Back to Journals » Drug Design, Development and Therapy » Volume 19
Optimizing Lidocaine Dosing in Hepatectomy Patients: A Population Pharmacokinetic Study of Active Metabolites
Authors He C, Qi X, Liu Y, Jin Y, Zhang M, Zhang Y, Fu L, Zheng L ![]() , Tu F
, Tu F ![]() , Wang Z
, Wang Z ![]()
Received 3 July 2024
Accepted for publication 4 July 2025
Published 22 July 2025 Volume 2025:19 Pages 6255—6268
DOI https://doi.org/10.2147/DDDT.S485389
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Georgios Panos
Chaoqun He,1– 3 Xiaohui Qi,1,3 Yixian Liu,1,3 Ying Jin,1,3 Mengyu Zhang,1,3 Yang Zhang,4 Lisha Fu,1,3 Li Zheng,1,3 Faping Tu,2 Zhenlei Wang1,3
1Department of Pharmacy, NMPA Key Laboratory for Clinical Research and Evaluation of Innovative Drug, West China Hospital, Sichuan University, Chengdu, Sichuan, 610041, People’s Republic of China; 2Department of Anesthesiology, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan, 637000, People’s Republic of China; 3Clinical Trial Center, West China Hospital, Sichuan University, Chengdu, Sichuan, 610041, People’s Republic of China; 4Department of Anesthesiology, Suining Central Hospital, Suining, Sichuan, 629000, People’s Republic of China
Correspondence: Faping Tu, Email [email protected] Zhenlei Wang, Email [email protected]
Background: Lidocaine and its active metabolites are metabolized mainly by the liver, and liver-compromised may slow the metabolism of lidocaine and its active metabolites. In addition to excessive lidocaine, accumulated active metabolites may also lead to lidocaine-related toxicity in liver-compromised patients. This study aimed to describe the population pharmacokinetics of lidocaine and its active metabolites in partial hepatectomy patients and propose a novel drug regimen involving lidocaine-weighted active metabolites.
Methods: The concentrations of lidocaine and its active metabolites from thirty-five patients underwent partial hepatectomy were analysed by non-linear mixed-effects models. The mean loading dose was 86.07 mg, and the median continuous infusion dose was 57.97 mg/h. A population pharmacokinetic model fitting the plasma concentrations of lidocaine and its active metabolites was built to explore the factors affecting the concentrations of lidocaine and its active metabolites.
Results: A two-compartment model with first-order elimination was used to determine the concentrations of lidocaine and its active metabolites. The different dosing simulations revealed that the selected appropriate loading dose did not exceed 1.5 mg/kg, and the continuous infusion dose of lidocaine should preferably not surpass 1.5 mg/kg/h in Chinese hepatectomy patients. The simulation results of long-term infusion of lidocaine during the postoperative stage after liver resection that showed there was a significant accumulation of MEGX after more than 24 hours of lidocaine infusion, and when the infusion rate reached 1 mg/kg/h, the MEGX concentration exceeded 5 μg/mL.
Conclusion: This study proposes for the first time the integration of lidocaine concentration with active metabolites and simulation-based dosing recommendations. During the 24-hour medication period for Chinese hepatectomy patients, the recommended safe dosage includes a loading dose not exceeding 1.5 mg/kg and an infusion dose not exceeding 1.5 mg/kg/h. Monitoring of active metabolites, in addition to lidocaine is also necessary for continuous infusion of lidocaine.
Trial Registration: The trial is registered at chictr.org.cn (ChiCTR2100042730).
Keywords: hepatectomy, lidocaine, active metabolites, population pharmacokinetics, dose simulation
Introduction
Hepatectomy is an important treatment for benign and malignant liver diseases, and China has the highest number of cases of liver resection worldwide.1 Previous studies have shown that approximately 60% of liver resection patients suffer from moderate-to-severe pain after surgery.2 Poor postoperative pain management may increase the incidence of postoperative complications in patients and affect rapid recovery.3,4 Epidural analgesia, as a first-line treatment for postoperative pain relief in abdominal surgery,5 is not suitable for all patients and may increase the risk of epidural hematoma in hepatectomy patients.6,7 Opioids can cause nausea and vomiting, suppress gastrointestinal motility and respiratory depression in patients, and affect postoperative recovery. Compared with epidural analgesia and opioids, intraoperative infusion of lidocaine shows excellent performance in reducing postoperative pain, reducing opioid consumption, and promoting postoperative recovery.8,9 The therapeutic concentration range of lidocaine is relatively narrow,10–13 and overdosing lidocaine may cause toxic events. Lidocaine and its active metabolites are metabolized mainly by the liver, so hepatic impairment patients are more prone to toxic events,14 which may limit the application of lidocaine in hepatectomy patients. In addition, hepatectomy is a controllable planned liver injury that differs from other liver injuries in terms of injury mechanisms. Compared to drug-induced or chronic viral hepatitis, hepatectomy patients provide a more homogeneous population for lidocaine PopPK modeling: (1) Drug-induced hepatitis patients are caused by taking hepatotoxic drugs. If lidocaine is added to drug-induced hepatitis patients at the same time, it may not only worsen liver damage but also introduce uncontrolled confounding factors (such as CYP450 interactions) into lidocaine PK studies.15 (2) Chronic hepatitis (decompensated cirrhosis): Fibrosis and portal hypertension alter lidocaine metabolism independently of liver volume. The injury mechanism of liver resection patients is single, and post-hepatectomy PK correlates directly with the fraction of liver remaining, making it a more predictable model.16 (3) Lidocaine is used for acute post-op pain in hepatectomy, whereas drug-induced/chronic hepatitis patients rarely require intravenous infusion of lidocaine.
A well known commonly used standard for evaluating safety is a concentration of lidocaine exceeding 5 µg/mL.17,18 More than 75% of lidocaine undergoes N-deethylation to form monoethylglycinexylidide (MEGX), while the remaining lidocaine is partially excreted in the prototype form or partially hydrolyzed or oxidized to produce other compounds.19 The metabolism of MEGX is similar to that of lidocaine but it is not completely transformed into glycinexylide (GX).19 The metabolites MEGX and GX are 99% and 26% as potent as lidocaine in terms of antiarrhythmic potency, respectively.20 The toxic effects of lidocaine not only are related to lidocaine but are also possibly associated with the accumulation of MEGX and GX.20,21 A subject who experienced blurred vision and numbness of the tongue during a GX injection was reported by Strong et al.21 Adverse events are more likely to occur when lidocaine and MEGX are injected simultaneously.22 Unfortunately, this safety standard seems to focus only on lidocaine and overlooks metabolites with the similar pharmacological activity,9,23 which may cause potential hazards to patients.
