Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 19
Oral Ivarmacitinib for Stable Vitiligo: Preliminary Observations from a Three-Patient Case Series
Authors Zhang W, Zhang Y ![]() , Wu R
, Wu R
Received 16 April 2026
Accepted for publication 1 July 2026
Published 15 July 2026 Volume 2026:19 617373
DOI https://doi.org/10.2147/CCID.S617373
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Michela Starace
Wei Zhang, Yingqi Zhang, Riga Wu
Department of Dermatology, The Affiliated Hospital of Inner Mongolia Medical University, Hohhot, 010050, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Riga Wu, Email [email protected]
Background: Vitiligo is an acquired autoimmune depigmenting disorder characterized by the loss of functional melanocytes. Patients with stable vitiligo may still experience slow repigmentation, marked inter-lesional variability, and limited responses to conventional therapies. The Janus kinase-signal transducer and activator of transcription (JAK-STAT) pathway is involved in the local immune-inflammatory response in vitiligo, and the highly selective JAK1 inhibitor ivarmacitinib may therefore warrant further investigation.
Case Description: This case series describes the 12-week clinical observations of three patients with stable vitiligo treated with oral ivarmacitinib. The patients included one male and two females, aged 12 to 50 years, with disease durations ranging from 9 to 36 months. The clinical subtypes included two cases of non-segmental generalized vitiligo and one case of non-segmental localized vitiligo. Two patients received ivarmacitinib 4 mg once daily, and one patient received 4 mg every other day. After 12 weeks of treatment, all three patients showed improvement in skin lesions compared with baseline. A total of 53 lesions were evaluated: 39 lesions (73.58%) showed complete or near-complete repigmentation, 12 lesions (22.64%) showed marked repigmentation, and 2 lesions (3.77%) showed moderate repigmentation; no lesions showed no response. Treatment response varied by anatomical site. Repigmentation was more pronounced on the face, neck, trunk, and extremities, whereas the response was slower on the hands and more limited on the elbows. VASI scores decreased from baseline in all three patients. No significant drug-related adverse reactions were observed during treatment.
Conclusion: This three-patient case series provides preliminary 12-week observational data on the use of oral ivarmacitinib for stable vitiligo. Owing to the small sample size, lack of a control group, inconsistent dosing regimens, and short follow-up period, these findings should be interpreted as descriptive clinical observations only and do not establish efficacy or long-term safety. Further validation in studies with larger sample sizes, standardized assessments, and prospective controlled designs is required.
Keywords: ivarmacitinib, vitiligo, JAK1 inhibitor, stable vitiligo, case series
Introduction
Vitiligo is an acquired autoimmune skin depigmentation disorder whose pathogenesis is closely associated with autoimmune responses, melanocyte destruction, and the local inflammatory microenvironment; current treatment options have limited efficacy.1 Recent studies have shown that Janus kinase (JAK) inhibitors can promote repigmentation by blocking the interferon-γ (IFN-γ) signaling pathway and inhibiting the recruitment of CD8⁺ T cells, highlighting their potential as a treatment option for vitiligo.2 JAK inhibitors are currently being explored for the treatment of vitiligo, with progress being made in this area. Topical formulations, such as 1.5% ruxolitinib cream, have been approved in multiple countries for the treatment of non-segmental vitiligo. Additionally, oral JAK inhibitors such as tofacitinib and baricitinib are also being used on an exploratory basis. Compared to topical formulations, oral JAK inhibitors may be more suitable for patients with multiple lesions, extensive affected areas, or those who do not respond significantly to topical treatment; however, their systemic safety still requires strict monitoring.
Ivarmacitinib is an oral, highly selective JAK1 inhibitor that, in theory, can more precisely block JAK1-mediated signaling pathways while minimizing interference with hematopoietic function, offering good safety potential.3 This drug has been approved in China for the treatment of moderate-to-severe atopic dermatitis and other conditions.4 However, clinical reports regarding its use for vitiligo are very limited.
Therefore, this study reports on the repigmentation outcomes and safety observations in three patients with stable-phase vitiligo following 12 weeks of oral ivarmacitinib treatment, aiming to provide preliminary case data to serve as a reference for future research.
