealed erosive lesions on the palatal area, particularly around teeth 16, 17, and 24, covered with pseudomembrane and accompanied by pain upon palpation, as can be seen in Figure 3. Additionally, a necrotic ulcer was observed on the palate, surrounded by a pseudomembrane and scattered whitish-red spots with diffuse borders, particularly around the region of the fovea palatina. The patient also reported significant pain in the affected areas. From the Debris and Calculus Examination, we found an OHI-s scores of 3,6 which is bad. There is no sign of mobilized teeth. Laboratory results shows Low Erythrocyte (3,17 million/uL), and Very Low Hemoglobin (6,8 g/dL), Hematocrit (19,9%), Leukocyte (1,56 x103/uL), Thrombocyte (16 thousand/uL).
 |
Figure 3 Initial Presentation: Greyish Pseudomembrane Necrotic Ulceration at regio: Whole Palatum Area (A); Attached gingiva regio 11–14 spreading to Right Fovea Palatine area (B); Attached gingiva regio 16–17 (C); Interdental Papillae 23–24 and Left Fovea Palatine area (D). |
Based on the clinical findings, the patient was then diagnosed as NUG and NUS and planned for gingival debridement using 3% H2O2. Additionally, the patient was instructed to use chlorine dioxide zinc mouthwash three times daily after tooth brushing, with each session followed by gargling for one minute and refraining from eating or drinking for 30 minutes afterward. Hyaluronic acid 0.025% was prescribed for topical application on the palatal area twice daily, and Vaseline was advised to be applied on the lips three times a day to maintain hydration. Administration of Metronidazole was also suggested to the Pediatric Department as a treatment of specific anaerobic bacterial infection. A full-mouth scaling procedure will be indicated once the patient’s general systemic condition is considered stable and ideal.
Results
Case 1 (NUG with ALL)
The patient is scheduled for control over a period of 4 days with improvements on each visit. Following the initial visit (Figure 4a), the patient was scheduled for subsequent follow-ups. During the second visit, marginal improvement was observed, characterized by a reduction in the area of necrotized margins, as can be seen in Figure 4b. By the third visit, the patient demonstrated significant clinical improvement, with a marked decrease in gingival inflammation and erythema, as well as an almost complete resolution of the necrotic areas, as can be seen in Figure 4c. At the final visit, only a minimal area of inflammation remained in the previously affected region, with complete resolution of gingival inflammation in the upper quadrant, as can be seen in Figure 4d.
 |
Figure 4 Progression of lesion: 1st Visit (A); 2nd Visit (B); 3rd Visit (C); 4th Visit (D). |
Case 2 (NUP with AML)
The patient is scheduled for a control period of 7 days in order to observe the progress of treatment. Following the treatment plan, the patient demonstrated noticeable improvement compared to initial presentation. At the second visit, a marked reduced gingival inflammation and hyperemia was observed as can be seen in Figure 5c. Also, necrotic area had significantly decreased, as can be seen in Figure 5d.
 |
Figure 5 Progression of lesion: 1st Visit before debridement (A); 1st Visit after debridement (B); 2nd Visit before debridement (C); 2nd Visit after debridement (D). |
Case 3 (NUS + NUG with ALL)
The patient was scheduled for several follow-up visits with a total of 10 days, with gradual improvements observed at each control period. At the second visit after initial admittance, the patient showed slight improvement, indicated by a reduction in the pseudomembrane plaque and a partial decrease in necrotic tissue. By the third visit, significant improvement was noted, with a major reduction in gingival inflammation and erythema. Complete healing was observed at the fourth visit, as can be seen in Figure 6, highlighting effectiveness of the treatment plan.