A large number of published clinical studies and meta-analyses have shown that perioperative infusion of lidocaine is indeed effective, but these results are likely produced by differences in load doses, infusion doses, and even infusion durations during nonhepatectomy.9 Kuo et al demonstrated that intravenous injection of lidocaine can effectively relieve pain, although compared to Koppert et al’s study protocol,24 patients undergoing the same type of surgery received higher loading (2.0 mg/kg) and infusion (3.0 mg/kg/h) doses.25 However, Kuo et al did not seem to have paid attention to the potential poisoning risk that high-dose lidocaine may have to patients. In addition, although hepatectomy patients also benefit,23 the metabolism of lidocaine and monoethylglycinexylidide (MEGX) may be easily affected in hepatectomy patients by hemodynamic changes,26 liver injury27,28 and liver cirrhosis,29 leading to an increase in exposure. The predetermined lidocaine administration regimen for hepatectomy patients may need to be adjusted after liver resection is completed. For the above reasons, it is difficult for anesthesiologists to determine when and how to adjust the infusion rate of lidocaine for hepatectomy patients, which may be why intravenous infusions of lidocaine have not been widely used in such patients.
The purpose of this study was to explore the effects of liver resection on the pharmacokinetics of lidocaine and its active metabolites and to propose a novel dosing regimen of lidocaine weighted activity metabolites, exploring whether the infusion rate of lidocaine needs to be adjusted by increasing or decreasing during liver resection or after liver tissue separation.
Methods
Study Design and Patients
We conducted a single-center, prospective and open-label study of partial hepatectomy patients with an initial diagnosis of liver tumor from January to December 2021 at the Affiliated Hospital of North Sichuan Medical College, Nanchong, China.30 All procedures in the experiment were carried out by the Helsinki Declaration. This study was approved by the Ethics Committee of the Affiliated Hospital of North Sichuan Medical College (2021ER029-1) and registered at the Chinese Clinical Trial Registry (http://www.chictr.org.cn; ChiCTR-2100042730).30 The patients could be included in the study only after providing informed written consent. The inclusion criteria was age 18 to 65 years with a body mass index (BMI) between 18 and 30 kg/m2. Severe hepatic insufficiency (total bilirubin > 2 mg/dL), severe renal dysfunction (glomerular filtration rate < 30 mL/min/1.73m2), severe heart disease (severe heart block, sinus bradycardia, Adams-stokes syndrome, and preexcitation syndrome, etc.), ideal body weight (IBW) < 40 kg, allergy, a history of epilepsy, and a long-term history of drug use affecting lidocaine metabolism constitute the exclusion criteria. Patients were given a loading dose of 1.5 mg/kg lidocaine at the initiation of anesthesia induction and the injection duration exceeded 10 min. Soon forward, lidocaine was continuously infused until the surgery was completed. Considering the safety of patients undergoing hepatectomy, the continuous infusion rate of lidocaine was adjusted from the recommended 1.5 mg/kg/h to 1.0 mg/kg/h.31 The specific time to discontinuous lidocaine infusion was determined by the anesthesiologist.
The characteristics of each patient were recorded, including age, sex, height, total body weight (TBW), IBW, BMI, preoperative liver function indices, extent of liver resection (segment or lobe resection), absence or presence of liver cirrhosis (Child-Pugh score), total number and duration of Pringle maneuvers, tumor size, and total doses of lidocaine.
Blood Sampling and Plasma Concentration Assay
Baseline blood samples were drawn through a central venous catheter just before induction of anesthesia. Subsequent samples (2 mL) were collected at 0.5 h and every 1 h after the start of the operation, as well as at 0, 0.5, 1, 2, 4, 8, and 12 h after the end of the operation. A centrifuge tube containing a 50 µL plasma sample was added to 150 µL acetonitrile containing 60 ng/mL internal standard for protein precipitation. Then, vortex for 1 min and centrifuge at 13000 rpm for 10 min to obtain the supernatant. Mix 40 µL of supernatant with 160 µL of mobile phase A formic acid water (1:1000, v/v), vortex again for 30s, and inject a volume of 7.5 µL. The concentrations of lidocaine and its active metabolites were measured via an ultra-performance liquid chromatography-tandem mass spectrometry method.32 The lower limit of qualification (LLOQ) of lidocaine, MEGX, and GX was 10, 2, and 2 ng/mL, respectively. And, the detection ranges for lidocaine, MEGX and GX are as follows: 10–5000 ng/mL, 2–1000 ng/mL and 2–500 ng/mL.
Population Pharmacokinetic Modeling
Lidocaine, MEGX and GX time courses were analyzed using first-order conditional estimation with the interaction method in NONMEM® (version 7.2.0; ICON Development Solutions, Ellicott city, MD, USA). R software (version 4.2.3; R Foundation for Statistical Computing, Vienna, Austria) and RStudio (version 22.0.3; RStudio, Inc., Boston, MA, USA) were used to graphically evaluate the goodness-of-fit (GOF) and prediction-corrected visual predictive check (pcVPC) of the final model (Supplymentary Material Table S1). Initially, one-, two-, and three-compartment models with and without delay time were used to fit the lidocaine data during the model development process. The distribution volume of metabolites was set equal to that of central lidocaine. This was not only due to the lack of metabolite pharmacokinetic data but also because the use of the same distribution volume could make the clearance of the lidocaine and its active metabolites more comparable.
The between-subject variability (BSV, η) was estimated by additive, proportional, and exponential models. Finally, an exponential model was introduced. The BSV was assumed to be log-normally distributed and was expressed as θi = θTV × exp (ηi), where θi represents the predictive values of individual i, θTV is the topical value of the population parameters, and ηi represents the BSV. In addition, the proportional errors model was considered to illustrate the residual variability (ε) caused by inexplicability between the predictive and observed data, shown as Yij = Fij × (1 + εij), where Yij represents the jth observed concentration of the ith individual, Fij is the jth predicted concentration of the ith individual, and εij represents residual error.
To screen out the potential covariates, we adopted the stepwise method to search for covariates (Supplementary Material Figure S1). Forward addition meant that covariates causing the decline of the objective function values (OFV, –2 log likelihood) exceeding 3.84 (χ2, P < 0.05) were successively added to the model. Subsequently, the model with the largest decrease in OFV was used as the basis for the second round of screening, and the covariates that could cause the most significant decrease in OFV in this round were added again. The process of forward addition was not completed until no remaining covariates were included or there were no longer covariates that could result in the OFV to decrease by more than 3.84. Backward elimination implemented a more stringent similarity strategy in which the removal of covariate would permanently be rejected from the model unless it resulted in a significant increase in OFV > 6.63 (χ2, P < 0.01). The process of backward election was not completed until all covariates that did not meet elimination strategy were removed or the removal of remaining covariates did not cause a significant increase in OFV.