Patients
This retrospective case series included three patients with stable vitiligo who received oral ivarmacitinib at the Department of Dermatology, The Affiliated Hospital of Inner Mongolia Medical University from March 2025 to March 2026. All three patients were evaluated at week 12, which was used as the primary assessment time point in this case series. Case 1 and Case 2 continued treatment beyond week 12 according to clinical response and follow-up availability, but only week 12 outcomes were included in the main analysis for consistency. Informed consent was obtained from all adult patients or guardians of minor patients.
Inclusion criteria were a diagnosis of vitiligo confirmed by Wood’s lamp or skin computed tomography according to the 2024 Chinese Consensus on Diagnosis and Treatment of Vitiligo; stable disease, defined as the absence of new lesions, no enlargement of existing lesions, no Koebner phenomenon for ≥1 year, and a Vitiligo Disease Activity (VIDA) score ≤0; poor response or ineffective to prior conventional treatments (such as corticosteroids or phototherapy); acceptable baseline laboratory results, including routine blood tests, liver/kidney function, coagulation profiles, hepatitis B screening, tuberculosis screening, and tumor marker assessments. Exclusion criteria were active infection, severe organ diseases, hematologic diseases, or malignancy; pregnancy or lactation; hypersensitivity to ivarmacitinib.
Treatment Regimen
Ivarmacitinib tablets (4 mg/tablet) were administered orally. Two patients (Case 1 and Case 3) received ivarmacitinib 4 mg once daily, and one patient (Case 2) received ivarmacitinib 4 mg every other day. During the 12-week observation period, no concomitant vitiligo-directed treatments, including topical corticosteroids, topical calcineurin inhibitors, phototherapy, or laser therapy, were administered.
Clinical Response Assessment
Baseline demographic and clinical data were collected, including age, sex, disease duration, lesion distribution, clinical subtype, Vitiligo Disease Activity score, and Vitiligo Area Scoring Index score. Clinical responses were assessed at week 12 using standardized clinical photographs and VASI changes.
Repigmentation was evaluated on a lesion-by-lesion basis and categorized as complete or near-complete repigmentation (≥90%), marked repigmentation (50–89%), moderate repigmentation (25–49%), or poor repigmentation (<25%). The proportion of lesions achieving complete or marked repigmentation was calculated descriptively. The proportion of lesions showing any measurable repigmentation, defined as complete, marked, or moderate repigmentation, was also summarized.
VASI scores at baseline and week 12 were recorded for each patient. The percentage improvement in VASI was calculated for each individual patient, and the mean value was presented descriptively. Because of the small sample size, absence of a control group, and heterogeneous dosing regimens, all response outcomes were interpreted as descriptive clinical observations rather than evidence of treatment efficacy.
Safety Monitoring
Routine blood tests, liver and kidney function, and lipid profiles were tested before and after treatment. Cutaneous and gastrointestinal adverse events were recorded.
Statistical Analysis
All data were analyzed descriptively. Continuous variables are presented as mean ± SD, and categorical variables as counts (percentages).
Case Report
Patient A, a 14-year-old female, presented to our outpatient clinic with multiple depigmented patches on the head, face, trunk, and limbs that had persisted for more than two years. She was diagnosed with stable non-segmental generalized vitiligo. At baseline, a total of 41 lesions were identified on the face, neck, trunk, and limbs (Figure 1A), and her VASI score was 11.43, representing the most extensive disease among the three patients. Previous treatment with topical and oral medications had produced poor responses, although the specific medications and dosages were not available. The patient received oral ivarmacitinib 4 mg once daily for 12 weeks. After 12 weeks of treatment, her VASI score decreased to 0.13. At the lesion level, 37 lesions showed ≥90% repigmentation, and 4 lesions showed 50–89% repigmentation (Figure 1B). During treatment, no clinically significant abnormalities were observed in complete blood count, liver or kidney function, or lipid profile, and no serious adverse events were recorded.