 |
Figure 6 Progression of lesion: Whole Palatum Area 1st Visit–4th Visit (Ai–iv); Attached Gingiva regio 11–14 and Right Fovea Palatine at 1st Visit–4th Visit (Bi–iv); Attached Gingiva regio 16–17 1st Visit–4th Visit (Ci–iv); Interdental Papillae 23–24 and Left Fovea Palatine area 1st Visit–4th Visit (Di–iv). |
Discussion
Oral necrotizing ulcerations in leukemia patients arise from a combination of immune suppression, microbiota imbalance, and barrier disruption in the oral mucosa. In patients with acute leukemia, particularly AML, chemotherapy-induced neutropenia compromises innate immune defenses, impairing the host’s ability to control microbial overgrowth. This immunosuppressed state is exacerbated by oral dysbiosis, where the loss of commensal microbial balance allows opportunistic pathogens like Candida spp. and Viridans Group Streptococci (VGS) to proliferate.9,10
Poor oral hygiene further exacerbates this imbalance, promoting the accumulation of biofilm composed of both fungal and bacterial species, which contributes to local inflammation and mucosal breakdown. As Sodré et al emphasized, the oral cavity houses complex fungal and bacterial communities capable of forming biofilms that invade mucosal tissues, especially when epithelial barriers are weakened and oral care is neglected.10
McMahon et al demonstrated that organisms typically responsible for bloodstream infections, such as Pseudomonas aeruginosa and VGS, were often enriched in the oral microbiome of AML patients, even in the absence of gastrointestinal domination.11 These pathogens may originate in the oral cavity and, through ulcerated or poorly maintained mucosa, translocate into the bloodstream, further endangering patients. Thus, bad oral hygiene not only fosters colonization by pathogenic species but also creates a portal of entry for invasive infections.12 Maintaining oral cleanliness is crucial in reducing microbial load and preventing necrotizing lesions in this vulnerable population.
Necrotizing oral ulcerations in leukemia patients result from a complex interaction between hematological decline, chemotherapeutic toxicity, and immune suppression, which collectively weaken the oral mucosal defense. Ptasiewicz et al emphasized that oral mucosal damage worsens in correlation with declining white and red blood cells and hemoglobin, with chemotherapy acting as the primary trigger for immunosuppression and mucosal fragility.4 The mucosa becomes highly susceptible to inflammatory and necrotic processes, especially in the presence of poor hygiene and microbial buildup.
Clinically, NUG, NUP, and NUS represent a spectrum of necrotizing periodontal diseases that differ primarily in the extent and anatomical area of tissue involvement.13 NUG is limited to the gingival tissues, particularly affecting the interdental papillae, which become necrotic, “punched-out,” and covered by a grayish pseudomembrane, without attachment or bone loss. In contrast, NUP extends beyond the gingiva to involve the periodontal attachment apparatus, resulting in rapid loss of clinical attachment and alveolar bone, often accompanied by severe pain and spontaneous bleeding. NUS represents the most severe form, in which necrosis spreads beyond the periodontal tissues to adjacent oral mucosa, including the buccal mucosa, lips, tongue, or palate, and may even lead to extensive soft tissue destruction.14 Therefore in Case 3, we diagnosed the patient with combination of NUS and NUG, because in several areas, the lesions were limited only in attachment gingivae and interdental papillae, suggesting the diagnosis of NUG, while the other lesions were expanding to adjacent oral mucosa suggesting the diagnosis of NUS.
NUS is not invariably a developmental continuation of NUG or NUP but can present as a primary and solitary necrotizing lesion, particularly in severely immunocompromised patients. While classic teaching places NUS at the extreme end of a necrotizing periodontal disease spectrum, accumulating clinical evidence indicates that NUS may arise independently on oral mucosal surfaces without preceding gingival or periodontal involvement.13 This phenomenon is most commonly observed in conditions marked by profound immune dysfunction, such as leukemia, advanced HIV infection, severe malnutrition, or neutropenia, where epithelial barrier failure and vascular compromise allow rapid plaque-induced mucosal necrosis apart from periodontal inflammation.13 In such settings, the absence of intact immune surveillance permits opportunistic pathogens to directly invade non-gingival mucosa, leading to ulceronecrotic destruction that does not require prior NUG or NUP as a precursor.15 Therefore, NUS should be understood not only as a potential progression of necrotizing periodontal disease but also as a distinct clinical entity that can manifest independently when systemic immunosuppression outweighs local periodontal initiating factors.