The evaluation of the final model was achieved through GOF, pcVPC and bootstrapping. The GOF was assessed by the visual inspection of data fitting and model diagnostic plots of GOF, including population predicted and individual predicted vs observed concentration plots, time and population prediction vs conditional weighted residual. The pcVPC checked the performance of the model by comparing the 5th, 50th, and 95th quantile concentrations of the simulated 95% confidence interval (1000 replicates) with the observed concentrations. The uncertainty of parameter evaluation was assessed by bootstrapping data sets (N = 1000) to obtain a 95% confidence interval (CI) for the final estimated value of each parameter.
Simulation and Weighted Lidocaine Exposure
To estimate the peak concentration (Cmax) of lidocaine, simulations of lidocaine concentrations at different loading doses (1.0, 1.5 and 2.0 mg/kg) and infusion doses (1.0, 1.5, 2.0 and 3.0 mg/kg/h) were performed. In addition, to investigate the concentrations of lidocaine and active metabolites continuously administered during the postoperative stage after liver resection, we also simulated the postoperative recommended lidocaine infusion doses in existing liver resection studies.23,33 The weighting scheme originated from Crouch et al’s exploration of whether the concentration of the independent lidocaine and the weighted concentration of lidocaine with active metabolites exceeded 5 µg/mL.33 The weighted concentrations of lidocaine, MEGX and GX were calculated as the sum of the concentrations: lidocaine + MEGX + 0.25 × GX.
Results
Patient Characteristics
The demographic data are listed in Table 1. Overall, 35 patients—28 males and 7 females—were included in this study. Among the 35 patients, 27 patients had postoperative pathological findings indicating hepatocellular carcinoma, 5 patients had cholangiocarcinoma, 2 patients had benign lesions with focal hyperplasia, and the remaining had liver metastasis from adrenal malignant mesothelioma. Among the 33 patients, except for one patient with a Child-Pugh B grade, the remaining 32 patients have a Child-Pugh A grade. The median age was 53 (20–65) years, and median short infusion dose was 86 (9.57) mg. The mean continuous infusion duration was 3.9 (1.62) h due to inconsistency in the surgical duration for each patient. Thus, the median infusion rate calculated from the IBW and infusion duration was 0.99 (0.62–1.54) mg/kg/h. No severe adverse events, deaths or serious postoperative complications were reported in any patients throughout the perioperative period.
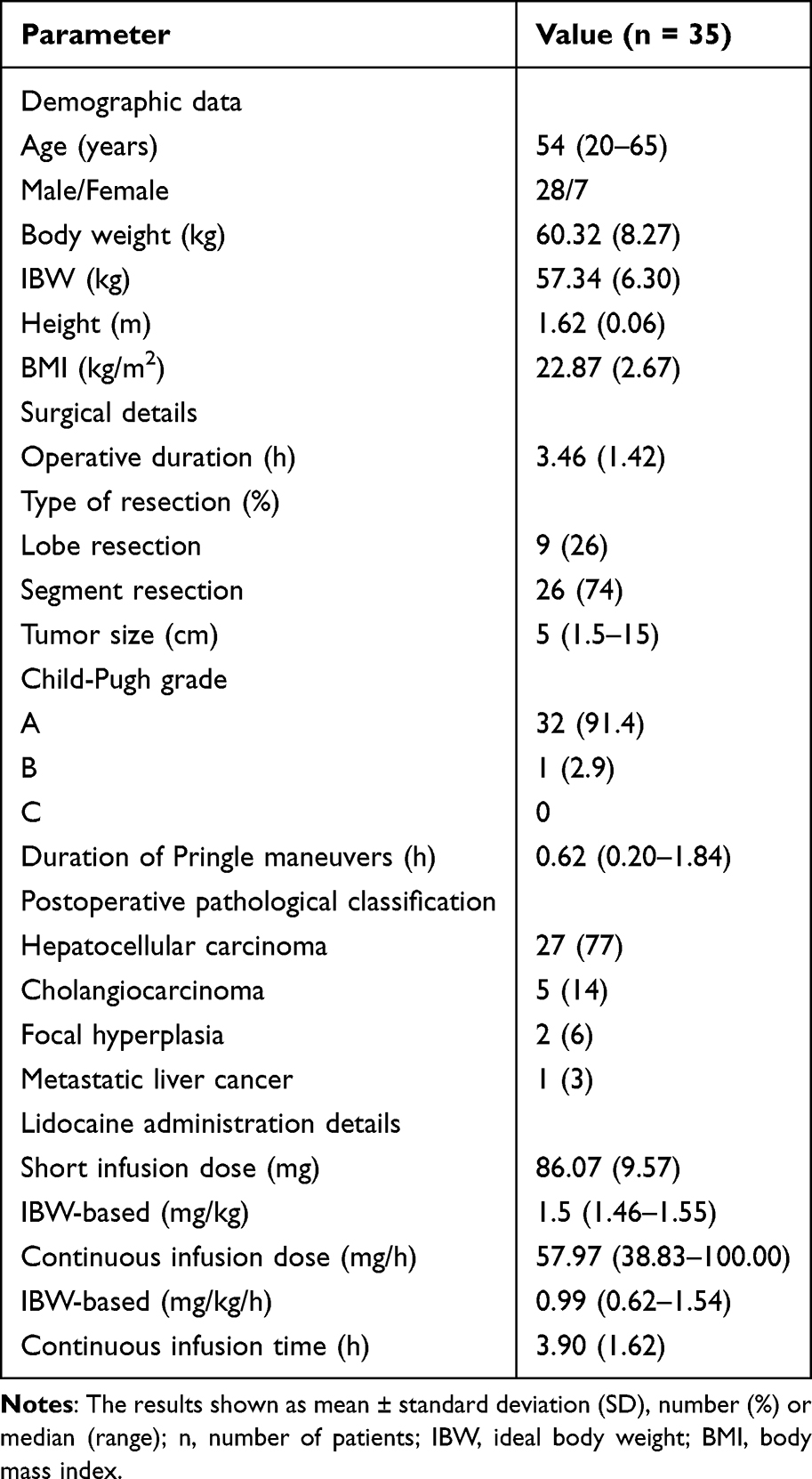 |
Table 1 Demographics Characteristics of Hepatectomy Patients in the Population Pharmacokinetic Model |
The observed and simulated lidocaine concentrations and weighted concentrations at various time points are summarized in Figure 1. The observed lidocaine Cmax of all patients was less than 5 µg/mL (Figure 1Ai), except for one patient sample collected 0.5 h at the beginning of surgery due to improper operation. Although the weighted Cmax also exceeded 5 µg/mL (Figure 1Aii), it seems that there was not much difference compared to the Cmax of observed lidocaine alone. Observation and follow-up of the patient during and after surgery did not reveal any serious cardiovascular, respiratory, or neurological symptoms related to lidocaine toxicity. By simulating the concentrations of lidocaine and its active metabolites, the median Cmax of lidocaine alone was determined to be 1.6 (1.0–3.4) µg/mL, and the median Cmax of weighted concentration is 1.9 (1.1–3.6) µg/mL (Figure 1Aii). The observed lidocaine concentration (Figure 1Bi) and the weighted concentration (Figure 1Ci) gradually increased and reached their Cmax during and after hepatectomy. The observed lidocaine concentration and the weighted concentration rapidly decreased at the end of the surgery, and by 4 hours after the surgery, the concentration had completely decreased below 1 µg/mL. The median concentration of immediate bolus lidocaine obtained from the simulation was 2.58 (0.96–4.91) µg/mL (Figure 1Bii).