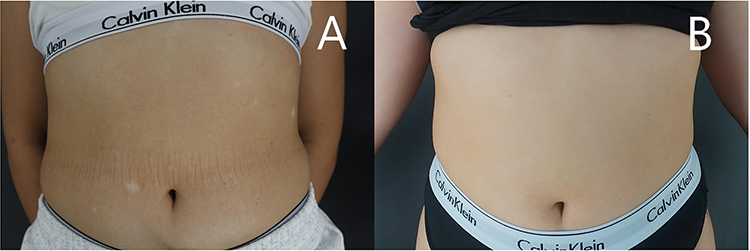 |
Figure 1 Patient A lesions on the trunk before (A) and after (B) treatment. |
Patient B, a 12-year-old female, presented with two depigmented patches on both elbows that had persisted for more than two years. She was diagnosed with stable non-segmental localized vitiligo. At baseline, the lesions were confined to the elbows, with a total of two patches (Figure 2A), and her VASI score was 0.50. Previous treatments included oral Qubai Babuqi tablets (two tablets three times daily), topical tacrolimus ointment, fluticasone propionate cream, 2% crisaborole ointment, and intermittent helium–neon (He–Ne) laser phototherapy; however, no significant improvement was observed. The patient received oral ivarmacitinib 4 mg every other day for 12 weeks. After 12 weeks of treatment, her VASI score decreased to 0.33, and both lesions showed 25–49% repigmentation (Figure 2B). During treatment, no clinically significant abnormalities were observed in complete blood count, liver or kidney function, or lipid profile, and no serious adverse events were recorded.
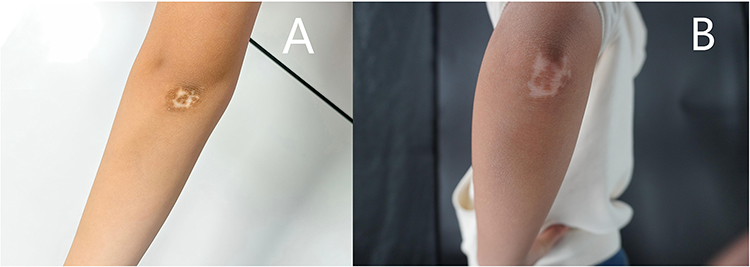 |
Figure 2 Patient B lesions on elbow before (A) and after (B) treatment. |
Patient C, a 50-year-old male, presented with depigmented patches on the fingertips of both hands that had persisted for more than six months. He was diagnosed with stable non-segmental generalized vitiligo. At baseline, the lesions were located on both hands, with a total of 10 patches (Figure 3A), and his VASI score was 1.20. Previous treatment with topical and oral medications had produced poor responses, although the specific medications and dosages were unknown. The patient received oral ivarmacitinib 4 mg once daily for 12 weeks. After 12 weeks of treatment, his VASI score decreased to 0.48. At the lesion level, 2 lesions showed ≥90% repigmentation, and 8 lesions showed 50–89% repigmentation (Figure 3B). During treatment, no clinically significant abnormalities were observed in complete blood count, liver or kidney function, or lipid profile, and no serious adverse events were recorded.
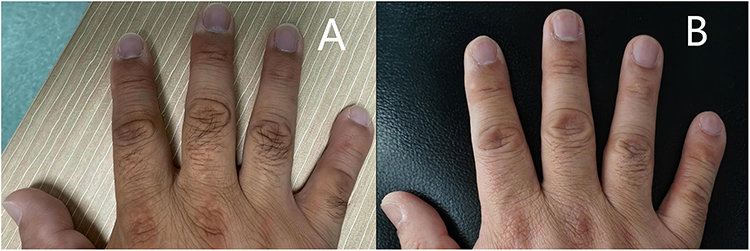 |
Figure 3 Patient C lesions on hands before (A) and after (B) treatment. |
Summary of Patient Demographics and 12-Week Observation Results
The baseline demographic and clinical characteristics of the three patients are summarized in Table 1. The patients included two females and one male, aged 12 to 50 years, with disease durations ranging from 9 to 36 months. Two patients had non-segmental generalized vitiligo, and one patient had non-segmental localized vitiligo. A total of 53 lesions were evaluated across the three patients. The 12-week clinical outcomes and VASI changes are summarized in Table 2. After 12 weeks of oral ivarmacitinib treatment, all three patients showed reductions in VASI scores, and all evaluated lesions showed measurable repigmentation.