The first and third cases in this series highlight the predisposition of ALL patients to oral necrotizing ulcerations. As reported by Aurora et al, such oral manifestations can often serve as clinical indicators of leukemia, including ALL.16 These symptoms arise from the proliferation of immature blood cells, which contribute to neutropenic sepsis and coagulopathy factors that significantly increase both morbidity and mortality in affected patients. Additionally, bone marrow necrosis may further aggravate oral health, characterized histologically by the depletion of fat cells and the presence of amorphous material.17
A parallel observation is noted in the second case, involving a patient with AML, who also presented with oral necrotizing ulcerations. This condition is primarily attributed to the immunosuppressive nature of AML itself, compounded by the effects of intensive chemotherapy regimens. According to Santibanez-Bedolla et al, the diminished immune response in these patients facilitates the proliferation of gram-negative bacilli, which are commonly found in hemato-oncologic individuals and are linked to infectious complications in the oral cavity.15 Furthermore, mucositis is frequently observed in such cases, especially among chemotherapy recipients, as a result of microbiota-driven inflammation that plays a central role in the pathogenesis of oral ulcerations.18
Analysis of the three cases demonstrates that aggressive necrotizing oral manifestations in leukemia patients are interconnected through a shared background of systemic immunosuppression yet remain clinically distinct due to differences in local contributing factors and the extent of tissue involvement. In all cases, leukemia-induced hematologic abnormalities, particularly neutropenia, anemia, and thrombocytopenia, significantly impaired host defense mechanisms, reduced mucosal resistance, and compromised wound healing, creating a favorable environment for rapid microbial proliferation and tissue necrosis.19 Local factors, especially poor oral hygiene and plaque accumulation, acted as critical initiating triggers by increasing the load of anaerobic and opportunistic pathogens, which precipitated necrotizing inflammation once immune control was lost.20 Despite this common pathophysiological foundation, the manifestations differed along a continuum of severity. In NUG, tissue damage is largely superficial and driven by acute inflammatory necrosis of the interdental papillae, where microbial virulence overwhelms a temporarily weakened immune defense but remains limited by residual host control. In contrast, NUP represents a more advanced breakdown characterized by rapid loss of periodontal attachment and alveolar bone, indicating a failure of both immune containment and tissue repair mechanisms, likely exacerbated by more profound neutropenia and systemic inflammatory burden. NUS reflects the most aggressive expression, marked by extension of necrosis beyond periodontal structures into the oral mucosa, suggesting severe epithelial barrier disruption and compromised vascular support that allow infection and inflammation to propagate horizontally across tissues.14,21,22 Thus, the distinction among these conditions is not merely topographical, but reflects a graded escalation of disease severity shaped by the intensity of immunosuppression, local microbial load, and the host’s diminished capacity to limit necrosis and regenerate damaged tissues in the leukemic state.
Standard initial treatment for patient with necrotic ulceration is the usage of Hydrogen Peroxide (H2O2) due to its antiseptic property which kills pathogens through oxidation burst and local oxygen production and its capability.23 Furthermore, in low concentration, it is capable to remove cells and pathologic debris and promote cytokine secretions making it ideal for spooling and debriding dead pathogen and cell tissues.24
In periodontal debridement, 3% H2O2 provides a stronger effervescent and antimicrobial effect, making it useful for heavy necrotic debris but with a higher risk of mucosal irritation and tissue damage, whereas 1.5% H2O2 offers adequate cleansing and oxygen release with improved tissue tolerance.25 The 1.5% concentration is preferred in young patients because it reduces the risk of chemical burns, cytotoxicity to healing tissues, and patient discomfort while still supporting effective debridement and wound healing.26 This is why there is a slight difference of our debridement plan in Case 1, which we use the concentration of 1,5% H2O2, compared to the 3% concentration we gave on Case 2 and 3. This is due to our consideration of patient’s age, as 3% concentration may cause a great discomfort to a patient at her age, and could be making the patient does not want to continue treatment.
Patients in this case was then prescribed for antibiotics both broad spectrum and those addressing anaerobic pathogen infections. In cases of necrotizing oral ulceration, anaerobic bacteria are usually present and as such necessitates the usage of antibiotics such as metronidazole in conjunction with broad spectrum antibiotics.27 One of the pathogens that is well documented as one of the main pathogenic findings in necrotizing oral ulcers is Fusobacterium nucleatum. This bacteria is considered to be an anaerobic bacteria and as such necessitates the usage of broad-spectrum antibiotics in combination with anaerobic pathogen specific antibiotics such as metronidazole.28,29
As a symptomatic therapy, Chlorine dioxide and Zinc compound is also well indicated as it shows antibacterial, antiviral and anti-inflammation property. As Permatasanti et al and Ridho et al noted that this compound can be used as an antioxidant mouthwash for treating oral lesions in patients with AML proving the capability to maintain oral pH, while zinc specifically contributes by transferring electrons to reactive oxidative stress (ROS). These findings shows that Chlorine Dioxide Zinc can accelerate the healing of oral lesions, reduce inflammation and reduce the discomfort caused by ulcers.30,31
This study is limited in our capacity to verify the species of bacteria involved in this disease by performing additional supportive diagnostic test such as oral lesion biopsy or microbiological test like ELISA, PCR, et cetera. This is due to the incapability to perform culture identification to the patients involved at that time.