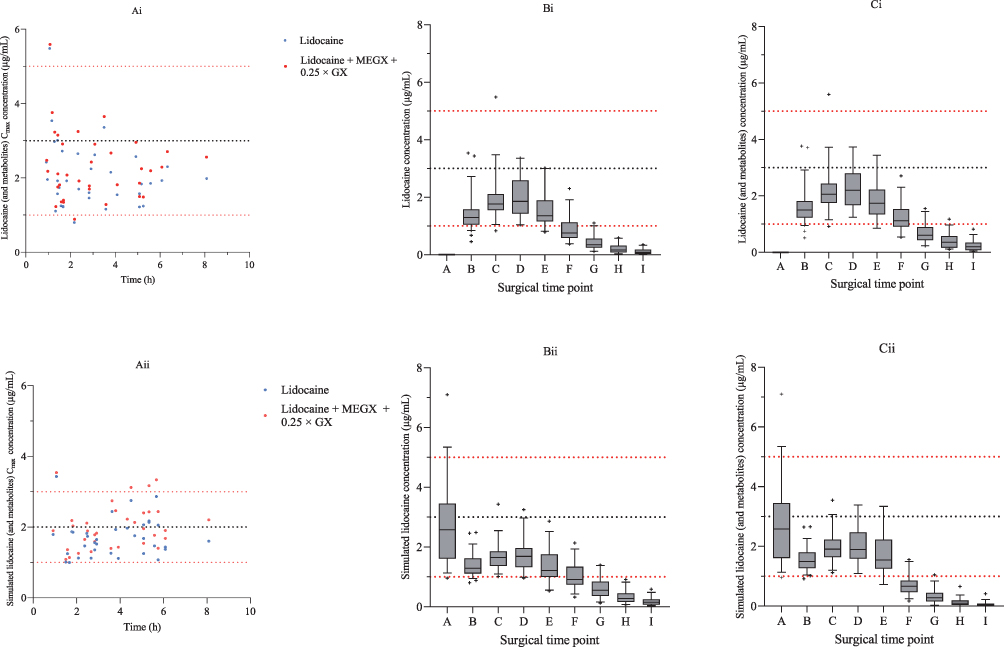 |
Figure 1 Summarized plasma concentrations of lidocaine and the weighted concentrations of lidocaine, MEGX and GX in observed and simulated results. Individual plasma lidocaine concentrations are represented by blue dots in both observed (Ai–Ci) and simulated (Aii–Cii) results, and the weighted peak concentration of lidocaine, MEGX and GX are represented by red dots. Notes: The values are at the following time points: column A, immediately after bolus (preoperative); column B, before hepatectomy; column C, during hepatectomy; column D, after hepatectomy; column E, immediately after the end of surgery; column F, 2 h after the end of surgery; column G; 4 h after the end of surgery; column H, 8 h after the end of surgery; column I, 12 h after the end of surgery. The red dashed lines represent the therapeutic concentration range of lidocaine 1–5 µg/mL, and the black dashed line represents the average and median (3 µg/mL) values of the therapeutic concentration range. “and Metabolites” is the weighted concentration of lidocaine, MEGX and GX, calculated as lidocaine + MEGX + 0.25 × GX. Box-whisker plot outliers are denoted by plus signs (+). |
Population Pharmacokinetic Modeling
During the model exploration process, the two-compartment model was more concise (OFV = 10208.28) and could better fit the concentration of lidocaine in Chinese hepatectomy patients. On the basis of the lidocaine model, two metabolite compartments were added with first-order elimination for the MEGX and GX (Figure 2). The significant covariates of the final pharmacokinetic model were identified as follows: total lidocaine dose affecting the concentrations of monoethylglycinexylide (MEGX), total lidocaine dose affecting the apparent distribution volume of the peripheral compartment and clearance of glycinexylide (GX) (Supplementary Material Table S2). The uncertainty of the parameters was considerably acceptable, and the median value obtained by bootstrapping was basically similar to the fixed effects, random effects, and residual values estimated by the model. In addition, not only was the 95% CI of the parameters within a reasonable range but the estimated value of each parameter in the final model also fell within the 95% CI (Table 2, Supplementary Material Table S3). The individual and population values of lidocaine, MEGX and GX predicted by the model were strongly correlated with the observed concentrations (Figure 3). The results of sensitivity analyses under different assumptions have been listed in Table S4 (Supplementary Material). The observed concentrations of lidocaine and active metabolites basically fell within the 95% CI of the predicted values obtained through 1000 simulations (Figure 4). The median value of the simulation prediction was consistent with the median value of the observed value and fell within the prediction CI, indicating that the model had good prediction performance. In addition, this study integrated diverse data from liver donation patients,33 obese patients,34 and patients undergoing major abdominal surgery,24 and preliminarily validated the applicability of the model across populations (Supplementary Material Figure S2). The metabolism of lidocaine depends on liver enzymes, and its metabolic pathway is highly conserved in different ethnic populations. The study in the American population by Crouch et al showed that the clearance rate of lidocaine decreased proportionally with residual liver tissue after liver resection,33 which is consistent with the prediction results of this model. This model has considered the influence of body weight through covariates. External validation shows that the observed data of 90% of obese patients are within the 95% confidence interval range of the model prediction, which meets the external validation criteria of the population pharmacokinetic model. Therefore, the validation results support the preliminary practicality of the model in obese patients, and the validation sample size of the extreme-weight population will be further expanded in the future.