 |
Table 1 Baseline Characteristics of Three Patients with Stable Vitiligo |
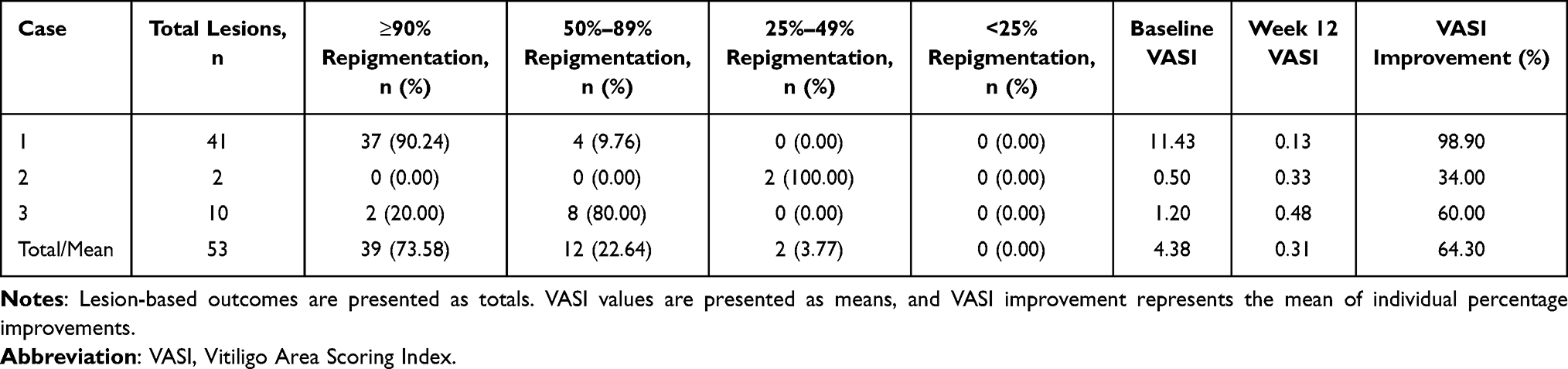 |
Table 2 Clinical Outcomes and VASI Changes After 12 weeks of Treatment |
Discussion
Vitiligo is a common acquired autoimmune depigmenting skin disorder that can occur at any age and affects approximately 0.36% of the global population.5 Vitiligo severely impairs patients’ quality of life. Although the pathogenesis of vitiligo has not yet been fully elucidated, available evidence indicates that CD8⁺ T cell-mediated melanocyte destruction is a key pathogenic mechanism.6 Activated CXCR3⁺ CD8⁺ T cells infiltrate lesional skin and secrete IFN-γ, which binds to receptors on keratinocytes and activates the JAK-STAT pathway, particularly JAK1/JAK2 and STAT1. This signaling cascade induces the expression of CXCL9, CXCL10, and CXCL11, which further recruit CXCR3⁺ CD8⁺ T cells, thereby forming a self-amplifying inflammatory loop that promotes melanocyte apoptosis.7 JAKs are a family of the cytoplasmic tyrosine kinases comprising four members: JAK1, JAK2, JAK3, and TYK2. Multiple cytokines exert their biological effects through the JAK/STAT pathway. In vitiligo, JAK1 and JAK2 are recruited by the IFN-γ receptor complex, leading to STAT phosphorylation, nuclear translocation, and subsequent transcriptional activation of IFN-γ-responsive genes.8 Based on this mechanism, JAK inhibitors suppress IFN-γ signaling, reduce chemokine production, and inhibit T-cell recruitment. Thus, blocking the JAK-STAT pathway is a rational therapeutic target in vitiligo.
JAK inhibitors, including ruxolitinib, baricitinib, and tofacitinib, have shown therapeutic potential in vitiligo.9,10 Compared with these agents, ivarmacitinib is a highly selective oral JAK1 inhibitor with approximately 9-fold selectivity for JAK2 and 77-fold selectivity for JAK3,11 which may theoretically reduce off-target inhibition of JAK2- and JAK3-mediated signaling pathways.12 It has been approved in China for the treatment of atopic dermatitis and has also demonstrated favorable efficacy and safety in clinical studies of alopecia areata.13,14 These pharmacological characteristics provide a rationale for further investigation of ivarmacitinib in vitiligo.