Conclusion
Oral Necrotizing Ulcerations, including NUG, NUP, and NUS, represent significant clinical manifestations of acute leukemia, reflecting the underlying immunosuppression, hematologic abnormalities, and oral microbial dysbiosis inherent to the disease. Early recognition of characteristic clinical features, followed by integrated local oral management and close coordination with systemic medical care for hematologic treatment, can lead to favorable healing outcomes despite profound hematologic compromise.
Consent Statements
The patients had approved and written informed consent for the publication of this case series, including the images. The institution has also approved the publication of this article.
Acknowledgments
This publication charge is funded by Universitas Padjadjaran through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Program (Contract No. 4303/ B3/DT.03.08/2025 and 3927/UN6. RKT/HK.07.00/2025).
The author would like to thank Wahyu Hidayat, drg., Sp.PM., Subsp.Inf.Im., and Nuri Fitriasari, drg., Sp.PM., who has guided and provided direction regarding patient care and making this case series. The author(s) also would like to thank Internal Medicine Department and Pediatric Department of Hasan Sadikin Central General Hospital for their cooperation in co-treating the contributing patients. The contributing patients and their family are appreciated too by the authors for their cooperation, understanding, and desire to be included in the preparation of this case series.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Berkman AM, Andersen CR, Cuglievan B, et al. Long-term outcomes among adolescent and young adult survivors of acute leukemia: a surveillance, epidemiology, and end results analysis. Cancer Epidemiol Biomarkers Prev. 2022;31(6):1176–11. doi:10.1158/1055-9965.EPI-21-1388
2. Herrera D, Alonso B, de Arriba L, Santa Cruz I, Serrano C, Sanz M. Acute periodontal lesions. Periodontol. 2000;65(1):149–177. doi:10.1111/prd.12022
3. Cammarata-Scalisi F, Girardi K, Strocchio L, et al. Oral manifestations and complications in childhood acute myeloid leukemia. Cancers. 12(6):1634.p.1–11. doi:10.3390/cancers12061634
4. Ptasiewicz M, Pawłowicz AK, Tymczyna-Borowicz B. Chemotherapy and oral health in leukemic patients. Polish J Environ Stud. 2020;29(5):3263–3271. doi:10.15244/pjoes/114234
5. Mougeot JLC, Beckman MF, Langdon HC, Brennan MT, Mougeot FB. Oral microbiome signatures in hematological cancers reveal predominance of actinomyces and rothia species. J Clin Med. 2019;9(12):1–19. doi:10.3390/jcm9124068
6. Strong J, Zhou AE, Alkaabba F, et al. A case of acute myeloid leukemia-associated necrotizing sweet syndrome. Case Rep in Dermatol. 2022;14(3):339–343. doi:10.1159/000527597
7. Stana P, Marina G, Anca D. Oral manifestations in acute leukemia as the first sign; the interdisciplinary approach of diagnosis and treatment. J Mind Med Sci. 2015;2(2):186–192. doi:10.22543/2392-7674.1021
8. Cammarata-Scalisi F, Girardi K, Strocchio L, et al. Oral Manifestations and Complications in Childhood Acute Myeloid Leukemia Cancers. 2020;12(6):1634. doi:10.3390/cancers12061634
9. Sodré CS, Rodrigues PMG, Vieira MS, et al. Oral mycobiome identification in atopic dermatitis, leukemia, and HIV patients–a systematic review. J Oral Microbio. 12(1):1807179. doi:10.1080/20002297.2020.1807179
10. Hamouda O. Oral Candidiasis in leukemia patients. In: Virology & Mycology 1 Virol Mycol. Vol. 10. Open Access; 2021.
11. McMahon S, Sahasrabhojane P, Kim J, et al. Contribution of the oral and gastrointestinal microbiomes to bloodstream infections in leukemia patients. Microbiol Spectrum. 2023;11(3). doi:10.1128/spectrum.00415-23
12. Peřina V, Šmucler R, Němec P, Barták V. Update on focal infection management: a czech interdisciplinary consensus. Int Dent J. 2024;74(3):510–518. doi:10.1016/j.identj.2023.11.001
13. Peacock ME, Ghaly M, Cornelius Timothius CJ. Emergent periodontal conditions: an overview. Dentistry Re. 2025;5(2):100155. doi:10.1016/j.dentre.2025.100155
14. Newman MG, Klokkevold PR, Elangovan S, Kapila Y, Carranza FA. Acute gingival infections and necrotizing ulcerative periodontitis. In: Newman and Carranza’s Clinical Periodontology and Implantology. Elsevier.2023.