 |
Figure 2 Schematic diagram of final model for lidocaine, MEGX, GX. Notes: The drug was administered into the central compartment (line topped with circle). Assuming that the apparent distribution volume (V1) of MEGX and GX were equal to central compartment (lidocaine). CL, lidocaine clearance; V2, apparent distribution volume of the peripheral compartment; CLD, inter-compartmental clearance. The formation of active metabolites was modeled through two metabolic compartments (MEGX and GX). Abbreviations: CLFM, the proportion of clearance for fraction metabolism of lidocaine to MEGX; CLE, elimination clearance of MEGX; CLEFM, the proportion of clearance for fraction metabolism of MEGX to GX; CLG, elimination clearance of GX. |
 |
Figure 3 Diagnostic scatter plot of the final model for lidocaine, MEGX, GX. Notes: The observed concentrations versus population-predicted concentrations and versus individual-predicted concentrations for lidocaine (A and B), MEGX (E and F) and GX (I and J), respectively. The black line represents the reference line (y = x) and is used to identify the deviation degree of the red line. The conditional weighted residual versus population predicted concentration and versus time for lidocaine (C and D), MEGX (G and H) and GX (K and L), respectively. Dashed and solid lines represent the reference line of y = ± 2 and y = 0, respectively. The red line indicates a locally weighted regression smoothing line. |
 |
Figure 4 Prediction-corrected visual predictive check (pcVPC) of final model of lidocaine (A), MEGX (B), GX (C). Notes: The observed values (black scatter points) were depicted with 50th percentile (red lines) and the 50th percentile predictions (black dashed lines) were depicted with the 95% confidence interval (blue shaded area). |
 |
Table 2 Population Pharmacokinetic Parameter Estimates and Median Parameters Value (5–95%) of Bootstrap of the Final Model |
Multiple testing corrections are generally not applied in population pharmacokinetic (PopPK) analyses, as their use (eg, Bonferroni correction) may result in excessive conservatism and reduced model sensitivity. Instead, PopPK models typically rely on statistical criteria such as the likelihood ratio test (LRT) or a decrease in the objective function value (OFV), as implemented in softwares like NONMEM, to control error rates, which is also the standard method recommended by regulatory authorities.35–37 These methods are based on statistical distributions that differ from those used in independent hypothesis tests. Furthermore, covariate selection in PopPK must be guided not only by statistical evidence but also by clinical plausibility (eg, the known relationship between renal clearance and creatinine clearance). A widely accepted methodological approach—often considered the gold standard—for systematic covariate evaluation and selection involves a stepwise procedure: forward selection followed by backward elimination. The final model is then validated using techniques such as visual predictive checks (VPC), rather than relying solely on p-values. Therefore, the primary objective of PopPK modeling is to develop models that are both mechanistically plausible and capable of accurate prediction, rather than achieving statistical significance alone.
Simulation and Weighted Lidocaine Exposure
The therapeutic concentration range of lidocaine is reportedly to be 1–5 µg/mL.10–13 To investigate the safe and effective therapeutic concentrations of lidocaine, MEGX and GX, the plasma concentrations per dose were simulated (1000 replicates) for a typical 60 kg, 55-year-old individual who had undergone a Pringle maneuver for 0.63 h. The simulation results for a 2.0 mg/kg loading dose accompanied by different infusion doses (1.0, 1.5, 2.0 and 3.0 mg/kg/h) show that the 95th percentile of the concentration of lidocaine at 0.2 h after administration exceeded 5.5 µg/mL, as shown in Figure 5Ci–iv). In addition, the results in Figure 5Aiv and Biv) show that at loading doses of 1.0 mg/kg and 1.5 mg/kg, respectively, as well as infusion doses of 3.0 mg/kg, plasma concentrations of lidocaine exceeding 5 µg/mL will last for 2 h. Considering the combined effect of lidocaine and its metabolites, the Cmax of the weighted concentrations exceeded 5 µg/mL at an infusion dose of 2 mg/kg/h (Figure 5Aiii and Biii), and the period when the weighted concentration of the loading dose of 1.5 mg/kg was greater than 5 µg/mL also lasted for nearly 1 h (Figure 5Biii).
 |
Figure 5 Simulations of lidocaine (blue) and weighted (purple) concentrations over time at different loading doses with infusion doses. Lines in the upper column show the concentration change at a loading dose of 1.0 mg/kg with infusion dose of 1.0 (Ai), 1.5 (Aii), 2.0 (Aiii) and 3.0 mg/kg/h (Aiv). Lines in the middle column show the concentration change at a loading dose of 1.5 mg/kg with infusion dose of 1.0 (Bi), 1.5 (Bii), 2.0 (Biii) and 3.0 mg/kg/h (Biv). Lines in the lower column show the concentration change at a loading dose of 2.0 mg/kg with infusion dose of 1.0 (Ci), 1.5 (Cii), 2.0 (Ciii) and 3.0 mg/kg/h (Civ). Notes: The black lines represent the median concentration and the red dashed lines represent the lidocaine therapeutic concentration range of 1 to 5 µg/mL, with the blue and purple area showing the 95% confidence interval of lidocaine, MEGX and GX. “and Metabolites” is the weighted concentration of lidocaine, MEGX and GX, calculated as lidocaine + MEGX + 0.25 × GX. |
The results of simulating long-term infusions of lidocaine at different doses during the postoperative stage after liver resection showed that as the dose increased, the concentration of the active metabolite MEGX increased more significantly than did the slow increase in lidocaine concentration (Figure 6), and the GX concentration remained stable between 0.01 and 0.1 µg/mL. When the infusion dose exceeded 1 mg/kg/h, the weighted concentration was significantly greater than that of lidocaine alone (Figure 6Av); however, when the infusion dose was 1.5 mg/kg/h, the highest weighted concentration reached 8.7 µg/mL, with the MEGX concentration already exceeding 5 µg/mL (Figure 6Avi). At each dose of lidocaine infusion, changes in the 95% CI range of lidocaine as well as small individual differences in plasma clearance might be explained by the active metabolites and covariates.
 |
Figure 6 The simulation shows the trend of changes in lidocaine (blue), MEGX (green) and GX (purple) concentrations over time during long-term infusion of lidocaine at doses of 0.15 mg/kg/h (Crouch et al33) and 0.3–1.5 mg/kg/h (Xu et al23) in the postoperative stage of liver resection. Notes: The black lines represent the median concentration and the red dashed lines represent the lidocaine therapeutic concentration range of 1 to 5 µg/mL, with the blue, green and purple area showing the 95% confidence interval of lidocaine, MEGX and GX. “and Metabolites” is the concentration of MEGX and GX. |
Discussion
The purpose of this study was to explore the effects of liver resection on the pharmacokinetics of lidocaine and its active metabolites and to propose a novel dosing regimen of lidocaine weighted activity metabolites, exploring whether the infusion rate of lidocaine needs to be adjusted by increasing or decreasing within a safe range during liver resection or after liver tissue separation.