In the present case series, oral ivarmacitinib treatment was associated with varying degrees of repigmentation in three patients with stable vitiligo after 12 weeks of observation. However, given the uncontrolled design and extremely small sample size, these findings should be interpreted as preliminary clinical observations. After 12 weeks of treatment, repigmentation was observed in all lesions in the three patients, with high rates of complete repigmentation on the face/neck, trunk, and limbs, followed by the hands, whereas the elbows responded more slowly. These findings are consistent with previous studies on JAK inhibitors, which showed that acral lesions (especially joint lesions) tend to respond less favorably, possibly due to differences in local hair follicle density, blood supply, and skin thickness.15,16 In this report, Case 1 and Case 3 received ivarmacitinib 4 mg once daily, whereas Case 2 received 4 mg every other day. Because of the very small sample size, heterogeneous lesion sites, and inconsistent dosing regimens, no conclusion regarding a dose-response relationship can be drawn from this case series. In particular, the relatively limited response in Case 2 may be related not only to the lower dosing frequency but also to the location of the lesions on the elbows, which are generally considered more difficult to repigment. During the 12-week observation period, no concomitant vitiligo-directed treatments, including topical corticosteroids, topical calcineurin inhibitors, phototherapy, or laser therapy, were administered. This reduces, but does not eliminate, uncertainty regarding treatment attribution. Because this was not a controlled study, spontaneous repigmentation, site-related variability, prior treatment effects, and assessment bias cannot be fully excluded. In terms of safety, no patients experienced significant adverse events with normal laboratory tests, consistent with the favorable safety profile of JAK inhibitors.17 Nevertheless, the short follow-up duration and small number of patients preclude any conclusion regarding the long-term safety of oral ivarmacitinib in patients with vitiligo. Systemic JAK inhibitors require careful safety monitoring, especially when used off-label or in pediatric patients.
This case series has several important limitations. First, the sample size was extremely small, and the study was conducted at a single center without a control group. Second, the dosing regimens were not uniform, and lesion sites differed among patients, which may have influenced treatment responses. Third, the follow-up period was limited to 12 weeks, and no data on long-term maintenance of repigmentation, relapse after discontinuation, or long-term safety were available. Fourth, clinical assessments were descriptive and may have been affected by non-blinded evaluation and photographic variability. Finally, lesion-level summaries may overrepresent responses in patients with multiple lesions and should therefore be interpreted cautiously.
Conclusion
This series of three cases describes repigmentation following 12 weeks of oral ivarmacitinib treatment for stable-phase vitiligo. Repigmentation of varying degrees was observed in all patients, and no serious adverse events were recorded in the short term. Given the extremely small sample size, lack of a control group, inconsistent dosing, and short follow-up period, these results should be considered only as exploratory clinical observations. The role of ivarmacitinib in stable-phase vitiligo requires further confirmation through prospective, controlled, standardized evaluation and long-term follow-up studies.
Ethics Review
This case series was conducted in accordance with the principles of the Declaration of Helsinki. According to the ethics review statement issued by the Ethics Office of The Affiliated Hospital of Inner Mongolia Medical University, this case series was not considered clinical research and therefore did not require formal ethics review. Written informed consent for treatment and for publication of anonymized clinical information and images was obtained from all patients or their legal guardians.
Acknowledgments
The authors thank the patients and their families for their participation and cooperation.