15. Rezeki S, Sasanti H. Necrotizing ulcerative stomatitis associated with hiv/aids: clinical findings and management (Case Report). Cakradonya Dent J. 2017. doi:10.24815/cdj.v9i2.9751
16. Aurora F, Arasaretnam A, Hobkirk A. The recognition of oral manifestations of haematological disease saves lives: a case report. Bull Natl Res Cent. 46(1). doi:10.1186/s42269-022-00915-9
17. Nicacio JM, Taveira MRV, de AACFF, LF S. Bone marrow necrosis caused by acute leukemia: a case report. Brazilian J Case Rep. 2022;2(2):24–30. doi:10.52600/2763-583X.bjcr.2022.2.2.24-30
18. Santibañez-Bedolla KE, Orozco-Uriarte MJ, Alvarez-Canales JA, Macias AE, Amador-Medina LF. Oral colonization by gram-negative bacilli in patients with hematologic malignancies and solid tumors compared with healthy controls. BMC Oral Health. 2023;23(1). doi:10.1186/s12903-023-03172-y
19. Rosa DE, Setiadhi R. Necrotizing ulcerative gingivitis as a complication of febrile neutropenia in acute myeloid leukemia. Dentino Jurnal Kedokteran Gigi. pp:204–210. 10.20527/dentino.v8i2.17535
20. Al Beesh FA, Martini N, Suleiman S, Aljoujou, Aljoujou A. A. Oral manifestations associated with neutropenia in Syrian patients diagnosed with hematological malignancies and undergoing chemotherapy: a cross-sectional study. Medicine. 2024;103(2):e36780. doi:10.1097/MD.0000000000036780
21. Gasner NS, Brizuela M, Schure RS. Necrotizing Periodontal Diseases. [Updated 2025 Jul 7]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Available from: https://www.ncbi.nlm.nih.gov/books/NBK557417/.
22. Quispe RA, Aguiar EM, de Oliveira CT, Neves ACX, Santos PSDS. Oral manifestations of leukemia as part of early diagnosis. Hematol Transfus Cell Ther. 2022;44(3):392–401. doi:10.1016/j.htct.2021.08.006
23. Gollapudi M, Mohod S, Pankey N, Gatlewar P. Acute necrotizing ulcerative gingivitis: a case report. Cureus. 2024;16(6):e63023. doi:10.7759/cureus.63023
24. Zhu G, Wang Q, Lu S, Niu Y. Hydrogen Peroxide: a Potential Wound Therapeutic Target? Med Princ Pract. 2017;26(4):301–308. doi:10.1159/000475501
25. Dumitrel S-I, Matichescu A, Dinu S, et al. New insights regarding the use of relevant synthetic compounds in dentistry. Molecules. 2024;29(16):3802. doi:10.3390/molecules29163802
26. Muniz FWMG, Cavagni J, Langa GPJ, Stewart B, Malheiros Z, Rösing CK. A systematic review of the effect of oral rinsing with H2O2 on clinical and microbiological parameters related to plaque, gingivitis, and microbes. Int J Dent. 2020;2020:8841722. doi:10.1155/2020/8841722
27. Bruno JS, Heidrich V, Knebel FH, et al. Commensal oral microbiota impacts ulcerative oral mucositis clinical course in allogeneic stem cell transplant recipients. Sci Rep. 2022;12(1). doi:10.1038/s41598-022-21775-3
28. Gazal G, Al-Samadani KH, Alsaidalani HM, Karbouji GA, Alharbi AM. A comparison of pre-emptive co-amoxiclav, postoperative amoxicillin, and metronidazole for prevention of postoperative complications in dentoalveolar surgery: a randomized controlled trial. Int J Environ Res and Public Health. 19(7):4178. doi:10.3390/ijerph19074178
29. Dash S, Behera B, Sarkar N, Viswan P. Necrotizing periodontal diseases: a diagnosis not to be missed. Indian Dermatol. Online J. 2025;16(2):299–300. doi:10.4103/idoj.idoj_41_24
30. Permatasanti A, Fitriasari N, Sari NM, Wahyuni IS. Antioxidant Effect Of Mouthwash Containing Zinc, Aloe Vera, And Stabilized Chlorine Dioxide For Oral Manifestation of Acute Myeloblastic Leukemia (AML). Int J Appl Pharm. 15(Special Issue 2):58–62. doi:10.22159/ijap.2023.v15s2.11
31. Ridho F, Fitriasari N, Zakiawati D. Efficacy of chlorine dioxide on oral lesions in acute myeloblastic leukemia patients undergoing chemotherapy. Int J Appl Pharm. 15;(Special Issue 2):52–57. doi:10.22159/ijap.2023.v15s2.10
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.