This is the first description of the population pharmacokinetics of lidocaine, MEGX and GX in Chinese hepatectomy patients who received a continuous infusion of lidocaine. In this study, a two-compartment model with covariates was used to estimate the pharmacokinetic parameters, between-subject variability and residual variability. There is no significant difference between the lidocaine clearance estimated by the final model (26.1 L/h) and that calculated by the non-compartmental analysis (30.8 L/h).30 However, in terms of the volume of distribution, final modeling provides a more detailed description of the concentration–time distribution of lidocaine compared to non-compartmental analysis. The standard two-stage method for the non-compartment analysis, although further exploratory analysis was conducted, confused between-subject variability and estimation error; thus, between-subject variability estimated by the population pharmacokinetics model may be more unreliable. The population pharmacokinetic analysis indicated that lidocaine clearance was proportional to the size of the tumor, but the decreased clearance did not result in significantly greater lidocaine concentrations as lidocaine infusion was discontinued at the end of the surgery, and the plasma concentration of lidocaine rapidly decreased (Figure 1). A study was also used to describe the pharmacokinetics of lidocaine and its active metabolites in living liver donor patients in the United States.33 Although our study and the study of living liver donor patients are both targeted at hepatectomy patients, there are still some differences that are worth investigating here. There was a correlation between the remaining liver tissue and the decrease in lidocaine clearance.33 Our study also showed that the clearance of lidocaine decreases with increasing liver tumor size, which indirectly reflects the size of the remaining liver mass. Crouch et al hypothesized that lidocaine was completely converted into MEGX, followed by MEGX being fully converted into GX, which seemed implausible.33 Therefore, the estimated rate of lidocaine conversion to MEGX was 0.475 L/h in this study, rather than the estimated 33.0 L/h reported by Crouch et al. In addition, the lidocaine clearance estimated by our study (26.1 L/h) was 79% of the estimated clearance (33.0 L/h) for live liver donation patients. The gap with a clearance exceeding 20% may be because most patients with mild cirrhosis in our study experienced multiple Pringle maneuvers and complex liver hemodynamics, while living liver donation candidates were healthy volunteers who underwent strict liver function screening.
The population model was used to simulate different loading and infusion doses of lidocaine in a typical liver resection patient. To avoid the 95th percentile of lidocaine concentrations exceeding 5 µg/mL, the maximum dose of loading and continuous infusion lidocaine should not surpass 1.5 mg/kg and 1.5 mg/kg/h, respectively, based on the results of the simulation (Figure 5). Moreover, the results we simulated were in line with the recommended dosage for infusion according to the international consensus statement on the efficacy and safety of intravenous lidocaine.31 This finding suggested that the recommended dosage range may still pose some risks in certain special populations, such as our patients who underwent liver resection. The difference in the recommended infusion dose may be because most patients with mild cirrhosis in our study experienced multiple Pringle maneuvers and had complex liver hemodynamics. Liver cirrhosis may lead to alterations in cytochrome P450, especially a decrease in the activity of the enzymes CYP1A2 and CYP3A4.38 The metabolism of lidocaine and MEGX relies not only on enzymes but also mainly on liver blood flow,27 which is easily affected by repeated Pringle maneuvers and controlled low central venous pressure. Thus, although this recommendation has also been applied in Chinese patients, to ensure the safety of hepatectomy patients and maintain an effective therapeutic concentration, high infusion doses should be used with some caution. Although the main metabolites (MEGX and GX) of lidocaine are active, their relationship with the toxicity and efficacy of lidocaine has not been fully recognized clinically. The population study on patients undergoing cardiac surgery conducted by Hsu et al only established a two-compartment model that well describes lidocaine concentrations, ignoring the role of active metabolites.39 This study has strengthened the focus on active metabolites, especially the simulated administration recommendations based on lidocaine weighted concentration of active metabolites.
A comparison of the observed lidocaine concentrations (1.9 µg/mL vs 2.1 µg/mL) and weighted concentrations (2.2 µg/mL vs 2.3 µg/mL) during liver resection and after liver tissue separation revealed that the concentration was slightly greater but not significant greater (Figure 1Bi and 1Ci). The simulated results were also similar (Figure 1Bii and 1Cii). In addition, the lidocaine concentration and weighted concentration rapidly decreased after the end of infusion. Therefore, we thought that there was no need to adjust the lidocaine infusion rate for hepatectomy patients with mild cirrhosis during liver resection and after liver tissue separation.
The final model was used to simulate the concentrations of lidocaine and its active metabolites after long term infusion of lidocaine in the patient-controlled i.v. analgesia (PCIA) pump used to alleviate postoperative pain in hepatectomy patients within 72 h after surgery. The concentration of lidocaine and its active metabolites over time tended to be relatively stable after approximately 24 hours of infusion (Figure 6). The simulation results showed that long-term infusion of lidocaine leads to the accumulation of the active metabolite MEGX, which may inhibit the biological transformation of lidocaine.40 When the continuous infusion dose exceeded 0.75 mg /kg/h, the steady-state concentration (Css) of MEGX was significantly higher than that of lidocaine (Figure 6Aiv). When the continuous infusion dose reached 1.5 mg/kg/h (Figure 6Avi), the Css of MEGX exceeded the toxic concentration, but this may have pose a large risk to patients despite reducing their pain. Some clinical studies have benefited from prolonging infusion time without adjusting the infusion dose, which may pose risks to patients because the accumulation of the active metabolite MEGX has not been considered.41,42 According to the simulation results, it is known that when a long-term infusion of lidocaine exceeds 24 hours due to the accumulation of the active metabolite MEGX, it is necessary to pay attention to whether the weighted concentration exceeds the toxicity threshold. Thus, if long-term infusion for more than 24 hours is needed, the infusion rate needs to be adjusted to half of the original value to avoid the risk of toxicity, which is consistent with safety recommendations.41,42 The occurrence of an infusion dose as high as 1.5 mg /kg/h is because, within 72 hours of infusion, 21 mg of lidocaine is injected every 15 min by pressing the PCIA pump, which may pose great risks to patients. The concentrations of lidocaine and MEGX at a background dose of 0.3 mg /kg/h were close to 1 µg/mL, but they had not reached the therapeutic concentration range, which may have led to insignificant improvements in patient pain and frequency increase of pressing the PCIA pump. The background dose of the PCIA pump can be adjusted according to the simulation results to maintain the lidocaine concentration within the therapeutic concentration range and avoid lidocaine and weighted concentrations exceeding the toxicity threshold. This opinion needs to be validated through subsequent pharmacokinetic and pharmacodynamic studies. The accumulation of metabolites during long-term lidocaine infusion is significant. To avoid the occurrence of lidocaine-related toxicity symptoms, in addition to monitoring lidocaine, active metabolites also need to be monitored during long-term infusion, and the possibility of incorporating these findings into the administration guidelines is also necessary. MEGX, as an alternative to dynamic liver function assessment, can directly reflect the metabolic activity and functional reserve of liver cells in terms of its generation rate.43 MEGX retains pharmacological activity similar to lidocaine, and continuous infusion or administration carries a risk of accumulation, which may synergistically increase the risk of neurological/cardiotoxicity, especially for patients with small residual liver volume. Therefore, monitoring MEGX can optimize the dosage and timing of lidocaine infusion. By combining MEGX concentration with imaging liver volume measurement, residual liver function can be quantified and the survival rate of transplanted liver can be evaluated.33,43 As a further metabolite of MEGX, although its concentration is low, GX may accumulate when liver function is impaired, and a comprehensive evaluation of total toxicity is needed. Although stopping medication during surgery can avoid delayed clearance of metabolites, the concentration of metabolites still needs to be monitored during postoperative liver function recovery, especially when combined with renal dysfunction (GX has a half-life of up to 10 hours).20 Although there have been studies on the use of lidocaine in Child-C grade non hepatectomy patients, this study only involved injections rather than long-term infusions,29 and there have been no pharmacokinetic studies of lidocaine pumped into patients with moderate-to-severe liver cirrhosis. It is possible to extrapolate to other similar populations through physiologically based pharmacokinetics, but due to racial differences in enzyme activity, it may be limited in generalizability.