Author Contributions
Wei Zhang and Yingqi Zhang contributed equally to this work and should be regarded as co-first authors. Riga Wu is the corresponding author. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas. All authors took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Natural Science Foundation of Inner Mongolia Autonomous Region (2020MS08112), Inner Mongolia Medical University (YKD2021MS039), and the Joint Research Fund for Public Hospitals of Inner Mongolia Academy of Medical Sciences–Key Project (2025GLLH0104).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Liu K, Zhou L, Shi M, et al. JAK inhibitors in immune regulation and treatment of vitiligo. Cytokine Growth Factor Rev. 2024;80:87–7. doi:10.1016/j.cytogfr.2024.11.002
2. Speeckaert R, Caelenberg EV, Belpaire A, Speeckaert MM, Geel NV. Vitiligo: from pathogenesis to treatment. J Clin Med. 2024;13(17):5225. doi:10.3390/jcm13175225
3. Yan T, Wang T, Tang M, Liu N. Comparative efficacy and safety of JAK inhibitors in the treatment of moderate-to-severe alopecia areata: a systematic review and network meta-analysis. Front Pharmacol. 2024;15:1372810. doi:10.3389/fphar.2024.1372810
4. J KS. Ivarmacitinib sulfate: first approval. Drugs. 2025;85(9):1163–1170. doi:10.1007/s40265-025-02202-z
5. Seneschal J, Bae JM, Ezzedine K, et al. Vitiligo. Nature Reviews Disease Primers. 2025;11(1):85. doi:10.1038/s41572-025-00670-x
6. Frisoli ML, Essien K, Harris JE. Vitiligo: mechanisms of pathogenesis and treatment. Ann Rev Immunol. 2020;38:621–648. doi:10.1146/annurev-immunol-100919-023531
7. Qi F, Liu F, Gao L. Janus kinase inhibitors in the treatment of vitiligo: a review. Front Immunol. 2021;12:790125. doi:10.3389/fimmu.2021.790125
8. Rosmarin D, Pandya AG, Lebwohl M, et al. Ruxolitinib cream for treatment of vitiligo: a randomised, controlled, Phase 2 trial. Lancet. 2020;396(10244):110–120. doi:10.1016/S0140-6736(20)30609-7
9. Samuel C, Cornman H, Kambala A, Kwatra SG. A review on the safety of using JAK inhibitors in dermatology: clinical and laboratory monitoring. Dermatol ther. 2023;13(3):729–749. doi:10.1007/s13555-023-00892-5
10. Inoue S, Suzuki T, Sano S, Katayama I. JAK inhibitors for the treatment of vitiligo. J Dermatological Sci. 2024;113(3):86–92. doi:10.1016/j.jdermsci.2023.12.008
11. Liu J, Jiang Y, Zhang S, et al. Ivarmacitinib, a selective Janus kinase 1 inhibitor, in patients with moderate-to-severe active rheumatoid arthritis and inadequate response to conventional synthetic DMARDs: results from a Phase III randomised clinical trial. Ann Rheumatic Dis. 2025;84(2):188–200. doi:10.1136/ard-2024-226385
12. Gupta AK, Bamimore MA, Mirmirani P, Piguet V, Talukder M. The relative efficacy and safety of monotherapies for alopecia areata: a Network Meta-Analysis Study. J Cosmet Dermatol. 2025;24(4):e70185. doi:10.1111/jocd.70185
13. Zhou C, Yang X, Yang B, et al. A randomized, double-blind, placebo-controlled Phase II study to evaluate the efficacy and safety of ivarmacitinib (SHR0302) in adult patients with moderate-to-severe alopecia areata. J Am Acad Dermatol. 2023;89(5):911–919. doi:10.1016/j.jaad.2023.02.063
14. Zhou C, Yang C, Fan W, et al. Ivarmacitinib for the treatment of adults with severe alopecia areata: results from a Phase 3 trial. J Am Acad Dermatol. 2026;94(1):161–171. doi:10.1016/j.jaad.2025.09.044
15. Phan K, Phan S, Shumack S, Gupta M. Repigmentation in vitiligo using Janus Kinase (JAK) inhibitors with phototherapy: systematic review and Meta-analysis. J Dermatol Treat. 2022;33(1):173–177. doi:10.1080/09546634.2020.1735615
16. Zhang R, Chen X, Huang H, et al. Targeted synergy for vitiligo in refractory areas: a real-world study of ruxolitinib cream combined with 308-nm excimer lamp. J Am Acad Dermatol. 2026;S0190-9622(26):00302–00306.
17. Mohammed AA, Lengyel AS, Meznerics FA, et al. Efficacy and safety of JAK inhibitors in the management of vitiligo: a systematic review and meta-analysis. Dermatol ther. 2025;15(7):1657–1679. doi:10.1007/s13555-025-01397-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.