This study had several limitations. First, the sample size of this study was relatively small, and the study was limited to a single center. Second, the apparent distribution volumes of the MEGX and GX were set equal to that of the lidocaine because the actual values were not available. Thus, this approach might lead to deviations in the estimated clearance of active metabolites and in the distribution volume of the peripheral compartment. The administration of active metabolites might solve this problem, but MEGX and GX are currently unavailable for human use. Third, because of insufficient sampling time, the blood concentration of lidocaine was not measured immediately after injection (Figure 1Bi), resulting in deviation between the peak time and concentration, and the inability to fully observe the pharmacokinetic characteristics of GX. Adding the sampling time immediately after administration and 24 to 48 hours after administration might provide sufficient pharmacokinetic data for active metabolites. Fourth, our study provided information only on tumor size provided by preoperative imaging and did not evaluate the remaining liver after surgery. Estimating the changes in clearance in preoperative and postoperative liver tissue can provide a more reasonable analysis of the impact of surgical procedures and hepatectomy on pharmacokinetic parameters. Therefore, further research will continue after addressing these limitations. Thus, these results provide a basis for further prospective clinical trials to better elucidate the pharmacokinetic effects of liver resection on lidocaine and its active metabolites.
In conclusion, this study developed a two-compartment model that adequately describes the concentrations of lidocaine, MEGX and GX in Chinese hepatectomy patients. This study proposes for the first time the integration of lidocaine concentration with active metabolites and simulation-based dosing recommendations. During the 24-hour medication period for Chinese hepatectomy patients, the recommended safe dosage includes a loading dose not exceeding 1.5 mg/kg and an infusion dose not exceeding 1.5 mg/kg/h. Although the dose simulation results and adjustments are in line with the recommended guidelines, these simulation results are derived from the integration of active metabolites with lidocaine. Therefore, monitoring of active metabolites in addition to lidocaine is also necessary for continuous infusion of lidocaine. The findings of this study will lay the foundation for further research on the improvement of postoperative pain in patients undergoing liver resection through continuous infusion of lidocaine with a larger sample size for validation.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no competing interests in this work.
References
1. Zhang B, Zhang B, Zhang Z, et al. 42,573 cases of hepatectomy in China: a multicenter retrospective investigation. Sci China Life Sci. 2018;61(6):660–670. doi:10.1007/s11427-017-9259-9
2. Behman R, Cleary S, Mchardy P, et al. Predictors of post-operative pain and opioid consumption in patients undergoing liver surgery. World J Surg. 2019;43(10):2579–2586. doi:10.1007/s00268-019-05050-7
3. Gan TJ. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J Pain Res. 2017;Volume 10:2287–2298. doi:10.2147/JPR.S144066
4. Shea RA, Brooks JA, Dayhoff NE, et al. Pain intensity and postoperative pulmonary complications among the elderly after abdominal surgery. Heart Lung. 2002;31(6):440–449. doi:10.1067/mhl.2002.129449
5. Wheatley RG, Schug SA, Watson D. Safety and efficacy of postoperative epidural analgesia. Br J Anaesth. 2001;87(1):47–61. doi:10.1093/bja/87.1.47
6. Pitkänen MT, Aromaa U, Cozanitis DA, et al. Serious complications associated with spinal and epidural anaesthesia inF inland from 2000 to 2009. Acta Anaesthesiol Scand. 2013;57(5):553–564. doi:10.1111/aas.12064
7. Wrighton LJ, O’Bosky KR, Namm JP, et al. Postoperative management after hepatic resection. J Gastrointest Oncol. 2012;3(1):41–47. doi:10.3978/j.issn.2078-6891.2012.003
8. Beaussier M, Delbos A, Maurice-Szamburski A, et al. Perioperative use of intravenous lidocaine. Drugs. 2018;78(12):1229–1246. doi:10.1007/s40265-018-0955-x
9. Dunn LK, Durieux ME. Perioperative use of intravenous lidocaine. Anesthesiology. 2017;126(4):729–737. doi:10.1097/ALN.0000000000001527
10. Hodgman T. Lidocaine. In: Cohen H, editor. Casebook in Clinical Pharmacokinetics and Drug Dosing. New York, NY: McGraw-Hill Education; 2015.
11. Horvat S, Staffhorst B, Cobben JM. Intravenous lidocaine for treatment of chronic pain: a retrospective cohort study. J Pain Res. 2022;Volume 15:3459–3467. doi:10.2147/JPR.S379208
12. Wallace MS, Ridgeway BM, Leung AY, et al. Concentration-effect relationship of intravenous lidocaine on the allodynia of complex regional pain syndrome types I and II. Anesthesiology. 2000;92(1):75–83. doi:10.1097/00000542-200001000-00017
13. Wallace MS, Laitin S, Licht D, et al. Concentration-effect relations for intravenous lidocaine infusions in human volunteers: effects on acute sensory thresholds and capsaicin-evoked hyperpathia. Anesthesiology. 1997;86(6):1262–1272. doi:10.1097/00000542-199706000-00006
14. Thomson PD, Melmon KL, Richardson JA, et al. Lidocaine pharmacokinetics in advanced heart failure, liver disease, and renal failure in humans. Ann Intern Med. 1973;78(4):499. doi:10.7326/0003-4819-78-4-499
15. Corsini A, Bortolini M. Drug-induced liver injury: the role of drug metabolism and transport. J Clin Pharmacol. 2013;53(5):463–474. doi:10.1002/jcph.23
16. Delcò F, Tchambaz L, Schlienger R, et al. Dose adjustment in patients with liver disease. Drug Saf. 2005;28(6):529–545. doi:10.2165/00002018-200528060-00005
17. Benowitz NL, Meister W. Clinical pharmacokinetics of lignocaine. Clin Pharmacokinet. 1978;3(3):177–201. doi:10.2165/00003088-197803030-00001
18. Gianelly R, von der Groeben JO, Spivack AP, et al. Effect of lidocaine on ventricular arrhythmias in patients with coronary heart disease. N Engl J Med. 1967;277(23):1215–1219. doi:10.1056/NEJM196712072772301
19. Difazio CA. Biotransformation of lidocaine. Int Anesthesiol Clin. 1975;13(4):21–32. doi:10.1097/00004311-197513040-00004
20. Strong JM, Mayfield DE, Atkinson AJ, et al. Pharmacological activity, metabolism, and pharmacokinetics of glycinexylidide. Clin Pharmacol Ther. 1975;17(2):184–194. doi:10.1002/cpt1975172184
21. Strong JM, Parker M, Atkinson AJ. Identification of glycinexylidide in patients treated with intravenous lidocaine. Clin Pharmacol Ther. 1973;14(1):67–72. doi:10.1002/cpt197314167
22. Thomson AH, Elliott HL, Kelman AW, et al. The pharmacokinetics and pharmacodynamics of lignocaine and MEGX in healthy subjects. J Pharmacokinet Biopharm. 1987;15(2):101–115. doi:10.1007/BF01062338
23. Xu Y, Ye M, Liu F, et al. Efficacy of prolonged intravenous lidocaine infusion for postoperative movement-evoked pain following hepatectomy: a double-blinded, randomised, placebo-controlled trial. Br J Anaesth. 2023;131(1):113–121. doi:10.1016/j.bja.2023.03.026
24. Koppert W, Weigand M, Neumann F, et al. Perioperative intravenous lidocaine has preventive effects on postoperative pain and morphine consumption after major abdominal surgery. Anesthesia Analg. 2004;98(4):1050–1055. doi:10.1213/01.ANE.0000104582.71710.EE
25. Kuo CP, Jao SW, Chen KM, et al. Comparison of the effects of thoracic epidural analgesia and i.v. Infusion with lidocaine on cytokine response, postoperative pain and bowel function in patients undergoing colonic surgery. Br J Anaesth. 2006;97(5):640–646. doi:10.1093/bja/ael217
26. Aldrete JA, Homatas J, Boyes RN, et al. Effects of hepatectomy on the disappearance rate of lidocaine from blood in man and dog. Anesth Analg. 1970;49(5):687–690. doi:10.1213/00000539-197009000-00007
27. Orlando R, Piccoli P, De Martin S, et al. Cytochrome p450 1A2 is a major determinant of lidocaine metabolism in vivo: effects of liver function. Clin Pharmacol Ther. 2004;75(1):80–88. doi:10.1016/j.clpt.2003.09.007
28. Huet P, Villeneuve J. Determinants of drug disposition in patients with cirrhosis. Hepatology. 1983;3(6):913–918. doi:10.1002/hep.1840030604
29. Orlando R, Piccoli P, De Martin S, et al. Effect of the CYP3A4 inhibitor erythromycin on the pharmacokinetics of lignocaine and its pharmacologically active metabolites in subjects with normal and impaired liver function. Br J Clin Pharmacol. 2003;55(1):86–93. doi:10.1046/j.1365-2125.2003.01718.x
30. He C, Jin Y, Zhang Y, et al. The pharmacokinetics and safety of lidocaine in liver cancer patients undergoing hepatic resection. Eur J Clin Pharmacol. 2023;79(6):829–839. doi:10.1007/s00228-023-03498-0
31. Foo I, Macfarlane AJR, Srivastava D, et al. The use of intravenous lidocaine for postoperative pain and recovery: international consensus statement on efficacy and safety. Anaesthesia. 2021;76(2):238–250. doi:10.1111/anae.15270
32. Jin Y, He C, Di X, et al. Simultaneous determination of lidocaine and its active metabolites in plasma by UPLC-MS/MS and application to a clinical pharmacokinetic study in liver cancer patients with laparoscopic hepatectomy. J Chromatogr B Analyt Technol Biomed Life Sci. 2022;1207:123362. doi:10.1016/j.jchromb.2022.123362
33. Crouch CE, Wilkey BJ, Hendrickse A, et al. Lidocaine intraoperative infusion pharmacokinetics during partial hepatectomy for living liver donation. Anesthesiology. 2022;138(1):71–81. doi:10.1097/ALN.0000000000004422
34. Tognolini AR, Liu X, Pandey S, et al. Dosing optimisation of intravenous lidocaine in patients with class 1–3 obesity by population pharmacokinetic analysis. Anaesthesia. 2025;80(5):511–521. doi:10.1111/anae.16531
35. U.S. Food and Drug Administration. Guidance for industry: population pharmacokinetics (Draft guidance). Available from: Https://www.fda.gov/media/128793/download.
36. Pharmaceuticals and Medical Devices Agency. Guideline on population pharmacokinetic and pharmacodynamic analysis. Available from: Https://www.pmda.go.jp/files/000230073.pdf#page=2.
37. European Medicines Agency. Guideline on reporting the results of population pharmacokinetic analyses. Available from: Https://www.ema.europa.eu/en/documents/scientific-guideline/guideline-reporting-results-population-pharmacokinetic-analyses_en.pdf.
38. Elbekai RH, Korashy HM, El-Kadi AOS. The effect of liver cirrhosis on the regulation and expression of drug metabolizing enzymes. Curr Drug Metab. 2004;5(2):157. doi:10.2174/1389200043489054
39. Hsu Y, Somma J, Newman MF, et al. Population pharmacokinetics of lidocaine administered during and after cardiac surgery. J Cardiothorac Vasc Anesth. 2011;25(6):931–936. doi:10.1053/j.jvca.2011.03.008
40. Suzuki T, Fujita S, Kawai R. Precursor-metabolite interaction in the metabolism of lidocaine. J Pharm Sci. 1984;73(1):136. doi:10.1002/jps.2600730140
41. Wongyingsinn M, Baldini G, Charlebois P, et al. Intravenous lidocaine versus thoracic epidural analgesia. Reg Anesth Pain Med. 2011;36(3):241–248. doi:10.1097/AAP.0b013e31820d4362
42. Kaba A, Laurent SR, Detroz BJ, et al. Intravenous lidocaine infusion facilitates acute rehabilitation after laparoscopic colectomy. Anesthesiology. 2007;106(1):11–18,5–6. doi:10.1097/00000542-200701000-00007
43. Ercolani G, Grazi GL, Calliva R, et al. The lidocaine (MEGX) test as an index of hepatic function: its clinical usefulness in liver surgery. Surgery. 2000;127(4):464–471. doi:10.1067/msy.2000.104743
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.